Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Ramadan and Diabetes: What About Non-Fasting Patients with Diabetes?
Authors Motaib I ![]() , Rhmari Tlemçani FZ
, Rhmari Tlemçani FZ ![]() , Khalis M
, Khalis M ![]() , Laidi S, Elamari S
, Laidi S, Elamari S ![]() , Chadli A
, Chadli A
Received 17 December 2021
Accepted for publication 17 March 2022
Published 28 June 2022 Volume 2022:15 Pages 1975—1983
DOI https://doi.org/10.2147/DMSO.S354627
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ming-Hui Zou
Imane Motaib,1 Fatima-Zahra Rhmari Tlemçani,1 Mohamed Khalis,2 Soukaina Laidi,1 Saloua Elamari,1 Asma Chadli1
1Department of Endocrinology, Diabetology, Metabolic Disease, and Nutrition, Cheikh Khalifa International University Hospital, Faculty of Medicine, Mohammed VI University of Health Sciences (UM6SS), Casablanca, Morocco; 2International School of Public Health, Mohammed VI University of Health Sciences (UM6SS), Casablanca, Morocco
Correspondence: Imane Motaib, Faculty of Medicine, Mohammed VI University of Health Sciences (UM6SS), Casablanca, 82403, Morocco, Email [email protected]; [email protected]
Background: The management of diabetes during Ramadan is well codified. International guidelines recommend avoiding fasting for patients with the risk of complications. However, during Ramadan drastic changes occur in lifestyles habits. Our study aims to evaluate the impact of the month of Ramadan on the lifestyle habits and metabolic profile of non-fasting patients with diabetes.
Patients and Methods: This observational cross-sectional study was carried out during 3 months of Ramadan in 2018, Ramadan 2019, and Ramadan 2021. We conducted 3 consultations (before, during, and after Ramadan). Before Ramadan, we collected anthropometric and metabolic parameters, and we assessed physical activity level and dietary intake. During Ramadan, we evaluated the occurrence of complications such as hyperglycemia and hypoglycemia, as well as we assessed physical activity level, dietary intake, and the number of meals. After Ramadan re-evaluate anthropometric and metabolic parameters.
Results: We included 155 patients, 93.5% had type 2 diabetes and 6.5% had type 1 diabetes. We found that glycated hemoglobin, LDL cholesterol, and Triglyceride increased significantly after Ramadan (p-value < 0.001). We also found that weight, body mass index, waist circumference. Caloric intake increased significantly during Ramadan (p-value < 0.001); this increase concerned 61.3% of patients. In terms of metabolic parameters, diabetes was unbalanced in 52.6% of patients, hypoglycemia occurs in 20.9% of patients, and hyperglycemia was experienced by 37% of patients during Ramadan. We found that LDL cholesterol increased in 48.4% of patients, triglycerides increased in 60.6% of patients and serum level of total cholesterol increased in 55% of patients.
Conclusion: Our study showed that during Ramadan risk of complications in patients with diabetes is not only related to fasting.
Keywords: Ramadan, diabetes, non-fasting patients, metabolic profile
Introduction
Ramadan is a holy month during which Muslims around the world observe a strict fast from eating and drinking from dawn until sunset. This month follows the lunar calendar and is spread over 29 to 30 days. The duration of the fast can be as long as 18 hours depending on the geographical location.
Fasting during Ramadan can lead to complications in patients with chronic diseases such as diabetes.1 Indeed, patients with diabetes who fast during this month are at risk of hypoglycemia, ketoacidosis, dehydration, and thrombosis.2,3 To prevent these complications, the International Diabetes Federation (IDF) recommends a pre-Ramadan assessment for patients with diabetes, in order to advise patients with risk of complications not to fast.4
However, during the month of Ramadan, the lifestyle and eating habits of Muslims undergo major changes. Studies have shown that there is a disruption of sleep patterns, a reduction in physical activity, as well as a change in the number and meals.5 Indeed, in the Moroccan cultural habits, the fasting period of the day is broken by a feasting period with high caloric content of meals6. All these changes could have an impact on the metabolic control of patients with diabetes during this month even if they do not fast and this question is not well documented. To answer this interrogation, we conducted a study that aimed to evaluate the impact of the month of Ramadan on the lifestyle habits and metabolic profile of non-fasting patients with diabetes during this month.
Patients and Methods
Study Design
This was an observational cross-sectional study conducted at the department of endocrinology and diabetology of the Sheikh Khalifa Ibn Zaid Hospital of Casablanca, Morocco. The study was conducted during 3 months of Ramadan in 2018 (between May 17th and June 15th), Ramadan 2019 (between May 7th and June 6th), and Ramadan 2021 (between 14th April and 13th May).
Study Population
In this study, we included all patients with a known diagnosis of diabetes, aged above 18 years old, who did not fast during Ramadan. The study included patients who have agreed to be followed during Ramadan and agreed to provide informed consent. We excluded pregnant women and patients who did not fully complete the follow-up during the study period.
Data Collection and Measurements
The study was conducted during the three Ramadans, during 6 weeks with 3 consultations. First consultation was conducted one week before the beginning of Ramadan, during this consultation we collected the following data: demographics (age, gender), type of diabetes, diabetes history (including duration of diabetes, diabetes medications, degenerative complications), fasting risk stratification according to the IDF-DAR recommendations,4 anthropometric parameters (weight, body mass index, waist circumference), metabolic parameters (glycated hemoglobin, fasting blood glucose and lipid profile), physical activity level and assessment of dietary intake before Ramadan. During the month of Ramadan, all patients performed self-monitoring of blood glucose using a blood glucose logbook.
The second consultation was performed the second week of Ramadan (mid-Ramadan) to assess physical activity level, dietary intake, and number of meals, as well as the occurrence of complications such as hyperglycemia and hypoglycemia. The third consultation was performed, during the first week after the end of Ramadan to re-evaluate the anthropometric and metabolic parameters previously mentioned.
In order to evaluate the impact of the month of Ramadan on non-fasting diabetic patients, we compared the anthropometric and metabolic parameters of all patients. We also evaluated these parameters in the group of patients on insulin therapy and patients on oral antidiabetics.
Definitions
Risk Stratification
Risk related to fasting was defined according to DAR-IDF recommendations.4 Patients were stratified into 3 categories:
- Very high risk included patients who presented acute complications such as severe hypoglycemia, ketoacidosis, or hyperosmolar hyperglycaemic coma within the 3 months before Ramadan, patients with a history of recurrent hypoglycemia or hypoglycemia unawareness, poorly controlled type 1 diabetic patients, patients with acute illness, patients with Chronic dialysis or chronic kidney disease stage 4 and 5, patients with advanced macrovascular complications and elderly patients with ill health. For patients in this category, fasting is prohibited.
- High-risk category included type 2 diabetic patients with sustained poor glycaemic control, well-controlled type 1 diabetic patients, Well-controlled patients with mixed insulin, patients with chronic kidney disease stage 3, patients with stable macrovascular complications, patients with comorbid conditions that present additional risk factors, patients with diabetes performing intense physical labor and patients with treatment with drugs that may affect cognitive function. For patients in this category, fasting is not recommended.
- Moderate/low-risk category included, well-controlled type 2 diabetic patients treated with Lifestyle therapy, metformin, acarbose, Thiazolidinediones, second-generation sulfonamide, incretin-based therapy (DPP-4 inhibitors or GLP-1 RAs), sodium-glucose cotransporter-2 (SGLT2) inhibitors, or basal insulin. For patients in this category, fasting is not recommended. For patients in this category, fasting may be allowed.
Anthropometric Parameters
Weight and height were measured by trained investigators using standard equipment, according to the recommendations of Lohman et al.7 Weight was measured in fasting patients, with light clothing and an empty bladder. Standing height was measured in patients without shoes. Waist circumference was measured at the midpoint between the iliac crest and the lowest rib according to the World Health Organization recommendations.8
Body mass index (BMI) was calculated as weight in kilograms divided by height in squared meters.
Metabolic Parameters
Glycated hemoglobin was measured using high-performance liquid chromatography method (HPLC) according to the National Glycohemoglobin Standardization Program standardization.9 Fasting blood samples were collected after 12 hours of overnight fasting to quantify fasting plasma glucose (FPG) levels and Lipid profile components which include high-density lipoprotein-cholesterol (HDL-C), total cholesterol (TC), triglyceride and Low-density lipoprotein-cholesterol (LDL-C).
Serum levels of Cholesterol, HDL-C, and triglyceride were measured using by direct enzymatic colorimetric method, LDL-C was calculated using the Friedewald formula.10 The cut-off values that were used as reference for cholesterol was TC < 200 mg/dL, TG < 150 mg/dL, and HDL-C > 40 mg/dL in men and >50 mg/dL in women, following the NCEP/ATP III.11 LDL-C targets were established following the American Diabetes Association recommendations.12 For diabetic patients with established atherosclerotic cardiovascular disease, the cute off the value of LDL-C was LDL-C≤ 70mg/dl, for all other patients this value was LDL-C≤ 100mg/dl.
Dietary Intake Assessment
Dietary intake assessment and caloric intake were performed using the 24-hour dietary recall method and a food frequency questionnaire adapted for Moroccan adult.13 Total energy intake was calculated by trained investigators.
Physical Activity
Physical activity level was assessed using the Global Physical Activity Questionnaire (GPAQ2), which includes estimates of physical activity in three domains (activity at work, activity travelling to and from places, recreational activities) as well as sedentary behavior.14 The intensity of physical activity was classified into three categories: light intensity, moderate intensity, and vigorous intensity.
Statistical Analysis
For the descriptive analysis, we described normally distributed continuous variables as mean with standard deviations (SD) and normally undistributed variables as medians with interquartile ranges (IQRs). Categorical variables were described as percentages and frequencies. The normality of continuous variables distribution was conducted using the Kolmogorov–Smirnov test. To compare data before and after Ramadan, the McNemar test was used to compare categorical data and the student test for paired samples was performed to compare normally distributed quantitative variables. The Wilcoxon test was used to analyze normally undistributed data. All P-values were two-sided, and those < 0.05 were considered statistically significant. Statistical analyses were performed using SPSS 20.0.
Ethical Considerations
The study was approved by the institutional ethics board of Cheikh Khalifa ibn Zaid International University Hospital. Our study complies with the Declaration of Helsinki.
Informed consent was obtained for all patients prior to inclusion. Data confidentiality and patient anonymity were maintained at all stages of the study. We deleted Patient-identifying information before analysing the database.
Results
During the study period, 155 patients were included. Baseline characteristics of the study population are represented in Table 1. The median (interquartile range IQR) age of patients was 64 (IQR 57.5–71) years and, 60.6% were men. Among our patients, 93.5% of them had type 2 diabetes and 6.5% had type 1 diabetes. Diabetes duration was above 10 years of diabetes in 36.1% of patients. Microangiopathy was found in 36.1% of patients, and macroangiopathy in 15.5% of patients. Stratification of risk related to fasting showed that 91.6% were classified among very high risk and 8.4% were classified among high risk. As represented in Table 2, the median baseline weight of patients was 77 kg (IQR 69–88), their median BMI was 28kg/m2 (IQR 24.9–31.9) and their median waist circumference was 99cm (IQR 91–105). Assessment of physical activity before Ramadan using the GPAQ score showed that 83.9% had low physical activity, 11.6% had moderate activity, and 4.5% had high physical activity. Medians of baseline glycated hemoglobin and baseline fasting blood glucose were respectively 8.45% (IQR7.7–10) and 180 mg/l (1.40–2.09). Medians of baseline serum levels of total cholesterol, HDL-C, LDL-C and triglycerides were respectively 1.70g/l (1.32–2.01), 0.42g/l (0.33–0.5), 1.01g/l (0.74–1.32), 1.2g/l (0.95–1.6). The median caloric intake before Ramadan was 1641.12 Kcal (1454–1915.16). The median number of meals per day before Ramadan was 4 (IQR 3–4). We found no significant difference in terms of physical activity before and during Ramadan (p-value=0.79).
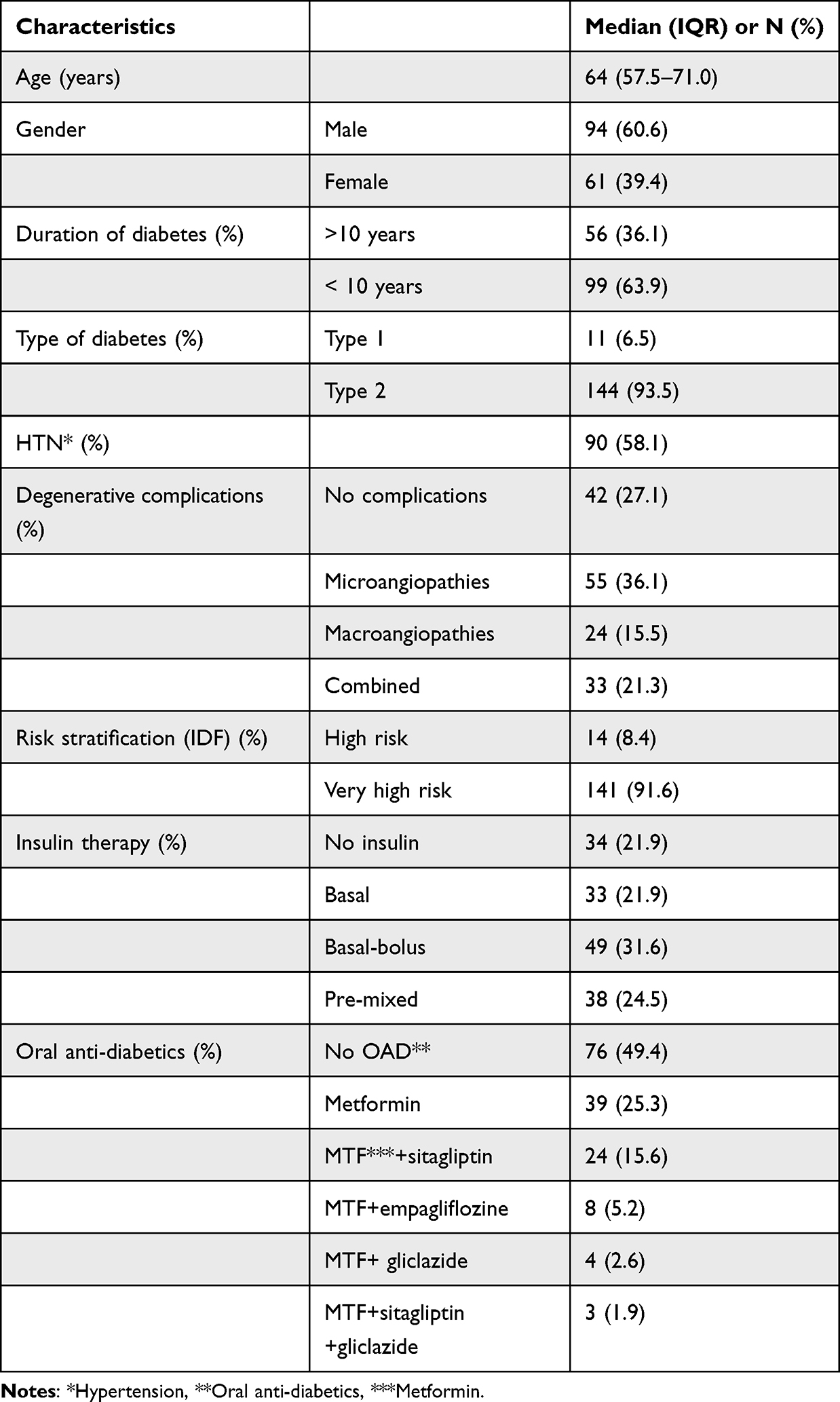 |
Table 1 Baseline Characteristics of Patients: Demographics, Diabetes History and Risk Stratification |
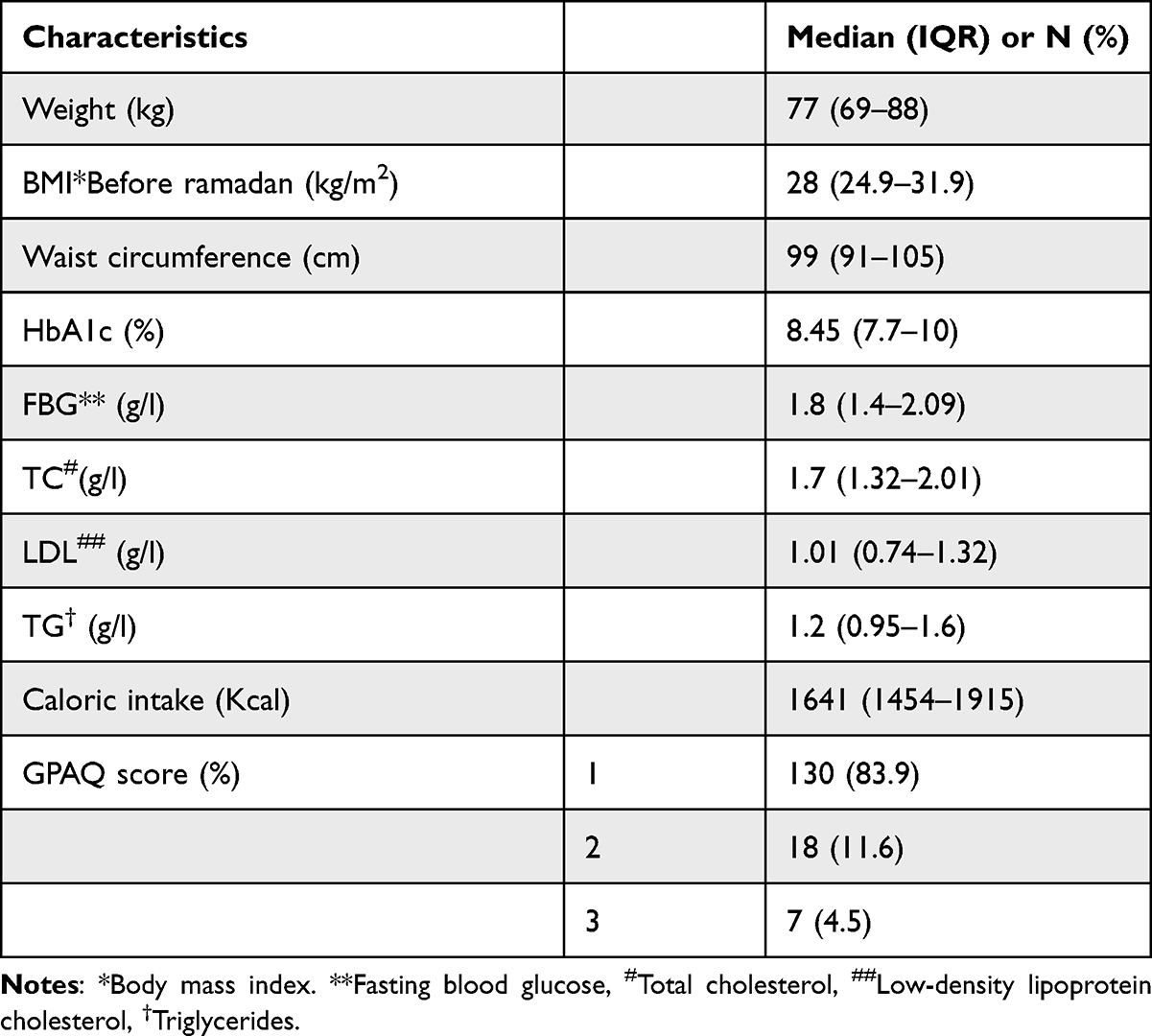 |
Table 2 Baseline Characteristics of Patients: Anthropometric and Metabolic Parameters, and Caloric Intake of Patients |
We found that 20.9% of patients presented hypoglycemia and 37.3% of patients presented hyperglycemia during Ramadan. The Median Number of meals during Ramadan was 4 meals (IQR: 4–5), 2.6% of patients had two meals per day, 46.4% had three meals, 41.8% had four meals, and 9.2% had five meals a day. There was no statistically significant difference between the number of meals before and after Ramadan (p=0.75). As represented in Table 3, caloric intake during Ramadan was significantly higher than before Ramadan (1861.78Kcal (IQR1549-2288) versus 1641.12 Kcal (1454–1915.16) respectively with p-value<0.01). The median evolution of caloric intake was +341.43 (IQR:0–465.4). We found that caloric intake increased in 61.3% of patients (Figure 1).
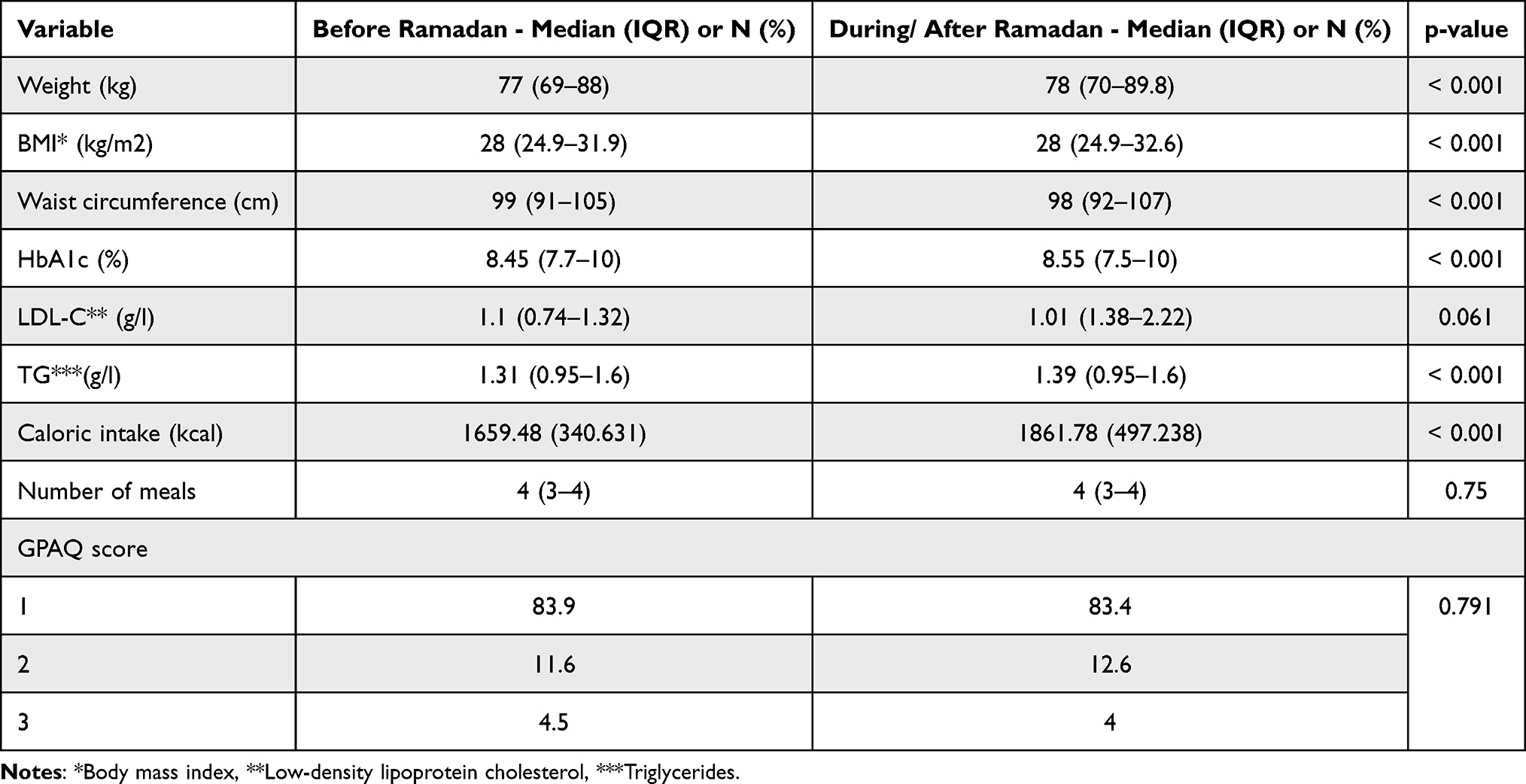 |
Table 3 Comparison of Caloric Intake, Physical Activity Level, Anthropometric and Metabolic Parameters Before and After Ramadan in All Non-Fasting Patients with Diabetes |
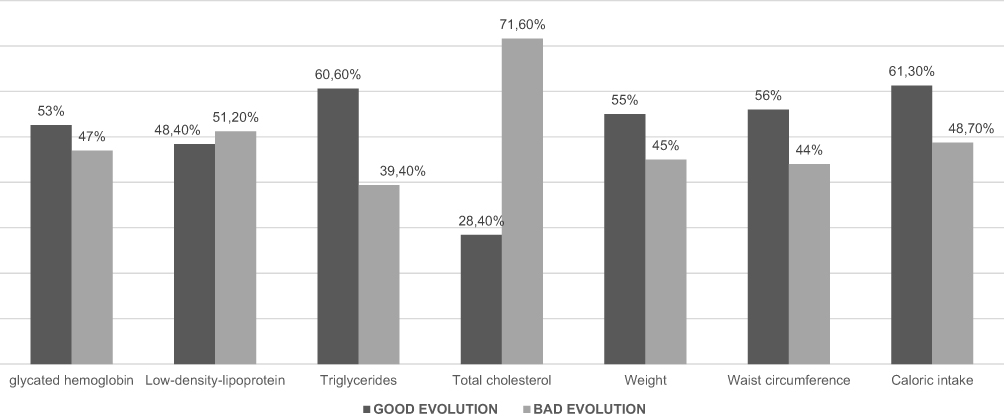 |
Figure 1 Evolution of anthropometric and metabolic parameters among non-fasting patients during Ramadan. |
In terms of anthropometric parameters, BMI, weight, and waist circumference increased significantly after Ramadan, p-values <0.001. The medians of evolutions of BMI, weight and waist circumference were respectively + 0.46kg/m2 (IQR: −0.75–1.49), +2 (IQR: −2–4) and +2 (IQR: −2- +3.75). Assessment of biochemical metabolic parameters after Ramadan showed that glycated hemoglobin after Ramadan increased significantly (8.55% (IQR: 7.5–10), p-value <0.001) with a median evolution of +0.1% (IQR: −0.75- +0.85). We noticed that 52.6% of the patients have unbalanced their diabetes (Figure 1).
Serum levels of total cholesterol after Ramadan was 1.69g/l (IQR:1.38–2.22) p-value:0.02, with a median evolution of +0.08 (IQR: −0.1-+0.3). There was no significant difference between levels of HDL-C, Triglycerides, and LDL-C before and after Ramadan (p-values were respectively 0.27, 0.45, and 0.07). However, we noticed that LDL-C level increased above the target in 48.4% of patients, hypercholesterolemia and hypertriglyceridemia were found in 28.4% and 60.6% of patients respectively after Ramadan (Figure 1).
As represented in Table 4, in patients on insulin therapy, we found that weight, BMI and waist circumference increased significantly after Ramadan (p values were p=0.001, p=0.008 and p=0.003 respectively). LDL-C serum level and caloric intake increased significantly after Ramadan (p-values were 0.008 and <0.0001 respectively). However, there was no statistically significant difference between levels of HBA1C and Triglycerides before and after Ramadan (p-values were respectively 0.67 and 0.57). In patients on oral antidiabetic agents, caloric intake increased significantly during Ramadan (p=0.004). However, there was no significant difference in terms of anthropometric and metabolic parameters before and after Ramadan in this group of patients (Table 4).
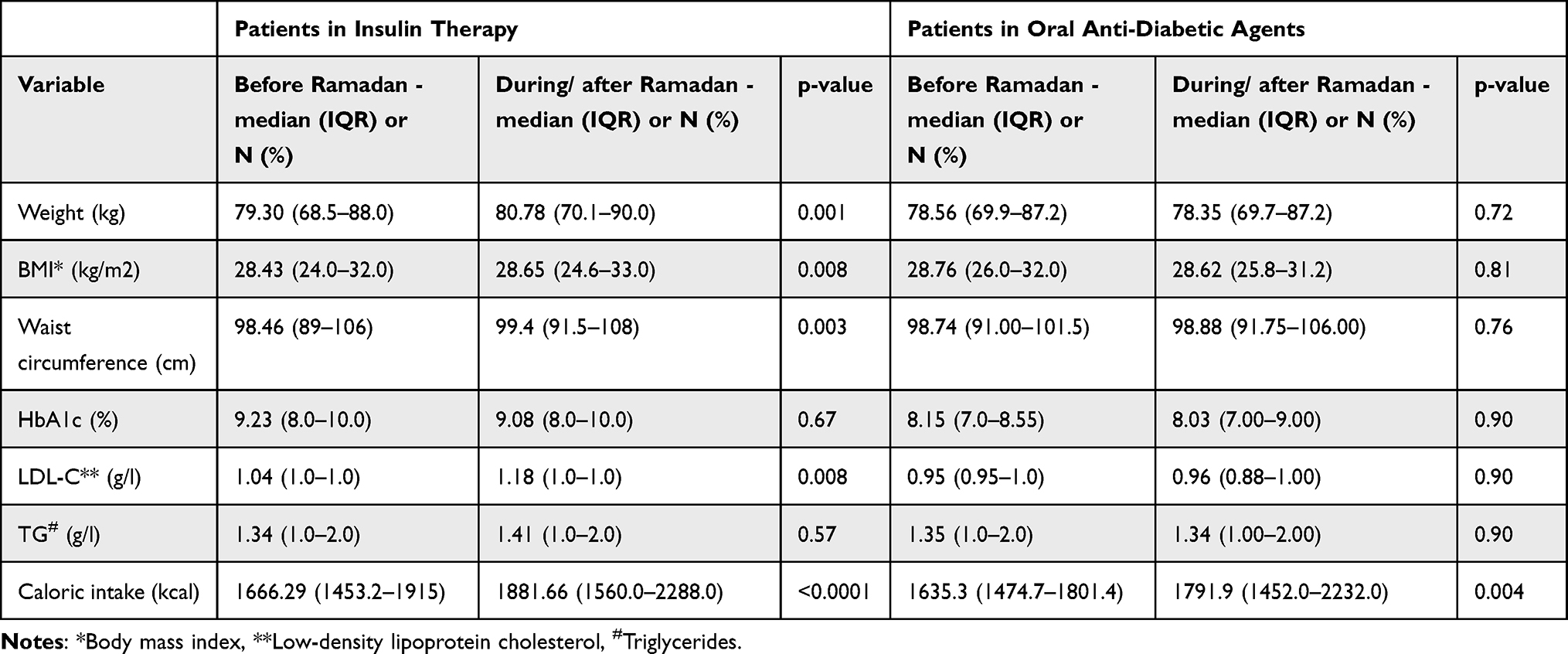 |
Table 4 Comparison of Caloric Intake, Anthropometric and Metabolic Parameters Before and After Ramadan in Patients’ Insulin Therapy and in Patients in Oral Antidiabetic Drugs |
Discussion
Management of diabetes during Ramadan is a challenging situation for professional healthcare, due to drastic changes in terms of diet, physical activity, and modification of the circadian rhythm. Indeed the EPIDIAR study showed that among patients with type 2 diabetes 36.8% have decreased their physical activity, 38.2% decreased sleeping duration, 18.6% increased their food intake and 19.1% had gained weight.3 Moreover, during this month there is a modification of the working hours, with greater involvement of the religious activity that leads to a decrease of the sleeping hours.15 In addition, it has been proven that sleep during the night-time is important for the metabolic process, which has been shown to facilitate blood glucose regulation that is essential for diabetes outcomes.16 Besides this, numerous studies have shown that the disturbance of the circadian rhythm can affect glucose homeostasis, insulin secretion, and insulin sensitivity and disturb glucose homeostasis, insulin secretion, and insulin sensitivity.15,17 Other studies showed that poor quality of sleep may increase glycated hemoglobin level.18 In addition, in non-diabetic people, drastic changes occur in terms of energy and water intake and glucose homeostasis. The time between meals is longer than outside Ramadan, meals are more consistent and are taken exclusively during the night.19
All these changes suggest that the risk of complications is not only related to fasting but also to these lifestyle changes. This puts patients with diabetes at risk of metabolic complications even if they do not fast.
Several studies have investigated the metabolic impact of Ramadan among fasting patients with diabetes. Indeed, D. Tahapary et al showed in a recent meta-analysis that fasting blood glucose decreased by 15.28 (95% CI −17.22, 13.34) mg/dL and glycated hemoglobin decreased by 0.27% (95% CI −0.32, 0.22) after Ramadan fasting. In terms of lipid profile, this meta-analysis showed that levels of total cholesterol, LDL-C, HDL-C and triglyceride decreased significantly (−12.88 (95% CI:-14.68, −11.09) mg/dL, −4.42 (95% CI:-6.17,-2.66) mg/dl, −1.09 (95% CI −1.71, −0.47) mg/dL and −2.47 (95% CI: −3.69,-1.24) mg/dL.20
The aim of our study was to investigate the impact of Ramadan on patients with diabetes who do not fast during this month. To the best of our knowledge very few studies investigated this question. We found that, in terms of anthropometric parameters, BMI, weight, and waist circumference increased significantly after Ramadan (p-values <0.001). Our study showed that 20.9% of patients had hypoglycemia which is probably due to the social pressure to skip lunch, especially in the workplace. We also found that 52.6% of our patients have unbalanced their diabetes and 37.3% of patients experimented hyperglycemia. This can be explained by the significant increase in caloric intake during the month of Ramadan with a p-value <0.001, because of the social and convivial aspect of meals, which leads patients to take part in the meals. This is consistent with the results of Sebbani et al,5 that compared dietary habits in fasting and non-fasting patients with type 2 diabetes, and found that caloric intake in non-fasting patients was significantly higher than the one in fasting patients (p-value 0.016) with a mean of 19,919.0 kcal (SD: 823.4). Moreover, it has been demonstrated that lifestyle habits including dietary intake contribute significantly to metabolic dysregulation through induction of adipogenesis and increased BMI. This leads to insulin resistance, impaired glucose metabolism, and dyslipidemia.21 This goes hand in hand with the results of our study that showed that 48.4% increased their LDL-C above the targets defined by the American diabetes association,12 60.6% increased their Triglycerides (TG) during the month of Ramadan. Furthermore, Sebbani et al5 found that the composition of total lipids of meals of non-fasting patients with diabetes were significantly higher in lipids than those of fasting patients with diabetes (p-value: 0.016).
The limitations of our study are the small sample of patients, monocentric study, and selection bias (hospital center of third grade). Additionally, we did not collect some variables that may influence anthropometric parameters, for example uncontrolled diabetes.
The strength of this study is its originality, as to the best of our knowledge there is no actual study that investigated the impact of Ramadan on non-fasting patients with diabetes during the month of Ramadan.
Conclusion
Our study showed that during Ramadan risk of complications in patients with diabetes is not only related to fasting. This highlights the importance of including all patients with diabetes even if they do not fast in specific therapeutic education programs. In non-fasting patients, these programs should be focused on lifestyle habits and nutritional plans during Ramadan. Moreover, these patients should not be excluded from the pre-Ramadan assessment and the follow-up during the month of Ramadan.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article and revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work. Both authors IM and FRT have contributed equally to this article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zaghlol LY, Beirat AF, Amarin JZ, et al. Effect of dosage reduction of hypoglycemic multidrug regimens on the incidences of acute glycemic complications in people with type 2 diabetes who fast during Ramaḍān: a randomized controlled trial. Front Endocrinol. 2021;12:613826. doi:10.3389/fendo.2021.613826
2. Jabbar A, Hassanein M, Beshyah SA, Boye KS, Yu M, Babineaux SM. CREED study: hypoglycaemia during Ramadan in individuals with Type 2 diabetes mellitus from three continents. Diabetes Res Clin Pract. 2017;132:19–26. doi:10.1016/j.diabres.2017.07.014
3. Salti I, Bénard E, Detournay B, et al. A population-based study of diabetes and its characteristics during the fasting month of Ramadan in 13 countries: results of the epidemiology of diabetes and Ramadan 1422/2001 (EPIDIAR) study. Diabetes Care. 2004;27(10):2306–2311. doi:10.2337/diacare.27.10.2306
4. IDF-DAR-practical-guidelines_15-April-2016_low_SA.pdf. Available from: https://www.daralliance.org/daralliance/wp-content/uploads/2018/01/IDF-DAR-Practical-Guidelines_15-April-2016_low_SA.pdf.
5. Sebbani M, Mghari G, Amine M, Amine M. Apports alimentaires durant le mois de ramadan chez le patient diabétique de type 2 marocain[Food intake during the month of Ramadan in Moroccan patients with type 2 diabetes]. East Mediterr Health J. 2013;19:276–281. French. doi:10.26719/2013.19.3.276
6. Barakat I, Chamlal H, El Jamal S, Elayachi M, Belahsen R, S. Razzaque M. Food expenditure and food consumption before and during Ramadan in Moroccan households. J Nutr Metab. 2020;2020:8849832. doi:10.1155/2020/8849832
7. Lohman TG, Roche AF, Martorell R. Anthropometric Standardization Reference Manual. Human Kinetics Books; 1988.
8. Consultation WH. Obesity: preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ Tech Rep Ser. 2000;894:
9. NGSP: HbA1c assay interferences. Available from: http://www.ngsp.org/interf.asp.
10. Martin SS, Blaha MJ, Elshazly MB, et al. Comparison of a novel method vs the Friedewald equation for estimating low-density lipoprotein cholesterol levels from the standard lipid profile. JAMA. 2013;310(19):2061–2068. doi:10.1001/jama.2013.280532
11. Cleeman J. ATP III guidelines At-A-glance quick desk reference; 2001:6.
12. Association AD. 10. cardiovascular disease and risk management: standards of medical care in diabetes—2021. Diabetes Care. 2021;44(Supplement1):S125–S150. doi:10.2337/dc21-S010
13. El Kinany K, Garcia-Larsen V, Khalis M, et al. Adaptation and validation of a food frequency questionnaire (FFQ) to assess dietary intake in Moroccan adults. Nutr J. 2018;17(1):61. doi:10.1186/s12937-018-0368-4
14. GPAQ_FR.pdf. Available from: https://www.who.int/ncds/surveillance/steps/GPAQ_FR.pdf.
15. Bahijri S, Borai A, Ajabnoor G, et al. Relative metabolic stability, but disrupted circadian cortisol secretion during the fasting month of Ramadan. PLoS One. 2013;8(4):e60917. doi:10.1371/journal.pone.0060917
16. Jauch-Chara K, Hallschmid M, Schmid SM, et al. Plasma glucagon decreases during night-time sleep in Type 1 diabetic patients and healthy control subjects. Diabet Med. 2007;24(6):684–687. doi:10.1111/j.1464-5491.2007.02116.x
17. Ajabnoor GM, Bahijri S, Borai A, Abdulkhaliq AA, Al-Aama JY, Chrousos GP. Health impact of fasting in Saudi Arabia during Ramadan: association with disturbed circadian rhythm and metabolic and sleeping patterns. PLoS One. 2014;9(5):e96500. doi:10.1371/journal.pone.0096500
18. Kermansaravi M, Omar I, Mahawar K, et al. Religious fasting of Muslim patients after metabolic and bariatric surgery: a modified delphi consensus. Obes Surg. 2021;31(12):5303–5311. doi:10.1007/s11695-021-05724-z
19. International Diabetes Federation and DAR International Alliance. Diabetes and Ramadan: practical guidelines, Brussels, Belgium: International Diabetes Federation; 2021. Available from: www.idf.org/guidelines/diabetes-in-ramadan.
20. Tahapary DL, Astrella C, Kristanti M, Harbuwono DS, Soewondo P. The impact of Ramadan fasting on metabolic profile among type 2 diabetes mellitus patients: a meta-analysis. Diabetes Metab Syndr. 2020;14(5):1559–1570. doi:10.1016/j.dsx.2020.07.033
21. Srivastava RAK. Life-style-induced metabolic derangement and epigenetic changes promote diabetes and oxidative stress leading to NASH and atherosclerosis severity. J Diabetes Metab Disord. 2018;17(2):381–391. doi:10.1007/s40200-018-0378-y
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.