")
Back to Journals » Clinical Ophthalmology » Volume 18
Rates of Laser Trabeculoplasty by Ophthalmologists and Optometrists: A Comparative Analysis of the CMS Medicare Public Use File
Authors Hussain ZS , Muayad J , Harvey BJ, Al-Aswad LA , Fakoya AO , Yousefi S
Received 24 September 2023
Accepted for publication 4 December 2023
Published 30 January 2024 Volume 2024:18 Pages 269—275
DOI https://doi.org/10.2147/OPTH.S438052
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Zain S Hussain,1,2 Jawad Muayad,3 Ben J Harvey,1 Lama A Al-Aswad,4 Adegbenro OJ Fakoya,5 Siamak Yousefi6
1Department of Ophthalmology, Dean McGee Eye Institute, Oklahoma City, OK, USA; 2Department of Ophthalmology, University of Medicine and Health Sciences, Basseterre, Saint Kitts and Nevis; 3Department of Ophthalmology, Texas A&M School of Medicine, Houston, TX, USA; 4Department of Ophthalmology, Scheie Eye Institute, University of Pennsylvania, Philadelphia, PA, USA; 5Department of Cellular Biology and Anatomy, Louisiana State University Health Sciences Center, Shreveport, LA, USA; 6Department of Ophthalmology, University of Tennessee Health Science Center Hamilton Eye Institute, Memphis, TN, USA
Correspondence: Siamak Yousefi, University of Tennessee Hamilton Eye Institute Department of Ophthalmology, 930 Madison Avenue, Memphis, TN, 38163, USA, Tel +1 901-448-7831, Email [email protected]
Purpose: To provide a comparative analysis of rates of laser trabeculoplasty (LTP) among eye care providers in the USA.
Methods: This retrospective cohort analysis utilized the Centers for Medicare and Medicaid Services (CMS) Public Use File (PUF), 2015– 2018. We used CPT code 65855 to select eye care providers who performed LTP in three key US states (KY, LA, and OK). Primary outcomes were eye provider differences in provider count, service count, unique beneficiary count, and Medicare-allowed payments. Asymptotic two-sided chi-squared tests were executed. Statistical significance was achieved at p< 0.05.
Results: The sum of Medicare-allowed payments for LTP in all three states in 2018 was roughly 26% lower than in 2015. The proportion of Medicare-allowed payments furnished by optometrists increased from 11.3% to 17.9% between 2015 and 2018 (p< 0.001). Relative to ophthalmologists, we observed significant increases in optometric Medicare-allowed payments in KY, LA, OK, and the all-inclusive tri-state cohort (all p< 0.001). Furthermore, significant optometric increases in number of providers performing LTP (p=0.007), number of unique Medicare beneficiaries seen (p< 0.001), and number of LTP services billed (p< 0.001) were observed relative to ophthalmologists.
Conclusion: The recent expansion of surgical authority by optometrists in key US states is creating a tangible impact on ophthalmologic and optometric practice patterns. The findings of this study may act as provision for policymakers in the context of continually evolving guidelines for optometric surgical expansion.
Keywords: surgical authority, optometric surgical expansion, policymaking, Medicare
Introduction
Currently, the American Academy of Ophthalmology (AAO), European Glaucoma Society (EGS), and South-East Asia Glaucoma Interest Group (SEAGIG) recommend laser trabeculoplasty (LTP) as an effective first-line treatment for open-angle glaucoma (OAG).1,2 LTP utilizes a short-pulse 532 nm neodymium-doped yttrium aluminum garnet (YAG) laser, and is a relatively common procedure that has demonstrated efficacious reduction in intraocular pressures while maintaining a cost-effective stance compared to alternative traditional glaucoma therapeutics, most notably in patients struggling with medication adherence.3,4
The surgical scope of practice has been continuously expanding for optometrists in the past few decades in the USA. Since the inception of the 1998 “optometry bill” in the state of Oklahoma, optometrists nationwide have promulgated their firm stance of rightful surgical authority for certain laser procedures, including selective laser trabeculoplasty (SLT).1,2 Recently, the state of Oregon deliberated House Bill 4541, which would authorize optometrists to perform traditional ophthalmology-specific procedures, including the use of lasers and ultrasound-guided technology.3 It is apparent that a state of heightened tension is created between ophthalmologic and optometric communities during similar deliberations. The outcomes of related congressional proposals are not uniform, with states such as Vermont and Idaho rejecting in-house proposals for optometric surgical expansion.4,5
Few US national studies have attempted to understand practice patterns and co-management rates between ophthalmologic and optometric communities. A Mayo Clinic study by Erie et al in 2016 utilized the Physician and Other Supplier Public Use File (PUF) provided by the Centers for Medicare and Medicaid Services (CMS) to characterize co-management rates of cataract surgery between ophthalmologists and optometrists.6 US national LTP rates for Medicare beneficiaries with OAG reached a historic high in 2006 at 824.3 per 10,000 person-years, then decreased to 741 per 10,000 person-years by 2009 (10.1% decrease, p=0.004).7 While this national decrease in LTP rates could be partly rationalized by reduced reimbursement rates, the timely advent of the new SLT procedure is likely the responsible factor. In addition, significant variations in geographical frequencies were characterized between 2002 and 2009, with a 93.2% increase from 314 to 607 per 10,000 OAG person-years in the East South-Central and East North-Central regions of the USA, respectively (p<0.001).7 The estimated travel time (ETT) among Medicare beneficiaries who were recipients of optometric surgical care was within 30 minutes of an ophthalmologist’s office for roughly 50% of the beneficiary population in Kentucky, Oklahoma, and New Mexico.8 In addition, no significant differences in geographical accessibility to YAG laser capsulotomy in Oklahoma were determined with respect to type of eye provider.9 In 2016, Stein et al specified 189% increased hazards of Medicare beneficiaries requiring an additional LTP in the same eye if an optometrist, as opposed to an ophthalmologist, had performed the first laser procedure.10 Lastly, Lee et al, in 2018, characterized a 19.11-fold increased rate of LTP for patients serviced at ophthalmology-only clinics compared to patients serviced at optometry-only clinics in the Veterans Affairs health care system.11
This pilot study of the CMS PUF shares a comparative national analysis of LTP-associated metrics between ophthalmologists and optometrists. The findings may act as provision for policymakers in the context of continually evolving guidelines for optometric surgical expansion, while also highlighting key areas warranting additional investigation in future works.
Materials and Methods
This retrospective cohort analysis utilized the CMS Provider Utilization and Payment Data 2015–2018: Physician and Other Supplier PUF.12 The PUF database includes claims for Medicare beneficiaries receiving LTP for the treatment of glaucoma. These claims are available as aggregated datasets organized by National Provider Identification (NPI) and Healthcare Common Procedure Coding System/Place of Service billing codes (HCPCS). Relevant variables of interest include provider type (ophthalmologist or optometrist), number of services performed by each provider (service count), and Medicare-allowed payment per service performed. The PUF does not yield data for providers who offered a specific service to 10 or fewer Fee-For-Service (FFS) Medicare beneficiaries, which acts to preserve patient confidentiality. We used CPT code 65855 to select only providers that have performed LTP, including argon laser trabeculoplasty (ALT) and SLT. We then selected a subset of data originating from three key states: Oklahoma (OK), Louisiana (LA), and Kentucky (KY). An all-inclusive cohort containing data from all three states was created to curate pooled comparisons.
We assessed differences in provider count, service count, and unique beneficiary count across a 4-year time interval based on asymptotic two-sided chi-squared statistical tests. All chi-squared analyses with low sample sizes were reserved for Fisher’s exact test analysis. We then aggregated the Medicare-allowed payments for LTP per provider type. Global probability plots of summed Medicare-allowed payments were created (Figure 1). Because we used publicly available, freely accessible, patient de-identified data, this scholarly work was not considered human subject research and did not require patient consent. Therefore, this study was exempt from IRB review. Statistical analyses were performed with IBM SPSS Premium Version 29 (IBM Corp, Armonk, NY, USA).
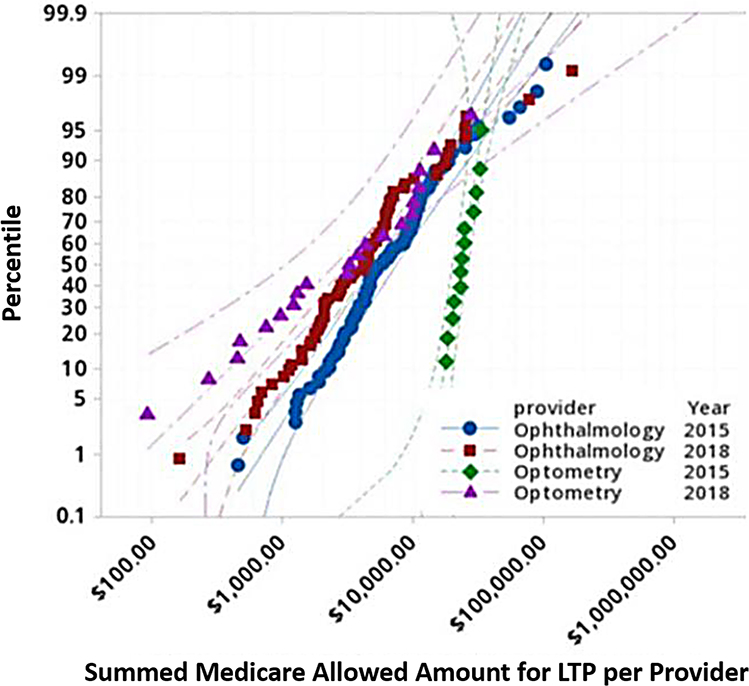 |
Figure 1 Probability Plot of Summed Fee-for-Service LTP Medicare Allowed Payment by Provider Type & Year. |
Results
In 2018, the total sum of Medicare-allowed payments for LTP billed by ophthalmologists and optometrists across the country was estimated to be $27,576,575, which was about 33% lower than the total sum of nationwide Medicare-allowed payments of $41,277,040 in 2015. Within the same Medicare-defined year, the total sum of Medicare-allowed payments from KY, LA, and OK altogether (tri-state cohort) was estimated to be $1,107,114, a 26% decrease from the 2015 tri-state sum of $1,511,594 in 2015. Despite these findings, the proportion of Medicare-allowed payments furnished by optometrists within the tri-state cohort increased from 11.3% ($171,966.5) to 17.9% ($198,953) between 2015 and 2018, with ophthalmologists receiving a consequential and proportionate decrease from 88.7% to 82.1% across the same time frame (p<0.001). Furthermore, similar ophthalmologic payment decreases were seen individually in all three states (KY, LA, and OK) (all p<0.001). Additional information regarding state-specific stratification of Medicare-allowed payments is provided in Table 1.
 |
Table 1 Fee-for-Service Medicare-Allowed Laser Trabeculoplasty Payments, $ (%) |
Of those performing LTP, ophthalmologic provider counts decreased by 21% (N=22) while optometric provider counts increased by 33% (N=7) in the tri-state cohort from 2015 to 2018 (p=0.01). Across the same time frame, no significant differences in state-stratified provider counts were observed in KY (p=0.33), LA (p=0.99), and OK (p=0.14), likely a result of low sample sizes. Regarding LTP service counts, we observed a 78.7%, 76.1%, and 58.8% increase in number of optometric LTP services in KY, OK, and the tri-state group, respectively (all p<0.001). Conversely, both ophthalmologic and optometric LTP service counts in LA within the same time period decreased by 23.5% and 34.4%, respectively. Regarding unique Medicare beneficiaries, our tri-state cohort observed a 52% increase in beneficiaries seen by optometrists; however, a 11% decrease in unique beneficiaries under ophthalmologic care was seen across the same time interval (KY, p<0.001; OK, p=0.048; tri-state cohort, p<0.001; LA, p=0.29).
Discussion
The Medicare PUF enables clinician and policymakers to evaluate practice patterns of health care services administered by physicians and non-institutional health care providers, including optometrists, among the FFS Medicare beneficiary patient population.13 Owing to the relatively low number of states allowing optometrists to perform LTP prior to 2015, in conjunction with an absence of CMS PUF edition release after 2018 at the time of analysis, we selected our time interval to provide an optimal setting for comparisons of ophthalmologic and optometric growth profiles in the context of LTP. We created a collation of the CMS PUF datasets from 2015 and 2018 and garnered inclusivity of LA, in addition to KY and OK, into our tri-state cohort.
Among both groups of eye care professionals, we highlight an obvious decline in total Medicare-allowed payments for LTP across the USA from 2015 to 2018, by $13,700,465 or roughly 33%. This joint decline is also evident in a pooled tri-state estimate of KY, LA, and OK from $1,511,594 in 2015 to $1,107,114 in 2018, representing a 26% decrease. Despite this net decrease, Medicare-allowed payments for LTP billed by optometrists increased by 6.6% within the tri-state cohort, from $171,966 to $198,953. Consequently, a decrease in Medicare-allowed payments for ophthalmologists from 88.7% to 82.0% was also observed (p<0.001).
According to the Association of Schools and Colleges of Optometry (ASCO) 2019–2020 Annual Student Data Report, the rate of change per academic year of full-time first-year students in professional Doctor of Optometry programs has incrementally increased by 2.8% and 7.6% since the academic years 1 and 5 years prior.14 While several mechanisms are implicated, a specific rationale is provided by Dr. Janice Law in her 2004 AAO’s “I Am An Advocate” piece, where she indicated a relative absence of ophthalmologic efforts in the congressional arena within the state of Tennessee.15 Consequently, the lack of political endorsement from policymakers acted as provision for an insufficient number of votes to fulfill the minimum threshold to cease effect of the relevant House Bill 555/Senate Bill 220. Shortly before the final vote, Dr. Law et al coordinated a mass effort from residents and medical students showcasing strength in numbers, which ultimately led to the tabling of the bill.15
The American Optometric Association (AOA) justifies continuing optometric laser privileges by stating a consequential, beneficial increase in access to necessary eye care.16 Despite this, the ETT among Medicare beneficiaries who were recipients of optometric surgical care was within 30 minutes of an ophthalmologist’s office for roughly 50% of the beneficiary population in KY, OK, and New Mexico.8 In addition, no significant differences in geographical accessibility to YAG laser capsulotomy in Oklahoma were determined with respect to eye provider type.9 Stein et al, in 2016, specified an objective finding of a 189% increased hazard of Medicare beneficiaries requiring an additional LTP in the same eye if an optometrist, as opposed to an ophthalmologist, had first performed this laser procedure.10 Despite these published findings, our outcomes indicate a near universal increase in number of optometrists performing LTPs, number of LTP services billed by optometrists, and the number of unique Medicare beneficiaries seen by optometrists (all p<0.05). Furthermore, our outcomes suggest that the primary driver for greater Medicare dollars spent is the increase in the number of optometrists performing LTP relative to the increases in services or unique beneficiaries per optometrist (Figure 1). These findings are predicated on the simultaneous observation of universal, proportionate decreases for the same metrics among ophthalmologists.
Our findings are partly rationalized by a comprehensive prevalence study of glaucoma, which highlighted universally decreased rates of open-angle glaucoma – suspect (OAG-s), OAG, and angle-closure glaucoma – suspect (ACG-s) in East South-Central USA (Alabama, Kentucky, Mississippi, and Tennessee).6 In fact, East South-Central was ranked the lowest in terms of diagnoses of OAG-s, OAG, and ACG-s.6 In their study, the USA was divided into nine geographical regions, with West South-Central comprising Arkansas, Louisiana, Oklahoma, and Texas.6 West South-Central showed similar trajectories to East South-Central, with a tie for second lowest unadjusted rate of OAG-s and third lowest unadjusted rate for OAG of the nine geographical regions studied.6 While these findings may support a universal decrease in our studied ophthalmologic metrics, especially in light of recent advances in first-line glaucoma therapy dictating LTP as a reasonable alternative to traditional hypotensive eyedrops, they do not properly rationalize increased optometric metrics. In addition, while comparative prevalence outcomes highlight decreased rates of glaucoma diagnoses in one geographical area versus another, overall rates of glaucoma diagnoses in both ophthalmologic and optometric provider groups across the nation significantly increased from 2002 to 2008, with an expectation of continual increases as our geriatric population ages.6 It is important to mention state-specific legislation is a continually changing landscape; in May 2019, optometrists residing in Oklahoma signed into action Senate Bill 100, which allows the provision of optometric services adjacent to large retail stores such as Walmart. In addition, no restrictions on optometric practices, including surgery, are inherent to this bill, unless mandated by the Oklahoma Association of Optometric Physicians.17
Uniquely, we noticed that only one state within the tri-state cohort, LA, displayed non-significant differences in service volume, beneficiary volume, and provider counts (p=0.909, p=0.354, and p=0.294, respectively). The reason for these discrepancies is unclear. In 1998, state-level optometric associations in OK successfully advocated for unprecedented optometric surgical expansion, including LTP.18 More recently, optometric associations in KY and LA followed in their footsteps with Senate Bill 110 in 2011 and House Bill 1065 in 2014, respectively.19 It is important to note that the start of our study time period pre-dates the recognition of optometric surgical expansion in the state of Louisiana by one year. This may explain the relatively decreased optometric surgical volumes by service count and unique Medicare beneficiaries in Louisiana. However, the substantial decreases in both ophthalmologic and optometric metrics in Louisiana suggest a rationale that is not inherent to optometric surgical expansion. In 2020, Miller et al determined that the youngest patient population treated by optometrists or ophthalmologists in the USA comprised patients treated by optometrists in the state of Louisiana.20 Furthermore, this study characterized significant differences in the racial composition of Medicare beneficiaries treated by both kinds of eye care professionals in all but eight US states, including Louisiana.20 CMS’s Hierarchical Condition Category (HCC) risk score analysis highlights that before and after 2014, no differences in the clinical complexity of patients were observed by optometrists in Louisiana. However, a significant increase in HCC scores for practicing ophthalmologists in Louisiana was observed after 2014, compared to before 2014 (p<0.05).20
The publicly accessible CMS Physician and Other Supplier PUF serves as a notable authority for nationally standardized registries regarding Medicare providers, services, payments, and patient volumes.12 Owing to an ever-growing elderly population in America, glaucoma diagnoses and management in the CMS PUF cohort, irrespective of LTP receipt, are accelerating towards an increasingly representative sample of the national population.13 Relevant limitations include exclusion of Medicare beneficiaries ascribing to private Medicare Advantage plans and providers exercising fewer than 10 LTPs per year.21 No literature exists to date regarding LTP service rates among patients within this subset. Various implications from this investigation can be derived to explain the observed eye care provider disparities; however, it is important to state that the containments of the CMS PUF do not address the underlying parameters that could ultimately lead to the given outcomes. Future study in this regard should unveil the plausible rationale underlying disparities within the optometric field, utilizing quantifiable metrics at a more granular level. Given significant differences in training, further research including comparisons of the safety and efficacy of surgical delivery between the two groups of eye care providers may be insightful. The recent expansion of surgical scope by optometrists in key US states is having a tangible impact on ophthalmologic and optometric practice patterns, with a consequential need for political advocacy by the ophthalmologic community. Ultimately, this study validates and characterizes an ongoing, national trend for optometric expansion within the realm of traditional ophthalmic surgeries.
Conclusion
The recent expansion of practice scope for optometrists in select U.S. states marks a significant evolution in the interplay between ophthalmologic and optometric care. This study highlights a national shift towards greater optometric involvement in traditional ophthalmic procedures. We underscore the importance of congressional advocacy and policymaking in ophthalmology, and highlight the consequential impact on delivery of eye care.
Acknowledgment
The abstract of this paper was presented at the Association for Research in Vision and Ophthalmology (ARVO) 2022 Annual Meeting as a poster presentation with interim findings. The poster’s abstract was published in the ‘2022 Abstract Issue’ in the journal Investigative Ophthalmology and Visual Science. https://iovs.arvojournals.org/article.aspx?articleid=2782282.
Disclosure
Dr. Lama A. Al-Aswad MD, MPH reports ownership in GlobeChek and consultancy for Al Optics, Topcon Medical Systems, Inc., and Aerie Pharmaceuticals. Dr. Siamak Yousefi PhD receives funding from the Bright Focus Foundation and National Eye Institute.
References
1. Garg A, Vickerstaff V, Nathwani N, et al. Primary selective laser trabeculoplasty for open-angle glaucoma and ocular hypertension: clinical outcomes, predictors of success, and safety from the laser in glaucoma and ocular hypertension trial. Ophthalmology. 2019;126(9):1238–1248. doi:10.1016/j.ophtha.2019.04.012
2. Gazzard G, Konstantakopoulou E, Garway-Heath D, et al. Selective laser trabeculoplasty versus eye drops for first-line treatment of ocular hypertension and glaucoma (LiGHT): a multicentre randomised controlled trial [published correction appears in Lancet. 2019 Jul 6;394(10192):e1]. Lancet. 2019;393(10180):1505–1516. doi:10.1016/S0140-6736(18)32213-X
3. Stein JD, Kim DD, Peck WW, Giannetti SM, Hutton DW. Cost-effectiveness of medications compared with laser trabeculoplasty in patients with newly diagnosed open-angle glaucoma. Arch Ophthalmol. 2012;130(4):497–505. doi:10.1001/archophthalmol.2011.2727
4. Cantor LB, Katz LJ, Cheng JW, Chen E, Tong KB, Peabody JW. Economic evaluation of medication, laser trabeculoplasty and filtering surgeries in treating patients with glaucoma in the US. Curr Med Res Opin. 2008;24(10):2905–2918. doi:10.1185/03007990802379996
5. Research and Policy. National conference of state legislatures web site. Available from: https://www.ncsl.org/research/health/optometrist-scope-of-practice.
6. Erie JC, Hodge DO, Mahr MA. Joint management of cataract surgery by ophthalmologists and optometrists. Ophthalmology. 2016;123(3):505–513. doi:10.1016/j.ophtha.2015.10.037
7. Jampel HD, Cassard SD, Friedman DS, et al. Trends over time and regional variations in the rate of laser trabeculoplasty in the Medicare population. JAMA Ophthalmol. 2014;132(6):685–690. doi:10.1001/jamaophthalmol.2014.369
8. Stein JD, Kapoor KG, Tootoo JL, et al. Access to ophthalmologists in states where optometrists have expanded scope of practice. JAMA Ophthalmol. 2018;136(1):39–45. doi:10.1001/jamaophthalmol.2017.5081
9. Mahr MA, Erie JC. Comparing access to laser capsulotomy performed by optometrists and ophthalmologists in Oklahoma by calculated driving distance and time. Ophthalmology. 2017;124(9):1290–1295. doi:10.1016/j.ophtha.2017.03.062
10. Stein JD, Zhao PY, Andrews C, Skuta GL. Comparison of outcomes of laser trabeculoplasty performed by optometrists vs ophthalmologists in Oklahoma. JAMA Ophthalmol. 2016;134(10):1095–1101.
11. Lee AY, Lee CS, Pieters M, Maa AY, Cockerham G, Lynch MG. Differences in tertiary glaucoma care in the veterans affairs health care system. JAMA Ophthalmol. 2018;136(11):1227–1234. doi:10.1001/jamaophthalmol.2018.3463
12. Medical Physician and Other Practitioners. Centers for medicare and Medicaid services web site. Available from: https://data.cms.gov/provider-summary-by-type-of-service/medicare-physician-other-practitioners.
13. Public Comment on the Release of Medicare Physician Data. Centers for Medicare and Medicaid Services web site. Available from: https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Medicare-Provider-Charge-Data/Public-Comment.
14. Annual Student Data Report. Association of Schools and Colleges of Optometry web site. Available from: https://optometriceducation.org/wp-content/uploads/2020/10/ASCO-Student-Data-Report-2019-2020.pdf.
15. I am an advocate. American Academy of Ophthalmology web site. Available from: https://www.aao.org/advocacy/i-am-an-advocate.
16. Scoping out optometry’s next era. Review of Optometry web site. Available from: https://www.reviewofoptometry.com/article/scoping-out-optometrys-next-era.
17. Week in review. Oklahoma Senate web site. Available from: https://oksenate.gov/news/week-monday-march-16-1998-thursday-march-19-1998.
18. Medicare advantage in 2021: enrollment update and key trends. Kaiser Family Foundation web site. Available from: https://www.kff.org/medicare/issue-brief/medicare-advantage-in-2021-enrollment-update-and-key-trends/.
19. Optometric physicians thank governor, legislature for passage of new optometry laws. Oklahoma Welcome web site. Available from: https://okwnews.com/news/lifestyle/health-wellness/optometric-physicians-thank-governor-legislature-for-passage-of-new-optometry-laws.
20. Miller DD, Stewart MW, Gagne JJ, Wagner AL, Lee AY, Surbhi S. Differences in characteristics of Medicare patients treated by ophthalmologists and optometrists. PLoS One. 2020;15(9):e0227783. doi:10.1371/journal.pone.0227783
21. Newman DK, Anwar S, Jordan K. Glaucoma screening by optometrists: positive predictive value of visual field testing. Eye. 1998;12(Pt 6):921–924. doi:10.1038/eye.1998.239
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.