")
Back to Journals » Psychology Research and Behavior Management » Volume 16
Racial and Ethnic Disparities in Weight Loss Behaviors Among US College Students
Authors Van Dyne A, Washington N, Villodas M, Cronan T
Received 8 November 2022
Accepted for publication 2 March 2023
Published 16 March 2023 Volume 2023:16 Pages 857—873
DOI https://doi.org/10.2147/PRBM.S395357
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Angelina Van Dyne, Nicole Washington, Miguel Villodas, Terry Cronan
Department of Psychology, San Diego State University, San Diego, CA, USA
Correspondence: Terry Cronan, Department of Psychology, San Diego State University, 5500 Campanile Drive, San Diego, CA, 92182-4611, USA, Tel +1619 594-6915, Fax +1619 594-1247, Email [email protected]
Purpose: Weight loss behaviors are prevalent among college students and are associated with adverse physical and psychological outcomes, such as an elevated risk of developing an eating disorder. While cross-ethnic differences have been reported, no consistent pattern has emerged. The purpose of this study was to examine racial and ethnic differences in weight loss behaviors among female and male college students.
Patients and Methods: The American College Health Association-National College Health Assessment (ACHA-NCHA) II-C survey data from the collection periods from 2015 to 2019 was used. A total of 426,425 students participated in the survey. Most participants were White (60%) and female (68.5%). Information on students’ age, body mass index (BMI), and self-rated health was also collected. Logistic regression analyses were performed to determine cross-ethnic differences in weight loss methods among female and male students.
Results: Students’ weight loss behaviors were assessed and included dieting, exercising, vomiting or taking laxatives, and the use of diet pills in the past 30 days. More than half of the participants attempted to lose weight through exercise (53.5%), and 40.3% of students dieted to lose weight in the past month. Purging and the use of diet pills were endorsed by 2.9% and 2.8% of the participants, respectively. With few exceptions, male students from racial and ethnic minority backgrounds were more likely to engage in extreme weight control practices (ie, vomiting or taking laxatives, taking diet pills) than White male students, while female students from racial and ethnic minority backgrounds were less likely to use diet and exercise as weight loss methods than White female students. For all outcomes, Biracial/Multiracial and Hispanic/Latino male students were more likely to attempt weight loss than White male students. Biracial/Multiracial female students more frequently endorsed extreme weight control behaviors than White female students.
Conclusion: The results of the present study add to the growing body of literature on the relationship between race and ethnicity and weight loss behaviors. The findings indicate the need for tailored educational and intervention programs on college campuses.
Keywords: ethnic minority, diet, exercise, diet pills, self-induced vomiting
Introduction
Unhealthy weight loss practices are prevalent and frequently result in the diagnosis of an eating disorder, adverse health consequences, depression, and future weight gain.1–5 These practices may include extreme dietary restrictions, compensatory exercise, the use of diet pills, self-induced vomiting, and the abuse of laxatives and stimulants.6 These behaviors are frequently accompanied by a preoccupation with one’s weight and size, as well as severe psychological distress.6,7 A complex interaction between psychological, social, and biological factors influences weight loss behaviors.8 However, there has been a recent increase in researchers’ interest in the role that society plays in shaping our attitudes and behaviors regarding body size, weight, food, and, consequently, weight loss attempts and methods. The increased academic and activist scrutiny of fatphobia, weight stigma (discrimination based on weight or size), and the proliferation of the thin ideal has contributed to this increased focus. Because of the unequal distribution of societal pressure, certain groups are disproportionately affected by body image concerns and weight-related issues.9 As a result, individuals from racial and ethnic minority backgrounds have recently come to the forefront of eating disorder research, as the racial roots of fatphobia have been examined.9–11 New evidence suggests that individuals from racial and ethnic minority backgrounds may have an equivalent or increased risk of disordered eating and eating disorders.12,13 Due to contradictory findings, however, less is known about the weight loss behaviors of individuals from various racial and ethnic minority backgrounds.
Dieting, exercise, the use of diet pills and laxatives, and self-induced vomiting are weight loss methods that have received the most research attention. Of these methods, diet and exercise remain the most used.14 The discourse surrounding the relationship between diet and exercise and an individual’s health, well-being, and weight is contentious. First, the term “dieting” encompasses a wide range of behaviors, from reducing the consumption of processed foods to engaging in potentially dangerous practices such as fasting.4,15 Although the definition of “dieting” varies, it generally refers to restricting or reducing food intake for the purpose of weight loss.
Even though quality nutrition is recommended for maintaining a healthy weight, research has failed to demonstrate the effectiveness of dieting for long-term weight loss and improvement of health outcomes.16,17 Furthermore, restrictive and compulsive weight loss-oriented dieting may have adverse effects on physical and psychological health. Dieting is a known risk factor for developing an eating disorder, and extreme dieting, such as fasting, can result in electrolyte and micronutrient deficiencies, as well as cardiac irregularities.2,4 While physical activity has been shown to reduce the risk of all-cause mortality, its effect on weight loss is unclear.18–21 Therefore, researchers advise against emphasizing weight loss as the main goal of exercise in an attempt to prevent discouragement from engaging in physical activity if weight loss results are not immediately apparent.21 In addition, individuals who engage in compensatory exercise in an attempt to “burn off” calories are more likely to develop an eating disorder.22 In extreme cases, individuals may develop exercise addiction characterized by loss of control over exercise habits and disruption of daily functioning.23 Exercise addiction has been linked to negative physical and psychological outcomes, including increased eating disorder pathology, social impairment, and physical injuries.23,24 Exercise addiction is also common, and according to a systematic review, its prevalence ranged from 3% to 21.4% among college and university students.25 Thus, given mixed findings on the effects of weight-loss oriented dieting and exercise, close monitoring of these behaviors is warranted.
Laxative abuse, the use of diet pills, and self-induced vomiting are considered to be especially dangerous weight loss practices, and previous researchers have categorized them as extreme weight control behaviors (EWCB).26 These methods are associated with an increased risk of depression, suicidality, adverse health outcomes, and future weight gain.1,5,27 Independently, diet pill use has been linked to cardiovascular and neurological problems,4 and side effects include psychiatric, gastrointestinal, and autonomic disturbances as well as an increased risk of strokes and myocardial infarctions.28 Similarly, purging behaviors, such as vomiting and laxative use, have been linked to negative health outcomes. As a method of weight management, self-induced vomiting may result in neuroendocrine abnormalities,29 deteriorated oral health, including dental erosion,30 gastroesophageal reflux disease, and an increased risk of esophageal cancer.31 Laxative abuse can cause structural colonic change, dehydration and electrolyte imbalance which in turn may result in muscle weakness and paralysis, renal dysfunction, and cardiac arrhythmia.31–34
Compared to other age groups, the college years are linked to a greater likelihood of developing an eating disorder and a higher incidence of unhealthy weight control behaviors.35 According to Wharton et al, 50% of college students in the United States attempted to lose weight in the past 30 days, and 12.3% used laxatives, diet pills, or self-induced vomiting as a weight loss strategy in the same time period.36 College students were more likely than other age groups to engage in EWCB, such as vomiting or taking diet pills,37 and an upward trend in the use of EWCB have been reported.38
Other demographic differences in weight loss behaviors have been observed. Researchers have shown that, when considering biological sex, women engage in weight control behaviors at a higher rate than men. This is likely driven by the fact that women experience more weight stigma than men and are attempting to counter it by losing weight.10,39 Female college students reported experiencing more weight stigma and engaging in more weight loss behaviors than male college students.40 Notably, similar proportions of both sexes use various weight loss strategies, with diet and exercise being the most prevalent among both women and men.41,42 However, weight loss behaviors remain understudied in men.41
Racial and ethnic disparities in weight loss behaviors have been reported by researchers. While young White women have been traditionally viewed as the primary risk group for developing unhealthy weight loss practices and, by extension, eating disorders, emerging research findings challenge this belief. For instance, Crago and Shisslak,43 in their review, found that women from racial and ethnic minority backgrounds were either equally or more likely than White women to engage in purging behaviors such as taking laxatives or self-induced vomiting, but dieting was more commonly endorsed by White female participants. However, when examining weight loss strategies more closely across specific racial and ethnic groups, no clear pattern emerges. Black, Hispanic/Latina, girls who identified as Other have been found to engage more EWCB that White adolescent girls; however, the findings have been inconsistent across studies.44–46 However, at least one nationally representative study found that White female youth engaged in more EWCB than females from other racial and ethnic backgrounds.15 In contrast, Native American girls did not differ from girls of other racial and ethnic backgrounds in their weight loss behaviors, but they were more likely than White girls to report wanting a larger body size.47 While most research has focused on female participants, male participants from racial and ethnic minority backgrounds have been studied. Researchers found that Black, Asian, Hispanic/Latino, Native American adolescents engage in more dieting and EWCB than White male adolescents; however, as with women, the results across studies have been inconsistent.44,45,47,48
Given the previous studies’ mixed findings, further investigation of the cross-ethnic differences in the prevalence of weight control patterns remains important. These findings have the potential to uncover risk factors associated with certain racial and ethnic groups to help inform the development and modification of treatment and prevention programs and decrease barriers to healthcare access.43,49 Because college students are disproportionately affected by eating disorders and harmful weight loss practices, college campuses are essential locations for promoting healthy behaviors and conducting research on weight loss techniques. Therefore, additional cohort-specific research on weight loss techniques is required.
The purpose of the present study was to identify racial and ethnic differences in the prevalence of various weight loss behaviors, utilizing a large sample of college students from a nationally representative survey. We hypothesized that 1) Female students from racial and ethnic minority backgrounds would be more likely to engage in weight loss behaviors than White female students; and 2) Male students from racial and ethnic minority backgrounds would be more likely to engage in weight loss behaviors than White male students. Because of inconsistent research findings, we did not make directional hypotheses about differences in the likelihood of engaging in weight loss behaviors among male or female students from specific racial and ethnic minority backgrounds.
Materials and Methods
Participants
The data from the American College Health Association-National College Health Assessment (ACHA-NCHA) II-C survey from the collection periods of Fall 2015 through Spring 2019 were examined (M age = 22.5, SD = 6.091). The ACHA-NCHA is a nationally representative survey of health-related behaviors of college and university students conducted biannually across US college campuses in the spring and fall. Between the fall of 2015 and the spring of 2019, a total of 426,425 college students who were at least 18 years of age or older completed the survey. On college and university campuses, the ACHA-NCHA II is administered according to each institution’s specific human research policies. The participating university administered surveys using either paper or electronic forms.
Demographic data are presented in Table 1. Most students were female (68.5%), White (60%), enrolled full-time (92.4%), attended a four-year college (94.7%), and participated in the online version of the survey (95.8%). The sample included 4.4% Black students, 10.5% Biracial/Multiracial students, 12.6% Asian students, 10.4% Hispanic or Latino/a students, 0.5% American Indian, Alaska Native, and/or Native Hawaiian students, and 1.6% students who self-identified as Other. Of the 10.5% of participants who were classified as Biracial/Multiracial, 4.4% selected that option, while the remaining 6.1% selected more than one option and were re-classified as Biracial/Multiracial. We expand more on the reasons to categorize those who selected more than one option as Biracial/Multiracial in the Measures section of this study.
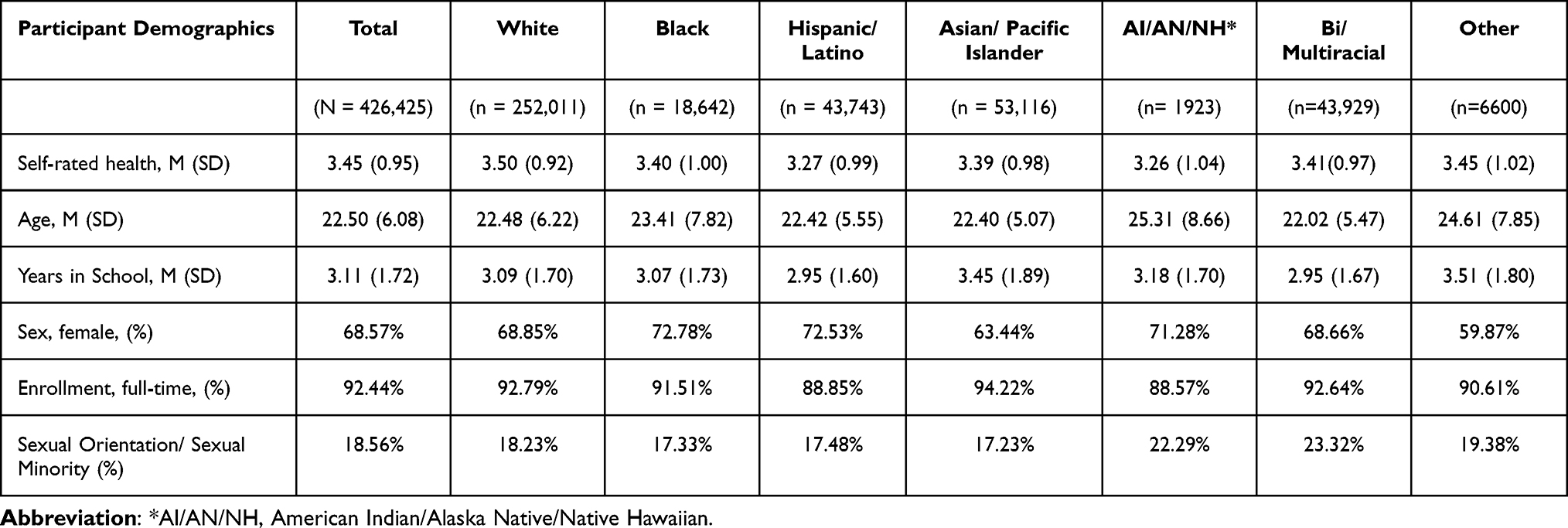 |
Table 1 Demographic Characteristics of the Sample |
Measures
Race and Ethnicity and Biological Sex
To indicate their race and ethnicity, students were asked to choose one or more of the following options: White, Black, Hispanic or Latino/a, Asian or Pacific Islander, American Indian, Alaska Native, or Native Hawaiian, and Biracial or Multiracial. Those who chose only Biracial/Multiracial and those who chose more than one option were categorized as Biracial/Multiracial. This decision was made on the basis of previous studies that analyzed the same dataset, as well as the theoretical framework presented by Burke et al which posits that holding multiple racial and ethnic identities may serve as an additional risk factor for the development of eating disorders and the combination of specific racial and ethnic backgrounds may entail different levels of risk.50–53
Biological sex was assessed with the question What sex were you assigned at birth, such as on an original birth certificate? The answers were female and male. Female was coded as 0, and male was coded as 1.
Control Variables
Self-rated health was assessed with the question: “How would you describe your general health?” The answers ranged from 1 (Excellent) to 5 (Poor) and were reverse coded for this study. In addition, age, sexual orientation, body mass index (BMI), and enrollment status were measured. Sexual orientation options included Asexual, Bisexual, Gay, Lesbian, Pansexual, Queer, Questioning, Same Gender Loving, Straight/Heterosexual, and Other. Because sexual orientation was used as a control variable it was dichotomized into straight and sexual minority for this study. Straight was coded as 0, and sexual minority was coded as 1. Enrollment was also dichotomized into part-time and full-time categories. Full-time enrollment was coded as 0, and part-time was coded as 1. In the analysis, age, BMI, and self-rated health variables were treated as continuous, while sex, sexual orientation, and enrollment status were treated as categorical.
Weight Loss Behavior
Weight loss behavior was assessed with the question:
Within the last 30 days, did you do any of the following: exercise to lose weight; diet to lose weight; vomit or take laxatives to lose weight; and/or take diet pills to lose weight?
Response options to each weight loss behavior were either no or yes. Thus, four separate weight loss behaviors were measured.
Statistical Analysis
Point biserial and tetrachoric correlations were calculated to detect potential covariates associated with the dichotomous weight loss behavior variables.
To ensure accurate analysis of the dichotomous outcome variables (exercise to lose weight, diet to lose weight, vomit or take laxatives to lose weight, and/or take diet pills to lose weight), four separate multivariable binary logistic regression analyses were conducted - one for each outcome variable. The variables found to be significant in the correlational analyses, ie, age, BMI, sexual orientation, self-rated health, and enrollment status, further referred to as control variables, were entered in block one, biological sex was entered in block two, racial and ethnic group - in block three. Interaction terms were created for each racial and ethnic group and biological sex and were entered in block four.
Interactions that were found significant were further probed by performing analyses separately for females and males with each behavior as the dependent variable (eg, exercise to lose weight, diet to lose weight, vomit or take laxatives to lose weight, take diet pills to lose weight). The control variables (age, BMI, sexual orientation, self-rated health, and enrollment status) were entered into block one, and racial and ethnic groups were entered in block two.
SPSS (version 28) was used for all the analyses. Across study variables, missing data ranged from 1.3% to 2.4% and listwise deletion was used for missing cases. The significance level was set at p < 0.05. All relevant assumptions were tested, and no violations were identified: 1) all observations were independent;54 2) the outcome categories were mutually exclusive; 3) according to Cook’s distance, there were no influential outliers in the data as no observations had a distance greater than 1. Correlational analysis did not reveal any evidence of multicollinearity.
Results
Overall, 53.5% of respondents exercised to lose weight, 40.3% dieted to lose weight, 2.8% vomited and used laxatives to lose weight, and 2.9% took diet pills. In addition, the majority’s BMI (57.4%) fell within the recommended range, 37.4% of students’ BMIs were overweight or obese, and 5.2% of students were underweight.
The results of correlation analysis are presented in Table 2. Age was positively correlated with exercising, dieting, and taking diet pills (r = 0.013, r = 0.062, r =0.013, respectively) but negatively correlated with vomiting or taking laxatives to lose weight (r = −0.025). There was a significant negative correlation between all four weight loss behaviors and biological sex (r = −0.124, for exercise; r = −0.111, for diet; r = −0.074, for vomiting and laxative use; r = −0.053, for diet pill use), indicating that women were more likely to engage in these behaviors than men. There was a significant negative correlation between weight loss behaviors and self-rated health (r = −0.009, for exercise; r = −0.070, for diet, r = −0.058, for vomiting and laxative use, and r = −0.047, for diet pill use). There was a significant positive relationship between body mass index (BMI) and all four weight loss methods (r = 0.208, for exercise; r = 0.251, for diet; r = 0.024, for vomiting and laxative use; r = 0.098, for diet pill use). Significant relationships between the outcome variables and sexual orientation and enrollment status were also observed. There was significant positive correlation between sexual orientation and vomiting or taking laxatives (r = 0.045) and sexual orientation and taking diet pills (r = 0.015), indicating that straight students were more likely to engage in these behaviors. Conversely, there was a negative correlation between sexual orientation and exercise (r = −0.036), with sexual minority students more likely to exercise as a weight loss method. Additionally, there was a positive correlation between enrollment status and certain weight loss behaviors, with those enrolled part-time more likely to use methods such as exercise, dieting, and diet pill use (r = 0.013, r = 0.037, r = 0.013 respectively) and those enrolled full-time more likely to use vomiting or taking laxatives as a weight loss method (r = −0.005).
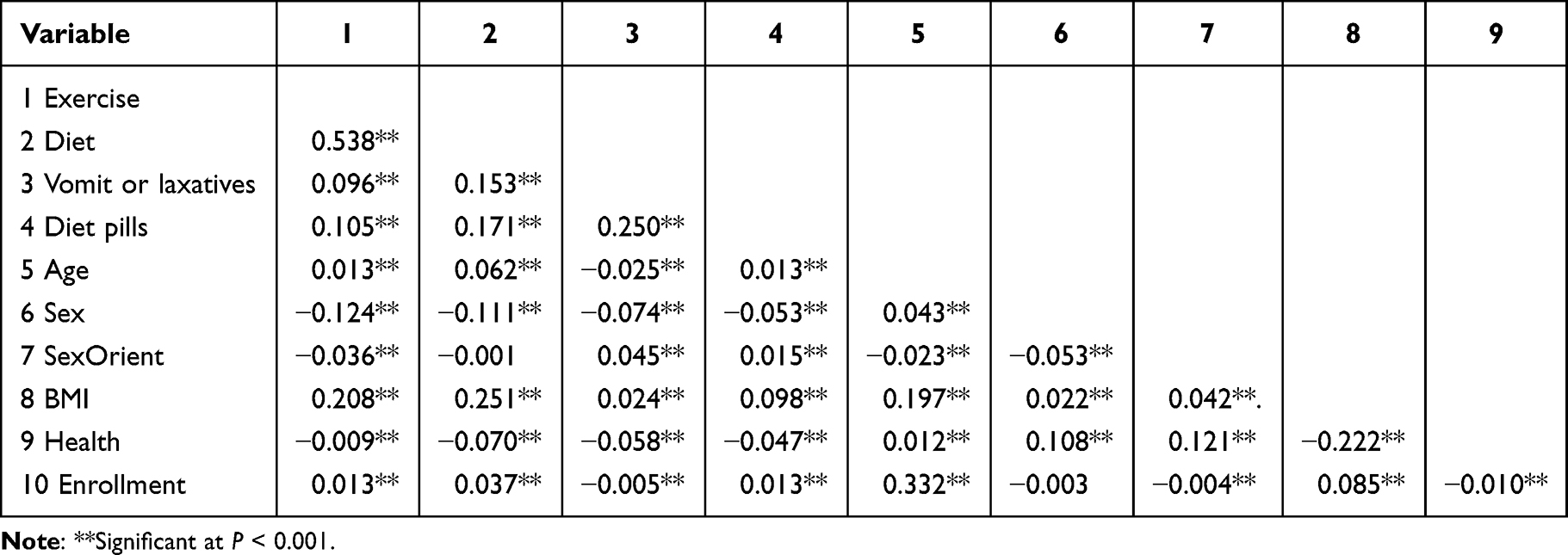 |
Table 2 Zero-Order Correlations Among Study Variables |
Exercise to Lose Weight
For exercise to lose weight, partial regression coefficients, ORs, and confidence intervals are presented in Table 3, as well as overall model fit statistics for the final block of the analyses. Here we present the change in model fit statistics for each block of the analyses.
 |
Table 3 Predictors of Exercising to Lose Weight Among College Students |
In block one, the control variables produced a significant improvement in model fit over a null model (χ2 (5) = 20,780.978, p < 0.001). In block two, biological sex produced a significant improvement in model fit above and beyond control variables (∆χ2(1) = 7773.385, p < 0.001). In block two, there was a significant relationship between biological sex and the likelihood of exercising to lose weight (OR = 0.532, 95% CI = [0.524, 0.539]). Thus, female students had 1.880 times higher odds of exercising to lose weight than male students.
In block three, race and ethnicity significantly improved model fit beyond control variables and biological sex (∆χ2(6) = 1198.594, p < 0.001). In block three, the odds of exercising to lose weight were 1.724 times higher for White students than Black students (OR = 0.580, 95% CI = [0.561, 0.600]), and 1.218 times higher than for students who identified as “Other” (OR = 0.821, 95% CI = [0.778, 0.867]). The odds of exercising to lose weight were 1.075 times higher for Asian students than for White students (OR = 1.075, 95% CI = [1.054, 1.097]). There were no significant differences in likelihood of exercising to lose weight between White and Hispanic/Latino students (p = 0.763), White and American Indian/Alaska Native and Native Hawaiian (AI/AN/NH) students (p = 0.390), or White and Biracial/Multiracial students (p = 0.548).
In block four, there was a significant improvement in model fit after adding the interaction terms (∆χ2(6) = 726.54, p < 0.001). The interaction terms between biological sex and race and ethnicity were significant (Supplemental Table 1). To further probe the interaction terms, two separate binary logistic regression analyses were performed for female and male groups.
For female students, in block one, control variables produced a significant improvement in model fit over a null model (χ2 (5) = 12,239.096, p < 0.001). Race and ethnicity were entered in block two and produced a significant improvement in model fit above and beyond control variables (∆χ2(6) =1039.629, p < 0.001). The results of the full model for female students are presented in Table 3 (the results of block two for female students). Black, Hispanic/Latino, Asian, and Biracial/Multiracial female students and students who identified as Other had lower odds of exercising to lose weight than their White counterparts. For White female students, the odds of exercising to lose weight were 1.818 times higher than for Black female students (OR = 0.550, 95% CI = [0.529, 0.571]), 1.157 times higher than for Hispanic/Latina female students (OR =0.864, 95% CI = [0.842, 0.887]), 1.053 higher than for Asian female students (OR = 0.950, 95% CI = [0.926, 0.974]), 1.058 times higher than for Biracial/Multiracial female students (OR = 0.945, 95% CI = [0.921, 0.970]), and 1.307 times higher than for students who identified as “Other” (OR = 0.765, 95% CI = [0.714, 0.819]). The odds of exercising to lose weight did not significantly differ for White female students relative to AI/AN/NH female students (p= 0.983).
For male students, there was a significant improvement over a null model in block one after entering control variables (χ2 (5) = 13,577.764, p < 0.001). In block two, ethnicity produced a significant improvement in model fit above and beyond control variables (∆χ2(6) = 685.188, p < 0.001). As can be seen from Table 3, in block two, Hispanic/Latino, Asian, and Biracial/Multiracial students had higher odds of exercising to lose weight than White students (OR = 1.428, 95% CI = [1.368, 1.491]- Hispanic/Latino; OR = 1.356, 95% CI = [1.310, 1.403] – Asian; OR = 1.125, 95% CI = [1.081, 1.171] – Biracial/Multiracial). Conversely, White male students had 1.418 times higher odds of exercising to lose weight than Black male students (OR = 0.705, 95% CI = [0.660, 0.753]). No significant differences were found between White and AI/AN/NH male students (p = 0.097) and White students and male students who identified as “Other” (p=0.071).
Diet to Lose Weight
Partial regression coefficients, ORs, and confidence intervals are presented in Table 4, as well as overall model fit statistics for the final block of the analyses. Here we present the change in model fit statistics for each block of the analyses.
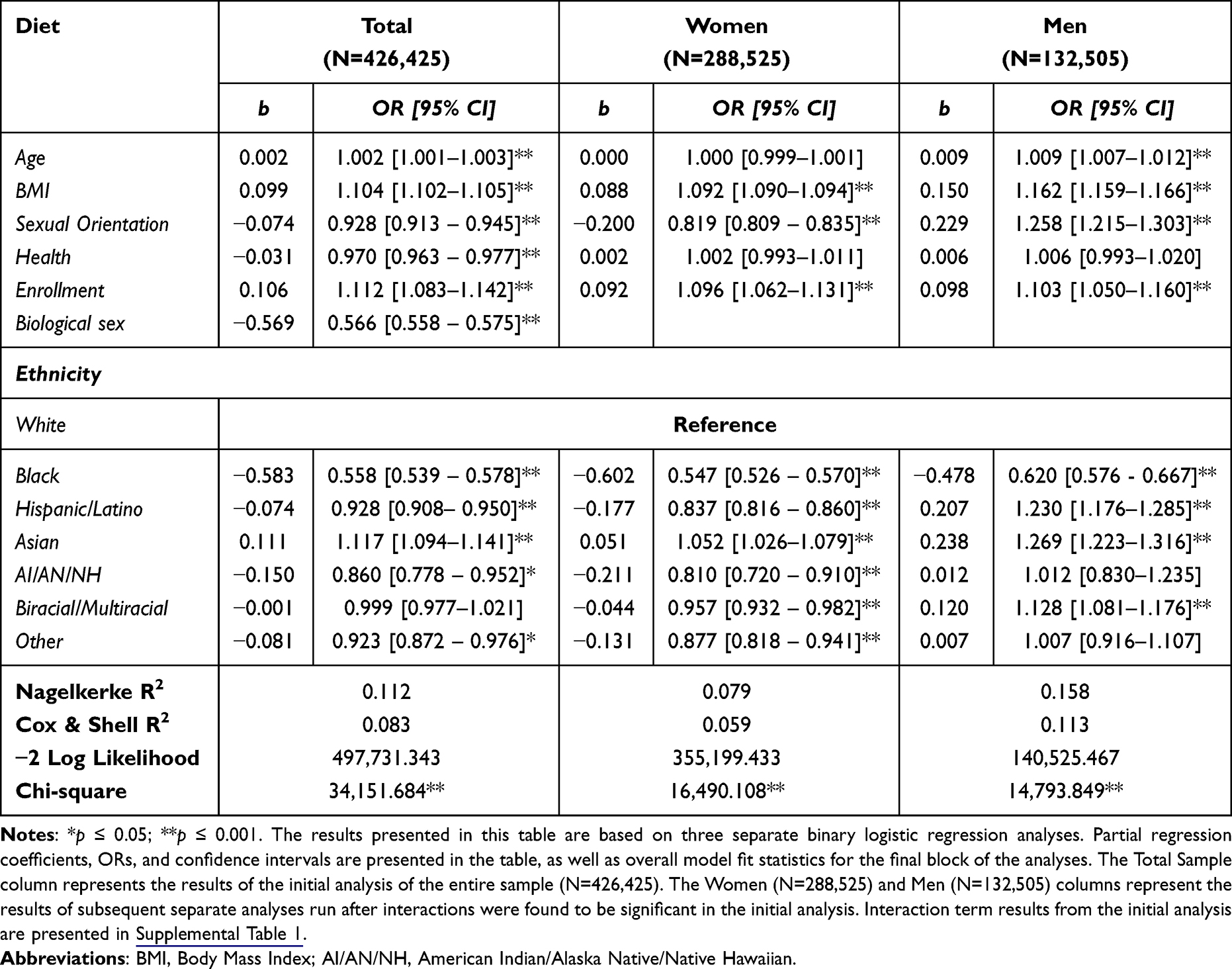 |
Table 4 Predictors of Dieting to Lose Weight Among College Students |
In block one, there was a significant improvement in model fit over a null model (χ2 (5) = 26,621.311, p < 0.001). Biological sex produced a significant improvement in model fit above and beyond control variables in block two (∆χ2(1) = 5838.349, p < 0.001). The odds of dieting to lose weight were 1.768 times higher for female than for male students (OR = 0.566, 95% CI = [0.558, 0.575]). In block three, ethnicity significantly improved model fit beyond control variables and biological sex (∆χ2(6) = 1319.999, p < 0.001). In block three, Black, Hispanic/Latino, AI/AN/NH, and students in the “Other” racial and ethnic group were less likely to diet to lose weight than White students. The odds of dieting to lose weight were 1.792 times higher for White students than for Black students (OR = 0.558, 95% CI = [0.539, 0.578]), 1.078 times higher than for Hispanic/Latino students (OR = 0.928, 95% CI = [0.908, 0.950]), 1.163 times higher than for AI/AN/NH (OR = 0.860, 95% CI = [0.778, 0.952]), and 1.083 times higher than for students who identified at Other (OR = 0.923, 95% CI = [0.872, 0.976]). However, the odds of dieting to lose weight were 1.117 times higher for Asian students than for White students (OR = 1.117, 95% CI = [1.094, 1.141]). There were no significant differences in the odds of dieting to lose weight between White and Biracial/Multiracial students (p = 0.907). In block four, interaction terms produced a significant improvement of model fit (∆χ2(6) = 372.025, p < 0.001). All interaction terms between biological sex and race and ethnicity were significant (Supplemental Table 1). To further probe the interaction terms, two separate binary logistic regression analyses were performed for female and male groups.
For female students, control variables produced a significant improvement in model fit (χ2 (5) = 15,400.823, p < 0.001). After controlling for covariates, ethnicity produced a significant improvement in model fit in block two (∆χ2(6) = 1089.285, p < 0.001). As can be seen from Table 4, in block 2, the odds of dieting to lose weight were 1.052 higher for Asian female students than for White female students (OR = 1.052, 95% CI = [1.026, 1.079]). However, compared to White female students, female students from other racial and ethnic minority backgrounds had lower odds of dieting to lose weight. Specifically, the odds of dieting to lose weight were 1.828 times higher for White female students than for Black female students (OR=0.547, 95% CI = [0.526, 0.570]). Likewise, the odds of dieting to lose weight were 1.195 times higher for White female students than for Hispanic/Latino female students (OR = 0.837, 95% CI = [0.816, 0.860]), 1.235 times higher than for AI/AN/NH students (OR = 0.810, 95% CI = [0.720, 0.910]), 1.045 times higher than for Biracial/Multiracial students (OR = 0.957, 95% CI = [0.932, 0.982]), and 1.140 times higher than for students who identified as Other (OR=0.877, 95% CI = [0.818, 0.941]).
For male students, in block one, control variables produced a significant improvement over a null model (χ2 (5) = 14,345.532, p < 0.001). After controlling for control variables, ethnicity produced a significant improvement in model fit above control variables in block two (∆χ2(6) = 448.317, p < 0.001). As evident from Table 4, male Hispanic/Latino, Asian, and Biracial/Multiracial students were more likely to diet to lose weight than White male students (OR =1.230, 95% CI = [1.176, 1.285]; OR = 1.269, 95% CI = [1.223, 1.316]; OR = 1.128, 95% CI =1.081, 1.176], respectively). However, the odds of dieting to lose weight were 1.613 times higher for White male students than for Black male students (OR= 0.620, 95% CI = [0.576, 0.667]. The odds of dieting to lose weight did not significantly differ for White male students relative to AI/AN/NH male students (p=0.906) or male students who identified as” Other’ (p=0.884).
Vomiting or Taking Laxatives to Lose Weight
Partial regression coefficients, ORs, and confidence intervals are presented in Table 5, as well as overall model fit statistics for the final block of the analyses. Here we present the change in model fit statistics for each block of the analyses.
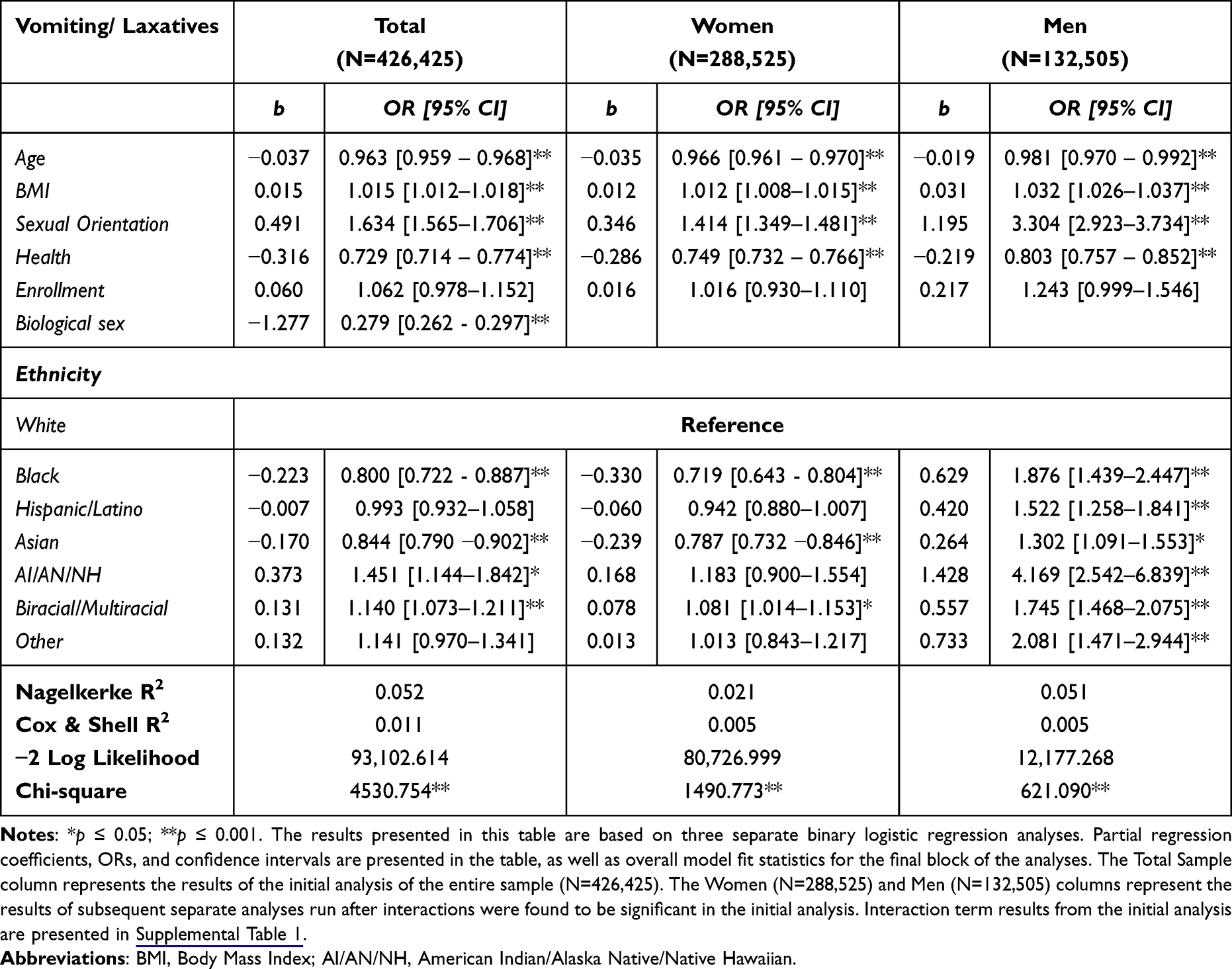 |
Table 5 Predictors of Vomiting or Taking Laxatives to Lose Weight Among College Students |
In block one, the control variables produced a significant improvement in model fit over a null model (χ2 (5) = 2160.256, p < 0.001). In block two, biological sex produced a significant improvement in model fit above and beyond control variables (∆χ2(1) = 2181.912, p < 0.001). The odds of vomiting or taking laxatives to lose weight were 4.673 times higher for women than for men (OR=0.279, 95% CI = 0.262, 0.297]). Race and ethnicity significantly improved model fit beyond control variables and biological sex in block three (∆χ2(6) = 82.713, p < 0.001). The odds of using vomiting or taking laxatives for weight loss were 1.250 times higher for White students than for Black students (OR = 0.800, 95% CI = [0.722, 887]), and the odds were also 1.185 times higher for White than for Asian students (OR = 0.844, 95% CI = [0.790, 0.902]). The odds of vomiting and taking laxatives to lose weight were 1.451 times higher for AI/AN/NH students (OR= 1.451, 95% CI = [1.144, 1.842]) and 1.140 times higher for Biracial/Multiracial students (OR= 1.140, 95% CI = [1.073, 1.211]) than for White students. The odds of vomiting and taking laxatives to lose weight did not differ significantly between White and students who identified as “Other” (p=0.111) and White and Hispanic/Latino students (p=0.826). In block four, interaction terms produced a significant improvement in model fit (∆χ2(6) = 105.874, p < 0.001). All interaction terms between biological sex and race and ethnicity were significant (Supplemental Table 1). In order to further probe the interaction terms, two separate binary logistic regression analyses were performed for female and male groups.
For female students (Table 5), in block one, there was a significant improvement in model fit over a null model (χ2 (5) = 1398.322, p < 0.001). In block two, ethnicity produced a significant improvement above and beyond control variables (∆χ2 (6) = 92.451, p < 0.001). The odds of vomiting and taking laxatives to lose weight were lower for Black and Asian female students than for White female students (OR = 0.719, 95% CI = [0.643, 0.804]; OR = 0.787, 95% CI = [0.732, 0.846], respectively). Thus, the odds of vomiting or taking laxatives to lose weight were 1.391 times higher for White female students than for Black female students and 1.271 times higher than for Asian women. The odds of vomiting or taking laxatives to lose weight were 1.081 times higher for Biracial/Multiracial students (OR = 1.081, 95% CI = [1.014, 1.153]. The differences in the odds of vomiting or taking laxatives to lose weight between White female students and Hispanic/Latina (p = 0.080), AI/AN/NH (p = 0.228), and female students who identified as “Other” (p= 0.891) were not significant.
For male students (Table 5), control variables produced a significant improvement in model fit over a null model in block one (χ2 (5) = 538.232, p < 0.001). In block two, after controlling for control variables, ethnicity was a significant predictor of vomiting or taking laxatives to lose weight (∆χ2(6) = 82.858, p < 0.001). Male students from racial and ethnic minority backgrounds were more likely to use vomiting or taking laxatives as weight loss methods than White male students. The odds of using vomiting or taking laxatives to lose weight were 1.876 times higher for Black male students (OR = 1.876, 95% CI = [1.439, 0.2.447]), 1.522 times higher for Hispanic/Latino students (OR = 1.522, 95% CI = [1.258, 1.841]), 1.302 times higher for Asian students (OR = 1.302, 95% CI = [1.091, 1.553]), 4.169 times higher for AI/AN/NH students (OR = 4.169, 95% CI = [2.542, 6.839]), 1.745 times higher for Biracial/Multiracial students (OR = 1.745, 95% CI = [1.468, 2.075]), and 2.081 times higher for students who identified as “Other” (OR = 2.081, 95% CI = [1.471, 2.944]), relative to White male students.
Diet Pills to Lose Weight
Partial regression coefficients, ORs, and confidence intervals are presented in Table 6, as well as overall model fit statistics for the final block of the analyses. Here we present the change in model fit statistics for each block of the analyses.
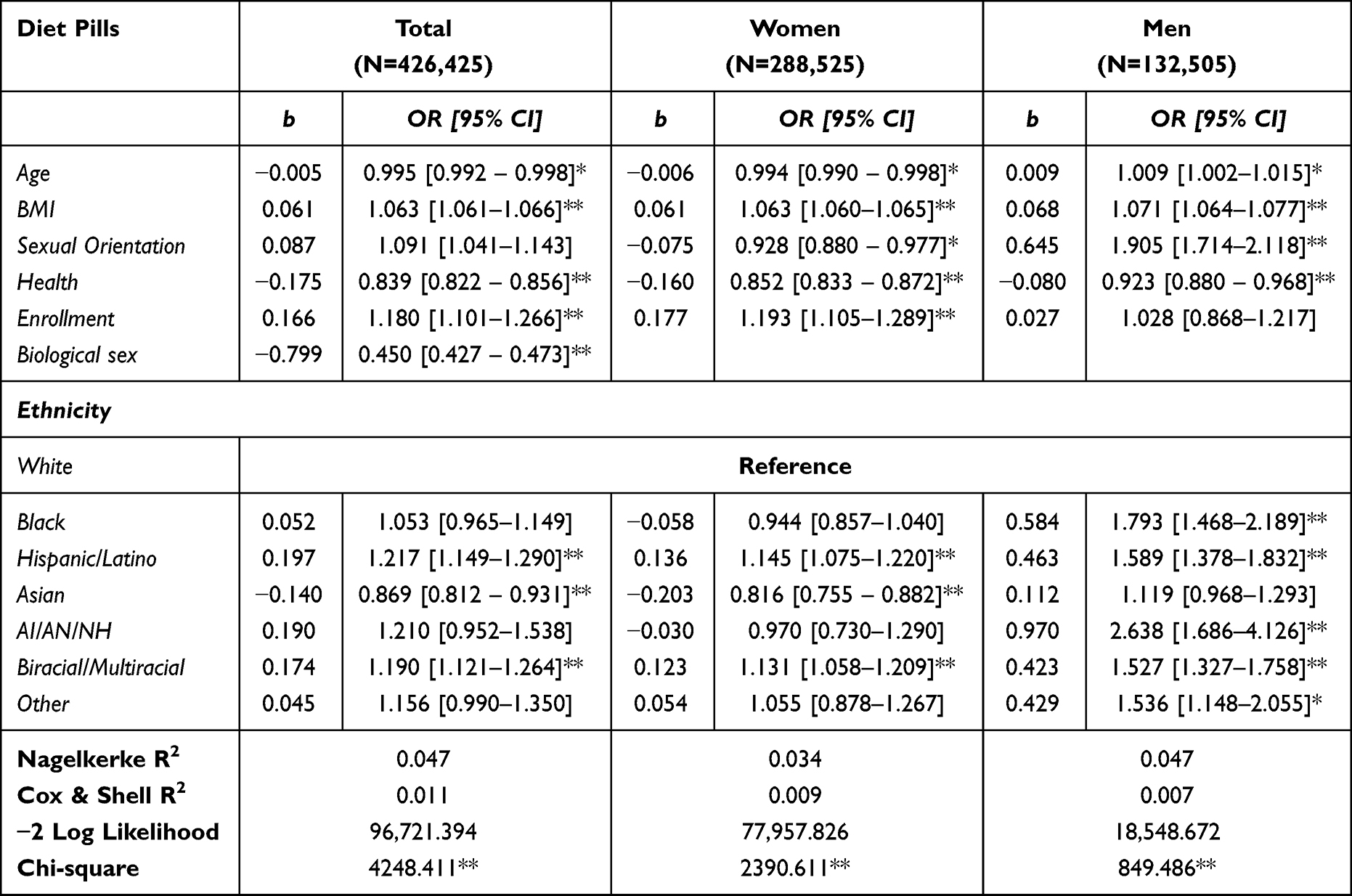 |
Table 6 Predictors of Taking Diet Pills to Lose Weight Among College Students |
In block one, the control variables produced a significant improvement in model fit over a null model (χ2 (5) = 3037.944, p < 0.001). Adding biological sex in block two produced a significant improvement in model fit above and beyond control variables (∆χ2(1) = 1110.624, p < 0.001). The odds of taking diet pills to lose weight were 2.222 times higher for women than men (OR = 0.450, 95% CI = [0.427, 0.473]). In block three, adding ethnicity significantly improved model fit beyond control variables and biological sex (∆χ2(6) = 99.842, p < 0.001). In block three, compared to White students, the odds of taking diet pills to lose weight were 1.217 times higher (OR = 1.217, 95% CI = [1.149, 1.290]) for Hispanic/Latino and 1.190 times higher (OR = 1.190, 95% CI = [1.121, 1.264]) for Biracial/Multiracial students. However, the odds of taking diet pills were 1.151 times higher for White students than for Asian students (OR = 0.869, 95% CI = [0.812, 0.931]). There were no significant differences in taking diet pills between White students and Black (p = 0.244), AI/AN/NH (p = 0.120), and students who identified as “Other” (p = 0.067). In block four, interaction terms produced a significant improvement in model fit (∆χ2(6) = 67.845, p < 0.001). All interaction terms between biological sex and race and ethnicity were significant (Supplemental Table 1). In order to further probe the interaction terms, two separate binary logistic regression analyses were performed for female and male groups.
For female students, adding control variables to block one produced a significant improvement over a null model (χ2(5) = 2322.251, p < 0.001). In block two, after adding ethnicity, there was a significant improvement in model fit above and beyond control variables (∆χ2(6) = 68.359, p < 0.001). As can be seen from Table 6, in block two, Hispanic/Latina (OR= 1.145, 95% CI = [1.075, 1.220]) and Biracial/Multiracial (OR= 1.131, 95% CI = [1.058, 1.209]) students were more likely to take diet pills than White female students. However, the odds of taking diet pills were 1.225 times higher for White female students than for Asian female students (OR = 0.816, 95% CI = [0.755, 0.882]). The odds of taking diet pills did not differ significantly between White female students and Black (p = 0.243), AI/AN/NH (p = 0.836), and female students who identified as “Other” (p = 0.567).
For male students, there was a significant improvement over a null model after adding control variables in block one (χ2(5) = 758.796, p < 0.001). In block two, entering ethnicity in block two produced a significant improvement above and beyond control variables (∆χ2(6) = 90.690, p < 0.001). Among male students (Table 6), in block two, Black, Hispanic/Latino, AI/AN/NH, Biracial/Multiracial, and Other students were more likely to take diet pills than White students (Black - OR= 1.793, 95% CI = [1.468, 2.189]; Hispanic/Latino - OR= 1.589, 95% CI = [1.378, 1.832]; AI/AN/NH - OR= 2.638, 95% CI = [1.686, 4.126]; Biracial/Multiracial - OR= 1.527, 95% CI = [1.327, 1.758]; Other – OR = 1.536, 95% CI = [1.148, 2.055]). There was no significant difference between Asian and White male students (p = 0.129).
Discussion
The purpose of the present study was to examine racial and ethnic differences in weight loss behaviors among a large diverse sample of college students. Overall, the prevalence of weight control behaviors was consistent with previous studies: more than half of the participants (53.5%) exercised to lose weight, and dieting prevalence was high (40.3%), while 2.8% of college students purged (vomited or took laxatives) to lose weight, and 2.9% took diet pills.36 Moreover, BMI was positively correlated with all four weight loss behaviors, indicating that individuals with higher BMI were more likely to engage in weight loss. This finding has been observed in previous research.45,47 However, despite the evidence to the contrary, it is still a widely held misconception that individuals with a higher BMI undertake fewer weight loss attempts and that their higher weight is solely the result of a lack of effort.10 This misguided belief leads to weight stigma, which in turn can result in significant psychological distress and the underdiagnosis of eating disorders in individuals with higher BMI.55–57 Several other notable findings emerged from this investigation.
In the present sample, female students were more likely than male students to engage in all types of weight control behaviors, which in consistent with previous reports.41,42 This result may be attributed to the fact that women are more likely to experience weight stigma and face greater pressure to conform to the thin ideal.40 However, men should not be overlooked in eating disorder research, as eating disorders and unhealthy weight loss practices among men are likely underdiagnosed, despite the fact that their prevalence continues to rise.58 Our findings suggest that men from racial and ethnic minority backgrounds may be at a higher risk for engaging in EWCB, as male students from racial and ethnic minority backgrounds engaged in more EWCB than White male students. Previous researchers have identified a similar pattern among adolescent boys: boys from racial and ethnic minority backgrounds were more likely than White boys to take diet pills and engage in purging and fasting behaviors, in a cross-sectional study involving more than 12,000 middle school students.45 Additionally, adolescent boys from Black, Hispanic/Latino, Asian, and combined Multiracial and Other backgrounds participated in EWCB at a higher rate than White boys.42 Native American boys engaged in more EWCB than Whites.47 To explain this phenomenon, researchers have hypothesized that males from racial and ethnic minority backgrounds are more susceptible to social and cultural isolation than White males making them more vulnerable to unhealthy weight loss behaviors (for a review, see Ricciardeli).59 The results from the present study have also extended those of previous researchers by analyzing separately Biracial/Multiracial and Other racial and ethnic groups, who were combined together in previous research studies.42 Despite constituting a substantial proportion of the population, Biracial/Multiracial and Other racial and ethnic groups are frequently ignored or grouped together in eating disorder research, obscuring the true prevalence of weight loss or disordered eating behaviors in these distinct populations.49,53
In accordance with previous research, Hispanic/Latino and Biracial/Multiracial male students were more likely to attempt losing weight, as they engaged in all four weight loss behaviors at a higher rate than White male students.42,53,60,61 Despite existing empirical data and theoretical models that include minority and acculturative stress, the precise mechanisms that lead to the over representation of these groups in disordered eating and weight loss behaviors remain unknown.53 Moreover, given not only substantial differences between Hispanic/Latino and Biracial/Multiracial groups of men, but also considerable heterogeneity within each group, it is likely that the pathways, through which these populations are affected, are distinct. For example, researchers conducting a recent qualitative study reported that Hispanic/Latino men found it particularly difficult to gain access to healthy food and a safe exercise environment, potentially making them more prone to unhealthy weight loss behaviors.62 A different mechanism might be responsible for engagement in weight loss behaviors among Biracial/Multiracial men. It has been hypothesized that the intersection of dual identities, minority stress and the need to balance two or more cultures might put Biracial/Multiracial men at an increased mental health risk, including an elevated incidence of an eating disorder diagnoses.53 Previous researchers have also found the specific makeup of Biracial/Multiracial identity may play a differential role in eating disorder behavior. Specifically, they found that Biracial men who were Black and White, Black and Hispanic/Latino, or Native Hawaiian and White were more likely to experience eating disorder symptoms than White men and other groups of Biracial men.53 Taken together, these findings indicate the need for further investigation of the contributing systematic factors affecting the two racial/ethnic groups.
Similarly, Black, AI/AN/NH, male students who identified as Other were more likely to use EWCBs in order to lose weight than White men. Similar findings have been reported by other researchers.44–48 However, the precise reasons for why Black, AI/AN/NH, and male students who identified as Other engaged in more EWCBs but not diet and exercise are not entirely clear. Some researchers suggest that higher BMI might be a risk factor for engaging in EWCB among Black and AI/AN/NH men.47,48 However, in the present study, BMI was controlled and yet the findings remained significant, suggesting that other factors may be at play. Researchers have also hypothesized that intergenerational trauma, such as that experienced by the AI/AN/NH population as a result of European colonization, is a possible reason for high rates of eating disorders and unhealthy weight control behaviors.63–65 Discussions about the historical origins of weight stigma have revealed that weight-based discrimination is deeply intertwined with racial discrimination, particularly in relation to Black bodies.66,67 Weight stigma, in turn, has been associated with EWCB in correlational and longitudinal studies, which suggests a possible mechanism that could explain higher rates of EWCB among Black men in comparison to their White counterpart.68,69 Less is known about men who identify as Other. One study found that college students in the Other racial and ethnic category had the highest prevalence of eating disorders.61 However, because of a small sample size, AI/AN/NH, Asian, and Biracial students were categorized as Other. Despite the lack of clear reasons, the findings of the present study are concerning, as those who engage in EWCB are at higher risk of poor physical outcomes and developing eating disorders and depression.3 Given the complex interaction of cultural, societal, and historical factors that influence weight loss behaviors of individuals from racial and ethnic minority backgrounds, as well as the heterogeneity of Black, AI/AN/NH, and male students who identified as Other, additional research into their weight loss behavior and experience is warranted.
In the present study, fewer cross-ethnic discrepancies in weight loss behaviors among female participants were observed; however, they merit further discussion. With few exceptions, female students from racial and ethnic minority backgrounds were less likely to diet and exercise than White female students. This finding is partially supported by previous reports that White women were more likely to restrict their food intake to lose weight than women from racial and ethnic minority backgrounds. Dieting and exercise are deeply ingrained in the predominantly White mainstream culture; therefore, White women who might identify with its values more than women from racial and ethnic minority backgrounds may be more susceptible to engaging in these behaviors.70 Notably, in this sample, Asian female students were more likely to diet than White female students, which is also consistent with previous research.71 Despite the fact that restrictive weight loss behaviors among Asian and White women have been described in the past, the precise causes remain unknown. Given that these groups frequently place a high value on restraint, it is plausible that cultural factors make Asian and White women more likely to diet.72,73
When examining weight loss behaviors across ethnicities, it appears that Biracial/Multiracial female students were more likely than their White counterparts to engage in EWCB, but less likely to diet and exercise. This finding is consistent with previous research, and, as with men, the intersection of multiple identities and minority stress have been implicated in this observation.53 It has been hypothesized that multiple or dual identities carry the risk of multiple discrimination for Biracial/Multiracial individuals, thereby increasing the risk of eating pathology.
An opposite trend was observed for Asian female students, who were, on the contrary, less likely to use EWCB to lose weight, but more likely to diet than White female students. Lower incidence of purging behavior and diuretic use among Asian women has been previously reported.74,75 Asian women’s lower BMI was used as an explanation for this finding,75 but in this study, BMI was controlled, reducing its potential impact on the results and suggesting that cultural factors might underlie this observation.
No other discernible patterns were identified on the prevalence of unhealthy weight control behaviors among female students, which is consistent with a growing body of evidence, and indicates that women from racial and ethnic minority backgrounds might be at an equal risk of engaging in disordered eating and weight loss behaviors than White women.12,49,76 However, the reasons for weight loss behaviors might differ between women from racial and ethnic minority backgrounds and White women. Multiple researchers have identified discrimination and acculturation stress as the driving forces behind eating disorders among individuals from racial and ethnic minority backgrounds, while the pressure to succeed have been associated with eating disorders among White women.73
Several limitations of the present study should be addressed. First, because this is a cross-sectional study, no conclusions regarding cause and effect can be drawn. Second, because a self-report questionnaire was used, recall bias may have affected the responses. In addition, only behaviors in the past 30 days were measured, and patterns over longer time periods may differ from those found in this study. Moreover, because of the nature of the questionnaire, the extent of the students’ exercise and dietary habits were not assessed and their effect on students’ well-being could not have been studied. Therefore, the results should be interpreted with caution. Diet and exercise encompass a broad spectrum of activities and practices, ranging from healthy to dangerous that can be associated with both positive and negative outcomes.4,15 Hence, it is important to consider the extent and effect of diet and exercise to lose weight across diverse racial and ethnic groups. Such considerations provide a valuable context for developing interventions, promoting health behaviors, and identifying health disparities. It is of note, however, that in the present study both diet to lose weight and exercise to lose weight were negatively correlated with students’ self-rated health. This indicates a potential negative effect on students’ health. Therefore, the results of the present study warrant additional research to determine the extent and effect of these behaviors among various racial and ethnic groups. Finally, many of the findings had small effect sizes, which may not represent meaningful differences due to the extremely large sample size
Despite the weaknesses, the current study has several noteworthy strengths. One strength is that the large sample size allowed us to discern between multiple racial and ethnic groups, including the often-overlooked Biracial/Multiracial individuals and those who identify as Other, and to detect differences in the prevalence of four prevalent weight loss practices. Moreover, the data for the present study came from a nationally representative cohort, increasing the generalizability of the findings.
Conclusion
In conclusion, the results of this study contributed to the growing body of literature on disordered eating and weight loss strategies among men and women from racial and ethnic minority backgrounds. A higher prevalence of EWCBs was detected among male college students from racial and ethnic minority backgrounds compared to White male college students, indicating that these unhealthy behaviors, previously observed among adolescents from racial and ethnic minority backgrounds, persist into adulthood. Racial and ethnic differences in these behaviors were more pronounced in males than females, with Hispanic/Latino and Biracial/Multiracial men at particular risk. Female students from racial and ethnic minority backgrounds were less likely to diet and exercise than White female students, but most female students from racial and ethnic minority backgrounds did not differ from White female students in engaging in EWCB. The results of the present study underscore the importance of campus-based culturally sensitive educational programs on unhealthy weight management and eating disorder prevention. Previous researchers have demonstrated that peer-led non-diet programs on college campuses are effective in improving nutrition- and exercise-related behaviors and thought patterns.77 Thus, as a future direction, it may be valuable to tailor these programs for students from racial and ethnic minority backgrounds in order to address and prevent EWCB and unhealthy weight management among these populations.
Ethics Statement
This research was exempt from the IRB approval because secondary de-identified data were used.
Acknowledgments
The opinions, findings, and conclusions reported in this article are those of authors and do not represent the corporate opinions, views, or policies of the American College Health Association (ACHA). ACHA does not warrant nor assume any liability or responsibility for the accuracy, completeness, or usefulness of any information presented in this article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Neumark-Sztainer D, Wall M, Guo J, Story M, Haines J, Eisenberg M. Obesity, disordered eating, and eating disorders in a longitudinal study of adolescents: how do dieters fare 5 years later? J Am Diet Assoc. 2006;106(4):559–568. doi:10.1016/j.jada.2006.01.003
2. Patton GC, Selzer R, Coffey C, Carlin JB, Wolfe R. Onset of adolescent eating disorders: population based cohort study over 3 years. BMJ. 1999;318(7186):765–768. doi:10.1136/bmj.318.7186.765
3. Levinson J, Sarda V, Sonneville K, Calzo J, Ambwani S, Austin SB. Diet pill and laxative use for weight control and subsequent incident eating disorder in US young women: 2001–2016. Am J Public Health. 2019;110:e1–e3. doi:10.2105/AJPH.2019.305390
4. Daee A, Robinson P, Lawson M, Turpin JA, Gregory B, Tobias JD. Psychologic and physiologic effects of dieting in adolescents. (Review Article). South Med J. 2002;95(9):1032–1042. doi:10.1097/00007611-200295090-00016
5. Crow S, Eisenberg ME, Story M, Neumark-Sztainer D. Are body dissatisfaction, eating disturbance, and body mass index predictors of suicidal behavior in adolescents? A longitudinal study. J Consult Clin Psychol. 2008;76(5):887–892. doi:10.1037/a0012783
6. Ferraro ZM, Patterson S, Chaput JP. Unhealthy weight control practices: culprits and clinical recommendations. Clin Med Insights Endocrinol Diabetes. 2015;8:7–11. doi:10.4137/CMED.S23060
7. Chaitoff A, Swetlik C, Ituarte C, et al. Associations between unhealthy weight-loss strategies and depressive symptoms. Am J Prev Med. 2019;56(2):241–250. doi:10.1016/j.amepre.2018.09.017
8. Jacobi C, Hayward C, de Zwaan M, Kraemer HC, Agras WS. Coming to terms with risk factors for eating disorders: application of risk terminology and suggestions for a general taxonomy. Psychol Bull. 2004;130(1):19–65. doi:10.1037/0033-2909.130.1.19
9. Stoll LC. Fat Is a Social Justice Issue, Too. Humanity Soc. 2019;43(4):421–441. doi:10.1177/0160597619832051
10. Puhl RM, Lessard LM. Weight stigma in youth: prevalence, consequences, and considerations for clinical practice. Curr Obes Rep. 2020;9(4):402–411. doi:10.1007/s13679-020-00408-8
11. Stoll LC, Meadows A, Liebenstein S, Carlsen CE. Fatphobia. Policy Press; 2022:37–44. Available from: https://bristoluniversitypressdigital.com/display/book/9781447367420/ch004.xml.
12. Smolak L, Striegel-Moore RH. Challenging the myth of the golden girl: ethnicity and eating disorders. In: Eating Disorders: Innovative Directions in Research and Practice. American Psychological Association; 2001:111–132. doi:10.1037/10403-006
13. Striegel-Moore RH, Bulik CM. Risk factors for eating disorders. American Psychologist. 2007;62(3):181–198. doi:10.1037/0003-066X.62.3.181
14. Martin CB, Herrick KA, Sarafrazi N, Ogden CL. Attempts to lose weight among adults in the United States, 2013–2016. NCHS Data Brief. 2018;313:1–8.
15. Chin SNM, Laverty AA, Filippidis FT. Trends and correlates of unhealthy dieting behaviours among adolescents in the United States, 1999–2013. BMC Public Health. 2018;18(1):439. doi:10.1186/s12889-018-5348-2
16. Miller WC, Koceja DM, Hamilton EJ. A meta-analysis of the past 25 years of weight loss research using diet, exercise or diet plus exercise intervention. Int J Obes Relat Metab Disord. 1997;21(10):941–947. doi:10.1038/sj.ijo.0800499
17. Mann T, Tomiyama AJ, Westling E, Lew AM, Samuels B, Chatman J. Medicare’s search for effective obesity treatments: diets are not the answer. American Psychologist. 2007;62:220–233. doi:10.1037/0003-066X.62.3.220
18. Li T, Wei S, Shi Y, et al. The dose–response effect of physical activity on cancer mortality: findings from 71 prospective cohort studies. Br J Sports Med. 2016;50(6):339–345. doi:10.1136/bjsports-2015-094927
19. Volaklis KA, Halle M, Meisinger C. Muscular strength as a strong predictor of mortality: a narrative review. Eur J Intern Med. 2015;26(5):303–310. doi:10.1016/j.ejim.2015.04.013
20. Kraus WE, Powell KE, Haskell WL, et al. Physical activity, all-cause and cardiovascular mortality, and cardiovascular disease. Med Sci Sports Exerc. 2019;51(6):1270–1281. doi:10.1249/MSS.0000000000001939
21. Cox CE. Role of physical activity for weight loss and weight maintenance. Diabetes Spectr. 2017;30(3):157–160. doi:10.2337/ds17-0013
22. Ackard DM, Brehm BJ, Steffen JJ. Exercise and eating disorders in college-aged women: profiling excessive exercisers. Eat Disord. 2002;10(1):31–47. doi:10.1080/106402602753573540
23. Szabo A, Griffiths MD, de La Vega Marcos R, Mervó B, Demetrovics Z. Methodological and conceptual limitations in exercise addiction research. Yale J Biol Med. 2015;88(3):303–308.
24. Lichtenstein MB, Hinze CJ, Emborg B, Thomsen F, Hemmingsen SD. Compulsive exercise: links, risks and challenges faced. Psychol Res Behav Manag. 2017;10:85–95. doi:10.2147/PRBM.S113093
25. Marques A, Peralta M, Sarmento H, Loureiro V, Gouveia ÉR, Gaspar de Matos M. Prevalence of risk for exercise dependence: a systematic review. Sports Med. 2019;49(2):319–330. doi:10.1007/s40279-018-1011-4
26. Hazzard VM, Simone M, Austin SB, Larson N, Neumark-Sztainer D. Diet pill and laxative use for weight control predicts first-time receipt of an eating disorder diagnosis within the next 5 years among female adolescents and young adults. Int J Eat Disord. 2021;54(7):1289–1294. doi:10.1002/eat.23531
27. Utter J, Denny S, Robinson E, Ameratunga S, Crengle S. Identifying the ‘red flags’ for unhealthy weight control among adolescents: findings from an item response theory analysis of a national survey. Int J Behav Nutr Phys Act. 2012;9(1):99. doi:10.1186/1479-5868-9-99
28. Saper RB, Eisenberg DM, Phillips RS. Common dietary supplements for weight loss. afp. 2004;70(9):1731–1738.
29. Kaye WH, Gwirtsman HE, George DT. The effect of bingeing and vomiting on hormonal secretion. Biol Psychiatry. 1989;25(6):768–780. doi:10.1016/0006-3223(89
30. Kisely S, Baghaie H, Lalloo R, Johnson NW. Association between poor oral health and eating disorders: systematic review and meta-analysis. Br J Psychiatry. 2015;207(4):299–305. doi:10.1192/bjp.bp.114.156323
31. Sato Y, Fukudo S. Gastrointestinal symptoms and disorders in patients with eating disorders. Clin J Gastroenterol. 2015;8(5):255–263. doi:10.1007/s12328-015-0611-x
32. Copeland PM. Renal failure associated with laxative abuse. Psychother Psychosom. 1994;62(3–4):200–202. doi:10.1159/000288923
33. Roerig JL, Steffen KJ, Mitchell JE, Zunker C. Laxative abuse: epidemiology, diagnosis and management. Drugs. 2010;70(12):1487–1504. doi:10.2165/11898640-000000000-00000
34. Vanin JR, Saylor KE. Laxative abuse: a hazardous habit for weight control. J Am Coll Health. 1989;37(5):227–230. doi:10.1080/07448481.1989.9939064
35. Eisenberg D, Nicklett EJ, Roeder K, Kirz NE. Eating disorder symptoms among college students: prevalence, persistence, correlates, and treatment-seeking. J Am Coll Health. 2011;59(8):700–707. doi:10.1080/07448481.2010.546461
36. Wharton CM, Adams T, Hampl JS. Weight loss practices and body weight perceptions among US college students. J Am Coll Health. 2008;56(5):579–584. doi:10.3200/JACH.56.5.579-584
37. Lowry R, Galuska DA, Fulton JE, Wechsler H, Kann L, Collins JL. Physical activity, food choice, and weight management goals and practices among US college students. Am J Prev Med. 2000;18(1):18–27. doi:10.1016/s0749-3797(99)00107-5
38. White S, Reynolds-Malear JB, Cordero E. Disordered eating and the use of unhealthy weight control methods in college students: 1995, 2002, and 2008. Eat Disord. 2011;19(4):323–334. doi:10.1080/10640266.2011.584805
39. Himmelstein MS, Puhl RM, Quinn DM. Intersectionality: an Understudied Framework for Addressing Weight Stigma. Am J Prev Med. 2017;53(4):421–431. doi:10.1016/j.amepre.2017.04.003
40. Diep J. Size Matters: The Impact of Weight-Based Discrimination on College Students’ Physical Health, Mental Health, and Academic Achievement. California State University, Long Beach; 2017.
41. Houle-Johnson SA, Kakinami L. Do sex differences in reported weight loss intentions and behaviours persist across demographic characteristics and weight status in youth? A systematic review. BMC Public Health. 2018;18(1):1343. doi:10.1186/s12889-018-6179-x
42. Neumark-Sztainer D, Story M, Falkner NH, Beuhring T, Resnick MD. Sociodemographic and personal characteristics of adolescents engaged in weight loss and weight/muscle gain behaviors: who is doing what? Prev Med. 1999;28(1):40–50. doi:10.1006/pmed.1998.0373
43. Crago M, Shisslak CM. Ethnic differences in dieting, binge eating, and purging behaviors among American females: a review. Eat Disord. 2003;11(4):289–304. doi:10.1080/10640260390242515
44. Rodgers RF, Peterson KE, Hunt AT, et al. Racial/ethnic and weight status disparities in dieting and disordered weight control behaviors among early adolescents. Eat Behav. 2017;26:104–107. doi:10.1016/j.eatbeh.2017.02.005
45. Rodgers RF, Watts AW, Austin SB, Haines J, Neumark-Sztainer D. Disordered eating in ethnic minority adolescents with overweight. Int J Eat Disord. 2017;50(6):665–671. doi:10.1002/eat.22652
46. Kennedy AK, Schneiderman JU, Ramseyer Winter V. Association of body weight perception and unhealthy weight control behaviors in adolescence. Child Youth Serv Rev. 2019;96:250–254. doi:10.1016/j.childyouth.2018.11.053
47. Lynch WC, Heil DP, Wagner E, Havens MD. Ethnic differences in BMI, weight concerns, and eating behaviors: comparison of native American, white, and Hispanic adolescents. Body Image. 2007;4(2):179–190. doi:10.1016/j.bodyim.2007.01.001
48. Chao YM, Pisetsky EM, Dierker LC, et al. Ethnic differences in weight control practices among U.S. adolescents from 1995 to 2005. Int J Eat Disord. 2008;41(2):124–133. doi:10.1002/eat.20479
49. Rodgers RF, Berry R, Franko DL. Eating disorders in ethnic minorities: an update. Curr Psychiatry Rep. 2018;20:10. doi:10.1007/s11920-018-0938-3
50. Liu CH, Stevens C, Wong SHM, Yasui M, Chen JA. The prevalence and predictors of mental health diagnoses and suicide among U.S. college students: implications for addressing disparities in service use. Depress Anxiety. 2019;36(1):8–17. doi:10.1002/da.22830
51. ElTohamy A, Hyun S, Macaranas AR, Chen JA, Stevens C, Liu CH. Testing positive, losing a loved one, and financial hardship: real-world impacts of COVID-19 on US college student distress. J Affect Disord. 2022;314:357–364. doi:10.1016/j.jad.2022.07.022
52. Walsh-Buhi ER, Helmy HL. Trends in long-acting reversible contraceptive (LARC) use, LARC use predictors, and dual-method use among a national sample of college women. J Am Coll Health. 2018;66(4):225–236. doi:10.1080/07448481.2017.1399397
53. Burke NL, Hazzard VM, Karvay YG, Schaefer LM, Lipson SK, Rodgers RF. Eating disorder prevalence among multiracial US undergraduate and graduate students: is multiracial risk different than the sum of each identity? Eat Behav. 2021;41:101501. doi:10.1016/j.eatbeh.2021.101501
54. Peng CYJ, Lee KL, Ingersoll GM. An introduction to logistic regression analysis and reporting. J Educ Res. 2002;96(1):3–14. doi:10.1080/00220670209598786
55. Sonneville KR, Lipson SK. Disparities in eating disorder diagnosis and treatment according to weight status, race/ ethnicity, socioeconomic background, and sex among college students. Int J Eat Disord. 2018;51(6):518–526. doi:10.1002/eat.22846
56. Lipson S, Sonneville K. Eating disorder symptoms among undergraduate and graduate students at 12 U.S. colleges and universities. Eat Behav. 2017;24:81–88. doi:10.1016/j.eatbeh.2016.12.003
57. Harrop EN, Mensinger JL, Moore M, Lindhorst T. Restrictive eating disorders in higher weight persons: a systematic review of atypical anorexia nervosa prevalence and consecutive admission literature. Int J Eat Disord. 2021;54(8):1328–1357. doi:10.1002/eat.23519
58. Strother E, Lemberg R, Stanford SC, Turberville D. Eating Disorders in Men: underdiagnosed, Undertreated, and Misunderstood. Eat Disord. 2012;20(5):346–355. doi:10.1080/10640266.2012.715512
59. Ricciardelli LA, McCabe MP, Williams RJ, Thompson JK. The role of ethnicity and culture in body image and disordered eating among males. Clin Psychol Rev. 2007;27(5):582–606. doi:10.1016/j.cpr.2007.01.016
60. Epperson AE, Song AV, Wallander JL, et al. Associations among body size, body image perceptions, and weight loss attempts among African American, latino, and white youth: a test of a mediational model. J Pediatr Psychol. 2014;39(4):394–404. doi:10.1093/jpepsy/jst096
61. Gentile K, Raghavan C, Rajah V, Gates K. It doesn’t happen here: eating disorders in an ethnically diverse sample of economically disadvantaged, urban college students. Eat Disord. 2007;15(5):405–425. doi:10.1080/10640260701667904
62. Garcia DO, Valdez LA, Hooker SP. Hispanic male’s perspectives of health behaviors related to weight management. Am J Mens Health. 2017;11(5):1547–1559. doi:10.1177/1557988315619470
63. Brave Heart MYH, DeBruyn LM. The American Indian holocaust: healing historical unresolved grief. Am Indian Alsk Native Ment Health Res. 1998;8(2):60–82. doi:10.5820/aian.0802.1998.60
64. Zohar AH, Giladi L, Givati T. Holocaust exposure and disordered eating: a study of multi-generational transmission. Eur Eat Disord Rev. 2007;15(1):50–57. doi:10.1002/erv.730
65. Striegel-Moore RH, Rosselli F, Holtzman N, Dierker L, Becker AE, Swaney G. Behavioral symptoms of eating disorders in Native Americans: results from the ADD health survey wave III. Int J Eat Disord. 2011;44(6):561–566. doi:10.1002/eat.20894
66. Strings S. Fearing the Black Body: The Racial Origins of Fat Phobia. NYU Press; 2019.
67. Strings S. Obese black women as “social dead weight”: reinventing the “diseased black woman. Signs. 2015;41:107. doi:10.1086/681773
68. Hunger JM, Tomiyama AJ. Weight labeling and disordered eating among adolescent girls: longitudinal evidence from the national heart, lung, and blood institute growth and health study. J Adolesc Health. 2018;63(3):360–362. doi:10.1016/j.jadohealth.2017.12.016
69. Vartanian LR, Porter AM. Weight stigma and eating behavior: a review of the literature. Appetite. 2016;102:3–14. doi:10.1016/j.appet.2016.01.034
70. Wilkes K. Eating, Looking, and Living Clean: Techniques of White Femininity in Contemporary Neoliberal Food Culture. Gender, Work & Organization; 2021; doi:10.1111/gwao.12620
71. Wildes JE, Emery RE, Simons AD. The roles of ethnicity and culture in the development of eating disturbance and body dissatisfaction: a meta-analytic review. Clin Psychol Rev. 2001;21(4):521–551. doi:10.1016/S0272-7358(99)00071-9
72. Kim BSK, Atkinson DR, Umemoto D. Asian cultural values and the counseling process: current knowledge and directions for future research. Couns Psychol. 2001;29:570–603. doi:10.1177/0011000001294006
73. Striegel-Moore RH, Smolak L. The influence of ethnicity on eating disorders in women. In: Handbook of Gender, Culture, and Health. Lawrence Erlbaum Associates Publishers; 2000:227–253.
74. Franko DL, Becker AE, Thomas JJ, Herzog DB. Cross-ethnic differences in eating disorder symptoms and related distress. Int J Eat Disord. 2007;40(2):156–164. doi:10.1002/eat.20341
75. Regan PC, Cachelin FM. Binge eating and purging in a multi-ethnic community sample. Int J Eat Disord. 2006;39(6):523–526. doi:10.1002/eat.20268
76. Cheng ZH, Perko VL, Fuller-Marashi L, Gau JM, Stice E. Ethnic differences in eating disorder prevalence, risk factors, and predictive effects of risk factors among young women. Eat Behav. 2019;32:23–30. doi:10.1016/j.eatbeh.2018.11.004
77. Keeler LA, Clifford DE, Buck A, Kowalski P, Morris MN. Examination of a peer-led, non-diet nutrition and exercise adherence pilot program on a college campus. Californian J Health Promot. 2013;11(1):84–96. doi:10.32398/cjhp.v11i1.1521
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.