")
Back to Journals » Open Access Surgery » Volume 15
Rate and Risk of Follicular Carcinoma in Patients with a Cytologic Diagnosis of Follicular Neoplasia: Experience from Tertiary Hospital in Ethiopia
Authors Teklewold B , Mekuria B, Chanie W
Received 25 December 2021
Accepted for publication 17 March 2022
Published 25 March 2022 Volume 2022:15 Pages 31—37
DOI https://doi.org/10.2147/OAS.S355808
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Luigi Bonavina
Berhanetsehay Teklewold, Berhanu Mekuria, Wuletaw Chanie
St Paul’s Hospital Millennium Medical College, Department of Surgery, Addis Ababa, Ethiopia
Correspondence: Berhanetsehay Teklewold, St Paul’s Hospital Millennium Medical College, Department of surgery, Addis Ababa, Ethiopia, Email [email protected]
Background: Differentiating benign from malignant thyroid nodules is not possible clinically. The aim of this study was to assess the prevalence and risk of malignancy postoperatively among patients who had a cytologic diagnosis of follicular neoplasia preoperatively.
Methods: All patients who were operated on with histopathologic diagnosis of follicular neoplasia from January 2015 to December 2019, at St Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia were studied retrospectively. Operation theatre log books and individual patient charts were reviewed for the study variables. Both patient and nodular characteristics were analyzed for risk of malignancy and an odds ratio was used to identify the association of factors for follicular carcinoma.
Results: A total of 110 patients’ charts were retrieved for analysis. Two-thirds of patients (78; 70.9%) had benign findings postoperatively and only 32 (29%) patients had malignancy consisting of 21 (19.1%) follicular carcinoma and 11 (10%) papillary carcinoma. The mean age of patients with malignant and benign histopathology is 48.3 (42.9– 53.7) and 41.7 (38.7– 44.7) respectively (p < 0.05). Only tumor size, consistency of nodules, and presence of associated symptoms of malignancy were identified as important predictors upon stepwise logistic regression. The odds of cancer for nodules greater than 4 cm is 4 times higher than the odds for smaller nodules.
Conclusion: In our finding, the prevalence of follicular carcinoma in patients with a cytologic diagnosis of follicular neoplasia is comparable to those reported in other pieces of literature. Clinical characteristics such as size of tumor, consistency of the nodule, and presence of associated symptoms of malignancy are still important predictors of malignancy.
Keywords: rate, risk, follicular carcinoma, follicular neoplasia, Ethiopia
Background
Cytological diagnosis of malignant follicular lesions is difficult because of its failure associated with an identification of either capsular or vascular growth in cytology.1 This failure of demonstrating either vascular or capsular invasion by thyroid cytology resulted in the term follicular neoplasia to reflect the limitations in cytological diagnosis.2 When abundant follicular epithelial cells are seen with macrophages and degenerated cells in the background of scanty colloid, diagnosis of follicular neoplasia is made.2
In 2009 the Bethesda system for reporting thyroid cytopathology was introduced to standardize terms used in thyroid cytology and it classified thyroid fine-needle aspiration cytology (FNAC) into six categories.3 Each category is linked to a certain risk of malignancy and diagnosis of follicular neoplasia or suspicious for follicular neoplasia is among the list of categories. Since FNAC does not differentiate benign from malignant lesions accurately, patients are subjected to surgical removal of nodules that are shown to have follicular neoplasia. Unfortunately, only 15–20% of these nodules postoperatively are proven histologically to have malignant lesions.3–7
According to the recommendations from the American thyroid association, diagnostic hemithyroidectomy is recommended for nodules with follicular neoplasia depending on clinical risk factors.8 Several pieces of literature suggested several clinical characteristics such as male gender, tumour size, and gland pattern that help in predicting the presence of malignancy in those patients with diagnosis follicular neoplasia.9,10
The aim of this study is therefore to evaluate the prevalence of follicular carcinoma and to assess risk factors associated with the risk of malignancy in patients with a preoperative diagnosis of follicular neoplasia.
Methods
A retrospective review of medical records of patients who were operated on for preoperative diagnosis of thyroid follicular neoplasm at St. Paul’s Hospital Millennium Medical college from January 2015 to December 2019 was made. FNAC report of suspicious for follicular neoplasm was also included in the study. A list of patients’ medical records was initially identified from operation theatre logbooks from which medical record numbers were obtained. The charts of the patients were then retrieved from the hospital’s archive. Relevant information including patient (demographic, clinical) and clinical tumour characteristics done by physical examination (size, consistency, and nodularity), imaging and final postoperative histologic findings were collected from charts using a structured checklist. Criteria used for tumour classification used were according to the recent WHO classification2 and the diagnosis of FTC was made when there was evidence of either capsular or vascular invasion in the cytology. Relevant information such as the presence of associated symptoms of malignancy, for example shortness of breath, hoarseness of voice, and difficulty of swallowing was also collected from the records. Only patients with postoperative biopsy results were included in the study to compare the difference in both pre- and post-operative pathological diagnosis. A comparison of clinical and tumour factors was made between patients with benign and malignant histopathologic diagnosis after thyroidectomy to identify relevant risk factors associated with the risk of follicular adenocarcinoma using both univariable and multivariable analysis. The risk for thyroid follicular carcinoma was expressed by odds ratio and a 95% confidence interval was calculated for the odds ratio. P values of less than 0.05 were taken for statistical significance. Univariate association between the presence of follicular carcinoma and clinical factors was analyzed using chi-square test and those variables with statistical significance upon univariable were assessed using stepwise logistic regression to identify independent factors.
Result
A total of 135 patients underwent thyroidectomy for follicular neoplasm in the study period but only the records of 110 patients were retrieved for analysis from medical archives. Of these 110 patients, 98 (89.1%) were female and 12 (10.9%) were male (F: M = 9:1). Among the 110 patients, 53 (48.2%) presented with less than 4 cm size of the mass, and 57 (51.8%) of them presented with greater than 4 cm size. Most of the patients (88; 80%) had associated symptoms of malignancy such as shortness of breath, hoarseness of voice, etc. The majority of patients (102; 90.9%) had firm consistency of the mass and 94 (85.4%) of them had multi-nodular patterns upon clinical examination (Table 1). The majority of patients (90%; 29/32) with malignant histology had multi-nodular character. Seventy-eight percent of patients (25/32) with malignant histology had the size of tumour greater than 4 cm but only 18.7% (6/32) of these were found to have hard consistency during physical examination (Table 1).
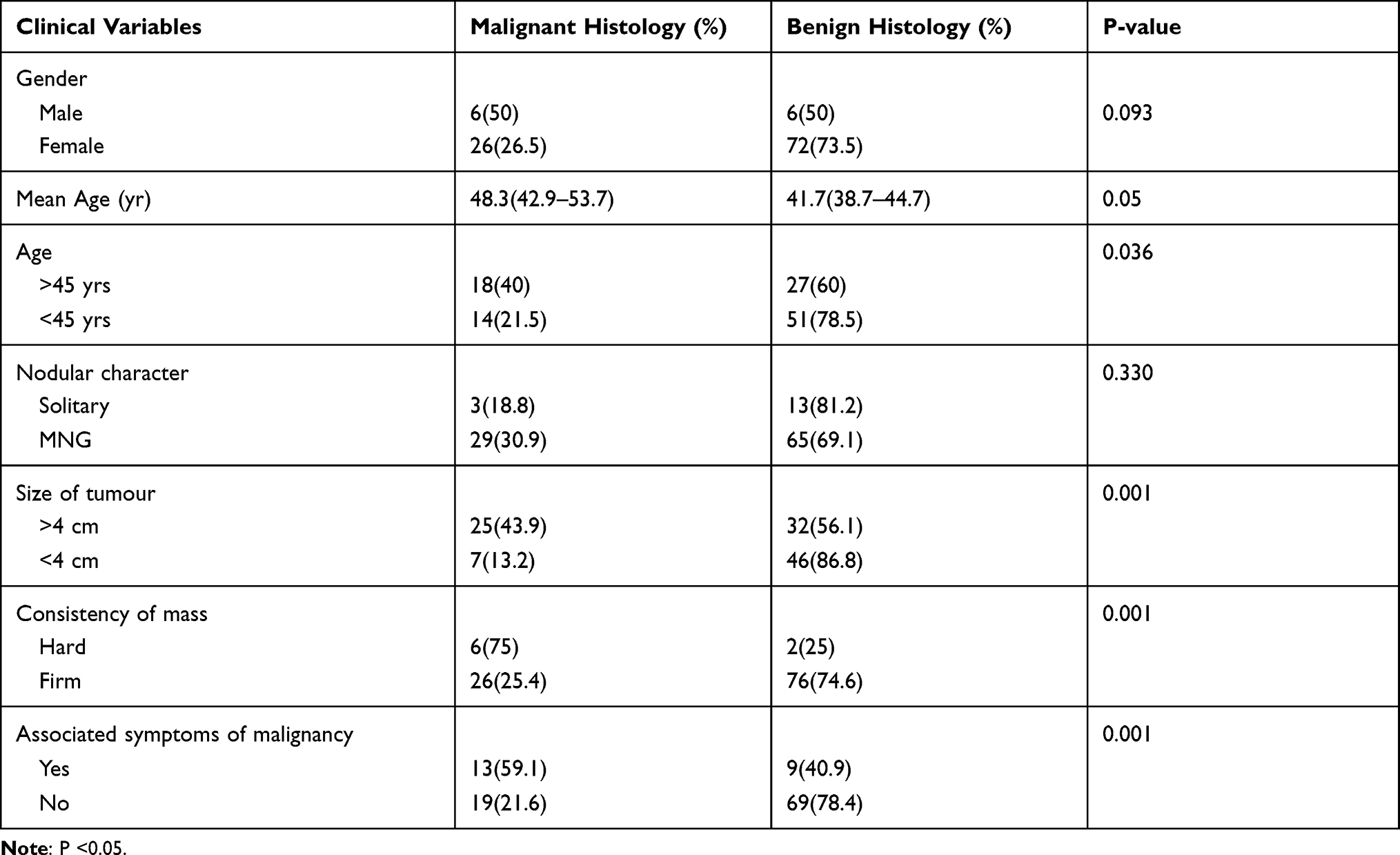 |
Table 1 Socio-Demographic and Clinical Characteristics of Patients Who Were Operated on from January 2015 to December 2019, at St Paul’s Hospital Millennium Medical College (N=110) |
Out of all histopathologies performed postoperatively, only 32 (29%) patients had malignancy, consisting of 21 (19.1%) follicular carcinoma and 11 (10%) papillary carcinoma. Otherwise, 78 (70.9%) had benign pathology with 48 (43.6%) being follicular adenoma (Table 2).
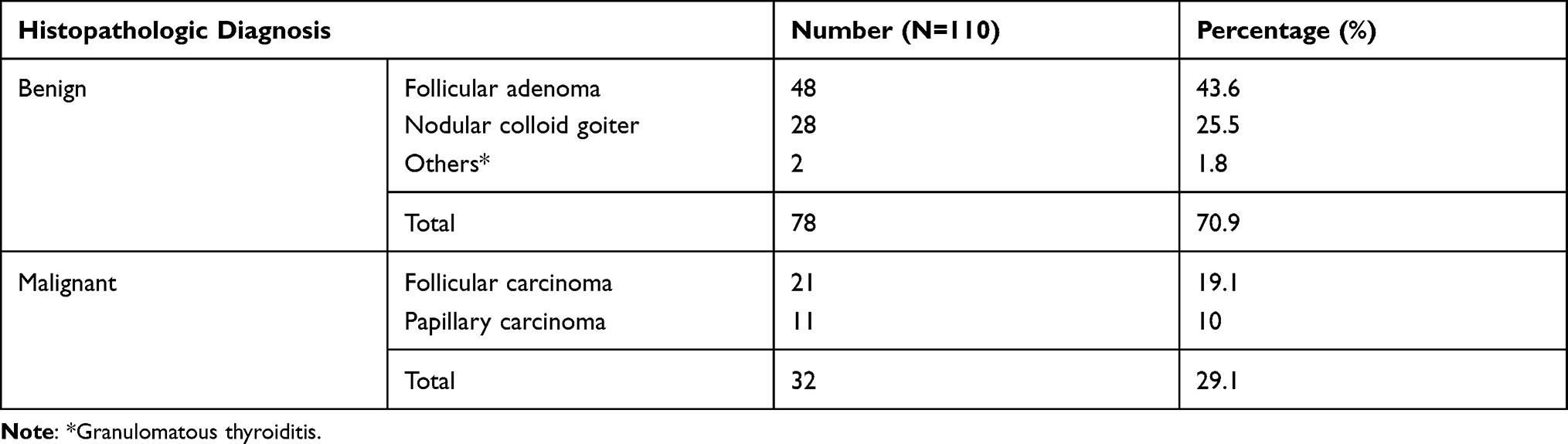 |
Table 2 Post-Operative Histopathologic Findings of the 110 Patients Who Were Operated on from January 2015 to December 2019, at St Paul’s Hospital Millennium Medical College |
A comparison of socio-demographic and clinical characteristics was made between those with malignant and benign histopathology (Table 1). The mean age of patients with malignant and benign histopathology is 48.3 (42.9–53.7) and 41.7 (38.7–44.7), respectively (p <0.05). A malignant diagnosis of follicular carcinoma was significantly more likely to be found in patients older than 45 years (40% vs 21.5%, p <0.036), and in those with clinical tumour size greater than 4 cm than those with smaller nodules (43.9% vs 13%, p <0.001). Furthermore, nodules with hard consistency were more likely to be malignant than those with firm consistency (75% vs 25%, p <0.001), and also patients with associated symptoms of malignancy were significantly more likely to have malignancy than those without these symptoms (59.1% vs 21.6%, p <0.001) (Table 1).
Gender and nodular characteristics of the mass did not significantly differ between patients found to have malignant lesions and those with benign histopathology (Table 1).
Data were analyzed both by univariable and multivariable analysis to determine important predictors associated with the presence of follicular carcinoma and the results are described in Table 3. Tumour size, consistency of nodules, and presence of associated symptoms of malignancy were identified as important predictors upon stepwise logistic regression. The odds of cancer for nodules greater than 4 cm is 4 times higher than the odds for smaller nodules. Patients with hard consistency of mass are 6 times at higher risk of having malignancy than those with firm consistency and patients with associated symptoms of malignancy such as shortness of breath are 4.8 times at higher risk of malignancy than those without symptoms.
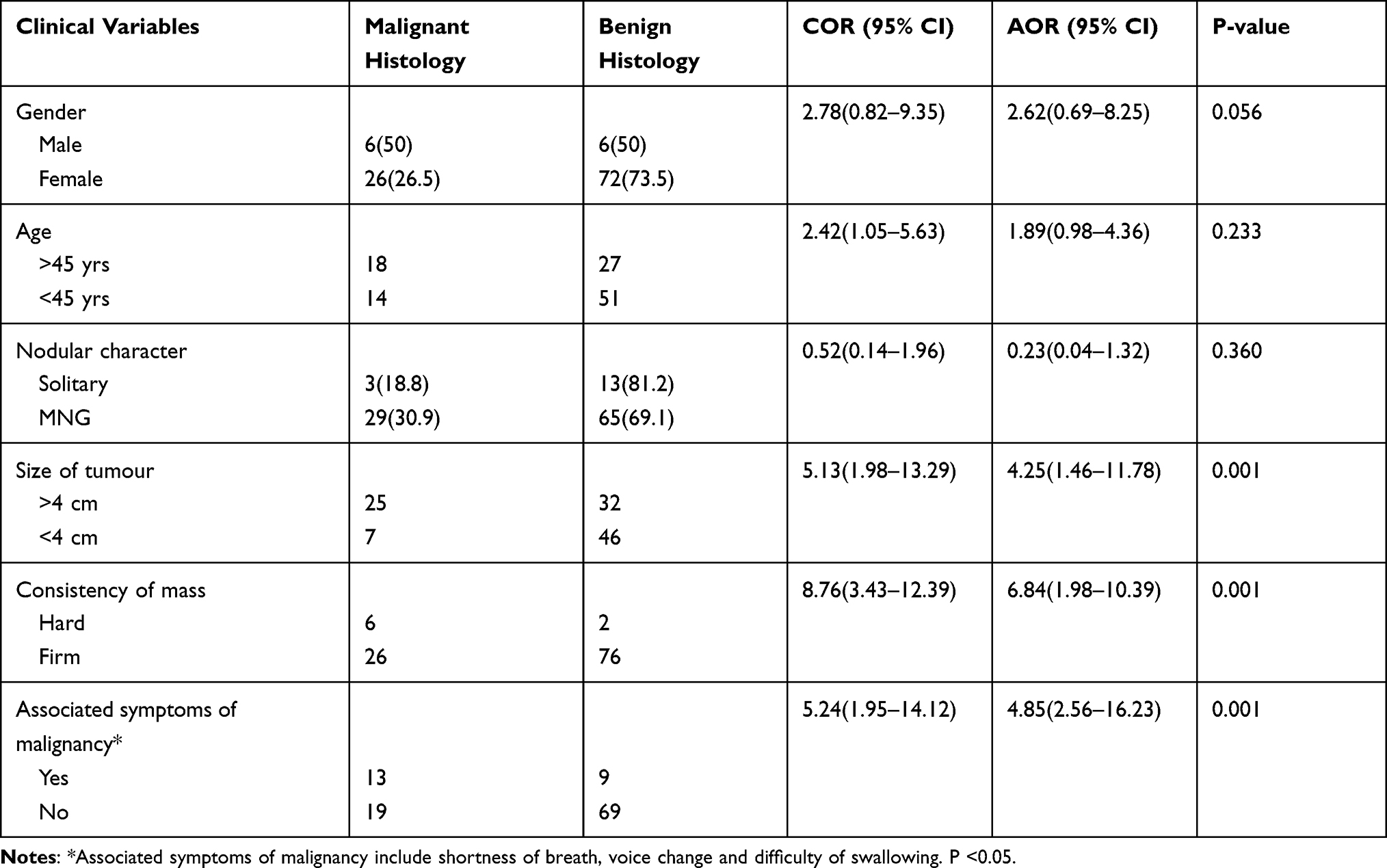 |
Table 3 Univariable and Multivariable Analysis of Clinical Factors Associated with Risk of Malignancy of Patients Who Were Operated on from January 2015 to December 2019, at St Paul’s Hospital Millennium Medical College |
Discussion
Diagnosis of carcinoma in the follicular lesion is often made following examination of biopsy sections after surgical procedure. This is because FNAC is unable to distinguish between adenoma and carcinoma though it is among the most reliable and cost-effective methods in diagnosing thyroid nodules. Patients are therefore subjected to diagnostic surgery to distinguish between the benign and malignant nodules by biopsy. Though diagnostic surgery is commonly performed there are reports that suggest centers use several clinical criteria to clinically follow patients with benign findings rather than subjecting them for surgery.11
We retrospectively studied 110 patients who had thyroid nodules which were read as follicular neoplasia by FNAC and evaluated postoperative biopsy results.
The reported rate of malignancy according to some literature in thyroid nodules with FNAC diagnosis of follicular neoplasia after surgery is between 20–30%.4,5,12,13
This study has also revealed a similar rate of malignancy of 29.1% that is consistent with the above studies. This is relatively higher when compared with other studies which reported from 16–18%.14,15 The reason for the higher rate can be attributed to the center being one of the tertiary care centers in the country that many referred patients visit.
Of the malignant lesions identified in our study, the majority (65%; 21/32) is follicular carcinoma and 35% (11/32) papillary. This is in line with reports by Chen et al. and Kim et al.12,16 The reason for the higher frequency of follicular carcinoma can be attributed partly to patient selection which was concentrated on lesions that were follicular from the outset but the fact that Ethiopia is among the countries that are iodine-deficient17 and since historically follicular carcinoma has been linked with regions of the world with iodine deficiency18 this might explain the higher rate of prevalence in our study. FTC is also said to arise from longstanding goiters and the majority of thyroid nodules in Ethiopia are multinodal goiter (MNG) according to some works of literature from Ethiopia.19,20
Several studies have tried to combine and integrate different combinations of factors that would help in predicting the risk of malignancy in patients with thyroid nodules with the diagnosis of follicular neoplasia.6,9,15,21–24 These authors have concluded that clinical features such as old age, male gender, tumour size greater than 4 cm, nodular characteristics, and consistency of tumour would be of help to define a sub-group of patients with high risk for malignancy.
The calculated risk of malignancy for women with greater than 4 cm solitary nodules was 45% according to Tuttle but our study revealed no association of gender with the risk of malignancy on univariable analysis.9
Our study has shown that older age greater than 45 years, clinical tumour size greater than 4 cm, hard consistency of tumour are all associated with significantly increased risk of malignancy. These findings correspond with similar reports from several pieces of research that noted an association of older age greater than 50 years6 and tumour size greater than 4 cm with an increased risk for malignancy.10
Although there are reports of association of risk of malignancy with a nodular character that noted a higher risk of malignancy with solitary nodule this was not seen with our study which showed no significant association of risk of malignancy with the nodular character of goiters in univariable analysis. The reason for this may be the use of only clinical examination in characterizing nodularity of thyroid which usually misses the presence of multiple nodules when compared with high-resolution ultrasound25 which in our case was not used for examination.
Univariable analysis in our study demonstrated that associated symptoms of malignancy such as shortness of breath, dysphagia, and change in voice are significantly associated with risk of malignancy (p <0.001) and there is only a single report by Tuttle et al. that showed no significant association of clinically worrisome features such as dysphagia and hoarseness of voice with the risk of malignancy.
Multivariable analysis using standard stepwise logistic regression in our study has shown that clinical size of tumour greater than 4 cm, hard consistency of thyroid nodule, and associated symptoms of malignancy are significant independent risk factors predictive of malignancy in our model. There are several pieces of research that tried to explore the interaction of multiple clinical factors that estimate the probability of malignancy for patients but there are no similar combinations of factors so far. Schlinkert et al. reported advanced age, size of the tumour, and solitary nodularity as independent risk factors for malignancy10 but Tuttle et al. demonstrated male gender, size of tumour greater than 4 cm, and solitary character were independently associated with risk of malignancy.9 Part of the explanation for such dissimilar conclusions would be the need for many years to accumulate the experience to incorporate a variety of clinical features into an estimation of risk of malignancy.9
The limitation of this study is that the data are from a single institution and a large number of patients were excluded because of the incompleteness of data. Since the use of ultrasound in predicting the risk of malignancy is currently being ascertained, failure of including ultrasound features in examining the risk of malignancy might have masked some of the features such as nodular characters of the tumors that are best seen by ultrasound.
We, therefore, conclude that simple clinical features such as the size of the tumor, hard consistency of the nodule, and symptoms associated with malignancy such as dysphagia and hoarseness of voice will help in identifying patients with an increased risk of malignancy when pre-surgical FNAC is used with follicular neoplasia. Integration of these simple features with cytologic findings might help physicians to stratify patients to high and low risk and also help in better decision making. Therefore we recommend careful clinical evaluation of patients to identify the risk of malignancy when pre-surgical FNAC shows follicular neoplasia.
Declarations
All methods were carried out in accordance with relevant guidelines and regulations. Consent to publish is not applicable as no identity revealing information is provided in the manuscript. The study was conducted in accordance with the Declaration of Helsinki.
Data Sharing Statement
The datasets used in this study are available upon request from corresponding author.
Ethical Approval and Consent to Participate
Ethical clearance was obtained from institutional review board (IRB) of St Paul hospital millennium medical college. As this was a purely retrospective review on medical records, informed consent was waived by St Paul hospital millennium medical college IRB and therefore was not taken.
Acknowledgment
The authors do not wish to acknowledge anybody.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation or in all these areas; took part in drafting, revising critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspect of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rosai J, Caracangiu ML, DeLellis RA. Atlas of Tumor Pathology: Tumors of the Thyroid Gland, 3rd Series. Washington DC: Armed Forces Institute of Pathology; 1992:31–50.
2. Klöppel G, Couvelard A, Hruban RH, et al. WHO Classification of Tumours of Endocrine Organs. Lyon, France: World Health Organization; 2017.
3. Wu HH, Swadley MJ. The Bethesda system for reporting thyroid cytopathology: into the clinic. Pathol Lab Med Int. 2015;7:47. doi:10.2147/PLMI.S59827
4. Gardner HAR, Ducatman BS, Wang HH. Predictive value of fine-needle aspiration of the thyroid in the classification of follicular lesions. Cancer. 1993;71(8):2598–2603. doi:10.1002/1097-0142(19930415)71:8<2598::AID-CNCR2820710826>3.0.CO;2-F
5. Miller JM, Kini SR, Hamburger JI. The diagnosis of malignant follicular neoplasms of the thyroid by needle biopsy. Cancer. 1985;55(12):2812–2817. doi:10.1002/1097-0142(19850615)55:12<2812::AID-CNCR2820551216>3.0.CO;2-N
6. Tyler DS, Winchester DJ, Caraway NP, Hickey RC, Evans DB. Indeterminate fine-needle aspiration biopsy of the thyroid allows identification of subgroups at high risk for invasive carcinoma. Surgery. 1994;116(6):1054–1060.
7. Rojeski MT, Gharib H. Nodular thyroid disease: evaluation and management. N Engl J Med. 1985;313(7):428–436. doi:10.1056/NEJM198508153130707
8. Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26(1):1–33. doi:10.1089/thy.2015.0020
9. Tuttle RM, LEMAR H, Burch HB. Clinical features associated with an increased risk of thyroid malignancy in patients with follicular neoplasia by fine-needle aspiration. Thyroid. 1998;8(5):377–383. doi:10.1089/thy.1998.8.377
10. Schlinkert RT, Van Heerden JA, Goellner JR, et al. Factors that predict malignant thyroid lesions when fine-needle aspiration is “suspicious for follicular neoplasm”. In Mayo Clinic Proc. 1997;72(10):
11. Kihara M, Hirokawa M, Ito Y, et al. Final pathology findings after immediate or delayed surgery in patients with cytologically benign or follicular thyroid nodules. World J Surg. 2011;35(3):558–562. doi:10.1007/s00268-010-0907-4
12. Chen H, Nicol TL, Udelsman R. Follicular lesions of the thyroid. Does frozen section evaluation alter operative management? Ann Surg. 1995;222(1):101. doi:10.1097/00000658-199507000-00016
13. McHenry CR, Thomas SR, Slusarczyk SJ, Khiyami A. Follicular or Hu ̈rthle cell neoplasm of the thyroid: can clinical factors be used to predict carcinoma and determine extent of thyroidectomy? Surgery. 1999;126(4):798–804. doi:10.1016/S0039-6060(99)70138-8
14. Goellner JR, Gharib H, Grant CS, Johnson DA. Fine needle aspiration cytology of the thyroid, 1980 to 1986. Acta Cytol. 1987;31(5):587–590.
15. Raber W, Kaserer K, Niederle B, Vierhapper H. Risk factors for malignancy of thyroid nodules initially identified as follicular neoplasia by fine-needle aspiration: results of a prospective study of one hundred twenty patients. Thyroid. 2000;10(8):709–712. doi:10.1089/10507250050137806
16. Kim ES, Nam-Goong IS, Gong G, Hong SJ, Kim WB, Shong YK. Postoperative findings and risk for malignancy in thyroid nodules with cytological diagnosis of the so-called “follicular neoplasm”. Korean J Intern Med. 2003;18(2):94. doi:10.3904/kjim.2003.18.2.94
17. Wolde-Gebriel Z, Demeke T, Westa CE, Van Der Haar F. Goitre in Ethiopia. Br J Nutr. 1993;69(1):257–268. doi:10.1079/BJN19930027
18. Asibey-Berko E Prevalence and severity of iodine deficiency disorders in Ghana.
19. Suga Y, Abebe E. Patterns of surgically treated thyroid disease: a two years review at St. Paul Hospital Millennium Medical College, Addis Ababa, Ethiopia. Ethiop J Health Sci. 2020;30(1):1. doi:10.4314/ejhs.v30i1.1
20. Bekele A, Osman M. Goitre in a teaching hospital in North Western Ethiopia. East Cent Afr J Surg. 2006;11(2):21–27.
21. Sahin M, Gursoy A, Tutuncu NB, Guvener DN. Prevalence and prediction of malignancy in cytologically indeterminate thyroid nodules. Clin Endocrinol. 2006;65(4):514–518. doi:10.1111/j.1365-2265.2006.02625.x
22. Miller B, Burkey S, Lindberg G, Snyder III WH, Nwariaku FE. Prevalence of malignancy within cytologically indeterminate thyroid nodules. Am J Surg. 2004;188(5):459–462. doi:10.1016/j.amjsurg.2004.07.006
23. Goldstein RE, Netterville JL, Burkey B, Johnson JE. Implications of follicular neoplasms, atypia, and lesions suspicious for malignancy diagnosed by fine-needle aspiration of thyroid nodules. Ann Surg. 2002;235(5):656. doi:10.1097/00000658-200205000-00007
24. Gharib H, Goellner JR, Zinsmeister AR, Grant CS, Van Heerden JA. Fine-needle aspiration biopsy of the thyroid: the problem of suspicious cytologic findings. Ann Intern Med. 1984;101(1):25–28. doi:10.7326/0003-4819-101-1-25
25. Wiest PW, Hartshorne MF, Inskip PD, et al. Thyroid palpation versus high‐resolution thyroid ultrasonography in the detection of nodules. J Med Ultrasound. 1998;17(8):487–496. doi:10.7863/jum.1998.17.8.487
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.