Back to Journals » OncoTargets and Therapy » Volume 9
Radiological response and survival in locally advanced non-small-cell lung cancer patients treated with three-drug induction chemotherapy followed by radical local treatment
Authors Bonanno L, Zago G, Marulli G, Del Bianco P, Schiavon M, Pasello G, Polo V, Canova F, Tonetto F, Loreggian L, Rea F, Conte P, Favaretto A
Received 16 October 2015
Accepted for publication 14 January 2016
Published 21 June 2016 Volume 2016:9 Pages 3671—3681
DOI https://doi.org/10.2147/OTT.S98435
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Daniele Santini
Laura Bonanno,1 Giulia Zago,1 Giuseppe Marulli,2 Paola Del Bianco,3 Marco Schiavon,2 Giulia Pasello,1 Valentina Polo,1,4 Fabio Canova,1 Fabrizio Tonetto,5 Lucio Loreggian,5 Federico Rea,2 PierFranco Conte,1,4 Adolfo Favaretto1
1Medical Oncology Unit 2, Veneto Institute of Oncology IOV-IRCCS, 2Thoracic Surgery Department, University of Padova, 3Clinical Trials and Biostatistics Unit, Veneto Institute of Oncology IOV-IRCCS, 4Department of Surgery, Oncology and Gastroenterology, University of Padova, 5Radiotherapy Unit, Veneto Institute of Oncology IOV-IRCCS, Padova, Italy
Objectives: If concurrent chemoradiotherapy cannot be performed, induction chemotherapy followed by radical-intent surgical treatment is an acceptable option for non primarily resectable non-small-cell lung cancers (NSCLCs). No markers are available to predict which patients may benefit from local treatment after induction. This exploratory study aims to assess the feasibility and the activity of multimodality treatment, including triple-agent chemotherapy followed by radical surgery and/or radiotherapy in locally advanced NSCLCs.
Methods: We retrospectively collected data from locally advanced NSCLCs treated with induction chemotherapy with carboplatin (area under the curve 6, d [day]1), paclitaxel (200 mg/m2, d1), and gemcitabine (1,000 mg/m2 d1, 8) for three to four courses, followed by radical surgery and/or radiotherapy. We analyzed radiological response and toxicity. Estimated progression-free survival (PFS) and overall survival (OS) were correlated to response, surgery, and clinical features.
Results: In all, 58 NSCLCs were included in the study: 40 staged as IIIA, 18 as IIIB (according to TNM Classification of Malignant Tumors–7th edition staging system). A total of 36 (62%) patients achieved partial response (PR), and six (10%) progressions were recorded. Grade 3–4 hematological toxicity was observed in 36 (62%) cases. After chemotherapy, 37 (64%) patients underwent surgery followed by adjuvant radiotherapy, and two patients received radical-intent radiotherapy. The median PFS and OS were 11 months and 23 months, respectively. Both PFS and OS were significantly correlated to objective response (P<0.0001) and surgery (P<0.0001 and P=0.002). Patients obtaining PR and receiving local treatment achieved a median PFS and OS of 35 and 48 months, respectively. Median PFS and OS of patients not achieving PR or not receiving local treatment were 5–7 and 11–15 months, respectively. The extension of surgery did not affect the outcome.
Conclusion: The multimodality treatment was feasible, and triple-agent induction was associated with a considerable rate of PR. Patients achieving PR and receiving radical surgery or radiotherapy (53%) achieved a median OS of 4 years.
Keywords: surgery, radiotherapy, neoadjuvant chemotherapy, stage III lung cancer, pneumonectomy
Introduction
Approximately 25%–30% of non-small-cell lung cancer (NSCLC) patients are diagnosed with locally advanced disease. The term refers to a heterogeneous group of nonprimarily resectable tumors due to local invasion of vital structure or the degree of nodal involvement.1 In recent years, no major improvement in the outcome of locally advanced patients has been achieved, and 5-year overall survival (OS) rate is generally <20%, with ~5% of “long-survivors”.2 A multidisciplinary management of these patients is mandatory, and the choice of treatment is still largely influenced by the single-center specific expertise.2,3 The multidisciplinary approach allows integrating different treatment modalities, taking into account the heterogeneity of stage III that includes potentially resectable and unresectable disease, ranging from stage T3N1 to T4N3.2 Different subgroups of staging imply different outcomes and treatment options, whereas further complexity has been generated by the new definition of the T parameter according to the most recent International Association for the Study of Lung Cancer staging system.2
Until recently, the treatment of locally advanced NSCLCs was mainly radiotherapy; the superiority of combined treatment has been demonstrated in the 1990s when induction chemotherapy followed by radiotherapy was compared to radiotherapy alone.4,5 The benefit in terms of OS was confirmed also after a 7-year follow-up analysis.6 Finally, the concurrent strategy was shown to improve the outcome of locally advanced NSCLC patients when compared to sequential chemoradiotherapy. An absolute OS improvement of 4.5% at 5 years emerged from an important meta-analysis, including patients’ data from six randomized clinical trials.7 This advantage was counterbalanced by increased toxicity, mainly esophagitis,7 whereas a recent meta-analysis suggests that the treatment-related deaths are not significantly increased by the concurrent strategy.8 The standard treatment of locally advanced NSCLC is thus considered concomitant chemoradiotherapy, when feasible, according to clinical condition and disease extension.1,3,9 However, induction treatment followed by radical-intent radiotherapy is considered an acceptable option in nonresectable stage III disease when the start of radiotherapy must be delayed due to technical problems or the extension of the disease.
Overall, chemotherapy has an unquestionable role in locally advanced NSCLC,3 and the use of induction treatment before surgery has a strong rationale in two main settings: low burden mediastinal lymph node (N2) judged as resectable at diagnosis and patients with advanced local tumor (T3–4) for whom radical surgery is not feasible at baseline.
No data are available to define the preferred induction chemotherapy, but a three-drug combination can increase the response rate (RR),10 thus allowing the best local treatment and finally improvement of the OS of patients whose disease is potentially resectable and/or not eligible for chemoradiotherapy d’emblée.
Our exploratory retrospective study evaluates the role of three-drug induction chemotherapy followed by multidisciplinary reevaluation for radical-intent local treatment in non primarily resectable locally advanced NSCLC patients.
Patients and methods
Patients and staging
We retrospectively collected clinical data and radiological imaging from patients radiologically staged as IIIA and IIIB NSCLC, according to the TNM Classification of Malignant Tumors–7th edition staging system.11
The patients were consecutively treated at Istituto Oncologico Veneto in Padova between January 2006 and September 2012. Selection criteria were radiological staging, multidisciplinary assessment indicating the potentiality of radical-intent surgery and/or lack of feasibility of concomitant chemoradiotherapy, and lack of contraindication to platinum-based chemotherapy.
Clinical stage at diagnosis was assessed by chest, abdomen, and brain computed tomography (CT) scan and confirmed by 18fluorodeoxyglucose-positron emission tomography-computed tomography (18-FDG-PET-CT). Histology was proven by bronchoscopy, CT-guided transthoracic biopsy, or mediastinoscopy. Each patient underwent bronchoscopy for planning local treatment. Pathological confirmation of N2–N3 lymph-node involvement was not mandatory but was performed when CT and PET/CT findings were judged as nonconclusive by the multidisciplinary team. N2 status was assessed by endobronchial ultrasound or mediastinoscopy, while supraclavicular N3 was assessed by ultrasound-guided fine-needle aspiration biopsy.
The Common Terminology Criteria for Adverse Events v 4.0 were used to report toxicity.
The Ethics Committee of Istituto Oncologico Veneto approved the study and the patients provided informed consent to be signed for the collection, analysis, and publication of data.
Chemotherapy treatment and postchemotherapy staging
We included in the study patients treated with induction chemotherapy, including carboplatin (AUC [area under the curve] 6, d [day] 1), paclitaxel (200 mg/m2, d1), and gemcitabine (1,000 mg/m2, d1,8) (paclitaxel-carboplatin-gemcitabine [TCG]),10 administered for three courses, followed by radiological disease reassessment with total-body CT with iodine contrast. Patients not experiencing more than one grade 3–4 hematological toxicity per cycle underwent a fourth cycle. Radiological response was assessed using Response Evaluation Criteria in Solid Tumors v 1.1.12 Before radical-intent local treatment patients also underwent FDG-PET/TC, cardiological assessment and pulmonary function test.18
Surgery and radiotherapy
Radical-intent local treatment was decided after discussion at the multidisciplinary tumor board including medical oncologists, thoracic surgeons, radiation oncologists, and radiologists.
Surgery was performed at the Thoracic Surgery Department of the University of Padova, whereas radiotherapy was performed at the Radiotherapy Unit of the Istituto Oncologico Veneto in Padova.
Surgery or radical-intent radiotherapy was planned 3 weeks after the last dose of chemotherapy was administered. The median delay to local treatment was calculated as the difference between the time to surgery or radiotherapy (number of weeks from the beginning of induction therapy and surgery) and the planned time.
Patients with pathologically confirmed N2 disease were treated with adjuvant 3D-conformal radiotherapy at the dosage of 54 Grays (Gy)/27 fractions (F): the radiation-field covered ipsilateral hilum and mediastinum.
Radical-intent radiotherapy was administered to patients not progressing after induction chemotherapy but not eligible for surgery: 3D-conformal radiotherapy at the dosage of 64 Gy/32F was administered on primary tumor and involved lymph-node regions.
Follow-up
After completing the multimodality treatment, regular follow-up was performed by the multidisciplinary team. Total-body CT with iodine contrast was performed two months after concluding the multimodal treatment. Patients receiving radiotherapy were restaged with 18FDG-PET/TC three months after the completion of radiotherapy and a chest–abdomen CT was repeated every three months for the first two years or when clinically indicated. For the subsequent years, CT scan, biochemistry and clinical evaluation were performed every six months until five years. Patients not receiving radiotherapy were followed using the same schedule, not including routine 18FDG-PET evaluation.
Statistical analyses
Progression-free survival (PFS) was calculated from the beginning of induction chemotherapy to demonstrated radiological progression or death from any cause. OS was calculated from the beginning of chemotherapy to death from any cause. Median PFS and OS were estimated using Kaplan–Meier methods. The influence of potential prognostic factors was analyzed using log-rank test and cox-regression method (univariate and multivariate analyses). Covariates able to affect outcome with statistical significance were included in multivariate analyses. The relationship between variables was assessed with chi-squared test. All the analyses were performed using Statistical Package for Social Science v 17. Significance was set at two-sided P<0.05.
Results
Patients’ characteristics and staging
A total of 58 patients diagnosed with stage IIIA or IIIB NSCLC were treated with TCG induction followed by surgery and/or radical-intent radiotherapy. The clinical features of the study population and details of radiological staging are summarized in Table 1. In particular, 40 (69%) patients were diagnosed with IIIA stage disease, whereas 18 (31%) presented stage IIIB. Out of the 18 cases, nine were cT4N2 and nine had single supraclavicular ipsilateral localization (detected either with PET/CT or with fine-needle aspiration biopsy) in the absence of radiological evidence of N2 involvement.
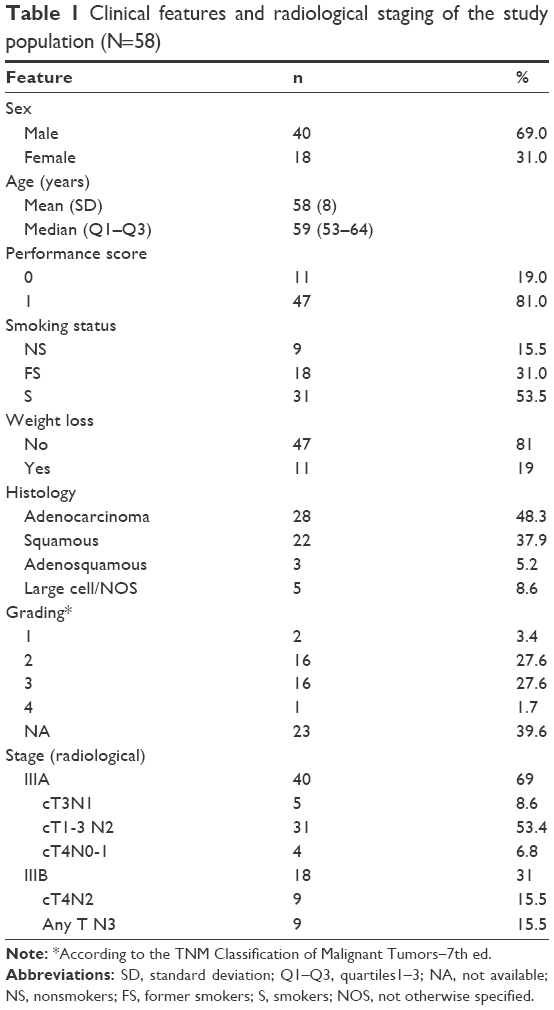 | Table 1 Clinical features and radiological staging of the study population (N=58) |
Treatment
Three cycles of TCG chemotherapy were administered to 29 (50%) patients while 27 (46%) patients received four cycles; two (3%) patients not receiving local treatment were treated with six courses of chemotherapy.
After three cycles of treatment, the patients were restaged and rediscussed by the multidisciplinary team. In all, 40 (69%) patients were judged eligible for radical-intent local treatments. One of these patients underwent exploratory surgery only because of the local extension of the disease observed at thoracotomy. Overall, 37 (63%) patients actually received radical surgery, while two underwent definitive radiotherapy (Figure 1). Among the 37 surgically treated patients, 24 (41%) underwent lobectomy or sleeve lobectomy, two (3%) had bilobectomy, and a pneumonectomy was necessary in eleven (19%) cases: eight on the right and three on the left lung (Figure 1). Resection of ipsilateral supraclavicular lymph node was performed in the four cases of patients undergoing surgery in the presence of baseline single supraclavicular lymph-node involvement. After surgery, 24 (41%) patients received adjuvant mediastinal radiotherapy (“Surgery and radiotherapy” section, Figure 1).
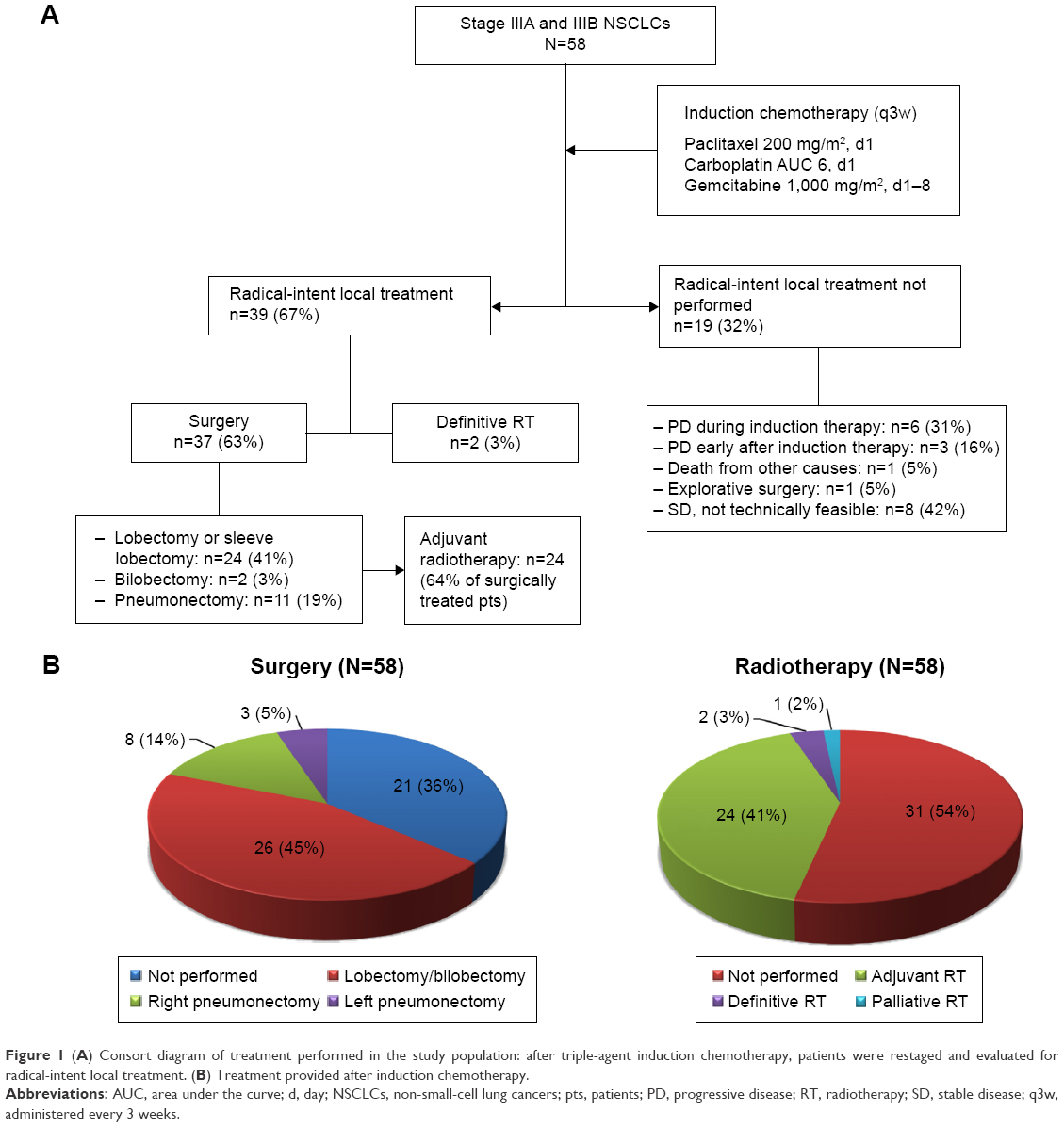 | Figure 1 (A) Consort diagram of treatment performed in the study population: after triple-agent induction chemotherapy, patients were restaged and evaluated for radical-intent local treatment. (B) Treatment provided after induction chemotherapy. |
One patient also received adjuvant radiotherapy due to positive bronchial margins (15 Gy/5 F high-dose rate brachytherapy). Among patients not receiving radical-intent local treatment, one patient underwent palliative thoracic radiotherapy (20 Gy/5 F) (Figure 1).
Feasibility of induction chemotherapy
Overall, no toxic death was reported, and only one patient was hospitalized due to treatment-related febrile neutropenia. Main toxicity was hematological, with 36 (62%) reported cases of grade 3 or 4 hematological toxicity. Only one case of grade 3 nonhematological toxicity was observed: a grade 3 diarrhea in a patient also experiencing grade 4 leukoneutropenia. The main nonhematological toxicities were mild (grade 1 or 2 according to Common Terminology Criteria for Adverse Events v 4.0), including fatigue, neuropathy, and arthralgia (Table 2).
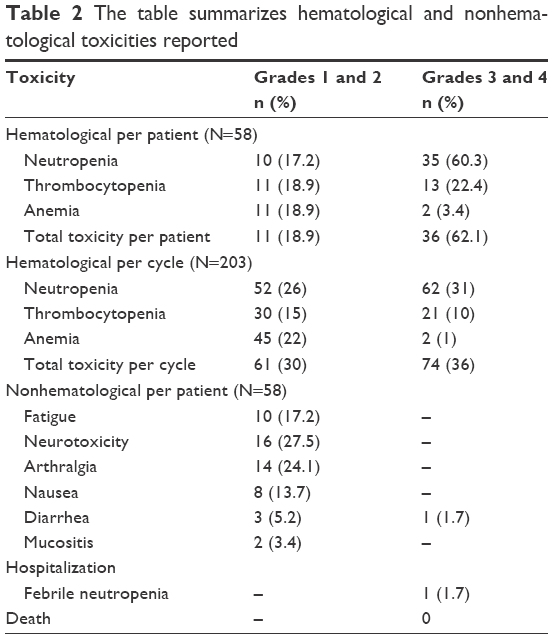 | Table 2 The table summarizes hematological and nonhematological toxicities reported |
Dose reduction was performed according to clinicians’ evaluation, and four (7%) patients received 75% of the dose of the three drugs as a third course of treatment. The details of dose reduction are specified in Table S1.
Response to induction treatment
Radiological response was assessed after the third course of chemotherapy. Partial response (PR) was obtained in 36 (62%) cases, whereas stable disease was observed in 16 (28%). Six (10%) patients had disease progression after three cycles of chemotherapy. Three patients progressed locally with the increase of primary tumor and mediastinal lymph-node involvement, whereas three patients experienced systemic progression with multiple sites of metastasis. Three patients obtaining PR unfortunately experienced rapid progression with multiple metastatic sites after the fourth course of treatment and were thus excluded from local treatment.
Among 37 patients undergoing surgery, no pathological complete response was observed. Complete pathological remission of nodal involvement was obtained in nine (24%) patients; overall, pathological remission of nodal involvement was achieved in 15 (41%) cases. Out of the 20 patients with pathological nodal involvement confirmation at baseline, seven underwent surgery and nodal downstaging was observed in five cases.
A high level of correlation between radiological response and feasibility of radical-intent local treatment was highlighted (χ2: 0.0001) (Table S2).
Toxicity of local treatment
Median delayed time to radical-intent local treatment was 2 (2.7; 95% confidence interval [CI]: 1.6–3.9) weeks.
No toxic death was reported, while perioperative complications, one chilothorax, one atrial fibrillation, and one dysphonia associated with prolonged air leak were observed.
Following radiotherapy, three patients experienced esophagitis, one patient had radiation pneumonitis, and two referred cough without radiological signs.
Pattern of relapse and postprogression treatment
Progression was mainly at distant sites. Two patients relapsed with brain metastases only; one of them underwent surgery and adjuvant brain radiotherapy and is still alive at 4 years without evidence of disease. Three patients received palliative thorax radiotherapy after disease progression. Four patients were not able to receive further systemic treatment. Details about further systemic treatment are depicted in Table S3. Overall, the three-drug chemotherapy induction treatment does not seem to affect the possibility of receiving further lines of systemic treatment.
Survival analysis
The estimated median follow-up was 68 (95% CI: 59–75) months. The median PFS of the study population was 10.8 (95% CI: 8–22) months, with 46% (95% CI: 33–59) of patients without evidence of disease after 1 year and 27% (95% CI: 16–39) after 3 years (Figure 2). The median OS of the study population was 22.8 (95% CI: 14–40) months. One-year OS rate was 72% (95% CI: 59–82), and 42% (95% CI: 29–55) of patients were alive 3 years after the diagnosis (Figure 2).
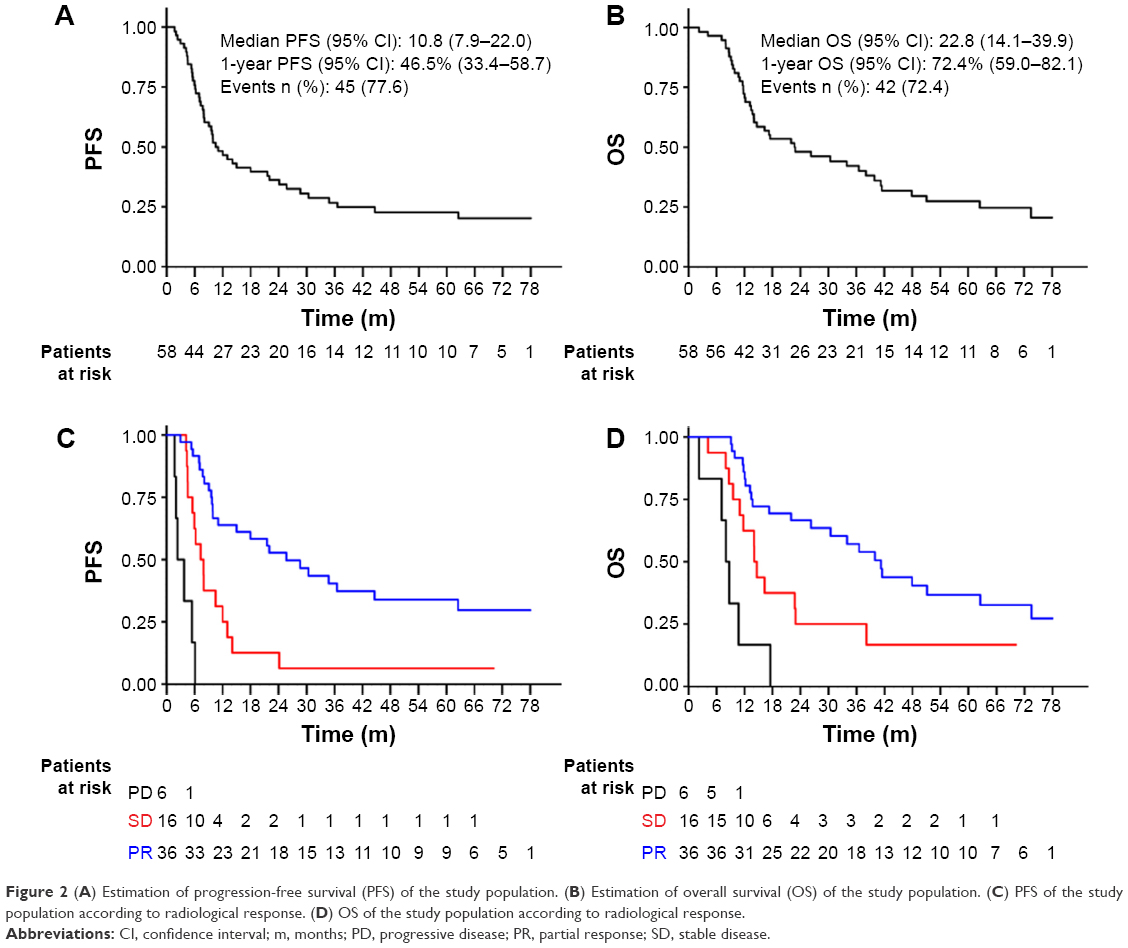 | Figure 2 (A) Estimation of progression-free survival (PFS) of the study population. (B) Estimation of overall survival (OS) of the study population. (C) PFS of the study population according to radiological response. (D) OS of the study population according to radiological response. |
The potential prognostic impact of clinicopathological features, radiological response, and local treatment performed are shown in Table 3: the variables affecting PFS and OS with statistical significance were radiological response and the performance of radical-intent local treatment (Figure 3). When we considered the differential impact of the type of local treatment performed, we were not able to identify any statistical prognostic difference (Table 3) and the median OS of patients undergoing pneumonectomy was similar to patients receiving lobectomy or radical-intent radiotherapy (Table 3).
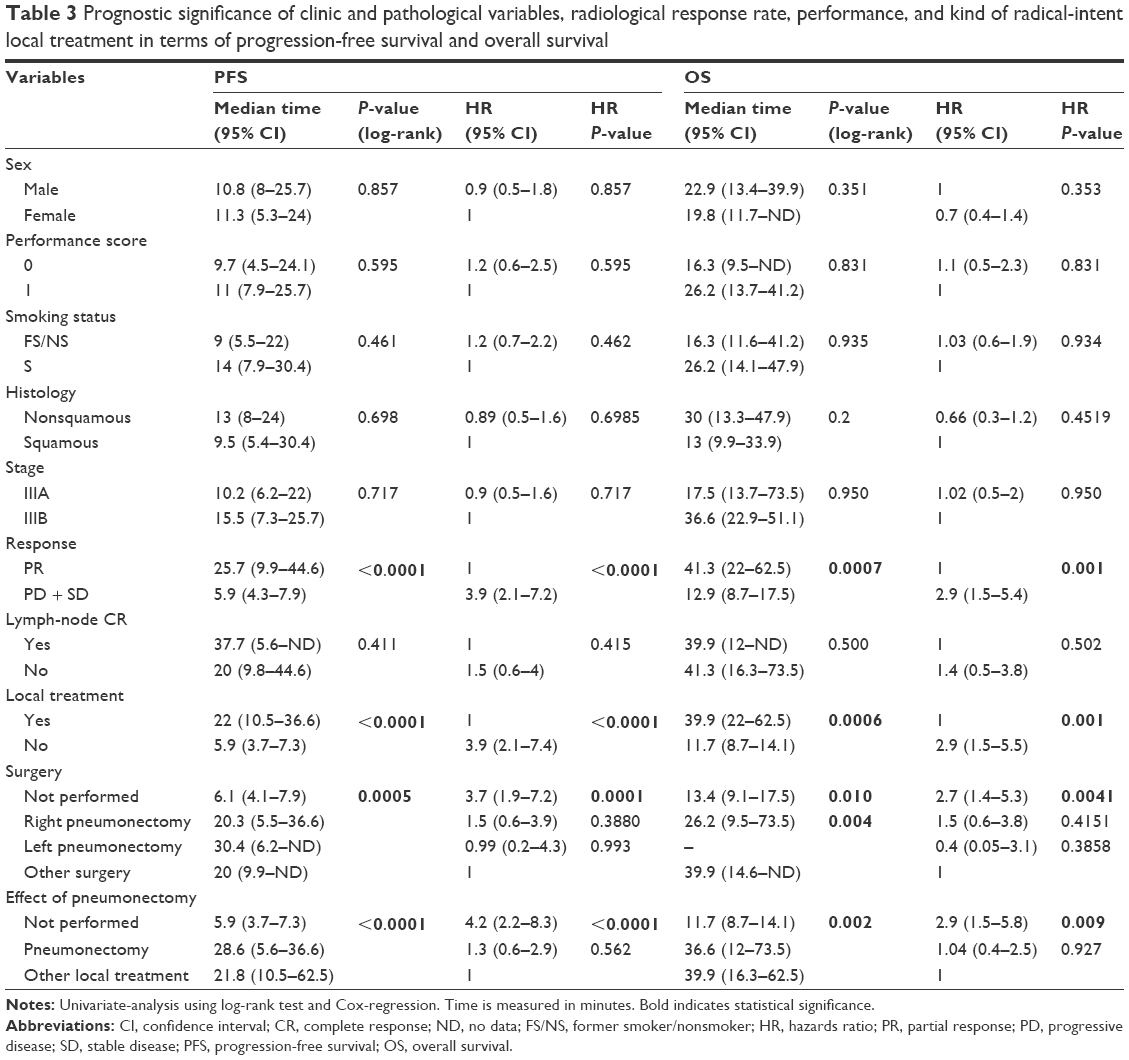 | Table 3 Prognostic significance of clinic and pathological variables, radiological response rate, performance, and kind of radical-intent local treatment in terms of progression-free survival and overall survival |
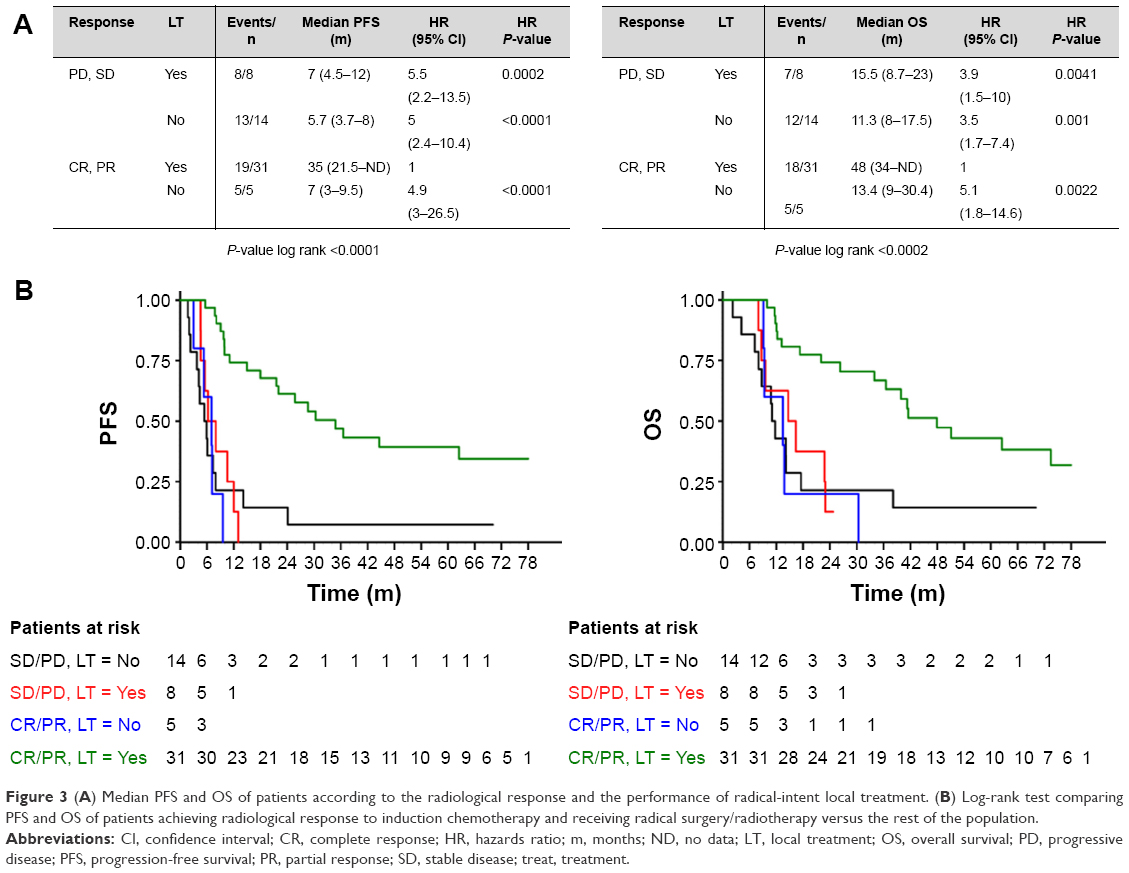 | Figure 3 (A) Median PFS and OS of patients according to the radiological response and the performance of radical-intent local treatment. (B) Log-rank test comparing PFS and OS of patients achieving radiological response to induction chemotherapy and receiving radical surgery/radiotherapy versus the rest of the population. |
Based on these results, we performed multivariate analysis, including RR and local treatment as covariates. The interaction test confirmed the two elements influenced both PFS and OS (P=0.002; P=0.02). The median PFS and OS of patients achieving a PR and receiving radical-intent local treatment were 34.8 months and 48 months, respectively. On the contrary, all the other groups of patients obtained disappointing results (PFS range: 5–7 months, OS range: 11–15 months) and patients undergoing local treatment in the presence of stable disease, apparently had no benefit from it (Figure 3).
Discussion
The study population was consecutively treated in our center with multimodality treatment, including triple-agent induction chemotherapy, followed by multidisciplinary rediscussion for radical-intent local treatment.
The protocol (Figure 1) was chosen taking into account practical clinical needs. Given the toxicity and unproved superiority of chemoradiotherapy as induction treatment,13,14 high heterogeneity of locally advanced disease, and technical difficulties of concomitant chemoradiotherapy as initial treatment, chemotherapy followed by radical-intent local treatment represents a reasonable option in clinical practice. In our study population, most of the patients were surgically treated after induction. Two randomized trials, INT-013915 and EORTC NCT 00002623,16 have not demonstrated significant OS improvement following the addition of surgery after chemoradiotherapy induction treatment. However, the high surgery-related mortality rate and the difference in OS according to the extension of surgery have a recognized role in the interpretation of the results. The authors of the most recent Phase III trial addressing this issue concluded that induction followed by surgery and chemoradiotherapy are two reasonable options and should be discussed by the multidisciplinary team for each individual patient.17 The most recent National Comprehensive Cancer Network Guidelines still suggests that a thoracic surgery evaluation should be performed for each potential candidate for curative treatment.1
The chemotherapy schedule used in our study has been tested prospectively in metastatic setting demonstrating an important increase in RR by adding gemcitabine to carboplatin and paclitaxel (46% vs 20%, P<0.0001).10 In the trial, an OS benefit was also highlighted,10 even though a previous meta-analysis concluded that triple-agent chemotherapy improves RR, but not OS, in metastatic NSCLC.18
The hypothesis at the basis of our analysis was that three-drug induction could improve the feasibility of radical-intent local treatment and the increased radiological RR could be a predictor of survival in this specific disease setting.
We firstly assessed the feasibility of the treatment. Chemotherapy toxicity profile was consistent with literature data,10 and there was only one hospitalization due to treatment-related toxicity. The median delay to local treatment was ~two weeks, which may be considered as acceptable in clinical practice. The limited toxicity correlated to local treatment confirms that this three-drug regimen did not affect its feasibility. No toxic death was recorded, whereas toxicity of multimodality treatment in this disease setting is traditionally expected to be higher with a mortality rate of ~5% in patients treated with surgery or concomitant chemoradiotherapy.16,19
The RR of the induction chemotherapy, the primary endpoint of the exploratory analysis, was higher than 60%, resulting in a median OS of 23 months. Comparison with literature data is rather difficult due to heterogeneity of inclusion criteria, stage definition, chemotherapy, and surgery-related morbidity and mortality. In particular, the results are not comparable with data from study population, including stage IB-II disease. A three-drug chemotherapy with cisplatin 50 mg/m2, gemcitabine 1,000 mg/m2, and paclitaxel 125 mg/m2 has been tested as induction treatment in NSCLCs with biopsy-proven N2 involvement: the RR was 73% and 55% of patients subsequently received surgery. The median OS achieved was 23 months.20 Our study population was completely different including patients who were judged as non primarily resectable due to tumor extension (T4) or nodal involvement (N3, bulky N2 or multistation N2) (Table 1). Induction chemotherapy with carboplatin AUC 5, gemcitabine 1,000 mg/m2, and paclitaxel 175 mg/m2 for three cycles has been studied before consolidation radiotherapy. In this trial, RR to chemotherapy was 55%, slightly inferior to what we found, and the median OS was 17 months.21
In our study population, a very favorable outcome was achieved by patients obtaining PR after chemotherapy and receiving local treatment. On the contrary, the outcome of the other groups of patients was similar to what is expected in metastatic disease. This suggests a potential role of chemotherapy in improving the selection of patients for local treatment. In parallel, increased RR associated with triple-agent chemotherapy could be translated as OS advantage in this specific disease setting. On the other hand, the prognostic role of radiological response to induction chemotherapy has also been observed in a previous analysis performed by our group in surgically treated patients.22 The obtained outcome results are also correlated to the feasibility of surgery and the absence of detrimental effect for pneumonectomies when performed in high-volume thoracic surgery centers.23,24
The potential advantages of the multimodality strategy include the feasibility in professional setting when compared to concomitant chemoradiotherapy, improved tolerability, and possibility of selection of patients to undergo radical-intent local treatment. The disadvantages may include delay of radical-intent local treatment and this may be relevant for unresectable disease, in which concomitant chemoradiotherapy was demonstrated to be superior to sequential strategy.1 On the other hand, induction chemotherapy could reduce the risk of distant metastasis, similar to what has been studied in locally advanced head-and-neck cancer, in which induction intensified chemotherapy has demonstrated great potentiality,25 even in the presence of solid evidence in favor of concomitant chemoradiotherapy strategy.
The main limitation of the study is its retrospective nature. In this context, given also the stage of the disease at baseline, we were not able to provide full information about molecular characterization, potentially affecting patients’ prognosis. Anyway, only three patients received targeted therapy (erlotinib) during the course of the disease and only one of them was known to be EGFR-mutated.
The analysis of the results must take into account the clinical selection of patients, being patients with ECOG PS of 0–1 at diagnosis and with a median age inferior to standard NSCLC population. However, baseline clinical selection strengthens the hypothesis of a prognostic role for radiological response.
Conclusion
The multimodality treatment was demonstrated to be feasible, and radiological response to induction chemotherapy could have a role in selecting non primarily resectable NSCLCs for radical-intent local treatment. Integration of treatment and specific expertise could potentially improve the outcome of locally advanced patients, and the presented multimodality approach warrants prospective validation and possibly prospective comparison with concurrent chemoradiotherapy approach.
Disclosure
The authors report no conflicts of interest in this work.
References
Ettinger DS, Wood DE, Akerley W, et al. Non-small cell lung cancer Version 4. 2014. NCCN Clinical Practice Guidelines in Oncology. 2014. Available from: https://www.nccn.org/professionals/physician_gls/f_guidelines.asp. Accessed May 20, 2016. | ||
Groome PA, Bolejack V, Crowley JJ, et al. The IASLC Lung Cancer Staging Project: validation of the proposals for revision of the T, N, and M descriptors and consequent stage groupings in the forthcoming (seventh) edition of the TNM classification of malignant tumours. Journal Thorac Oncol. 2007;2(8):694–705. | ||
Vansteenkiste J, De Ruysscher D, Eberhardt WE, et al. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2013;24(Suppl 6):vi89–vi98. | ||
Dillman RO, Seagren SL, Propert KJ, et al. A randomized trial of induction chemotherapy plus high-dose radiation versus radiation alone in stage III non-small-cell lung cancer. N Engl J Med. 1990;323(14):940–945. | ||
Sause W, Kolesar P, Taylor S IV, et al. Final results of phase III trial in regionally advanced unresectable non-small cell lung cancer: radiation Therapy Oncology Group, Eastern Cooperative Oncology Group, and Southwest Oncology Group. Chest. 2000;117(2):358–364. | ||
Dillman RO, Herndon J, Seagren SL, Eaton WL Jr, Green MR. Improved survival in stage III non-small-cell lung cancer: seven-year follow-up of cancer and leukemia group B (CALGB) 8433 trial. J Natl Cancer Inst. 1996;88(17):1210–1215. | ||
Aupérin A, Le Péchoux C, Rolland E, et al. Meta-analysis of concomitant versus sequential radiochemotherapy in locally advanced non-small-cell lung cancer. J Clin Oncol. 2010;28(13):2181–2190. | ||
Zhao J, Sadek RF, Albasheer A, Hao Z, Mott F, Kong FM. Treatment-related deaths after concurrent chemoradiotherapy in locally advanced non-small cell lung cancer: a meta-analysis of randomized studies. J Clin Oncol. 2014;32:5s(abstr 7561). | ||
Farray D, Mirkovic N, Albain KS. Multimodality therapy for stage III non-small-cell lung cancer. J Clin Oncol. 2005;23(14):3257–3269. | ||
Paccagnella A, Oniga F, Bearz A, et al. Adding gemcitabine to paclitaxel/carboplatin combination increases survival in advanced non-small-cell lung cancer: results of a phase II-III study. J Clin Oncol. 2006;24(4):681–687. | ||
Travis WD, Brambilla E, Noguchi M, et al. International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. J Thorac Oncol. 2011;8(2):244–285. | ||
Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–247. | ||
Shah AA, Berry MF, Tzao C, et al. Induction chemoradiation is not superior to induction chemotherapy alone in stage IIIA lung cancer. Ann Thorac Surg. 2012;93(6):1807–1812. | ||
Pless M, Stupp R, Ris H, et al. Final results of the SAKK 16/00 trial: a randomized phase III trial comparing neoadjuvant chemoradiation to chemotherapy alone in stage IIIA/N2 non-small cell lung cancer (NSCLC). Ann Oncol. 2014;24(Suppl 4):iv417–iv425. | ||
Albain KS, Swann RS, Rusch VW, et al. Radiotherapy plus chemotherapy with or without surgical resection for stage III non-small-cell lung cancer: a phase III randomised controlled trial. Lancet. 2009;374(9687):379–386. | ||
van Meerbeeck JP, Kramer GW, Van Schil PE, et al. Randomized controlled trial of resection versus radiotherapy after induction chemotherapy in stage IIIA-N2 non-small-cell lung cancer. J Nat Cancer Inst. 2007;99(6):442–450. | ||
Eberhardt W, Gauler T, Pottgen C, et al. Phase III study of surgery (S) versus definitive concurrent chemoradiotherapy boost (def ccCRTx-BOx) in patients (pts) with operable (OP+) stage IIIA(N2)/selected IIIb (sel IIIB) non-small cell lung cancer (NSCLC) following induction (IND) chemotherapy (CTx) and concurrent CRTx (ESPATUE). J Clin Oncol. 2014;32:5s(suppl; abstr 7510). | ||
Delbaldo C, Michiels S, Syz N, Soria JC, Le Chevalier T, Pignon JP. Benefits of adding a drug to a single-agent or a 2-agent chemotherapy regimen in advanced non-small-cell lung cancer: a meta-analysis. JAMA. 2004;292(4):470–484. | ||
Eberhardt WE, Gauler TC, Lepechoux C, et al. 10-year long-term survival (LTS) of induction chemotherapy with three cycles cisplatin/paclitaxel followed by concurrent chemoradiation cisplatin/etoposide/45 Gy (1.5 Gy bid) plus surgery in locally advanced non-small-cell lung cancer (NSCLC)-a multicenter phase-II trial (CISTAXOL). Lung cancer. 2013;82(1):83–89. | ||
De Marinis F, Nelli F, Migliorino MR, et al. Gemcitabine, paclitaxel, and cisplatin as induction chemotherapy for patients with biopsy-proven Stage IIIA (N2) nonsmall cell lung carcinoma: a Phase II multicenter study. Cancer. 2003;98(8):1707–1715. | ||
Schallier D, Bral S, Ilsen B, et al. Final overall results of a study with a novel triplet induction chemotherapy regimen (PACCAGE) followed by consolidation radiotherapy in locally advanced inoperable non-small cell lung cancer (NSCLC). J Thorac Oncol. 2009;4(6):728–735. | ||
Marulli G, Verderi E, Zuin A, et al. Outcomes and prognostic factors of non-small-cell lung cancer with lymph node involvement treated with induction treatment and surgical resection. Interact Cardiovasc Thorac Surg. 2014;19(2):256–262; discussion 262. | ||
Ramnath N, Dilling TJ, Harris LJ, et al. Treatment of stage III non-small cell lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143(5 Suppl):e314S–e340S. | ||
Weder W, Collaud S, Eberhardt WE, et al. Pneumonectomy is a valuable treatment option after neoadjuvant therapy for stage III non-small-cell lung cancer. J Thorac Cardiovasc Surg. 2010;139(6):1424–1430. | ||
Ghi MG, Paccagnella A, Ferrari D, et al. Concomitant chemoradiation (CRT) or cetuximab/RT (CET/RT) versus induction Docetaxel/Cisplatin/5-Fluoruracil (TPF) followed by CRT or CET/RT in patients with Locally Advanced Squamous Cell Carcinoma of Head and Neck (LASCCHN). A randomized phase III factorial study (NCT0186826). J Clin Oncol. 2014;32:5s(abstr 6004). |
Supplementary materials
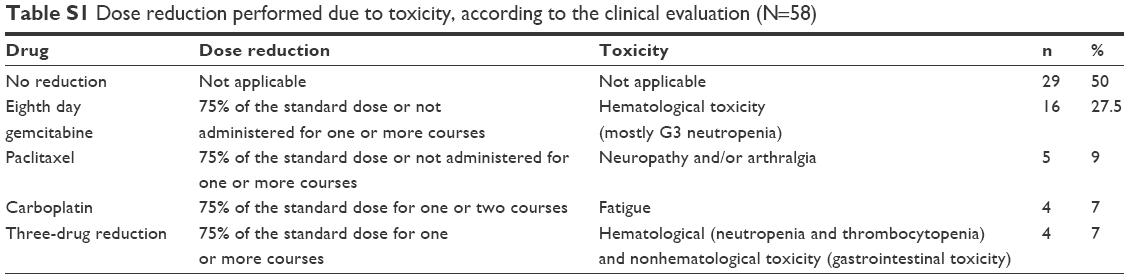 | Table S1 Dose reduction performed due to toxicity, according to the clinical evaluation (N=58) |
 | Table S2 Correlation between radiological response and the performance of radical-intent surgery or radiotherapy |
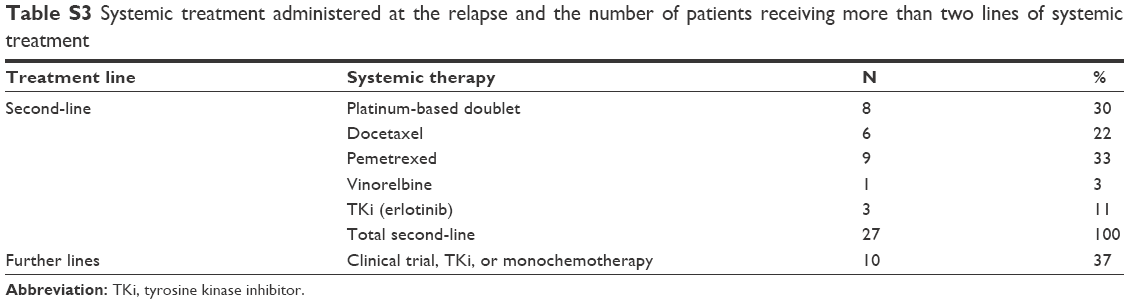 | Table S3 Systemic treatment administered at the relapse and the number of patients receiving more than two lines of systemic treatment |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.