Back to Journals » Patient Preference and Adherence » Volume 17
Quantitative Adherence Level Evaluation Among Long-Term Antiretroviral Therapy Patients in Latvia
Authors Gavrilova A ![]() , Zolovs M
, Zolovs M ![]() , Urtāne I, Šmits D
, Urtāne I, Šmits D ![]()
Received 30 August 2023
Accepted for publication 21 November 2023
Published 5 December 2023 Volume 2023:17 Pages 3147—3154
DOI https://doi.org/10.2147/PPA.S437611
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Anna Gavrilova,1 Maksims Zolovs,2,3 Inga Urtāne,1 Dins Šmits4
1Department of Pharmaceutical Chemistry, Faculty of Pharmacy, Rīga Stradiņš University, Riga, LV-1007, Latvia; 2Statistical Unit, Faculty of Medicine, Rīga Stradiņš University, Riga, LV-1048, Latvia; 3Institute of Life Sciences and Technology, Daugavpils University, Daugavpils, LV-5401, Latvia; 4Department of Public Health and Epidemiology, Faculty of Public Health and Social Welfare, Rīga Stradiņš University, Riga, LV-1007, Latvia
Correspondence: Anna Gavrilova, Pharmaceutical Education and Research Centre, Faculty of Pharmacy, Department of Pharmaceutical Chemistry, 21 Konsula street, Riga, LV-1007, Latvia, Email [email protected]
Introduction: The global prevalence of human immunodeficiency virus (HIV) remains substantial, particularly in regions with limited resources, despite the progress in scientific knowledge and the accessibility of antiretroviral therapy (ART). ART is the cornerstone of HIV treatment. Ensuring proper adherence to medication therapy is essential for effective HIV infection control. Meanwhile, Latvia reported one of the highest rates of HIV infections among EU countries.
Purpose: This study aimed to assess adherence levels to ART among long-term users by utilizing the National Health Service prescription electronic database records. It is essential to determine whether non-adherence is a problem at the state level.
Patients and Methods: This retrospective study was conducted utilizing the Latvian National Health Service’s reimbursed prescription database, covering the period from January 2017 to December 2018. The analysis included ART prescriptions. Medication adherence was assessed using a Proportion of Days Covered (PDC) calculation. The adherence rates were categorized into three groups: (1) < 80% (non-adherence), (2) 80% to 90% (suboptimal adherence), and (3) > 90% (optimal adherence) groups.
Results: A total of 25,892 ARV medicines prescription records for 1471 patients were analysed. The adherence level of long-term ART was 38.3%. Of all patients, only 37 (2.5%) had achieved an optimal and 25 (1.7%) suboptimal adherence level. Meanwhile, the remaining patients (95.8%) were identified as non-adherent to therapy. It has been determined that 96.1% (n=1414) of patients experienced a time gap of more than 90 days between their prescriptions at least once. On average, each patient had 3.5 of these gaps, with a maximum of 7 times.
Conclusion: Medication adherence level to ART is low in Latvia. Less than 3% of patients achieved optimal adherence levels with a PDC higher than 90%. These results are concerning. Further studies and interventions must be conducted to enhance adherence levels.
Keywords: HIV, AIDS, ART, PDC, National Health Service
Introduction
Human Immunodeficiency Virus (HIV) is undeniably a significant global health problem. According to World Health Organisation data, an estimated 39.0 million [33.1–45.7 million] people were living with HIV at the end of 2022.1 Despite the advancements in medical science and the availability of antiretroviral therapy (ART), HIV continues to impact millions worldwide, particularly in resource-limited regions. Meanwhile, Latvia reported one of the highest rates of HIV infections among EU countries.1–3
HIV is a virus that attacks the body’s immune system, specifically CD4 cells, which play a vital role in helping the body fight off infections.4 If left untreated, HIV can lead to acquired immunodeficiency syndrome (AIDS), a condition where the immune system is severely weakened, leaving individuals susceptible to life-threatening illnesses.1,5–8 There is no cure for HIV infection. However, with access to effective HIV prevention, diagnosis, treatment and care, including for opportunistic infections, HIV infection has become a manageable chronic health condition, enabling people with HIV to live long and healthy lives.9–12
ART is the cornerstone of HIV treatment. ART consists of a combination of medications that work to suppress the replication of the virus in the body, slowing down the progression of HIV and reducing the viral load to undetectable levels.7,13 Achieving and maintaining an undetectable viral load is a key goal of HIV treatment, as it not only improves the individual’s health but also prevents the transmission of the virus to others.5,14,15
Adherence to ART is consistent and timely prescription medication intake as directed by healthcare professionals.16 It is paramount in managing HIV effectively for several reasons, such as viral suppression, delaying disease progression, reducing drug resistance, improved quality of life, and preventing transmission.17,18 However, adherence to ART can be challenging for some individuals due to various factors, including medication complexity, side effects, stigma, mental health concerns, and socioeconomic barriers.19–23
The number of HIV-infected patients in Latvia, mainly males, is increasing annually.3 Based on 2019 statistical data, HIV cases were detected more often in persons aged 30 to 39 years (33.5%), and most cases of infection occurred through heterosexual transmission.24 The Latvian healthcare system provides medical care and support for people living with HIV, including counselling, education, and regular monitoring of their health. However, certain restrictions significantly affected the availability of medical care in previous years. Decentralization was implemented only in 2019, allowing patients to receive medication prescriptions from their nearest infectologist practice instead of in the capital city (Riga, Latvia). Also, ART medicine government reimbursement depended on the patient’s laboratory CD4 test results. As of the second half of 2018, initiation of ART with reimbursement support requires solely an approved HIV diagnosis.25,26
Ensuring proper adherence to medication therapy is essential for effective HIV infection control.16,27 However, assessing the degree of adherence frequently presents difficulties in real-life scenarios.21 Several methods are used to determine medication adherence, including patient questionnaires, pill counts, assessment of patient clinical outcomes, and electronic medication monitoring systems. However, each method has its advantages and disadvantages.28–30
Quantitative methods to determine adherence levels are data-driven approaches that use numerical values to assess and measure a patient’s adherence to a prescribed medication regimen.29,31 Estimating medication adherence through data calculations from the electronic prescriptions database, using metrics like Medication Possession Ratio (MPR) and Proportion of Days Covered (PDC), is extremely important.32,33 The MPR is calculated by dividing the days’ supply of medication dispensed during the treatment period by the total number of days in that period. This method takes into consideration any medication obtained through early refills, which could potentially result in adherence values exceeding 100%. The PDC method is a comparable approach, but it imposes limitations on medication supplies overlapping, resulting in a more precise calculation of adherence.29,34–36 Based on clinical evidence, it is recommended to maintain a Proportion of Days Covered (PDC) threshold of 80% to be adherent to therapy. Previous research indicates that achieving viral suppression and preventing resistance mutations in ART requires a PDC threshold of at least 95%. Through the years, adherence to treatment regimens has improved, leading to the observation of viral suppression even with reduced levels of adherence (above 90%).15,37–40
This study aimed to assess adherence levels to ART among long-term users by utilizing the National Health Service prescription electronic database records. Since Latvia has one of the highest rates of HIV infections in Europe, it is essential to determine whether non-adherence is a problem at the state level.2
Materials and Methods
Study Design and Data Collection
This retrospective study was conducted utilizing the Latvian National Health Service’s (NHS) reimbursed prescription database, covering the period from January 2017 to December 2018. The analysis included prescriptions based on diagnoses coded according to the International Statistical Classification of Diseases and Related Health Problems for HIV infection (B20.0-B20.9, B21.0-B21.3, B21.7-B21.9, B22.0-B22.2, B22.7, B23.0-B23.2, B23.8 and B24).26,41 The cohort of long-term ART users was identified based on their prescription history, specifically individuals who received one or more ART prescriptions in 2016 and continued in 2019, respectively. Patients who initiated therapy after 2016 or who were discontinued before 2019 were not included in this study analysis. The cancellation of CD4 laboratory tests for initiating ART with reimbursement government support in the second half of 2018 did not impact the data processing, as this study’s analysis exclusively included prescriptions for long-term ART users. Furthermore, the study incorporated subjects aged 18 years or older to ensure relevance to adult populations. There was one exclusion criterion, which was patients with limited prescription data. As a result, adherence levels could not be estimated.
All reimbursed outpatient care prescription data were recorded in the NHS database. Also, reimbursed paper prescriptions data were immediately input into the NHS prescription database after medicine dispensing at pharmacies. It means that all dispensed medicine prescriptions (paper and electronic) reimbursed for patients by the government were analysed. Regrettably, due to limitations in the system’s data availability, the study could not collect data on prescriptions that patients were prescribed but did not purchase.
To preserve data privacy and security, anonymous and encrypted records were procured from the NHS. Reverse identification was impossible. Each prescription record covered patients’ data as age and gender, information related to the dispensed drug marketing authorisation number, brand name or international non-proprietary name and the diagnosis for which the medication was prescribed.
Measurements of Adherence
Medication adherence was assessed using a modified Proportion of Days Covered (PDC) calculation, which relied on medication dispensing data. While several methods are available in the literature to calculate medication adherence using pharmacy refill data, the PDC measure was selected based on its endorsement by Pharmacy Quality Alliance and various previous studies.21,32,34,36,37,42
The PDC was computed by dividing the total number of days covered by the medicine regimen by the number of days between the patient’s first and last dispensing dates, excluding the doses of the last prescription. In cases where a patient had overlapping fills for the same drug (due to early refilling), the dispensed medicine amount was adjusted to account for the remaining number of doses plus the newly dispensed amount.32,34,37 The PDC was individually calculated for each medication used by the patient. Patient total adherence levels were then established by identifying the lowest adherence rate among all the medications they were prescribed. The values for PDC range from 0 to 100%, with higher values indicating higher adherence to the ART medication regimen. This methodology ensured medication adherence assessment, accounting for treatment continuity while appropriately handling overlapping prescription fills to avoid potential overestimating adherence. In this study, the adherence rates were categorized into three groups: (1) < 80% (non-adherence), (2) 80% to 90% (suboptimal adherence), and (3) > 90% (optimal adherence) groups.21,35 Based on the Latvia reimbursement system, prescriptions can only be prescribed for a maximum 3-month course. Therefore, a maximum time gap of 90 days between prescriptions was defined.
We did not seek approval of an Ethics Committee since our research is based on a retrospective database analysis where all received data were anonymized by NHS and cannot be traced to individual persons. According to local data protection regulations, no approval from the ethics committee was required for this study.43,44
Statistical Analysis
The assumption of data distribution was assessed by the Shapiro–Wilk test and inspection of the normal Q-Q plots. The assumption of homogeneity of variance was tested by the Levene’s test. The Mann–Whitney U-test was used to test the difference in adherence between gender and medication presentation (monocomponent or FDC). The Welch’s ANOVA was used to test the difference in age between adherence groups (< 80%, 80–90% and > 90%). The chi-square test of homogeneity was used to test the difference in proportion of gender between adherence groups. To test correlation between age and adherence, the Spearman correlation test was used. All statistical analyses were performed by using the Jamovi statistical software (https://www.jamovi.org). An alpha level of 0.05 was used for all the statistical analyses.
Results
A total of 25,892 ARV medicines prescription records for 1471 patients (2 patients were excluded), of whom 64.7% (n=952) were males, were included in this study analysis. Long-term ARV therapy users’ mean age was 42.3 (SD=9.9) years. Over a period of two years, patients dispensed ART medicines on average 8.9 (SD=2.9) times, with a maximum of 23 times. It has been determined that 96.1% (n=1414) of patients experienced a time gap of more than 90 days between their prescriptions at least once. On average, each patient had 3.5 of these gaps, with a maximum of 7 times. More detailed information about patients’ characteristics and used ARV therapy is available in Table 1.
 |
Table 1 Patients’ Demographics and Prescribed Medications |
The total adherence level of long-term ART on average was 38.3% (SD=0.15%). There were no statistically significant differences of adherence levels between gender (p=0.590) or medication formulations (p=0.140). As well, there was no difference in age between adherence groups (p>0.05), as well as no correlation between age and adherence (p>0.05). The adherence level for each medication is shown in Figure 1. Of all patients, only 37 (2.5%) had achieved an optimal adherence level, with a PDC of over 90%, and 25 (1.7%) patients in the 80% to 90% range. Meanwhile, the remaining patients (95.8%) had PDC lower than 80%, identifying them as non-adherent to therapy.
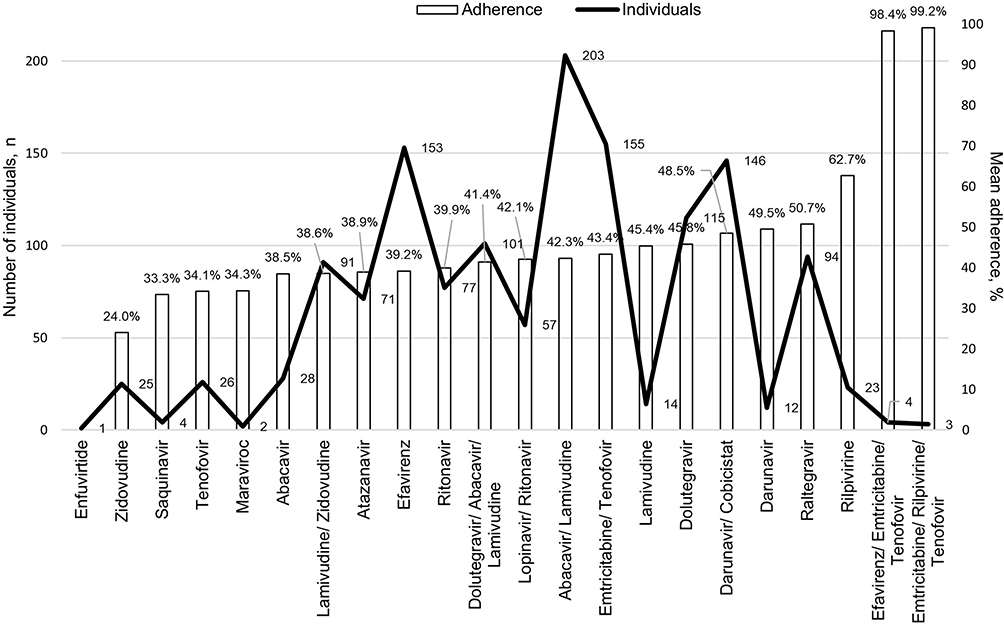 |
Figure 1 Adherence level of each medication and number of prescribed prescriptions. |
Discussion
In this retrospective Latvian study, including more than 1000 patients who received ART from January 2017 through December 2018, we found that the average adherence level (based on PDC) to therapy was 38.3%. The main findings of this study indicate a concerning estimate of low adherence to ART among patients with HIV. Our examination of the Latvian NHS’s prescription database showed that a significant number of individuals using long-term ART did not adhere to their medication schedule as directed. This result is particularly distressing as poor adherence to ART can lead to compromised viral suppression, increased risk of drug resistance, and adverse health outcomes. The data highlights the pressing need for targeted interventions and enhanced support systems to address adherence challenges among this patient population to improve treatment efficacy and overall well-being.
Most research examining adherence to ART defines adherence based on either medication possession ratio (MPR) or proportion of days covered (PDC). This study’s result aligned with the common challenge faced in HIV management, indicating that suboptimal adherence remains a persistent issue. Of concern, the adherence level in Latvia appears not only low but also comparatively lower than findings from other research data, mainly studying American and African people living with HIV.27,45,46 Only 2.5% of patients in Latvia achieved an optimal adherence level (PDC≥90%) for ART. For instance, in a study conducted by Grace A. McComsey et al, 38.7% of patients achieved this level, with an overall adherence rate of 74.1%.21 In J. Kim et al research, not visiting tertiary hospitals was a risk factor for lower adherence.27 However, a significant presence of medication dispensing gaps exceeding 90 days among long-term ART users was noted in our study, negatively influencing the overall adherence rate.
Our study design did not allow to conclude whether patients are taking their medication as prescribed, even if they are refilling their prescriptions, as they may purchase the medication but not actually use it. No significant differences were found between patients’ demographics and taking medicine formulation. This suggests the presence of other factors that could potentially challenge achieving high adherence levels. One of contributing factors could be limited access to healthcare services. Historically, ART medication prescriptions were prescribed only by infectologists or pediatricians located in Latvia’s capital city, Riga. However, this changed only in 2019, when the process was decentralized.26 This marked a significant advancement as it eased the burden on patients who previously faced challenges regarding time and financial constraints, especially related to transportation costs. Furthermore, the extended waiting times for doctors’ appointments could surpass the duration of the previously prescribed medication regimen. This situation leads to non-adherence, as patients may encounter interruptions in their treatment due to the misalignment between appointment availability and medication refill needs. An additional notable point is the absence of data on disruption in the supply of ART medications, as these issues were not publicly reported during the 2018–2019 period. As disruptions in medication supply can significantly impact adherence rates and subsequently affect the effectiveness of treatment outcomes.
The study is subject to certain limitations, (1) notably the utilization only of 2017–2018 period data that may not reflect the present circumstances, potentially affecting the relevance of findings to healthcare practices. Analysis of the latest data is essential for retrospective evaluation of the impact of implemented changes in HIV patient management after 2018. In general, (2) prescribed but not dispensed medication data was not recorded in the system which was not analyzed, impacting study results. It would be helpful to have more information about the availability of medications at pharmacies for studies conducting quantitative medication adherence evaluations. Additionally, (3) the study focused only on a quantitative adherence measure using medicine prescription refills data without exploring into the broader context of patient behaviour and factors influencing non-adherence. Qualitative data elements, including patients’ socio-demographic details, duration of ART, symptom severity, comorbidities, and health literacy, were not examined in analysing a non-adherence problem. Although (4) neither quantitative metric can verify the actual ingestion or adherence to the prescribed medication, they can offer insights into whether the medication was accessible to the individual for potential consumption.
This study represents a first-time utilization of the Latvian National Health Service database of prescription data to assess medication adherence. This novel approach has the potential to significantly advance the monitoring of patient medicine utilization, offering valuable insight for future research and healthcare management improvement. Furthermore, this technique can assess the impact of previously enacted changes by analysing this data longitudinally. Potentially in the future, collaboration with the NHS and strict adherence to data privacy regulations, proactive communication with non-adherent patients based on medication prescription data could lead to facilitating an in-depth exploration of the underlying factors contributing to non-adherence and developing strategies to improve adherence rates.
Conclusion
The National Health Service prescription database analysis demonstrated low adherence to ART. Less than 3% of patients achieved optimal adherence levels with a PDC higher than 90%. These results are concerning not only for patients with HIV but also for society as a whole because effective therapy targets were not achieved, as patients did not use medicine as prescribed, leading to risks of ART therapy resistance, health complications, higher transmission rates, and increased healthcare costs. Furthermore, a large number of gaps between dispensing times were observed, negatively impacting the total adherence level. This situation accentuates the immediate requirement for identifying non-adherence factors and precisely targeted interventions aimed at improving it, thereby ensuring treatment efficacy.
Acknowledgments
The authors express their gratitude to The National Health Service of Latvia for its support.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. HIV and AIDS. Available from: https://www.who.int/news-room/fact-sheets/detail/hiv-aids.
2. World Health Organization. HIV/AIDS Surveillance in Europe 2022 – 2021 Data. Vol. 03. World Health Organization; 2022. doi:10.2900/818446
3. Latvian Centre for Disease Prevention and Control. HIV/AIDS statistics. Available from: https://www.spkc.gov.lv/lv/hivaids-statistika.
4. Peña Donati A, Laufer M. Acquired Immune Deficiency Syndrome. In: Pediatric Respiratory Diseases: A Comprehensive Textbook. StatPearls Publishing; 2020:517–528. doi:10.1007/978-3-030-26961-6_51
5. Menéndez-Arias L, Delgado R. Update and latest advances in antiretroviral therapy. Trends Pharmacol Sci. 2022;43(1):16–29. doi:10.1016/j.tips.2021.10.004
6. Pasternak AO, Berkhout B. HIV persistence: silence or resistance? Curr Opin Virol. 2023;59. doi:10.1016/j.coviro.2023.101301
7. Shahzad M, Chen H, Akhtar T, Rafi A, Zafar MS, Zheng YT. Human immunodeficiency virus: the potential of medicinal plants as antiretroviral therapy. J Med Virol. 2022;94(6):2669–2674. doi:10.1002/jmv.27648
8. Annor FB, Chiang LF, Oluoch PR, et al. Changes in prevalence of violence and risk factors for violence and HIV among children and young people in Kenya: a comparison of the 2010 and 2019 Kenya violence against children and youth surveys. Lancet Glob Heal. 2022;10(1):e124–e133. doi:10.1016/S2214-109X(21)00457-5
9. Poorolajal J, Hooshmand E, Mahjub H, Esmailnasab N, Jenabi E. Survival rate of AIDS disease and mortality in HIV-infected patients: a meta-analysis. Public Health. 2016;139:3–12. doi:10.1016/j.puhe.2016.05.004
10. Gueler A, Moser A, Calmy A, et al. Life expectancy in HIV-positive persons in Switzerland: matched comparison with general population. AIDS. 2017;31(3):427–436. doi:10.1097/QAD.0000000000001335
11. Teeraananchai S, Kerr SJ, Amin J, Ruxrungtham K, Law MG. Life expectancy of HIV-positive people after starting combination antiretroviral therapy: a meta-analysis. HIV Med. 2017;18(4):256–266. doi:10.1111/hiv.12421
12. Marcus JL, Chao CR, Leyden WA, et al. Narrowing the gap in life expectancy between HIV-Infected and HIV-uninfected individuals with access to care. J Acquir Immune Defic Syndr. 2016;73(1):39–46. doi:10.1097/QAI.0000000000001014
13. Esté JA, Cihlar T. Current status and challenges of antiretroviral research and therapy. Antiviral Res. 2010;85(1):25–33. doi:10.1016/j.antiviral.2009.10.007
14. Rodger AJ, Cambiano V, Phillips AN, et al. Risk of HIV transmission through condomless sex in serodifferent gay couples with the HIV-positive partner taking suppressive antiretroviral therapy (PARTNER): final results of a multicentre, prospective, observational study. Lancet. 2019;393(10189):2428–2438. doi:10.1016/S0140-6736(19)30418-0
15. Altice F, Evuarherhe O, Shina S, Carter G, Beaubrun AC. Adherence to HIV treatment regimens: systematic literature review and meta-analysis. Patient Prefer Adher. 2019;13:475–490. doi:10.2147/PPA.S192735
16. Neupane S, Dhungana GP, Ghimire HC. Adherence to antiretroviral treatment and associated factors among people living with HIV and AIDS in CHITWAN, Nepal. BMC Public Health. 2019;19(1):1–9. doi:10.1186/s12889-019-7051-3
17. Goldschmidt RH, Chu C, Dong BJ. Initial management of patients with HIV infection. Am Fam Physician. 2016;94(9):708–716.
18. Bekker LG, Alleyne G, Baral S, et al. Advancing global health and strengthening the HIV response in the era of the sustainable development goals: the international AIDS society—lancet commission. Lancet. 2018;392(10144):312–358. doi:10.1016/S0140-6736(18)31070-5
19. Astuti N, Maggiolo F. Single-tablet regimens in HIV therapy. Infect Dis Ther. 2014;3(1):1–17. doi:10.1007/s40121-014-0024-z
20. World Health Organization. Adherence to long-term therapies. Evidence for Action; 2003. Available from: http://www.who.int/chp/knowledge/publications/adherence_introduction.pdf%0Ahttp://www.who.int/chp/knowledge/publications/adherence_introduction.pdf?ua=1%0Ahttp://www.who.int/chp/knowledge/publications/adherence_introduction.pdf.
21. McComsey GA, Lingohr-Smith M, Rogers R, Lin J, Donga P. Real-world adherence to antiretroviral therapy among HIV-1 patients across the United States. Adv Ther. 2021;38(9):4961–4974. doi:10.1007/s12325-021-01883-8
22. Kalungwe M, Mbalinda SN, Karonga T, Simwanza NR, Mumba Mtambo CM, Nyashanu M. Exploring barriers to antiretroviral therapy adherence among pregnant women: a scoping literature review. Int J Gynecol Obstet. 2022;159(2):343–350. doi:10.1002/ijgo.14130
23. Daltro ACB, Almeida CS, Unfried AGC, de Aquino TR, Travassos AGÁ. Virological failure and adherence to antiretroviral therapy in adolescents and young adults living with human immunodeficiency virus. Trop Med Int Heal. 2023;28(3):162–174. doi:10.1111/tmi.13854
24. Ministry of Health of Latvia. Adopt new rules to prevent and limit the spread of HIV. Available from: https://www.vm.gov.lv/lv/jaunums/pienem-jaunus-noteikumus-hiv-profilaksei-un-izplatibas-ierobezosanai.
25. Ministry of Health of Latvia. PROTOCOL No. 35 of the meeting of the coordination commission for limiting the spread of HIV infection, tuberculosis and sexually transmitted infections. Available from: https://www.vm.gov.lv/lv/media/2377/download?attachment.
26. The National Health Service of Latvia. Reimbursement Medicine Lists. Available from: https://www.vmnvd.gov.lv/lv/kompensejamo-zalu-saraksti.
27. Kim J, Lee E, Park BJ, Bang JH, Lee JY. Adherence to antiretroviral therapy and factors affecting low medication adherence among incident HIV-infected individuals during 2009–2016: a nationwide study. Sci Rep. 2018;8(1):3133. doi:10.1038/s41598-018-21081-x
28. Lam WY, Fresco P. Medication adherence measures: an overview. Biomed Res Int. 2015;2015:1–12. doi:10.1155/2015/217047
29. Anghel LA, Farcas AM, Oprean RN. An overview of the common methods used to measure treatment adherence. Med Pharm Reports. 2019;92(2):117–122. doi:10.15386/mpr-1201
30. Nassar RI, Basheti IA, Saini B. Exploring validated self-reported instruments to assess adherence to medications used: a review comparing existing instruments. Patient Prefer Adher. 2022;16:503–513. doi:10.2147/PPA.S352161
31. Tibble H, Sheikh A, Tsanas A. Estimating medication adherence from electronic health records: comparing methods for mining and processing asthma treatment prescriptions. BMC Med Res Methodol. 2023;23(1):1–11. doi:10.1186/s12874-023-01935-3
32. Prieto-Merino D, Mulick A, Armstrong C, et al. Estimating proportion of days covered (PDC) using real-world online medicine suppliers’ datasets. J Pharm Policy Pract. 2021;14(1):1–14. doi:10.1186/s40545-021-00385-w
33. Asamoah-Boaheng M, Bonsu KO, Farrell J, Oyet A, Midodzi WK. Measuring medication adherence in a population-based asthma administrative pharmacy database: a systematic review and meta-analysis. Clin Epidemiol. 2021;13:981–1010. doi:10.2147/CLEP.S333534
34. Canfield SL, Zuckerman A, Anguiano RH, et al. Navigating the wild west of medication adherence reporting in specialty pharmacy. J Manag Care Spec Pharm. 2019;25(10):1073–1077. doi:10.18553/jmcp.2019.25.10.1073
35. Rathbun RC, Lewis MM, Yuet WC, Woo S, Miller JL, Skrepnek GH. The medication possession ratio as a predictor of longitudinal HIV-1 viral suppression. Ann Pharmacother. 2023;57(11):1264–1272. doi:10.1177/10600280231156624
36. Loucks J, Zuckerman AD, Berni A, Saulles A, Thomas G, Alonzo A. Proportion of days covered as a measure of medication adherence. Am J Heal Pharm. 2022;79(6):492–496. doi:10.1093/ajhp/zxab392
37. Pharmacy Quality Alliance. PQA measures: overview types of PQA measure; 2022.
38. Murphy P, Cocohoba J, Tang A, Pietrandoni G, Hou J, Guglielmo BJ. Impact of HIV-specialized pharmacies on adherence and persistence with antiretroviral therapy. AIDS Patient Care STDS. 2012;26(9):526–531. doi:10.1089/apc.2012.0189
39. Bezabhe WM, Chalmers L, Bereznicki LR, Peterson GM. Adherence to antiretroviral therapy and virologic failure. Medicine. 2016;95(15):e3361. doi:10.1097/MD.0000000000003361
40. Byrd KK, Hou JG, Hazen R, et al. Antiretroviral adherence level necessary for HIV viral suppression using real-world data. J Acquir Immune Defic Syndr. 2019;82(3):245–251. doi:10.1097/QAI.0000000000002142
41. Harrison JE, Weber S, Jakob R, Chute CG. ICD-11: an international classification of diseases for the twenty-first century. BMC Med Inform Decis Mak. 2021;21(1):21. doi:10.1186/s12911-021-01534-6
42. McMahon JH, Jordan MR, Kelley K, et al. Pharmacy adherence measures to assess adherence to antiretroviral therapy: review of the literature and implications for treatment monitoring. Clin Infect Dis. 2011;52(4):493–506. doi:10.1093/cid/ciq167
43. Latvian Association of Sociologists. Latvian association of sociologists professional code for conducting social and market research; 2008. Available from: http://sociologija.lv/etika-2/lsa-kodekss/.
44. Rutkovska I, Seilis A, Neikena Z, Poplavska E. Impact of risk minimisation measures on valproate use among women of reproductive age in Latvia between 2013 and 2020: a 7-year nationwide prescription database study. Drugs Real World Outcome. 2023;10(1):1–11. doi:10.1007/s40801-023-00394-y
45. Nachega JB, Hislop M, Dowdy DW, et al. Adherence to highly active antiretroviral therapy assessed by pharmacy claims predicts survival in HIV-infected South African adults. J Acquir Immune Defic Syndr. 2006;43(1):78–84. doi:10.1097/01.qai.0000225015.43266.46
46. Mills EJ, Nachega JB, Buchan I, et al. Adherence to antiretroviral therapy in sub-Saharan Africa and North America: a meta-analysis. JAMA. 2006;296(6):679–690. doi:10.1001/jama.296.6.679
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.