Back to Journals » Vascular Health and Risk Management » Volume 17
Radiofrequency Ablation for Axial Reflux Associated with Foam Sclerotherapy for Varicosities in One-Step Approach: A Prospective Cohort Study Comprising Large Diameters Saphenous Veins
Authors Poschinger-Figueiredo D ![]() , Virgini-Magalhães CE
, Virgini-Magalhães CE ![]() , Porto LC
, Porto LC ![]() , Amorim CS, de Araujo Gomes CF
, Amorim CS, de Araujo Gomes CF ![]() , Riguetti-Pinto CR
, Riguetti-Pinto CR ![]() , Mayall MR
, Mayall MR ![]() , de Castro LS, Fagundes FB
, de Castro LS, Fagundes FB
Received 31 March 2021
Accepted for publication 2 June 2021
Published 2 July 2021 Volume 2021:17 Pages 379—387
DOI https://doi.org/10.2147/VHRM.S313282
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Harry Struijker-Boudier
Douglas Poschinger-Figueiredo,1 Carlos Eduardo Virgini-Magalhães,1,2 Luís Cristóvão Porto,3,4 Claudia Salvador Amorim,1 Cristiane Ferreira de Araujo Gomes,1 Cristina Ribeiro Riguetti-Pinto,1,2 Monica Rochedo Mayall,1 Leonardo Silveira de Castro,1 Felipe Borges Fagundes1
1Teaching and Health Care Unit of Vascular and Endovascular Surgery’s Medical Staff, Pedro Ernesto University Hospital (HUPE), Rio de Janeiro State University (UERJ), Rio De Janeiro, Brazil; 2Medical Sciences College (FCM), Rio de Janeiro State University (UERJ), Rio de Janeiro, Brazil; 3Histocompatibility and Cryopreservation Laboratory (HLA), Rio de Janeiro State University (UERJ), Rio de Janeiro, Brazil; 4Roberto Alcantara Gomes Biology Institute (IBRAG), Rio de Janeiro State University (UERJ), Rio de Janeiro, Brazil
Correspondence: Douglas Poschinger-Figueiredo
Teaching and Health Care Unit of Vascular and Endovascular Surgery’s Medical Staff, Pedro Ernesto University Hospital (HUPE), Rio de Janeiro State University (UERJ), Boulevard Vinte e Oito de Setembro, N 77, 4th Floor, Vila Isabel, Rio De Janeiro, RJ, 20551– 030, Brazil
Tel +55 21 2686-8643
Fax +55 21 2587-4010
Email [email protected]
Objective: This study assessed the outcomes and impact on the quality of life following one-step outpatient radiofrequency ablation (RFA) and ultrasound guided foam sclerotherapy (USGFS) for large reflux with varicosities in the great saphenous vein (GSV).
Design: Prospective, single-centre, analytical cohort.
Materials and Methods: Thirty symptomatic patients having reflux in the GSV and varicosities (CEAP C3 to C6) were treated with RFA and USGFS simultaneously, in a single-step procedure, from March 2016 to December 2016. They were followed up at 1 week, 6 months, 1 and 3 years. Clinical outcomes, changes in the Quality of Life (QOL) questionnaires SF-36™, VCSS and AVVQ, evolutive vein occlusion rates were assessed by duplex ultrasound, and ulcer closure was checked.
Results: The sample was divided into two groups: (Group 1) GSV diameter ≥ 13.0 mm (median 19.0 [14– 24]), 17 subjects, and (Group 2) GSV diameter ≤ 12.9 mm (median 10.3 [10– 12]), 16 subjects. No major adverse event was observed, and the postoperative minor adverse event rates were similar between the two groups. A significant improvement was observed in VCSS and AVVQ from the preoperative levels to the sixth month and the third-year follow-up. Twelve of 13 ulcers had healed at 1 year and remained closed until 3 years. The entire sample had a significant increase in all short form 36 domains, except for mental health in the Group 2 (GSV ≥ 13.0 mm). Overall first week occlusion rate for the whole sample was 90.9% and 69.7% at the 3-year follow-up. No difference in occlusion rate was observed between the two groups at any time.
Conclusion: Exclusively outpatient combined techniques were safe and feasible in this study with no major adverse events, despite the large diameters of the GSV or ulcer presence. Within 3 years, both diameter groups showed equivalent improvement in all QOL parameters, satisfactory axial occlusion, and maintained ulcer closure.
Keywords: saphenous vein, varicose veins, varicose ulcer, quality of life, catheter ablation, sclerotherapy
Introduction
Worldwide reports of prevalence estimates that Chronic Venous Disease (CVD) varies from <1–73% and Chronic Venous Insufficiency (CVI) from <1%–40%.1
In the early twentieth century, Professor William Babcock developed High Ligation and Stripping (HL/S) of Great Saphenous Vein (GSV) technique,2 which was widely used to treat axial reflux with marked improvement in the quality of life.3,4
Currently, treatment for varicose veins has undergone significant changes following the introduction of new, less invasive techniques with better clinical results.5,6 Several guidelines advocate endovenous thermal ablation, with laser or radiofrequency as the first-line treatment, followed by Ultrasound Guided Foam Sclerotherapy (USGFS) and HL/S as the third option to treat the axial disease, and USGFS as the first option for treating varicose veins.7–11
In cases that require treatment of both, GSV reflux and varicosities, many surgeons postpone the USGFS as the second step, to be performed weeks after the main axial thermal ablation surgery.12,13 This traditional approach requires more resources, repeated medical visits, and more time.14
A combined procedure with Radiofrequency Ablation (RFA) and USGFS, is safe and successful and can become an important treatment option.15,16 However, there are limited data on the efficacy and safety of this combined procedure in patients with large GSV diameters.
The study aims to evaluate the safety, clinical outcomes, impact on the quality of life, rate of ulcer closure, and the rate of occlusion of GSV following radiofrequency ablation associated with USGFS, to treat varicosities in a one-step outpatient basis approach in a cohort of patients with different GSV diameters.
Materials and Methods
Study Overview
Approval of this prospective non-randomized cohort study was granted by the Pedro Ernesto University Hospital Research Ethics Committee, and was conducted in accordance with the Declaration of Helsinki. (CAEE: 16437219.1.0000.5259). The Brazilian Health System supported the viability of the research. The same team of experienced surgeons performed all procedures at the university’s ambulatory surgery centre. The physicians involved in direct patient care managed data entry. The authors take responsibility for adherence to the protocol, reported data, and the analyses.
Patients
A cohort of 30 subjects who required treatment for varicose veins, were sequentially recruited from March to November 2016, during consultation at the university’s vascular surgery clinic in Rio de Janeiro.
Inclusion criteria were age between 18 and 65 years, ASA physical status 1 or 2,17 the presence of primary symptomatic varicose veins greater than 3 mm in diameter,9 Clinical Etiologic Anatomic Pathophysiologic (CEAP) class 3 or higher,18 GSV diameter in the mid-thigh at least 6 mm, from intima to intima, away from focal dilatation, with reflux greater than 0.5 seconds measured by Doppler ultrasonography in the standing position after calf compression/release, and willingness to provide written informed consent.
Exclusion criteria were a history of peripheral arterial disease, ankle brachial pressure index below 0.9, pregnancy, a history of thrombophilia, previous deep vein thrombosis, pulmonary embolism, thrombophlebitis of the GSV, current cancer, immobility, absolute contraindications to the use of foam19 or tortuosity rendering the GSV unsuitable for catheter progression.
Participants matching the inclusion criteria were concurrently referred for the first consultation, the baseline data collection, QOL questionnaire filling and duplex analysis.
Assessments
At the time of inclusion in the study as well as at each follow-up assessment, patients’ clinical history was collected, and they were submitted to physical exam and duplex ultrasonography. Data about the CEAP clinical class, the Visual Analogue Scale (VAS) score evaluated for pain after venous physical or chemical ablation,20 the Venous Clinical Severity Score (VCSS)21 and the Aberdeen Varicose Veins Questionnaire (AVVQ)22 were also documented. The Medical Outcome Study Short Form 36 (SF-36™)23 was administered during the first examination (preoperative) and six months after the intervention. The patients were followed up on the 7th day, six months, one, two and three years after the procedure.
An occluded or absent GSV was defined as technical success. If a segment length greater than 10 cm with flow or reflux was seen in a previously occluded GSV, it was defined as axial vein recanalisation.5
Study Treatment
The RFA was performed using the ClosureFast™ (Medtronic, San Jose, CA, USA) catheter according to the described technique.24 A point just below the knee was preferred for cannulation; however, a distal segment of reflux in GSV in the thigh was also acceptable. After advancing the catheter tip until 2 cm below the saphenofemoral junction, the Cold Tumescent Anaesthesia (CTA),25 a formula derived from Klein’s Solution26 containing epinephrine, lidocaine, and saline, was injected manually in the saphenous compartment at a rate of 10 mL/cm through a 22 G x 88 mm needle. All steps were performed under ultrasound guidance.
Each patient underwent two cycles of ablation at 120º C for 20 seconds in the first segment of the GSV and one cycle per segment until the last segment in the thigh during the withdrawal of the catheter.
Next, USGFS of the varicosities was performed under 26 G needle (Descarpack, São Paulo, Brazil) spot anaesthesia to minimise puncture discomfort. The foam was prepared according to the Tessari’s technique27 in a ratio of 2-mL polidocanol (Polidocanol; Victa Manipulation Laboratory; São Paulo; Brazil) to 4-mL air, in which 1.5 to 3.0% polidocanol concentration was used according to the size of the varicosities. The estimate cylinder volume was used to guide the solution administration and no more than 10 mL was injected per session.19 A butterfly needle 23 G (Descarpack, São Paulo, Brazil) was used to inject the foam into the varicosities under Duplex ultrasound guidance and control. Varicose vein entry spot far from the saphenous confluence was preferred to avoid the polidocanol chemical effect in GSV. Direct injection into the saphenous trunk was not part of the protocol.
Light compression sterile bandage was applied with 48h programmed removal after the procedure. General postoperative self-care orientation and a direct contact to anticipate the first assessment, to inform an adverse event or to report unstoppable pain was provided. Both RFA and USGFS procedure were done entirely on an outpatient basis and in a single-step approach.
Groups According to the GSV Calibre
The patients were split into two groups according to the greatest GSV truncal Calibre and the total treated limbs group median diameter was used as the cut-off point. They were compared for adverse events, postoperative pain, quality of life questionnaires, ulcer closure, and venous occlusion rates. The objective of splitting the groups was to maximise the analyses of possible outcomes for GSV with extra-large diameters.
Statistical Analysis
Descriptive analysis shows measures of central tendency and range for the numeric data or frequency and percentage for the categorical variables. Some numeric variables did not exhibit a Gaussian distribution; hence, they were expressed as median and interquartile range (IQR). To assess the normality of data distribution to the 5% level, we used histogram’s graphical analysis and the Shapiro Wilk’s test. All reported P values are 2-sided, and P < 0.05 was considered to infer statistical significance.
Baseline variables between the groups were compared using independent samples t-test or Mann–Whitney U-test for numeric measures and chi-square test (χ2) or Fisher’s exact test for categorical variables. The latter tests were also used to analyse differences in the occurrence of postoperative adverse events.
For longitudinal analysis of VCSS, AVVQ, VAS, and SF-36, the Mann–Whitney U-test was used for comparison between the groups. To evaluate the evolution of VCSS, AVVQ, and VAS through time, we used the Friedman’s ANOVA test.28 Nemenyi’s test was performed to analyse differences in the three variables of postoperative assessments.29 To analyse the short form 36 scores, we used the Wilcoxon signed-rank test. For increasing the statistical power and consistency of the results, data of three VCSS and AVVQ assessments were analysed, namely, preoperative, six months and 3-year postoperative. The VAS and occlusion rate were assessed on the 7th day, six months, and 3-year postoperative. Short form 36 was assessed preoperatively and at six months postoperatively compared. Postoperative adverse events were evaluated at each follow-up.
To evaluate GSV occlusion rate alterations over time, we used repeated measures of categorical data ANOVA according to The CATMOD Procedure of SAS™ software.30 Corrected McNemar test was used to identify differences between the groups at specific time points.
The data analysis for this paper was performed using SPSS, Version 26.0 and SAS™ software, Version 6.11 (SAS Institute Inc., Cary, NC, USA).
Results
In the total sample of 30 participants, 33 treated limbs were split into two groups: (1) those with GSV diameter of 13.0 mm or more (median 19.0 [14–24]) with 17 subjects, and (2) those with maximum diameter up to 12.9 mm (median 10.3 [10–12]), with 16 subjects. Due to the small number of bilaterally treated limbs, no impact was observed on analysis using treated legs instead of treated patient.
Baseline Variables
The descriptive baseline variables were compared between the groups. Except for a higher proportion of subjects with a family history of CVD in the GSV ≤ 12.9 mm group (p < 0.05), there were no other differences in the homogeneity (Table 1) between the groups.
 |
Table 1 Baseline Characteristics of the Included Participants in a Total of Treated Limbs and Divided According to the Great Saphenous Vein Diameter Range |
Adverse Events and Other Complications
In the immediate postoperative period, there were no cases of malaise, flush, allergy, neck constriction, cough, chest or neurological symptoms. One patient complained of transient pain, which resolved without medications. No contact for anticipates the scheduled assessment, to inform unstoppable pain or impaired walking abilities occurred within the first postoperative week.
On the seventh postoperative day (D7), 4/33 limbs developed symptomatic superficial varicosities thrombophlebitis and required non-steroidal anti-inflammatory drugs (NSAIDs) without coagulum drainage (GSV ≥ 13.0 mm: 3/4; GSV ≤ 12.9 mm: 1/4 [p = 0.32]). Symptoms were absent at 6-month follow-up (D180).
Thigh bruising on the medial side was present on D7 in 13/33 limbs (GSV ≥ 13.0 mm: 4/13; GSV ≤ 12.9 mm: 9/13 [p = 0.06]) and was absent at D180. Hyperpigmentation was seen on D180 in 14/33 limbs (GSV ≥ 13.0 mm: 8/14; GSV ≤ 12.9 mm: 6/14 [p = 0.58]) and at 3 years in 9/33 limbs (GSV ≥ 13.0 mm: 5/9; GSV ≤ 12.9 mm: 4/9 [p = 0.54]). Clinical residual or recurrent varicose veins were seen on D7 in 14/33 (GSV ≥ 13.0 mm: 6/14; GSV ≤ 12.9 mm: 8/14 [p = 0.39]), on D180 in 21/33 (GSV ≥ 13.0 mm: 11/21; GSV ≤ 12.9 mm: 10/21 [p = 0.90]) and at 3 years in 25/33 limbs (GSV ≥ 13.0 mm: 14/25; GSV ≤ 12.9 mm: 11/25 [p = 0.31]).
There were no other adverse events such as oedema, skin burns, endothermal heat induced thrombosis (EHIT), deep vein thrombosis, pulmonary embolism, or death during the follow-up period.
The rate of postoperative adverse events between the two groups was similar.
VCSS, AVVQ, VAS, Ulcer Closure and Short Form 36
Table 2 presents the comparisons between the groups for each postoperative assessment and for each of them in the following time pairs: (a) preoperative and D180, (b) preoperative and 3 years and (c) D180 and 3 years. VAS had three analytical pairs, (a) D7 and D180, (b) D7 and 3 years and (c) D180 and 3 years. Short form 36 had one analytical pair: preoperative and D180 and is presented in Table 3.
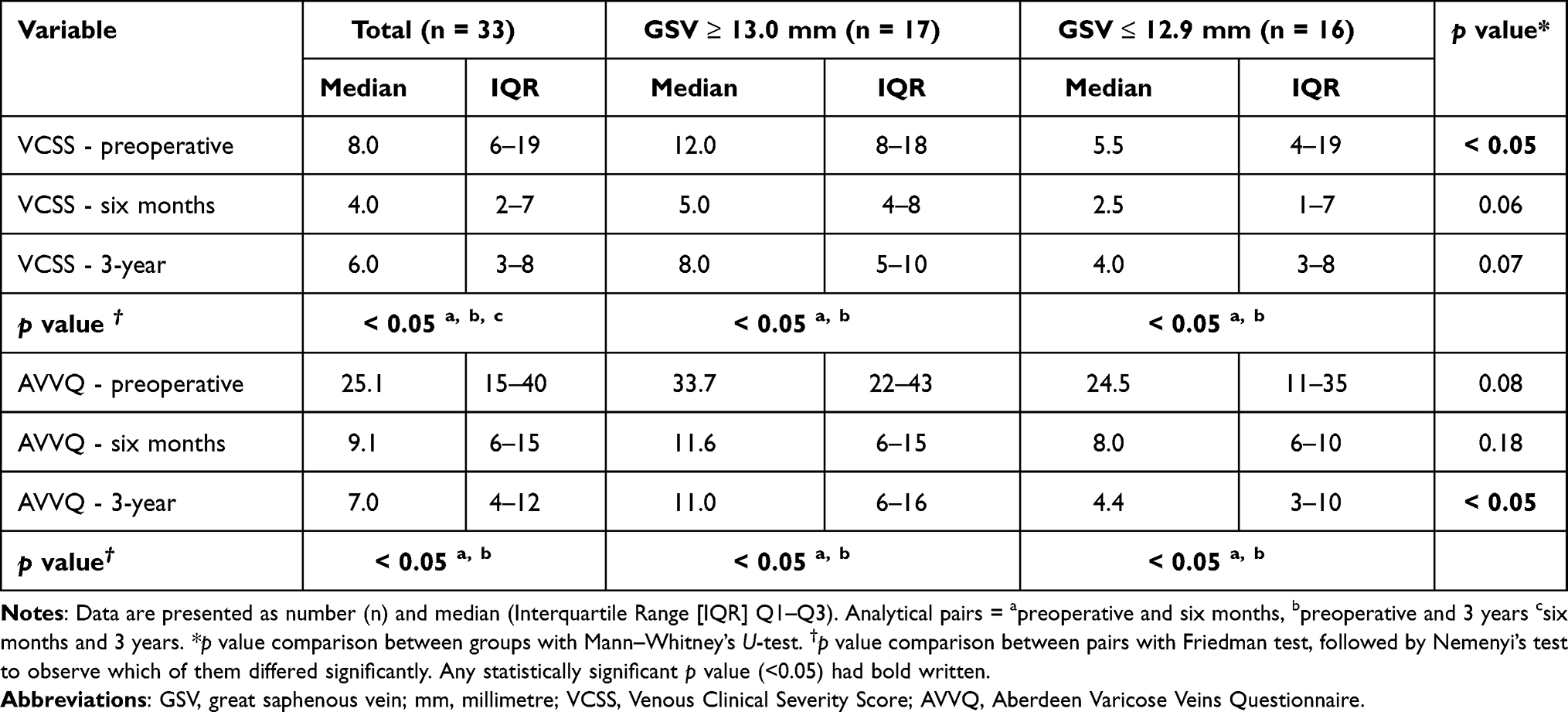 |
Table 2 Venous Clinical Severity Score and Aberdeen Varicose Veins Questionnaire Preoperative and Postoperative Values in a Total of Treated Limbs and Divided According to the Great Saphenous Vein Diameter Range |
 |
Table 3 Short Form 36 Preoperative and Postoperative Values in a Total of Treated Limbs and Divided According to the Great Saphenous Vein Diameter Range |
The total sample had median VAS scores as follows: D7 (2[0 4.5]); D180 and 3-year (0[0 0]). The GSV ≥ 13.0 mm group had median VAS scores as: D7 (2[0 5.0]); D180 and 3 years (0[0 0]). The GSV ≤ 12.9 mm group had median VAS scores as: D7 (0[0 2.8]); D180 (0[0 0.8]) and 3 years (0[0 0]). No significant reduction from D7 scores to D180 was observed and the VAS scores did not differ significantly between the groups at any assessment.
A significant improvement was seen in VCSS and AVVQ from preoperative to D180 and preoperative to 3 years, for the entire sample and in each group.
Except for significant worsening in VCSS in the total sample, no other differences were observed from D180 to 3-year postoperative assessments.
AVVQ measures at 3 years were higher in the GSV ≥13.0 mm group compared to the GSV ≤ 12.9 mm group.
In the D180 assessment, 11/13 ulcers had healed, which increased to 12/13 at one year assessment. There was no difference in the rate of ulcer closure or time to heal between the groups (p = 0.42).
There was a significant improvement in all short form 36 domains from preoperative to D180 in the total sample and in the GSV ≥13.0 mm group, except for the mental health domain in the latter. The GSV ≤ 12.9 mm group had a statistically significant improvement in Physical Functioning, Role Physical, Role Emotional, Vitality and Health Change. The GSV ≥13.0 mm group had higher Health Change values than the GSV ≤ 12.9 mm group.
Great Saphenous Vein Occlusion
The rate of GSV occlusion at D7 postoperative assessment was 30/33 in the entire sample (Table 4). No difference in occlusion rate was observed between the two groups on follow-up assessments. Within each group, no difference was observed when pairs in time were compared, except for the total sample itself, which presented a significant decrease in the rate of occlusion from D7 postoperative to 3-year postoperative (p < 0.05). One case of axial occlusion failure required additional USGFS session after one month and two cases with clinical recurrence were seen at one year postoperative assessment.
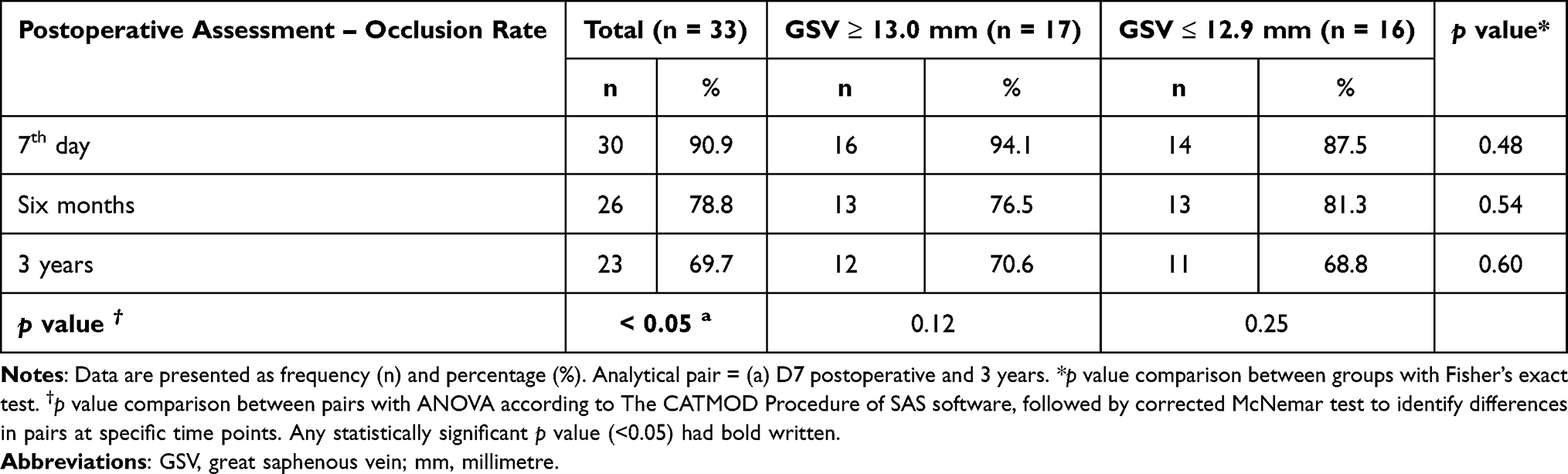 |
Table 4 Postoperative Occlusion Rates in a Total of Treated Limbs and Divided According to the Great Saphenous Vein Diameter Range |
Among the seven patients with an initial axial well-succeed ablative treatment in the 7th day, followed by GSV occlusion failure at six months or three-year postoperative assessments, three experienced important proximal stump reflux increases, defining occlusion failure. No additional significant proximal stump reflux length increase was observed in the total group of patients.
Six cases of perforator veins with reflux were treated with no ultrasonographical recurrence until the third year of follow-up.
Discussion
The uncommonly wide diameters observed in this study could be accounted to the tertiary centre profile and treatment delay, allowing disease’s progression and venous enlargement.31 Such measures are unfrequently seen in developed countries, as observed in a recognised observational cohort study conducted in the United Kingdom, with a maximum referred venous diameter of 9.2 mm.32
The rate of thrombophlebitis on the seventh day postoperative could be associated with inflammation related to the polidocanol sclerotherapy technique.5,33 All four cases of thrombophlebitis in the study had an extra clinical assessment at one month and were asymptomatic for this adverse event. Bruising was not an element of concern among participants, but highly observed in some until the end of the first month.
Almost half of the legs treated were of Mixed or Afro-Latin American individuals, a known risk factor for hyperpigmentation, contributing to the higher observed in the study. Series with higher rates of Caucasian individuals usually presents a lower hyperpigmentation incidence range of 10–30% and diminish over time.34 The GSV diameter cannot be considered a risk factor since no statistical difference was seen; however, more information is required about the incidence in these individuals.
Residual or recurrent varicose veins were cumulatively seen in 76% of the limbs, probably due to the limited amount of foam up to 10 mL injected per session.19 It is supported by an initial rate of 42% residual varicose veins in the D7 postoperative assessment. In the absence or improvement of remaining symptoms, conservative treatment was followed. Despite the discrepant diameter measures seen, there was no difference in the recurrence rate between the groups.
A recently published systematic review with meta-analysis including 6915 limbs treated in single or in multiple stages showed no difference in the safety profile.35 In this study, the absence of major adverse events, equivalent minor adverse events and outcomes in both groups suggests that the ambulatory combined intervention could be feasible and safe for several GSV diameters. The feasibility of offering a safe and less invasive treatment, even for highly symptomatic patients with wider GSV, with or without open ulcer, is a considerable achievement.
Preoperatory QOL comparison findings converge with a recent systematic review observation, where truncal venous diameter is not directly linked to AVVQ and short form 36 clinical scales. Otherwise, a VCSS worst median was observed in the broader GSV group, following the same study conclusions.36
We observed a substantial early postoperative improvement in the Quality of Life (QOL) questionnaires, AVVQ, VCSS and short form 36 in the overall sample and in both groups, reinforcing previous reports about the potential for marked improvement after axial treatment.37 The low total sample VCSS score was not maintained from six months to three years, perhaps due to increasing recurrence of reflux and varicose veins. A valid strategy to prevent the scale downsize could be sclerotherapy of all remaining varicosities despite satisfactory clinical achievements.
Both, AVVQ and short form 36, showed significantly better or comparable results in both groups indicating the feasibility of combined treatment even for broad GSV diameters. The relatively greater improvement of quality of life until the third year in the subgroup with more severe disease, reinforces the relevance of treating axial disease with varicosities despite the anatomical odds against expected success. The high rate of ulcer healing, with equivalent results between the groups reaffirms this strategy.
The axial recanalisation can reach rates greater than 30% in a GSV treated with a thermal ablation technique.38 This study observed significant GSV occlusion rates reduction in the total sample and a statistical tendency of axial reflux recurrence inside the groups. However, no difference appeared between the groups rate comparisons.
One limb with an ulcer in the GSV ≥13.0 mm group, in which the reflux persisted since the D7 assessment, did not heal. Nevertheless, all other leg ulcers healed in the first year and remained closed until the third year assessment. The correlation between reduction in GSV occlusion rate and maintained ulcer closure is unclear and needs further research.39 Initial truncal reflux treatment might be necessary to achieve sustained healing over time in this group.
The statistical comparison between the groups has a limited strength due to the small sample size and the study design; nevertheless it indicates that large GSV diameters are not an absolute limitation for low adverse events, perform a secure treatment, achieve greater improvements in QOL, and comparable rates of ulcer closure.
In this study, the outpatient combined technique was safe and feasible in this population with no major adverse events, despite the large diameters of GSV and a considerable proportion of leg ulcers. Within the third year, the total sample and both saphenous vein diameter range subgroups showed equivalent improvement in VAS, VCSS, and AVVQ quality of life questionnaires, satisfactory axial occlusion, and maintained ulcer closure.
Acknowledgments
The authors thank their colleagues in the Teaching and Health Care Unit of Vascular and Endovascular Surgery for all diligent work done throughout the time of the study.
Disclosure
The authors reported no conflicts of interest for this work.
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
References
1. Beebe-Dimmer JL, Pfeifer JR, Engle JS, Schottenfeld D. The epidemiology of chronic venous insufficiency and varicose veins. Ann Epidemiol. 2005;15(3):175–184. doi:10.1016/j.annepidem.2004.05.015
2. Laios K. Professor William Wayne Babcock (1872–1963) and his innovations in surgery. Surg Innov. 2018;25(5):536–537. doi:10.1177/1553350618781618
3. Durkin M, Turton EP, Wijesinghe L, Scott DJ, Berridge D. Long saphenous vein stripping and quality of life – a Randomised Trial. Eur J Vasc Endovasc Surg. 2001;21(6):545–549. doi:10.1053/ejvs.2001.1364
4. MacKenzie RK, Paisley A, Allan PL, Lee AJ, Ruckley CV, Bradbury AW. The effect of long saphenous vein stripping on quality of life. J Vasc Surg. 2002;35(6):1197–1203. doi:10.1067/mva.2002.121985
5. Rasmussen LH, Lawaetz M, Bjoern L, Vennits B, Blemings A, Eklof B. Randomized clinical trial comparing endovenous laser ablation, radiofrequency ablation, foam sclerotherapy and surgical stripping for great saphenous varicose veins. Br J Surg. 2011;98(8):1079–1087. doi:10.1002/bjs.7555
6. Nesbitt C, Bedenis R, Bhattacharya V, Stansby G. Endovenous ablation (radiofrequency and laser) and foam sclerotherapy versus open surgery for great saphenous vein varices. Cochrane Database Syst Rev. 2014;(7):CD005624. doi:10.1002/14651858.CD005624.pub3
7. Zimmet S. Recommendations for the referral and treatment of patients with lower limb chronic venous insufficiency. Phlebol J Venous Dis. 2011;26(3):89–90. doi:10.1258/phleb.2011.011e03
8. Gloviczki P, Comerota AJ, Dalsing MC, et al. The care of patients with varicose veins and associated chronic venous diseases: clinical practice guidelines of the society for vascular surgery and the American Venous Forum. J Vasc Surg. 2011;53(5):2S–48S. doi:10.1016/j.jvs.2011.01.079
9. Gloviczki P, Gloviczki ML. Guidelines for the management of varicose veins. Phlebology. 2012;27(Suppl 1):2–9. doi:10.1258/phleb.2012.012s28
10. Wittens C, Davies AH, Bækgaard N, et al. Editor’s choice – management of chronic venous disease. Eur J Vasc Endovasc Surg. 2015;49(6):678–737. doi:10.1016/j.ejvs.2015.02.007
11. Onida S, Davies AH. Varicose veins: diagnosis and management. Nurs Times. 2013;109(41):16–17.
12. Rasmussen L, Lawaetz M, Serup J, et al. Randomized clinical trial comparing endovenous laser ablation, radiofrequency ablation, foam sclerotherapy, and surgical stripping for great saphenous varicose veins with 3-year follow-up. J Vasc Surgery Venous Lymphat Disord. 2013;1(4):349–356. doi:10.1016/j.jvsv.2013.04.008
13. Brittenden J, Cooper D, Dimitrova M, et al. Five-year outcomes of a randomized Trial of treatments for varicose veins. N Engl J Med. 2019;381(10):912–922. doi:10.1056/NEJMoa1805186
14. Jarjous F, Jarjous R, Nahhas G. One-step approach to treating venous insufficiency. J Clin Med Res. 2015;7(9):681–684. doi:10.14740/jocmr2205w
15. Pihlaja T, Romsi P, Ohtonen P, Jounila J, Pokela M. Post-procedural compression vs. no compression after radiofrequency ablation and concomitant foam sclerotherapy of varicose veins: a randomised controlled non-inferiority Trial. Eur J Vasc Endovasc Surg. 2020;59(1):73–80. doi:10.1016/j.ejvs.2019.08.020
16. Cabrero Fernandez M, Martinez Lopez I, Hernandez Mateo MM, et al. Prospective study of safety and effectiveness in the use of radiofrequency ablation for incompetent great saphenous vein ≥12 mm. J Vasc Surg Venous Lymphat Disord. 2017;5(6):810–816. doi:10.1016/j.jvsv.2017.05.021
17. De Cassai A, Boscolo A, Tonetti T, Ban I, Ori C. Assignment of ASA-physical status relates to anesthesiologists’ experience: a survey-based national-study. Korean J Anesthesiol. 2019;72(1):53–59. doi:10.4097/kja.d.18.00224
18. Eklöf R, Bergan C, Gloviczki K, et al. Revision of the CEAP classification for chronic venous disorders: a consensus statement. Vasa. 2005;34(3):157–161. doi:10.1024/0301-1526.34.3.157
19. Rabe E, Breu F, Cavezzi A, et al. European guidelines for sclerotherapy in chronic venous disorders. Phlebol J Venous Dis. 2014;29(6):338–354. doi:10.1177/0268355513483280
20. Bond MR, Pilowsky I. Subjective assessment of pain and its relationship to the administration of analgesics in patients with advanced cancer. J Psychosom Res. 1966;10(2):203–208. doi:10.1016/0022-3999(66)90064-x
21. Rutherford RB, Padberg FT, Comerota AJ, Kistner RL, Meissner MH, Moneta GL. Venous severity scoring: an adjunct to venous outcome assessment. J Vasc Surg. 2000;31(6):1307–1312. doi:10.1067/mva.2000.107094
22. Garratt AM, Macdonald LM, Ruta DA, Russell IT, Buckingham JK, Krukowski ZH. Towards measurement of outcome for patients with varicose veins. Qual Health Care. 1993;2(1):5–10. doi:10.1136/qshc.2.1.5
23. Ware JE. SF-36 health survey update. Spine (Phila Pa 1976). 2000;25(24):3130–3139. doi:10.1097/00007632-200012150-00008
24. Proebstle TM, Vago B, Alm J, Göckeritz O, Lebard C, Pichot O. Treatment of the incompetent great saphenous vein by endovenous radiofrequency powered segmental thermal ablation: first clinical experience. J Vasc Surg. 2008;47(1):151–156.e1. doi:10.1016/j.jvs.2007.08.056
25. Ceccarino R, Di Micco R, Cappelletti R. Aesthetic breast surgery under cold tumescent anesthesia. Ann Plast Surg. 2019;83(4):384–387. doi:10.1097/SAP.0000000000001798
26. Klein JA. The tumescent technique for lipo-suction surgery. Am J Cosmet Surg. 1987;4(4):263–267. doi:10.1177/074880688700400403
27. Tessari L, Cavezzi A, Frullini A. Preliminary experience with a new sclerosing foam in the treatment of varicose veins. Dermatologic Surg. 2001;27(1):58–60. doi:10.1046/j.1524-4725.2001.00192.x
28. Hollander M, Wolfe A. Nonparametric Statistical Methods. New York: John Wiley & Sons, Ltd; 1973.
29. Nemenyi P. Distribution-Free Multiple Comparisons. Princepton University; 1963.
30. Stanish WM, Koch GG. The use of CATMOD for repeated measurement analysis of categorical data.
31. Hamel-Desnos CM, De Maeseneer M, Josnin M, et al. Great saphenous vein diameters in phlebological practice in France: a Report of the DIAGRAVES Study by the French Society of Phlebology. Eur J Vasc Endovasc Surg. 2019;58(1):96–103. doi:10.1016/j.ejvs.2018.09.011
32. Lane TRA, Varatharajan L, Fiorentino F, et al. Truncal varicose vein diameter and patient-reported outcome measures. Br J Surg. 2017;104(12):1648–1655. doi:10.1002/bjs.10598
33. Toniolo J, Chiang N, Munteanu D, Russell A, Hao H, Chuen J. Vein diameter is a predictive factor for recanalization in treatment with ultrasound-guided foam sclerotherapy. J Vasc Surgery Venous Lymphat Disord. 2018;6(6):707–716. doi:10.1016/j.jvsv.2018.05.029
34. Goldman MP, Sadick NS, Weiss RA. Cutaneous necrosis, telangiectatic matting, and hyperpigmentation following sclerotherapy etiology, prevention, and treatment. Dermatologic Surg. 1995;21(1):19–29. doi:10.1111/j.1524-4725.1995.tb00107.x
35. Aherne TM, Ryan ÉJ, Boland MR, et al. Concomitant vs. staged treatment of varicose tributaries as an adjunct to endovenous ablation: a systematic review and meta-analysis. Eur J Vasc Endovasc Surg. 2020;60(3):430–442. doi:10.1016/j.ejvs.2020.05.028
36. Tan MKH, Sutanto SA, Onida S, Davies AH. The relationship between vein diameters, clinical severity, and quality of life: a systematic Review. Eur J Vasc Endovasc Surg. 2019;57(6):851–857. doi:10.1016/j.ejvs.2019.01.024
37. García-Madrid C, Pastor Manrique JO, Gómez-Blasco F, Sala Planell E. Update on endovenous radio-frequency closure ablation of varicose veins. Ann Vasc Surg. 2012;26(2):281–291. doi:10.1016/j.avsg.2011.01.014
38. Donnell TFO, Balk EM, Dermody M, Tangney E, Iafrati MD. Recurrence of varicose veins after endovenous ablation of the great saphenous vein in randomized trials. J Vasc Surg. 2014;4(1):97–105. doi:10.1016/j.jvsv.2014.11.004
39. Gohel MS, Heatley F, Liu X, et al. A randomized trial of early endovenous ablation in venous ulceration. N Engl J Med. 2018;378(22):2105–2114. doi:10.1056/NEJMoa1801214
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.