Back to Journals » Patient Preference and Adherence » Volume 19
Quantifying the Tolerability of Antipsychotic Treatment-Related Side Effects in Schizophrenia: A Survey Study of Patients and Caregiver Proxies
Authors Maravic MC, Birch K, Nguyen ATH, Subasinghe A, Stafford E, Zacker C
Received 28 March 2024
Accepted for publication 1 January 2025
Published 9 September 2025 Volume 2025:19 Pages 2821—2834
DOI https://doi.org/10.2147/PPA.S466742
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michael Ortiz
Melissa Culhane Maravic,1 Kelly Birch,1 Anh Thy H Nguyen,1 Alicia Subasinghe,2 Elizabeth Stafford,3 Christopher Zacker2
1Precision AQ, New York, NY, USA; 2Cerevel Therapeutics, Cambridge, MA, USA; 3National Alliance on Mental Illness, Arlington, VA, USA
Correspondence: Melissa Culhane Maravic, Precision AQ, 133 Federal Street, Boston, MA, 02110, USA, Email [email protected]
Background: Antipsychotic medications are considered the mainstay of treatment for schizophrenia. However, these medications are associated with a wide range of side effects, which may be tolerated differently by patients, and may impact initiation and continuation of treatment.
Purpose: This study aimed to assess the tolerability of antipsychotic medication side effects for patients with schizophrenia and understand how side effects may impact decisions to initiate and remain in treatment.
Methods: A cross-sectional survey was conducted with 200 people living with schizophrenia and 100 caregiver proxies for those with severe disease presentation. The survey utilized the Maximum Difference Scaling (MaxDiff) approach to quantify preferences and a direct elicitation survey to rank specific side effects. Descriptive analysis and statistical analyses were conducted to address the study objectives.
Results: Results indicated that extrapyramidal side effects such as pseudoparkinsonism and tardive dyskinesia, as well as feeling detached and memory and cognitive issues were ranked as the least tolerable. In contrast, side effects such as reduced interest in/enjoyment of sex, feeling tired or drowsy, and dry mouth were perceived as more tolerable. Caregivers’ perspectives closely aligned with the care recipients’ rankings, with an additional particular concern for high blood sugar that may lead to diabetes. Side effects such as pseudoparkinsonism, memory and cognitive problems, and weight gain were associated with unwillingness to initiate or continue an effective antipsychotic medication.
Conclusion: These findings highlight the importance of considering side effect profiles when selecting and discussing treatment options with patients. Side effects can potentially impact patients’ willingness to start or switch medications, therefore, prescribing decisions should take into consideration patients’ tolerance for potential adverse effects. Engaging patients and caregivers in treatment decisions can enhance shared decision-making and treatment satisfaction. Healthcare providers should consider these findings when prescribing antipsychotic medications to people living with schizophrenia.
Plain Language Summary: Schizophrenia is a disease that disrupts a person’s thought processes, perceptions, emotional responsiveness, and social interactions. Individuals living with schizophrenia generally require continuous psychiatric care, drug treatment, and other support services throughout their lives. Antipsychotic medications can help reduce symptoms of psychosis and psychiatric hospitalizations and can improve daily functioning. However, antipsychotics have a wide range of side effects, which makes regularly taking the medication less desirable. This study found that medications used for schizophrenia are highly bothersome, and people who take these medications may view side effects as a barrier to staying consistent with treatment. Side effects like having symptoms that imitate Parkinson’s disease, problems with feeling detached from one’s surroundings, problems with memory and cognition, and significant weight gain are of most concern to people living with schizophrenia. New antipsychotic treatments with minimal side effects would likely be well received by patients and may increase consistent treatment.
Keywords: MaxDiff, direct elicitation, caregiving, treatment tolerability, treatment initiation, quantifying preferences
Introduction
Antipsychotics are considered the mainstay treatment approach for schizophrenia and are associated with improved symptoms of psychosis, reduced psychiatric hospitalizations, and improved ability to partake in activities of daily living.1,2 However, despite their efficacy, antipsychotics are associated with a range of metabolic, cardiovascular, and neurological side effects for individuals living with schizophrenia.
The side effects associated with antipsychotic medications can often lead to significant discomfort, reduce quality of life for patients, as well as hesitations in initiating therapy and posing challenges in maintaining long-term adherence.3–7 While not all antipsychotic medications are known to produce the same side effects, side effects of note include anticholinergic effects (dry mouth, blurry vision, etc), parkinsonism, reduction in sex drive, tardive dyskinesia, weight gain, and tiredness.5 While some side effects may be viewed as relatively minor, the cumulative impact of these side effects is important to patients, and prior research has indicated that the presence of side effects is significantly correlated with treatment nonadherence.8
Therefore, properly eliciting patient perspectives on side effects related to schizophrenia treatment is paramount in evaluating patient preferences. For this study, we conducted a Maximum Difference Scaling (MaxDiff) analysis to quantify patient and caregiver preferences of side effect tolerability across 11 different antipsychotic medication related side effects. The side effects assessed included pseudoparkinsonism, tardive dyskinesia, feeling detached or like a “zombie”, cognitive problems, high blood sugar, weight gain, akathisia, insomnia, reduced interest in sex, tiredness, and dry mouth.
Moreover, recognizing the considerable unmet need for more tolerable, and thus potentially more consistently maintained, treatment approaches in schizophrenia, is imperative to gain a deeper understanding of how individuals with schizophrenia and caregivers evaluate and consider the potential side effects when making decisions about treatment. By exploring the perspectives of people living with schizophrenia and caregivers of people with schizophrenia, healthcare providers can tailor treatment regimens and provide more patient-centered care.4,9,10 Research exploring patient navigations of antipsychotic medications depicts these experiences as complex.3 While antipsychotics allow patients to better manage their schizophrenia, treatment-related side effects can create additional unwanted burdens for patients, initiating a series of trade-offs for patients to consider surrounding treatment decision-making and treatment adherence.3 Previous studies show that when perspectives of patients with schizophrenia are included in the treatment decision-making process, patients are more likely to receive a treatment regimen that fits their needs.11 Consequently, exploring patient perspectives on key areas of the therapeutic process, such as side effect tolerance and unmet needs, can facilitate treatment regimens that are not only aligned towards improving the patient's disease symptoms, but to their overall goals and lifestyle as well.12,13 This in turn can help facilitate better outcomes for patients with schizophrenia and may lead to better overall treatment adherence.13
Therefore, this study was designed to gain a more comprehensive understanding of tolerance for various side effects associated with antipsychotic medications among patients with schizophrenia. To achieve this, we surveyed 200 patients with reported mild-to-moderate schizophrenia along with 100 caregiver proxies of people living with more severe schizophrenia, where patients may not have been able to complete the survey independently. Severe schizophrenia is commonly associated with reduced cognitive and functional abilities that could impact an individual’s ability to access the survey, interpret questions appropriately, and respond to survey questions in a manner that accurately reflects their current preferences and tolerance of side effects.14,15 Thus, we included caregiver proxies of those with severe schizophrenia in this study to provide an opportunity to include the voice and experience of those who may be unable to participate in this research without assistance. We aimed to identify the specific side effects that patients perceive as least tolerable, the factors influencing their decision-making process, and the equipoise required when selecting and transitioning between antipsychotic treatments.
Methods
Study Design
This observational, cross-sectional survey study evaluated 11 side effects commonly associated with antipsychotic medications, which were identified and selected via a targeted literature review and through discussion with the study team. The selected side effects that emerged from the literature as those (a) most commonly experienced by patients taking antipsychotics and (b) often identified as bothersome or as influencing treatment choice in previous patient preference studies.8,16–20
Separate but nearly identical survey instruments were fielded to patients and caregiver proxies. Both surveys incorporated a MaxDiff component, which is a quantitative survey methodology used to identify consumer preferences among brands, attributes, or items across a single dimension. MaxDiff has become a common technique to elicit utility scores in social science research and has been employed to capture patient priorities and trade-offs in treatment decision-making across various therapeutic areas,21–23 including to rank treatment goals among people living with schizophrenia.24 MaxDiff requires respondents to identify both the “best” and “worst” desirable option available within a given set of choices, allowing for the identification of the maximum difference in preference between choices.
The MaxDiff task used a balanced incomplete block design (BIBD),25 in which subsets comprising 5 of the 11 side effects are shown, and respondents identify which is most and least tolerable to them. An example choice question is shown below in Figure 1. The BIBD approach ensures that each side effect and each pair of side effects appear an equal number of times. By indicating the most and least tolerable side effects across the series of choice questions, data analysis allows us to produce a complete ranking of side effects from the most to the least tolerable.
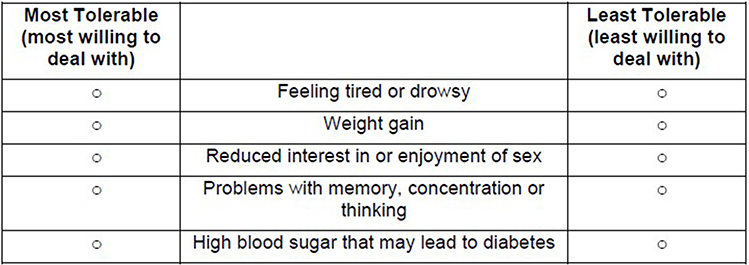 |
Figure 1 Example MaxDiff choice set. |
Both survey versions included a direct elicitation module to identify the three least tolerable side effects of the 11. Subsequent questions determined the likelihood of initiating, switching, or stopping an antipsychotic medication due to the presence of each of the three least tolerable side effects, and assessed the satisfaction with and impact of antipsychotic side effects on physical and mental health. Collecting data from the direct elicitation module and the implicit ranking (MaxDiff) task provided an opportunity to compare results and obtain a more complete picture of patient willingness to tolerate certain side effects. The caregiver proxy survey included proxy versions of all standardized instruments and all questions were phrased to elicit the perspective of the patient with schizophrenia. Additionally, the caregiver proxy survey included questions about the caregiver demographic characteristics and asked the caregiver to select the three antipsychotic side effects that were least tolerable from their point of view, rather than from the point of view of the patient.
This study protocol was reviewed by the Advarra IRB and was granted an exemption from a full review.
Study Population
The study population included a total of 300 participants: people living with schizophrenia (“patients”) who are presumed to have mild or moderate schizophrenia, as evidenced by their ability to complete the survey (n = 200), and caregivers of people living with more severe schizophrenia who served as proxies for this group that may be unable to participate in the survey independently (n = 100). Thus, two-thirds of the total sample (n = 200) represented people with mild or moderate schizophrenia (self-report) and one-third (n = 100) represented people with severe schizophrenia (proxy report). Caregiver proxy participants were recruited as a separate sample (ie, the patients they care for did not participate in the survey) and this study did not include patient and caregiver dyads (patients and their caregivers).
Eligible participants were required to be adult residents of the United States who have reached the age of majority in their state of residence (ie, over 18 for most states, 19 for Nebraska and Alabama, 21 for Mississippi), be proficient in English, and complete an informed consent form. Participants with schizophrenia were required to self-report a diagnosis of schizophrenia, report currently taking an oral antipsychotic medication to treat their schizophrenia, and obtain a score of 80% or higher on a 5-item test (ie, 4 out of 5 correct answers) designed to assess comprehension of research study participation. Caregiver proxies were required to self-report being the primary unpaid or informal caregiver of an individual diagnosed with schizophrenia who is currently taking an oral antipsychotic medication to treat their schizophrenia. In order to be eligible as a caregiver proxy for the study, caregivers were required to report a current score of 50 or lower (serious symptoms or impairment) on the Global Assessment of Functioning (GAF) measure for their care recipient, indicating serious impairment due to schizophrenia. The GAF was selected for its brevity and ease of use by a non-clinical population.26 To ensure that the sample of patients with schizophrenia was as representative as possible of the broader schizophrenia population in the United States, we established race and ethnicity quotas to govern our sampling strategy. A previous analysis using the Medical Expenditure Panel Survey (MEPS) from the years 2006–2015 reported on the demographic characteristics of community-dwelling individuals diagnosed with schizophrenia. In this study, 64% of individuals with schizophrenia were non-Hispanic white, 12% were non-Hispanic Black, and 17% were Hispanic. In terms of gender, 49% of the sample were male.
Data Source
Data for this study were derived from the online survey administered to qualified participants recruited from existing survey panels and trusted clinical partners. A third-party survey research vendor was utilized to program and deploy the online surveys, qualify respondents and track recruitment goals. Participants were recruited through the National Alliance on Mental Illness (NAMI) constituency, a community-based recruitment partner, Savvy Cooperative, and through a survey vendor, Sago. Surveys were administered via an online platform using unique enrollment links and patient IDs ensured patients were qualified to participate and did not submit multiple responses. Participants received an honorarium following completion of the survey. Pilot qualitative interviews with four patients and four caregivers proxy participants were conducted in November and December 2022. Following minor adaptations, the final survey was fielded from January-February 2023.
While there is no standardized sample size calculation that governs the MaxDiff approach, general guidance recommends a sample of at least 100 per subgroup. As such, our study included 200 patients and 100 caregiver proxies.
Statistical Analysis
Descriptive Analysis
Descriptive analyses were conducted on all variables collected in the survey modules. Continuous variables were summarized using measures of central tendency (ie, means, medians, standard deviation, ranges) and categorical or dichotomous variables were summarized using frequencies and percentages. Survey data cleaning, management, and analysis were conducted using SAS 9.4.
MaxDiff Analysis
For the main MaxDiff analysis, the individual-level utility (“tolerability”) coefficients were estimated using an empirical Bayesian approach, as described by Lipovetsky and Conklin (2015). These coefficients represent the relative level of tolerability of each side effect. Individual-level coefficients were averaged for each side effect to obtain aggregate rankings. R Software Packages “bwsTools” was used for the MaxDiff analysis.27,28
Direct Elicitation Ranking Analysis
Direct elicitation ranking questions were analyzed using frequency counts and percentages (ie, the percentage of respondents who ranked each sub-side effect as “least tolerable”).
Results
Demographic and Clinical Characteristics of Study Cohort
The study cohort consisted of 300 total participants: 200 people living with schizophrenia and 100 caregiver proxies. Table 1 describes the demographic characteristics of those with schizophrenia (n = 300), as self-reported and as reported by the caregiver proxies. The mean age of people living with schizophrenia was 41.3 years (SD: 12.5), and 54.7% were female. In terms of racial and ethnic background, 22.7% were Black, and 22.0% were Hispanic/Latino.
 |
Table 1 Demographics and Clinical Characteristics of Patients Living with Schizophrenia |
More than half (54.3%) of those with schizophrenia were diagnosed within the past 5 years, while 20.7% had received their diagnosis more than 10 years ago. All of those with schizophrenia were reported currently taking an oral antipsychotic medication, as required by the study inclusion criteria (100%), with 30.0% reported receiving a long-acting injectable (LAI) formulation. Many also reported currently taking antidepressants (51.0%), anti-anxiety medications (42.3%), and mood stabilizers (38.7%). The most reported antipsychotics were Abilify (aripiprazole) (31.7%), followed by Seroquel (quetiapine) (24.0%) and Risperdal (risperidone) (17.7%). Data are shown by respondent type (eg, caregiver proxy v. person living with schizophrenia) in Supplemental Table 1.
Caregiver proxies (Supplemental Table 2) had a mean age of 40.3 years (SD: 13.0), 57.0% reported that the care recipient was their spouse or partner and 60.0% were female. Twenty percent described themselves as Black, and 15.0% as Hispanic/Latino. Caregiver proxies reported spending an average of 49.4 hours per week (SD: 31.2) providing support to their care recipient with schizophrenia. Nearly half (47.0%) had been in a primary caregiving role for between 3 and 5 years. Caregiver proxies reported a mean GAF score of 30.8 (SD: 12.9) for their care recipient.
Tolerability Results from MaxDiff
The results of the MaxDiff analysis using pooled data from patients and caregiver proxies revealed that pseudoparkinsonism was ranked as the least tolerable side effect (tolerability weight of 0.07 (SD: 0.02)), followed by tardive dyskinesia (tolerability weight of 0.08 (SD: 0.02)) and feeling detached or like a “zombie” (tolerability weight of 0.08 (SD: 0.02)). Reduced interest in/enjoyment of sex, feeling tired or drowsy, and dry mouth were perceived as more tolerable side effects compared to others (tolerability weight of 0.10 (SD: 0.02), 0.11 (SD: 0.02), 0.12 (SD: 0.02), respectively) (Figure 2).
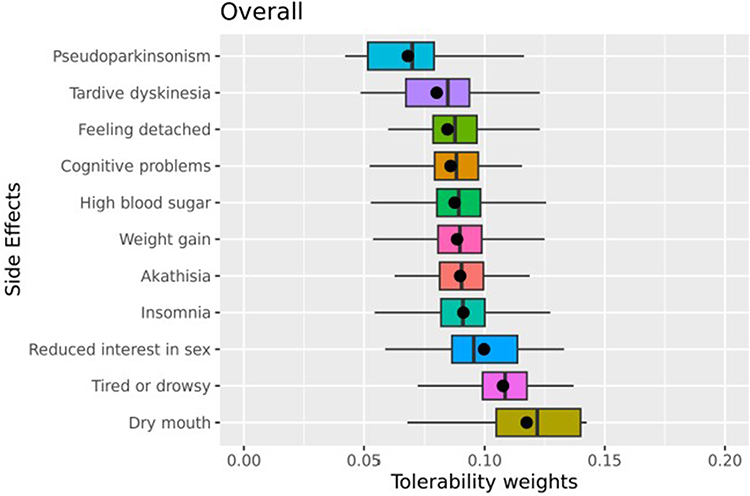 |
Figure 2 MaxDiff results of overall tolerability of treatment-related side effects. |
Comparing MaxDiff results by the respondent group showed consistent results between patient and caregiver proxy respondents (Supplemental Figure 1) with regard to the most and least tolerable side effects, providing a level of validation for caregiver proxy’s ability to ascertain side effect tolerance on behalf of their care recipient.
Tolerability Results from Direct Elicitation
Separately from the MaxDiff module, respondents (n = 300, including patients and proxies) were asked to select the top three side effects from the full list of 11 that they considered to be the least tolerable. Similar to the MaxDiff results, the most frequently selected least tolerable side effects were pseudoparkinsonism (49.7%) and memory or cognitive problems (35.3%). The third most frequently selected least tolerable side effect from the direct elicitation module was a significant weight gain (35.0%). Of note, in a follow-up question, participants reported a mean threshold of 24.7 pounds (SD: 10.7, median: 25.5) to be considered an unacceptable amount of weight gain. Similar to the MaxDiff results, dry mouth was perceived as the most tolerable side effect (6.3%) (Figure 3). These findings were generally consistent with the results obtained from the MaxDiff analysis, with the exception of significant weight gain, which was ranked on average as moderately tolerable in the MaxDiff findings.
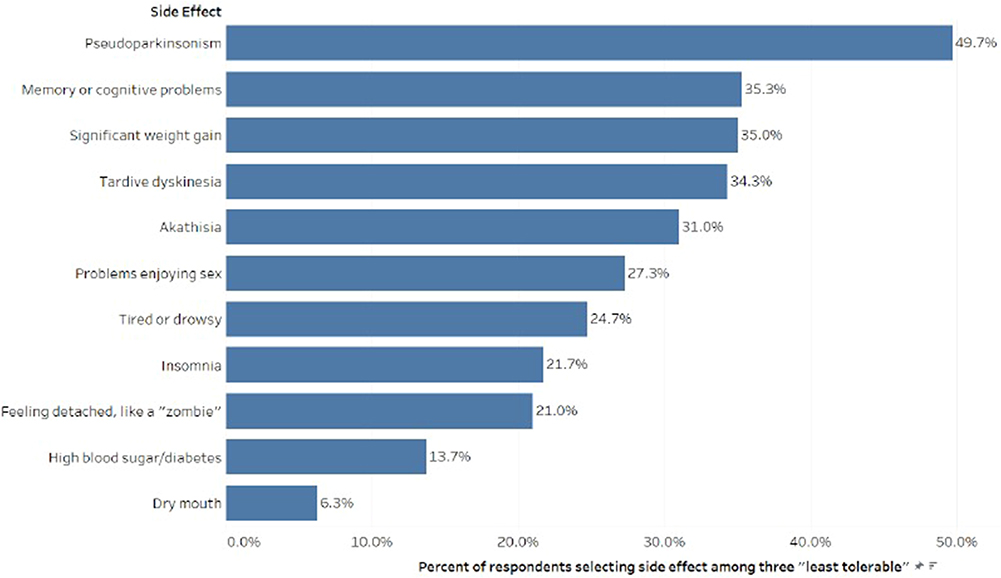 |
Figure 3 Results from direct elicitation on treatment-related side effect tolerability. |
Impact of Side Effects on Initiation and Switching of Antipsychotic Medications
Following the direct elicitation module, which asked participants to select the top three least tolerable side effects, participants were asked to then assess their willingness to start or switch an antipsychotic medication with the potential for each of the three side effects, even if the medication would improve their schizophrenia symptoms. Notably, 32.2% of respondents expressed extreme unwillingness to start a medication that could potentially cause pseudoparkinsonism and 46.3% indicated a desire to definitely want to switch to another medication, despite the medication’s effectiveness in managing their schizophrenia symptoms (Figure 4A). Fewer participants (7.6%) expressed extreme unwillingness to start a medication that could potentially cause memory or cognitive problems, and an additional 21.7% were somewhat unwilling to start. Whereas 22.6% indicated they would definitely want to switch to another medication, despite the medication’s effectiveness in managing their schizophrenia symptoms. Similarly, 9.5% of participants expressed extreme unwillingness to start a medication that could potentially cause significant weight gain, and an additional 25.7% were somewhat unwilling to start. Whereas 19.1% indicated they would definitely want to switch to another medication if it was associated with significant weight gain, despite the medication’s effectiveness in managing their schizophrenia symptoms (Figure 4B).
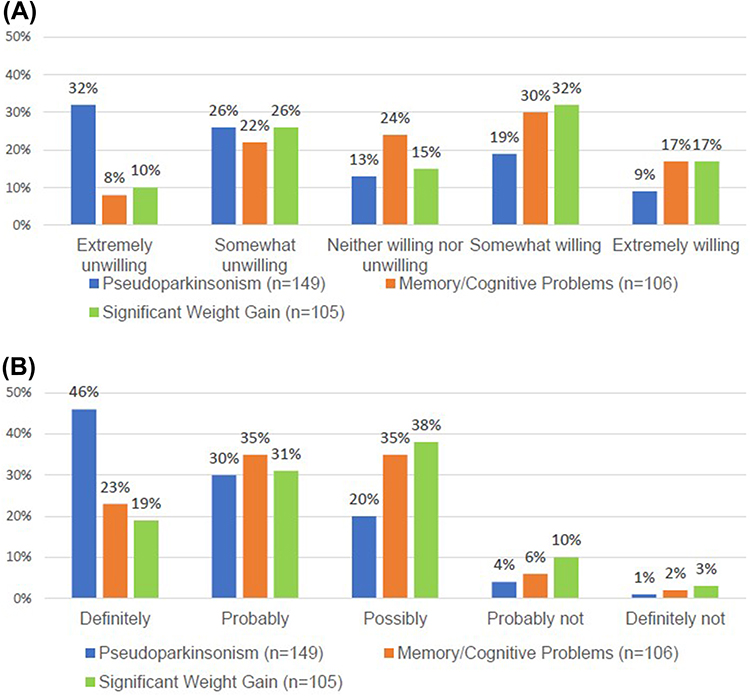 |
Figure 4 (A) Reported willingness to start an antipsychotic medication that may cause low-tolerability side effects. (B) Reported desire to switch medications if low-tolerability side effects were experienced. |
Caregiver Perspective
In addition to completing the MaxDiff and direct elicitation tolerability tasks from the perspective of the care recipient, caregivers were asked to rank the tolerability of the 11 side effects from their own perspective as a caregiver. The caregiver’s perceptions of side effect tolerability aligned with those they reported from the perspective of the care recipient, but results were not identical, indicating that caregiver proxies were capable of reporting tolerance for side effects from both the patient and caregiver perspective. Pseudoparkinsonism, feeling like a “zombie”, and tardive dyskinesia, and were consistently ranked as highly intolerable side effects by caregivers (average ranks were 7.5, 7.3 and 7.2, respectively). However, the side effect most frequently ranked as least tolerable from the caregiver perspective was high blood sugar, which could lead to diabetes (average rank of 8.5) (Figure 5).
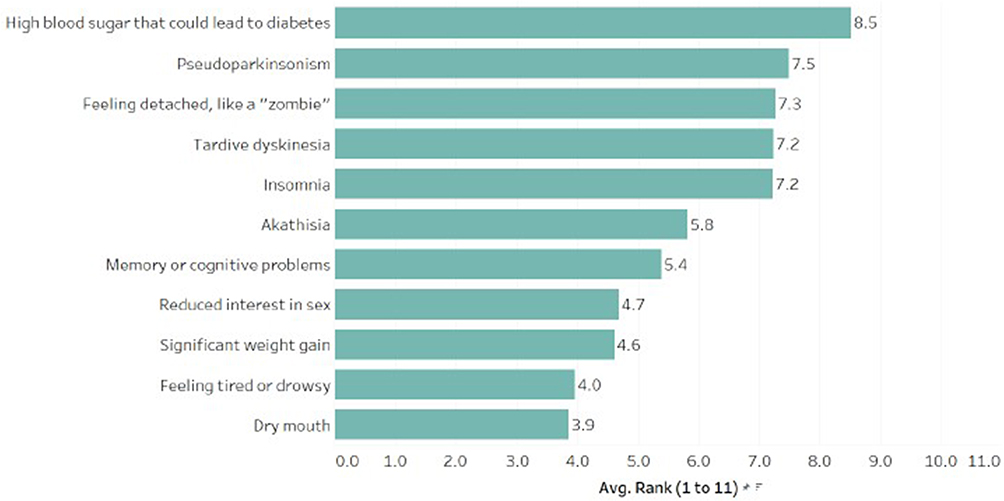 |
Figure 5 Results from caregiver perspectives on treatment-related side effect tolerability. |
Discussion
In accordance with existing research, we found that medication side effect profiles may impact treatment choice.17,29 Specifically, our findings indicated that extrapyramidal side effects, such as pseudoparkinsonism and tardive dyskinesia, were viewed as the least tolerable among all 11 side effects presented. The potential for a hypothetical antipsychotic medication to cause pseudoparkinsonism was associated with nearly one-third (32.2%) of respondents to be extremely unwilling to start the medication, which is similar to existing research.30 Previous research has shown that patients also indicated a strong preference for medications that do not negatively impact their cognitive functioning.31 Our findings revealed that the second least tolerable side effect (after pseudoparkinsonism) was memory or cognitive problems, with nearly one-third of participants (29.3%) expressing unwillingness to initiate a medication with the potential to cause memory or cognitive problems. Significant weight gain was also viewed as impacting willingness to start an effective antipsychotic medication with 36.0% indicating that it would make them somewhat or extremely unwilling to start. This finding is in line with existing research indicating that anticipated weight gain had a negative influence on willingness to try a new treatment, with over half of respondents indicating they would decline to try a new treatment that would result in weight gain of 20 pounds or more.18
Concern for side effects was also found to impact willingness to start or continue antipsychotics. Our findings suggest that the potential for several common side effects may prompt a patient to switch antipsychotic medications. Nearly half (46.3%) indicated they would definitely want to switch to another medication if it carried the risk of pseudoparkinsonism, even if the medication was effective in managing their schizophrenia symptoms. Approximately 20% of the participants indicated they would definitely want to switch to another medication with the potential to cause memory or cognitive problems, despite the medication’s effectiveness in managing their schizophrenia symptoms. Similarly, 19.1% of the participants indicated they would definitely want to switch to another medication if it was associated with significant weight gain, despite the medication’s effectiveness in managing their schizophrenia symptoms. Switching antipsychotic medications is a substantial barrier to effectiveness; previous studies have indicated that patients who switch antipsychotic medication experience significantly higher risk of relapse, acute-care and crisis services utilization, and furthermore, acute-care services were used significantly sooner. Further, switching is also associated with a significant increase in total healthcare costs.32,33
Comparisons of caregiver proxy and patient findings revealed consistency regarding pseudoparkinsonism as the least tolerable side effect from the patient perspective, however caregivers ranked high blood sugar as the least tolerable when responding based on their own feelings. This “discrepancy” or incongruent viewpoint reinforces the idea that while caregivers can be reliable proxies to communicate the patient’s preferences, they also have their own preferences and priorities, potentially increasing the complexity of shared decision-making. Providers must ensure that when a caregiver is involved in treatment decision-making discussions, they are able to clearly articulate, validate and address potential differences in priorities between patients and caregivers (eg, treating a caregivers’ concern about high blood sugar seriously and offering resources/support, even if the patient does not seem to have significant concerns).
The importance of understanding patients’ perspectives on side effect tolerability and preferences and incorporating these perspectives wherever possible is vital to effective shared decision-making for people living with schizophrenia. Shared-decision-making may help physicians optimize prescribing choices, which may lead to enhanced patient satisfaction and quality of life and improve treatment outcomes.34,35 Healthcare providers should consider these findings when prescribing antipsychotic medications to people living with schizophrenia, to promote effective treatment initiation, continuation and satisfaction. Finally, further research around the impact of side effect tolerability and the inclusion of patient-reported outcomes (PROs), particularly those focused on side effects, in clinical trials of antipsychotics medications is crucial for patient-focused drug development.
Limitations
As with all survey-based research, participation is voluntary, and thus self-selection bias may be present. The web-based nature of the survey is also likely to result in a respondent sample with adequate access to and ability to use technology. Participants with schizophrenia and the care recipients of the caregiver proxies were required to be at the age of majority for their state or older, which limits the generalizability of these findings. Caregivers who respond as proxies for those with severe illness also may not be able to respond on behalf of the recipient with complete accuracy. However, our subgroup analysis comparing patients and caregiver proxies’ tolerability for side effects found similar results. Further, all information collected is self-reported and thus prone to reporting bias.
The MaxDiff choice questions require respondents to make a hypothetical decision and thus may not reflect real-world decision choices. Responses may also have been affected by previous experience of side effects; for example, patients who have experienced extrapyramidal symptoms in the past may have placed greater importance on avoiding these effects in the future, potentially impacting responses to questions about initiation and switching medications associated with these side effects. Additionally, the survey questions inherently required people to imagine the impact of a side effect they may or may not have experienced, which may have influenced the importance they attributed to certain side effects. Choice questions can be cognitively demanding, though we attempted to mitigate this by using a manageable number of choice sets based on simple experimental design. Side effects included in this study were chosen following a targeted literature review and discussion with patient advocates; however, other side effects not studied here may be important to patients.
Further, in describing tardive dyskinesia, we did not specify that the effects can be permanent, and the reporting of this side effect as least tolerable may have been influenced by this omission.
Conclusion
In conclusion, this study highlights the potential impact of antipsychotic side effects on treatment choice in patients with schizophrenia. Antipsychotic side effects were found to be highly bothersome, with patients reporting interference with their mental and physical health. Pseudoparkinsonism, tardive dyskinesia, feeling detached or “like a zombie”, problems with memory and cognition, and significant weight gain were revealed to be among the least tolerable side effects. Understanding and addressing patient preferences and concerns regarding side effects are crucial for promoting treatment adherence and shared decision-making between physicians and patients with schizophrenia. Further research is needed to explore the relationship between side effect intolerability and treatment outcomes in this population.
Abbreviations
MaxDiff, Maximum Difference Scaling; BIBD, balanced incomplete block design; SF-12, 12-Item Short Form Health Survey; GASS, Glasgow Antipsychotic Side-effect Scale; GAF, Global Assessment of Functioning; MEPS, Medical Expenditure Panel Survey; NAMI, National Alliance on Mental Illness; LAI, long-acting injectable; PROs, patient-reported outcomes.
Ethics Approval and Informed Consent
This study was conducted with approval from the Ethics Committee of Advarra Institutional Review Board. Written informed consent was obtained from all participants prior to survey completion. The procedures of this study were followed according to the regulations established by the declaration of Helsinki.
Acknowledgments
The authors would like to acknowledge Jonathon Wong for his invaluable contribution to the writing of this manuscript. The abstract of this paper was presented at the 2023 Schizophrenia International Research Society (SIRS) conference in Toronto, Canada as a poster presentation with interim findings.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Cerevel Therapeutics.
Disclosure
MCM and AHN are employees of Precision AQ, a consulting firm awarded funding by Cerevel Therapeutics to conduct this study. KB is a former employee of Precision AQ. MCM owns equity interest in Precision Medicine Group, the parent company of Precision AQ. CZ and AS are employees of Cerevel Therapeutics who provided funding for this study. At the time of this research, ES was an employee of the National Alliance on Mental Illness (NAMI), which has received research funding from Cerevel Therapeutics. The authors report no other conflicts of interest in this work.
References
1. Ceraso A, Lin JJ, Schneider-Thoma J, et al. Maintenance treatment with antipsychotic drugs for schizophrenia. Cochrane Database Syst Rev. 2020;8(8):CD008016. doi:10.1002/14651858.CD008016.pub3
2. Oluboka O, Clerzius G, Janetzky W, et al. Improvement of functioning in patients with schizophrenia: real-world effectiveness of aripiprazole once-monthly (REACT study). BMC Psychiatry. 2023;23(1):383. doi:10.1186/s12888-023-04893-8
3. Doane MJ, Sajatovic M, Weiden PJ, et al. Antipsychotic treatment experiences of people with schizophrenia: patient perspectives from an online survey. Patient Prefer Adherence. 2020;14:2043–2054. doi:10.2147/PPA.S270020
4. Southern J, Elliott P, Maidment I. What are patients’ experiences of discontinuing clozapine and how does this impact their views on subsequent treatment? BMC Psychiatry. 2023;23(1):353. doi:10.1186/s12888-023-04851-4
5. Stroup TS, Gray N. Management of common adverse effects of antipsychotic medications. World Psychiatry. 2018;17(3):341–356. doi:10.1002/wps.20567
6. Zichlin ML, Mu F, Leo S, Ayyagari R. The impact of antipsychotic dose reduction on clinical outcomes and health care resource use among medicare patients with schizophrenia. Clin Drug Investig. 2021;41(10):853–863. doi:10.1007/s40261-021-01060-3
7. Baumgardner J, Shahabi A, Linthicum M, Vine S, Zacker C, Lakdawalla D. Greater spending associated with improved survival for some cancers in OCM-defined episodes. J Manag Care Spec Pharm. 2018;24(6):504–513. doi:10.18553/jmcp.2018.24.6.504
8. Dibonaventura M, Gabriel S, Dupclay L, Gupta S, Kim E. A patient perspective of the impact of medication side effects on adherence: results of a cross-sectional nationwide survey of patients with schizophrenia. BMC Psychiatry. 2012;12:20. doi:10.1186/1471-244X-12-20
9. Townsend M, Pareja K, Buchanan-Hughes A, et al. Antipsychotic-related stigma and the impact on treatment choices: a systematic review and framework synthesis. Patient Prefer Adherence. 2022;16:373–401. doi:10.2147/PPA.S343211
10. Yeo V, Dowsey M, Alguera-Lara V, Ride J, Lancsar E, Castle DJ. Antipsychotic choice: understanding shared decision-making among doctors and patients. J Ment Health. 2019;30(1):66–73. doi:10.1080/09638237.2019.1630719
11. Mucci A, Kawohl W, Maria C, Wooller A. Treating schizophrenia: open conversations and stronger relationships through psychoeducation and shared decision-making. Front Psychiatry. 2020;11:761. doi:10.3389/fpsyt.2020.00761
12. Mahone IH, Maphis CF, Snow DE. Effective strategies for nurses empowering clients with schizophrenia: medication use as a tool in recovery. Issues Ment Health Nurs. 2016;37(5):372–379. doi:10.3109/01612840.2016.1157228
13. Pérez-Revuelta JI, González-Sáiz F, Pascual-Paño JM, et al. Shared decision making with schizophrenic patients: a randomized controlled clinical trial with booster sessions (DECIDE study). Patient Educ Couns. 2023;110:107656. doi:10.1016/j.pec.2023.107656
14. O’Carroll R. Cognitive impairment in schizophrenia. Adv Psychiatric Treat. 2000;6(3):161–168. doi:10.1192/apt.6.3.161
15. McCutcheon RA, Keefe RSE, McGuire PK. Cognitive impairment in schizophrenia: aetiology, pathophysiology, and treatment. Mol Psychiatry. 2023;28(5):1902–1918. doi:10.1038/s41380-023-01949-9
16. de Araújo AA, de Araújo Dantas D, Do Nascimento GG, et al. Quality of life in patients with schizophrenia: the impact of socio-economic factors and adverse effects of atypical antipsychotics drugs. Psychiatr Q. 2014;85(3):357–367. doi:10.1007/s11126-014-9290-x
17. Levitan B, Markowitz M, Mohamed AF, et al. Patients’ preferences related to benefits, risks, and formulations of schizophrenia treatment. Psychiatric Serv. 2015;66(7):719–726. doi:10.1176/appi.ps.201400188
18. Achtyes E, Simmons A, Skabeev A, et al. Patient preferences concerning the efficacy and side-effect profile of schizophrenia medications: a survey of patients living with schizophrenia. BMC Psychiatry. 2018;18(1):292. doi:10.1186/s12888-018-1856-y
19. Leucht S, Cipriani A, Spineli L, et al. Comparative efficacy and tolerability of 15 antipsychotic drugs in schizophrenia: a multiple-treatments meta-analysis. Lancet. 2013;382(9896):951–962. doi:10.1016/s0140-6736(13)60733-3
20. Tandon R, Lenderking WR, Weiss C, et al. The impact on functioning of second-generation antipsychotic medication side effects for patients with schizophrenia: a worldwide, cross-sectional, web-based survey. Ann Gen Psychiatry. 2020;19:42. doi:10.1186/s12991-020-00292-5
21. Cheung KL, Wijnen BFM, Hollin IL, et al. Using best-worst scaling to investigate preferences in health care. Pharmacoeconomics. 2016;34(12):1195–1209. doi:10.1007/s40273-016-0429-5
22. Mooney-Doyle K, Deatrick JA, Ulrich CM, Meghani SH, Feudtner C. Parenting in childhood life-threatening illness: a mixed-methods study. J Palliat Med. 2018;21(2):208–215. doi:10.1089/jpm.2017.0054
23. Rosa WE, Chittams J, Riegel B, Ulrich CM, Meghani SH. Patient trade-offs related to analgesic use for cancer pain: a MaxDiff analysis study. Pain Manag Nurs. 2020;21(3):245–254. doi:10.1016/j.pmn.2019.07.013
24. Bridges JF, Beusterien K, Heres S, et al. Quantifying the treatment goals of people recently diagnosed with schizophrenia using best-worst scaling. Patient Prefer Adherence. 2018;12:63–70. doi:10.2147/PPA.S152870
25. Campbell BF, Sengupta S, Santos C, Lorig KR. Balanced incomplete block design: description, case study, and implications for practice. Health Educ Q. 1995;22(2):201–210. doi:10.1177/109019819502200208
26. Aas IHM. Guidelines for rating Global Assessment of Functioning (GAF). Ann Gen Psychiatry. 2011;10:2. doi:10.1186/1744-859X-10-2
27. White MH. bwsTools: an R package for case 1 best-worst scaling. J Choice Model. 2021;39:100289. doi:10.1016/j.jocm.2021.100289
28. Charrad M, Ghazzali N, Boiteau V, Niknafs A. NbClust: an R package for determining the relevant number of clusters in a data set. J Stat Softw. 2014;61(6). doi:10.18637/jss.v061.i06
29. Chiang YL, Klainin‐Yobas P, Ignacio J, Chng CML. The impact of antipsychotic side effects on attitudes towards medication in people with schizophrenia and related disorders. J Clin Nurs. 2011;20(15–16):2172–2182. doi:10.1111/j.1365-2702.2010.03659.x
30. Tandon R, Jibson M. Extrapyramidal side effects of antipsychotic treatment: scope of problem and impact on outcome. Ann Clin Psychiatry. 2002;14(2):123–129. doi:10.3109/10401230209149099
31. McCrone P, Mosweu I, Yi D, Ruffell T, Dalton B, Wykes T. Patient preferences for antipsychotic drug side effects: a discrete choice experiment. Schizophr Bull Open. 2021;2(1). doi:10.1093/schizbullopen/sgab046
32. Faries DE, Ascher-Svanum H, Nyhuis AW, Kinon BJ. Clinical and economic ramifications of switching antipsychotics in the treatment of schizophrenia. BMC Psychiatry. 2009;9:54. doi:10.1186/1471-244X-9-54
33. Ayyagari R, Thomason D, Mu F, Philbin M, Carroll B. Association of antipsychotic treatment switching in patients with schizophrenia, bipolar, and major depressive disorders. J Med Econ. 2019;23(2):204–212. doi:10.1080/13696998.2019.1685818
34. Torrecilla-Olavarrieta R, Pérez-Revuelta J, García-Spínola E, et al. Satisfaction with antipsychotics as a medication: the role of therapeutic alliance and patient-perceived participation in decision making in patients with schizophrenia spectrum disorder. Int J Psychiatry Clin Pract. 2020;25(3):268–276. doi:10.1080/13651501.2020.1804942
35. Hatano M, Takeuchi I, Yamashita K, et al. Satisfaction survey on antipsychotic formulations by schizophrenia patients in Japan. Clin Psychopharmacol Neurosci. 2021;19(4):610–617. doi:10.9758/cpn.2021.19.4.610
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.