Back to Journals » Advances in Medical Education and Practice » Volume 13
Readiness for Interprofessional Learning Among First Year Medical and Dental Students in Nepal
Authors Jha N ![]() , Palaian S
, Palaian S ![]() , Shankar PR
, Shankar PR ![]() , Poudyal S
, Poudyal S
Received 15 December 2021
Accepted for publication 1 March 2022
Published 12 May 2022 Volume 2022:13 Pages 495—505
DOI https://doi.org/10.2147/AMEP.S354210
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Nisha Jha,1 Subish Palaian,2,3 Pathiyil Ravi Shankar,4 Sijan Poudyal5
1Department of Pharmacology, KIST Medical College, Lalitpur, Bagmati, Nepal; 2Department of Clinical Sciences, College of Pharmacy and Health Sciences, Ajman University, Ajman, United Arab Emirates; 3Center of Medical and Bio-Allied Health Sciences Research, Ajman University, Ajman, United Arab Emirates; 4IMU Centre for Education, International Medical University, Kuala Lumpur, Malaysia; 5Department of Community Dentistry, KIST Medical College, Lalitpur, Bagmati, Nepal
Correspondence: Nisha Jha, Department of Clinical Pharmacology and Therapeutics, KIST Medical College, Imadol, Lalitpur, Bagmati, Nepal, Tel +977 9841 602 808, Email [email protected] Subish Palaian, Department of Clinical Sciences, College of Pharmacy and Health Sciences, Ajman University, Ajman, United Arab Emirates, Email [email protected]
Introduction: Health professional education curricula in Nepal do not include interprofessional education (IPE). Though a previous study conducted in Nepal identified positive attitudes among medical and nursing students, so far there are no studies assessing the health professional students’ readiness toward IPE. The aim of the study was to assess the readiness for IPE among medical and dental students.
Methods: The present cross-sectional study explored the readiness of conveniently selected first-year medical and dental students towards IPE and compared readiness among subgroups of respondents. The readiness was assessed through an online survey using the standard Readiness for Interprofessional Learning Scale (RIPLS) during June 2021. The nineteen questions in RIPLS were categorized under four domains: teamwork and collaboration (items 1– 9), negative professional identity (items 10– 12), positive professional identity (items 13– 16), and roles and responsibilities (items 17– 19). The individual statements were scored and assessed as per the study objectives. The scores were not normally distributed, so non-parametric tests (Mann–Whitney U-test and Kruskal Wallis test) were used.
Results: A total of 83 students (69 medical and 14 dental) students responded. The median total score was 75, IQR 6 with the maximum score being 95. The median (IQR) scores for the domains teamwork and collaboration were 38 (IQR 3), negative professional identity 11 (IQR 2), positive professional identity 16 (IQR 3), roles and responsibilities 10 (3). The scores were different between students aged 20 years and below = 37, and above 20 years = 38; (p =< 0.001) in the negative professional identity domain and the total score (p = 0.001). The scores were also different among those with and without previous learning exposure with other discipline students in the same class (p = 0.046). A high median score of 5 was achieved for 8 out of 19 statements in the questionnaire.
Conclusion: The findings showed a high level of readiness for IPE among student respondents. Study findings can be considered as a positive factor for implementing IPE sessions.
Keywords: dental, interprofessional education, medical, Nepal, undergraduate students
Introduction
The holistic nature of health-care demands effective collaboration between various health-care providers.1 For effective collaboration, there should be respect, trust, and communication between diverse health-care workers. To address this issue, the World Health Organization (WHO) has recommended interprofessional education (IPE) which offers a platform among students from different health-care professions to appreciate the strengths of various disciplines and be able to develop and improve teamwork and communication. WHO defines IPE as “an experience that occurs when students from two or more professions learn about, from, and with each other”.2 IPE prepares the future health professional for using the right care efficiently and utilizing everyone’s roles and responsibilities to improve health outcomes.3 Due to the increase in diversity, complex medical cases and limited health-care budgets, health-care students are expected to work effectively in a team after graduation.4 To practice interprofessional collaboration, health workers should be oriented and adapted towards working together with multiple health professionals. This culture can be incorporated while they are students by introducing them to the concept of “learning together” which helps them understand each other’s roles and develop a positive attitude towards each other. Thus, many institutions worldwide have implemented IPE in their curriculum to implant the culture of learning and working together right from the student level. The concept of IPE is well developed in certain countries and health profession students learn various topics together using student research projects, collaborative case presentations, seminars, etc.5 In the United States (US), IPE has been recognized as a core component of health professions education and accreditors seek evidence of the same as a mandatory requirement. The Health Professions Accreditors Collaborative (HPAC)6 and National Center for Interprofessional Practice and Education on Guidance on Developing Quality Interprofessional Education for the Health Professions provide detailed guidance on requirements of health programs to incorporate IPE in their curriculum.
Nepal is a lower-middle-income country with low health-care indicators. Healthcare is delivered through public-funded and privately-run health-care centers. Like the health-care centers, health profession education is also provided by both government and private institutions.7,8 Considering the shortage of the health workforce in Nepal, as evident during the COVID-19 pandemic9 it is important to include health personnel from different fraternities in the health-care team and optimize the existing resources. A study published over a decade ago from Nepal showed a positive attitude among medical and nursing students towards IPE.10 A similar observation was noted in a neighboring country, India.11 There exists a hierarchical nature in Asian culture, and medical doctors hold the highest position in the health-care team whereas other health professionals hold less important positions, which can affect IPE and interprofessional collaboration. In a country like Nepal, where the education system is arranged as single health professions disciplines, and where practitioners of a discipline teach students of the same discipline,12 learning from different professions together becomes a difficult task. This difficulty can be lessened by IPE by its innate nature of learning from students from diverse professions. In Nepal, students who have studied medicine or dentistry on a government scholarship, have to serve in rural areas for two years after graduation.13 Rural Nepal faces several problems such as lack of access to basic medical care, poorly developed health-care facilities, shortage of essential medicines, migration of health workers, inadequate financing of health-care facilities.14 In such challenging situations, recent graduates must work together and often lead health-care teams and IPE can serve achieving these goals by fresh graduates. IPE faces challenges for effective implementation in terms of differences in work schedules of different professions, differences in student number, in curricula and teaching approaches but student’s attitude towards this new learning approach is considered as the most challenging factor.14 IPE has a positive impact on students’ role regarding interprofessional collaboration.15 However, IPE can be effective only if health professional students are willing to learn from each other and hence it is crucial to assess the readiness of students toward IPE.
Readiness for IPE has been studied globally among both medical and other health professional students. In Australia, paramedical students’ readiness for IPE was not influenced by their gender or their paramedical course of study.16 Their mean scores (standard deviation) for each RIPLS subscale were: “teamwork and collaboration” 28.71 (3.94); “negative professional image” 15.29 (2.93); “positive professional image” 14.61 (3.76) and “roles and responsibilities” 13.10 (1.61). At an American university, attitude toward IPE was studied among first-year medical, nursing and physician associate students and the scores among all three groups were high.17 The mean total score among medical students was 76.41 and it was higher among physician associate students at 76.84 and was the highest among nursing students at 83.06. Readiness for IPE was studied at the University of Kansas Medical Center in the US and the authors observed that an interprofessional educational experience significantly improved scores among medicine, nursing, pharmacy, and students of other health professions.18 The scores were also studied among students enrolled in medical, veterinary science and dual degree programs at an offshore university in Granada in the Caribbean.19 The authors did not calculate the total subscale scores and only measured the scores for individual statements. The scores ranged between 4.65 and 2.66 and varied according to the course of study.
The readiness for interprofessional learning scale (RIPLS) has been widely used during the last two decades. The questionnaire has been modified and translated into several languages. A four-factor sub scale model developed by McFadyen and coauthors was published in 2009.20 Medical and nursing student attitudes towards IPE were studied in Nepal using RIPLS.10 The authors had used statements derived from RIPLS along with other statements in their study. The instrument with the four factor-subscale was used in a study among health professional students in Sri Lanka.21 Their mean total score was 69.15. Thus, RIPLS has been used in previous studies in South Asia. There have been doubts about the validity of RIPLS. Some authors have argued that the overall structure and scores of RIPLS are good but there have been problems regarding the subscales and the factors.22 There may be considerable overlap between the factors and low internal consistency of the subscales. We selected RIPLS as it has been used for over two decades, the instrument has been used in Asia and South Asia and the statements appeared to be relevant to the Nepalese context.
Thus, assessing medical and dental students’ readiness for interprofessional learning provides important insights for its implementation. In the context of Nepal, the concept of IPE is still in the embryonic stage and more needs to be done. The present study evaluates readiness for IPE among medical and dental students, identify their readiness to learn from and with other health professional students, and compares the readiness for IPE among different cohorts of students. Further, the first-year students were chosen because the authors intend to study specifically the readiness among newly joined students since they are more open to accepting changes.
Materials and Methods
Study Design
A cross-sectional questionnaire-based exploratory study involving first year medical and dental students.
Ethical Approval
The current research proposal was approved by the Institutional Review Committee (IRC) at KIST Medical College, Nepal as per the letter reference number 2077/78/60, dated 23rd June 2021.
Study Respondents
First-year medical and dental students from KIST Medical college, Lalitpur, Nepal. The institution runs a five-year undergraduate medical program (MBBS) and a five-year undergraduate dental medicine program (BDS). Generally, students from Nepal enroll in the programs. During the study period, there were a total of 108 (medical 89 and 19 dental) students in their first year of study.
Informed Consent
Student respondents consented to participate in the survey by completing the online consent prior to responding to the survey. The first part of the questionnaire had a section mentioning consent and participants were given the opportunity to decline if they were not willing to respond to the survey. The researchers followed all the guidelines outlined by the IRC at KIST Medical College.
Sampling Method and Technique
The sampling method adopted for the study was population sampling23 and all students eligible (n = 108) and willing to be a part of the research were included in the study.
Data Collection Tool
Authors selected the standard Readiness for Interprofessional Learning Scale (RIPLS) Questionnaire24. The publicly available, adapted version of RIPLS used by the Latrobe Community Health Service & the Health & Social care Interprofessional Network (HSN) was used and is available at https://nexusipe-resource-exchange.s3-us-west-2.amazonaws.com/Tool.Readiness%20for%20Interprofessional%20Learning%20Scale%20%28RIPLS%29.pdf. Though the RIPLS has been modified multiple times, the authors in this research used the initial version due to the ease in administration and greater experience with the original tool that has been translated into multiple languages. However, for better analysis and presentation of results, authors have chosen the four subscales of McFadyen modification of the tool20 “teamwork and collaboration”, “negative professional identity”, ‘positive professional identity’ and “roles and responsibility”. The degree of agreement of respondents with different statements was measured using the following scale: 1 = strongly disagree with the statement, 2 = disagree, 3 = undecided, 4 = agree and 5 = strongly agree. Upon scoring, the total score attainable by any respondent ranges from 19 to 95. A higher score represents greater readiness for IPE. The statements 10, 11 and 12 were negatively worded. Their scores were reversed while calculating the scores of individual statements.20
Validity and Internal Consistency of the Tool
Though this questionnaire has been used in various studies previously, there have been concerns regarding the validity of the tool.22,25 However, the authors decided to use this questionnaire due to its wide use, simplicity, and availability free of cost. It is also worth mentioning that the tool had demonstrated good validity and internal consistency in studies conducted in Iran,26 and China.27 Moreover, the tool has been already used successfully in the neighboring country India, with minor modifications.11 In another research involving general practitioners, nurses and pharmacists, RIPLS yielded a Cronbach alpha value of 0.76.28 In order to confirm the internal consistency, the reliability was calculated by administering the questionnaire to 10 students and the overall Cronbach alpha value was 0.57. Performing the reliability analysis with a greater number of students may have been better. However, due to the low number of available respondents the authors decided to choose only 10 respondents for the reliability analysis. The authors did not remove any questions from the tool since it could lead to deficiency in measuring the specific domains if items were deleted.
Method of Data Collection
The data were collected during the last week of June 2021. The principal investigator distributed the online questionnaire through Google form. Students who did not respond were given reminders with one-week gap.
Data Analysis
The completed questionnaires were transferred to SPSS Version 26 and normality of distribution of the total and subscale scores were checked. The normality testing showed the date was not normally distributed (one sample-KS test) and hence nonparametric tests (Mann–Whitney U-test for variables and Kruskal Wallis test for variables with more than two responses) were used. The statistical significance was determined at alpha=0.05.
Results
Eighty-three of the 108 students (76.8%) participated. The response rate among MBBS students was 69 out of 89 students (77.5%) and for BDS students the rate was 73.7% (14 out of 19 students). Most students were not exposed to IPE and more students were female (see Table 1).
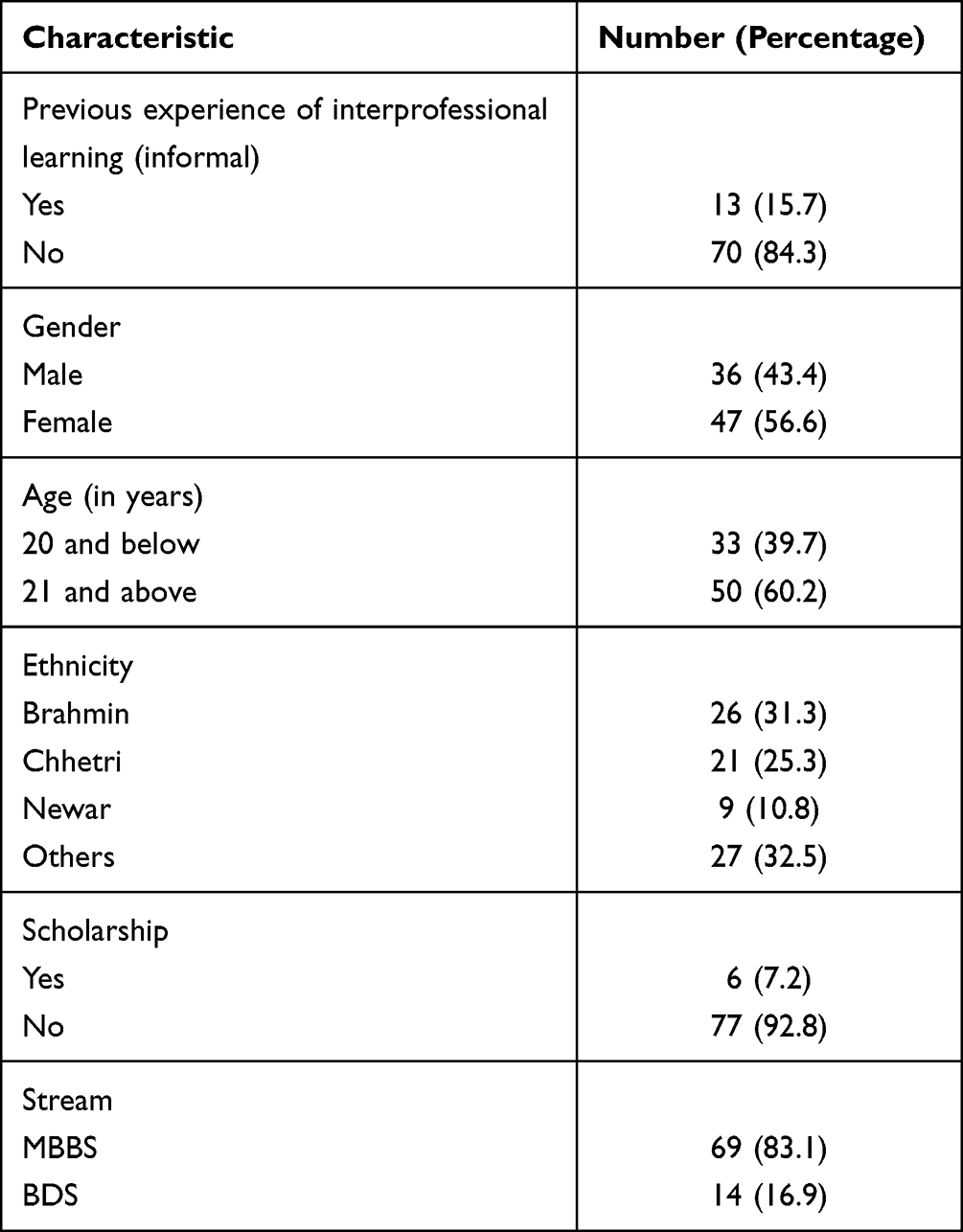 |
Table 1 Demographic Characteristics of Respondents (n = 83) |
The median teamwork and collaboration score were 38 (IQR 3). The maximum possible score was 45. The median negative professional identity score was 11 (IQR 2) with the maximum possible score being 15. For positive professional identity, the median score was 16 (IQR 3) and maximum possible score was 20. For roles and responsibilities, the median (IQR) score was 10 (3) with the maximum score being 15. The median total score was 75, IQR 6 with the maximum score being 95.
Table 2 shows the total and subscale scores among different subgroups of respondents. The total scores were higher among younger respondents, those with previous exposure to learning with other discipline students on basic sciences subjects like anatomy, physiology in the same class and varied according to ethnic groups. This learning cannot be regarded as IPE as it did not fulfil most necessary characteristics of the same. The negative professional identity score was higher among students below 20 years of age and the total score was also higher in this subgroup. The positive professional identity scores varied according to ethnic groups and so did the total score. The positive professional identity score was significantly higher among Newars (an ethnic group predominantly residing in the Kathmandu valley) compared to others (p = 0.011), and the total score was also higher among Newars compared to others (p = 0.002).
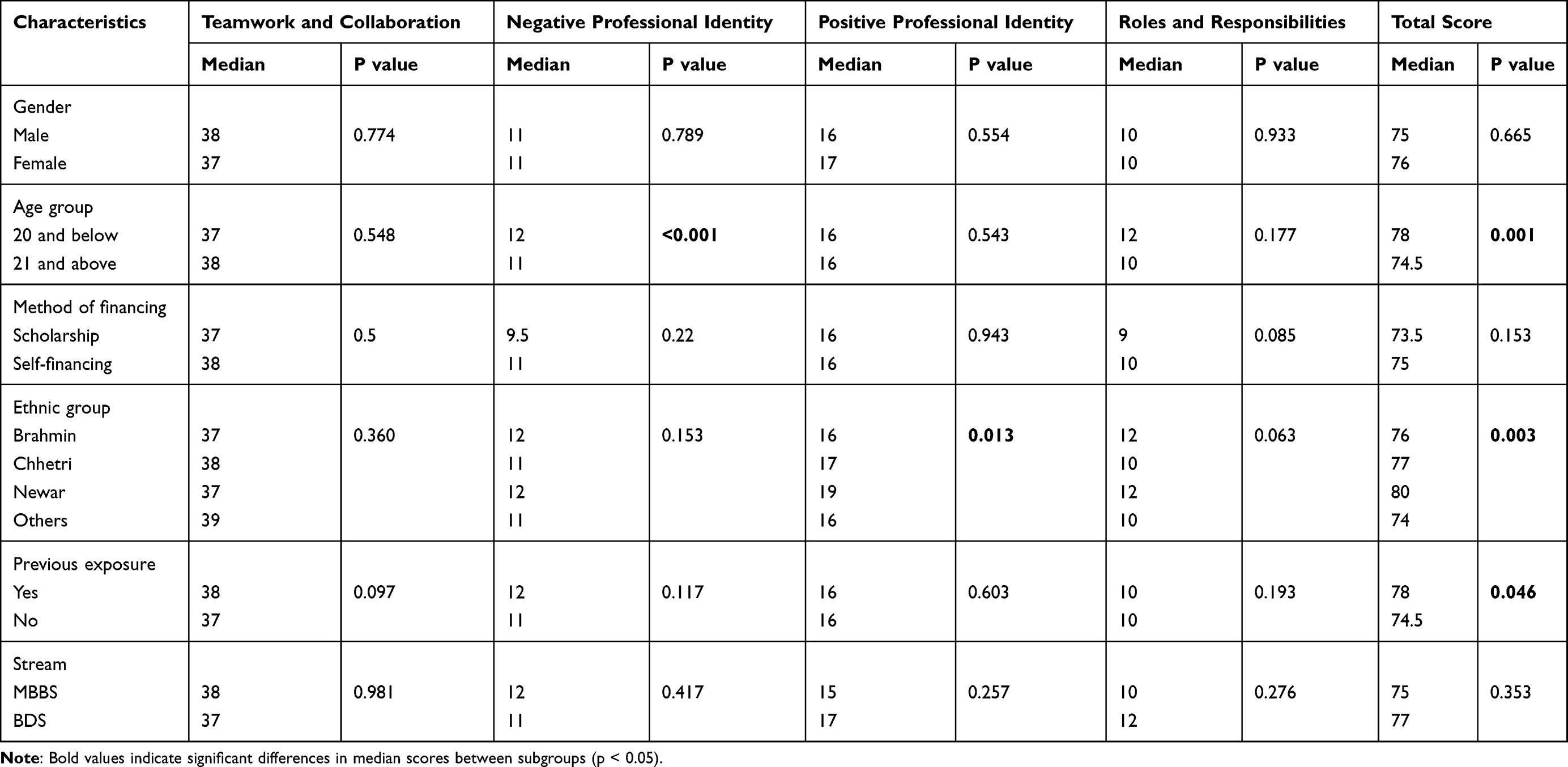 |
Table 2 Median Subscale and Total Scores According to Demographic Characteristics of Respondents |
Table 3 shows the median scores of individual statements. The scores of statement regarding “patients benefiting significantly if HCPs work together”, “shared learning helping the student understand his/her own professional limitations”, “learning together will improve working relationships”, “shared learning will help the respondent think positively about other HCPs”, “shared learning will help with better communication”, “they would like the opportunity to work on small group projects with other HCPs and ‘shared learning would help them clarify the nature of their patient’s problems and help them become a better team worker” were 5. The median scores of certain statements were 3.
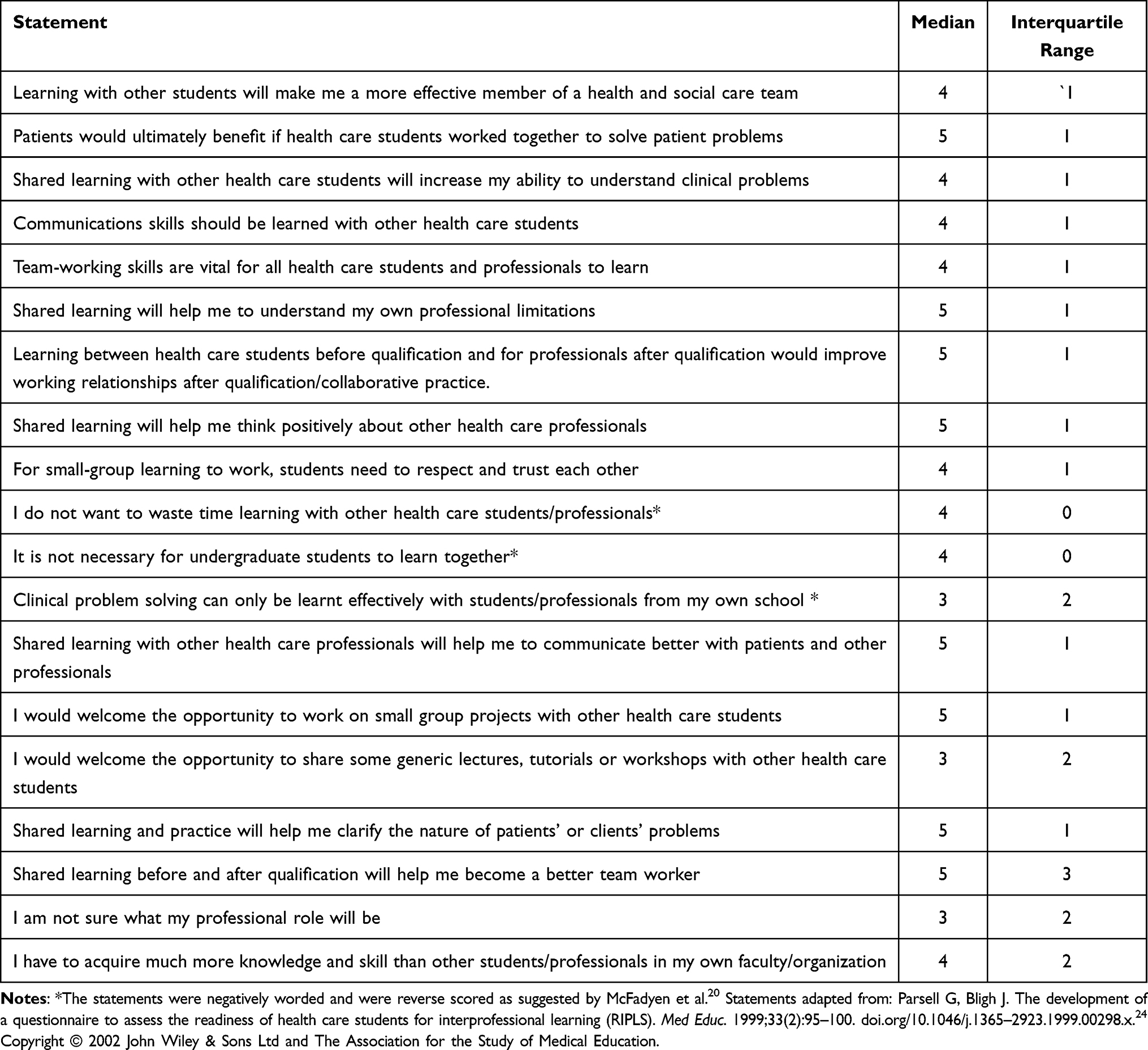 |
Table 3 Median (Interquartile Range) Scores of Individual Statements |
Discussion
The textbook by Maxwell titled “Teamwork Makes the Dreamwork” clearly demonstrates that a person cannot achieve one’s dream by working all alone by himself/herself.29 The healthcare settings traditionally were physician dominated with the physician being considered as the team leader and assisted by trained professionals/nonprofessionals supporting the physician. More recently, the concept of patient-centered care has been adopted by health-care practitioners and every professional is given their due importance in managing patients, and the focus is more towards the “patient” rather than an individual health-care member. Teamwork in healthcare is expected to improve patient care as mentioned by several researchers.15,30–32
The present study assessed the readiness towards IPE among first year medical and dental students in Nepal where the curriculum is offered as integrated organ system-based system modules. The need for interprofessional collaboration among medical and dental practitioners is well documented in the literature33 and these professionals are required to collaborate with nurses, pharmacists, laboratory technologists and others to optimize care to their patients. A previous study from Nepal in 2010 conducted among final year medical and third year (four-year course) nursing students demonstrated students to be aware about the concept and importance of IPE.10 The present study had a different focus, assessing the readiness towards IPE among first year medical and dental students. The findings overall show medical and dental students were aware of the importance of IPE and ready to collaborate with other health professional students as reflected by a total RIPLS score 75 (maximum score 95). Thus, the study findings were similar to other studies reported from Saudi Arabia (mean score 86.8)34 and Iran (mean score 84.2)35 where students showed a high readiness for IPE. It is important to notice that the total score in the present study was not influenced by demographic parameters like the Saudi Arabian study wherein gender, and year of study had no association with the scores.34
The students felt that learning with students from other health disciplines will enable them to be a more effective member of a health and social care team as demonstrated by a high score of 38 out of 45. Similar findings were reported by other researchers wherein student respondents felt teamwork to be important.36 However, one can clearly note the lacunae in interprofessional collaborative practice in health-care settings. Such a shift in attitude from studentship to practitioners shows that students who initially appreciate other professions may change their perspective during their educational programs. This shift can be further promoted by the existing culture of practice in health-care settings. Interventions may be required to sustain the readiness. In the present research, a high median score of “5” was achieved for the statement “Patients would ultimately benefit if health-care students/professionals worked together”. This is a positive and welcoming attitude that shows students’ willingness to participate in IPE. Willingness to learn together can be also considered as a predictive factor for working together in the future.37 Patient benefits due to professionals’ teamwork and collaboration are significant.
Teamwork in healthcare is known to reduce medical errors, thus improving patient safety.38 Teamwork also encourages shared decision-making and empowers patients. Present study findings agree with another study from Saudi Arabia conducted among medical and dental students39 wherein students reported collaboration improves their services to patients and the community. Though students exhibited positive opinions, in the reality there are challenges in achieving teamwork at various levels; organizational level, team level, and at individual team member level and these include differences in professional power, knowledge bases, and professional culture.40,41 Strategies to overcome these barriers should be in place.
Further, respondents felt team-working skills are important for all health-care students. It is advisable to incorporate IPE skills in health professions education at a much earlier stage42 as they are vulnerable to hierarchical work patterns observed from their role models during the later phase of educational programs especially during clinical training. Thus, implementing IPE is feasible and sustainable only if the practice perspectives also incorporate interprofessional collaboration. As shown by the present study results, students felt that shared learning will help them understand their own professional limitations and help them think positively about other health-care professionals. In general, health professionals, mainly physicians, might not perceive the importance of other professionals and prefer to work independently.43 This barrier can be overcome if these concepts are incorporated earlier in their course so that they can appreciate the strengths and weaknesses of each professional and be able to take help from other professionals in the future. Students also felt that respect and trust among students/professionals are needed for small group learning to work. The scores obtained on teamwork and collaboration were not different among subgroups according to age, gender, method of financing and most other characteristics.
The median negative professional identity score was 11 out of 15. Respondents in this study disagreed on time wastage due to learning together with students from other professions. Our findings agree with a Pakistani study wherein more than two-thirds [105 (64.45%)] disagreed with the negative attitude.44 They also felt it was necessary for undergraduate and postgraduate health-care students/professionals to learn together. However, it was important to know that students generally felt clinical problem solving can only be learned effectively with students/professionals from their own school/organization suggesting the need for more education on IPE and the opportunity to practice IPE. Research evidence clearly demonstrates clinical case learning involving students of multiple professions can be fruitful45 wherein students from each profession can contribute in their areas of expertise.
Gilbee et al46 described guidelines for interprofessional case presentation and its assessment which can be considered useful by educators while implementing interprofessional case presentations. As reported in this research, the negative professional identity domains were influenced by age wherein respondents with age 20 years or less had a slightly higher score further suggesting the importance of an early introduction of IPE modules to have maximum impact. A scoping review of 49 published articles showed age to have an influence on the readiness of IPE.47 There is a possibility that as age increases the student is exposed more to the hierarchical constructs which can prevent them learning from others. This can be more among medical students as reported in a Korean study conducted among medical, nursing and pharmacy students, wherein nursing students had a high perception about the importance, preference, and effectiveness of IPE compared to a lower score among medical students.48
For positive professional identity, the median score was 16 (maximum score 20). It was good to know that students felt they will be able to communicate better with patients and other professionals if they learned together. Like the Pakistani study44 in which 70–80% of respondents showed a positive professional identity, the present study also demonstrated the same. They welcomed the opportunity to work together on small group projects and felt working in groups comprising other profession students helps them clarify the nature of patients’ or clients’ problems. The medical student focuses on the diagnosis, nursing students on the nursing care, and pharmacy students on pharmacotherapy-related issues. For roles and responsibilities, the median score was 10 with the maximum score being 15. Student had a high agreement for the statement “Shared learning before and after qualification will help me become a better team worker”, which is to be welcomed.
Strengths and Limitations
This study is the first one in Nepal to assess the readiness of IPE among health profession students though a previous study assessed the knowledge and awareness but did not evaluate the readiness to practice.10 The study also had a few limitations. The study was conducted during the COVID-19 pandemic wherein students were mostly attending online sessions and hence may not perceive the importance of collaboration. The sample size of the study is also low limiting its generalizability. The responses were gathered by faculty members who were involved in the academic teaching of the students which could have influenced students. Moreover, this study was conducted among first-year students at the preclinical level and their readiness could change while progressing to subsequent years, potentially influenced by their mentors and role models. The RIPLS used in the study is the initial one developed by Parsell and Bligh in 1999.24 The revised version by McFadyen et al in 200520 may have yielded more reliable results. The internal consistency of the questionnaire was studied only among 10 responses due to the lesser number of available respondents and can be considered a limitation.
Recommendations
IPE should be initiated in health-care programs in Nepal. Curricular and noncurricular IPE sessions can be implemented. The present study findings can serve as baseline data for the readiness of medical and dental students towards IPE. Probably the readiness may be similar even among nursing and other paramedical students. To begin with IPE can be started with students from two health professions and later more professions can be added. IPE can be implemented by presenting clinical case studies to be addressed by different profession students, each focusing on their areas of expertise. This approach gives an opportunity for everyone to appreciate the strength and expertise of other professions. Since the respondents had a positive attitude towards IPE it would be easier to implement. Research evidence clearly shows IPE training significantly influences students’ understanding of collaboration and improves their attitudes towards interprofessional teamwork.15,49 To begin with there can be IPE sessions such as collaborative case presentations, seminars, role plays, etc. The universities and councils should make it mandatory to incorporate IPE in health professional curricula. The HPAC and National Center for Interprofessional Practice and Education recommendations on Guidance on Developing Quality Interprofessional Education for the Health Professions can be consulted while implementing IPE in curricula.
Further, based on the current research findings, authors notice a decline in the readiness with increase in respondents’ age suggesting the need for offering IPE at the beginning of their study. Since previous exposure to learning with other discipline students on basic sciences subjects like anatomy, physiology in the same class improved readiness scores, it can be considered as a good venue to encourage IPE and incorporate group learning among different health profession students.
Conclusion
A high readiness among students offers greater scope for incorporating IPE among medical and dental students, beginning from their first year of study. The study findings can be considered as baseline evidence regarding the readiness of medical and dental students in an institution in Nepal towards interprofessional learning. Though bringing together students from multiple professions can be challenging, a well-planned curriculum with mandatory IPE modules can certainly incorporate teamwork and collaborative practice culture among future health-care practitioners. The success stories from developed countries can be taken as a model while implementing IPE in Nepal.
Acknowledgments
The authors would like to acknowledge the students who spent their valuable time completing the survey questionnaire. The authors also thank Ajman University for paying the article processing fee.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lestari E, Stalmeijer R, Widyandana D, Scherpbier A. Understanding students’ readiness for interprofessional learning in an Asian context: a mixed-methods study. BMC Med Educ. 2016;16. doi:10.1186/s12909-016-0704-3
2. Framework for action on interprofessional education & collaborative practice. Available from: https://www.who.int/publications-detail-redirect/framework-for-action-on-interprofessional-education-collaborative-practice.
3. Kersbergen MJ, Creugers NHJ, Hollaar VRY, Laurant MGH. Perceptions of interprofessional collaboration in education of dentists and dental hygienists and the impact on dental practice in the Netherlands: a qualitative study. Eur J Dent Educ. 2020;24(1):145–153. doi:10.1111/eje.12478
4. Huebner S, Tang QC, Moisey L, Shevchuk Y, Mansell H. Establishing a baseline of interprofessional education perceptions in first year health science students. J Interprof Care. 2021;35(3):400–408. doi:10.1080/13561820.2020.1729706
5. Herath C, Zhou Y, Gan Y, Nakandawire N, Gong Y, Lu Z. A comparative study of interprofessional education in global health care. Medicine. 2017;96(38):e7336. doi:10.1097/MD.0000000000007336
6. Health Professions Accreditors Collaborative. IPE guidance. Available from: https://healthprofessionsaccreditors.org/ipe-guidance/.
7. Health Affairs. The high costs of Nepal’s fee-for-service approach to health care. Available from: https://www.healthaffairs.org/do/10.1377/hblog20150720.049382/full/.
8. Ranabhat CL, Subedi R, Karn S. Status and determinants of enrollment and dropout of health insurance in Nepal: an explorative study. Cost Eff Resour Alloc. 2020;18(1):40. doi:10.1186/s12962-020-00227-7
9. Shortage of health workers a challenge as country braces for Covid-19 third wave. Available from: https://kathmandupost.com/health/2021/07/22/shortage-of-health-workers-a-challenge-as-country-braces-for-covid-19-third-wave.
10. Regmi KR, Regmi S. Medical and nursing students attitudes towards interprofessional education in Nepal. J Interprof Care. 2010;24(2):150–167. doi:10.3109/13561820903362254
11. Mohammed CA, Narsipur S, Vasthare R, Singla N, Yan Ran AL, Suryanarayana JP. Attitude towards shared learning activities and Interprofessional education among dental students in South India. Eur J Dent Educ. 2021;25(1):159–167. doi:10.1111/eje.12586
12. Baral B, Prajapati R, Karki KB, Bhandari K. Distribution and skill mix of health workforce in Nepal. J Nepal Health Res Counc. 2013;11(24):126–132.
13. Shankar PR. Undergraduate medical education in Nepal: one size fits all? J Educ Eval Health Prof. 2011;8(9):9. doi:10.3352/jeehp.2011.8.9
14. Mishra SR, Khanal P, Karki DK, Kallestrup P, Enemark U. National health insurance policy in Nepal: challenges for implementation. Glob Health Action. 2015;8:28763. doi:10.3402/gha.v8.28763
15. Wang Z, Feng F, Gao S, Yang J. A systematic meta-analysis of the effect of interprofessional education on health professions students’ attitudes. J Dent Educ. 2019;83(12):1361–1369. doi:10.21815/JDE.019.147
16. Williams B, Boyle M, Brightwell R, et al. A cross-sectional study of paramedics’ readiness for interprofessional learning and cooperation: results from five universities. Nurse Educ Today. 2013;33(11):1369–1375. doi:10.1016/j.nedt.2012.06.021
17. Talwalkar JS, Fahs DB, Kayingo G, Wong R, Jeon S, Honan L. Readiness for interprofessional learning among healthcare professional students. Int J Med Educ. 2016;7:144–148. doi:10.5116/ijme.570d.7bd8
18. Zaudke JK, Paolo A, Kleoppel J, Phillips C, Shrader S. The impact of an interprofessional practice experience on readiness for interprofessional learning. Fam Med. 2016;48(5):371–376.
19. Roopnarine R, Boeren E. Applying the Readiness for Interprofessional Learning Scale (RIPLS) to medical, veterinary and dual degree Master of Public Health (MPH) students at a private medical institution. PLoS One. 2020;15(6):e0234462. doi:10.1371/journal.pone.0234462
20. McFadyen AK, Webster V, Strachan K, Figgins E, Brown H, McKechnie J. The readiness for interprofessional learning scale: a possible more stable sub-scale model for the original version of RIPLS. J Interprof Care. 2005;19(6):595–603. doi:10.1080/13561820500430157
21. Herath C. Sri Lankan undergraduate healthcare student’s perceptions of interprofessional learning: a cross-sectional study. Ann Clin Med Case Rep. 2020;5(4):1–8.
22. Mahler C, Berger S, Reeves S. The Readiness for Interprofessional Learning Scale (RIPLS): a problematic evaluative scale for the interprofessional field. J Interprof Care. 2015;29(4):289–291. doi:10.3109/13561820.2015.1059652
23. Taherdoost H. Sampling methods in research methodology; how to choose a sampling technique for research. Int j Acad Res Manag. 2016;5(2):18–27. doi:10.2139/ssrn.3205035
24. Parsell G, Bligh J. The development of a questionnaire to assess the readiness of health care students for interprofessional learning (RIPLS). Med Educ. 1999;33(2):95–100. doi:10.1046/j.1365-2923.1999.00298.x
25. Schmitz C, Brandt B. To RIPLS or not to RIPLS: that is only part of the question. National Centre for Interprofessional Practice and Education. Available from: https://nexusipe.org/informing/about-national-center/news/ripls-or-not-ripls-only-part-question.
26. Batool A, Shoaleh B, Mandana S, Mohammad MS. Validity and reliability of the readiness for interprofessional learning. J Payavard-Salamat. 2016;10:51–58.
27. Li Z, Sun Y, Zhang Y. Adaptation and reliability of the readiness for inter professional learning scale (RIPLS) in the Chinese health care students setting. BMC Med Educ. 2018;18:309. doi:10.1186/s12909-018-1423-8
28. Reid R, Bruce D, Allstaff K, McLernon D. Validating the Readiness for Interprofessional Learning Scale (RIPLS) in the postgraduate context: are health care professionals ready for IPL? Med Educ. 2006;40(5):415–422. doi:10.1111/j.1365-2929.2006.02442.x
29. Maxwell JC. Teamwork Makes the Dreamwork.
30. Capella J, Smith S, Philip A, et al. Teamwork training improves the clinical care of trauma patients. J Surg Educ. 2010;167(6):439–443. doi:10.1016/j.jsurg.2010.06.006
31. Clark PR. Teamwork: building healthier workplaces and providing safer patient care. Crit Care Nurs Q. 2009;32(3):221–231. doi:10.1097/CNQ.0b013e3181ab923f
32. Manser T. Teamwork and patient safety in dynamic domains of healthcare: a review of the literature. Acta Anaesthesiol Scand. 2009;53(2):143–151. doi:10.1111/j.1399-6576.2008.01717.x
33. Zhang S, Lo EC, Chu CH. Attitude and awareness of medical and dental students towards collaboration between medical and dental practice in Hong Kong. BMC Oral Health. 2015;15(1):1–6.
34. Alruwaili A, Mumenah N, Alharthy N, Othman F. Students’ readiness for and perception of Interprofessional learning: a cross-sectional study. BMC Med Educ. 2020;20(1):390. doi:10.1186/s12909-020-02325-9
35. Keshtkaran Z, Sharif F, Rambod M. Students; readiness for and perception of interprofessional learning: a cross-sectional study. Nurse Educ Today. 2014;34(6):991–998. doi:10.1016/j.nedt.2013.12.008
36. Aase I, Hansen BS, Aase K. Norwegian nursing and medical students’ perception of interprofessional teamwork: a qualitative study. BMC Med Educ. 2014;14(1):1–9. doi:10.1186/1472-6920-14-170
37. Maharajan MK, Rajiah K, Khoo SP, et al. Attitudes and readiness of students of healthcare professions towards interprofessional learning. PLoS One. 2017;12(1):e0168863. doi:10.1371/journal.pone.0168863
38. Baker DP, Gustafson S, Beaubien JM, et al. Medical team training programs in health care. In: Henriksen K, Battles JB, Marks ES, et al. editors. Advances in Patient Safety: From Research to Implementation. Rockville (MD): Agency for Healthcare Research and Quality (US); 2005.
39. Al-Shaikh GK, Al-Madi EM, Masood J, et al. Interprofessional learning experiences: exploring the perception and attitudes of Saudi Arabian medical and dental students. Med Teach. 2018;40(sup1):S43–S48. doi:10.1080/0142159X.2018.1465180
40. Steihaug S, Johannessen AK, Ådnanes M, Paulsen B, Mannion R. Challenges in achieving collaboration in clinical practice: the case of Norwegian health care. Int J Integr Care. doi:10.5334/ijic.2217
41. World Health Organization. Being an effective team player. Available from: http://www.who.int/patientsafety/education/curriculum/who_mc_topic-4.pdf.
42. Ammar A, Mueller P, Trabelsi K, et al. Psychological consequences of COVID-19 home confinement: the ECLB-COVID19 multicenter study. PLoS One. 2020;15(11):e0240204. doi:10.1371/journal.pone.0240204
43. Berger AS. Arrogance among physicians. Acad Med. 2002;77(2):145–147. doi:10.1097/00001888-200202000-00010
44. Alzamil H, Meo SA. Medical students’ readiness and perceptions about Interprofessional Education: a cross sectional study. Pak J Med Sci. 2020;36(4):693–698. doi:10.12669/pjms.36.4.2214
45. Curran VR, Sharpe D, Forristall J, Flynn K. Student satisfaction and perceptions of small group process in case-based interprofessional learning. Med Teach. 2008;30(4):431–433. doi:10.1080/01421590802047323
46. Gilbee A, Baulch J, Leech M, Levinson M, Kiegaldie D, Hood K. A guide for interprofessional case presentations. Clin Teach. 2014;11(4):297–300. doi:10.1111/tct.12220
47. Slater CE, Cusick A. Factors related to self-directed learning readiness of students in health professional programs: a scoping review. Nurse Educ Today. 2017;52:28–33. doi:10.1016/j.nedt.2017.02.011
48. Yune SJ, Park KH, Min YH, Ji E. Perception of interprofessional education and educational needs of students in South Korea: a comparative study. PLoS One. 2020;15(12):e0243378. doi:10.1371/journal.pone.0243378
49. McNair R, Stone N, Sims J, Curtis C. Australian evidence for interprofessional education contributing to effective teamwork preparation and interest in rural practice. J Interprof Care. 2005;19(6):579–594. doi:10.1080/13561820500412452
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.