Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Ready, Set, Coach: A Mixed Methods Pilot Study Exploring the Impact of Implementation Coaching to Optimize the Allied Health Assistant Workforce in Public Health Settings
Authors Whelan L ![]() , McLean SL, Edwards A
, McLean SL, Edwards A ![]() , Glagovski S, Huglin J, Golder JE, Foster AM
, Glagovski S, Huglin J, Golder JE, Foster AM
Received 20 August 2025
Accepted for publication 30 January 2026
Published 27 March 2026 Volume 2026:19 562058
DOI https://doi.org/10.2147/JMDH.S562058
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr David C. Mohr
Lucy Whelan,1 Sharon L McLean,1 Alexandra Edwards,1,2 Sandra Glagovski,1,2 Jessica Huglin,1 Janet E Golder,1,3 Abby M Foster1,2,4
1Allied Health Workforce Innovation, Strategy, Education & Research (WISER) Unit, Monash Health, Melbourne, VIC, Australia; 2School of Primary and Allied Health Care, Monash University, Frankston, VIC, Australia; 3Department of Nutrition, Dietetics and Food, School of Clinical Sciences, Faculty of Medicine, Nursing and Health Sciences, Monash University, Notting Hill, VIC, Australia; 4School of Allied Health, Human Services & Sport, La Trobe University, Melbourne, VIC, Australia
Correspondence: Lucy Whelan, Allied Health Workforce Innovation, Strategy, Education & Research (WISER) Unit, Monash Health, 400 Warrigal Road, Heatherton, VIC, 3202, Australia, Email [email protected]
Background: The Victorian Allied Health Assistant Workforce Project delivered eighteen recommendations and accompanying resources supporting optimal utilization of allied health assistants (AHAs) across health, aged care, and disability sectors, in late 2022. Uptake of these evidence-based, ready-to-use resources in public health settings was yet to be evaluated. This was the impetus for an implementation coaching program, delivered to enhance application of the developed recommendations and resources. The aim of this project was to design, deliver and evaluate the impact of a pilot implementation coaching program to embed and put into practice the Victorian Allied health assistant workforce recommendations and resources in a public health setting.
Methods: A non-experimental, pre- and post- mixed methods design was used to evaluate the outcomes of the tailored implementation coaching program. Measures included Organizational Readiness for Implementing Change (ORIC) scale survey, a bespoke workforce survey, the Goal Attainment Scale (GAS), post implementation interviews, and research team reflections on the process.
Results: Six Victorian public health organizations participated in the pilot implementation program. Findings indicate attainment of positive change in GAS scores following the sixteen-week implementation program (p=0.001), with pre-intervention ORIC scores an unreliable indicator of potential change success. Factors pertaining to size and geography of coaching participant (CP) pair’s organization, local managerial or executive support of the change, experience and influence of the CPs and the project coaching team’s (PCT) experience and credibility, all have impact on successful implementation coaching outcomes for the optimization of the AHA workforce in a Victorian context.
Conclusion: This research provides new insights into the value of coaching to support the implementation of statewide workforce recommendations and resources in public health settings. This study provides a model for other organizations to consider and to reference when embarking on the process of implementing workforce recommendations and resources, directed at workforce optimization.
Keywords: allied health, allied health assistant, support workforce, implementation, coaching, optimization, healthcare
Introduction
Allied health assistants (AHAs) are an established support workforce across Victorian health settings, supporting Allied health professionals (AHPs) to meet workforce and workload demands.1 Engagement of AHAs to support AHPs enables an efficient allocation of workforce resources.2,3 Innovative and contemporary models of care have demonstrated that the optimal utilization of AHAs gives greater access to care for a larger number of consumers, whilst allowing AHPs to work at the top of their scope of practice.2
AHAs have been the subject of extensive research over the last several years,1,2,4–10 in the face of marked AHP workforce shortages.11 Proposed flexible models of care,6,8 to ensure service equity in an environment of scarce resource and growing demand,1,11,12 have been discussed, with particular focus on the barriers and enablers to optimizing the AHA workforce1,5 and feasible methods by which to support optimization of this workforce.6,10
Development of the Allied Health Assistant Workforce Optimization Recommendations and Resources
Prior studies identified multiple barriers and enablers to optimizing the AHA workforce1,5,10 and resources that may assist in addressing these barriers.10 In response, the Department of Health in the state of Victoria, Australia recently released a suite of recommendations and resources to optimize the AHA workforce,13 building on previously released frameworks.14 This suite of recommendations and resources aims to address known barriers and enablers to optimizing the AHA workforce in health, disability, and aged care settings across Victoria. Huglin et al1 identified that historically, frameworks without associated resources for implementation have not been well adopted. Furthermore, Whelan et al10 identified that these resources developed as part of this project were well received by the health sector and were deemed ready-to-adopt. Implementation coaching is one method that may support the translation of recommendations and resources into practice.15
Supporting Optimization of the AHA Workforce Through Implementation Coaching
Implementation coaching has been used in other health workforce contexts with a degree of success.16,17 The goal of implementation training is to embed target recommendations into an organization’s culture and practices, rather than just implementing them as a one-time event. There is not a single approach considered best practice for implementation coaching. The term coach, implementation advisor or facilitator refers to an expert either internal or external to the organization who shares their knowledge and expertise with others to achieve a specific outcome.12
The experience and credibility of the coach,18 the ability to engage and develop a rapport with those being coached,18 the ability to access and provide supporting resources and the time allocated to the coaching program12 are all factors identified as impacting the outcome of the coaching program. Conversely, there are factors beyond the coach’s influence. These include the ability to directly influence the change process in organizations where they have no authority,19 the level of expertise of those being coached,20 and the maintaining of momentum once the coaching program has concluded.19 These principles, combined with available resources, informed the design and delivery of a novel sixteen-week implementation coaching program.
While recommendations and resources are readily available and considered fit-for-purpose,10 the impetus and time required to implement these may be lost in the competing demands placed on a public health service. To date, the literature is limited regarding the impact implementation coaching can have on the uptake of healthcare workforce recommendations.
This pilot study delivered implementation coaching to six Victorian public health services to understand the different experiences of this cohort in implementing the recommendations and resources and whether implementation coaching had an impact on AHA workforce optimization in these settings.
The research question for this study was: what is the impact and experience of implementation coaching on the optimization of AHA workforce in the Victorian public health setting?
Materials and Methods
Study Setting
A pair of coaching participants (CPs) from six Victorian public health services (three metropolitan, scoring MM1, and three regional, scoring MM2 or MM3 on the Modified Monash Model21 (which is a country-specific model for defining rural and remote areas with a range of MM1 as a major city up to MM7 which is very remote), took part in the implementation coaching program, delivered via a combination of online and face-to-face modalities in 2023, to optimize their AHA workforce in alignment with the Victorian AHA Workforce Recommendations and Resources.13
Study Design
A non-experimental, pre- and post- concurrent mixed methods design was used to evaluate the experiences and outcomes of the pilot tailored implementation coaching program. This study was conducted from an interpretivist perspective, utilizing a combination of validated outcome measures, a purpose-designed workforce survey, semi-structured interviews, and reflective journals.
The pilot implementation program had a pre-determined format, modality, frequency and duration, modelled on coaching factors known to have positive impacts, as highlighted previously.12,18 The content of the coaching was co-designed with the CPs, based on their context-specific goals and was iterative in nature.
Research Team Positionality and Reflexivity Statement
Research team members participated in a reflexivity exercise as described by Barry et al20 at the outset of this study to establish a shared understanding of individual team member perspectives related to the project. The research team chose this reflexivity tool over the more sophisticated methods of Braun and Clark,22 as it was a simpler reflexivity exercise for a team with a range of research expertise. Team members represented many years of AHP and AHA clinical practice, education, and training, with varied levels of operational, governance, policy, leadership, and research experience. The research team met regularly throughout the project to review data collection, analysis, and interpretation as a collective.
Study Participants and Recruitment Method
In October 2022, all Victorian Public Health Services were invited to submit an Expression of Interest (EOI) form to participate in the implementation coaching program commencing in 2023. EOI forms were distributed by the research team via the Monash Health Victorian AHA Workforce project webpage, Email contact lists, and social media.
Eligibility required participating health organizations to: (a) be in the state of Victoria; (b) be a public health service; (c) employ both AHPs and AHAs; and (d) complete the expression of interest process. No exclusion criteria were imposed.
EOIs provided demographic information including submitter’s work role (AHA, AHP or allied health leader), their location (metropolitan or regional Victoria) and the key areas which they felt required optimization for their AHA workforce. Using a purposive maximum variation sampling approach, with size of the allied health assistant workforce and location (metropolitan/regional status) considered as factors for variation, an EOI assessment matrix was used in consultation with the Victorian Department of Health to determine the six public health services who would participate in the coaching program.
Six organizations were offered an informal interview to further discuss their EOI and clarify expectations of the coaching recipients. These expectations were that the CP team included an AHA and AHP and that the team dedicated eight hours per week to the coaching program over the sixteen weeks. All six organizations were offered a position in the coaching program and organizational requirements led two to start in February (Cohort A) and four in July (Cohort B) (See Figure 1).
 |
Figure 1 Implementation coaching selection process. |
Once a health organization confirmed that they wished to participate in the implementation coaching program, a Participant Consent and Information Form was provided to each CP, along with a detailed verbal explanation of the research, its aims, and likely outcomes.
All AHPs, AHAs and program managers employed at the participating health organizations were invited to participate in the program evaluation. The size of these populations was ascertained prior to survey distribution, with variation across health services anticipated.
Procedure
Figure 2 depicts the outcome measures used at each stage of implementation coaching.
 |
Figure 2 Implementation coaching outcome measures. |
Screening
As part of the EOI process, potential participants were required to complete the Progress measurement tool resource for health13 to establish their progress to date and identify gaps against the relevant Victorian AHA Workforce Recommendations.
Pre-Implementation Coaching
A pre-implementation workforce implementation survey based on the Theoretical Domains Framework (TDF),23 (Supplementary File 1) was distributed to participating health organizations four weeks prior to commencing the implementation coaching program. Researchers requested that the health organization circulate the 23-item, Likert-scale Microsoft Forms survey via Email to all AHPs and AHAs across their organization. It was anticipated that the survey, designed to evaluate barriers and enablers to implementation, would take approximately 10–15 minutes to complete.
In addition, CPs selected to participate in the implementation coaching program were required to undertake a baseline measure of organizational readiness prior to commencing the program. The Organizational Readiness for Implementing Change (ORIC) scale24 is a brief, reliable and valid measure to assess organization readiness for change based on four domains: change-specific efficacy, appropriateness, management support, and personal valence.24
Prior to commencement, each CP took part in a verbal scoping survey further examining organizational practice across each of the five areas of Victorian AHA recommendations;13 pre-employment training, workforce planning and governance, consumer-centered therapy and supports, recruitment and induction, workplace training, and development (Supplementary file 2).
Implementation Coaching
The sixteen-week implementation program was delivered online by the project coaching team (PCT), with sessions held weekly. Site visits by the PCT were offered to all CPs.
The initial coaching meeting reviewed local AHA and AHP survey findings and undertook a process of goal setting. CPs established six to eight Specific, Measurable, Achievable, Relevant and Time-bound (SMART) goals6,25 aligned to the initial scoping survey and the Victorian workforce recommendations.13
These goals formed the foundation of the individualised implementation coaching programs. For each of the goals, the CP and PCT together devised a series of actions, that intended to create change within the CP’s organization.
Progress towards achievement of the SMART goals was measured using the Goal Attainment Scale (GAS),26 as per the procedure described by Turner-Stokes.9 Phases 1–4 (identify goals, weight goals, define the expected outcomes, scoring baseline and interval scoring) occurred in the initial coaching session.9 Scoring was influenced by both the importance of the goal and the perceived difficulty to attain the goal. GAS data was collected manually during the initial, midway, and final coaching sessions. The data was de-identified for analysis.
A reflective journal was kept by the PCT (SM, SG, AE, and LW) throughout the course of the implementation coaching initiative.
Post-Implementation Coaching
Following the completion of the implementation coaching program, goal attainment scoring (Phase 5 of the procedure described by Turner-Stokes, 2014) was undertaken against each SMART goal using the GAS.
A post-implementation workforce implementation survey (modified from the pre-implementation workforce survey; see Supplementary file 1) was distributed to all AHPs and AHAs employed by participating health organizations two weeks following the final implementation coaching session. The purpose of this survey was to understand any immediate change in attitude/perception of the local workforce.
Two researchers (AMF and JG), independent of the coaching team, facilitated the in-depth semi-structured individual or dyadic interviews with CPs to understand their experience of taking part in the implementation coaching program. An interview guide (see Supplementary file 3) was used to inform the interviews. All interviews were conducted online, recorded and transcribed via Microsoft Teams and de-identified prior to analysis. Interviews lasted approximately one hour. Post-interview debriefing notes were completed by the interviewers after each interview and discussed with the research team to inform analysis.
Data Analysis and Integration
Informally, data were used throughout the pilot implementation coaching program to inform goal setting, content design, and reiteration of SMART goals as necessary over the coaching period.
Formal data analysis was undertaken on outcome measures and qualitative data, as outlined in Table 1. Due to the exploratory nature of this research, sample size was pragmatically determined to meet feasibility requirements. No power calculations were undertaken. ORIC data was analyzed using descriptive statistics. GAS data was analyzed using a Wilcoxon signed-rank test. Employee implementation survey data were analyzed using a chi-square test to ascertain the differences and the magnitude of these differences from pre- to post-implementation coaching. Statistical analysis was supported by a biostatistician external to the research team. Data was analysed individually for each CP and each phase and then integrated for final analysis and interpretation.
 |
Table 1 Data Analysis of Mixed Methods Study |
De-identified transcripts of the in-depth interviews were analyzed in NVivo (version 14).27 Data was coded using a deductive content analysis, with data mapped to the TDF by two researchers (AMF and JG). A sample of the transcripts were coded collaboratively to establish a shared understanding of the data and the coding system. The TDF domains most relevant to AHA workforce implementation were identified based on (a) the frequency of specific domains, (b) the strength of responses provided, and (c) presence of conflicting themes between participants.23
Ethical Considerations
Reporting of study findings was informed by the Standards for Mixed Methods Reporting in Rehabilitation & Health Sciences (MMR-RHS).28 This study was conducted in accordance with the Declaration of Helsinki. Ethical approval was granted by the Monash Health Human Research Ethics Committee (RES-20-0000-356 L / ERM 64899).
Results
A total of fourteen EOIs were received from health services based in Victoria. Six of these health organizations were invited to participate in the pilot implementation coaching program. Six organizations participated: three regional (1, 2, 6) and three metropolitan (3, 4, 5), evenly split between smaller (one to two sites) and multi-site organizations. Each health service allocated one AHA and one AHP as a CP in the program. Outcome measures and observations are summarized in Table 2.
 |
Table 2 Summary of Outcome Measures and Observations |
Organizational Readiness for Change
Variation in readiness to change scores was observed across (mean 48, range 38–57). Commitment and efficacy scores showed minimal differences by size or geographical location (Supplementary file 4).
Implementation Coaching Participation
Weekly online coaching sessions were held for each CP over sixteen weeks. Session attendance rate was high (mean attendance rate 91%), and the average length of sessions was forty minutes (range 15–90). Time associated with implementation activities undertaken by CPs outside of coaching sessions was not recorded.
Workforce Perceptions of Barriers and Enablers to Implementation of AHA Recommendations and Resources
On statistical analysis of the pre and post AHA survey results for the six organizations, the survey item “The Allied health assistant role is well respected in my workplace” was the only item to gain statistically significant change (p=0.036; Supplementary file 5.
Progress Towards Achievement of AHA Optimization Recommendations
CPs identified SMART goals across the five Victorian Allied Health Assistant Workforce Recommendations domains (See Table 3).
 |
Table 3 SMART Goal Comparison Across Six Participating CPs |
All six CPs identified context-specific SMART goals in three common areas; 1) developing competency based-training; 2) aligning recruitment and orientation to Victorian recommendations; and 3) establishing a delegation framework. Non-parametric testing demonstrated significant positive change in pre-post coaching GAS scores of these three common SMART goals across all six CPs (see Table 4).
 |
Table 4 SMART Goal GAS Scores Pre and Post Coaching (with Significance Set at P< 0.05) |
Each CP made progress in implementing the Victorian AHA Workforce Recommendations and utilizing the resources as required throughout the sixteen-week coaching period (see Table 5). The group mean (SD) difference in GAS scores 22.8 (8.2) points, indicating a positive change post coaching (p=0.001).
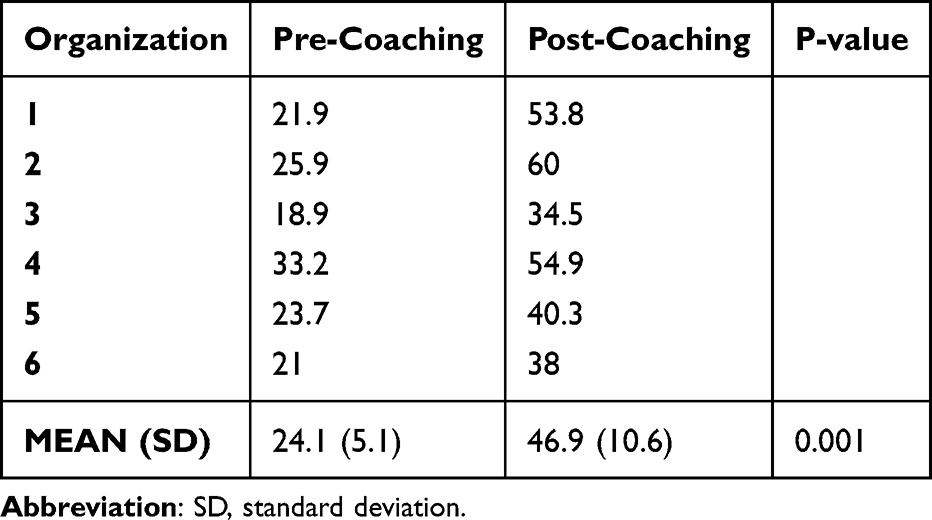 |
Table 5 Individual Organization and Mean (SD) Goal Attainment Scale (GAS) Measures for Coaching Participants (n=6) Pre and Post Coaching (with Significance Set at P< 0.05) |
The Relationship Between Organizational Readiness and Goal Attainment
Organizational readiness to change was not a reliable indicator of ability to change and adopt resources within this study. Organization 1 (regional) had the highest overall ORIC score reported as 57, and a large change in GAS of 31, while Organization 5 (metropolitan) had the second highest overall ORIC score reported as 53, yet one of the smallest changes in GAS of 16.6 (see Table 4 below). No significant relationship was found between ORIC scores and GAS changes (Supplementary file 4).
Perceptions of Barriers and Enablers to Implementing Change
Analysis of the PCT reflective journal and post-coaching interviews with CPs are presented below. They identify barriers and enablers to implementation, through the lens of the TDF.
From Overwhelmed to Supported: Emotional Change Across the Coaching Period
Commencing in the implementation coaching program, many CPs described emotions including feeling “borderline overwhelm[ed.] so rapid and intense was the first few weeks” (AHAMet5). The PCT observed that the experience of overwhelm was exacerbated when the requirement of coaching and clinical caseloads resulted in divided memory, attention, and decision processes. This was quickly alleviated, however, with support from the project team.
The Development of Knowledge and Skills Built Self-Belief in Capabilities
CPs found coaching enhanced their knowledge and skills pertaining to AHA workforce optimization. At the commencement of the coaching program, participants described having “some ideas of some work that we needed to do” (AHPMet5) but finding that “some of the language [was] quite new and it took a while for me to get my head around where everything fitted in together” (AHAReg1). Similarly, the PCT observed that CPs without prior project experience found the pace and structure of the program challenging.
For recommendations CPs felt unfamiliar with, knowledge was built through interactions with the PCT. CPs felt that “having the [coaching] team explain things well, that was really good” (AHAMet5). In addition, CPs reported that implementation coaching improved their skills required for implementation of the AHA recommendations and resources, reflecting on “the processes we’ve put in place to get to where we are” (AHAMet3). By the end of the coaching period, CPs held local expertise in the AHA workforce, enhancing their belief about capabilities to create change: “the managers are now asking me about [AHA workforce issues] and I can give them the appropriate advice” (AHPMet5).
The Influence of Organizational Size and Structure on Change
The coaching program supported CPs to navigate challenges related to the environmental context and resources. This involved navigating complex organizational structures and processes in which changes need to “go through multiple departments, multiple levels, be reviewed” (AHAMet3). The PCT observed that, in contrast, smaller health organizations saw change occur at a faster rate, with less apparent barriers.
Where knowledge of the environment was limited, such as in newly amalgamated organizations or when CPs were new to the organization themselves, the PCT observed that restricted relationships and organizational background context knowledge made progress difficult across the sixteen-week program.
Interpersonal Processes That Influenced Behaviour Change
The PCT observed social influences shaping implementation. Where close working relationships were observed between the AHA and AHP within the CP pair, progress over the coaching period was enabled and cultural shift within the organization was more likely. When collaborative relationships evolved in the latter weeks of coaching, PCTs observed that progress within the action log became more rapid.
CPs felt that having a dedicated PCT allowed them to “really sink their teeth into the project” (AHPReg6). Instances where leadership support for the project was high, characterised by “buy in from a lot of operational and line managers” (AHPMet5), and strong and direct managerial support created a culture for change. Streamlined communication channels to the leadership team, providing the ability to speak directly to leadership, highlighting the importance of the project, and enabling any request for change to be addressed promptly, was observed to be of benefit by the PCT.
All CPs reported that implementation was both shaped by, and created the beginnings of, positive change in organizational culture pertaining to AHA identity and value. The PCT observed that one organization benefited from having a centralised AHA governance structure in place prior to commencing coaching, ensuring dedicated time was allocated to the project. The inclusion of AHAs in the program was described as “a historical sort of precedent” (AHAMet3) for AHAs to be engaged in directing their own workforce, resulting in an incremental cultural shift and shaping CPs’ beliefs about consequences of the implementation: “we’re part of the way there, but I think we’re at the very start and it’s gonna take a bit of time to I suppose, develop those connections and change our culture a bit” (AHPMet5).
Coaching Provided a Structure to Enable Implementation
Coaching supported CPs to set goals, provided reinforcement, and enacted behavioural regulation. Support to establish and articulate clear goals allowed the PCT to “guide [CPs] in maybe the direction that we wanted to head but weren’t necessarily heading specifically” (AHPReg6). Some found the frequency of regular opportunity to maintain “kind of like, that accountability” (AHPMet4), while others felt the frequency increased pressure. Coaching sessions provided “some feedback and some support and some ideas on how to get where we’re going” (AHAMet3) as a means of reinforcement. One CP contrasted this with previous attempts at implementation within their organization:
Like, I know that there was a whole lot of work done in [our organization in the past]. and there are so many half-finished resources on our drives. so much work was done, but obviously the actual foundation wasn’t there because these things weren’t rolled out and there was so much work (AHPMet3)
Positive Intentions and Optimism for the Future
CPs came into implementation coaching with clear intentions that remained stable across the coaching period. Despite CPs acknowledging they still had “a few battles to keep going with in the future” (AHPReg6) to sustain change following coaching, they largely expressed optimism in their capacity to maintain change: “We’re really optimistic that we’ll be able to put something in place that supports AHA workforce ongoing so that the work we’ve started continues” (AHPReg1).
Discussion
This study offers new insights into how implementation coaching can optimize the AHA workforce in public healthcare settings. This was achieved by modifying the capability, opportunity, and motivation of CPs to enable the behaviour change necessary for the implementation of the statewide AHA workforce recommendations. To reflect this, the COM-B model29 is used to structure this discussion.
The Capability to Optimize the AHA Workforce
The findings of this study assert the key role that implementation coaching can play in enhancing the capability of coaching participants. While physical capability was not identified as a barrier and therefore not addressed in coaching, our findings suggest that psychological capability, such as the knowledge and skills of CPs, influenced and were influenced by participation in the program. Further to this, variation in knowledge and skill required a flexible coaching approach.
The literature around implementation coaching identifies just as coaching styles vary, the method and level of support provided will necessarily vary dependent on the CPs’ level of confidence, exposure to the subject matter, and their ability to facilitate the dispersion of knowledge to the various levels of the organization.30
CPs project management experience influenced the ability to prioritize and execute tasks, despite the guidance of the PCT. Reliance on third parties to complete tasks was a barrier in the progression of some actions and goals. Those who had no prior project management experience found the coaching timeframe to be limiting and were more reliant on support from the PCT. The CP’s knowledge of, and ability to influence and navigate complex channels of management hierarchy, especially in larger health organizations will determine their ability to effectively influence the change process.
The Opportunity to Optimize the AHA Workforce
The provision of both physical and social opportunity was afforded to CPs as part of the coaching program. These external factors that make the execution of behaviour change possible were highly influential on the relative success of goal achievement within the implementation coaching program.
Physical Opportunity
One of the most common barriers to implementation of behaviour change is a perceived lack of time.31,32 This coaching program provided a pre-determined and limited timeframe of sixteen weeks allocated time for CPs. Regardless of a regional or metropolitan setting, with the appropriate CPs and managerial support, sixteen weeks was demonstrated within this study to be sufficient time to demonstrate achievement or progress towards stated goals. Even within the short timeframe, there was a positive change in the GAS for the combined six CPs, demonstrating that change in the workforce can occur over this period with dedicated staffing and coaching support.
Organizations that were able to allocate protected time for CPs dedicated to the project were observed to have an advantage over those who were trying to manage clinical caseloads as well. This may be attributable to a reduction in the goal conflict experienced by CPs between clinical and implementation goals, which is known to influence how people perceive, spend and value their time.33 This experience of competing time demands often occurred with the AHA representative, creating a barrier to collaboration between the AHA and AHP CP.
This study also recognised the capability of the AHA workforce to be agents for change and thus included provided the opportunity for AHA involvement by design. Prior research into AHA workforce optimisation1,2,5,7,10 highlights that recommendations are not readily adopted unless AHAs are involved in identifying the barriers and are provided access to the required resources.10 By providing both AHPs and AHAs a formalized opportunity to contribute their existing expertise, while also providing them with accessible and ready-to-use resources to support implementation, behaviour change was enabled within the context of this study.
Social Opportunity
Strong collaboration within each CP as well was another enabler to change. Those CPs who had a strong relationship between the AHA and AHP and were able to work collaboratively, actioned tasks at a much faster rate and were able to create a cultural change in their organization with the AHA voice dominant in the project’s work. This is key to enabling long-term change, as supported by the Fair Work Ombudsman.34 Conversely, those that did not have an AHA and AHP working collaboratively, and had the AHP leading the project, ran the risk of not engaging the targeted AHA workforce, resulting in slow progression and hindering the ability to create change.
The characteristics of the coach and their relationships with CPs were also identified as influential factors. The literature scan identified that the experience and credibility of the coach and their ability to engage and develop a rapport with those being coached35 can impact the outcome of the coaching program. The implementation coaching was undertaken by four experienced allied health clinicians, all of whom had extensive experience in working in allied health. The lead coach had over a decade of experience in governing AHAs and had led consultations on the topic of AHA workforce optimization for three years prior to coaching as part of a broader project.1,10 This allowed credibility to be set early, and trust was developed through co-design of SMART goals and early discussions around accountability and shared expectations of the coaching program.
The size of the organisation also influenced the social opportunity of each CP group. Previous studies have identified differences between regional and metropolitan readiness to adopt change. Findings suggest that regional health service, often smaller in size, may be more readily able to adopt change quickly due to size but may have less robust governance to assist in resourcing and sustaining the change.10
Despite the smaller regional organizations often progressing their action logs more quickly, our overarching data set suggests that within the context of this study, metropolitan organizations had the advantage; often already part way to achieving their SMART goals prior to commencement of coaching. This may be attributable to increased resources and established AHA workforces enabling the capacity to share the workload (Table 3).
The size of the organization also played a key role in their relative progress. Smaller organizations appeared to have less barriers for approval, enabling change to be implemented quicker compared to the larger, often metropolitan organizations. This highlighted that the timeframe of sixteen weeks for coaching was substantial enough to allow for minor changes to occur but only enabled the building blocks for greater change. More time is required for complex changes to be achieved such as governance structure and competency processes.
The Motivation to Optimize the AHA Workforce
Motivation speaks to the influence decision-making and behavior. Our findings highlight the impact internal processes that of motivation at an organizational, executive, and professional level influenced the change implementation.
Organization readiness to implement change scales are designed to measure an organization’s appetite for change.24 Within this trial, an unpredictable relationship between organizational readiness (as measured by the ORIC) and implementation (as measured by the GAS) was observed. This could be the case for several reasons, including the small sample size not being sufficient to identify correlations or the awareness of the individual completing the survey of the broader organizational climate. In this context, the ORIC scale may be more a measure of appetite for change rather than a measure of readiness for change, as despite organizations demonstrating an appetite for such, transformational change is rarely fast.
Post implementation workforce survey data did not reflect a significant statistical change although subjectively, it was reported by most CPs that there had been a shift in workforce culture, especially regarding the level of respect and value AHAs felt by their colleagues. These results are limited by survey participant response levels; CPs had no control over the number of respondents, and a lack of participant matching meant it was unclear if it the same survey participant answering the survey pre- and post-coaching. Further to this, it is noted that in general there is variation in the size of the AHA and AHP workforce; this was reflected in the response rate, with a greater number of responses from AHPs which may skew the data to reflect a particular experience.
An enabler for change included having a centralised AHA governance structure. Centralised governance within the leadership team provides a voice for AHAs, supporting faster escalation, avoiding the need for approval from multiple managers before a change can occur. Equally important is executive support to enable any change within a workforce. As discussed by Dean et al,36 a strategic change needs to have support from an executive level with high-level prioritisation This was clearly demonstrated by those CPs who had managerial and higher-level support throughout the sixteen-week coaching period, as those CPs were able to implement change at a faster rate. This is likely due to managerial roles being able to reduce the barriers to approval for change.
AHAs are driven to see their workforce develop and grow,1,7,37 and seek active involvement in the decision-making underpinning the expansion and structure of the AHA workforce of the future. Our findings reinforce this, showing that embedding AHAs as both coaches and recipients of coaching elevated their perceived value and influence in shaping workforce optimization.
Limitations and Challenges
The experiences documented as a part of this study are relevant to the public health sector in Victoria. The transferability of these learnings to other sectors, including disability and aged care, and other geographical areas, with different meso and macro environmental influences, requires further study. The small sample size for the SMART goal analysis may limit the interpretation of the statistical data. A consideration for future coaching is also the robustness of the CP– most were comprised of only two individuals: an AHA and an AHP. This meant any planned or unplanned absences slowed progression, a consequential impact when considering the coaching period was sixteen weeks. One option would be to create a larger CP team with others, across the project, who can assist when required.
Conclusion
AHAs have a role in meeting increased health care service demands, under the delegation and supervision of AHPs. Implementation coaching enabled marked progression towards AHA workforce optimization in public healthcare setting, most notably in delegation processes and practice, consistent recruitment and onboarding processes and the establishment of competency-based training frameworks. The ability to create change was shaped by the capability, motivation and opportunity afforded to the CPs. Additional benefits of implementation coaching included an increased confidence in CPs to deliver change implementation, and an increased value placed on the AHA role in the individual organization. Further research is required to ascertain whether sustained change has been achieved and if findings are transferrable across sectors and jurisdictions employing AHAs.
Abbreviations
AHA, Allied health assistant; AHP, Allied health professional; CP, coaching participant; GAS, Goal Attainment Scale; PCT, Project coaching team; SMART, Specific, measurable, achievable, relevant, timebound; VET, Vocational education and training; SMART, Specific, measurable, achievable, relevant, timebound; PCT, Project coaching team.
Data Sharing Statement
The datasets supporting the conclusions of this manuscript are included within the manuscript (and Supplementary files). The raw data from this study are not available due to the conditions of the ethical approval for this study.
Ethics Approval and Consent to Participate
All methods were performed in accordance with the National Statement on Ethical Conduct in Human Research (NHMRC, 2018). This study was conducted in accordance with the Declaration of Helsinki. Ethical approval was granted by the Monash Health Human Research Ethics Committee (RES-20- 0000-356 L / ERM 64899). All study participants provided written informed consent to participate in the research protocol using institutional consent forms.
Acknowledgments
The authors would like to thank the Victorian Department of Health for their contribution to this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Huglin J, Whelan L, McLean S, et al. Exploring utilisation of the allied health assistant workforce in the Victorian health, aged care and disability sectors. BMC Health Serv Res. 2021;21(1):1–14. doi:10.1186/s12913-021-07171-z
2. Nancarrow SA, Roots A, Grace S, Moran AM, Vanniekerk-Lyons K. Implementing large-scale workforce change: learning from 55 pilot sites of allied health workforce redesign in Queensland, Australia. Human Resources Health. 2013;11(1):66. doi:10.1186/1478-4491-11-66
3. Markham D. Allied health: leaders in health care reform. Aust Health Rev. 2015;39(3):248. doi:10.1071/AH14210
4. Department of Health and Human Services. Victorian allied health workforce research project: allied health assistant workforce report. Available from: https://www2.health.vic.gov.au/health-workforce/allied-health-workforce/allied-health-research.
5. King OA, Pinson JA, Dennett A, Williams C, Davis A, Snowdon DA. Allied health assistants’ perspectives of their role in healthcare settings: a qualitative study. Health Soc Care Commun. 2022;30(6):e4684–e4693. doi:10.1111/hsc.13874
6. Nancarrow SA. Six principles to enhance health workforce flexibility. Human Resources Health. 2015;13(1):9. doi:10.1186/1478-4491-13-9
7. Snowdon DA, King OA, Dennett A, et al. Delegation of patient related tasks to allied health assistants: a time motion study. BMC Health Serv Res. 2022;22(1):1–8. doi:10.1186/s12913-022-08642-7
8. Somerville L, Davis A, Milne S, Terrill D, Philip K. Exploration of an allied health workforce redesign model: quantifying the work of allied health assistants in a community workforce. Aust Health Rev. 2018;42(4):469–474. doi:10.1071/AH16266
9. Turner-Stokes L. Goal attainment scaling (GAS) in rehabilitation: a practical guide. Clin Rehab. 2009;23(4):362–370. doi:10.1177/0269215508101742
10. Whelan L, McLean S, Edwards A, Huglin J, Farlie MK. The evaluation of health, disability and aged care-sector engagement with resources designed to support optimisation of the allied health assistant workforce: a qualitative study. BMC Health Serv Res. 2024;24(1):848. doi:10.1186/s12913-024-11253-z
11. World Health Organization. Global strategy on human resources for health: workforce 2030. Available from: https://apps.who.int/iris/handle/10665/250368.
12. Flaherty E, Bartels SJ. Addressing the community‐based geriatric healthcare workforce shortage by leveraging the potential of interprofessional teams. J Am Geriatr Soc. 2019;67(S2):S400–S408. doi:10.1111/jgs.15924
13. Department of Health. Victorian allied health assistant workforce recommendations and resources. Available from: https://www.health.vic.gov.au/allied-health-workforce/victorian-allied-health-assistant-workforce-recommendations-resources.
14. Victorian Department of Health. Victorian assistant workforce model (allied health). Available from: https://www2.health.vic.gov.au/health-workforce/allied-health-workforce/victorian-assistant-workforce-model/about-this-manual.
15. Donaldson N, Rutledge D, Geiser K. Advances in Patient Safety: New Directions and Alternative Approaches. Agency for Healthcare Research; 2008.
16. Scandiffio J, Zhang M, Karsan I, et al. The role of mentoring and coaching of healthcare professionals for digital technology adoption and implementation: a scoping review. Digital Health. 2024;10:20552076241238075. doi:10.1177/20552076241238075
17. Agency for healthcare research and quality. Implementation coaching. Available from: https://www.ahrq.gov/teamstepps-program/curriculum/implement/activity/coach.html.
18. Etikan I, Musa S, Alkassim R. Comparison of convenience sampling and purposive sampling. Am J Theoretic Appl Stat. 2016;5(1):1–4. doi:10.11648/j.ajtas.20160501.11
19. Gunderson LM, Willging CE, Trott Jaramillo EM, et al. The good coach: implementation and sustainment factors that affect coaching as evidence-based intervention fidelity support. J Children Ser. 2018;13(1):1–17. doi:10.1108/JCS-09-2017-0043
20. Barry CA, Britten N, Barber N, Bradley C, Stevenson F. Using reflexivity to optimize teamwork in qualitative research. Qual Health Res. 1999;9(1):26–44. doi:10.1177/104973299129121677
21. Department of health, disability and ageing. modified monash model. Available from: https://www.health.gov.au/topics/rural-health-workforce/classifications/mmm?language=en.
22. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
23. Atkins L, Francis J, Islam R, et al. A guide to using the Theoretical Domains Framework of behaviour change to investigate implementation problems. Implement Sci. 2017;12(1):77. doi:10.1186/s13012-017-0605-9
24. Shea CM, Jacobs SR, Esserman DA, Bruce K, Weiner BJ. Organizational readiness for implementing change: a psychometric assessment of a new measure. Implement Sci. 2014;9(1):7. doi:10.1186/1748-5908-9-7
25. Bowman J, Mogensen L, Marsland E, Lannin N. The development, content validity and inter-rater reliability of the SMART-Goal evaluation method: a standardised method for evaluating clinical goals. Australian Occup Ther J. 2015;62(6):420–427. doi:10.1111/1440-1630.12218
26. Kiresuk T, Smith A, Cardillo J. Goal Attainment Scale: Applications, Theory, and Management. Psychology Press; 2014.
27. Lumivero. NVivo (version 14). Available from: https://www.lumivero.com.
28. Tovin MM, Wormley ME. Systematic development of standards for mixed methods reporting in rehabilitation health sciences research. Phys Ther Rehab J. 2023;103(11):1. doi:10.1093/ptj/pzad084
29. Michie S, Atkins L, West R. The Behaviour Change Wheel: A Guide to Designing Interventions. Silverback Publishing; 2014.
30. Spears-Jones C, Myles R, Porch T, Parris S, Ivy-Knudsen M, Dean HD. Leading organizational change: improved leadership behaviors among public health leaders after receiving multirater feedback and coaching. Workplace Health Safety. 2021;69(9):400–409. doi:10.1177/21650799211001728
31. Robinson SA, Bisson AN, Hughes ML, Ebert J, Lachman ME. Time for change: using implementation intentions to promote physical activity in a randomised pilot trial. Psychol Health. 2019;34(2):232–254. doi:10.1080/08870446.2018.1539487
32. Ford JH, Gilson AM, Maurer MA, Hoffman KA, Garner BR. A peek behind the curtain: exploring coaching styles within the implementation and sustainment facilitation (ISF) strategy in the substance abuse treatment to HIV care study. Implement Sci Commun. 2021;2(1):140. doi:10.1186/s43058-021-00246-2
33. Etkin J, Evangelidis I, Aaker J. Pressed for time? Goal conflict shapes how time is perceived, spent, and valued. J Market Res. 2015;52(3):394–406. doi:10.1509/jmr.14.0130
34. Fair Work Ombudsman. Consultation and cooperation in the workplace. Available from: https://www.fairwork.gov.au/tools-and-resources/best-practice-guides/consultation-and-cooperation-in-the-workplace.
35. Ritchie MJ, Parker LE, Kirchner JE. From novice to expert: methods for transferring implementation facilitation skills to improve healthcare delivery. Implement Sci Commun. 2021;2(1):39. doi:10.1186/s43058-021-00138-5
36. Dean HD, Myles RL, Spears-Jones C, Bishop-Cline A, Fenton KA. A strategic approach to public health workforce development and capacity building. Am J Preventive Med. 2014;47(5):S288–S296. doi:10.1016/j.amepre.2014.07.016
37. HealthWork AHP Workforce. Four essential factors to optimise the way you work with AHAs: the assistants’ perspective. Available from: https://ahpworkforce.com/models-of-care/four-factors-to-optimise-ahas/.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Approaches That Simplify Implementation of Complex Interventions in Healthcare System Change: “Scoping Review”
Alsaqqa HH
Journal of Multidisciplinary Healthcare 2025, 18:6719-6732
Published Date: 15 October 2025