Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 13
Randomized Study Comparing Vildagliptin vs Glibenclamide on Glucose Variability and Endothelial Function in Patients with Type 2 Diabetes Mellitus and Hypertension
Authors Cosenso-Martin LN ![]() , Takaoka LY, Vilela-Martin JF
, Takaoka LY, Vilela-Martin JF ![]()
Received 10 April 2020
Accepted for publication 29 July 2020
Published 15 September 2020 Volume 2020:13 Pages 3221—3229
DOI https://doi.org/10.2147/DMSO.S257096
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Muthuswamy Balasubramanyam
Luciana Neves Cosenso-Martin, Lais Yumi Takaoka, Jose Fernando Vilela-Martin
Internal Medicine Division, State Medical School at Sao Jose do Rio Preto (FAMERP), Hospital de Base, Sao Jose do Rio Preto, Sao Paulo, Brazil
Correspondence: Jose Fernando Vilela-Martin
State Medical School at Sao Jose do Rio Preto (FAMERP), Hospital de Base, Ave Brig. Faria Lima 5416, Sao Jose do Rio Preto, Sao Paulo 15090-000, Brazil
Tel +55 17 32015727
Email [email protected]
Background: Glucose variability (GV) is considered an important factor for cardiovascular disease (CVD) in patients with type 2 diabetes mellitus (T2DM). High GV causes endothelial dysfunction and increased oxidative stress. Dipeptidyl peptidase-4 (DPP-4) inhibitors may improve endothelial function and decrease GV. The aim of this study was to investigate the effects of vildagliptin, a DPP-4 inhibitor, compared with glibenclamide in GV and endothelial function in patients with T2DM and arterial hypertension.
Methods: This is a prospective, randomized, open and drug-controlled study. Fifty patients older than 35 years with T2DM and hypertension without CVD were randomized to receive vildagliptin (n=25) or glibenclamide (n=25), both in added-on metformin. Laboratory tests and analysis of endothelial function were performed before and 12 weeks after treatment. Endothelial function, defined by reactive hyperemia index (RHI), was analyzed by peripheral artery tonometry (endo-PAT2000). GV was evaluated by capillary glucose with intermittent monitoring device, six measurements per day, for three days, before and after treatment. The median of standard deviation (SD) of mean blood glucose (MBG) was used to evaluate GV.
Results: GV decreased in the vildagliptin group (35.2 to 30.7, P=0.037) but did not change with glibenclamide (37.6 to 37.5, P=0.765). Glycated hemoglobin was similar in both groups. MBG decreased only in glibenclamide group, without difference with vildagliptin group (P=0.374). There were no changes in the RHI in both groups and there was no correlation between GV and RHI (P=0.658).
Conclusion: Vildagliptin reduces GV; however, the action on endothelial function was not demonstrated. In addition, there was no correlation between GV and endothelial function.
Keywords: type 2 diabetes, hypertension, glycemic variability, vascular endothelium, dipeptidyl-peptidase IV inhibitors, arterial stiffness
Background
Cardiovascular disease (CVD) is the leading cause of death globally, including developing and developed countries, and claiming an estimated 17.9 million lives each year.1 Identifying the main risk factors involved in the development of CVD is extremely important to ensure appropriate treatment and prevent premature deaths. Thus, among the several risk factors, type 2 diabetes mellitus (T2DM) and hypertension represent the main etiologies of CVD. Studies suggest that patients with both hypertension and T2DM have increased arterial stiffness, showing that these diseases together have an increment of CVD outcomes.2
With endothelial dysfunction in T2DM, vascular dyshomeostasis occurs leading to excessive production of reactive oxygen species and platelet aggregation and decrease in the production of nitric oxide. These events can increase the chances of development of CVD, doubling or even quadrupling the probability of cardiovascular outcomes. Hyperglycemia increases the formation of advanced glycation end products (AGEs), and it is implicated in vascular damage and increased chances of CVD events.3,4
Some studies have shown that, in addition to prolonged hyperglycemia, large fluctuations in blood glucose levels also have a role in CVD development. Glucose variability (GV) expresses the daily variation in glucose, involving postprandial blood glucose raising and hypoglycemic peaks. High GV also can lead to oxidative stress and its vascular damage consequences, which can be worse than prolonged hyperglycemia according to some research studies, even though this relation is controversial.5–7 Various methods of GV calculation have been used as parameters, such as standard deviation (SD), mean amplitude of glycemic excursions (MAGE), coefficient of variation (CV) and continuous overlapping net glycemic action (CONGA).7,8
As the treatment of diabetes may provoke some complications like hypoglycemia and GV, the clinical management of T2DM involves not only lowering glycated hemoglobin (HbA1c) levels, but also controlling GV.9 Nowadays, dipeptidyl dipeptidase-4 (DPP-4) inhibitors are drugs that improve the action of endogenous incretin, such as glucagon-like peptide-1 (GLP-1), with increased insulin secretion and reduced glucagon secretion, both in a glucose dependent manner. Vildagliptin, a DPP-4 inhibitor, was effective in reducing GV in T2DM women in a similar way to gliclazide.10 In addition, it was demonstrated that infusion of GLP-1 receptor agonists and improvement in daily glucose fluctuation were associated with decreased oxidative stress.9
DPP-4 inhibitors may reduce cardiovascular complications.11,12 According to a previous study, vildagliptin and glibenclamide similarly have no effect on endothelial function and arterial stiffness in diabetic and hypertensive patients without cardiovascular events.13 Moreover, three large multicenter trials testing saxagliptin, alogliptin and sitagliptin failed to demonstrate benefits of the DPP-4 inhibitors on the cardiovascular system.14–16
Thus, the purpose of this study was to evaluate the effects of vildagliptin compared to glibenclamide on GV, and consequent improvement on the vascular function, which are markers of CVD.
Research Design and Methods
Study Design
This was a randomized open-label trial described previously.17 This study was registered in clinicaltrials.gov (identifier: NCT02145611). The aim of the research was to evaluate the action of vildagliptin on GV and endothelial function in patients with T2DM and hypertension compared to glibenclamide. The metformin and glibenclamide doses were adjusted according to glycemic control assessed by fasting blood glucose sample three weeks after randomization.
Study Population
Between July 2013 and February 2016, 50 patients from the regional reference Diabetes and Hypertension Outpatient Clinic of a governmental institution participated in this study. The project was approved by the Ethics Committee of the State Medical School at Sao Jose do Rio Preto (CAAE no. 11665513.7.0000.5415, no. 211.243–03/12/2013). The patients accepted to participate in this trial with the informed consent, which is in line with the 1975 Declaration of Helsinki.
The inclusion and exclusion criteria were described previously.17 The inclusion criteria are briefly described in this paper: history of T2DM and mild hypertension for no longer than 15 years, age ≥35 years, HbA1c from 7.0–10.5% (53–91 mmol/mol) and body mass index (BMI) <35 kg/m2. Clinical history of CVD or cerebrovascular disease, smoking, resistant hypertension, and insulin use were the main exclusion criteria. CVD was defined by clinical history and altered treadmill stress test, or myocardial scintigraphy and coronary angiography when necessary.
Randomization and Study Intervention
A computer-validated software (random allocator) was used for random allocation of participants to use vildagliptin or glibenclamide. The study period lasted for 12 weeks after randomization. Clinical outcome, adherence, and adverse events were confirmed. Clinical and biochemical data were evaluated at baseline and at the final visit.
Study Outcomes
The aim of this study was to evaluate GV changes after 12 weeks of treatment with vildagliptin vs glibenclamide and the correlation with endothelial function, according to treatment performed.
Measurement of Endothelial Function
Peripheral arterial tonometry (PAT) tests were performed using an Endo-PAT 2000 device (Itamar Medical Ltd, Caesarea, Israel) following the manufacturer’s guidelines and was described previously.17 This device calculates reactive hyperemia index (RHI) by measuring the volume changes in the fingertip after five minutes of blood flow occlusion. Furthermore, it assesses arterial stiffness by calculating the augmentation index corrected for heart rate of 75 bpm (AIx75).
Biochemical Tests
As described previously,17 blood samples were drawn after 12 h of fasting to measure total cholesterol (TC), high-density lipoprotein cholesterol (HDLc), triglycerides (TG), glycemia, serum creatinine, and alanine aminotransferase. All the tests were determined by electrochemiluminescence method using a COBAS C 501 device with the Roche reagent. LDL-cholesterol (LDLc) fraction was calculated by the Friedewald formula [LDLc=TC−HDLc−TG/5 (for TG <400 mg/dL)]. In addition, the glomerular filtration rate (GFR) was estimated using the modification of diet in renal disease (MDRD) formula and microalbuminuria was performed by the urinary-to-creatinine ratio obtained from urine samples collected in the morning (COBAS C 501 device with the Roche reagent). HbA1c was measured with high-performance liquid chromatography method using the Premier HB 9210 device. Biochemical tests were evaluated before and after 12 weeks of treatment.
Glycemic Variability
Self-monitoring of blood glucose is considered an important adjunct to HbA1c as it can demonstrate fasting, preprandial, and postprandial hyperglycemia, assessing glycemic excursions, and documenting hypoglycemic events. Thus, all subjects were provided with a blood glucose meter (Accu-Chek Performa, Roche Diagnostics, Indianapolis, IN, USA) and glucose monitoring strips for the study period. Patients were trained in the use of a glucose meter. GV was evaluated using capillary glucose values performed by a blood glucose meter device with intermittent monitoring, with six measurements per day during three days at baseline and at the end of treatment. Schedules of measures: fasting, two hours after breakfast, before lunch, two hours after lunch, before dinner, two hours after dinner. The method chosen for the calculation of glycemic variability was the median of the SD of mean blood glucose (MBG) of capillary glucose mensuration.
According to a GV evaluation study, it was established that GV must be <50 mg/dL18,19 or a maximum of one third of MBG. These studies also sustain that good glycemic control criteria include MBG <150 mg/dL and keeping blood glucose between 70 and 180 mg/dL.18,19 In this study, we used a GV (SD) <40 mg/dL, MBG <150 mg/dL and MBG range of 70–180 mg/dL as parameters of good glycemic control.
Statistical Analysis
The sample size was estimated using the site http://www.lee.dante.br/pesquisa, considering a 30% change in the RHI, and a standard deviation of 0.3. A total of 21 subjects would be required to detect a 30% change in the RHI with a power of 80% at a significance level of <5%. However, considering a potential 20% dropout or lost to follow-up rate, a total of 50 patients (25 for each group) were enrolled, initially.17 All analyses were performed using SPSS Software (IBM SPSS Statistics, Version 24, IBM Corporation, NY, USA). Continuous variables are presented as mean ±SD and categorical variables as frequencies. The normal distribution of continuous variables was analyzed by skewness, kurtosis and Kolmogorov–Smirnov test. Differences between both groups at baseline were evaluated using the unpaired t-test or the Mann–Whitney test for continuous variables. The chi-squared test or Fisher’s exact test was employed to compare categorical variables. Changes from baseline to 12 weeks of follow-up in both groups were evaluated using the paired t-test for continuous variables. Pearson’s correlation analysis was performed to assess the relationship between HbA1c level with RHI and AIx75 after confirming the similarity between groups. Spearman correlation was performed to calculate the correlation of GV with HbA1c, lipid parameters, microalbuminuria, GFR, and arterial stiffness. Wilcoxon signed-rank test was used to assess changes in GV between related groups (before and after 12 weeks of treatment). Comparative GV analysis of the patients’ proportion with SD <40 mg/dL and ≥40 mg/dL before and after treatment was evaluated using McNemar's test. All statistical tests were considered significant at an alpha error of 5% (P<0.05).
Results
Clinical and Biochemical Parameters
A total of 148 participants were invited to participate in this trial, 50 met the criteria for inclusion and were randomly assigned to the present study, as described in a previous study.13 According to previous publication, no differences were described between the groups with respect to age, duration of T2DM or hypertension, office BP level, body mass index (BMI), HbA1c level, eGFR, lipid parameters, and microalbuminuria (Table 1).
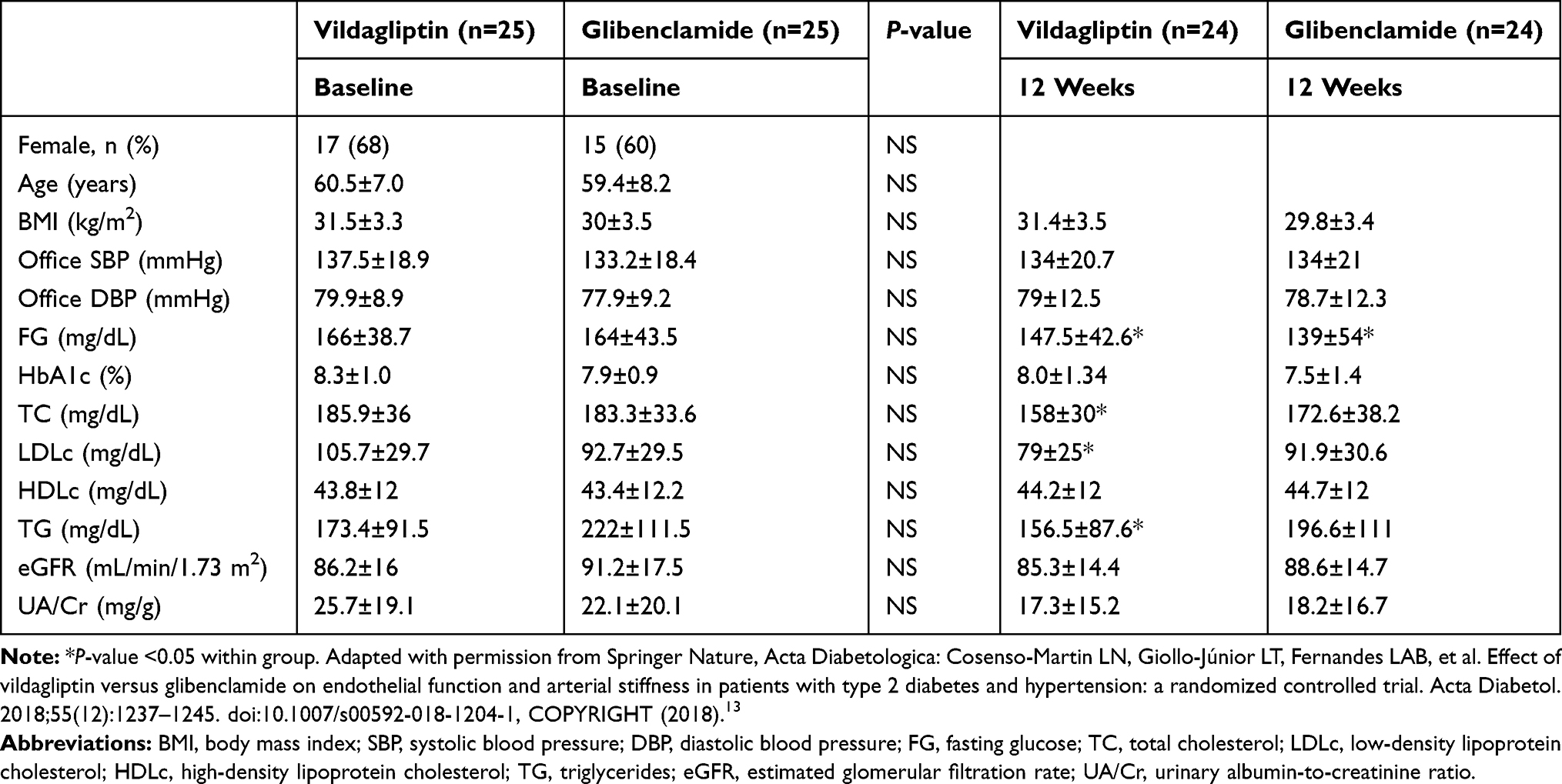 |
Table 1 Clinical and Biochemical Profile at Baseline and After 12 Weeks of Treatment in Vildagliptin and Glibenclamide Groups |
Glycemic Variability
MBG comparative analysis shows that the means of glibenclamide and vildagliptin groups at baseline presented no statistically significant difference (P=0.704). Furthermore, comparing the two groups before and after treatment, there were no differences (P=0.374). However, it was observed that only the glibenclamide group had a statistically significant decrease of MBG (P=0.029) (Table 2). Considering the whole group, the percentage of patients with MBG <150 mg/dL improved from 34.7% to 55.6% (P=0.039). But this improvement was not observed when the groups were separately analyzed (Table 3).
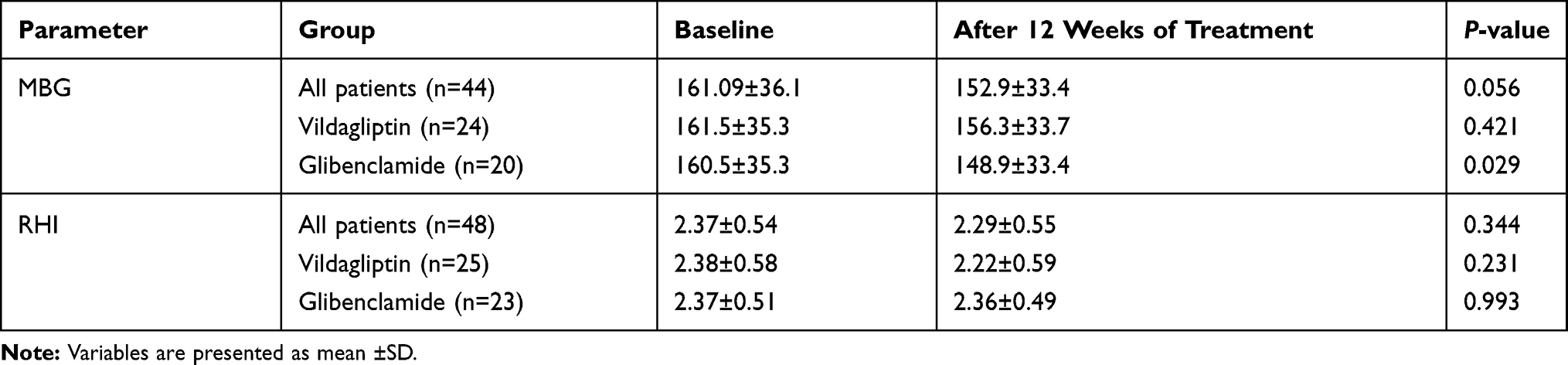 |
Table 2 Parameters of Mean Blood Glucose (MBG), Reactive Hyperemia Index (RHI) in Vildalgliptin and Glibenclamide Groups at Baseline and After 12 Weeks of Treatment |
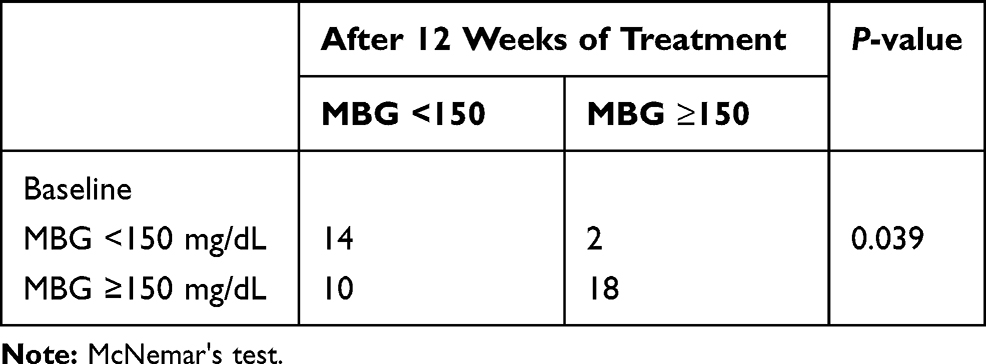 |
Table 3 Proportion of Patients with Mean Blood Glucose Below (MBG) <150 mg/dL at Baseline and After 12 Weeks of Treatment, Whole Group |
The GV analyses from the whole group demonstrated no statistically significant difference between the visits (P=0.208). However, analysis of GV considering separated groups showed a significant decrease only in the vildagliptin group (P=0.037) (Table 4). There was no correlation of the GV with lipid parameters (TC, HDLc, LDLc, and TG), eGFR, fasting glucose and microalbuminuria after treatment.
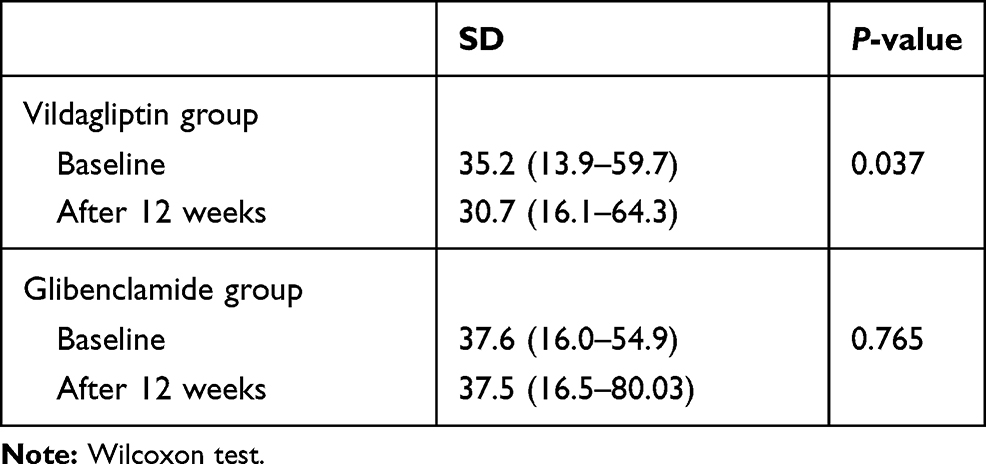 |
Table 4 Glycemic Variability Evaluated by Median of Standard Deviation (SD) of Mean Blood Glucose Between Baseline and After 12 Weeks, Separated by Drug Groups |
The proportion of patients with SD <40 mg/dL and SD ≥40 mg/dL before and after drug treatment was calculated. Applying McNemar's test and considering SD <40 mg/dL as an adequate result for GV, a GV decrease after treatment was observed (P=0.031). However, this difference was demonstrated only in the vildagliptin group (P=0.041) (Table 5).
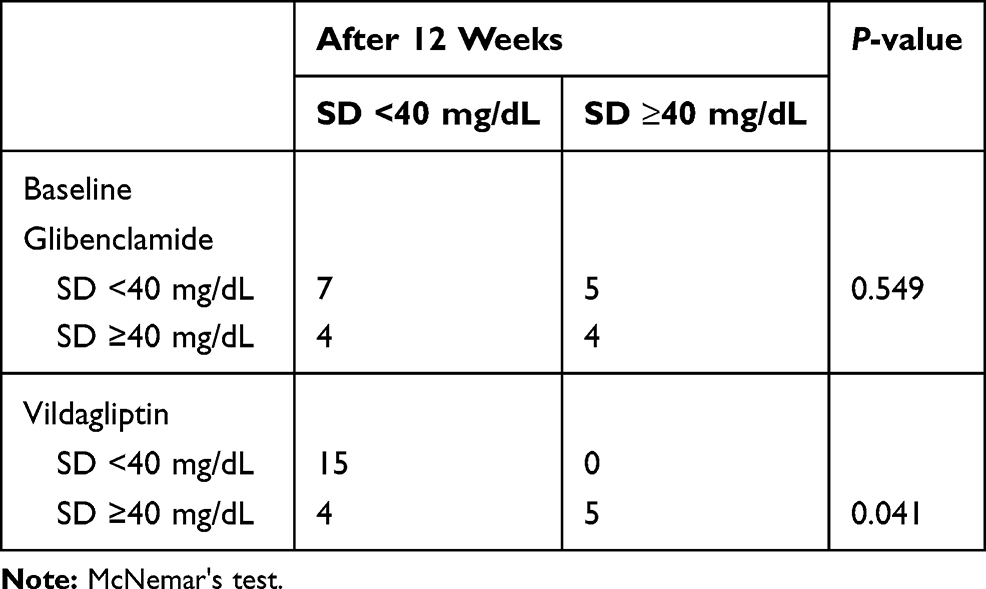 |
Table 5 Comparative Analysis Between the Proportion of Patients of Median of Standard Deviation (SD) <40 mg/dL or ≥40 mg/dL Between Baseline and After 12 Weeks of Treatment in the Glibenclamide and Vildagliptin Groups |
Endothelial Function (RHI) and Arterial Stiffness (A1x75 PAT)
The RHI was not different between the groups at baseline and did not change in the whole group or between them after treatment. In addition, there was no correlation between MBG and GV with RHI for the whole group or for separated groups (Table 2). Furthermore, the correlation of MBG and GV with arterial stiffness (A1x75 PAT) in the whole group or in the separated drug group was not observed, P>0.05.
Glycated Hemoglobin (HbA1c)
Analysis of the correlation between MBG and HBA1c from the whole group and in separated groups was positive at baseline and after treatment (P=<0.05). Similarly, the correlation of GV with HbA1c was present at the whole group (P=0.014). However, the separated analysis demonstrated the statistically difference only at the glibenclamide group (P=0.002). For the vildagliptin group, there was no statistically significant difference.
Discussion
This randomized, open-label, prospective study compared the effects of vildagliptin and glibenclamide added-on to metformin on GV and vascular function in hypertensive diabetic patients without CVD. Although the MBG decreased only in the glibenclamide group, this difference was not observed comparing the two groups after treatment. In addition, GV decreased only in the vildagliptin group. Similarly, a previous study demonstrated that vildagliptin compared to gliclazide reduced similarly GV on T2DM women, but only vildagliptin significantly decreased the SD of the mean glucose and the mean of the daily differences (MODD).10 The cited study strengthens the outcomes of the present study in GV. Considering that high GV can cause oxidative stress and vascular damage, both trials demonstrate that vildagliptin might be an antidiabetic drug effective in decreasing CVD. However, there are some differences between the methodologies used: period of treatment (24 weeks), gender (only women), use of continuous glucose monitoring (CGM) and other GV parameters besides SD (MAGE, CV, CONGA, MODD).
When GV, DPP-4 inhibitors, and GLP-1 receptor agonists were evaluated, a controversy occured, mainly when endothelial function is also studied. Thus, no change on GV was observed after 30 min of aerobic exercise in patients on treatment with vildagliptin or glibenclamide.20 However, the systolic blood pressure (SBP) decreased with both drugs, and the variability of SBP was lower in the vildagliptin group, showing the vascular effect of the vildagliptin.20 However, the present study demonstrated that vildagliptin decreased GV associated with lack of effect on endothelial function, as described previously.21 Therefore, with a distinguished methodology, using CGM, which is more expensive, and assessing endothelial function by flow mediated dilatation (FMD), both trials failed to demonstrate that vildagliptin acts on endothelial function in patients treated for 12 weeks. In addition, comparing two GLP-1 receptor agonists, dulaglutide was better in reducing GV after 24 weeks of treatment.22 In contrast, there were no differences in oxidative stress and endothelial function, which was assessed by RHI index,22 the same device used in the present study.
Furthermore, considering the effect of DPP-4 inhibitors or GLP-1 receptor agonists on endothelial function alone, the controversy remains, since there are several devices to measure the endothelial function. Although the present study demonstrated no effect on endothelial function as assessed by Endo-PAT 2000, a previous study showed an improvement in vascular function with vildagliptin.23 The different methodologies used in both research studies might explain the controversial results found. In addition, the current study evaluated endothelial function before and after treatment, and not only after treatment as previously demonstrated.23 Endo-PAT 2000 has been validated as a noninvasive measurement of endothelial function with adequate results.24 Similarly to our study, PAT was also used in a trial with liraglutide, a GLP-1 analogu, and had no significant effect on vascular function.25 However, other researchers demonstrated effects on endothelial function: a direct effect of GLP-1 analogu, measured by FMD of the brachial artery,26 an antioxidant response of cell culture treated with teneligliptin, a DPP-4 inhibitor, with improvement in the endothelial function27 and endothelium-dependent relaxation of the aorta from mice with T2DM treated with linagliptin, a DPP-4 inhibitor.28 Therefore, the conflicting results about the DPP-4 inhibitors and endothelial function might be explained by the different methodologies used, the type of study (clinical, experimental, or randomized) and the size of the study population.
The lack of endothelial action of the present study is based on the recent large clinical trials that showed that DPP-4 inhibitors have a neutral effect on CVD outcomes.14–16 Recently, CARMELINA study showed that linagliptin has no inferiority compared to placebo in CVD outcomes.29 These clinical trial results reinforce our results that DPP-4 inhibitors improve glycemic control, but no effect was observed on CVD outcome. Thus, DPP-4 inhibitors have no vascular effects.
The relationship between GV and diabetic complications has been identified in T2DM30,31 and in type 1 diabetes.32 A T2DM cohort study demonstrated correlation of GV, defined by fasting glucose and HbA1c, with micro and macrovascular complications of diabetes.30 In addition, a meta-analysis reported that variability of HbA1c was associated with both microvascular and macrovascular complications and mortality.31 In type 1 diabetes, GV (assessed by CGM) was associated with cardiovascular autonomic neuropathy.32 Furthermore, improvements in MBG and GV were correlated with decrease in oxidative stress after 24 weeks of treatment.9 In contrast with a previous study that showed association among plasma glucose, glycated hemoglobin and glycated albumin with pulse wave velocity,33 the correlation of the GV, MBG and the HbA1c with parameters of vascular function was not found in our study. Thus, as demonstrated previously, the treatment of blood pressure with renin–angiotensin system (RAS) blockers was made in all the patients and this might explain the neutral effect of DPP-4 inhibitor observed on the endothelial function,13 according to a previous report which showed protective action by sitagliptin against oxidative stress only in rats not treated with RAS blockers.34 In addition, the small size of subjects in the present study is also a limitation to be considered. As anteriorly described by our team, both groups demonstrated improvements in the 24-h systolic and diastolic blood pressure, measured by ambulatory blood pressure monitoring. However, the office blood pressure was unchanged.13
The relationship between HbA1c level and GV is questioned. While in some studies the level of HbA1c was not related to GV in patients with well or poorly controlled diabetes,35 GV was associated with HbA1c in others.6 The present study demonstrated association between GV and HbA1c only at the glibenclamide group. As the GV evaluated by the SD was associated with the risk of hypoglycemia in T2DM,6 hypoglycemia might occur with glibenclamide, in contrast to vildagliptin, which protects the patient from this adverse effect.
In summary, vildagliptin significantly decreased GV in comparison to glibenclamide. This parameter is important to fix the advantage of this drug to prevent microvascular and macrovascular complications. The lack of correlation between GV and endothelial function might be explained by the methodology used in the present study, although the device was a noninvasive and validated method.
This study has limitations to be considered. Patients were followed-up for a short period of time and a small population size was studied, although with statistical power. Another potential limitation was the evaluation of the GV by self-monitoring of blood glucose capillary with intermittent monitoring device.
The strengths of this study must be reported. This was a prospective, randomized study, open label, compared by drug. Unlike other studies that assessed GV and endothelial function, eligibility criteria included noninsulin-dependent type 2 diabetic and controlled hypertensive patients, including non-smoking patients. The individuals were CVD-free, including coronary artery disease, stroke and peripheral arterial disease. The exclusion of CAD included clinical history and imaging exams (exercise test, myocardial scintigraphy or arteriography). All the patients were taking RAS blockers and approximately 70% were using lipid-lowering drugs, according to what was described in a previous publication.13 In addition, this research used the capillary glucose monitoring, which is a cheap and easy method to evaluate the GV, and a noninvasive and validated method to assess the endothelial function. Moreover, the two groups presented baseline homogeneous characterization.
Conclusions
Vildagliptin reduces GV, which may decrease endothelial dysfunction risk. Glibenclamide does not reduce GV. Both vascular parameters are not altered after treatment with vildagliptin or glibenclamide. In addition, there is no correlation between GV and endothelial function. More studies are necessary to investigate if DPP-4 inhibitors have an effect on cardiovascular outcomes.
Abbreviations
AGEs, advanced glycation end products; AIx75, augmentation index corrected for heart rate of 75 bpm; BMI, body mass index; BP, blood pressure; CONGA, continuous overlapping net glycemic action; CGM, continuous glucose monitoring; CV, coefficient of variation; CVD, cardiovascular disease; DBP, diastolic blood pressure; DPP-4, dipeptidyl peptidase-4; eGFR, estimated glomerular filtration rate; FG, fasting glucose; FMD, flow mediated dilatation; GV, glycemic variability; HbA1c, glycated hemoglobin; HDLc, high-density lipoprotein cholesterol; LDLc, low-density lipoprotein cholesterol; MAGE, mean amplitude of glycemic excursions; MBG, mean blood glucose; MDRD, modification of diet in renal disease; MODD, mean of the daily differences; PAT, peripheral arterial tonometry; RAS, renin-angiotensin system; RHI, reactive hyperemia index; SBP, systolic blood pressure; SD, standard deviation; TC, total cholesterol; TG, triglycerides; T2DM, type 2 diabetes mellitus; UA/Cr, urinary albumin-to-creatinine ratio.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request. The data intended for sharing will be deidentified.
Compliance with Ethical Standards
The study protocol (no. 11665513.7.00005415) was approved by the Research Ethics Committee of State Medical School at Sao Jose do Rio Preto (FAMERP) and the study was conducted in accordance with the principles of the Declaration of Helsinki. The research was registered in clinicaltrials.gov (identifier: NCT02145611).
Informed Consent
Written, informed consent was obtained from all participants being included in the study prior to the start.
Disclosure
The abstract of this paper was presented at 101st Annual Meeting of the Endocrine (The ENDO 2019) as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in the Journal of the Endocrine Society 2019;3(Sup 1): SAT-141. DOI: https://doi.10.1210/js.2019-SAT-141. Lais Yumi Takaoka reports grants from Brazilian National Council for Scientific and Technological Development (CNPq), during the conduct of the study. The authors report no other potential conflicts of interest for this work.
References
1. Lennon RP, Claussen KA, Kuersteiner KA. State of the heart: an overview of the disease burden of cardiovascular disease from an epidemiologic perspective. Prim Care. 2018;45(1):1–15. doi:10.1016/j.pop.2017.11.001
2. Smulyan H, Lieber A, Safar ME. Hypertension, diabetes type II, and their association: role of arterial stiffness. Am J Hypertens. 2016;29(1):5–13. doi:10.1093/ajh/hpv107
3. Kibel A, Selthofer-Relatic K, Drenjancevic I, et al. Coronary microvascular dysfunction in diabetes mellitus. J Int Med Res. 2017;45(6):1901–1929. doi:10.1177/0300060516675504
4. Shi Y, Vanhoutte PM. Macro- and microvascular endothelial dysfunction in diabetes. J Diabetes. 2017;9(5):434–449. doi:10.1111/1753-0407.12521
5. Jangam SR, Hayter G, Dunn TC. Individuals with type 1 and type 2 diabetes mellitus trade increased hyperglycemia for decreased hypoglycemia when glycemic variability is not improved. Diabetes Ther. 2018;9(1):395–402. doi:10.1007/s13300-017-0340-x
6. Luo J, Qu Y, Zhang Q, Chang AM, Jacober SJ. Relationship of glucose variability with glycated hemoglobin and daily mean glucose: a post hoc analysis of data from 5 Phase 3 studies. J Diabetes Sci Technol. 2018;12(2):325–332. doi:10.1177/1932296817736315
7. Nusca A, Tuccinardi D, Albano M, et al. Glycemic variability in the development of cardiovascular complications in diabetes. Diabetes Metab Res Rev. 2018;34(8):e3047. doi:10.1002/dmrr.3047
8. Gómez AM, Muñoz OM, Marin A, et al. Different indexes of glycemic variability as identifiers of patients with risk of hypoglycemia in type 2 diabetes mellitus. J Diabetes Sci Technol. 2018;12(5):1007–1015. doi:10.1177/1932296818758105
9. Ohara M, Nagaike H, Goto S, et al. Improvements of ambient hyperglycemia and glycemic variability are associated with reduction in oxidative stress for patients with type 2 diabetes. Diabetes Res Clin Pract. 2018;139:253–261. doi:10.1016/j.diabres.2018.02.017
10. Vianna AGD, Lacerda CS, Pechmann LM, Polesel MG, Marino EC, Faria-Neto JR. A randomized controlled trial to compare the effects of sulphonylurea gliclazide MR (modified release) and the DPP-4 inhibitor vildagliptin on glycemic variability and control measured by continuous glucose monitoring (CGM) in Brazilian women with type 2 diabetes. Diabetes Res Clin Pract. 2018;139:357–365. doi:10.1016/j.diabres.2018.03.035
11. Scheen AJ. Cardiovascular effects of new oral glucose-lowering agents: DPP-4 and SGLT-2 inhibitors. Circ Res. 2018;122(10):1439–1459. doi:10.1161/CIRCRESAHA.117.311588
12. Xie W, Song X, Liu Z. Impact of dipeptidyl-peptidase 4 inhibitors on cardiovascular diseases. Vascul Pharmacol. 2018;109:17–26. doi:10.1016/j.vph.2018.05.010
13. Cosenso-Martin LN, Giollo-Júnior LT, Fernandes LAB, et al. Effect of vildagliptin versus glibenclamide on endothelial function and arterial stiffness in patients with type 2 diabetes and hypertension: a randomized controlled trial. Acta Diabetol. 2018;55(12):1237–1245. doi:10.1007/s00592-018-1204-1
14. Scirica BM, Bhatt DL, E B, et al.; SAVOR-TIMI 53 Steering Committee and Investigators. Saxagliptin and cardiovascular outcomes in patients with type 2 diabetes mellitus. N Engl J Med. 2013;369(14):1317–1326. doi:10.1056/NEJMoa1307684
15. White WB, Cannon CP, Heller SR, et al.; EXAMINE Investigators. Alogliptin after Acute Coronary Syndrome in Patients with Type 2 Diabetes. N Engl J Med. 2013;369(14):1327–1335. doi:10.1056/NEJMoa1305889
16. Green JB, Bethel MA, Armstrong PW, et al.; TECOS Study Group. Effect of sitagliptin on cardiovascular outcomes in type 2 diabetes. N Engl J Med. 2015;373(3):232–242. doi:10.1056/NEJMoa1501352
17. Cosenso-Martin LN, Giollo-Junior LT, Martinelli DD, et al. Twelve-week randomized study to compare the effect of vildagliptin vs. glibenclamide both added-on to metformin on endothelium function in patients with type 2 diabetes and hypertension. Diabetol Metab Syndr. 2015;7:70. doi:10.1186/s13098-015-0062-z
18. Pimazoni-Netto A, Rodbard D, Zanella MT; Diabetes Education and Control Group. Rapid improvement of glycemic control in type 2 diabetes using weekly intensive multifactorial interventions: structured glucose monitoring, patient education, and adjustment of therapy - a randomized controlled trial. Diabetes Technol Ther. 2011;13(10):997–1004. doi:10.1089/dia.2011.0054
19. Brazilian Diabetes Society Guidelines: 2019–2020 [homepage on the Internet]. Sao Paulo: Clannad. Sociedade Brasileira de Diabetes; 2019. Available from: https://www.diabetes.org.br/profissionais/images/DIRETRIZES-COMPLETA-2019-2020.pdf.
20. Fofonka A, Bock PM, Casali KR, et al. Impact of treatment with glibenclamide or vildagliptin on glucose variability after aerobic exercise in type 2 diabetes: a randomized controlled trial. Diabetes Res Clin Pract. 2018;143:184–193. doi:10.1016/j.diabres.2018.07.007
21. Kim G, Oh S, Jin SM, et al. Safety of adding either vildagliptin or glimepiride to ongoing metformin therapy in patients with type 2 diabetes mellitus. Expert Opin Pharmacother. 2017;18(12):1179–1186. doi:10.1080/14656566.2017.1353080
22. Nagaike H, Ohara M, Kohata Y, et al. Effect of dulaglutide versus liraglutide on glucose variability, oxidative stress, and endothelial function in type 2 diabetes: a prospective study. Diabetes Ther. 2019;10(1):215–228. doi:10.1007/s13300-018-0560-8
23. van Poppel PC, Netea MG, Smits P, Tack CJ. Vildagliptin improves endothelium- dependent vasodilatation in type 2 diabetes. Diabetes Care. 2011;34(9):2072–2077. doi:10.2337/dc10-2421
24. Bonetti PO, Pumper GM, Higano ST, Jr DR H, Kuvin JT, Lerman A. Noninvasive identification of patients with early coronary atherosclerosis by assessment of digital reactive hyperemia. J Am Coll Cardiol. 2004;44(11):2137–2141. doi:10.1016/j.jacc.2004.08.062
25. Faber R, Zander M, Pena A, Michelsen MM, Mygind ND, Prescott E. Effect of glucagon-like peptide-1 analogue liraglutide on coronary microvascular function in patients with type 2 diabetes – a randomized, single-blinded, cross-over pilot study. Cardiovasc Diabetol. 2015;14:41. doi:10.1186/s12933-015-0206-3
26. Ceriello A, Novials A, Canivell S, et al. Simultaneous GLP-1 and insulin administration acutely enhances their vasodilatory, antiinflammatory, and antioxidant action in type 2 diabetes. Diabetes Care. 2014;37(7):1938–1943. doi:10.2337/dc13-2618
27. Pujadas G, De Nigris V, Prattichizzo F, La Sala L, Testa R, Ceriello A. The dipeptidyl peptidase-4 (DPP-4) inhibitor teneligliptin functions as antioxidant on human endothelial cells exposed to chronic hyperglycemia and metabolic high-glucose memory. Endocrine. 2017;56(3):509–520. doi:10.1007/s12020-016-1052-0
28. Woodman OL, Ortega JM, Hart JL, Klein T, Potocnik S. Influence of type-4 dipeptidyl peptidase inhibition on endothelium-dependent relaxation of aortae from a db/db mouse model of type 2 diabetes: a comparison with the effect of glimepiride. Diabetes Metab Syndr Obes. 2019;12:1449–1458. doi:10.2147/DMSO.S215086
29. Rosenstock J, Perkovic V, Johansen OE, et al.; CARMELINA Investigators. Effect of linagliptin vs placebo on major cardiovascular events in adults with type 2 diabetes and high cardiovascular and renal risk: the CARMELINA randomized clinical trial. JAMA. 2019;321(1):69–79. doi:10.1001/jama.2018.18269
30. Cardoso CRL, Leite NC, Moram CBM, Salles GM. Long-term visit-to-visit glycemic variability as predictor of micro- and macrovascular complications in patients with type 2 diabetes: the Rio de Janeiro type 2 diabetes cohort study. Cardiovasc Diabetol. 2018;17(1):33. doi:10.1186/s12933-018-0677-0
31. Gorst C, Kwok CS, Aslam S, et al. Long-term glycemic variability and risk of adverse outcomes: a systematic review and meta-analysis. Diabetes Care. 2015;38(12):2354–2369. doi:10.2337/dc15-1188
32. Jun JE, Lee SE, Lee YB, et al. Continuous glucose monitoring defined glucose variability is associated with cardiovascular autonomic neuropathy in type 1 diabetes. Diabetes Metab Res Rev. 2019;35(2):e3092. doi:10.1002/dmrr.3092
33. Wen J, Hu F, Yang Q. Comparison of hemoglobin alc, glycated albumin and fasting plasma glucose for prediction of arterial stiffness in chinese adults. Diabetes Metab Syndr Obes. 2020;13:65–70. doi:10.2147/DMSO.S230435
34. Alam MA, Chowdhury MRH, Jain P, Sagor MAT, Reza HM. DPP-4 inhibitor sitagliptin prevents inflammation and oxidative stress of heart and kidney in two kidney and one clip (2K1C) rats. Diabetol Metab Syndr. 2015;7:107. doi:10.1186/s13098-015-0095-3
35. Borkowska A, Szymanska-Garbacz E, Kwiecinska E, Ignaczak A, Czupryniak L. Glucose variability and glycated hemoglobin HbA1c in type 1 and type 2 diabetes. Clin Diabetol. 2017;6(2):48–56. doi:10.5603/DK.2017.0009
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.