Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
Rare Long-Term Transformation from Solitary Hepatocellular Carcinoma to Synchronous Double Primary Hepatocellular Carcinoma and Intrahepatic Cholangiocarcinoma: A Case Report and Literature Review
Authors Qiao L, Wei P, Lo C, Luo Y ![]() , Peng Y, Kang Z, Gao J, Zhu J, Li Z
, Peng Y, Kang Z, Gao J, Zhu J, Li Z
Received 14 February 2026
Accepted for publication 21 May 2026
Published 28 May 2026 Volume 2026:13 598850
DOI https://doi.org/10.2147/JHC.S598850
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr David Gerber
Liyi Qiao,1– 4,* Pengcheng Wei,1– 4,* Chen Lo,1– 4 Yongjing Luo,1– 4 Yun Peng,1– 4 Zhuoliang Kang,1– 4 Jie Gao,1– 4 Jiye Zhu,1– 4 Zhao Li1– 4
1Department of Hepatobiliary Surgery, Peking University People’s Hospital, Beijing, People’s Republic of China; 2Beijing Key Surgical Basic Research Laboratory of Liver Cirrhosis and Liver Cancer, Peking University People’s Hospital, Beijing, People’s Republic of China; 3Peking University Center of Liver Cancer Diagnosis and Treatment, Peking University People’s Hospital, Beijing, People’s Republic of China; 4Peking University Institute of Organ Transplantation, Peking University People’s Hospital, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhao Li, Department of Hepatobiliary Surgery, Peking University People’s Hospital, Beijing, 100044, People’s Republic of China, Email [email protected]
Abstract: Synchronous double primary hepatocellular carcinoma and intrahepatic cholangiocarcinoma (sdpHCC-ICC) is rare, particularly when evolving metachronously from solitary HCC. This study reports a unique case of such transformation over two decades and reviews the relevant literature. A 55-year-old male with chronic hepatitis B underwent curative resection for HCC in 2005. Following multiple recurrences treated with local therapies over 19 years, subsequent resection in 2024 revealed two distinct malignancies: recurrent HCC and a spatially separate intrahepatic cholangiocarcinoma (ICC), confirmed by immunohistochemistry. We additionally analyzed 31 reported sdpHCC-ICC cases to summarize their clinicopathological characteristics and outcomes. The patient eventually developed systemic metastases despite adjuvant therapy. Our review highlights the marked biological heterogeneity and diagnostic challenges associated with sdpHCC-ICC. This case suggests that prolonged tumor evolution in chronically injured livers may be associated with biological heterogeneity and phenotypic divergence. Our findings support the potential value of long-term surveillance and repeated pathological reassessment in selected long-term HCC survivors with atypical recurrence patterns.
Keywords: liver neoplasms, tumor heterogeneity, phenotypic plasticity, hepatic progenitor cells, immunohistochemistry, clinical surveillance
Introduction
Hepatocellular carcinoma (HCC) is the most common primary liver malignancy, accounting for approximately 75%–85% of primary liver cancers worldwide.1–3 Intrahepatic cholangiocarcinoma (ICC) is the second most common subtype, representing approximately 10%–15% of primary liver tumors.4,5 Although HCC and ICC typically occur as distinct entities, they can rarely develop simultaneously within the same liver but in separate foci—a phenomenon known as synchronous double primary hepatocellular carcinoma and intrahepatic cholangiocarcinoma (sdpHCC-ICC).
Unlike combined hepatocellular-cholangiocarcinoma (cHCC-CCA), in which hepatocytic and cholangiocytic differentiation coexist within the same tumor nodule, sdpHCC-ICC refers to two spatially distinct primary tumors arising separately within the liver. This distinction is clinically important because the biological behavior, pathological interpretation, and therapeutic implications may differ substantially. Synchronous double primary HCC-ICC is extremely rare, with an estimated incidence ranging from 0.4% to 14.2%, depending on diagnostic criteria and the population studied.6,7 Most reported cases are diagnosed synchronously at initial presentation, with both HCC and ICC components coexisting in separate nodules.8,9 However, metachronous development—where a patient initially diagnosed with solitary HCC subsequently develops sdpHCC-ICC after curative treatment—is exceedingly rare and sparsely reported in the literature. Its pathogenesis remains poorly understood but may involve tumor heterogeneity, hepatic progenitor cell differentiation, or clonal evolution under therapeutic pressure.
Herein, we report a rare case of a patient initially diagnosed with solitary HCC who developed sdpHCC-ICC several years after curative resection. This case highlights the potential dynamic pathological evolution of liver tumors over long-term follow-up with multiple recurrences and includes a comprehensive literature review discussing its clinicopathological features, potential mechanisms, and clinical management implications.
Case Presentation
Initial Diagnosis and Treatment (2005)
A 55-year-old man with a 20-year history of chronic hepatitis B infection, hypertension, and long-term smoking was first evaluated in August 2005 after a routine health examination revealed an incidental hepatic lesion. Apart from these chronic conditions, his past medical history was otherwise unremarkable. Contrast-enhanced CT demonstrated a 3.0 cm mass in segment 3 (S3) of the left lateral lobe adjacent to the hepatic fissure. The lesion slightly protruded beyond the liver surface and showed arterial phase hyperenhancement with subtle portal venous washout. The lesion had ill-defined margins blending with the surrounding parenchyma, raising suspicion for hepatocellular carcinoma. Serum alpha-fetoprotein (AFP) and carbohydrate antigen 19–9 (CA19-9) levels were within normal limits.
Exploratory laparotomy was performed in September 2005. Intraoperatively, a firm 4.0×4.0 cm mass was identified in S3, partially adherent to the hepatic capsule. Anatomical resection with an approximately 1 cm surgical margin was performed. Histopathological examination confirmed a well-differentiated hepatocellular carcinoma measuring 2.0 cm, arising in a cirrhotic liver with mild steatosis. The postoperative course was uneventful, and the patient was discharged on postoperative day 10. Postoperatively, adjuvant hepatic arterial infusion chemotherapy (HAIC) with epirubicin, cisplatin, and mitomycin was administered. Follow-up imaging in November 2005 revealed no residual or recurrent disease, and adjuvant treatment was continued. During the subsequent eight years of follow-up, no tumor recurrence or metastasis was detected, while hepatitis B–related cirrhosis remained stable under antiviral therapy.
Tumor Recurrences and Local Therapies (2013–2020)
In July 2013, surveillance imaging detected a new 0.9×0.8 cm nodule in the right posterior inferior segment (S6). Magnetic resonance imaging suggested recurrent hepatocellular carcinoma. Serum AFP was mildly elevated, whereas CA19-9 remained within normal limits. The lesion was treated with ultrasound-guided radiofrequency ablation, followed one month later by transarterial chemoembolization (TACE). The patient remained recurrence-free during the subsequent seven years of follow-up.
In September 2020, tumor recurrence was identified in segment S6, measuring 1.9×1.4 cm. The lesion showed typical arterial-phase hyperenhancement consistent with HCC, while tumor markers remained within normal ranges. Repeat radiofrequency ablation achieved complete tumor eradication, and follow-up imaging remained negative for the subsequent four years.
Emergence of sdpHCC-ICC (2024)
In October 2024, a new disease progression was observed. At the age of 76, the patient developed new hepatic lesions in segments S5/6 and S6, suspicious for tumor recurrence or intrahepatic metastases (Figure 1). AFP levels remained within normal limits, whereas CA19-9 levels were elevated. His medical history was notable for a 40-year history of HBV infection, 30 years of hypertension, coronary artery disease diagnosed five years earlier, and an abdominal aortic aneurysm identified four years prior. Following vascular surgery consultation, endovascular stent graft placement was successfully performed.
 |
Figure 1 Dynamic contrast-enhanced magnetic resonance imaging (MRI) of the liver. (A) Axial T2-weighted fat-suppressed images demonstrate an irregular hyperintense lesion in segment S5/6 measuring approximately 2.9×2.0 cm, while a smaller lesion in segment S6 shows heterogeneous signal intensity with indistinct margins, measuring approximately 0.9×0.6 cm. (B) Diffusion-weighted imaging reveals marked hyperintensity of the S5/6 lesion and mildly increased signal intensity of the S6 lesion. (C) On T1-weighted images, the S5/6 lesion appears hypointense, whereas the S6 lesion shows isointense signal relative to the surrounding liver parenchyma. (D) During the arterial phase, the S5/6 lesion remains hypointense, while the S6 lesion shows no definite arterial enhancement. (E) In the portal venous phase, peripheral enhancement is observed in the S5/6 lesion, whereas no obvious enhancement is identified in the S6 lesion. (F) Delayed-phase images demonstrate relative hypointensity of the S5/6 lesion and decreased signal intensity of the S6 lesion compared with the surrounding liver parenchyma. White arrows indicate the locations of the intrahepatic lesions. |
After recovery, the patient underwent laparoscopic partial hepatectomy under intraoperative ultrasound and fluorescence guidance. Two hepatic lesions were identified: a 3.0 cm mass in S5/6 involving the right posterior branch of the portal vein, and a smaller 1.0 cm nodule in S6. Intraoperative frozen-section analysis revealed two distinct tumor entities: the S5/6 lesion was ICC, whereas the S6 lesion represented recurrent HCC. Both lesions were completely resected with tumor-free margins of approximately 2 cm. The postoperative course was uneventful, and the patient was discharged on postoperative day 5.
Pathological Findings
Final pathological examination confirmed a moderately to poorly differentiated ICC in segments S5/6 (2.9 × 2.0×2.0 cm), with microvascular and perineural invasion (M1) and negative surgical margins. Immunohistochemical staining showed: GPC-3 (−), CD34 (+), Arg-1 (−), HSP70 (+), GS (partial +), reticulin (+), CK7 (+), CK19 (+), and Hepatocyte (−). The S6 nodule was diagnosed as high-grade HCC (0.9 × 0.6 cm), without vascular or perineural invasion, and with negative margins. Immunohistochemical analysis demonstrated HepPar-1 (weak +), AFP (−), GPC-3 (+), CD34 (+), Arg-1 (weak +), HSP70 (+), GS (+), and reticulin (+) (Figure 2). All immunohistochemical staining was performed following standard institutional clinical protocols. Appropriate positive and negative tissue controls were concurrently evaluated for each marker to validate the staining specificity and accuracy.
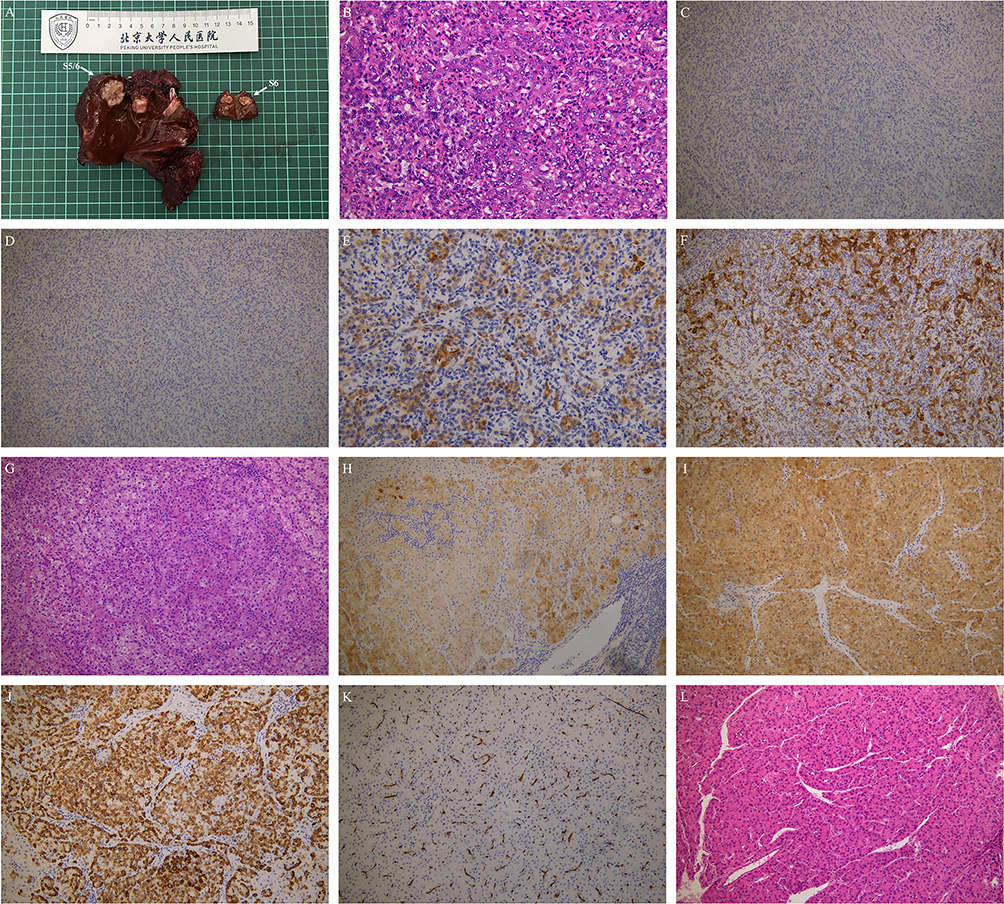 |
Figure 2 Gross pathology, histopathological features, and immunohistochemical profiles of the resected synchronous double primary hepatocellular carcinoma and intrahepatic cholangiocarcinoma, together with histology of the initial hepatocellular carcinoma resected at first diagnosis. (A) Gross specimen showing two distinct tumors: a moderately to poorly differentiated intrahepatic cholangiocarcinoma (ICC) located in segment S5/6 measuring 2.9×2.0 cm, and a well-differentiated hepatocellular carcinoma (HCC) in segment S6 measuring 0.9×0.6 cm. (B) Hematoxylin and eosin (H&E) staining of the S5/6 lesion demonstrates histological features consistent with ICC (original magnification ×200). (C and D) Immunohistochemical staining of the S5/6 lesion shows negative expression of glypican-3 (GPC-3) and arginase-1 (Arg-1) (×200). (E and F) The S5/6 lesion shows positive staining for cytokeratin 7 (CK7) and cytokeratin 19 (CK19), supporting a biliary epithelial phenotype (×200). (G) H&E staining of the S6 lesion reveals well-differentiated trabecular architecture consistent with HCC (×200). (H–J) Immunohistochemical analysis of the S6 lesion demonstrates positive expression of GPC-3, Arg-1, and hepatocyte paraffin 1 (HepPar-1), confirming hepatocellular differentiation (×200). (K) CD34 immunostaining highlights sinusoidal capillarization in the S6 lesion (×200). (L) Representative H&E section of the initial S3 tumor resected at first diagnosis shows well-differentiated hepatocellular carcinoma measuring approximately 2.0 cm (×200). |
Systemic Therapy and Follow-Up (2025)
Adjuvant therapy was initiated, consisting of one cycle of capecitabine monotherapy followed by combination therapy with capecitabine and gemcitabine. Tumor genomic profiling performed in March 2025 identified no actionable mutations (Table 1). However, by June 2025, imaging revealed multiple right hepatic metastases, retroperitoneal and perirenal nodules, as well as bone involvement. Combined immunotherapy and targeted therapy were initiated; however, the patient subsequently developed significant cancer-related pain.
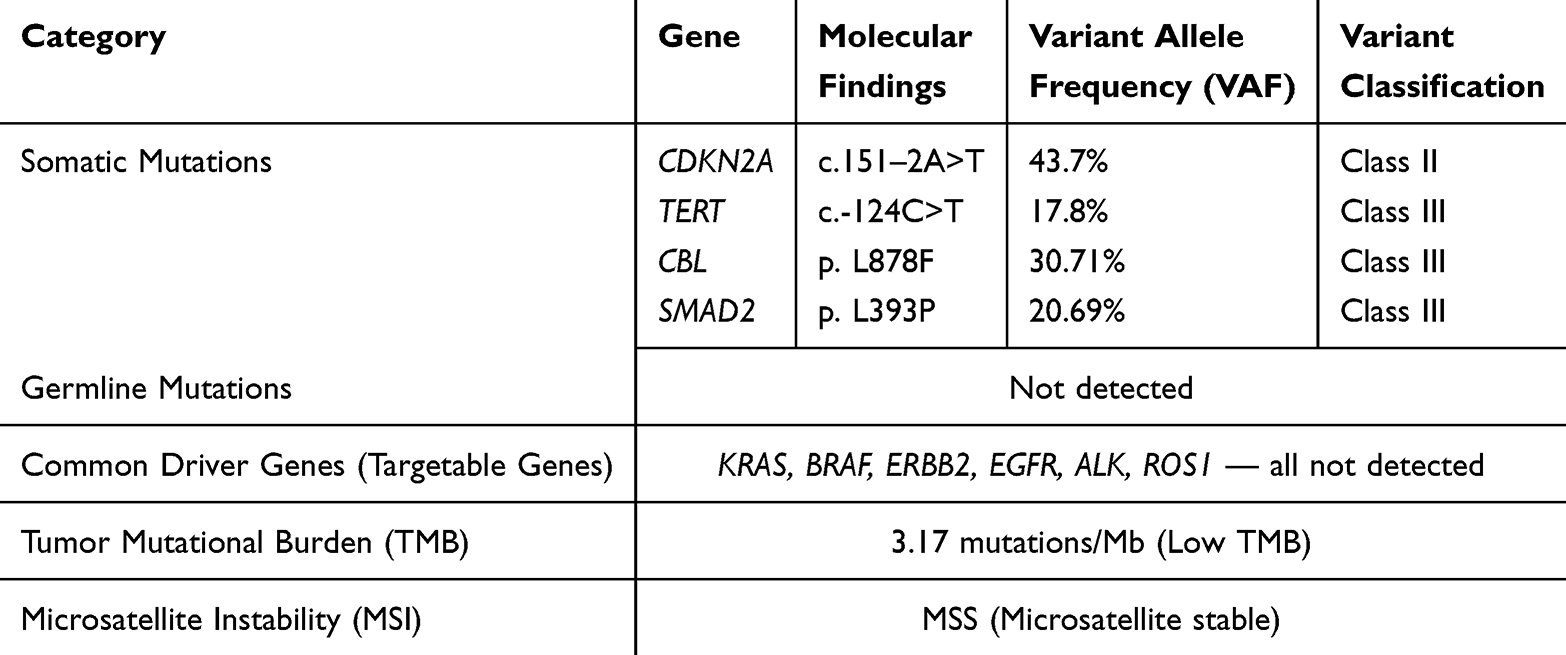 |
Table 1 The Results of the Next-Generation Sequencing (NGS) Analysis of 576 Relevant Genes From the Resected S5/6 Intrahepatic Cholangiocarcinoma Specimen in This Case |
At the most recent follow-up on December 25, 2025, the patient remained on combination systemic therapy. No new lesions were detected on follow-up imaging. Although his overall condition was fragile, the disease remained clinically and radiologically stable under ongoing systemic therapy (Figure 3).
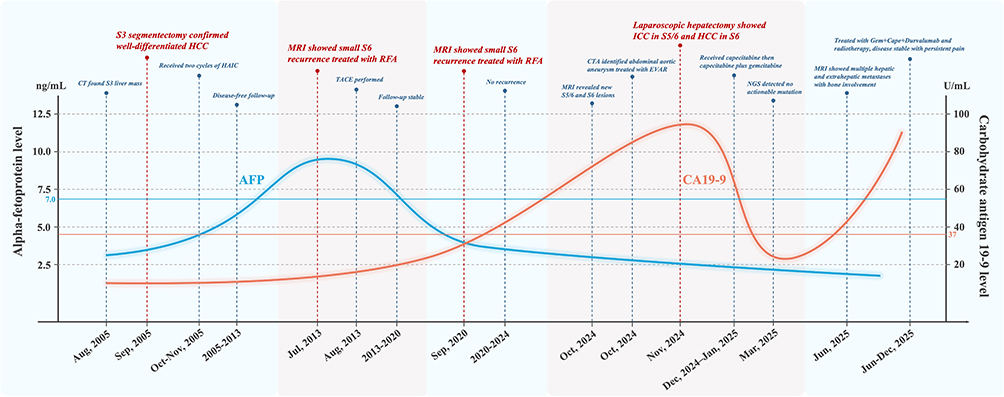 |
Figure 3 Timeline of clinical events and serum alpha-fetoprotein (AFP) and carbohydrate antigen 19–9 (CA19-9) levels. The normal upper reference limits are 7 ng/mL for AFP and 37 U/mL for CA19-9. |
Literature Review
Search Strategy and Selection Criteria
A literature search was performed in PubMed up to November 2025 using combinations of the following keywords: “synchronous double primary hepatocellular carcinoma”, “intrahepatic cholangiocarcinoma” and “dual primary liver cancer”. Published reports describing pathologically confirmed sdpHCC-ICC were reviewed. Cases involving combined HCC-CCA or metastatic disease without clear pathological distinction were excluded. Given the limited number and heterogeneity of published cases, only descriptive analyses were performed. We summarized 31 representative sdpHCC-ICC cases reported in the literature (Tables 2 and 3). Collectively, these cases delineate the demographic characteristics, clinical manifestations, pathological features, and prognostic patterns of this rare disease entity.
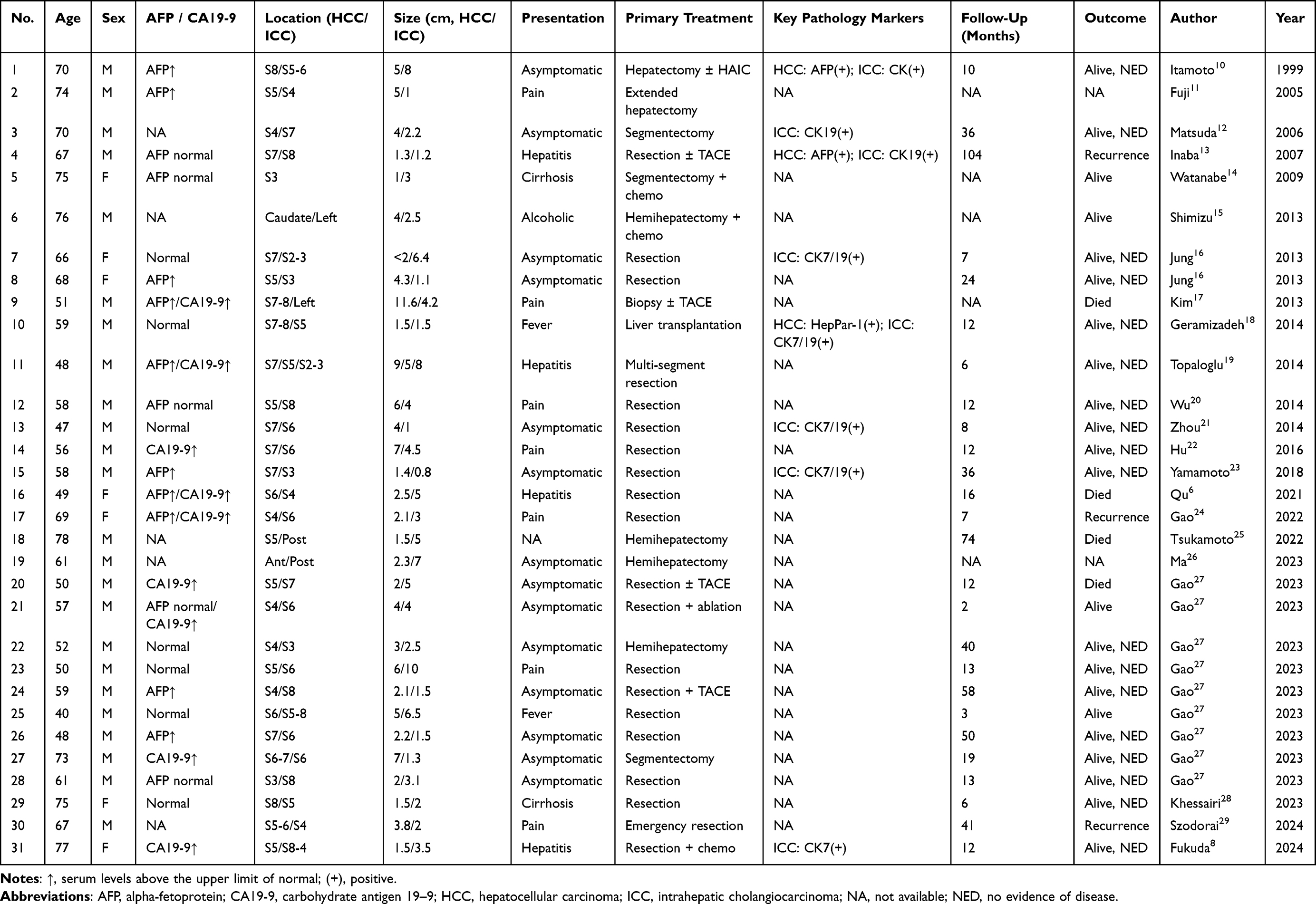 |
Table 2 Reported Cases of Synchronous Double Primary Hepatocellular Carcinoma and Intrahepatic Cholangiocarcinoma |
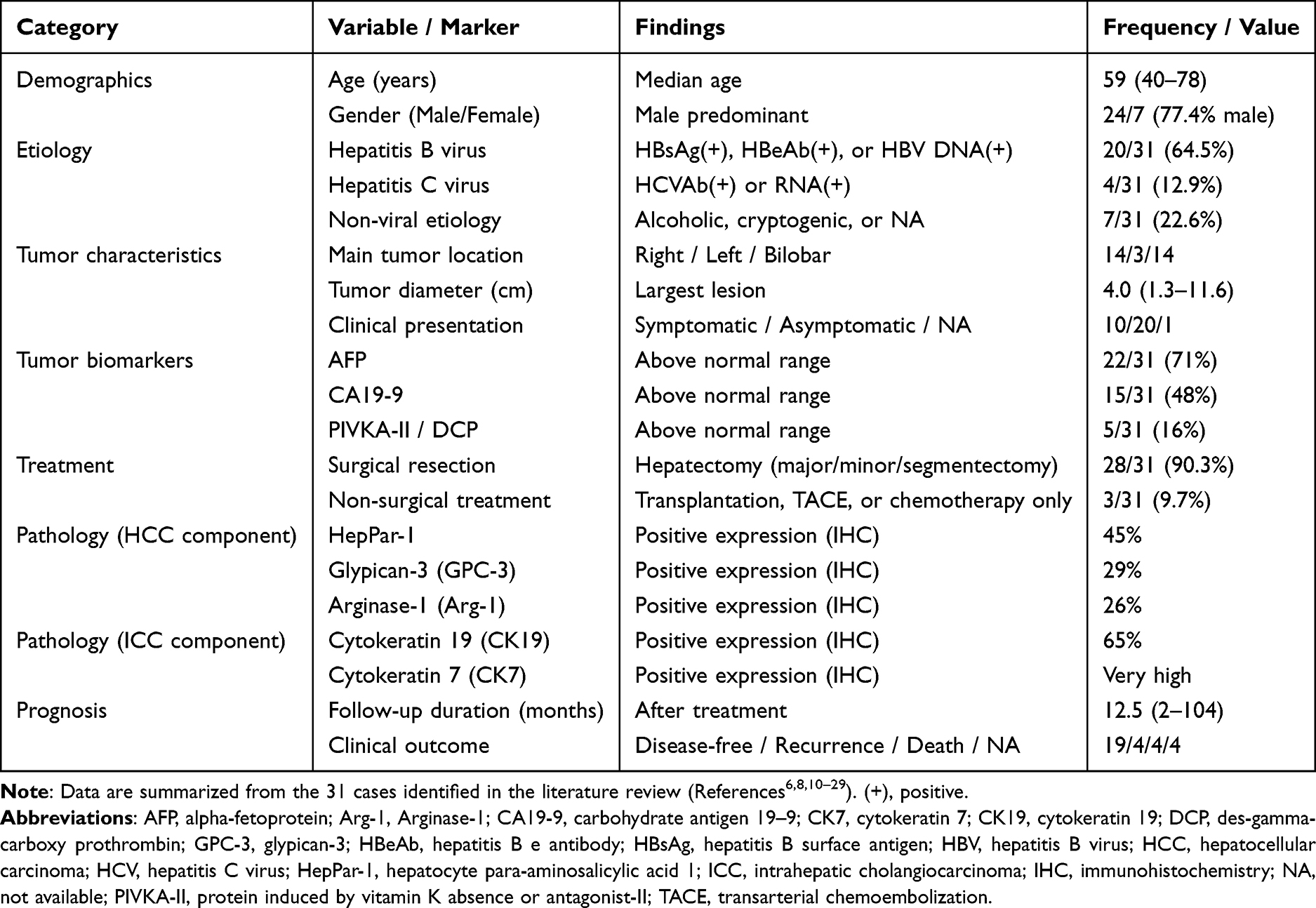 |
Table 3 Clinicopathological Characteristics and Molecular Features of Reported Cases of Synchronous Double Primary Hepatocellular Carcinoma and Intrahepatic Cholangiocarcinoma |
Demographic and Clinical Characteristics
Regarding the demographic and clinical characteristics of the cohort, the reported patients ranged in age from 40 to 78 years and showed a clear male predominance, consistent with the known male bias of hepatocellular carcinoma, particularly in the setting of chronic liver disease. Most patients had underlying chronic liver disease, most commonly hepatitis B virus infection, while a smaller proportion had hepatitis C infection or alcohol-related cirrhosis. Baseline tumor marker levels were heterogeneous: AFP and CA19-9 varied widely, and in a substantial proportion of cases, both markers remained within normal ranges. This lack of consistent tumor marker elevation highlights the diagnostic challenge of sdpHCC-ICC, particularly in the preoperative setting.
Tumor Features and Treatment Modalities
In terms of tumor characteristics and treatment modalities, the distribution was highly variable. Tumors were distributed across multiple hepatic segments, with segments 5–8 being the most frequently involved. Tumor size ranged from subcentimeter nodules to large masses exceeding 10 cm, and no consistent dominance in size or morphology was observed between the HCC and ICC components. Clinically, presentations ranged from incidental detection in asymptomatic patients to symptoms such as abdominal pain, malaise, or complications related to cirrhosis. Surgical resection remained the primary treatment modality, ranging from segmentectomy to lobectomy and, in selected cases, more extensive combined procedures. Adjunctive therapies, including TACE, HAIC, radiofrequency ablation, and systemic chemotherapy, were frequently employed depending on tumor stage and clinical context. Pathological examination consistently demonstrated two distinct malignant components—hepatocellular and cholangiocellular—distinguishable by histological architecture and immunohistochemical features. Immunohistochemical markers such as HepPar-1, CK7, CK19, GPC3, and CD34 were essential for distinguishing the two components, particularly when morphological features overlapped. The proliferative index, commonly assessed by Ki-67, varied widely, reflecting biological heterogeneity between the two tumor components.
Prognostic Patterns and Clinical Outcomes
Analysis of prognostic patterns and clinical outcomes revealed a highly variable course. While a subset of patients achieved prolonged disease-free survival following R0 resection, a significant proportion experienced early intrahepatic recurrence or distant metastases. Variables such as advanced age, large tumor burden, and incomplete resection were frequently associated with a poorer prognosis. Despite the heterogeneity of the reported data, these recurrence patterns underscore the need for individualized, multidisciplinary, and long-term management strategies.
Overall, the literature characterizes sdpHCC-ICC as a rare but clinically challenging entity with well-defined pathological features and unpredictable clinical behavior. In the context of our patient, who experienced multiple recurrences and treatments over two decades, these published cases provide valuable comparative insights, reinforcing the necessity of prolonged surveillance and repeated pathological reassessment.
Discussion
Phenotypic Evolution and Clinical Surveillance
This case describes an exceptionally rare and prolonged clinical course in which an initial solitary hepatocellular carcinoma evolved into synchronous double primary hepatocellular carcinoma and intrahepatic cholangiocarcinoma over nearly two decades. In contrast to most reported cases, in which HCC and ICC are diagnosed simultaneously at initial presentation, our patient first developed a solitary HCC, experienced multiple recurrences, and only later developed a distinct ICC component. This unusually long interval supports the concept that primary liver malignancies arising in chronically injured livers are dynamic and evolutionarily plastic rather than biologically static entities.30 Although similar long-term phenotypic evolution has been sporadically reported, it remains poorly characterized in the literature, underscoring both the rarity and clinical relevance of this case.
From a clinical perspective, this case highlights the necessity of lifelong surveillance in patients with chronic liver disease, even after apparently curative treatment. Current surveillance guidelines from the American Association for the Study of Liver Diseases (AASLD) and the European Association for the Study of the Liver (EASL) recommend continued imaging follow-up in patients with cirrhosis or chronic viral hepatitis, as the risk of de novo hepatobiliary malignancies persists indefinitely.31–33 Our case extends this concept by demonstrating that long-term survivors of HCC remain at risk not only for recurrence of the original tumor but also for the development of a second, biologically distinct primary malignancy within the liver.
Hypothesized Mechanisms of Phenotypic Divergence
The mechanisms underlying this phenotypic evolution are likely multifactorial and remain incompletely understood (Figure 4). Chronic hepatic inflammation, progressive fibrosis, and repeated therapeutic interventions may collectively create a permissive microenvironment that facilitates clonal diversification. The hepatic progenitor cell (HPC) hypothesis provides a biologically plausible framework, as bipotent progenitor cells residing in the canals of Hering retain the capacity to differentiate into either hepatocytic or cholangiocytic lineages under specific signaling conditions.34 Experimental and pathological studies have demonstrated that HPC activation is closely associated with chronic liver injury and correlates with the emergence of tumors exhibiting mixed or ambiguous differentiation patterns.35,36 Furthermore, the critical role of cancer stem cells (CSCs) or progenitor-like cells in driving therapeutic resistance and tumor relapse has been increasingly recognized, as they possess unique self-renewal and lineage-plasticity capabilities under chronic stress.37
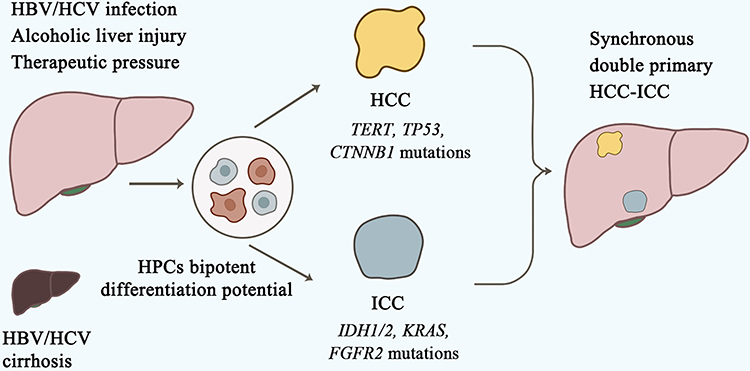 |
Figure 4 Hypothetical model illustrating the potential mechanisms underlying phenotypic divergence from solitary hepatocellular carcinoma (HCC) to synchronous double primary HCC and intrahepatic cholangiocarcinoma (ICC). Chronic liver injury, cirrhosis, and therapeutic pressure may promote hepatic progenitor cell activation and lineage plasticity, contributing to divergent hepatocytic and cholangiocytic differentiation pathways. |
At the molecular level, HCC and ICC are traditionally characterized by distinct mutational landscapes. HCC frequently harbors alterations in TERT, TP53, and CTNNB138 whereas ICC is more commonly associated with mutations in IDH1/2, KRAS, and FGFR2 fusions.39 Notably, next-generation sequencing in our patient did not identify these canonical driver mutations, suggesting that alternative mechanisms may have contributed to tumor evolution. Recent bioinformatics and translational studies have highlighted that beyond DNA mutations, the dysregulation of specific transcriptional networks, non-coding RNAs, and hub genes can profoundly influence HCC growth, cell phenotype, and clinical prognosis.40–43 Emerging evidence indicates that epigenetic remodeling, chromatin reprogramming, and tumor–microenvironment interactions can drive lineage plasticity independently of classical oncogenic mutations.44 Studies using lineage tracing and epigenomic profiling have shown that hepatocytes can undergo transdifferentiation toward a biliary phenotype under sustained inflammatory or oncogenic stress, raising the possibility that mutation-independent mechanisms may contribute to phenotypic divergence in selected cases.45,46
Diagnostic Challenges
From a diagnostic perspective, this case highlights the inherent limitations of conventional imaging modalities and serum biomarkers in complex hepatobiliary malignancies. The recurrent lesions exhibited overlapping radiological characteristics, while AFP levels remained persistently within the normal range, likely reflecting the well-differentiated nature of the HCC component. Several studies have reported that sdpHCC-ICC and related mixed tumors often lack the classic enhancement patterns characteristic of either HCC or ICC, resulting in frequent preoperative misclassification.47,48 Consequently, histopathological examination remains the diagnostic gold standard for definitive classification. In our case, immunohistochemical profiling—particularly the combined application of hepatocellular markers (HepPar-1, GPC-3, Arg-1) and biliary markers (CK7, CK19)—was essential for confirming the coexistence of two distinct primary malignancies.49 These findings emphasize the importance of comprehensive pathological evaluation, particularly in patients with atypical imaging features or discordant tumor marker profiles.
Therapeutic Perspectives and Outcomes
From a therapeutic perspective, the patient’s clinical course underscores the potential benefit of aggressive, multidisciplinary management in carefully selected cases. Repeated local therapies, including surgical resection, radiofrequency ablation, and transarterial interventions, contributed to prolonged disease control over an extended period. Although evidence remains limited, several retrospective studies suggest that repeat hepatectomy may confer meaningful survival benefits in patients with preserved liver function and localized recurrence.50 However, following the emergence of the ICC component, disease behavior became more aggressive, consistent with the generally poorer prognosis associated with ICC compared with HCC.51,52 This shift highlights the importance of reassessing tumor biology at each recurrence, rather than assuming biological continuity with the initial malignancy.
The most striking feature of this case is the exceptionally long latency preceding the emergence of the ICC component. While most reported dual primary tumors are synchronous at diagnosis, our case demonstrates that phenotypic divergence may occur after prolonged disease evolution and repeated therapeutic interventions. Clinically, this finding mandates a high index of suspicion during long-term surveillance. Small or atypical recurrent lesions should not be automatically classified as recurrent HCC without histological confirmation, as misclassification may delay appropriate treatment and adversely affect clinical outcomes. Distinguishing between simple recurrence, clonal evolution, and the emergence of a second primary malignancy has direct implications for prognosis, treatment selection, and patient counseling.
Limitations
Several limitations should be acknowledged. First, this study represents a single case observation, limiting the generalizability of the findings. Second, clonality analysis and longitudinal molecular profiling of sequential lesions were unavailable, precluding definitive conclusions regarding tumor origin and evolutionary trajectory. Third, the literature review was based primarily on published case reports with heterogeneous clinical data and incomplete follow-up information. Future multicenter studies incorporating longitudinal genomic and spatial transcriptomic analyses are warranted. Ultimately, addressing these complex clinical scenarios requires a comprehensive approach, as emphasized by the current guidelines for holistic integrative management of liver cancer, to optimize long-term patient outcomes.53
Conclusion
This case describes a rare long-term clinical evolution from solitary HCC to sdpHCC-ICC. Although the underlying mechanism remains uncertain, the findings highlight the diagnostic complexity and biological heterogeneity of primary liver malignancies arising in chronically injured livers. Clinically, this underscores an actionable takeaway: atypical or late recurrent lesions in long-term HCC survivors should prompt repeated pathological reassessment rather than empirical treatment, ensuring accurate diagnosis and appropriately tailored management.
Abbreviations
cHCC-CCA, combined hepatocellular-cholangiocarcinoma; sdpHCC-ICC, Synchronous double primary hepatocellular carcinoma and intrahepatic cholangiocarcinoma; HCC, Hepatocellular carcinoma; ICC, Intrahepatic cholangiocarcinoma; S3, Segment 3; AFP, Alpha-fetoprotein; CA19-9, Carbohydrate antigen 19-9; HAIC, Hepatic arterial infusion chemotherapy; TACE, Transarterial chemoembolization; AASLD, American Association for the Study of Liver Diseases; EASL, European Association for the Study of the Liver; HP, Hepatic progenitor cell.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of Peking University People’s Hospital (Approval No. 2024PHB395-001) and conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Specifically, Liyi Qiao and Pengcheng Wei drafted the manuscript. Pengcheng Wei, Jie Gao, Jiye Zhu, and Zhao Li performed the surgery. Liyi Qiao, Pengcheng Wei, Chen Lo, Yongjing Luo, Yun Peng, and Zhuoliang Kang analyzed the pathological data.
Funding
This research was funded by the National Natural Science Foundation of China (Grant No. 82472662), the Beijing Municipal Natural Science Foundation (Grant No. L258067), and the Noncommunicable Chronic Diseases-National Science and Technology Major Project (Project No. 2023ZD0502003).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Toh MR, Wong EYT, Wong SH, et al. Global epidemiology and genetics of hepatocellular carcinoma. Gastroenterology. 2023;164(5):766–13. doi:10.1053/j.gastro.2023.01.033
2. Elena P, Ariana MC, Bryar H, et al. Robotic laparoscopic resection for hepatocellular carcinoma. Mini-Invasive Surg. 2023;7:13. doi:10.20517/2574-1225.2022.112
3. Hwang SY, Danpanichkul P, Agopian V, et al. Hepatocellular carcinoma: updates on epidemiology, surveillance, diagnosis and treatment. Clin Mol Hepatol. 2025;31(Suppl):S228–S254. doi:10.3350/cmh.2024.0824
4. Alexandra MA, Hop STC. Minimally invasive approaches to intrahepatic cholangiocarcinoma. Mini-Invasive Surg. 2023;7:18. doi:10.20517/2574-1225.2023.12
5. Moris D, Palta M, Kim C, et al. Advances in the treatment of intrahepatic cholangiocarcinoma: an overview of the current and future therapeutic landscape for clinicians. CA Cancer J Clin. 2023;73(2):198–222. doi:10.3322/caac.21759
6. Qu MM, Zhu YH, Li YX, et al. Synchronous double primary hepatocellular carcinoma and intrahepatic cholangiocarcinoma: a case report and review of the literature. Medicine. 2021;100(46):e27349. doi:10.1097/MD.0000000000027349
7. Jung DH, Hwang S, Kim KH, et al. Clinicopathological features and post-resection prognosis of double primary hepatocellular carcinoma and intrahepatic cholangiocarcinoma. World J Surg. 2017;41(3):825–834. doi:10.1007/s00268-016-3787-4
8. Fukuda T, Onoe T, Tanimine N, et al. A rare case of synchronous double primary hepatocellular carcinoma and intrahepatic cholangiocarcinoma: a case report. Int J Surg Case Rep. 2024;118(C):109599. doi:10.1016/j.ijscr.2024.109599
9. Sakata M, Kitada K, Omote R, et al. Synchronous double primary combined hepatocellular-cholangiocarcinoma and cholangiolocarcinoma in a cirrhotic liver. J Clin Transl Hepatol. 2023;11(4):991–997. doi:10.14218/JCTH.2022.00382
10. Itamoto T, Asahara T, Katayama K, et al. Double cancer—hepatocellular carcinoma and intrahepatic cholangiocarcinoma with a spindle-cell variant. J Hepatobiliary Pancreat Surg. 1999;6(4):422–426. doi:10.1007/s005340050144
11. Fuji N, Taniguchi H, Amaike H, et al. Synchronously resected double primary hepatic cancer, hepatocellular carcinoma and cholangiocarcinoma. J Gastroenterol Hepatol. 2005;20(6):967–969. doi:10.1111/j.1440-1746.2005.03806.x
12. Matsuda M, Hara M, Suzuki T, et al. Synchronously resected double primary hepatic cancers—hepatocellular carcinoma and cholangiolocellular carcinoma. J Hepatobiliary Pancreat Surg. 2006;13(6):571–576. doi:10.1007/s00534-006-1118-0
13. Inaba K, Suzuki S, Sakaguchi T, et al. Double primary liver cancer (intrahepatic cholangiocarcinoma and hepatocellular carcinoma) in a patient with hepatitis C virus-related cirrhosis. J Hepatobiliary Pancreat Surg. 2007;14(2):204–209. doi:10.1007/s00534-006-1134-0
14. Watanabe T. Synchronous development of HCC and CCC in the same subsegment of the liver in a patient with type C liver cirrhosis. World J Hepatol. 2009;1(1):103–109. doi:10.4254/wjh.v1.i1.103
15. Shimizu S, Oshita A, Tashiro H, et al. Synchronous double cancers of primary hepatic adenosquamous carcinoma and hepatocellular carcinoma: report of a case. Surg Today. 2013;43(4):418–423. doi:10.1007/s00595-012-0346-y
16. Jung KS, Chun KH, Choi GH, et al. Synchronous development of intrahepatic cholangiocarcinoma and hepatocellular carcinoma in different sites of the liver with chronic B-viral hepatitis: two case reports. BMC Res Notes. 2013;6(1):520. doi:10.1186/1756-0500-6-520
17. Kim JO, Jun DW, Jang K. Synchronous double primary hepatic cancer: hepatocellular carcinoma and intrahepatic cholangiocarcinoma [in Korean]. Korean J Gastroenterol. 2013;62(2):135. doi:10.4166/kjg.2013.62.2.135
18. Geramizadeh B, Gity R, Bahraini A, et al. Synchronous hepatocellular carcinoma and cholangiocarcinoma in a patient transplanted for cryptogenic cirrhosis. Int J Organ Transplant Med. 2014;5(3):125–128.
19. Topaloglu S, Saglam K, Calik A, et al. Synchronous occurrence of hepatocellular carcinoma and intrahepatic cholangiocarcinoma in both lobes of the liver. Turk J Gastroenterol. 2014;25(2):209–211. doi:10.5152/tjg.2014.6188
20. Wu C, Bai DS, Jiang GQ, et al. Synchronous double cancers of primary hepatocellular carcinoma and intrahepatic cholangiocarcinoma: a case report and review of the literature. World J Surg Oncol. 2014;12(1):337. doi:10.1186/1477-7819-12-337
21. Zhou R, Zhang M, Cheng N, et al. Double primary hepatic cancer (hepatocellular carcinoma and intrahepatic cholangiocarcinoma) in a single patient: a case report. Oncol Lett. 2016;11(1):273–276. doi:10.3892/ol.2015.3896
22. Hu J, Yuan R, Huang C, et al. Double primary hepatic cancer (hepatocellular carcinoma and intrahepatic cholangiocarcinoma) originating from hepatic progenitor cell: a case report and review of the literature. World J Surg Oncol. 2016;14(1):218. doi:10.1186/s12957-016-0974-6
23. Yamamoto M, Oshita A, Nishisaka T, et al. Synchronous double primary hepatic cancer consisting of hepatocellular carcinoma and cholangiolocellular carcinoma: a case report. J Med Case Rep. 2018;12(1):224. doi:10.1186/s13256-018-1762-4
24. Gao L, Huang JY, Lu ZJ, et al. Contrast-enhanced ultrasound manifestations of synchronous combined hepatocellular-cholangiocarcinoma and hepatocellular carcinoma: a case report. World J Clin Cases. 2022;10(11):3615–3623. doi:10.12998/wjcc.v10.i11.3615
25. Tsukamoto T, Kodai S, Nobori C, et al. Synchronous double primary non-B, and non-C intrahepatic cholangiocarcinoma and hepatocellular carcinoma-a case report [in Japanese]. Gan To Kagaku Ryoho. 2022;49(4):486–488.
26. Ma H, Wu X. Surgical resection of synchronous double primary hepatocellular carcinoma and intrahepatic cholangiocarcinoma: a case report [in Chinese]. J Clin Med Pract. 2023;8:667–669.
27. Gao Y. Clinical characteristics and surgical prognosis of synchronous double primary hepatocellular carcinoma and intrahepatic cholangiocarcinoma [in Chinese]. Chin J Gen Surg. 2023;32:200–205.
28. Khessairi N, Mallek I, Laabidi T, et al. Synchronous presentation of hepatocellular carcinoma and intrahepatic cholangiocarcinoma: report of an exceptional case with review of the literature. Int J Surg Case Rep. 2024;114(C):109140. doi:10.1016/j.ijscr.2023.109140
29. Szodorai R, Fülöp E, Fülöp A, et al. Synchronous hepatocellular and intrahepatic cholangiocellular carcinoma with predominant ductal plate malformation pattern. A case report and review of the literature. Cancer Rep. 2025;8:e70085.
30. Sia D, Villanueva A, Friedman SL, et al. Liver cancer cell of origin, molecular class, and effects on patient prognosis. Gastroenterology. 2016;152(4):745–761. doi:10.1053/j.gastro.2016.11.048
31. Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 practice guidance by the American association for the study of liver diseases. Hepatology. 2018;68(2):723–750. doi:10.1002/hep.29913
32. Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology. 2018;67(1):358–380. doi:10.1002/hep.29086
33. European Association for the Study of the Liver. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69(1):182–236. doi:10.1016/j.jhep.2018.03.019
34. Roskams T. Liver stem cells and their implication in hepatocellular and cholangiocarcinoma. Oncogene. 2006;25(27):3818–3822. doi:10.1038/sj.onc.1209558
35. Heim D, Wege H. Hepatic stem and progenitor cells in liver diseases and hepatocarcinogenesis. Minerva Gastroenterol Dietol. 2009;55(2):111–121.
36. Rosenberg N, Van Haele M, Lanton T, et al. Combined hepatocellular-cholangiocarcinoma derives from liver progenitor cells and depends on senescence and IL-6 trans-signaling. J Hepatol. 2022;77(6):1631–1641. doi:10.1016/j.jhep.2022.07.029
37. Tang KY, Du SL, Wang QL, et al. Traditional Chinese medicine targeting cancer stem cells as an alternative treatment for hepatocellular carcinoma. J Integr Med. 2020;18(3):196–202. doi:10.1016/j.joim.2020.02.002
38. Schulze K, Imbeaud S, Letouzé E, et al. Exome sequencing of hepatocellular carcinomas identifies new mutational signatures and potential therapeutic targets. Nat Genet. 2015;47(5):505–511. doi:10.1038/ng.3252
39. Jusakul A, Cutcutache I, Yong CH, et al. Whole-genome and epigenomic landscapes of etiologically distinct subtypes of cholangiocarcinoma. Cancer Discov. 2017;7(10):1116–1135. doi:10.1158/2159-8290.CD-17-0368
40. Xu W, Liao S, Hu Y, et al. Upregulation of miR-3130-5p enhances hepatocellular carcinoma growth by suppressing ferredoxin 1: miR-3130-5p enhances HCC growth via inhibiting FDX1. Curr Mol Pharmacol. 2024;17:e18761429358008. doi:10.2174/0118761429358008250305070518
41. Gudivada IP, Amajala KC. Integrative bioinformatics analysis for targeting hub genes in hepatocellular carcinoma treatment. Curr Genomics. 2025;26(1):48–80. doi:10.2174/0113892029308243240709073945
42. Ye W, Wang J, Zheng J, et al. Association between higher expression of Vav1 in hepatocellular carcinoma and unfavourable clinicopathological features and prognosis. Protein Pept Lett. 2024;31(9):706–713. doi:10.2174/0109298665330781240830042601
43. Mu R, Chang M, Feng C, et al. Analysis of the expression of PRDX6 in patients with hepatocellular carcinoma and its effect on the phenotype of hepatocellular carcinoma cells. Curr Genomics. 2024;25(1):2–11. doi:10.2174/0113892029273682240111052317
44. Davies A, Zoubeidi A, Beltran H, et al. The transcriptional and epigenetic landscape of cancer cell lineage plasticity. Cancer Discov. 2023;13(8):1771–1788. doi:10.1158/2159-8290.CD-23-0225
45. Gadd VL, Aleksieva N, Forbes SJ. Epithelial plasticity during liver injury and regeneration. Cell Stem Cell. 2020;27(4):557–573. doi:10.1016/j.stem.2020.08.016
46. Tsuchiya A, Lu WY. Liver stem cells: plasticity of the liver epithelium. World J Gastroenterol. 2019;25(9):1037–1049. doi:10.3748/wjg.v25.i9.1037
47. Li R, Cai P, Ma KS, et al. Dynamic enhancement patterns of intrahepatic cholangiocarcinoma in cirrhosis on contrast-enhanced computed tomography: risk of misdiagnosis as hepatocellular carcinoma. Sci Rep. 2016;6(1):26772. doi:10.1038/srep26772
48. Horvat N, Nikolovski I, Long N, et al. Imaging features of hepatocellular carcinoma compared to intrahepatic cholangiocarcinoma and combined tumor on MRI using liver imaging and data system (LI-RADS) version 2014. Abdom Radiol. 2018;43(1):169–178. doi:10.1007/s00261-017-1261-x
49. Brunt E, Aishima S, Clavien PA, et al. cHCC-CCA: consensus terminology for primary liver carcinomas with both hepatocytic and cholangiocytic differentation. Hepatology. 2018;68(1):113–126. doi:10.1002/hep.29789
50. Itamoto T, Nakahara H, Amano H, et al. Repeat hepatectomy for recurrent hepatocellular carcinoma. Surgery. 2007;141(5):589–597. doi:10.1016/j.surg.2006.12.014
51. Lin RY, Kahramangil D, Ozer M, et al. Patient outcomes in resected combined hepatocellular cholangiocarcinoma (cHCC-ICC) and intrahepatic cholangiocarcinoma: a single center study. Cancers. 2024;16(22):3878. doi:10.3390/cancers16223878
52. Yang JQ, Wang XG, Wu B. Incidence trend and prognosis of intrahepatic cholangiocarcinoma: a study based on the SEER database. Transl Cancer Res. 2023;12(11):3007–3015. doi:10.21037/tcr-23-1278
53. Zhang N, Lu L, Cao B, et al. Liver protection of CACA technical guidelines for holistic integrative management of cancer. Holist Integr Oncol. 2025;4(1):28. doi:10.1007/s44178-025-00157-5
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.