")
Back to Journals » Research Reports in Clinical Cardiology » Volume 14
Rare Case of Mitral Valve and Tricuspid Valve Aneurysm Presented with Progressive Dyspnea
Authors Abdi IA , Elmi Abdi A, Farah Yusuf Mohamud M
Received 3 August 2022
Accepted for publication 8 March 2023
Published 11 March 2023 Volume 2023:14 Pages 9—12
DOI https://doi.org/10.2147/RRCC.S384517
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Kones
Ishak Ahmed Abdi,1 Ahmed Elmi Abdi,1 Mohamed Farah Yusuf Mohamud2
1Department of Cardiology, Mogadishu Somali Turkish Training and Research Hospital, Mogadishu, Somalia; 2Mogadishu Somali Turkish Training and Research Hospital, Mogadishu, Somalia
Correspondence: Ishak Ahmed Abdi, Email [email protected]
Introduction: Mitral valve aneurysm (MVA) is a saccular, bulging structure of the mitral leaflet that expands during systole and collapses during diastole. Morand provided the first description of the MVA case in 1729. There are no symptoms or indicators particular to an aneurysm in MVA; instead, the clinical findings are comparable to those in mitral regurgitation. Tricuspid valve aneurysms are a bulging or outpouching of the septal leaflet of the tricuspid valve and have been documented in the literature less frequently in association with endocarditis, but as congenital anomaly they have not yet been reported.
Case Presentation: We present a case of mitral valve aneurysm and tricuspid aneurysm causing progressive dyspnea. To our knowledge this is the first case of an incidental finding of bilateral atrioventricular valve aneurysm. The patient cardiac findings were limited to mild symptoms and were managed with a medical approach.
Conclusion: Atrioventricular aneurysm discovery by accident is infrequent. Shortness of breath and increasing dyspnea may result from this. Only a few cases have been described in the medical literature. In this instance, an unexpected cause of dyspnea in an elderly patient is presented.
Keywords: tricuspid valve aneurysm, mitral valve aneurysm, pulmonary hypertension
Background
Mitral valve aneurysm (MVA) is a saccular, protruding structure of the mitral leaflet that expands during systole and shrinks during diastole.1 However, it is unclear what caused it to arise in the first place. Endocarditis, rheumatic disease, and other connective tissue disorders such mitral valve prolapse, osteogenesis imperfecta, Marfan syndrome, and pseudoxanthoma elasticum may cause the mitral leaflet to weaken.2 In patients receiving TEE, the incidence of MVA has been reported to be only 0.2–0.29% in the past.3 There have been a few incidental case reports of tricuspid valve aneurysm in the literature.4 We present a case of mitral valve aneurysm and tricuspid aneurysm causing progressive dyspnea.
Case Presentation
A 56-year-old male presented to the cardiology outpatient with exertional dyspnea and fatigue. There was no history of medical condition, bad habits, or family history of cardiac disease. The patient maintained a healthy condition but had experienced exertional dyspnea and weakness for one week, not associated with fever or cough. He was vitally stable. On cardiac examination the patient had mild lower limb edema grade 1, NYHA class 1, no JVD, loud S2, and no additional murmur was noted on the examination. The basic blood tests of the patient were unremarkable. Twelve-lead EKG showed sinus rhythm and complete right bundle branch block. The basic blood tests including D-dimer and troponin I were normal. The transthoracic echocardiogram (TTE) showed normal systolic ejection fraction, normal left chamber size, and mitral valve aneurysm (Figure 1A and B) plus tricuspid septal valve aneurysm, tricuspid peak velocity 3 m/s, systolic pulmonary hypertension (SPAP) 45 mmHg, mild tricuspid regurgitation with eccentric jet, and normal right ventricular function parameters. Figure 2A and B.
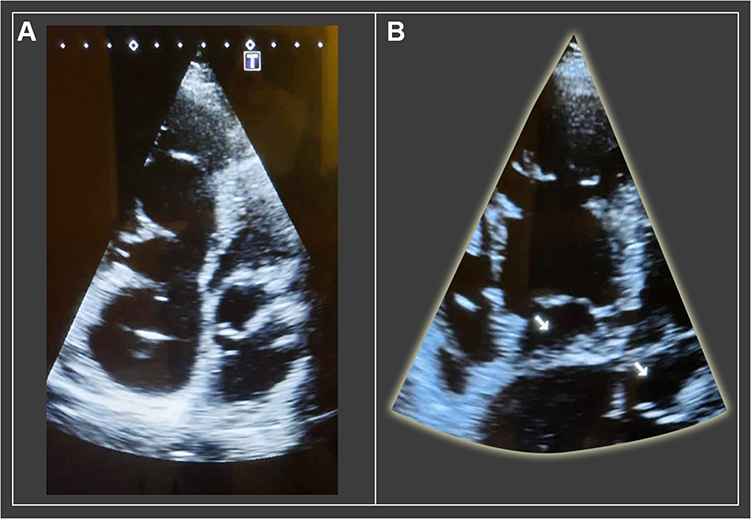 |
Figure 1 (A) Outpouching of mitral valve that is expanding during systole and collapsing during diastole. (B) Bilateral aneurysm of the mitral and tricuspid valve. |
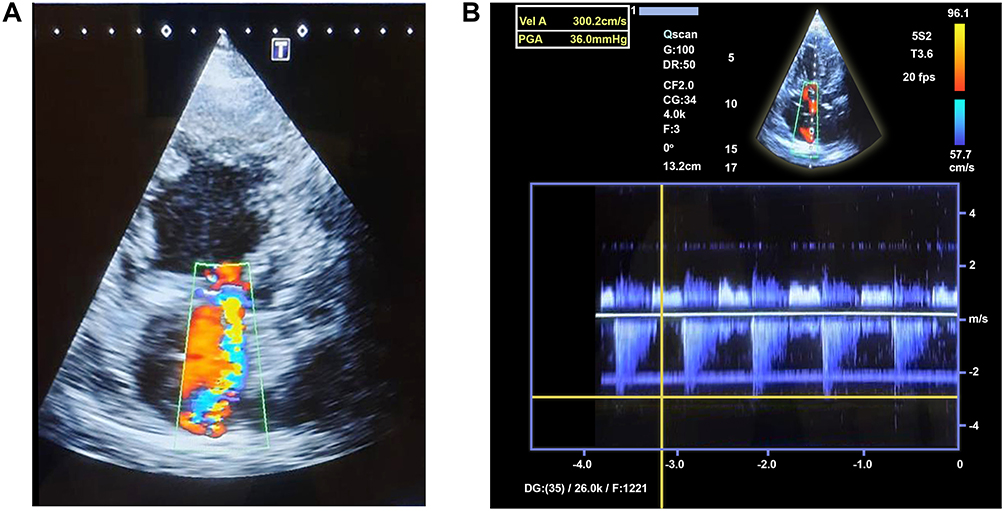 |
Figure 2 (A) Eccentric jet directed to the septal tricuspid leaflet. (B) TR velocity 3 cm/s and SPAP ≈45 mmHg. |
After evaluating the symptoms of the patient it was supposed that the clinical findings were due to pulmonary hypertension impacted by tricuspid valve aneurysm.
The patient was managed with a low dose of diuretic and a low dose of B-blocker as there were minimal symptoms, and further management, including imaging, was suggested at an advanced center.
Discussion
In patients undergoing TEE, the incidence of MVA has previously been reported to be 0.2–0.29%, with the posterior leaflet being much less frequently affected than the anterior leaflet. It is a typical symptom of infective endocarditis.3,5,6 Increased pressure from the left ventricle causes the leaflet to protrude into the left atrium. Degenerative changes brought on by age may be the underlying cause of leaflet failure and mitral valve aneurysm in the absence of any other cardiac or systemic disease.7 In our patient a specific etiology could not be identified. There are no symptoms or indicators particular to an aneurysm in MVA; instead, the clinical findings were similar to those in mitral regurgitation. The most dangerous MVA consequence, perforation, causes severe regurgitation. Microscopically, a single valve aneurysm that has the potential to burst is typically discovered; nevertheless, reports of numerous aneurysms have also been made.8 Even though TTE can occasionally detect minor valvular anomalies, TEE’s superior resolution allows for a more certain identification of these uncommon lesions. Flow-of-color Doppler shows a straight connection between the aneurysm and the left ventricle, separating the aneurysm from other anomalies. Regardless of how the mitral valve aneurysm forms, there is a substantial risk of life-threatening consequences such as valvular perforation.9,10
Aneurysms of the tricuspid valve have been previously reported in the literature less frequently. However, the regurgitant jet and transthoracic, two-dimensional appearance are the same as those mentioned in mitral valve aneurysm. Although the specific cause of a tricuspid leaflet aneurysm is unknown, it may be caused by a ruptured valve abscess that allows direct right ventricle communication with the cavity that receives the regurgitant flow.4 Our case study patient presented with growing dyspnea and fatigue, which were mostly triggered by atrioventricular valve aneurysms, but were complicated by tricuspid regurgitation and mildly elevated pulmonary arterial pressure. Because the patient exhibited right ventricular dilatation, pulmonary embolism was ruled out with a normal D-dimer titer because the patient had a low risk probability. Ultimately the patient was managed with a low dose of diuretic therapy and B-blocker, and further imaging was suggested.
Nevertheless, the current case describes a rare development of a mitral valve aneurysm and tricuspid valve aneurysm in an old patient without any underlying pathology that could be identified.
Conclusion
Incidental finding of atrioventricular aneurysm is unusual. This can be a cause of shortness of breath and progressive dyspnea. In the medical literature only few cases have been reported. In this case we present an unusual cause of dyspnea in an old patient.
Ethics Approval
Based on the regulations of the review board of the Mogadishu Somali Turkish Training and Research Hospital, institutional review board approval is not required for case reports.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
We declared that we have not received any financial support for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rückel A, Erbel R, Henkel B, Krämer G, Meyer J. Mitral valve aneurysm revealed by cross-sectional echocardiography in a patient with mitral valve prolapse. Int J Cardiol. 1984;6(5):633–637. doi:10.1016/0167-5273(84)90010-X
2. Mollod M, Felner KJ, Felner JM. Mitral and tricuspid valve aneurysms evaluated by transesophageal echocardiography. Am J Cardiol. 1997;79(9):1269–1272.
3. Vilacosta I, San Román JA, Sarriá C, et al. Clinical, anatomic, and echocardiographic characteristics of aneurysms of the mitral valve. Am J Cardiol. 1999;84(1):110–113.
4. Miga DE, Meyer KB, Fyfe DA. Tricuspid valve aneurysm formation in a child with suspected endocarditis. Echocardiography. 1996;13(1):99–102.
5. Işılak Z, Uzun M, Yalçın M, Kılıçaslan F. E-sayfa Özgün Görüntüler E-page original images E-25 an adult patient with the ruptured aneurysm of mitral valve posterior leaflet. Anadolu Kardiyol Derg. 2013;13:E25–9.
6. Reid CL, Chandraratna PA, Harrison E, et al. Mitral valve aneurysm: clinical features, echocardiographic-pathologic correlations. J Am Coll Cardiol. 1983;2(3):460–464.
7. Tariq M, Zahid I, Sami S. Rare aneurysm of anterior mitral valve leaflet-a case report. J Cardiothorac Surg. 2019;14(1):1–4.
8. Ryu YG, Baek MJ. Fibrous skeleton endocarditis causing septated aneurysm on the anterior mitral leaflet. Eur Heart J. 2010;31(9):1123.
9. Decroly PH, Vandenbossche JL, Englert M. Anterior mitral valve aneurysm perforation secondary to aortic valve endocarditis detected by Doppler colour flow mapping. Eur Heart J. 1989;10(2):186–189.
10. Behnam R, Bommer W. Fenestrated aneurysm of the mi- tral valve. Echocardiography. 1991;8:523–526.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.