")
Back to Journals » Research and Reports in Urology » Volume 14
Racial Disparities in Prostate Cancer Stage at Diagnosis Persist Despite Community Affluence
Authors Nemesure B, Scarbrough KH, Mermelstein L
Received 6 May 2022
Accepted for publication 6 August 2022
Published 30 August 2022 Volume 2022:14 Pages 305—312
DOI https://doi.org/10.2147/RRU.S371838
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Guglielmo Mantica
Barbara Nemesure,1 Kathleen H Scarbrough,1 Linda Mermelstein2
1Department of Family, Population and Preventive Medicine, Stony Brook Medicine, Stony Brook, NY, USA; 2Stony Brook Cancer Center, Stony Brook Medicine, Stony Brook, NY, USA
Correspondence: Barbara Nemesure, Department of Family, Population and Preventive Medicine, Stony Brook Medicine, 100 Nicolls Road, Stony Brook, NY, 11794, USA, Tel +1 631-444-1293, Fax +1 631-444-7525, Email [email protected]
Purpose: The aims of this investigation were to evaluate racial disparities in prostate cancer among men living in a relatively affluent community with access to high quality healthcare.
Patients and Methods: This retrospective study included 1363 cases with prostate cancer entered into the Stony Brook Cancer Center registry between 2010 and 2020. Demographic and other factors, including the Distressed Community Index (DCI) which provides an indicator of socioeconomic status by zip code, were analyzed as predictors of later stage disease using logistic regression.
Results: Approximately 60% of cases resided in a “prosperous” zip code (DCI< 20) with median (range) DCI of 16.3 (1.1, 61.8). Black men were diagnosed with later stage disease at a higher rate (p=0.03) and were more likely to be diagnosed at a younger age (p< 0.01) compared to White men. However, the distribution of cancer stage stratified by DCI and race did not differ among groups. Black men were 3 times more likely to have Medicaid and a history of diabetes, as well as 33% more likely to have hypertension than White men. Black race (OR=2.08, (1.26, 3.42)), older age (OR=2.56 (1.67, 3.90)) and current smoking (OR=1.61 (1.07, 2.42)) were significant contributors of later stage cancer.
Conclusion: Black men residing in a relatively affluent suburb were diagnosed at younger ages, later stages, and were more likely to have additional comorbidities compared to White men. This study highlights the complexity of the environmental, societal, and biological contributors to racial disparities that warrants further investigation into the underlying causes for the excess burden on Black men.
Keywords: prostate cancer, racial differences, risk factors, community-based
Introduction
Prostate cancer has the most pronounced racial disparities of all cancer types. Annual prostate cancer incidence in the US is 75% higher in Black men compared to White men (172.6 per 100,000 vs 99.9 per 100,000, respectively) and death rates are more than 2 times greater in the former group (37.9 per 100,000 vs 17.8 per 100,000, respectively).1 While socioeconomic status (SES) and access to quality healthcare have been implicated as key contributors to the increased prostate cancer burden on Black men, these factors do not fully explain the noted disparities. According to the US census, Hispanic men were 1.7 times more likely than Black men and 3.2 times more likely than White males to be uninsured,2 yet despite these notable differences in access to care, prostate cancer incidence and mortality among Hispanic men is less than half the rates of Black men (incidence: 85.3 per 100,000; mortality: 15.6 per 100,000).1
Prostate cancer health disparities are likely the result of a complex multifactorial array of environmental factors, social determinants, and biological contributors. Although some studies have reported differences in rates of mortality associated with varying levels of SES,3,4 several investigations including men enrolled in the Veterans Affairs (VA) equal-access medical system found similar survival rates among Black and White veterans with prostate cancer who received their care within this infrastructure.5–8 The VA system represents a unique construct of healthcare delivery in the US and may not be representative of prostate cancer related outcomes in the general population. The purpose of this investigation was to provide data that will assist in evaluating racial disparities in prostate cancer among men who live in a relatively affluent community in the Northeast with access to high quality medical care.
Material and Methods
Stony Brook University Hospital (SBUH) is located in Suffolk County, New York. This Northeastern suburb located on Long Island includes approximately 1.5 million residents of which 84% are White, 9% are Black, and 7% are from other racial/ethnic backgrounds.9 More than 90% of adults residing in Suffolk have graduated high school and the median household income in the county is $101,031.
The affiliated Stony Brook Cancer Center maintains a registry that captures demographic and medical history information, as well as cancer histology and staging data for all patients diagnosed with any type of cancer at SBUH. This retrospective study included all prostate cancer cases entered into the registry between 2010 and 2020. The data abstracted from the repository included age at diagnosis, year of diagnosis, race, marital status, type of insurance coverage, family history of cancer, tobacco history, history of alcohol consumption, ICD 9 and ICD 10 codes for history of diabetes and hypertension,10 stage of cancer, and patient zip code at time of diagnosis.
The Distressed Community Index (DCI) is an interactive web-based tool which provides an indicator of socioeconomic status (SES) for regions in the US.11 A composite score based on economic and other factors compiled from the US census is assigned to each zip code with scores ranging from 0–100 such that higher values represent increased distress. Communities with DCI values <20 are considered “prosperous” while those >80 are defined as “distressed”. Each zip code in this study was paired with its corresponding DCI score and was used as a proxy to evaluate the impact of SES on the outcomes.
Statistical Analyses
Stage at diagnosis was defined using the American Joint Committee on Cancer (AJCC) guidelines.12 The American Society of Clinical Oncology (ASCO) provides the following staging framework:13 Stage I is defined as a small cancer that is confined to one area; Stages II and III are larger and have grown into nearby tissue or lymph nodes; Stage IV has spread to other parts of the body. Given these criteria, “early” stage was defined as stage 1 cancer in this investigation and “later” stage was considered stages 2 and above. Chi-squared tests were used to independently evaluate associations between stage and each potential risk factor, as well as associations between race and each variable. Logistic regression was used to determine predictors of late stage disease at the time of diagnosis. Factors from the univariate analyses with p<0.10 were included in the multivariate logistic models which were further adjusted by year of diagnosis. Odds ratios (ORs) and 95% confidence intervals (CIs) are presented. SPSS version 21 was used to conduct these analyses.
The Stony Brook University Institutional Review Board (IRB) approved this study (IRB #2021-00479) and the committee waived ascertainment of informed consent since the investigation did not include personal identifiers. The guidelines in the Declaration of Helsinki were upheld.
Results
This investigation of 1363 men diagnosed with prostate cancer at Stony Brook Cancer Center between 2010 and 2020 included 131 (9.6%) Black and 1134 (84.7%) White men, along with 78 males (5.7%) of other racial/ethnic backgrounds. Table 1 presents the demographic and medical history characteristics of the cohort, stratified by stage at diagnosis. Twenty-nine percent (n=395) of the cases were diagnosed at an early stage and these men were significantly more likely to be younger than those presenting with more advanced disease (p<0.01). Additionally, Black men tended to be diagnosed with later stage disease compared to those in the other groups (p=0.03).
 |
Table 1 Demographic and Personal History Characteristics of 1363 Prostate Cancer Cases Diagnosed at Stony Brook Cancer Center Between 2010 and 2020, Stratified by Stage (Early vs Late) |
This study included 124 zip codes. Indicators of SES showed high levels of affluence in this community with a median (range) DCI of 16.3 (1.1, 61.8) and more than 95% of the cases having some type of medical insurance. DCI ranged from 2.5 to 61.8 among Black men with a median score of 28.2, while the range for White men was 1.1 to 61.8 with a median of 14.9. Although DCI was not associated with stage at diagnosis, type of insurance coverage was significantly related to disease stage at presentation (p<0.01). Among individuals residing in the most affluent communities (DCI<20), 42.9% of Black men had managed care insurance and 26.2% were covered by Medicare. Among White men with DCI<20, 35.3% maintained managed care coverage and 57.4% utilized Medicare. A significant positive association was also found with a history of tobacco use (p=0.01), while a marginal inverse relationship was noted for a history of alcohol consumption (p=0.06). Stage at diagnosis was unrelated to marital status, family history of cancer and history of diabetes and hypertension.
Table 2 presents the distribution of prostate cancer risk factors stratified by race. The findings indicate that Black men were significantly more likely to be diagnosed at a younger age (<60 years) than White men (38.9% vs 21.7%, p<0.01) and that approximately 60% of the former group were married compared to more than 75% in the other 2 groups (p<0.01). While 9.3% of Black men did not have insurance coverage, this proportion was significantly higher than among White men (p<0.01). Additionally, Black and Other men were 3 times more likely to have Medicaid as their primary insurance plan. The distribution of DCI was also significantly different among the groups with 61.8% of White men living in a “prosperous” zip code compared to 33.1% of Black men (p<0.01). There was no difference in tobacco history between the groups, however White men were significantly more likely than other groups to consume alcohol (p<0.01). With respect to comorbidities, Black men were 3 times more likely than the other 2 groups to have a history of diabetes (p<0.01) and almost twice as likely as non-Whites to have hypertension (p=0.01).
 |
Table 2 Demographic and Personal History Characteristics of 1363 Prostate Cancer Cases Diagnosed at Stony Brook Cancer Center Between 2010 and 2020, Stratified by Race |
Although an association was noted between race and DCI, the distribution of early vs late stage cancer stratified by these 2 other variables did not yield any significant findings (Table 3). Table 4 presents the full logistic regression models for prostate cancer severity (early vs late stage) by factors found to be significant in the univariate analyses. The findings indicate that older age (70+ years; (OR=2.56 (1.67, 3.90))), Black race (OR=2.08, (1.26, 3.42)) and a history of smoking (current smokers: OR=1.61 (1.07, 2.42); former smokers: OR=1.35 (1.02, 1.77)) were significant risk factors for late stage of diagnosis. While type of insurance coverage did not predict the outcome, alcohol consumption (at the time of diagnosis) was found to be a protective factor (OR=0.74 (0.55, 0.98)).
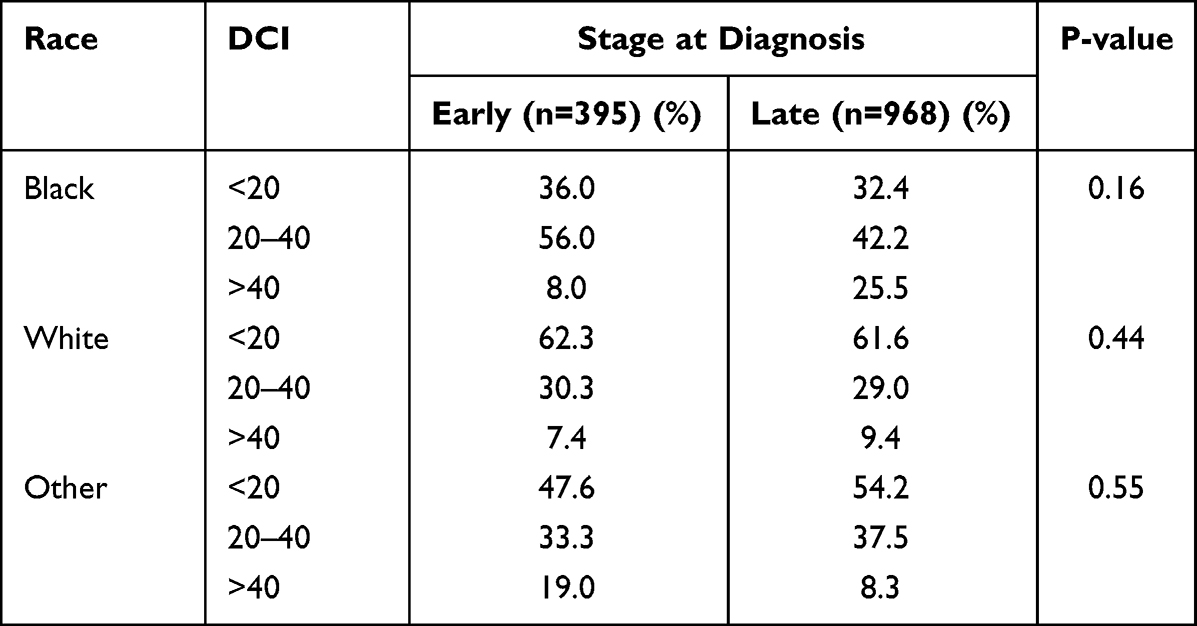 |
Table 3 Distribution of Early vs Late Stage Prostate Cancer Stratified by Race and Distressed Community Index (DCI) |
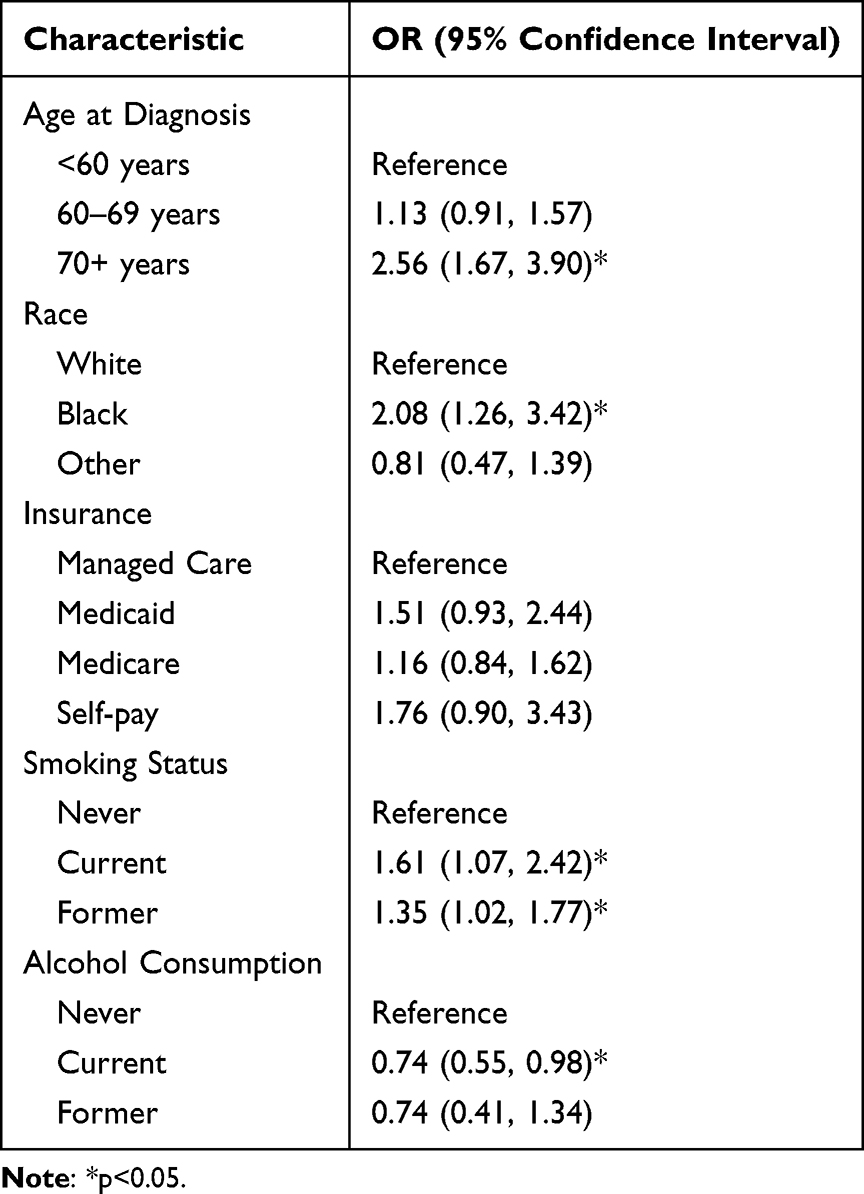 |
Table 4 Logistic Regression Models for Prostate Cancer Severity (Early vs Late Stage) at Diagnosis |
Discussion
Although prostate cancer incidence and mortality rates have declined nationally over the past 2 decades, mainly due to earlier detection and advances in treatment, significant racial disparities persist.1 In the present study, findings from the multivariable logistic regression models, based on more than 1300 men residing in a relatively affluent suburb in the Northeast, indicate that although insurance coverage was not a significant predictor of disease severity in this study, Black men were 2 times more likely than White men to be diagnosed at later stage of disease and were 1.8 times more likely to be diagnosed before the age of 60 years. The inverse was true for White men who were 1.8 times more likely to be diagnosed after the age of 70 years. These findings suggest that economic determinants may only be partially responsible for the racial inequities associated with prostate cancer.
The increased burden of prostate cancer among Black men compared to other groups is likely the result of a complex multifactorial interplay of social determinants, economic and lifestyle factors, environmental exposures and genetic contributors.14–16 Several retrospective studies utilizing the Veterans Affairs (VA) database evaluated whether a medical system which provides equal access to care would result in reduced racial disparities for prostate cancer.5–8 In one such investigation which included more than 60,000 veterans diagnosed with the disease, survival rates in Black men were found to be similar to those in White men.5 Likewise, in a large multi-cohort study of more than 300,000 prostate cancer cases (which also included a subset of data from the VA), Black men and White men who received equal access to care and standardized treatment protocols were found to have similar rates of prostate cancer-specific mortality.17
While the VA investigations support equities in survival with equal access to care, other studies have reported disparities in prostate cancer mortality rates with increases in SES.3,4 Death rates were shown to decrease among White men with increases in SES, however a similar trend was not found among more affluent Black men.
The present study used the DCI score as a proxy for SES to evaluate the impact of social determinants on prostate cancer outcomes. The DCI is based on the US Census statistics and utilizes 7 metrics (education (no high school diploma), poverty rate, unemployment rate, housing vacancy rate, median household income, and changes in numbers of employees and establishments located in the geographical location) to calculate a composite score to represent the economic well-being of a particular geographic location.11 An interactive map is available for more than 25,000 zip codes, thereby capturing 99% of the population in the US.
Findings from this investigation indicated that while the distribution of DCI scores differed among the racial/ethnic groups (Table 2), these differences did not significantly impact the stage of prostate cancer at diagnosis (Table 3). This may be due to the relative affluence in the overall community or perhaps the limited sample size of Black and Other men in the cohort.
Several studies have suggested that prostate cancer screening is lower among Black men compared to other groups,18–20 while other reports have indicated that such screening rates are comparable.21 Although economics and access to care have been implicated as key contributors to the reduced screening rates, these factors alone are not sufficient to explain the reduced screening rates among men of African descent. In a population-based study among older men, PSA screening rates among Black males persisted to be significantly lower even after adjustment for poverty level and comorbidities.22
Although prostate cancer screening data were not available for this study, an investigation to assess screening awareness in a convenience sample of men attending the Emergency Department at Stony Brook University Hospital during 2014–2015 revealed that among 470 men surveyed, 46% reported having had a digital rectal exam (DRE) and half indicated having had a prostate exam.23 The study did not report the screening findings stratified by race, however Black men were found to be equally as likely as White men to have heard of a prostate exam (93% in both groups) and were less likely to have heard of a DRE (70% vs 77%, respectively). Knowledge about prostate-specific antigen (PSA) testing was differentially low in both groups (54% among White men; 35% among Black men). While awareness of screening modalities does not necessarily equate to health seeking behaviors, this study suggests that racial disparities related to knowledge and prostate cancer screening practices may exist in this community.
A history of tobacco use was implicated as a risk factor for later stage of prostate cancer at diagnosis in the present investigation, however there were no statistically significant differences in smoking status between Black and White men in this study. Additionally, about 42% of men in both groups abstained from smoking prior to disease onset. As such, while a history of tobacco use may be a significant predictor of later stage of disease onset, the data do not support smoking status as a key explanatory factor for the noted racial disparities related to prostate cancer.
A growing evidence base is emerging to implicate genetic determinants as explanatory factors for the disparate rates of prostate cancer incidence and mortality between Black and White men. More than 250 single nucleotide polymorphisms (SNPs) have been implicated in prostate cancer pathogenesis.24 Differences in (epi)genetic alterations, immune system function, comorbidities and therapeutic resistance across races suggest an underlying biological mechanism that may help to partially explain the sub-optimal prostate cancer outcomes in the former group.16 In the largest genome wide association study of prostate cancer to date, Conti et al reported that among 107,247 cases and 127,006 controls, genetic risk was more than twice as high in Black men compared to their White counterparts.24 The authors further state that this finding was not commonly observed with other types of cancer, thus suggesting strong heritability for this disease. Additionally, DNA repair genes and androgen receptors (AR) have been differentially expressed in Black men with prostate cancer.16,25
While race is a social construct and not a biological variable and the present investigation did not directly evaluate genetic contributions to prostate cancer, the findings from this study may indirectly support a hypothesis of genetic variations for the noted disparities. Consistent with other studies, Black men in this investigation were diagnosed at a significantly younger age than White men.26 This earlier age of disease onset may indicate an underlying biological mechanism. Additionally, Black men were 3 times more likely to have a history of diabetes and 33% more likely to have a history of hypertension. While younger age at diagnosis and higher comorbidity rates may have various underlying genetic predispositions in different groups, we hypothesize that the impact of these factors on prostate cancer carcinogenesis is likely the result of a combination of both heredity and environment. It remains unclear, however, whether increased mortality among Black men is a consequence of the late diagnosis or something more systemic.27,28
Limitations
Although this study is among the first in the general (non-VA) population to evaluate prostate cancer racial disparities in a community with broad access to high quality healthcare, this investigation had several limitations. Most notably was the limited number of Black men included in the study. Although Black men only comprised about 10% of the study cohort, this distribution closely matched the county demographic, thus suggesting a decreased likelihood of selection bias. However, it should be noted that patients of mixed race, who may have different biological behaviors and genetic patterns, may consider themselves as Black. This investigation did not include a subgroup for mixed race men, which represents a second limitation of the study.
This study also lacked person-based SES data. While DCI was used as a proxy for economic well-being, zip code level data may not adequately reflect the true status of each patient. The direction of such inherent biases, however, are indeterminate and the multivariate models indicated that type of medical insurance coverage was not a significant predictor of later stage of disease in this investigation. These findings suggest that economics may not be the sole driver of prostate cancer racial disparities.
Additional limitations of the study also include its potential lack of generalizability to more ethnically and economically heterogeneous populations and the unavailability of data related to prostate cancer screening and suspected genetic determinants. Such potentially important risk factors are hypothesized to be key contributors to the noted racial disparities in prostate cancer.
Conclusion
Black men in this study, who reside in a relatively affluent suburb of New York, were diagnosed at an earlier age and with later stage of prostate cancer compared to White men. These findings highlight the complexity of the environmental, societal and biological contributors to the racial disparities of this disease and warrant further investigation to determine the underlying causes for the excess burden on Black men.
Funding
This work was funded through a grant from the Miriam & David Donoho Academy of Clinical and Educational Scholars (ACES).
Disclosure
The authors report no conflicts of interest in this work.
References
1. American Cancer Society. Available from: https://cancerstatisticscenter.cancer.org/#!/cancer-site/Prostate.
2. Keisler-Starkey K, Bunch L. Health insurance coverage in the United States: 2019; US Census Bureau current population reports; P60-271. 2020.
3. Cheng I, Witte JS, McClure LA, et al. Socioeconomic status and prostate cancer incidence and mortality rates among the diverse population of California. Cancer Causes Control. 2009;20(8):1431–1440. doi:10.1007/s10552-009-9369-0
4. Liu L, Cozen W, Bernstein L, Ross RK, Deapen D. Changing relationship between socioeconomic status and prostate cancer incidence. J Natl Cancer Inst. 2001;93(9):705–709. doi:10.1093/jnci/93.9.705
5. Riviere P, Luterstein E, Kumar A, et al. Survival of African American and non-Hispanic white men with prostate cancer in an equal-access health care system. Cancer. 2020;126(8):1683–1690. doi:10.1002/cncr.32666
6. Daskivich T, Kwan L, Dash A, Litwin M. Racial parity in tumor burden, treatment choice and survival outcomes in men with prostate cancer in the VA healthcare system. Prostate Cancer Prostatic Dis. 2015;18(2):104–109. doi:10.1038/pcan.2014.51
7. McKay RR, Sarkar RR, Kumar A, et al. Outcomes of Black men with prostate cancer treated with radiation therapy in the Veterans Health Administration. Cancer. 2021;127(3):403–411. doi:10.1002/cncr.33224
8. Berger AD, Satagopan J, Lee P, Taneja SS, Osman I. Differences in clinicopathologic features of prostate cancer between black and white patients treated in the 1990s and 2000s. Urology. 2006;67(1):120–124. doi:10.1016/j.urology.2005.08.005
9. United States Census. Available from: https://www.census.gov/quickfacts/fact/table/suffolkcountynewyork,nassaucountynewyork/PST045221.
10. Centers for Medicare and Medicaid Services. Available from: https://www.cms.gov/Medicare/Coding/ICD9ProviderDiagnosticCodes/codes.
11. Economic Innovation Group. Available from: https://eig.org/distressed-communities/.
12. Available from: https://www.cancer.org/cancer/prostate-cancer/detection-diagnosis-staging/staging.html.
13. Available from: https://www.cancer.net/navigating-cancer-care/diagnosing-cancer/stages-cancerAlso.
14. Pernar CH, Ebot EM, Wilson KM, Mucci LA. The epidemiology of prostate cancer. Cold Spring Harb Perspect Med. 2018;8(12):a030361. doi:10.1101/cshperspect.a030361
15. Chowdhury-Paulino IM, Ericsson C, Vince Jr., R, Spratt DE, George DJ, Mucci LA. Racial disparities in prostate cancer among black men: epidemiology and outcomes. Prostate Cancer Prostatic Dis. 2021;24:1–6. doi:10.1038/s41391-021-00451-z
16. Lowder D, Rizwan K, McColl C, et al. Racial disparities in prostate cancer: a complex interplay between socioeconomic inequities and genomics. Cancer Lett. 2022;531:71–82. doi:10.1016/j.canlet.2022.01.028
17. Dess RT, Hartman HE, Mahal BA, et al. Association of black race with prostate cancer–specific and other-cause mortality. JAMA Oncol. 2019;5(7):975–983. doi:10.1001/jamaoncol.2019.0826
18. Roberts LR, Wilson CM, Stiel L, Casiano CA, Montgomery SB. Prostate cancer screening among high-risk Black men. J Nurse Pract. 2018;14(9):677–682. doi:10.1016/j.nurpra.2018.07.005
19. Kearns JT, Adeyemi O, Anderson WE, et al. Contemporary racial disparities in PSA screening in a large, integrated health care system. J Clin Oncol. 2020;38:308. doi:10.1200/JCO.2020.38.6_suppl.308
20. Vince RA, Jamieson S, Mahal B, Underwood W. Examining the racial disparities in prostate cancer. Urology. 2021;S009042952100772X. doi:10.1016/j.urology.2021.08.004
21. Horton B, Alexeeff S, Prausnitz S, Avins AL, Presti J. Race-specific trends in prostate cancer screening and presentation before and after the 2012 United States Preventive Services Task Force Statement. Urol Pract. 2022;9(1):64–71. doi:10.1097/UPJ.0000000000000274
22. Gilligan T, Wang PS, Levin R, Kantoff PW, Avorn J. Racial differences in screening for prostate cancer in the elderly. Arch Intern Med. 2004;164(17):1858–1864. doi:10.1001/archinte.164.17.1858
23. Leonard JA, Wells JB, Brandler ES. Awareness of prostate cancer and screening modalities among long island men. Am J Mens Health. 2017;11(2):365–368. doi:10.1177/1557988316681219
24. Conti DV, Darst BF, Moss LC, et al. Trans-ancestry genome-wide association meta-analysis of prostate cancer identifies new susceptibility loci and informs genetic risk prediction. Nat Genet. 2021;53(1):65–75. doi:10.1038/s41588-020-00748-0
25. Mahal BA, Alshalalfa M, Kensler KH, et al. Racial differences in genomic profiling of prostate cancer. N Engl J Med. 2020;383(11):1083–1085. doi:10.1056/NEJMc2000069
26. Tewari A, Horninger W, Pelzer AE, et al. Factors contributing to the racial differences in prostate cancer mortality. BJU Int. 2005;96(9):1247–1252. doi:10.1111/j.1464-410X.2005.05824.x
27. Ellis L, Canchola AJ, Spiegel D, Ladabaum U, Haile R, Gomez SL. Racial and ethnic disparities in cancer survival: the contribution of tumor, sociodemographic, institutional, and neighborhood characteristics. J Clin Oncol. 2018;36(1):25. doi:10.1200/JCO.2017.74.2049
28. Klebaner D, Courtney PT, Rose BS. Effect of healthcare system on prostate cancer-specific mortality in African American and non-Hispanic white men. J Clini Oncol. 2021;39:23. doi:10.1200/JCO.2021.39.6_suppl.23
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.