")
Back to Journals » International Medical Case Reports Journal » Volume 16
Rare Cystic Hygroma of the Axilla and Breast in Adults, Case Report, Long-Term Follow-Up and Literature Review: An Experience from Saudi Arabia
Authors Al-Ameer AY , Alahmar SM, Shawafgfeh NN, Miskeen E
Received 22 August 2022
Accepted for publication 26 November 2022
Published 5 January 2023 Volume 2023:16 Pages 1—6
DOI https://doi.org/10.2147/IMCRJ.S387082
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ronald Prineas
Ahmed Y Al-Ameer,1 Soha M Alahmar,2 Nidal N Shawafgfeh,3 Elhadi Miskeen4
1Department of Surgery, College of Medicine, University of Bisha, Bisha, Saudi Arabia; 2Department of Surgery, King Faisal Medical City of Southern Region, Abha-Aseer, Saudi Arabia; 3Department of Surgery, Mafraq Sarah Specialty Hospital, Al-Mafraq, Jordan; 4Department of Obstetrics and Gynaecology, College of Medicine, University of Bisha, Bisha, Saudi Arabia
Correspondence: Ahmed Y Al-Ameer, Department of Surgery, College of Medicine, University of Bisha, P.O. Box 1290, Bisha, 1922, Saudi Arabia, Tel +966558407322, Email [email protected]
Introduction: Cystic hygroma (CH) in adults is a rare condition. Most CH cases are diagnosed at birth or during the first two years of life. Head and neck are the most common sites. There is scanty information about the natural history and follow-up of adult patients with axillary and breast CH. Hence, we present this case to shed some light on the natural history, complications, and a new suggested modality of treatment to deal with the complications.
Case Presentation: We report a case of a 39-year-old female who presented after ten years of excision of the right axillary CH with massive breast edema and recurrence of cysts in the ipsilateral breast and axilla. The insertion treated the edema of a breast-peritoneal shunt.
Discussion: The procedure was performed by inserting a normal V-P shunt catheter without a reservoir through a small incision in the inframammary fold toward the breast and another tiny incision at 10 of the clock in the right breast for fixation in the breast parenchyma. A catheter was inserted through a small incision on the right lumbar spine without intraperitoneal fixation after the catheter was inserted subcutaneously.
Conclusion: This case report shows that adult CH can reoccur. To our knowledge, this is the second case of CH concomitantly involving the breast and axilla. The shunt of the edematous fluid to the peritoneal cavity can give hope for intractable breast edema treatment.
Keywords: cystic hygroma, adult, case report
Introduction
A cystic hygroma (CH) is commonly presented in the first trimester of pregnancy as a small, thin hypogenic protrusion in the posterior fetal neck and is considered a normal finding. In some cases, the space is enlarged due to a cystic hygroma.1,2
Ninety percent of CH is diagnosed in infancy or before two years of life, and 75% occur in the cervicofacial region.3 Adult mammary CH is rare and has been reported as an isolated axillary or simultaneous with another CH in the breast. Park et al4 2018 reported the first simultaneous breast and axillary CH case.
The cause of CH is generally unknown, but there is evidence of causes,5 such as viral infections, trauma, and congenital misrouting between lymphatic and venous pathways. Chromosomal abnormalities have been identified at CH, commonly involving Noonan syndrome, trisomies 13, 18, and 21, and Turner syndrome. However, there is little literature on chromosomal abnormalities in CH adults.6
Several classifications and staging systems of CH have been suggested and adopted for better management.7–9 There is scanty information about the natural history and follow-up of adult patients with axillary and breast CH. Hence, we present this case to shed some light on the natural history, complications, and a new suggested modality of treatment to deal with the complications.
Case Report
A 39-year-old female premenopausal, P4 +0, presented to the breast surgery clinic with right breast swelling for ten years. The swelling started gradually following the excision of a right axillary lump. The mass was diagnosed as a right axillary CH of about 2cm × 1cm in dimensions. Just before her presentation, the swelling became big enough to disturb her daily activities. She had no family history of breast cancer. There were no other swellings elsewhere in her body. She was not a smoker or alcoholic, and there was no previous surgery or chronic illnesses. Examination revealed a swollen right breast with “peau d’ orange” and erythema around the right nipple-areola complex (NAC). There was asymmetry in the shape of the right breast compared to the left and right breast ptosis. The skin was thickened and red but no hotness or tenderness. No masses were felt in the right breast. The right NAC appeared normal. Apart from the linear scar of the previous CH excision in the right axilla, the axilla was normal. Left breast and axilla examination revealed no obvious or palpable abnormalities (Figure 1). Ultrasound examination of the breast and axilla revealed mild skin thickening. The breast parenchyma was dense and showed an anechoic tubular and round structure. The right breast showed a loculated cystic area with internal septations. It measured 3.4cm × 1.2cm × 5.1cm and multiple smaller cyst (Figure 2A). The mammogram showed marked skin thickening with edema (Figure 2B).
 |
Figure 1 Patient in supine position before the shunt surgery and after aspiration of the cyst. |
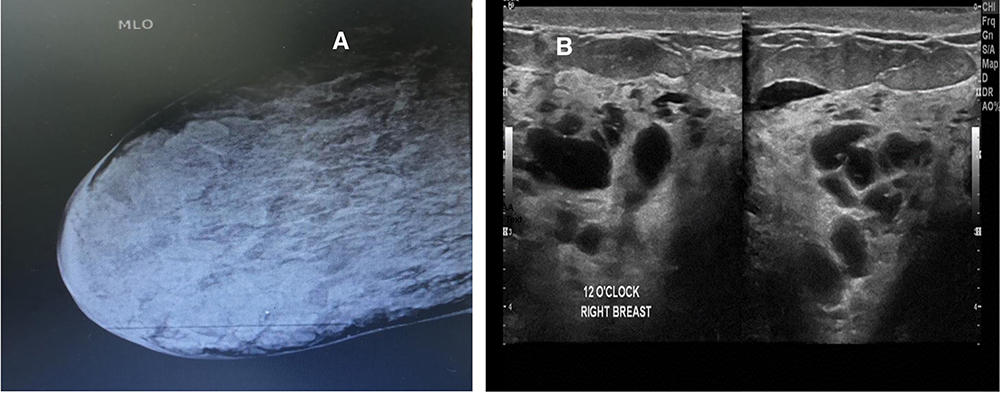 |
Figure 2 (A) Right mediolateral oblique mammogram. (B) Ultrasound shows multiple cystic lesions preoperatively. |
We attempted needle aspiration away from the cysts, and the fluid was easily aspirated from the edematous breast tissues. The fluid was watery and clear yellowish. The laboratory result of the fluid was lymphatic fluid. Aspiration trials were repeated twice with almost a complete resolution of the edema, but there was a recurrence within two weeks in every aspiration attempt. Subsequently, the patient consented to a shunt catheter placement between the edematous breast and the peritoneal cavity, a relatively new technique for breast edema secondary to CH. There was a partial resolution of the breast edema after the shunt surgery. The patient was followed up for five years. The last ultrasound and mammogram showed recurrence of cysts of the same axilla, and new cysts appeared in the breast (Figure 3A and B).
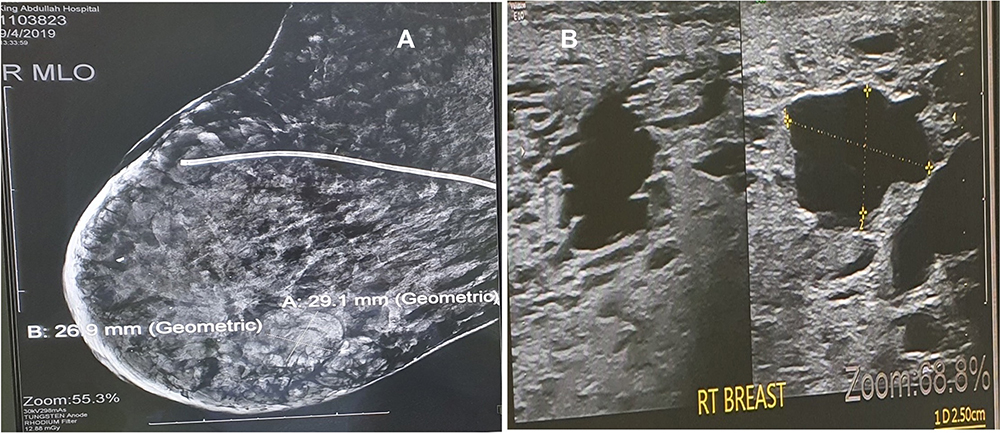 |
Figure 3 (A) Mammogram shows recurrence of cystic lesions in the breast and partial resolution of edema shunt in the breast tissue. (B) Cystic lesion recurrence on ultrasound. |
Discussion
Adult mammary cystic hygroma (CH) is a benign condition of unknown cause.3 Congenital failure in the lymphatic and venous pathways result in CH in newborn and those in the first two years of age. These cases represent 90% of CH and mainly involve the head and neck region.
Adult mammary CH cases are exceedingly rare.4,5 Few cases have been reported in the last 50 years worldwide, majority reported cases were female. Park et al4 2018 reported the first simultaneous breast and axillary CH case. We report this as a second concomitant breast and axillary CH case.
Several causes of adult CH have been suggested.6 In addition to congenital miscommunication between lymphatic and venous pathways, trauma, viral infection, and chromosomal abnormalities were suggested. However, no chromosomal studies on adult CH were reported.
Several classification systems for CH have been suggested and adopted based on size, location, and histological appearance.7–9 Such classifications unified the terms used in clinical practice and improved management (Table 1).
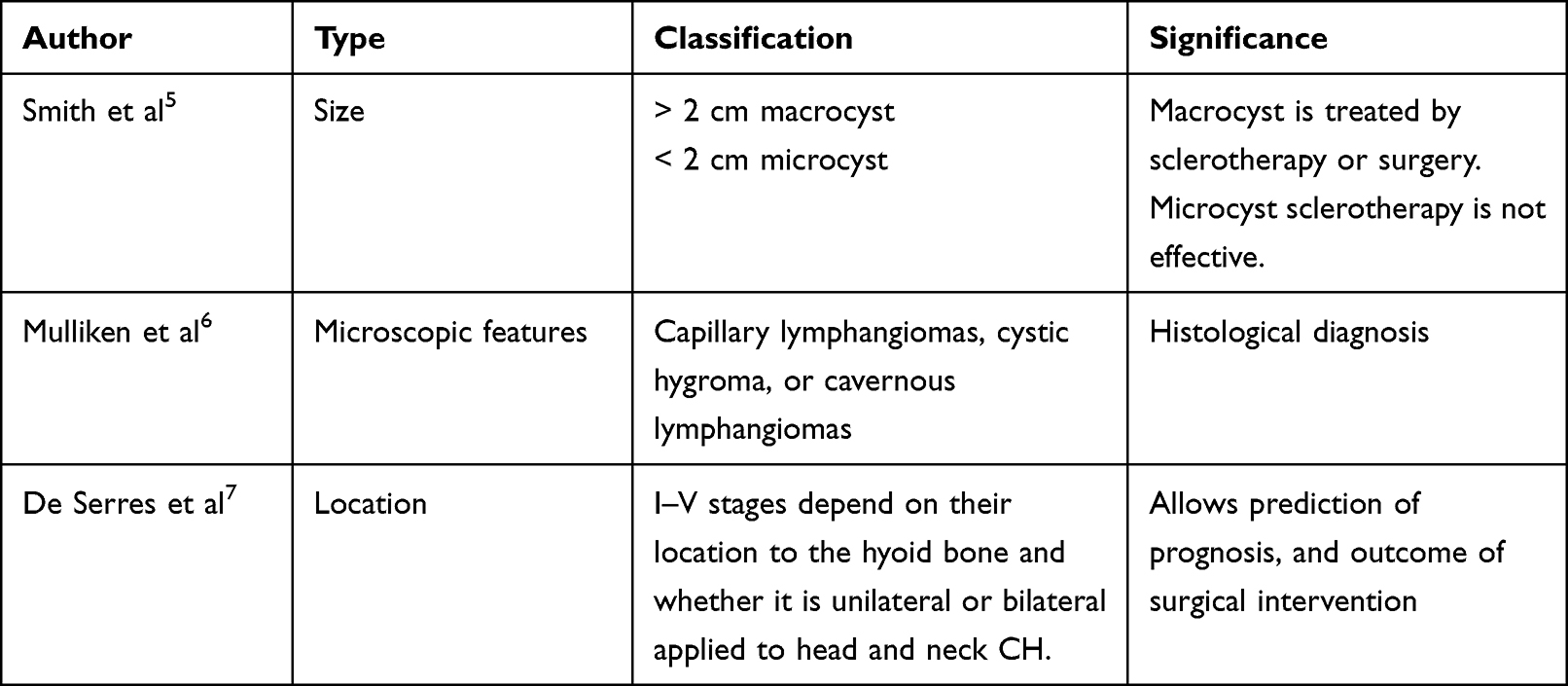 |
Table 1 Classification Systems for CH |
The most common clinical presentation of mammary CH10 is painless, slowly growing breast or axillary mass. Our case presented the same early presentations in the course of her illness, lately complicated with massive breast edema and a new appearance of lesions in the ipsilateral breast and axilla.
The diagnosis of such cases can be confirmed by several radiological modalities such as ultrasound, computed tomography, magnetic resonance imaging, and laboratory test of the aspirated fluids.
The mainstay of treatment of CH6,10 is surgery or sclerotherapy. In our case, there were multiple cysts in the breast and axilla, and the main complaint was breast edema. Burezq et al11 also stated that aspiration of cystic hygroma is a safe and effective treatment, so we found aspiration of the recurrent cysts is an attractive treatment modality; otherwise, she would have ended up with mastectomy. At this stage, we believed that the cause of the breast edema was a regional lymphatic system failure. The mastectomy was inadvisable because of the expected postoperative seroma and the impossibility of reconstructive surgery post-mastectomy. The trials of aspiration of the breast tissue edema encouraged us to put a shunt between the breast and peritoneal cavity. After explaining the possible options to the patient, she agreed with the shunt procedure.
Informed consent was obtained from the patient. The procedure was performed by inserting a regular V-P shunt catheter without a reservoir through a small inframammary fold incision toward the breast tissue and another tiny incision at 10 o’clock right breast for fixation in the breast parenchyma. A catheter was introduced through a small right lumbar incision without intraperitoneal fixation after passing the catheter subcutaneously (Figure 4A–C).
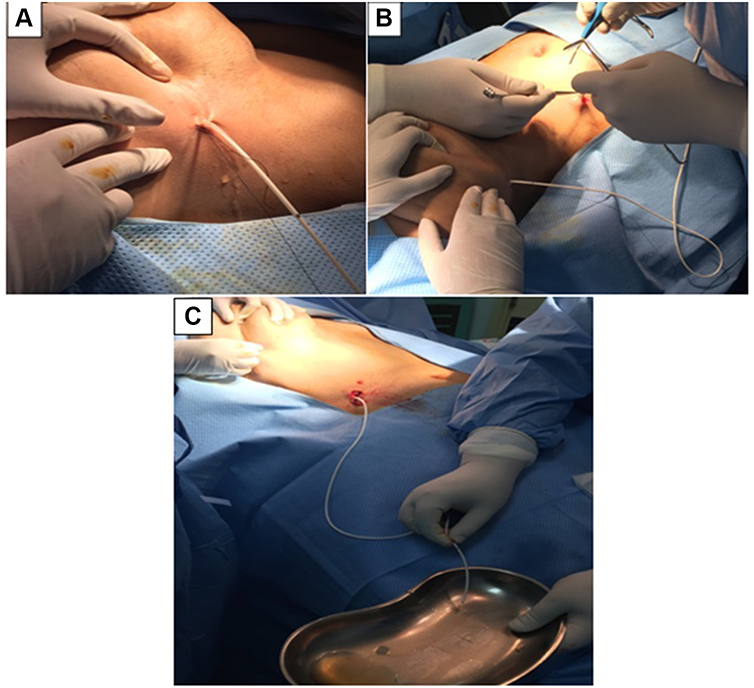 |
Figure 4 (A) Inframammary fold incision for the catheter insertion in the right breast. (B) The right lumber region incision for the catheter insertion. (C) The fluid is freely draining from the breast tissue before insertion into peritoneal cavity. |
Chest and abdominal x-ray were to ensure the catheter was in place (Figure 5). We followed up with the patient for five years. A few months later, she had a recurrent cyst aspirated again, and edema had improved, and the risk linked to the procedure including infection risk as possible complication.
 |
Figure 5 Arrow shows the catheter. |
Conclusion
Adult patients with CH should have life-long follow-ups. The disease can reoccur even after complete excision. Inserting a shunt between the breast and peritoneum might give hope for intractable edema. Still, more cases need to be done to determine the validity and efficacy of such a treatment modality.
Ethical Approval
Ethical approval was issued by Research Ethics Local Committee on 21/05/2020 (Ref No: UBCOM.RELOC)/H-06-BH-087.
Consent
Written informed consent was obtained from the patient to publish this case report and accompanying images. On request, a copy of the written permission is available for review by the Editor-in-Chief of this journal.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, case report and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. All authors contributed to the case report and management, have agreed on the journal and gave final approval of the version to be published. Al Ameer and Soha; data acquisition, manuscript preparation; AlAmeer, editing, and final approval; Nidal and Miskeen.
Funding
The authors declare that this study had no funding resources. There is no sponsor for this study. The author covers all expenses.
Disclosure
The authors report no conflicts of interest related to this article.
References
1. Scholl J, Durfee SM, Russell MA, et al. First-trimester cystic hygroma: relationship of nuchal translucency thickness and outcomes. Obstet Gynecol. 2012;120(3):551–559. doi:10.1097/AOG.0b013e318264f829
2. Graesslin O, Derniaux E, Alanio E, et al. Characteristics and outcome of fetal cystic hygroma diagnosed in the first trimester. Acta Obstet Gynecol Scand. 2007;86(12):1442–1446. doi:10.1080/00016340701644843
3. Phillip C, Liaqat A, Shaukat M. Spontaneous lymphocoele: an unusual cause of an axillary mass. BMJ Case Rep. 2016;2016:bcr2015213088. doi:10.1136/bcr-2015-213088
4. Park T, Lee HS, Jung EJ, et al. Concomitant breast and axillary lymphangioma in an adult: a case report and a review of the literature. Medicine. 2018;97(45):e12946. doi:10.1097/MD.0000000000012946
5. Shukla S, Shivhare R, Lal V, Rathore D. Cystic lymphangioma of breast and axillary region in an adult: a rare presentation. Int Surg J. 2021;8(1):391–394. doi:10.18203/2349-2902.isj20205911
6. McCaffrey F, Taddeo J. Surgical management of adult-onset cystic hygroma in the axilla. Int J Surg Case Rep. 2015;7C:29–31. doi:10.1016/j.ijscr.2014.11
7. Adams MT, Saltzman B, Perkins JA. Head and neck lymphatic malformation treatment: a systematic review. Otolaryngol Head Neck Surg. 2012;147(4):627–639. doi:10.1177/0194599812453552
8. Mulliken JB, Glowacki J. Hemangiomas and vascular malformations in infants and children: a classification based on endothelial characteristics. Plast Reconstr Surg. 1982;69(3):412–422. doi:10.1097/00006534-198203000-00002
9. de Serres LM, Sie KC, Richardson MA. Lymphatic malformations of the head and neck. A proposal for staging. Arch Otolaryngol. 1995;121(5):577–582. doi:10.1001/archotol.1995.01890050065012
10. Huanga YH, Laia YW, Hsieha TY. Axillary cystic hygroma in an adult. Formosan J Surg. 2014;47:105–107. doi:10.1016/j.fjs.2013.10.004
11. Burezq H, Williams B, Chitte SA. Management of cystic hygromas: 30-year experience. J Craniofac Surg. 2006;17:815–818. doi:10.1097/00001665-200607000-00041
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.