")
Back to Journals » Patient Preference and Adherence » Volume 17
Readiness for Hospital Discharge After a Cesarean Section and Associated Factors Among Chinese Mothers: A Single Centre Cross-Sectional Study
Authors Xia ML , Lin WX, Gao LL , Zhang ML, Li ZY, Zeng LL
Received 2 February 2023
Accepted for publication 4 April 2023
Published 12 April 2023 Volume 2023:17 Pages 1005—1015
DOI https://doi.org/10.2147/PPA.S404137
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Mei-Ling Xia,1 Wen-Xuan Lin,2 Ling-Ling Gao,3 Mao-Ling Zhang,1 Zhi-Yun Li,4 Li-Ling Zeng4
1Reproductive Centre, Guangdong Women and Children Hospital, Guangzhou, People’s Republic of China; 2Nursing Department, Guangdong Women and Children Hospital, Guangzhou, People’s Republic of China; 3School of Nursing, Sun Yat-Sen University, Guangzhou, People’s Republic of China; 4Obstetric Department, Guangdong Women and Children Hospital, Guangzhou, People’s Republic of China
Correspondence: Ling-Ling Gao, School of Nursing, Sun Yat-sen University, Guangzhou, People’s Republic of China, Tel +86-20-87335013, Fax +86-20-87333043, Email [email protected]
Purpose: Knowledge of the readiness for hospital discharge can help health care professionals accurately determine the patients’ discharge time. However, few studies were on the readiness for discharge and its related factors among mothers with cesarean sections. Thus, this study aims to examine the readiness for hospital discharge and its associated factors among Chinese mothers with cesarean sections.
Patients and Methods: A single-centre cross-sectional study was conducted from September 2020 to March 2021 in Guangzhou, China. Three hundred thirty-nine mothers with cesarean sections completed the questionnaires on demographic and obstetric characteristics, readiness for hospital discharge, quality for discharge teaching, parenting sense of competence, family function, and social support. Multiple linear regression analysis was used to identify independent factors influencing readiness for hospital discharge among mothers with cesarean sections.
Results: The total score of readiness for hospital discharge was 136.47 ± 25.29. The quality of discharge teaching, parenting sense of competence, number of cesareans, family function, and attending antenatal classes were independent factors influencing the readiness for hospital discharge (P < 0.05) among mothers with cesarean sections.
Conclusion: The readiness for hospital discharge of mothers with cesarean sections need to be improved. Improving the quality of discharge teaching, parenting sense of competence, and family function may help improve the readiness for hospital discharge of mothers with cesarean sections.
Keywords: patient discharge, cesarean section, nursing, postpartum period, parenting, postoperative care
Introduction
Cesarean section rates are increasing worldwide and in mainland China.1 The total cesarean section rate in China increased from 28.8% in 2008 to 34.9% in 2014,2 much higher than the rate of lower than 15% recommended by the World Health Organization.3 Cesarean delivery is firmly established as the safest type of delivery for pregnancies with specific clinical conditions, such as placenta previa, placenta implantation, or intrauterine fetal distress. Compared with vaginal delivery, cesarean delivery poses a greater risk of maternal morbidity and mortality, including cardiac arrest, wound hematoma, hysterectomy, major puerperal infection, and venous thromboembolism.4,5 Besides physiological effects, the cesarean section increases the risk of postpartum depression.6,7 Moreover, the cesarean section also hurts the infant’s health, increasing neonatal intensive care unit admissions.8,9 In addition, the cesarean section also impacted the gut micro-flora, interfering with the development of the child’s immune system and increasing the risk of allergies and obesity later in life.10
Health care professionals must provide high-quality postpartum care to mothers with cesarean section to protect and facilitate maternal and child health. Mothers with cesarean sections usually stay in hospital for 2 to 6 days after delivery,11 which was determined by the inter-hospital variation and patient situation.12,13 The period of hospitalization after cesarean section is the critical time for maternal learning puerperal rehabilitation knowledge and preparing for discharge from hospital.
Health care professionals must evaluate the mothers’ readiness for discharge before discharging them from the hospital. Fenwick14 defined readiness for hospital discharge (RHD) as an assessment in which health care professionals integrate a patient’s physiological, psychological, and social phenomenon to analyze whether the patient can leave the hospital home and achieve further rehabilitation. Health care professionals can more accurately determine the patient’s discharge time by evaluating the patient’s RHD. Studies have indicated that patients with greater RHD have fewer unplanned clinical visits15 and a lower incidence of readmission.16
Recent studies showed that the RHD score of each sample varies and that mothers with higher quality of discharge teaching (QDT),17 vaginal delivery, more children, bottle feeding,18 and better maternal and neonatal health19 have higher RHD scores. Some studies have also shown a strong relationship between RHD and social support.7,20 However, Yanikkerem’s19 study showed a weak positive correlation between them (r = 0.270, P < 0.001).
RHD among mothers with cesarean sections may also relate to the family function and parenting sense of competence. Good family function contributes to parental role adaptation and improves the postpartum quality of life and marital relationships.21 Family function during the postpartum period is also a protective factor against postpartum depression.22 In addition, a good family function also enables mothers to have better parenting self-efficacy and satisfaction.23 Parenting sense of competence refers to the efficiency and ability of parents to meet various needs in childcare.24 According to Bandura,25 parents who feel more competent in their parental role will persist in the demanding parenting tasks, avoid self-blame, and achieve a sense of accomplishment and satisfaction. However, researchers have not evaluated the influence of family function and parenting sense of competence on the discharge preparation of mothers with cesarean sections.
Knowing the readiness for hospital discharge can help health care professionals to facilitate the women’s readiness for discharge and accurately determine the patients’ discharge time. However, the results on the RHD and its associated factors among mothers with cesarean sections were rare and inconsistent. Therefore, this study aimed to investigate the level of RHD of mothers with cesarean sections, identify the limitations of their preparation before discharge, and explore the influencing factors to provide a theoretical basis for clinical intervention.
Materials and Methods
Design, Setting, and Participants
A descriptive cross-sectional survey was conducted at a regional tertiary hospital in Guangzhou, China, from September 10, 2020, to March 30, 2021. This study was executed and reported in accordance with STROBE Statement: guidelines for reporting observational studies. The study recruited a consecutive convenient sample of 339 mothers with the cesarean sections. The inclusion criteria were as follows: (1) single pregnancy with a gestational age of at least 37 weeks and having a cesarean delivery; (2) the neonate having scores on the activity, pulse, grimace, appearance and respiration at 1, 5, and 10 min after delivery > 7 points. The exclusion criteria were: (1) the neonate admitted to the intensive care unit after delivery; (2) the mother having severe intraoperative and postoperative complications, including intraoperative or postoperative hemorrhage, amniotic fluid embolism, intraoperative or postoperative rescue, and severe puerperal infection.
Measures
Outcome Variable
Readiness for hospital discharge among mothers with cesarean sections was measured by the Chinese version of the readiness for hospital discharge scale-new mother form (RHDS-NMF). This scale was compiled by Weiss.26 It was translated and adapted into Chinese, and its reliability and validity were verified in 2020.27 The RHDS-NMF has four dimensions: (a) personal condition (items 2–5), which assesses the mother’s current physical and emotional conditions; (b) knowledge (items 6–12), which refers to information about the common concerns and problems of the mothers and babies during the post-hospitalization period; (c) coping ability (items 13–15), which is related to the mother’s ability to cater for her personal and the baby’s health care needs after discharge; and (d) expected social support (items 16–19), which is defined as the emotional and instrumental assistance expected to be available following hospital discharge. This scale is a self-evaluation scale that contains a total of 19 items. The first item is not included in the total score because it is a dichotomous item (yes/no), which asks the subjects whether they are ready to be discharged. The remaining items are scored from 0 to 10 points. 0 points means “completely unknown” or “not at all”, and 10 points means “completely know” or “completely able”. The total score were summed by adding all the item scores, with higher scores indicating greater RHD.
Study Factors
Sociodemographic characteristics included age, education, work status, marital status, per capita monthly household income, attending antenatal classes, main caregiver, planned feeding, and checking or not into a confinement service centre after discharge. Obstetric characteristics included primipara or not, number of cesareans, pregnancy complications, anesthesia method, neonate gender, intraoperative pain degree, and current pain degree. The obstetric characteristics were collected from the medical records.
Quality of discharge teaching was measured by the Chinese version of the quality of discharge teaching scale (QDTS).28 Discharge teaching was conceptualized as the composite of all teachings received by the mothers during their hospitalization.16 The scale consists of 18 items in three dimensions: content needed, content received, and content delivery. The content needed and content received dimensions include six pairs of parallel entries (items 1–6), and the delivery dimension includes the remaining 12 items (items 7–18). The content needed dimension measures how much information the mothers thought they needed before discharge and is used for comparison with the content received dimension, which is a measure of how much information the mothers actually received. The content delivery dimension refers to the skill of the nurses in providing the information needed for discharge. Each item score ranges from 0 to 10. The total score of the scale is the sum of the scores on the subscale of content received and delivery, with higher total scores indicating better discharge teaching.16
The parenting sense of competence was measured by the Parenting Sense of Competence Scale (PSOC).29 The Chinese version was validated to have satisfactory validity and reliability.30 It has 17 items and contains two subscales, including the efficacy and satisfactory subscales. Each item scores from 1 to 6, which means “absolutely disagree” to “absolutely agree”. Item 2–5, 8, 9, 12, 14, 16 were scored backwards. The higher the total score of POSC, the higher the mother’s parenting sense of competence.
Social support was measure by the maternity social support scale (MSSS).31 The Chinese version of the scale has a total of six items, using a 5-point scoring method from 1 to 5 points. Higher score indicates more sufficient social support; 0–18 is considered as low level of social support, 19–24 as medium, and > 24 is considered as adequate support. The reported Cronbach’s α coefficient was 0.75, and the test-retest reliability was 0.71.32
Family function was measured by the Family Adaptation, Partnership, Growth, Affection, Resolve (APGAR) questionnaire.33 The Chinese version of APGAR questionnaire has five questions. Each question has three choices, including “almost rarely”, “sometimes”, and “often”, which are counted 0–2 points, respectively. The lower the score, the worse the family function. The reported Cronbach’s α coefficient was 0.94, and the test-retest reliability was 0.80 ~ 0.83.34
Ethical Consideration and Procedure
Ethical approval was obtained from the Institutional Review Board (IRB) of the study hospital (approval number: 202001188). The research conforms to the provisions of the Declaration of Helsinki as revised in Edinburgh in 2000. All participants were assured that their data would be kept confidential, the participation was entirely voluntary, and they could withdraw from the study at any time. All women’ s written consents were obtained before inclusion.
Two nurses who had worked in the postpartum ward over 5 years were selected and trained to collect data as research assistant (RA). In the morning of the day the mothers were discharged, the RAs identified the eligible mothers and explained the aim, content, risks, and benefits of the study to them. Then, the mothers were requested to sign the informed consent form and complete the questionnaires, which took 15 to 30 min. The RAs checked and asked the mothers to complete the missing items, if any. Then, the RAs collected the maternal information by reviewing the medical records.
Data Analysis
Data were analyzed using IBM SPSS Statistics 25.0. Descriptive statistics were used to present sociodemographic and obstetric characteristics and the variables. The Q-Q plot and P-P plot were used to test the normality of the variables. All the data of the RHD, QDTS, POSC, MSSS, and APGAR were indicated normal distributions. Therefore, Pearson Correlation analysis was conducted to determine the correlations between the RHD and the QDTS, POSC, MSSS, and APGAR scores. The effect of each factor on the RHD score was analyzed by univariate analysis. The significant factors were then analyzed by multiple linear regression analysis. All models used a forward stepwise likelihood ratio. A two-sided P < 0.05 was considered statistically significant in this study.
Results
The Characteristics of the Mothers with Cesarean Sections
A total of 379 mothers were approached in this study, and six of them refused to participate due to physical exhaustion and having no time. Among the mothers who agreed to participate in the study, two did not returned the questionnaires, leaving a response rate of 99.5%. Among them, 339 questionnaires were valid, with an effective rate of 91.4%.
Table 1 presented the sociodemographic and obstetric characteristics of the mothers. The ages of the mothers ranged from 21 to 44 years old, with an average age of 31.16 years old (SD: 4.37). Most mothers were married (98.5%) and employed (79.7%). The majority of the mothers had an education of junior college or higher vocational school or above. Over half of the mothers had a per capita monthly household income of more than 10,000 yuan. Only 8.8% of mothers attended all the antenatal classes provided freely by the study hospital.
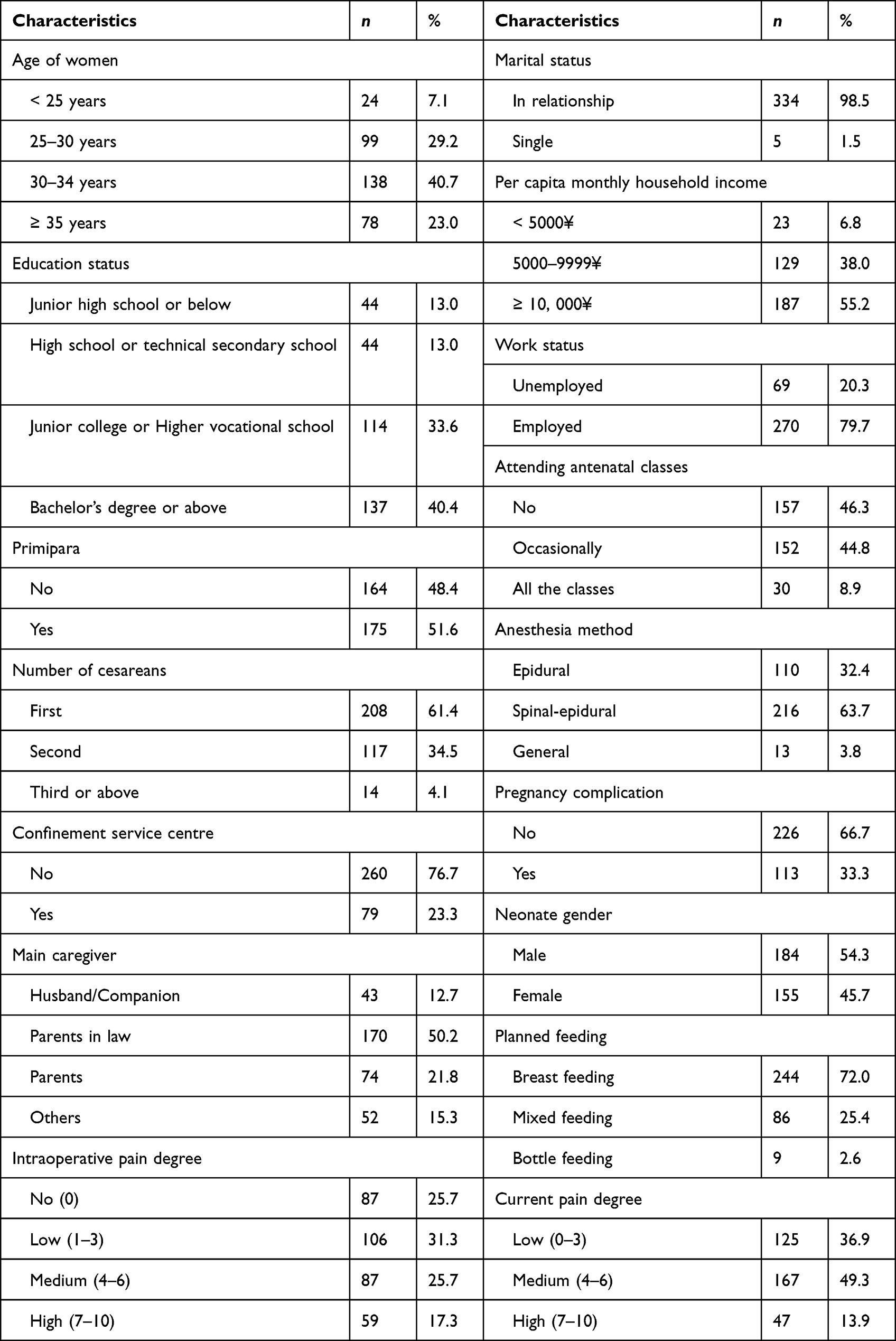 |
Table 1 Sociodemographic and Obstetrics Characteristics of the Participants (n = 339) |
Half of the mothers were primipara. About two thirds (61.4%) of the present cesarean sections were the first one. The average length of stay in hospital after delivery was 3.27 days (SD: 0.61), ranging from 3 to 7 days. The average score of current pain was 4.35 ± 1.89, ranging from 0 to 10. The pain degree was medium.
The RHD, QDTS, PSOC, MSSS, and APGAR Among Mothers with Cesarean Sections
Table 2 presented the descriptive statistics of the study variables. Most (94.4%) of the mothers with cesarean sections reported that they were prepared for discharge. The total score of the RHD ranged from 55 to 180, with an average of 136.47± 25.29, and the average score of each item was 7.58 ± 1.41. Dimensions with scores from high to low were expected social support, personal condition, knowledge, and coping ability.
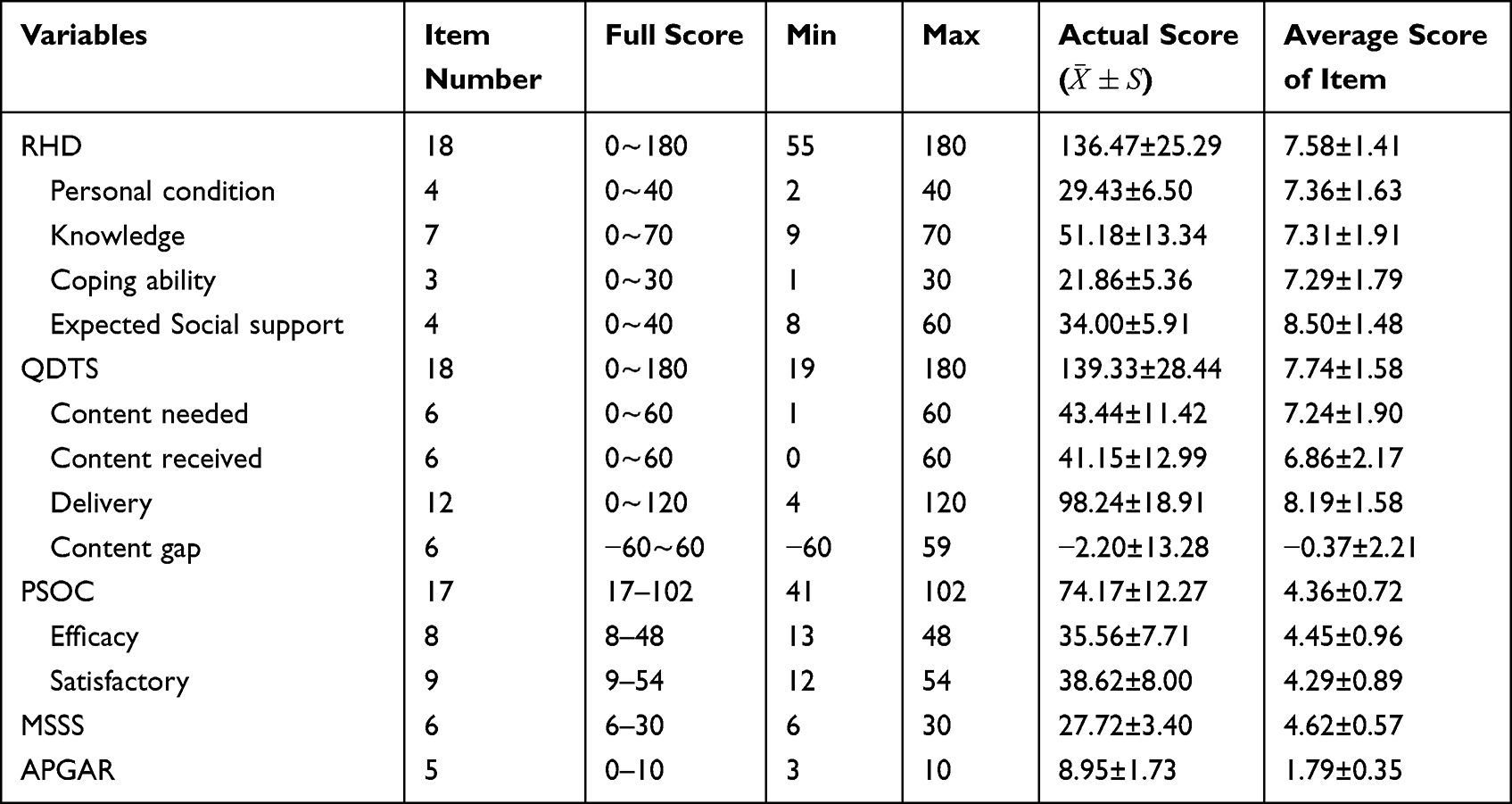 |
Table 2 Descriptive Statistics of the Study Variables (n=339) |
The total score of the QDTS was 139.33 ± 28.44, and the average score of each item was 7.74 ± 1.58. The dimensions with scores from low to high were content received, content needed, and delivery. The two items with the lowest average scores of the QDTS were items 2b (How much information did you receive from your nurses about your emotions after you go home?) and 4b (How much training do you get in medical treatment before you left the hospital and went home?). The total score of the PSOC was 74.17 ± 12.27, with an average item score of 4.36 ± 0.72. The average score of each item of the MSSS and the APGAR was 4.62 ± 0.57 and 1.79 ± 0.35, respectively.
Correlation Between the RHD and the Study Factors Among Mothers with Cesarean Sections
Table 3 demonstrated the correlation between the RHD and the study factors. The total score of the RHD was significantly correlated with the total score of the QDTS (r = 0.678, P < 0.001), PSOC (r = 0.517, P < 0.001), MSSS (r = 0.398, P < 0.001), and APGAR (r = 0.345, P < 0.001).
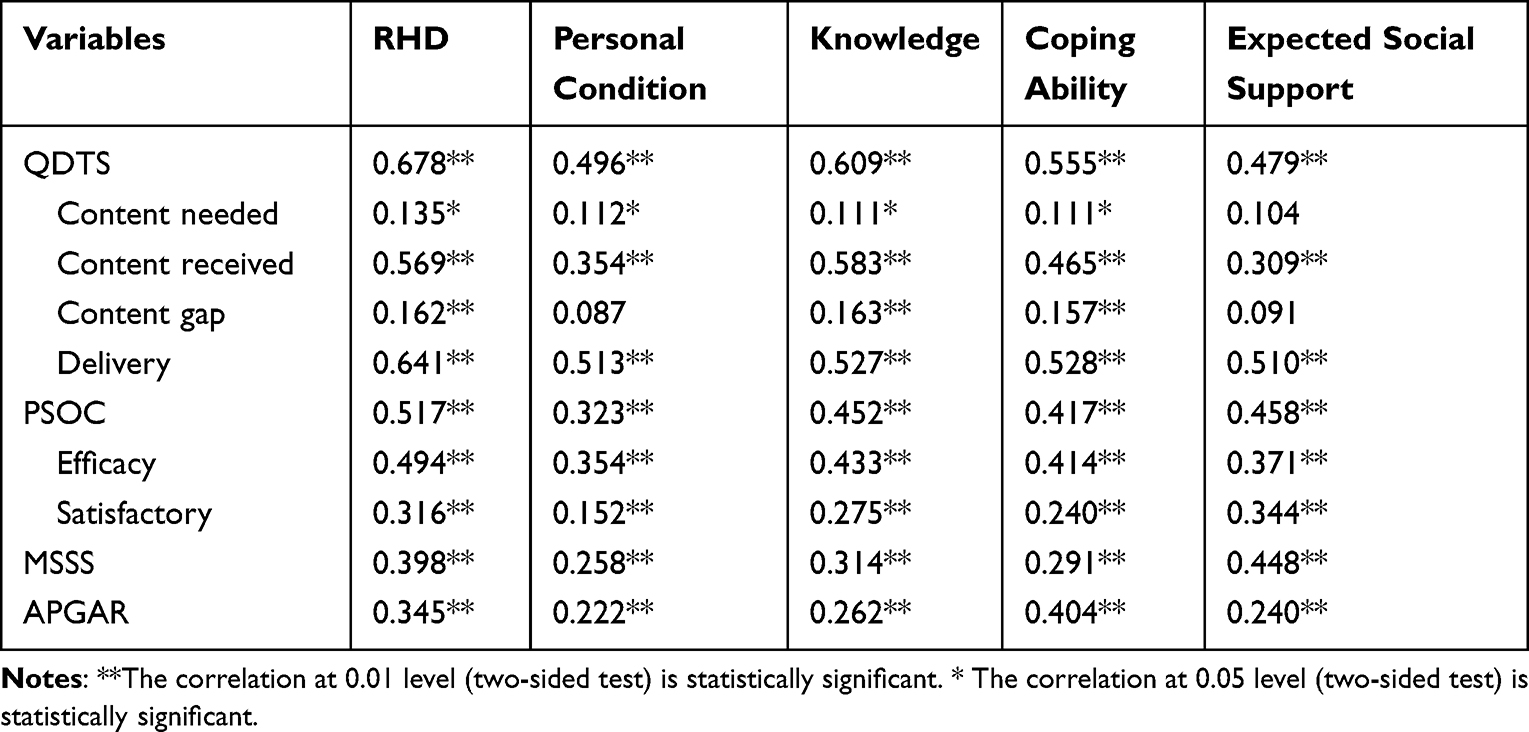 |
Table 3 Correlation Between the RHD and QDTS, PSOC, MSSS and APGAR of Mothers with Cesarean Section (n = 339) |
The Factors Independently Associated with the RHD Among Mothers with Cesarean Sections
Table 4 presented the differences on the RHD among various groups. Factors including attending antenatal classes, checking or not into a confinement service centre, primipara or not, number of cesareans, and intraoperative and current pain degree had a statistically significant effect on the RHD of the mothers with cesarean sections (P < 0.05). The results presented no statistical significance in univariate analysis was showed in Supplementary Table 1.
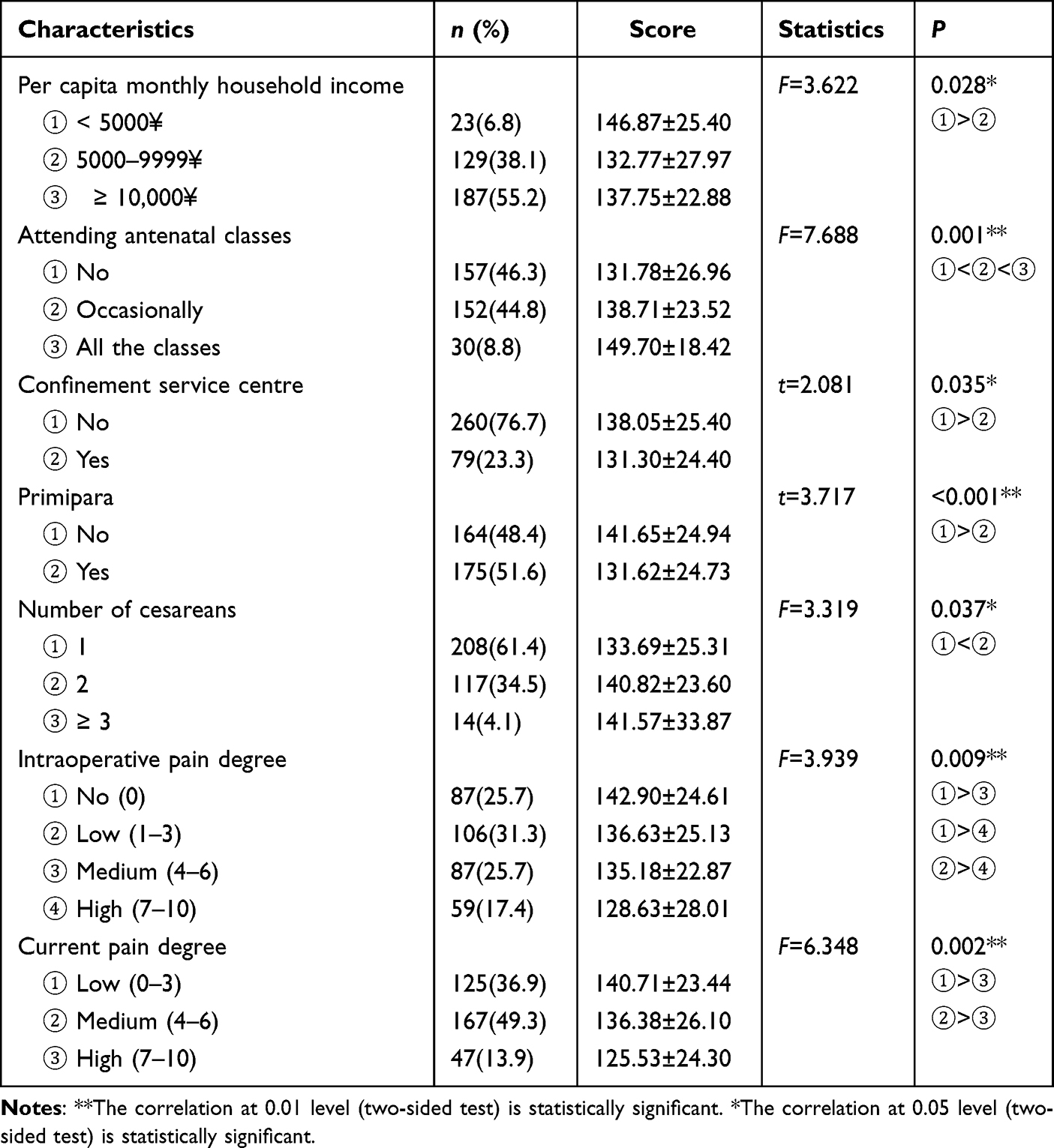 |
Table 4 Differences on the RHD Scores Among Various Groups (n = 339) |
The total score of the RHD was taken as the dependent variable, and the factors with statistical significance (P < 0.05) in the univariate analysis and factors that significantly correlated with RHD (r ≥ 0.3, P < 0.05) in the correlation analysis were used as the independent variables. A stepwise multiple linear regression analysis was applied. In addition, variance inflation factor (VIF) is used to judge the multicollinearity between independent variables. When the VIF is greater than 4, there may be collinearity problem. The results of the multiple linear regression were shown in Table 5.
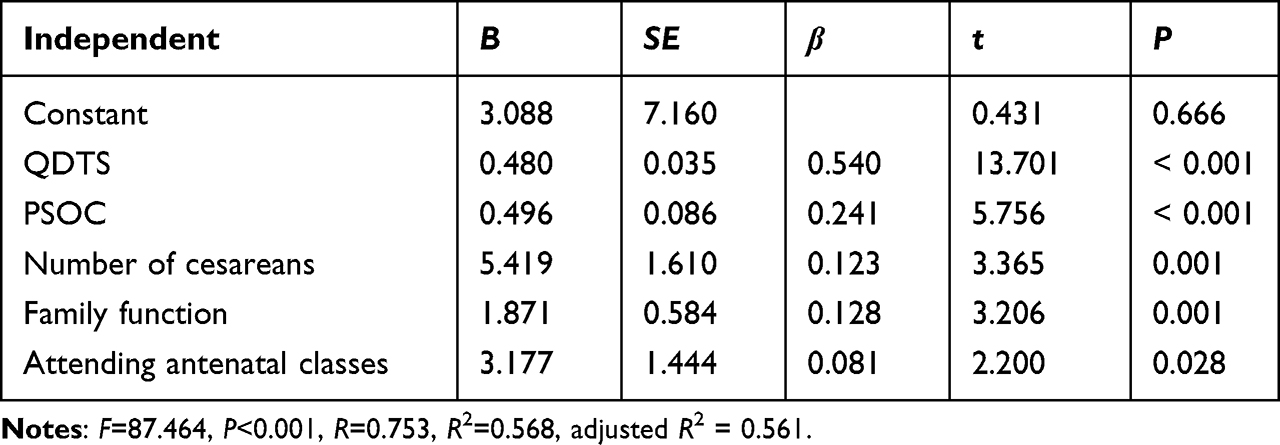 |
Table 5 The Results of the Multiple Linear Regression Analysis (Stepwise) (n = 339) |
The results showed that the total score of the QDTS and PSOC, number of cesareans, family function, and attending antenatal classes were the main factors influencing RHD among mothers with cesarean sections (adjusted R2 = 0.561, F = 87.464, P < 0.001). VIF of the independent variable ranges from 1.025 to 1.345, indicating that there is no multicollinearity problem between variables.
Discussion
An understanding of the readiness for discharge and its associated factors in mothers with cesarean sections is important to guide the health care professionals to help the mothers preparing for discharge from hospital. Now in mainland China, nearly 99.9% women are given birth in the hospitals. Most women choose public hospitals, and their medical cost are covered by the public health insurance.35 A minority of women choose private hospitals to give birth and the cost are not covered by public health insurance. The community nurses give three home visits at 3, 14 and 28 days after mothers are discharged from hospital, respectively.36
The present study found that although 94.4% of the mothers with the cesarean sections were ready for discharge from hospital, the total score of the RHD was only 136.47 ± 25.29, which was lower than those of the studies by Malagon-Maldonado,37 Weiss & Lokken,17 and Yanıkkerem.19 It may be due to that all the mothers in the present study had a cesarean section. The moderate level of current pain affected their sleeping quality. Mothers with cesarean sections must endure physical pain while completing self-care, infant feeding, and even housework. They also need to master more medical knowledge and skills, such as disinfection of surgical incisions, changing dressings, and other medical treatments. In addition, most of the mothers (61.4%) in this study were having their first cesarean section. During the short period of hospitalization, they experienced surgery, delivery, and discharge, and completed the mother role transition. Lack of experience and knowledge may decrease their coping ability.
The mothers in the present study had the lowest score on the knowledge dimension of the RHD. This can be explained by three reasons. Firstly, the average length of stay in hospital after delivery was short. Secondly, most of the mothers were having their first cesarean section, and half of them were primiparas without previous experiences. A large amount of knowledge needs to be mastered during hospitalization, including care of the maternal puerperium, surgical wounds, newborns, and breastfeeding. Thirdly, assessing the maternal knowledge was not an routine procedure before discharge.
The present study found that quality of discharge teaching was the most important factors independently associated with the RHD. However, the mothers in the present study reported that their actual content received from discharge teaching did not fully meet their expectations. It may be due to the fact that the discharge teaching was delivered on the morning of the day of discharge. Due to the COVID-19 pandemic, husbands were not allowed to accompany the mothers. On the day of discharge, the mothers were busy caring for their babies and handling discharge matters, and they may have no interest in discharge teaching. It suggested that health care professionals may give the discharge teaching in the earlier days of hospitalization rather than on the day of discharge. More they should avoid delivering a large amount of knowledge in a short time, or even at one time. For example, health care professionals allow mothers to observe the nurses bathing the babies and disinfecting the umbilical cord, and guide them on relevant skills.
In addition, the item with the lowest average score belonged to the coping ability dimension. That is, “how much do you know about services and information available to you in your community after you go home”. In recent years, the Chinese government vigorously strengthened the construction of community health services, but citizens’ awareness and utilization of these services were still low.38 Health care professionals can give guidance on community service resources to increase their utilization and avoid patients gathering in higher-level hospitals and aggravating the shortage of medical resources.
The two items with the lowest average scores of the QDTS were items 2b and 4b, indicating that the mothers were lacking in guidance on emotional regulation and medical treatment training before discharge. The traditional Chinese culture produces limitations in terms of correct cognition regarding mothers’ psychological problems. Mothers are not good at diverting and venting bad emotions. Moreover, they are ashamed to seek help from professionals and lack channels and resources for psychological counseling. Therefore, health care professionals should provide support in emotional regulation. They can incorporate the knowledge of prevention, clinical manifestations, and treatment of postpartum anxiety and depression into the content of discharge teaching and provide access to professional help such as psychological counseling. However, faced with the current shortage of health care professionals in China, nursing managers should allocate nurses’ time reasonably. More attention should be directed to guidance and training in medical treatment using various forms of teaching methods such as video, live demonstrations, group teaching, and feedback questions to improve the quality of discharge teaching. Health care professionals can provide educational videos and materials to supplement the lack of discharge guidance of family members and main caregivers.
Apart from the quality of discharge teaching, the present study found that the RHD among the mothers with cesarean sections were related to parenting sense of competence, family function, number of cesarean sections, and attending antenatal classes. The parenting sense of competence refers to the efficiency and ability of parents to meet various needs in the process of parenting.24 The mothers in the present study had a moderate level of parenting sense of competence. Due to the limited activities after surgery, mothers found it difficult to take care of the newborn independently. In addition, they were worried about their competence in childcare without professional guidance after discharge, which affected their readiness for hospital discharge. Therefore, health care professionals should strengthen the guidance of parenting knowledge for mothers with cesarean sections, especially the identification and treatment of the physiological changes and common abnormalities of infants and young children, to improve their parenting sense of competence. By recognizing the behaviors, facial expressions and cries of infants to understand their needs, mothers can gain a sense of parenting accomplishment, thereby improving their readiness for discharge.
The mothers with better family function also had better readiness for discharge. In most Chinese families, grandparents take care of the baby. With better family function, family members do not only share most of the housework and baby care, but also show strong family stress flexibility. Moreover, mothers with sufficient social support can obtain emotional support and knowledge about postpartum rehabilitation and parenting, alleviating the anxiety caused by poor role transition after discharge. Therefore, mothers who had better family function showed better readiness for discharge.
The present study also found that mothers with the second cesarean section had better readiness for discharge than those with the first one because of existing experience in childbirth and parenting. They presented a greater ability to deal with emergencies after discharge. Regarding attending the antenatal classes, mothers who attended regularly and completed all the antenatal classes got the highest RHD score. Then, those who attended occasionally had higher RHD scores than those who never attended. The antenatal classes in the study hospitals involved high-risk pregnancy management, nutrition and exercise during pregnancy, perinatal emotional management, childbirth knowledge, postpartum rehabilitation, neonatal bathing and massage, and breastfeeding. Mothers with cesarean sections who attended and completed the antenatal classes acquired comprehensive health care knowledge on women and babies during the perinatal period. It laid a theoretical foundation for the learning of rehabilitation and parenting skills later, which effectively enhanced the level of readiness for discharge. Health care professionals should be aware of the importance of antenatal education.
The Limitations of the Study
The findings of this study are subject to limitations. Firstly, the study was conducted with a convenient sample from a single site. Secondly, studies have indicated that nurses and patients have different perceptions of RHD,39,40 but only patients’ perceptions of RHD were assessed in this study. These perceptions reflected the patient’s reality but may not have represented the reality of the clinical environment or the actual teaching. The hospital may need to shorten the length of staying in the hospital because of the limited health insurance.35
Future studies could be implemented from the perspectives of other stakeholders, such as those of the family members and health care professionals, to ensure a further comprehensive understanding of mothers’ RHD. All these factors limit the generalizability of the findings. However, given the paucity of literature related to RHD among mothers with cesarean sections, this study provides insight for future research.
Conclusion and Implication
The present study found that the RHD in mothers with cesarean sections was independently related to the quality of discharge teaching, parenting sense of competence, family function, number of cesarean sections, and attending antenatal classes. Clinical interventions such as increasing antenatal classes attendance, improving the quality of discharge teaching, and family function promotion could be integrated into postpartum care in China.
Abbreviations
APGAR: Family Adaptation, Partnership, Growth, Affection, Resolve; CVI: Content validity index; IRB: Institutional Review Board; MSSS: Maternity social support scale; PSOC: Parenting sense of competence scale; QDT: Quality of discharge teaching; QDTS: Quality of discharge teaching scale; RA: Research assistant; RHD: Readiness for hospital discharge; RHDS-NMF: Readiness for Hospital Discharge Scale-New Mother Form.
Data Sharing Statement
All data generated and analyzed during this study are included in this published article and its Supplementary Information Files.
Acknowledgments
The authors sincerely thank Wei-xia Wu, Jing Zhang and Lin Shi for data collection. And we also thank Li-ping Zhou and Li Huang for providing excellent technical support.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Funding
No funding support.
Disclosure
The authors declare that they have no conflicts of interest in this study.
References
1. Vogel JP, Betran AP, Vindevoghel N, et al. Use of the Robson classification to assess caesarean section trends in 21 countries: a secondary analysis of two WHO multicountry surveys. Lancet Glob Health. 2015;3(5):e260–e270. doi:10.1016/S2214-109X(15)70094-X
2. Li HT, Luo S, Trasande L, et al. Geographic Variations and Temporal Trends in Cesarean Delivery Rates in China, 2008-2014. JAMA. 2017;317(1):69–76.
3. Who. Appropriate technology for birth. Lancet. 1985;2(8452):436–437.
4. Liu S, Liston RM, Joseph KS, et al. Maternal mortality and severe morbidity associated with low-risk planned cesarean delivery versus planned vaginal delivery at term. CMAJ. 2007;176(4):455–460.
5. Clark SL, Belfort MA, Dildy GA, et al. Maternal death in the 21st century: causes, prevention, and relationship to cesarean delivery. Am J Obstet Gynecol. 2008;199(1):31–36, 91–92.
6. Xu H, Ding Y, Ma Y, et al. Cesarean section and risk of postpartum depression: a meta-analysis. J Psychosom Res. 2017;97:118–126.
7. Zhao XH, Zhang ZH. Risk factors for postpartum depression: an evidence-based systematic review of systematic reviews and meta-analyses. Asian J Psychiatr. 2020;53:102353.
8. Kupari M, Talola N, Luukkaala T, et al. Does an increased cesarean section rate improve neonatal outcome in term pregnancies? Arch Gynecol Obste. 2016;294(1):41–46.
9. Khasawneh W, Obeidat N, Yusef D, et al. The impact of cesarean section on neonatal outcomes at a university-based tertiary hospital in Jordan. BMC Pregnancy Childbirth. 2020;20(1):335.
10. Cegolon L, Mastrangelo G, Maso G, et al. Understanding Factors Leading to Primary Cesarean Section and Vaginal Birth After Cesarean Delivery in the Friuli-Venezia Giulia Region (North-Eastern Italy), 2005-2015. Sci Rep. 2020;10(1):380.
11. Pan J, Hei Z, Li L, et al. The Advantage of Implementation of Enhanced Recovery After Surgery (ERAS) in Acute Pain Management During Elective Cesarean Delivery: a Prospective Randomized Controlled Trial. Ther Clin Risk Manag. 2020;16:369–378.
12. Cegolon L, Mastrangelo G, Campbell OM, et al. Length of stay following cesarean sections: a population based study in the Friuli Venezia Giulia region (North-Eastern Italy), 2005-2015. PLoS One. 2019;14(2):e210753.
13. Cegolon L, Mastrangelo G, Maso G, et al. Determinants of length of stay after cesarean sections in the Friuli Venezia Giulia Region (North-Eastern Italy), 2005-2015. Sci Rep. 2020;10(1):19238.
14. Fenwick AM. An interdisciplinary tool for assessing patients’ readiness for discharge in the rehabilitation setting. J Adv Nurs. 1979;4(1):9–21.
15. Meng N, Liu R, Wong M, et al. The association between patient-reported readiness for hospital discharge and outcomes in patients diagnosed with anxiety disorders: a prospective and observational study. J Psychiatr Ment Health Nurs. 2020;27(4):380–392.
16. Weiss ME, Piacentine LB, Lokken L, et al. Perceived readiness for hospital discharge in adult medical-surgical patients. Clin Nurs Spec. 2007;21:31–42.
17. Weiss ME, Lokken L. Predictors and outcomes of postpartum mothers’ perceptions of readiness for discharge after birth. J Obstet Gynecol Neonatal Nurs. 2009;38(4):406–417.
18. Malagon-Maldonado G, Connelly CD, Bush RA. Predictors of Readiness for Hospital Discharge After Birth: building Evidence for Practice. Worldviews Evid Based Nurs. 2017;14(2):118–127.
19. Yanikkerem E, Esmeray N, Karakus A, et al. Factors affecting readiness for discharge and perceived social support after childbirth. J Clin Nurs. 2018;27(13–14):2763–2775.
20. Zhang J, Yao S, Huang F, et al. Exploring the Role of Social Support between Discharge Teaching and Readiness for Discharge in Ocular Fundus Disease Patients: a Cross-Sectional Study. J Ophthalmol. 2021;2021:5547351.
21. Ngai FW, Ngu SF. Family sense of coherence and family and marital functioning across the perinatal period. Sex Reprod Healthc. 2016;7:33–37.
22. Xie RH, Yang J, Liao S, et al. Prenatal family support, postnatal family support and postpartum depression. Aust N Z J Obstet Gynaecol. 2010;50(4):340–345.
23. Angley M, Divney A, Magriples U, et al. Social support, family functioning and parenting competence in adolescent parents. Matern Child Health J. 2015;19(1):67–73.
24. Suwansujarid T, Vatanasomboon P, Gaylord N, et al. Validation of the parenting sense of competence scale in fathers: thai version. Southeast Asian J Trop Med Public Health. 2013;44(5):916–926.
25. Bandura A. Self Efficacy: The Exercise of Control. New York: W.H. Freeman; 1997.
26. Weiss ME, Ryan P, Lokken L. Validity and reliability of the Perceived Readiness for Discharge After Birth Scale. J Obstet Gynecol Neonatal Nurs. 2006;35(1):34–45.
27. Chen X, Zhao T, Liu L, et al. Chinesization of Readiness for Hospital Discharge Study ⁃ New Mother Form (RHDS⁃NMF) and its reliability and validity test. Chine Nursing Res. 2020;34(3):407–413.
28. Wang B, Wang H, Yang C. Reliability and validity of the Chinese version of the Quality of Discharge Teaching Scale. Chin J Nurs. 2016;51(6):752–755.
29. Gibaud-Wallston. Self-esteem and situational stress: factors related to sense of competence in new parents. George Peabody College Teachers. 1977;1:453.
30. Wang B, Wang H, Yang C. The reliability and validity of the Chinese version of Parenting Sense of Competence Scale. Chine J Nursing. 2014;51(6):752–755.
31. Webster J, Linnane JW, Dibley LM, et al. Measuring social support in pregnancy: can it be simple and meaningful? Birth. 2000;27(2):97–101.
32. Li G, Wei H, Du K, et al. Reliability and validity of the Chinese version of Maternity Social Support Scale. Sichuan Mental Health. 2020;33(3):268–271.
33. Smilkstein G, Ashworth C, Montano D. Validity and reliability of the family APGAR as a test of family function. J Fam Pract. 1982;15(2):303–311.
34. Nan H, Ni MY, Lee PH, et al. Psychometric evaluation of the Chinese version of the Subjective Happiness Scale: evidence from the Hong Kong FAMILY Cohort. Int J Behav Med. 2014;21(4):646–652.
35. Qiao J, Wang Y, Li X, et al. A Lancet Commission on 70 years of women’s reproductive, maternal, newborn, child, and adolescent health in China. Lancet. 2021;397(10293):2497–2536.
36. Ministry of health of the people’s republic china. Notification of Issuance Maternal Health Care Management Criterion and Maternal Health Care Service Criterion. Available from: http://www.nhc.gov.cn/zwgkzt/wsbysj/201107/52320.shtml.
37. Malagon Maldonado G, Connelly CD, Bush RA. Predictors of Readiness for Hospital Discharge After Birth: building Evidence for Practice. Worldviews Evidence Based Nursing. 2017;14(2):118–127.
38. Zhao P, Han X, You L, et al. Maternal health services utilization and maternal mortality in China: a longitudinal study from 2009 to 2016. BMC Pregnancy Childbirth. 2020;20(1):220.
39. Weiss M, Yakusheva O, Bobay K. Nurse and patient perceptions of discharge readiness in relation to postdischarge utilization. Med Care. 2010;48(5):482–486.
40. Staveski SL, Parveen VP, Madathil SB, et al. Nurse and parent perceptions associated with the Parent Education Discharge Instruction Programme in southern India. Cardiol Young. 2016;26(6):1168–1175.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.