")
Back to Journals » International Medical Case Reports Journal » Volume 16
Rare Recurrence of Sydenham Chorea in an Adult: A Case Report
Received 3 February 2023
Accepted for publication 4 May 2023
Published 9 May 2023 Volume 2023:16 Pages 265—268
DOI https://doi.org/10.2147/IMCRJ.S405371
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Gashaw Solela, Medina Fedlu
Department of Internal Medicine, Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia
Correspondence: Gashaw Solela, Tel +251 921562995, Email [email protected]
Background: Sydenham chorea is thought to be an autoimmune condition that usually develops following a group A beta-hemolytic streptococcal infection.The onset of Sydenham chorea in adults is rare and most of the adult cases usually are secondary to recurrence following childhood illness. Risk factors for chorea recurrence include irregular antibiotic prophylactic use, failure to reach remission within 6 months, and symptom persistence for longer than a year.
Case Presentation: A 27-year-old young adult Ethiopian female patient with chronic rheumatic valvular heart disease for the last 8 years experienced repetitive uncontrollable movements of her extremities and torso for three years prior to her current visit. Physical examination was significant for holosystolic murmur at the apical area radiating to the left axilla and choreiform movements apparent on all limbs and trunk. Investigations were significant for mildly raised ESR, echocardiography findings of thickened mitral valve leaflets and severe mitral regurgitation. She was successfully treated with valproic acid and the frequency of penicillin injection was made every 3 weeks with no recurrence for the first 3 months follow-up period.
Conclusion: We believe that this is the first case report of adult onset recurrent Sydenham chorea (SC) from a resource-limited setting. Though Sydenham chorea and its recurrence is rare in adults, it should be considered in adults after ruling out other competing differential diagnoses. Because of the lack of evidence on treatment of such rare cases, individualized mode of therapy is advised. Valproic acid is preferred for symptomatic treatment and more frequent benzathine penicillin G injections, for example every three weeks, may help in the prevention of recurrence of Sydenham chorea.
Keywords: Sydenham chorea, rheumatic fever, recurrence
Background
Sydenham chorea (SC) is thought to be an autoimmune condition that usually develops following a group A beta-hemolytic streptococcal infection. The immune system antibodies that are produced in response to the streptococcal bacterial infection, presumably have a cross-reaction with the basal ganglia cells, which play crucial roles in regulating motor activity. The onset of Sydenham chorea in adults is rare and most of the adult cases usually are secondary to recurrence following childhood illness.1 Females are twice more affected than males.2 SC ranges in severity from mild to severe and has an impact on a variety of daily tasks, including writing, walking, eating, and getting dressed.3
The reason for recurrence of Sydenham chorea is not yet clearly known. Recurrent chorea and rheumatic fever do not share the same underlying etiology and recurrent chorea is not always brought on by rheumatic fever. Following a single attack of Sydenham chorea, the basal ganglia may sustain persistent subclinical injury or a basic abnormality leading to recurrence.4 Risk factors for chorea recurrence include irregular antibiotic prophylactic use, failure to reach remission within 6 months, and symptom persistence for longer than a year.5
Case Presentation
A 27-year-old young adult Ethiopian female patient who is known to have chronic rheumatic valvular heart disease for the past 8 years started to experience repetitive uncontrollable movements of her extremities and trunk since 3 years ago and which were occurring once to three times per month. The abnormal body movements usually lasted up to a week duration and got worse while she tried to sit or walk and improved with rest. She was consistently taking intramuscular injection of benzathine penicillin G 1.2 million units every month for the past 8 years. She did not have previous history of behavioral and emotional lability. She does not remember childhood history of rheumatic fever or movement disorder. She did not use oral or injectable hormonal agents. There was no family history of rheumatic fever, social stress, psychiatric disease, or tic disorders. Upon physical examination, temperature was 36.7°C, heartbeat was 90 beats per minute, and blood pressure was 100/70 mmHg. There was holosystolic murmur at the apical area radiating to the left axilla. Choreiform movements were apparent on all limbs and trunk.
Laboratory investigations revealed moderate leukopenia (but with a normal repeat complete blood count after 3 days), normal liver enzymes, normal renal function tests, erythrocyte sedimentation rate of 37 mm/hour, negative qualitative C-reactive protein, weakly positive anti-streptolysin O antibody, negative qualitative antinuclear antibody, negative urine human chorionic gonadotrophin and normal level of thyroid stimulating hormone. Magnetic resonance imaging of the brain showed left parietal periventricular tiny white matter non-specific lesion. Rheumatic heart involvement was confirmed by echocardiography which showed thickening of mitral valve leaflets with severe mitral regurgitation (Figure 1).
 |
Figure 1 Transthoracic echocardiography from a patient with rheumatic valvular heart disease and recurrent Sydenham chorea in parasternal long axis view. Mitral valve leaflets are thickened (arrows). Abbreviations: LA, left atrium; LV, left ventricle; Ao, aorta. |
The present case was diagnosed as recurrent Sydenham chorea based on clinical evidence and she was prescribed valproic acid 500 mg PO/day for 2 weeks and benzathine penicillin G injection was made every 3 weeks. She was re-evaluated after 2 weeks and she had significant improvement with good control of motor activity and reduced involuntary movements of her extremities and trunk. She was then followed every 3 weeks for the subsequent 3 months and she did not have any abnormal body movement. She was finally referred to an advanced cardiac center for possible mitral valve replacement.
Discussion and Conclusions
Patient characteristics, associated clinical features and treatment outcomes of Sydenham chorea in the present case report are quite different from those of the available case reports (Table 1). In contrast to a prior case series of children with SC, where the time between the initial episode and the recurrence ranged from 3 months to 10 years,4 the recurrence in the present case was once to three times per month. Adult patients may experience neuropsychiatric consequences of Sydenham chorea such as chorea gravidarum, obsessive-compulsive disorder, and schizophrenia.5 In contrast to a case report of an adult male patient who had psychiatric manifestations including emotional incontinence and abnormal behavior accompanying chorea,6 there was no associated psychiatric symptom in this case report.
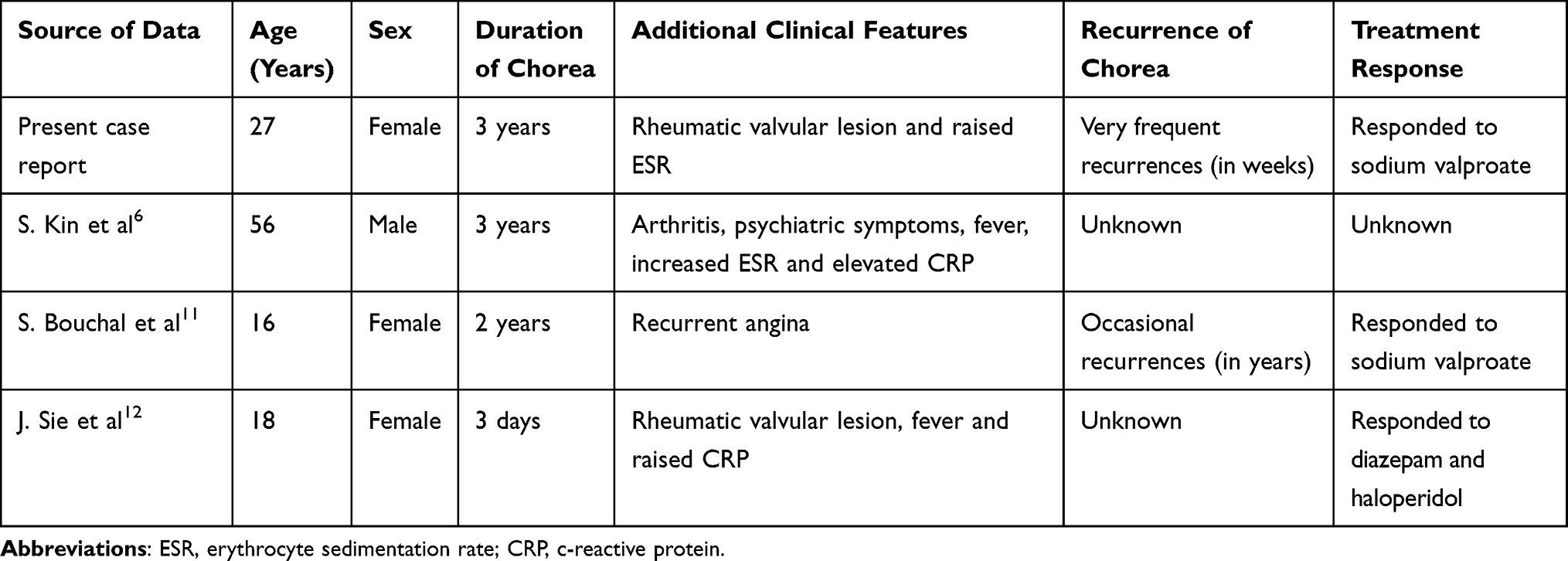 |
Table 1 Case Reports of Sydenham Chorea in Adolescents and Adults |
The risk of recurrence of SC in the present case may be explained by the absence of remission in the first 6 months of onset of SC and its extension beyond a year. This is supported by findings of a study done by Gurkas et al, which found that failure to achieve remission within 6 months and prolongation of symptoms for more than 1 year were important risk factors for recurrence of SC.7
Our patient had recurrence of SC despite taking monthly benzathine penicillin G, unlike the findings of a study done in children with SC, which showed a significant reduction of recurrence for those who were given prophylactic long-acting penicillin G compared with those who were not given this.8
In the previous case reports, where most patients were children, those developing recurrent or non-recurrent SC were oftentimes treated effectively with valproic acid and neuroleptic agents.4,9 Despite the paucity of data on how to treat recurrent or non-recurrent SC in adults, symptomatic treatment of the present case with valproic acid was successful. There was no recurrence while she was followed for three months, which might be because of the more frequent administration of benzathine penicillin G injection.
A study done by Dean et al reviewed available case reports and case series and finally recommended the initial use of valproic acid or carbamazepine instead of neuroleptics for symptomatic treatment of Sydenham chorea. Neuroleptics are not preferred because of their adverse effects and lack of evidence to show their superior efficacy.10 A similar response to sodium valproate was seen in a case report of a 16-year-old female patient with recurrent Sydenham chorea after failure of haloperidol.11 Another case report has shown that an 18-year-old female patient with Sydenham chorea responded to diazepam and haloperidol.12
In conclusion, we believe that this is the first case report of adult onset recurrent Sydenham chorea from a resource-limited setting with frequent episodes of choreiform movements in the background of chronic rheumatic valvular disease. Though SC and its recurrence is a rare condition in adults, it should be considered in the appropriate clinical context after ruling out other competing differential diagnoses. Because of the lack of evidence on treatment of such rare cases, individualized mode of therapy is advised. For symptomatic treatment, we favor valproic acid instead of haloperidol to make sure patients are treated with an effective and well-tolerated drug. In settings with a burden of group A streptococcal infection, we advise more frequent benzathine penicillin G injections, which might help to curb the recurrence of Sydenham chorea.
Limitations of the Case Report
The first limitation is the short follow-up period of the patient, which is not adequate to trace for any recurrence of Sydenham chorea. The second limitation is the absence of adequate similar case reports to compare and contrast with the current case report.
Ethical Clearance
Ethical clearance including publication of this patient’s case details was obtained from Yekatit 12 Hospital Medical College Review Board.
Consent for Publication
The patient gave a written informed consent for the publication of her case details including the history, physical findings, laboratory reports, and the echocardiography image.
Acknowledgment
We would like to thank all the staff of Yekatit 12 Hospital Medical College and Wudassie Diagnostic Center for their unreserved cooperation in the investigation and management of the patient. We would also like to thank the patient for the written consent she gave for publication of her case details.
Disclosure
We don’t have conflicts of interest in this work.
References
1. Beier K, Pratt DP. Sydenham Chorea. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430838/.
2. Zomorrodi A, Wald ER. Sydenham’s chorea in western Pennsylvania. Pediatrics. 2006;117:e675. doi:10.1542/peds.2005-1573
3. Walker KG, Wilmshurst JM. An update on the treatment of Sydenham’s chorea: the evidence for established and evolving interventions. Ther Adv Neurol Disord. 2010;3(5):301–309. doi:10.1177/1756285610382063
4. Korn-Lubetzki I, Brand A, Steiner I. Recurrence of Sydenham Chorea: implications for pathogenesis. Arch Neurol. 2004;61(8):1261–1264. doi:10.1001/archneur.61.8.1261
5. Moore DP. Neuropsychiatric aspects of Sydenham’s chorea: a comprehensive review. J Clin Psychiatry. 1996;57(9):407–414. PMID: 9746449.
6. Kin S, Taniwaki T, Shigeto H, Nomura T, Ohyagi Y. 精神症状を伴う成人発症型シデナム舞踏病の1例 [A case of adult-onset Sydenham chorea accompanied with psychiatric symptoms]. No to Shinkei. 2006;58(2):155–159. Japanese. Japanese.
7. Gurkas E, Karalok ZS, Taskin BD, et al. Predictors of recurrence in Sydenham’s chorea: clinical observation from a single center. Brain Dev. 2016;38(9):827–834. doi:10.1016/j.braindev.2016.04.010
8. Gebremariam A. Sydenham’s chorea: risk factors and the role of prophylactic benzathine penicillin G in preventing recurrence. Ann Trop Paediatr. 1999;19(2):161–165. PMID: 10690256. doi:10.1080/02724939992482
9. Tata G. Recurrence of Sydenham’s Chorea. Turk J Neurol. 2018;24:188–189. doi:10.4274/tnd.24482
10. Dean SL, Singer HS. Treatment of Sydenham’s Chorea: a review of the current evidence. Tremor Other Hyperkinet Mov. 2017;7:456. PMID: 28589057; PMCID: PMC5459984. doi:10.7916/D8W95GJ2
11. Bouchal S, Ouali O, Belahsen MF. Réponse spectaculaire au valproate de sodium d’une chorée de Sydenham récurrente [Exceptionally good response to sodium valproate in patients with recurrent Sydenham’s chorea]. Pan Afr Med J. 2017;27:212. French. doi:10.11604/pamj.2017.27.212.11383
12. Sie J, Sumada K. Case report: chorea Sydenham in young adult females as symptom of rheumatic fever. Callosum Neurol J. 2020;3(1):30–36. doi:10.29342/cnj.v3i1.84
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.