Back to Journals » Journal of Asthma and Allergy » Volume 19
Racial and Socioeconomic Differences in Real-World Use of Biologic Therapy for Asthma
Authors Littlejohn M ![]() , Zuckerman AD
, Zuckerman AD ![]() , Gargurevich N, Choi L, Lubwama R
, Gargurevich N, Choi L, Lubwama R ![]() , Stanford RH
, Stanford RH ![]() , Campbell C, Nunez M, Petruski-Ivleva N, Tardy AL, Cruchelow K
, Campbell C, Nunez M, Petruski-Ivleva N, Tardy AL, Cruchelow K
Received 27 December 2025
Accepted for publication 4 May 2026
Published 5 June 2026 Volume 2026:19 587574
DOI https://doi.org/10.2147/JAA.S587574
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Monica Littlejohn,1 Autumn D Zuckerman,1 Nicolas Gargurevich,2 Leena Choi,2 Robert Lubwama,3 Richard H Stanford,4 Caresse Campbell,5 Manuel Nunez,6 Natalia Petruski-Ivleva,7 Anne-Laure Tardy,8 Katie Cruchelow1
1Vanderbilt Specialty Pharmacy, Vanderbilt University Medical Center, Nashville, TN, USA; 2Department of Biostatistics, Vanderbilt University Medical Center, Nashville, TN, USA; 3Health Outcomes and Value Assessment (HEVA) Specialty Care, Sanofi, Bridgewater, NJ, USA; 4Strategic Partnerships, AESARA, Inc, Chapel Hill, NC, USA; 5Medical Value Evidence and Insight, Sanofi, Cambridge, MA, USA; 6Neurology Medical Affairs, Sanofi, Bridgewater, NJ, USA; 7Health Outcomes and Value Assessment (HEVA) Specialty Care, Sanofi, Cambridge, MA, USA; 8Health Outcomes and Value Assessment (HEVA) Specialty Care, Sanofi, Gentilly, France
Correspondence: Monica Littlejohn, Vanderbilt Specialty Pharmacy, Vanderbilt University Medical Center, Nashville, TN, USA, Tel +1 615-875-2755, Email [email protected]
Purpose: Determine if there is a difference in race, socioeconomic factors and baseline asthma severity at the time of biologic initiation and whether those characteristics are associated with response to therapy within 18 months of initiation. Additionally, evaluate racial differences in clinic engagement, healthcare utilization, and biologic adherence.
Patients and Methods: Retrospective review of patients initiating biologic therapy for moderate-severe asthma from January 1, 2019–June 30, 2022. Multiple linear regression analyses were performed to examine whether race and socioeconomic status were associated with race-neutral percent predicted forced expiratory volume in one second (ppFEV1) prior to biologic prescription and within 18 months post biologic initiation. Differences in clinic engagement and healthcare utilization by race were assessed using Wilcoxon rank sum tests. Adherence was calculated using proportion of days covered (PDC).
Results: Patients (N=215) were White (69%) or Black or African American (27%). Most had commercial (54%) or Medicare (22%) insurance. At the time of biologic initiation, Black or African American/Other patients were estimated to have a 6.9% lower ppFEV1 than White patients (p=0.057), had a higher percentage of no-show appointments (p< 0.001), and there was a significant difference in distribution of percentage of appointments cancelled between White and Black or African American/Other patients (p = 0.0038). No significant differences in healthcare utilization were found by race. At follow-up, racial differences in ppFEV1 were 0.6% after adjusting for covariates and baseline ppFEV1 (p=0.893). Median PDC of biologic therapy was 0.96 (IQR 0.88– 1.00), with no significant difference between race. Socioeconomic status was similar between the cohorts.
Conclusion: Although not statistically significant, our findings suggest a possible trend where Black or African American/Other patients had lower ppFEV1 at the time of biologic initiation, indicating an opportunity for earlier interventions.
Keywords: asthma, health inequities, social factors, social determinants of health
Introduction
Asthma is a heterogeneous inflammatory disease characterized by chronic airway obstruction manifesting with symptoms such as wheezing, cough, dyspnea, and chest tightness.1 Approximately 25 million people in the United States have asthma, including 6 million children under the age of 18 years.2 The Centers for Disease Control (CDC) estimates 11.8% of the 25 million individuals with asthma are considered below 100% of the poverty threshold.2 The inverse association between low socioeconomic status (SES) and morbidity and mortality in patients with chronic diseases is well established.3–7 Underserved groups, primarily in Black, Hispanic, American Indian and Alaska native populations and patients who are financially disadvantaged, are disproportionately burdened with management of their asthma disease and often have poorer asthma outcomes.8–10 In addition, environmental inequalities among these populations further perpetuate this disparity.11 Studies have demonstrated air pollutants can exacerbate asthma symptoms and prolonged exposure can contribute to airway remodeling due to oxidative stress, airway inflammation and hyperresponsiveness.12–19
Biologic therapies have been shown to significantly reduce asthma exacerbations in patients with severe, uncontrolled disease.20,21 The 2021 Global Initiative for Asthma Guidelines (GINA) recommends consideration of biologic therapies as adjunct therapy in patients with severe asthma. Severe asthma is defined by patients requiring high dose inhaled corticosteroids (ICS) with a second controller drug (ex. long-acting beta antagonist), or those whose symptoms persist and/or experience frequent exacerbations despite these interventions.18,20,21 However, biologic therapies are expensive and often require a complex insurance approval process and subsequent financial assistance obtainment, which can be particularly challenging for low socioeconomic status and financially disadvantaged individuals.22 Delays in initiating therapeutic biologic asthma therapies may increase systemic steroid exposure, urgent care and hospitalization visits and risk of developing irreversible structural airway changes.23 Evidence suggests racial and ethnic minorities experience greater disease severity such as increased hospitalizations, emergency department visits, and mortality. Louie et al reported patients from an urban outpatient pulmonary and allergy clinic experienced less emergency department, and less average number of emergency department visits per year, after biologic initiation.5
Several factors, such as health disparities, low socioeconomic status, health literacy, or environmental exposure may contribute to patients presenting with uncontrolled disease.24 Access to therapies in the real world often requires a referral from a specialty clinician and insurance approval. Coordination and scheduling specialist visits can be difficult for patients with low SES and vulnerable populations. Insurance coverage, transportation challenges, and a shortage of specialist clinicians in underserved populations have been highlighted as critical barriers to vital healthcare.25 Akenroye et al found that patients from a historically marginalized group who were prescribed biologic therapy were 25% less likely to initiate treatment. Furthermore, patients with public insurance were less likely to initiate biologic therapy compared to those with private insurance.26
This study aimed to understand if patients in underserved populations and those with low SES have more uncontrolled asthma at the time of biologic prescription. This study also aims to examine how racial and socioeconomic factors influence medication adherence and persistence, clinic engagement patterns, and healthcare resource utilization during the first 12 months after the initiation of biologics. Finally, this study aims to evaluate if race or SES impact response to therapy within the first 18 months of biologic therapy initiation. Understanding factors that impact disease status at baseline and patient outcomes on therapy can facilitate targeted patient engagement and interventions to promote health equity.
Materials and Methods
Study Design
This was a single-center, retrospective study of pediatric and adult patients with moderate-to-severe asthma at the Vanderbilt University Medical Center (VUMC) Allergy/Immunology/ Pulmonology clinics. Data for analysis of baseline status prior to biologic initiation was collected for patients 1 year before their biologic medication referral date. Follow-up data was collected up to 18 months after biologic initiation (Figure 1).
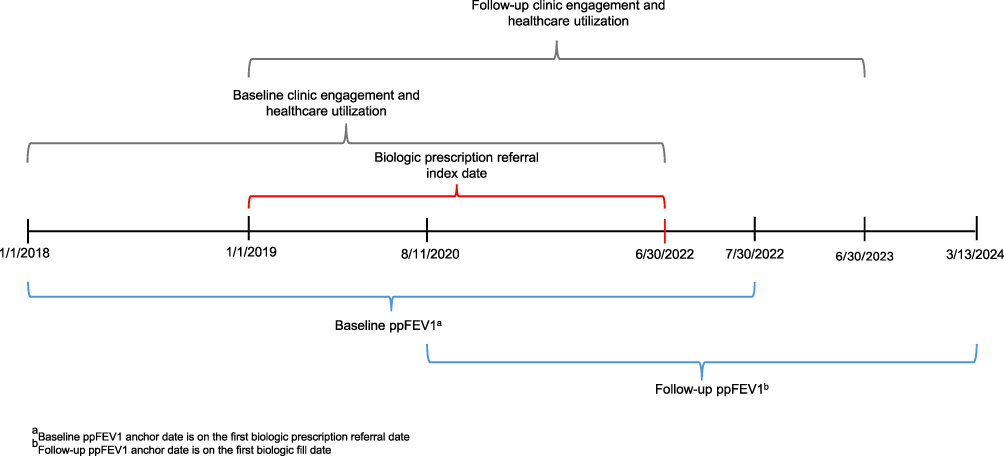 |
Figure 1 Study Design Timeline. |
Study Population
Patients were included if they had at least one diagnosis of moderate-to-severe asthma (ICD10 of J45.4 or J45.5) and were initiated on benralizumab, dupilumab, mepolizumab or omalizumab from VUMC Allergy/Immunology/Pulmonology clinic provider for moderate-to-severe asthma between January 1, 2019, and June 30, 2022. Patients were excluded if they had an indication for a biologic other than moderate-to-severe asthma, the biologic was not prescribed by a Vanderbilt provider, and if the patient had biologic use (provider administered or self-administered) within 6 months prior to the index date for an asthma indication (Figure 2).
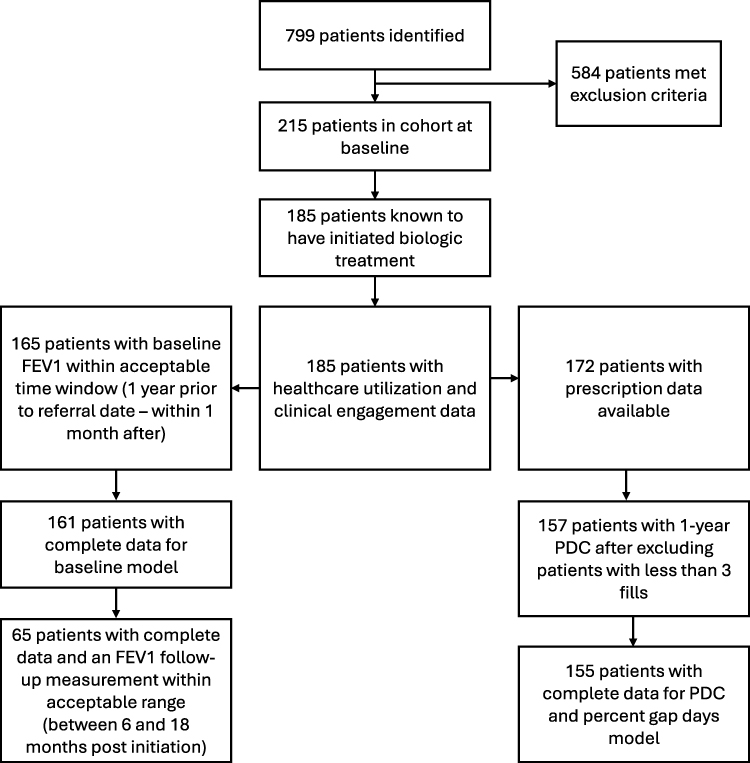 |
Figure 2 Patient Consort Diagram. |
Setting
This study was conducted at an academic medical center located in the southeastern United States, which operates an integrated health system specialty pharmacy (HSSP). The Vanderbilt Specialty Pharmacy (VSP) employs a collaborative care practice model that integrates pharmacists directly into outpatient specialty disease clinics at VUMC. This approach facilitates seamless care coordination and optimizes access to and management of specialty medications. Within the allergy and pulmonary clinics, specialty pharmacists and pharmacy technicians are embedded into both the pediatric and adult care teams. Pharmacists maintain transparent communication with healthcare providers and clinic staff through the electronic health record (EHR) system. The integrated collaborative practice model enhances care coordination and improves access to and management of specialty medications.22,27
Data Collection
Patient demographic, diagnosis, smoking status, prescription history, clinic engagement (percentage of appointments attended, cancelled, and no-show), laboratory data, health care utilization visits (including asthma exacerbation-related hospitalizations, urgent care visits and ambulatory care visits), were collected at baseline and during follow-up from the EHR. Pulmonary function test results for forced expiratory volume in one second (FEV1) were collected from the EHR. Biologic medication prescriptions and medication history data were obtained using the EHR. Biologic dispenses were obtained from the integrated specialty pharmacy patient management system. Air Quality Index (AQI) information was sourced from the Environmental Protection Agency (EPA) AQI database.28 This AQI includes measured Fine Particulate Matter (PM2.5) and Nitrous Oxide (NO2) at a zip code level. The Pipeline for Offline Conversion and Integration of Geocodes and Neighborhood Data (POINT) geocoder tool developed and maintained by VUMC was utilized to estimate geographic coordinates using patient demographic address and used to assign deprivation index values, which were calculated using Principal Component Analysis (PCA) with United States Census Data as outlined in Brokamp et al 2018.29 A higher deprivation index score indicates lower socioeconomic status, or greater deprivation. We considered the effect of the worldwide pandemic by assessing COVID-19 pandemic time course divided by 3 periods (Period 1: before COVID pandemic, ie, 1/1/2019 – 01/30/2020; Period 2: from the start of COVID pandemic to appearance of COVID variants, ie, 01/31/2020 – 12/31/2020; Period 3: after appearance of COVID variants, ie, 1/1/2021–06/30/2022 or the study end date). Data was collected between April 2022 through July 2024. Data were managed using REDCap (Research Electronic Data Capture) hosted at VUMC.30,31 This study was approved by the Vanderbilt University Medical Center Institutional Review Board.
Outcomes
Primary Outcome: Race Neutral Percent Predicted FEV1 at Baseline
The primary outcome, race-neutral percent predicted FEV1 (ppFEV1) prior to biologic initiation was calculated using the Global Lung Function Initiative (GLI) equation with FEV1 value measured at the closest time to biologic prescription referral (within 12 months or 30 days after).32
Secondary outcomes: Clinic Engagement, Healthcare Utilization, Adherence, Gap Days, and Persistence
The secondary outcomes included clinic engagement and healthcare utilization evaluated within the 12 months prior to biologic prescription referral and 12 months post biologic therapy initiation respectively. Clinic engagement was defined as the percent of scheduled appointments that resulted in a no show and the percent of appointments that resulted in a cancellation without rescheduling. Healthcare utilization was defined as the number of events for asthma-related hospitalizations, ED/urgent care visits, and ambulatory care visits.
The secondary outcomes also included adherence, gap days, and persistence calculated from the time of first biologic fill through the last fill within 12 months. Adherence was calculated using proportion of days covered (PDC). Patients were required to have at least 3 fills to be included in the PDC calculation. Gap days were defined as the percentage of days for which patients had a medication deficit. Medication deficit was defined as the difference between the number of days spanning one fill and the next, and the days’ supply of the fill, accounting for any surplus from previous fills. Persistence was defined as time to discontinuation of all biologic asthma therapy with no biologic prescriptions within 3 months of the end of the last biologic dosing interval.
Exploratory Outcomes: Race Neutral Percent Predicted FEV1 at Follow-Up
The exploratory outcome was race-neutral ppFEV1 measured between 6 and 18 months post biologic therapy initiation in those patients with a ppFEV1 measurement in both the pre and post biologic period.
Statistical Analysis
For descriptive analysis, categorical variables were described using frequencies and percentages, and continuous variables were described using medians and interquartile ranges (IQR).
A multiple linear regression analysis was performed to assess the direct associations between the primary outcome of race-neutral ppFEV1 and race as well as deprivation index as a surrogate of SES. SES data was calculated from geocoding and U.S. Census data. The model adjusted for potential confounding factors such as smoking status, COVID period in which measurement took place, insurance type, and average distance to care in a patient’s geographical area. For the analysis assessing the associations between the follow-up race-neutral ppFEV1 and race as well as deprivation index, the same regression approach was used adjusting for a reduced set of covariates (ie, smoking status, insurance type) along with the baseline ppFEV1 (ie, the primary outcome), considering a smaller number of patients having the follow-up ppFEV1. Age and gender were not included in the regression since ppFEV1 calculation accounts for both age and gender. Racial difference in absolute change in ppFEV1 from baseline to follow-up was assessed using Wilcoxon rank sum test.
Differences in clinic engagement and healthcare utilization by race were assessed 12 months prior to biologic therapy initiation, and from baseline to 12 months post biologic initiation using Wilcoxon rank sum tests. The relationship between deprivation index and clinic engagement was examined using a scatter plot, while the association between deprivation index and healthcare utilization was assessed using univariate ordinal regression. An ordinal regression was performed to assess the associations between medication adherence and race and deprivation index accounting for age, sex, smoking status, COVID period in which patient-initiated medication, insurance type, and average distance to care. The percentage of gap days between the first and last fill within 12 months of biologic therapy initiation was similarly evaluated using an ordinal regression adjusting for the same covariates listed above. Due to insufficient non-persistence events to perform a regression analysis, persistence was evaluated using a Kaplan–Meier analysis stratified by race. A sensitivity analysis was performed using multiple imputations for the analysis of the primary outcome as the set of geocoded variables was missing for 4 patients. All statistical analyses were performed using R programing language (Version 4.4.0, R Core Team, http://www.r-project.org).33
Results
Patients’ Characteristics at Biologic Treatment Referral
A total of 215 patients were included (Figure 2). Patients were a median 48 years of age (Interquartile Range [IQR] 26–60), 68% White, 27% Black or African American, and 5% Other (ie, American Indian or Alaska Native, Native Hawaiian or Other Pacific Islander, Guamanian or Chamorro, Middle Eastern, Other, Decline to Answer, Unknown, Null, or None of These). Gender distribution among patients was 55% female and 45% male. Most patients had commercial (54%) or Medicare (22%) insurance. Asthma severity was split between those with severe disease (47%) and moderate disease (53%), and 60% of patients reported never smoked/never exposed (Tables 1 and S1). Black or African American/Other patients were younger (median [IQR] age 35 [16–50] vs 53 [37–62] years) and had a higher proportion of severe-persistent asthma (50.7% vs 45.9%). Insurance coverage patterns also differed, with Black or African American/Other patients more likely to have Medicaid (31.3% vs 9.5%) and less likely to have Medicare (11.9% vs 27.0%). Additional patient characteristic comparisons by race can be found in Table 1. Differences in patient demographics and clinical characteristics for patients included in the baseline and follow-up models can be found in Tables S4 and S5.
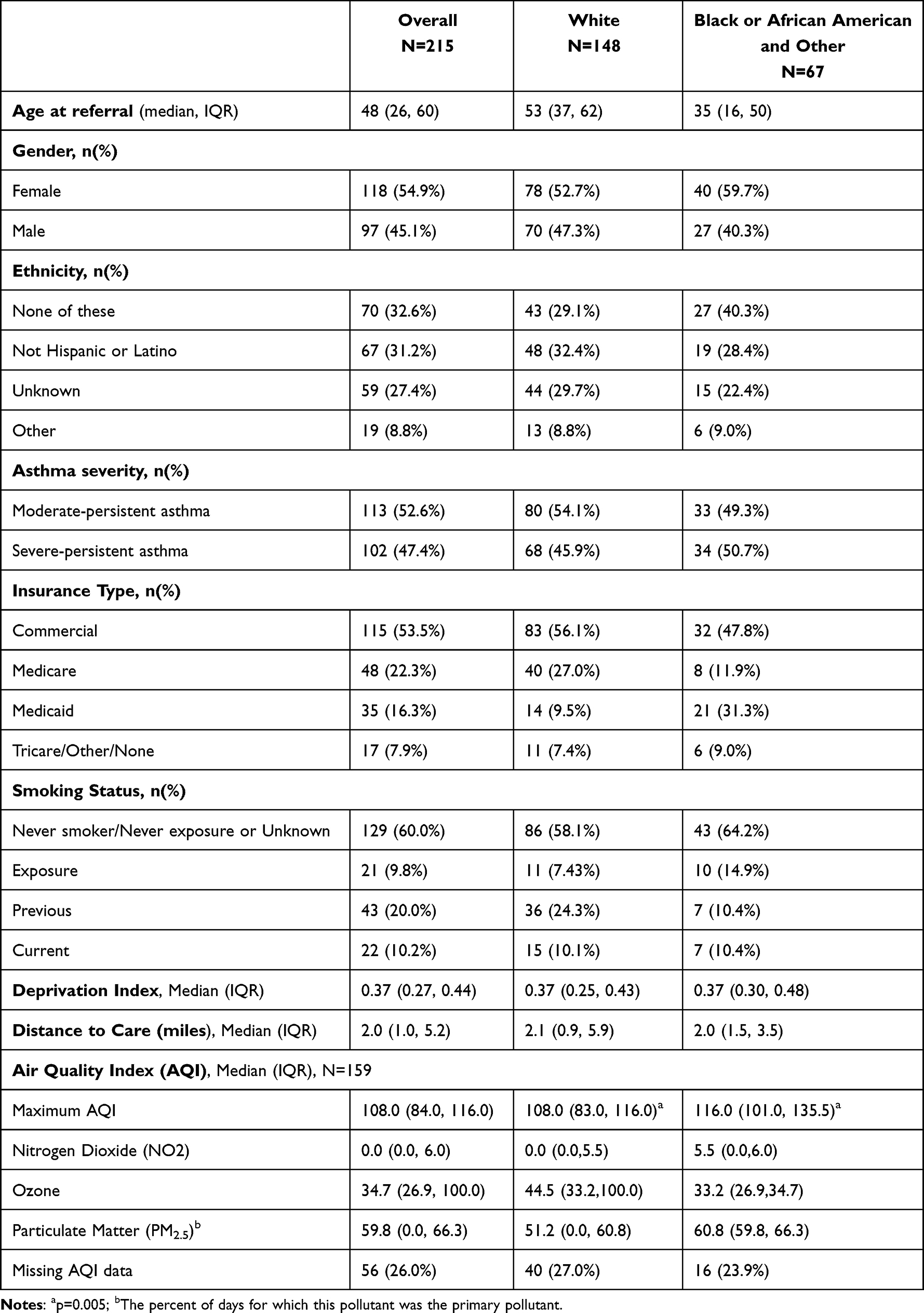 |
Table 1 Patient Demographic and Clinical Characteristics at Time of Biologic Referral Overall and According to Race |
The ppFEV1 at baseline was reported in 165 patients. Black or African American/Other patients had a lower median ppFEV1 than that of the White patients (64.3% vs. 72.7%) (Figure 3). Of the 159 patients with data available, air quality index was on average worse for Black or African American/Other patients compared to White patients with maximum AQI of 116 (IQR 101–135.5),] and 108 (IQR 83–116), respectively (p=0.005). Overall, 61.6% of our study cohort had a deprivation index greater than the median US deprivation index score of 0.33.
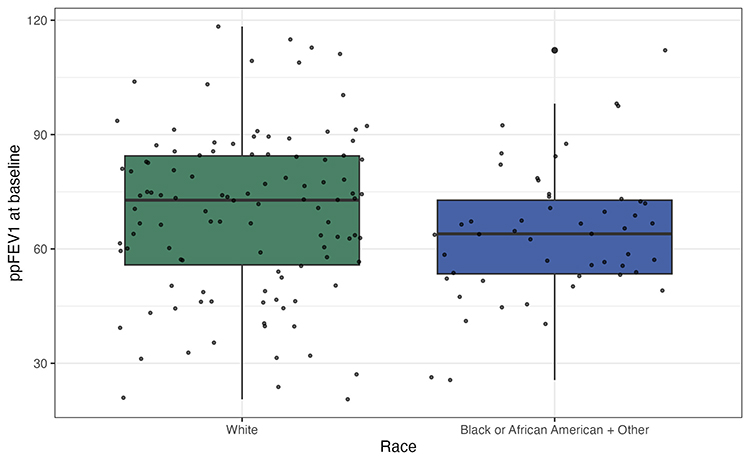 |
Figure 3 ppFEV1 at Baseline by Race. |
Primary Outcome: Factors Influencing ppFEV1 Prior to Biologic Prescription Referral
Of the 215 patients, 161 had a ppFEV1 and complete covariate data at baseline. After adjusting for the covariates, analysis demonstrated a possible trend that being Black or African American/Other was associated with a lower ppFEV1 at baseline (mean difference: −6.9% [−14.0, 0.2], p=0.057). Additionally, previous and current smokers had a lower estimated ppFEV1 at baseline than nonsmokers or those never exposed (−9.5% [−17.8, −1.3], p=0.024 and −15.1% [−26.4, −3.8], p=0.009, respectively). Deprivation index, COVID period, insurance type, and average distance to care were not significantly associated with the baseline ppFEV1 (Figure 4). The results were similar in the sensitivity analysis with multiple imputations for missing covariates.
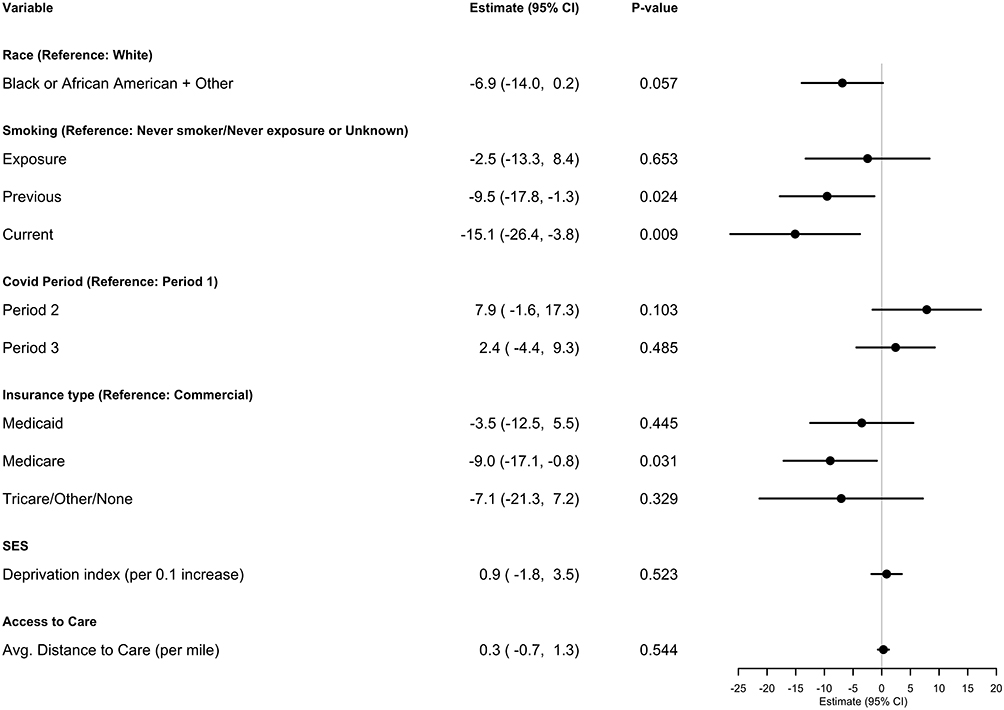 |
Figure 4 Multiple Linear Regression Summary and Forest Plot for ppFEV1 at Baseline. |
Secondary Outcomes: Impact of Racial and SES Factors on Clinic Engagement, Healthcare Resource Utilization, Adherence, Gap days, and Persistence
For clinic engagement in the 12 months prior to biologic, a median of 0% (IQR 0–14.3%) of appointments had been cancelled per patient and a median of 0% (IQR 0–0%) of appointments had resulted in a no show in the 12 months prior to biologic initiation. Black or African American/Other patients were found to have a higher percentage of appointments no show (0% [IQR 0–11.3%] vs. 0% [IQR 0–0%]; p = 0.001) at baseline, (Table 2), but there was no significant difference in the percent of appointments cancelled by race (p = 0.131), and no discernable differences by SES. At follow up, there was a significant difference in the distribution of percentage of appointments cancelled between White and Black or African American/Other patients (median 6.1% [IQR 0–33.3%] and 0% [IQR 0–13.6%], respectively; p = 0.0038), and percentage of appointment no shows (0% [IQR 0–0%] and 0% [IQR 0–25%], respectively; p < 0.001) (Table 2). There were no discernable differences in clinic engagement at follow-up by deprivation index.
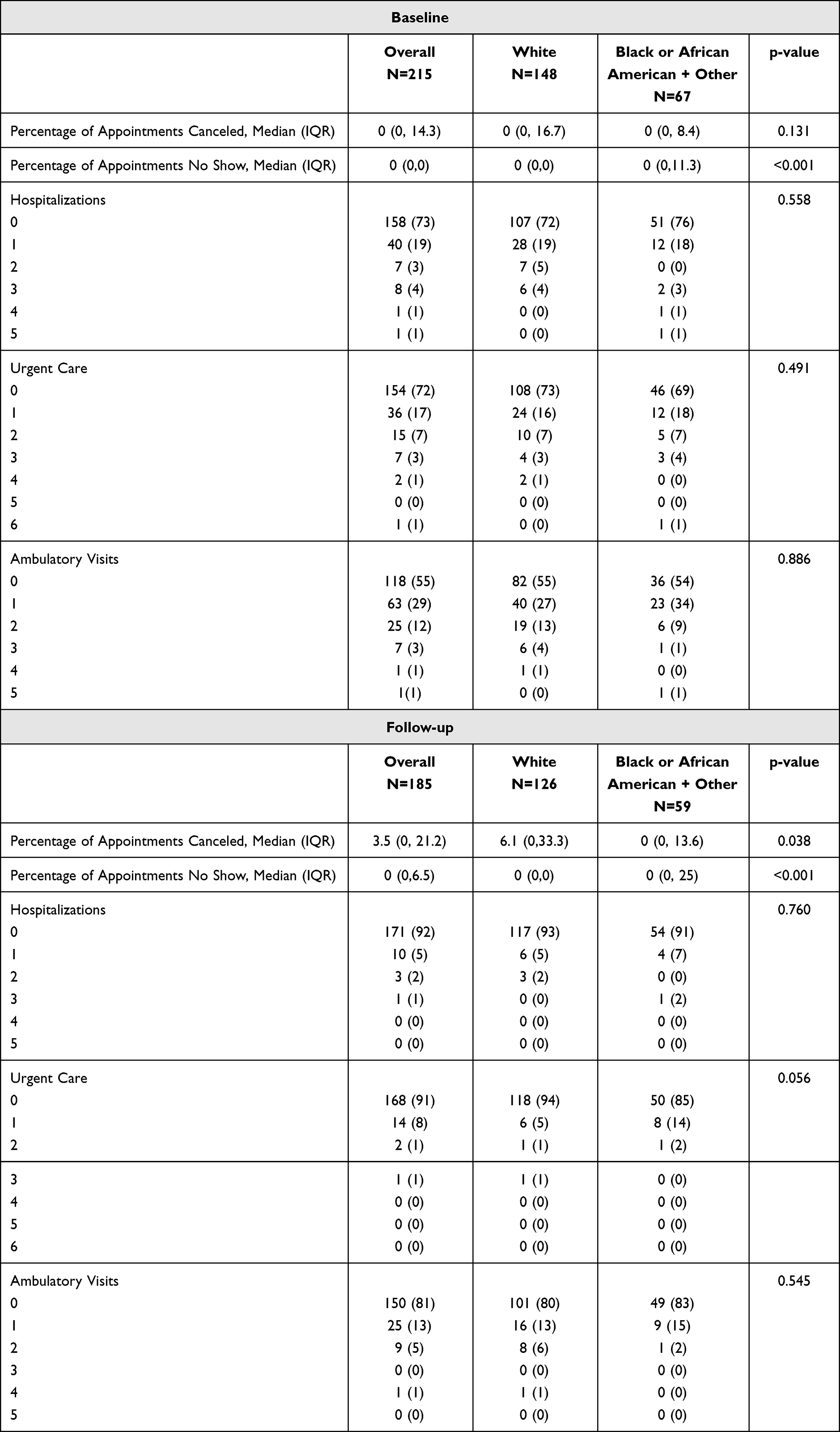 |
Table 2 Wilcoxon Rank Sum Results for Clinic Engagement and Healthcare Utilization vs Race at Baseline and Follow-Up |
For healthcare utilization, 26% of patients had at least one hospitalization, 28% had at least one urgent care visit, and 45% had at least one ambulatory care visit 12 months prior to biologic initiation. No significant differences in healthcare utilization were found by race (Table 2). However, patients with lower deprivation index scores were associated with a 27% (odds ratio [OR] 0.73 [0.56, 0.94], p = 0.013) less likelihood of having urgent care visits at baseline (Table 3). Finally, 8% of patients had at least one hospitalization, 9% had at least one urgent care visits, and 19% had at least one ambulatory care visits at follow-up (Table 2), which were not significantly different by race or SES (Table 3).
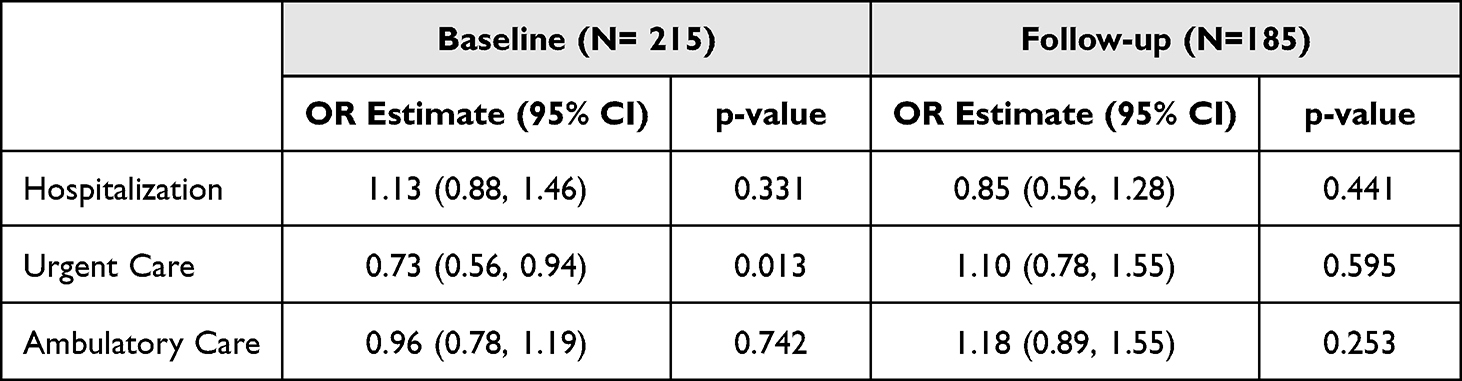 |
Table 3 Univariate Ordinal Regression for Healthcare Utilization vs. SES at Baseline and Follow-Up |
Within 12 months of biologic therapy initiation, the overall population had a median PDC of 0.96 (IQR 0.88–1.00) and a median percentage of gap days of 3.8% (IQR 0.3–12.5%). White patients demonstrated a slightly higher PDC of 0.97 (IQR 0.91–1.00) with fewer gap days (median 2.7%, IQR 0.2–9.6%) (Figure S1). Black or African American/Other patients had a PDC of 0.95 (IQR 0.74–0.99) with more gap days (median 5.3%, IQR 0.6–5.7%) (Table 4 and Figure S2). Non-persistence was observed in 8 instances (5.1% of the total population), with 6 cases (5.8%) among White patients and 2 cases (3.8%) among Black or African American/Other patients. Black or African American/Other patients showed a trend towards lower PDC (estimate 0.65, p=0.183) and higher gap days (estimate 1.53, p=0.193) compared to the White patients, but these differences were not statistically significant. For every 0.1 increase in the deprivation index, there was a slight trend towards lower PDC (estimate 0.84, p=0.191) and higher gap days (estimate 1.19, p=0.189), but again, not statistically significant. COVID-19 period impacted medication adherence. Period 2 showed a trend towards lower PDC (estimate 0.37, p=0.060) and higher gap days (estimate 2.74, p=0.0586) compared to Period 1 and Period 3, which showed significantly lower PDC (estimate 0.36, p=0.0253) and significantly higher gap days (estimate 2.78, p=0.024) compared to Period 1. However, age, gender, smoking, distance to care and insurance type did not significantly impact PDC or gap days (Table 5).
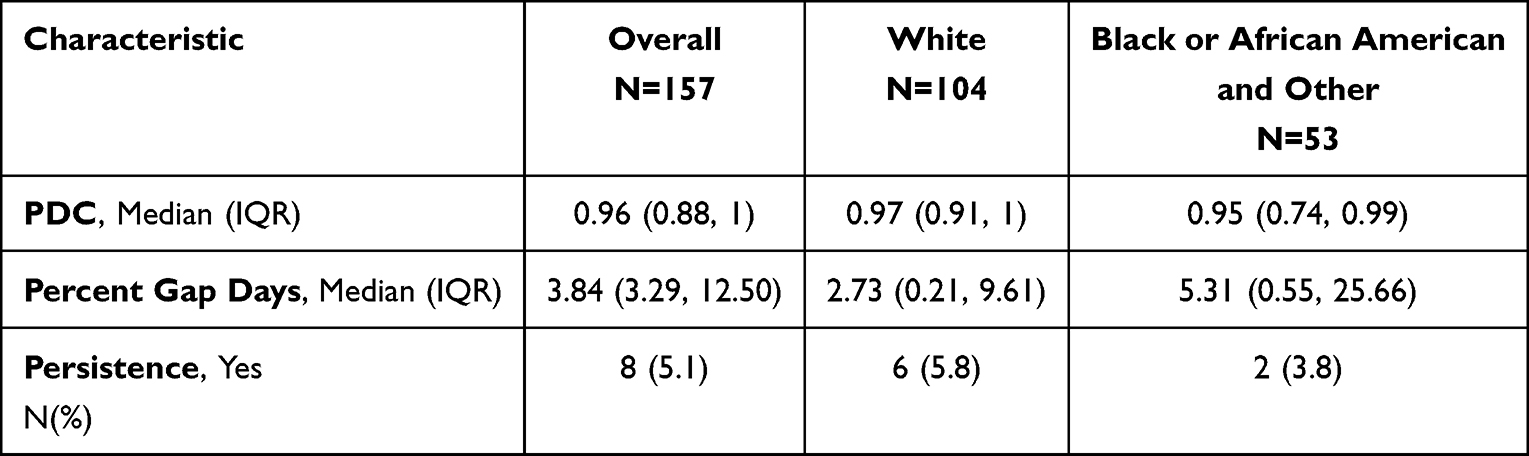 |
Table 4 PDC, Percent Gap Days, and Persistence By Race |
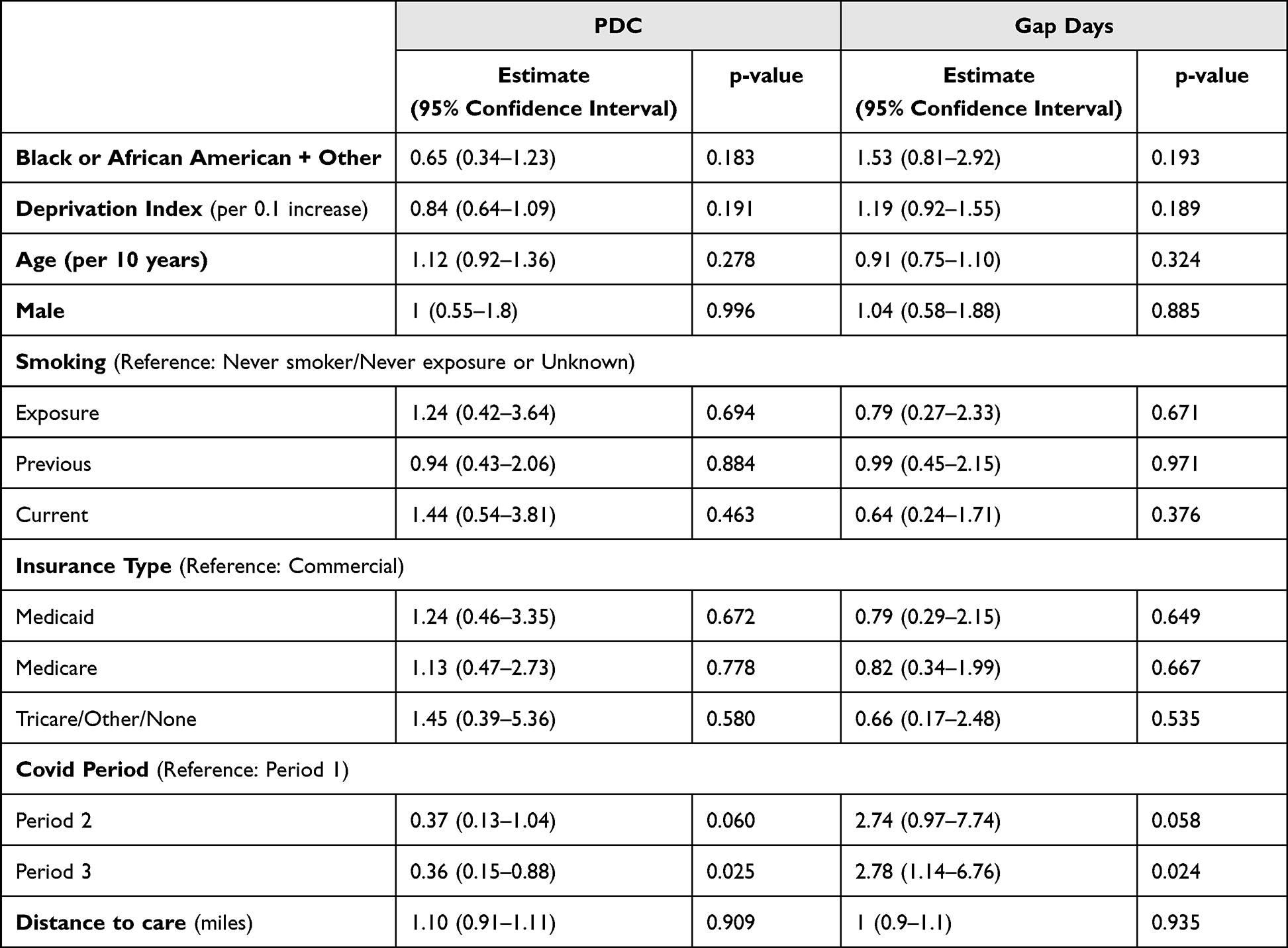 |
Table 5 Ordinal Regression Analysis Summaries for PDC and Gap Days |
Exploratory Outcomes: Impact of Race, SES and Smoking on Biologic Treatment Response
Of the 165 patients with a baseline ppFEV1, 65 patients had ppFEV1 prior to biologic initiation and at 6 to 18 months after biologic initiation. Baseline ppFEV1 was significantly associated with higher follow-up ppFEV1 (0.64% [0.44, 0.84]; p < 0.001). After adjusting for covariates and baseline ppFEV1, there was no difference in observed follow-up ppFEV1 between Black or African American/Other and White patients (mean difference 0.6% [−8.3, 9.5]; p=0.893). Similarly, smoking status, insurance type, and deprivation index were not significantly associated with follow-up ppFEV1 (Table S2). Black or African American/Other patients saw a median increase of 4% in ppFEV1 [IQR –6–24], while White patients saw a median increase of 2% in ppFEV1 [IQR –2–10], though this was not a significant racial difference (p=0.558) (Table S3).
Discussion
Though not statistically significant, this study suggests a possible trend in which Black or African American/Other patients had lower ppFEV1 at the time of biologic initiation compared to White patients. In this study, using deprivation index, SES did not differ between the groups and was not associated with worse lung function. This finding should be interpreted within the broader context of existing literature. Several negative social determinants (ie. racism, environmental injustice, poverty, higher rates of mortality, decreased access to healthcare) have been reported in the literature to contribute to health disparities among patients who identify as Black or African American and those of lower socioeconomic status.11,24,34,35 In addition, literature has attributed 10% of differences in lung function to be a result of social determinants of health. Adibi et al found that social determinants of health explained approximately 25% of the differences between their Black and White cohorts.34 Possible explanations for the lack of association observed in this study is heterogeneity and insufficient sample size. Overall, 62% of the study population had a deprivation index greater than the median US deprivation index score, suggesting that this cohort may overall be of lower SES. Deprivation index was used as an imperfect proxy measure for SES, as the study used the overall deprivation index for the corresponding census tract for each patient as opposed to their individual measures of SES such as income and education level due to a lack of data availability of this data.
Black or African American/Other patients in this study were more likely to miss their scheduled appointments 12 months before biologic initiation. Delays in initiating therapeutic biologic asthma therapies may increase systemic steroid exposure, urgent care and hospitalization visits and risk of developing irreversible structural airway changes.16 Among an adult population with severe asthma treated at an urban outpatient clinic, patients receiving biologic therapy for at least 6 months led to decreased oral corticosteroid use, ED visits, and median daily systemic steroid dosage.5 These results highlight that an opportunity exists to improve engagement and retention in care earlier in a patient’s disease course so that patients can begin biologic therapy before disease progression.
After initiating biologic therapy, race was not found to be associated with response to treatment measured by ppFEV1 within 12 months. Black or African American/Other patients had on average a greater percent change in ppFEV1 from baseline to follow-up obtaining a similar ppFEV1 to the White patient cohort, though this was not found to be statistically significant. This underscores the importance of early treatment intervention targeting lung function for Black or African American/Other patients to improve lung function earlier in the disease course. Louie et al reported among adult patients with severe asthma treated at an urban outpatient clinic, with 93% of patients who self-reported as Hispanic or African American race, patients receiving biologic therapy for at least 6 months significantly improved ACT scores, and increased their mean FEV1.5 Despite approximately 11% of patients with asthma being Black or African American/Other and 8% to 9% affecting people with lower income, racial and ethnic representation in the clinical trials evaluating biologics’ efficacy were not always representative of the population disproportionately affected by the disease.26,36,37 Similar to this study’s findings, post-market studies have not shown differences in biologic efficacy among racial and ethnic groups.15 This study adds novel insight into racial disparities that may exist in patients with moderate-to-severe asthma needing biologic therapy, while also highlighting the improvement in lung function is observed regardless of race once started on a biologic.
Opportunities to Improve Care Post-Initiation Adherence
Patients in the current study demonstrated high overall adherence rates, though differences were observed between White and Black or African American/Other patients. Previous studies have reported biologic therapy is effective when taken as prescribed, reducing asthma exacerbations by 50%, which aligns with the current study findings.21,38 Medication adherence is multi-factorial and may be affected by reasons such as affordability, access to therapy, medication fears, lack of trust in healthcare provider, lack of disease awareness, psychological and practical barriers and mode of administration.13,14 One explanation for high adherence to biologic therapy could be due to the HSSP care model in which the study occurred. Specialty clinical pharmacists offer an enhanced level of patient care, following a patients journey through medication access, treatment initiation, and treatment monitoring.39 Pharmacists and other healthcare team members managing patients on biologic therapy should use a patient-centered approach that addresses all factors related to adherence. Additionally, although PDC was high in this study, Black or African American/Other patients had longer prescription gap days compared to White patients. PDC calculations are not able to identify reasons for gaps in therapy; therefore more data is needed to address these gaps.40 There is limited research available on the impact of biologic gap days, and future studies should explore how gap days can affect patient outcomes.
Clinic Engagement
Despite improving lung function, disparities were still seen among Black and African American/Other patient’s post-biologic initiation, including higher rates of missing scheduled clinic visits. Evidence suggests no-show appointments can have a significant impact on health outcomes and lead to financial loss for the institution with non-reimbursable appointments.41–43
EPA – Air Quality
In the current study, race was significantly associated with the percentage of days of ambient air pollutant exposure to PM2.5. Additionally, Black or African American/Other patients experienced PM2.5 exposure on more than 60% days of the days studied. Exposure to PM2.5, regardless of duration, has been shown to perpetuate oxidative stress in multiple organs. This oxidative stress may mediate respiratory problems, including pneumonia, asthma and/or chronic obstructive pulmonary disease (COPD) exacerbation, and increase risk of morbidity and mortality.10,12 In addition, studies have shown an association between exposure to particulate matter and incidence of developing childhood asthma and number of respiratory related hospital admissions.9–11,13 Bennett et al reported that life expectancy due to PM2.5 was lower in counties with a family income below the poverty threshold and those who are of Black or African American race.12 These results further highlight the racial inequities of environmental exposure and opportunities to improve air quality and educate patients on the role of air quality and asthma exacerbations.
Limitations
One limitation of this study was the relatively small sample size, particularly for the follow-up ppFEV1 analysis, which may be attributed to data collection during the COVID-19 pandemic when lung function testing was not frequently conducted. Due to the low sample size, a larger follow-up window between 6 and 18 months after biologic initiation was used. Future studies should examine the association between race, socioeconomic status and asthma severity outside of the COVID-19 pandemic time period in order to obtain a larger sample size. Second, as this study used a convenience sample of patients initiating biologic therapy at the HSSP, no formal power calculation was performed to determine the required sample size. However, we acknowledge that the sample size may be insufficient to detect statistically significant differences in the primary outcomes between the major comparison groups. This could, in turn, affect the primary outcome where the statistically significant results may not be detected. Additionally, patients without a baseline spirometry or those with low ppFEV1 that did not have a baseline spirometry may have been excluded which may lead to a sampling bias. There was a significant difference in age at initiation and race, between patients with available data available for follow-up analysis. This study was carried out at a single center with a homogenous population, that may limit the generalizability of the findings to broader populations. Finally, socioeconomic status data was generated from geocoding and U.S. Census data. These data were used to calculate the overall deprivation index for the corresponding census tract for each patient. Future studies with larger sample size using geocoding from U.S. Census data could help discern those census tract level trends. Enhancing SES data collection through direct EHR reporting could improve the robustness of the findings.
Conclusion
Prior to biologic initiation, Black or African American/Other patients had worse lung function than White patients and were more likely to miss their scheduled appointments. After biologic initiation, patients in both groups had a similar improvement in lung function after treatment and reported high adherence and persistence. However, Black or African American/Other patients continued to have high rates of missed scheduled clinic visits. These results indicate an opportunity based on lung function for earlier interventions in Black or African American/Other patients with moderate-to-severe asthma and higher engagement post-initiation.
Ethical Approval
This study was conducted in accordance with the ethical guidelines and principles outlined in the Declaration of Helsinki. Ethical approval for the study was obtained from the Institutional review board committee, HS3 at Vanderbilt University Medical Center. The approval reference number is 220419. As this was a retrospective study that utilized anonymized patient data, informed consent was not required according to the regulations of the Institutional Review Board at Vanderbilt University Medical Center. The research protocol was reviewed and approved by the ethics committee to ensure compliance with ethical standards for studies involving retrospective data analysis.
Acknowledgments
Authors are grateful for the research support of Briana Hunt, Amanda Kibbons and Carsyn Snagg. Data management services for this study were provided by REDCap (Research Electronic Data Capture) through Vanderbilt Institute for Clinical and Translational Research.
Firstly, this paper was presented at the American Academy of Allergy, Asthma & Immunology Meeting as a poster presentation talk with interim findings. The poster’s abstract was published in “Poster Abstracts” in The Journal of Allergy and Clinical Immunology: Impact Of Race on Baseline Asthma Severity and Response to Biologic Therapy in the First 12 Months Post Biologic Initiation – Journal of Allergy and Clinical Immunology. Secondly, the abstract of the paper was presented at the American Society of Health-System Pharmacists Midyear Clinical Meeting and Exhibition as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in American Journal of Health-System Pharmacy: 2024 ASHP Midyear Clinical Meeting Poster Abstracts | American Journal of Health-System Pharmacy | Oxford Academic. Third, the abstract of the paper was presented at the National Association of Specialty Pharmacy Annual Meeting & Expo as an encore poster with interim findings. The encore poster was published at National Association of Specialty Pharmacy: 2125-OPR35-EN-Poster-AM25.pdf. Finally, the abstract of the paper was presented at the National Association of Specialty Pharmacy Annual Meeting & Expo as an encore poster with interim findings. The encore poster was published at National Association of Specialty Pharmacy: 2126-OPR34-EN-Poster-AM25.pdf.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was sponsored by Sanofi UA Services, Inc.
Disclosure
ML received advisor fees for serving as a consultant for AstraZeneca, and research support paid to the institution from Sanofi, Inc. AZ received research support paid to her institution from Sanofi, Inc, AstraZeneca, Pfizer, UCB, Beigene, Takeda Inc, Celltrion, and BridgeBio. RL, CC, MN, NP and AT are employees of Sanofi and may hold stocks and/or stock options in the company. RS is an employee of Aesara and a paid consultant for Sanofi. KC received research support paid to the institution from Sanofi, Inc, and BridgeBio. The authors report no other conflicts of interest in this work.
References
1. Dubin S, Patak P, Jung D. Update on asthma management guidelines. Mo Med. 2024;121(5):364–15. doi:10.1378/chest.130.1_suppl.4s
2. Prevention CfDCa. 2019 National health interview survey data. Available from: https://www.cdc.gov/asthma/nhis/2019/data.htm.
3. Bacon SL, Bouchard A, Loucks EB, Lavoie KL. Individual-level socioeconomic status is associated with worse asthma morbidity in patients with asthma. Respir Res. 2009;10(1):125. doi:10.1186/1465-9921-10-125
4. Seibert RG, Winter MR, Cabral HJ, Wolf MS, Curtis LM, Paasche-Orlow MK. Health literacy and income mediate racial/ethnic asthma disparities. Health Lit Res Pract. 2019;3(1):e9–e18. doi:10.3928/24748307-20181113-01
5. Louie J, Anto AM, Venkatram S, Huggins C, Diaz-Fuentes G. Real-world outcomes of biologic therapy for severe asthma in a high-burden urban population. Cureus. 2025;17(7):e88756. doi:10.7759/cureus.88756
6. Zárate RA, Bhavnani D, Chambliss S, et al. Neighborhood-level variability in asthma-related emergency department visits in Central Texas. J Allergy Clin Immunol. 2024;154(4):933–939. doi:10.1016/j.jaci.2024.05.024
7. Wohlford EM, Huang PF, Elhawary JR, et al. Racial/ethnic differences in eligibility for asthma biologics among pediatric populations. J Allergy Clin Immunol. 2021;148(5):1324–1331.e12. doi:10.1016/j.jaci.2021.09.005
8. McCallum GB, Morris PS, Brown N, Chang AB. Culture-specific programs for children and adults from minority groups who have asthma. Cochrane Database Syst Rev. 2017;8(8):Cd006580. doi:10.1002/14651858.CD006580.pub5
9. Forno E, Celedón JC. Health disparities in asthma. Am J Respir Crit Care Med. 2012;185(10):1033–1035. doi:10.1164/rccm.201202-0350ED
10. Micheals K, Bhavnani D, Matsui EC. Examining disparities in biologic therapy initiation: the intersection of race/ethnicity and insurance type. J Allergy Clin Immunol. 2025;155(3):810–812. doi:10.1016/j.jaci.2025.01.002
11. Mathiarasan S, Hüls A. Impact of environmental injustice on children’s health-interaction between air pollution and socioeconomic status. Int J Environ Res Public Health. 2021;18(2):795. doi:10.3390/ijerph18020795
12. McCarron A, Semple S, Braban CF, Gillespie C, Swanson V, Price HD. Personal exposure to fine particulate matter (PM2.5) and self-reported asthma-related health. Soc sci med. 2023;337:116293. doi:10.1016/j.socscimed.2023.116293
13. Jo YS, Lim MN, Han YJ, Kim WJ. Epidemiological study of PM(2.5) and risk of COPD-related hospital visits in association with particle constituents in Chuncheon, Korea. Int J Chron Obstruct Pulmon Dis. 2018;13:299–307. doi:10.2147/copd.S149469
14. Surit P, Wongtanasarasin W, Boonnag C, Wittayachamnankul B. Association between air quality index and effects on emergency department visits for acute respiratory and cardiovascular diseases. PLoS One. 2023;18(11):e0294107. doi:10.1371/journal.pone.0294107
15. Tamayo JM, Osman HC, Schwartzer JJ, Pinkerton KE, Ashwood P. Characterizing the neuroimmune environment of offspring in a novel model of maternal allergic asthma and particulate matter exposure. J Neuroinflammation. 2023;20(1):252. doi:10.1186/s12974-023-02930-7
16. Bennett JE, Tamura-Wicks H, Parks RM, et al. Particulate matter air pollution and national and county life expectancy loss in the USA: a spatiotemporal analysis. PLoS Med. 2019;16(7):e1002856. doi:10.1371/journal.pmed.1002856
17. Xu X, Zhang J, Yang X, Zhang Y, Chen Z. The role and potential pathogenic mechanism of particulate matter in childhood asthma: a review and perspective. J Immunol Res. 2020;2020:8254909. doi:10.1155/2020/8254909
18. Asthma. GIf. Global strategy for asthma management and prevention. Available from: https://ginasthma.org/wp-content/uploads/2021/05/GINA-Main-Report-2021-V2-WMS.pdf.
19. Fiter RJ, Murphy LJ, Gong MN, Cleven KL. The impact of air pollution on asthma: clinical outcomes, current epidemiology, and health disparities. Expert Rev Respir Med. 2023;17(12):1237–1247. doi:10.1080/17476348.2024.2307545
20. Saco TV, Pepper A, Casale TB. Uses of biologics in allergic diseases: what to choose and when. Ann Allergy Asthma Immunol. 2018;120(4):357–366. doi:10.1016/j.anai.2018.02.029
21. Saxena S, Rosas-Salazar C, Fitzpatrick A, Bacharier LB. Biologics and severe asthma in children. Curr Opin Allergy Clin Immunol. 2023;23(2):111–118. doi:10.1097/aci.0000000000000880
22. Bagwell A, Kelley T, Carver A, Lee JB, Newman B. Advancing patient care through specialty pharmacy services in an academic health system. J Manag Care Special Pharm. 2017;23(8):815–820. doi:10.18553/jmcp.2017.23.8.815
23. Farinha I, Heaney LG. Barriers to clinical remission in severe asthma. Respir Res. 2024;25(1):178. doi:10.1186/s12931-024-02812-3
24. America AaAFo. Asthma disparities in America: a roadmap to reducing burden on racial and ethnic minorities. Available from: https://aafa.org/asthma-allergy-research/our-research/asthma-disparities-burden-on-minorities/.
25. Ezeonwu MC. Specialty-care access for community health clinic patients: processes and barriers. J Multidiscip Healthc. 2018;11:109–119. doi:10.2147/jmdh.S152594
26. Akenroye A, Keet C. Underrepresentation of blacks, smokers, and obese patients in studies of monoclonal antibodies for asthma. J Allergy Clin Immunol Pract. 2020;8(2):739–741.e6. doi:10.1016/j.jaip.2019.08.023
27. Zuckerman AD, Carver A, Cooper K, et al. An integrated health-system specialty pharmacy model for coordinating transitions of care: specialty medication challenges and specialty pharmacist opportunities. Pharmacy. 2019;7(4):163. doi:10.3390/pharmacy7040163
28. Agency EP. Air Quality Index (AQI) database. Available from: https://www.epa.gov/outdoor-air-quality-data/air-quality-index-report.
29. Brokamp C, Beck AF, Goyal NK, Ryan P, Greenberg JM, Hall ES. Material community deprivation and hospital utilization during the first year of life: an urban population-based cohort study. Ann Epidemiol. 2019;30:37–43. doi:10.1016/j.annepidem.2018.11.008
30. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010
31. Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: building an international community of software platform partners. J Biomed Inform. 2019;95:103208. doi:10.1016/j.jbi.2019.103208
32. Bowerman C, Bhakta NR, Brazzale D, et al. A race-neutral approach to the interpretation of lung function measurements. Am J Respir Crit Care Med. 2023;207(6):768–774. doi:10.1164/rccm.202205-0963OC
33. R: a language and environment for statistical computing. R Foundation for Statistical Computing; 2025. Available from: https://www.R-project.org/.
34. Adibi A, Carlsten C, Brigham EP, Sin DD, Loewen P, Sadatsafavi M. Social determinants of health and racial disparities in lung function: findings from the national health and nutrition examination survey, 2007–2012. Am J Respir Crit Care Med. 2025;211(11):2117–2126. doi:10.1164/rccm.202501-0280OC
35. Hegewald MJ, Crapo RO. Socioeconomic Status and Lung Function. Chest. 2007;132(5):1608–1614. doi:10.1378/chest.07-1405
36. Prevention USCfDCa. Most Recent National Asthma Data; 2023. Available from: https://www.cdc.gov/asthma/most_recent_national_asthma_data.htm.
37. Inselman JW, Jeffery MM, Maddux JT, Shah ND, Rank MA. Trends and disparities in asthma biologic use in the United States. J Allergy Clin Immunol Pract. 2020;8(2):549–554.e1. doi:10.1016/j.jaip.2019.08.024
38. Brusselle GG, Koppelman GH. Biologic therapies for severe asthma. N Engl J Med. 2022;386(2):157–171. doi:10.1056/NEJMra2032506
39. Kibbons AM, Moore R, Choi L, Zuckerman AD. Patient-tailored interventions to improve specialty medication adherence: results from a prospective randomized controlled trial. Am J Med. 2023;136(7):694–701.e1. doi:10.1016/j.amjmed.2023.03.007
40. Paolella D, Cherry E, Jolly JA, DeClercq J, Choi L, Zuckerman A. Closing the gap: identifying rates and reasons for nonadherence in a specialty population. J Manag Care Spec Pharm. 2019;25(11):1282–1288. doi:10.18553/jmcp.2019.25.11.1282
41. Williamson AE, McQueenie R, Ellis DA, McConnachie A, Wilson P. “Missingness” in health care: associations between hospital utilization and missed appointments in general practice. A retrospective cohort study. PLoS One. 2021;16(6):e0253163. doi:10.1371/journal.pone.0253163
42. Nguyen DL, Dejesus RS. Increased frequency of no-shows in residents’ primary care clinic is associated with more visits to the emergency department. J Prim Care Community Health. 2010;1(1):8–11. doi:10.1177/2150131909359930
43. Perron NJ, Dao MD, Kossovsky MP, et al. Reduction of missed appointments at an urban primary care clinic: a randomised controlled study. BMC Fam Pract. 2010;11(1):79. doi:10.1186/1471-2296-11-79
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.