Back to Journals » Patient Preference and Adherence » Volume 16
Quality Perceptions and Choice of Public Health Facilities: A Mediation Effect Analysis of Outpatient Experience in Rural China
Received 19 April 2022
Accepted for publication 2 August 2022
Published 12 August 2022 Volume 2022:16 Pages 2089—2102
DOI https://doi.org/10.2147/PPA.S370805
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Naifeng Liu
Shuying Yin,1,2 Min Hu,1 Wen Chen1
1Department of Health Economics, School of Public Health, Fudan University, Shanghai, People’s Republic of China; 2Research Department I, Shenzhen Health Development Research and Data Management Center, Shenzhen, People’s Republic of China
Correspondence: Wen Chen; Min Hu, The Department of Health Economics, School of Public Health, Fudan University, No. 187 Box, 138 Yixueyuan Road, Xuhui District, Shanghai, 200032, People’s Republic of China, Tel +86 13818325486 ; +86 17717031079, Email [email protected]; [email protected]
Purpose: Outpatients have choices of providers in the hierarchical health service delivery system of China. Understanding how quality perceptions and outpatient experience affect the choice of health facility would help inform decisions about priorities for action aimed at guiding the use of primary care. This study examines how quality perceptions of outpatient service affect the facility level choice in rural China.
Methods: Household surveys were conducted in 2011, 2012 and 2015 in Ningxia Hui Autonomous Region, China. We selected 968 respondents as the study sample, who had at least two outpatient visits to the public health facilities during each survey period. Prior quality perceptions of the outpatient service at the village clinics, township centers, and county hospitals were reported on an 8-item Quality Indicator questionnaire. Experienced quality perception from the first outpatient visit was also reported. The outcome of interest was outpatients’ facility level choices. We used regression and mediation analysis to explore whether and how outpatient experience at a specific health facility would mediate the relationship between prior quality perceptions and the facility level choice.
Results: Overall, the quality perception was positively and significantly associated with outpatients’ staying at the same or lower levels of care (β=0.265, P=0.007). This effect was fully mediated by experienced quality perception (z=2.985, P=0.003). The indirect effect was significant for three particular dimensions, including quality perceptions of the environment (β=0.075, P=0.025), doctor-patient communication (β=0.065, P=0.022), and physician ability (β=0.062, P=0.021).
Conclusion: Outpatient quality perceptions—especially positive perceptions regarding environment, doctor-patient communication, and physician ability—could contribute to minimizing upward referral via improvement in outpatient experience. Policymakers and health care providers may need to therefore optimize outpatient experience as they push to develop a more locally responsive primary care system.
Keywords: perceived quality, choice of provider, outpatient care, questionnaire, China
Plain Language Summary
What was already known?
- Quality perceptions of health care affect the patients’ choice of health facility.
What does this study add?
- This study investigated whether and how outpatients’ quality perceptions affect their choice of health facility.
- Outpatients’ quality perceptions of the service quality predicted their staying at the same level of care or downward-referral.
- The effect of outpatients’ quality perceptions on patient choice occurred indirectly via change to the quality perception of outpatient experience.
- Positive quality perceptions regarding the health facility environment, doctor-patient communication, and physician ability—could contribute to minimizing upward referral via improvement in outpatient experience.
What do the findings imply?
- The role of the betterment of outpatient experience appears to be marginal and worthy of reconsideration by policymakers and other stakeholders.
- To direct access choices towards primary care facilities, improvements in patients’ subjective feeling about the environment, the doctor-patient informative communication, and the physician’s ability at primary care facilities are likely to be required.
Introduction
In China, the primary health facilities are frequently bypassed by outpatients in favor of secondary or tertiary-level health facilities,1 despite the substantial additional time and financial costs. Studies have shown that concerns about the quality of primary health facilities may be an important factor.2,3 Patients subconsciously deem the high-tier health facilities to provide more valuable health care, and their health seeking behavior inadvertently promotes further concentration of market resources towards high-tier health facilities. For the last decade, the Chinese government has implemented a series of financial investment and related policies4 to improve the infrastructure and quality of primary health services, especially in rural areas,5 but the progress in encouraging the utilization of primary care has so far been limited. Clarifying the relationship between the quality perceptions of different tier health facilities and the facility-level choice in rural China therefore has significant policy implications.
Quality of health care is the criteria that measures the performance of a health care system, such as the service accessibility, level of health technology, efficiency of intersectoral cooperation and community participation.6 Quality perception is here defined as the evaluation of health care from patients’ perspective,7 a process through which the patients’ expectations are balanced with the perceptions of the care they receive.8 The perceptions are generated by the patient’s expectations and experiences, including but not limited to patient views, opinions or experiences of accessing health care services.
Studies have suggested that quality perceptions of health care exert an effect on the patients’ healthcare-seeking behavior.9–11 Perceptions of healthcare quality have been associated with patients’ preference for different health care providers,12 affecting subsequent behaviors.13 Suppose the prior perception of a health care provider is favorable. In that case, it may enhance future health service utilization with the specific provider, adherence to the recommended treatment, and generate desired clinical outcomes. Furthermore, the choice of health facility is likely to be conditional on the initial service experience. It is important for outpatients to have favorable experience while using health care, to achieve behavioral loyalty to certain healthcare providers.14,15 Consider, for example, the prior quality perception could be an antecedent to the perception of a certain service experience,16–19 the effect of prior quality perception on the choice of health facility is likely to occur indirectly through making changes in perception about the service experience. Therefore, it is likely that both prior quality perception and experienced quality perception are determinants of patient choice.
By linking quality perceptions, outpatient experience to facility-level choice, a dynamic understanding of how outpatients decide upon the optional health facilities would be informed. While studies have explored how quality perceptions might matter for patients’ revisiting behavior or loyalty,9–11 the effect of quality perceptions on patient behavior as mediated by patient experience is scarce in literature.20 Given the primary health facilities’ important role in gatekeeping services from higher tier health facilities in rural China, our intended choice outcome would be the outpatients’ retention at the same level of care or downward-referral. Until now, no study in China has been able to delineate whether outpatients’ retention at the same level of care or downward-referral might occur due to quality perceptions.
With the growing attention on patient-centered care,21,22 measurements of the relationship between different dimensions of quality perceptions and the choice of provider help to identify what aspects matter most to patients,9,23–26 and are accordingly, informative in delivering patient-centered health care service by taking targeted measures to make health service responsive to the patient demands. Previous studies have helped identify the important drivers of positive perception of service experiences, such as patient-doctor communication,24,25 waiting time,23 environment26 and physician ability.9 These results are inconsistent across study regions. This study also adds to the mixed results by identifying which aspects of outpatient experiences at public health facilities may matter most to patients and drive their reports of positive perceptions with the service, and thus contributing to the choice outcome in rural China.
This study aims to examine whether quality perceptions predict the outpatients’ choice of level of care in public health facilities. We specifically investigated whether outpatients’ prior quality perception directly affects their choice of health facility, or whether outpatient experience mediates this effect. If the second case is true, we would further disaggregate the mediation effect for different quality perception dimensions.
Research Framework and Hypotheses
Figure 1 shows the proposed research model. The effect of quality perception on outpatients’ choice of health facility is divided into two pathways. One is the direct effect of prior quality perception on outpatients’ choice of health facility, the other is the indirect pathway through the outpatient experience. We validated this model in the context of rural China by considering the hypotheses as follows:
H1: Prior quality perception of a health facility has positive effect on the probability of outpatients choosing that health facility. H2: Prior quality perception of a health facility has positive effect on the experienced quality perception of that health facility. H3: Experienced quality perception of a health facility has positive effect on the probability of outpatients choosing that health facility. H4: Outpatient experience mediates the relationship between prior quality perception and the choice of health facility.
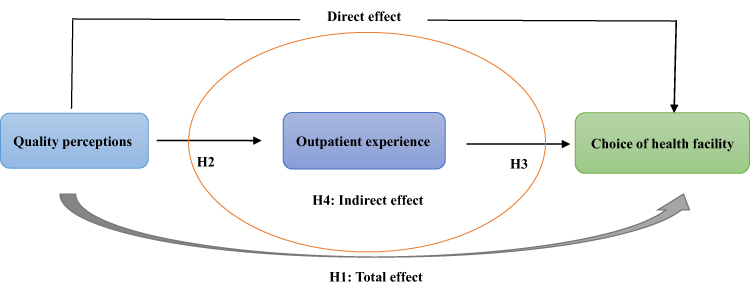 |
Figure 1 Proposed research model. |
Materials and Methods
Study Setting
The context of the current study is in Ningxia Hui Autonomous Region, a northwest rural area with a population of 6.252 million. Ningxia had the third lowest level of Gross Domestic Product (GDP) per capita among all provinces in China during the study27 so it could be seen as representative of less-developed areas of China. The Chinese government has targeted village clinics (VCs) and township centers (THCs) as primary care gatekeepers to higher tiers of health care services in the rural regions, but there have been no designated medical institutions for outpatients seeking health care. This study considered outpatients’ choice under the public health facilities setting, but it is worthy to note that there are also private clinics in the studied area, accounting for less than 10% of all the health facilities.
Questionnaire Survey
Face-to-face household surveys were conducted in 2011, 2012 and 2015 at Ningxia Hui Autonomous Region, using multistage stratified sampling from 6702 households, comprising 28,548 individuals from 78 townships and 917 villages. The household attrition rates were 18.39% and 31.61% for the 2012 and 2015 waves, respectively. We replaced households with which we could not follow up during the 2012 and 2015 waves with randomly selected households from the same village.
The household questionnaire was initially developed in Chinese. The surveys captured the respondents’ demographic characteristics, health status, comorbidities, the family’s economic level and household size. The surveys also included the outpatients’ 8-item quality perceptions of different tier health facilities (Appendix 1), and the evaluation of each outpatient visit (Appendix 1). The internal consistency for the questionnaire using Cronbach’s alpha test was 0.903 for the 8-item quality perception section. Cronbach’s alpha is deemed excellent if higher than 0.9. Additionally, a pilot study was conducted in 2009 to ensure all questions were clear and reliable to the Chinese population. The results obtained in the pilot study were not included in this analysis.
Sampling Procedures
The minimum sample size required to conduct this study was calculated based on a confidence level (Cl) of 95%, a 4% margin of error, and a 50% distribution response for a population of over 20,000. As a result, the minimum required sample size was found to be 583.
The inclusion criteria of study samples were: i) patients sought outpatient care, ii) had at least two contacts, iii) at public health facilities, including village clinics, township centers and county hospitals over the past 14 days before the household surveys. The exclusion criteria of study samples was: the respondents who had exordinary higher out-of-pocket payments (higher or equal to 10,000 Yuan) for the second outpatient visit compared with other respondents. As a result, 968 respondents were enrolled in the study, as shown in the flow diagram (Figure 2).
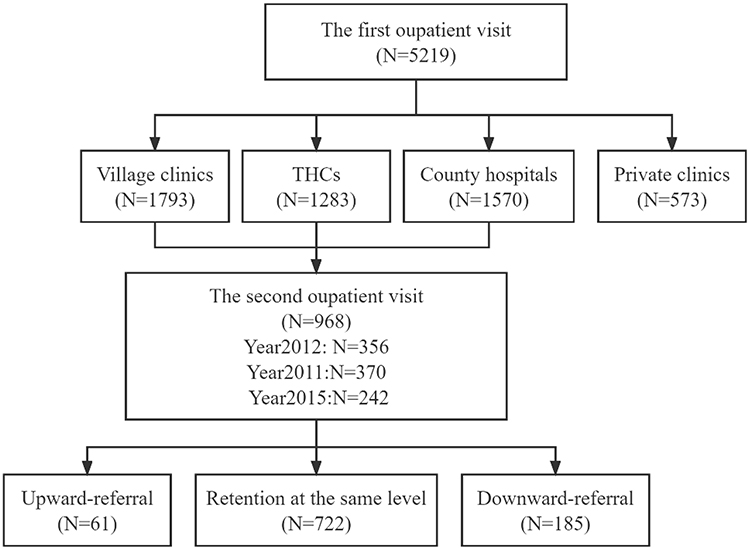 |
Figure 2 The enrollment of study samples. |
Ethics
The study was conducted in accordance with the Declaration of Helsinki. The study received ethical approval from the University of Oxford Review Committee, Ningxia Medical University Ethical Review Board and Fudan University Ethical Review Board (IRB00002408). Respondents gave their informed consent for inclusion orally before participating in the study. As this is a non-invasive, survey-type study, the research involved no procedures for which written consent is usually required. The verbal informed consent was approved by the institutional review boards upon reviewing the study protocol. Respondents under 18-years old were approved by the ethics committees to provide informed consent either on their own behalf or by their parents.
Measurements
Outpatients’ Choice of Health Facility
We assume that the health service quality of the same tier health facility is homogeneous. Considering the importance of strengthening gate-keeping role of the primary care in rural China, we specifically expected that patients retained at the same tier health facility or referred downward. The outcome variable–outpatients’ choice of health facility, was a binary variable, with outpatients’ retention or downward-referral denoting 1 and outpatients’ upward-referral denoting 0.
Prior Quality Perceptions
The quality perceptions of outpatient care were reported on an 8-item Quality Indicator questionnaire (Appendix 1), which was developed from the patients’ perspective by Hu Min, Winnie Yip, etc.28 A five point Likert-type scale, ranking from (1) “Very poor” to (5) “Very good”, was used to measure the prior quality perceptions. Apart from the overall quality perception, seven dimensions of outpatients’ quality perceptions were measured using the following items: i) waiting time (WT), ii) the environment cleanliness and comfort level (ECCL), iii) physician politeness and consideration of patients (PPCP), iv) physician description of illness, causes, and treatment plan (PDICTP), drug availability (DA), vi) equipment sophistication (ES), vii) physician ability to diagnose and treat illness (PADTI).
Potential Mediator: Experienced Quality Perception
Literature has widely shown that service experience can contribute to the formation of healthcare quality perceptions.10,12,16 Based on the two outpatient visits over the 14 days we observed, the evaluation of the first outpatient experience at a specific health facility was measured to bridge the link from prior quality perception to the choice of health facility (Appendix 1: Panel B1). In response to the evaluation of the first outpatient experience, a five-point Likert-type scale, ranking from (1) represents “Very poor” to (5) represents “Very good” was used.
Covariates
According to Anderson’s framework,29 the extent to which an individual chooses to use healthcare services depends on three types of factors: predisposing characteristics, the need for services and enabling factors. Drawing on this model, we controlled for potential confounding by assessing the following characteristics on outpatients’ choice of health facility: predisposing characteristics (age, gender, educational attainment, marital status, household size); their need for services (self-reported health, chronic disease conditions and disease types); and enabling considerations (asset index, employment status). The missing data for marriage were replaced and categorized into “Divorced/Widowed/Else”. Year effects and county effects were controlled in each regression model. Different insurance types were not included in the analysis, as more than 93.5% of the residents in these 5 counties were covered exclusively by the New Rural Cooperative Medical Care System.
Data Analysis
Frequency distribution and mean statistics were used to describe the patients’ characteristics. The dropout analysis is shown in Figure 2.
To verify the relationships in the proposed model, the data were fit to three multiple linear regression models, which controlled for patient characteristics, year effects and county effects. These three regression models were developed using Baron and Kenny’s procedure,30 to determine whether prior quality perceptions predicted the outpatients’ choice of health facility directly or indirectly via outpatient experience. If it occurred indirectly, we could conclude that it was mediated by the outpatient experience. In the first model, outpatients’ prior quality perception and the choice of health facility were entered as the independent and dependent variables, respectively. In the second model, prior quality perception and experienced quality perception of an outpatient visit were entered as the independent and dependent variables, respectively. In the third model, prior quality perception and experienced quality perception of an outpatient visit were both entered as independent variables, and outpatients’ choice of health facility was entered as the dependent variable. Sobel tests31 were further conducted to examine the mediatory effects.
If the mediation effect exists, the next step was to disaggregate the effect of prior quality perception. To remove the potential risk of mediator-outcome confounding, we further conducted a mediation analysis proposed by Karlson, Hom, and Breen32 (KHB). The basic idea of the KHB approach was to compare the full model with a reduced model that substitutes the residuals of the mediator from a regression of the mediator on the key variables. Compared with the estimates from Baron and Kenny’s procedure, in the case of binary outcomes such as the outpatients’ choice in our case, the KHB method allows separation of the change in the coefficient due to either confounding or rescaling.33,34
All statistical analysis was performed using Stata 15.1 statistical software.
Results
Patients’ Characteristics
Table 1 shows the socio-demographic characteristics of the study sample. Women accounted for more than half of the participants. Over 51.88% of the respondents’ age was between 41 and 65 years. Over 61.24% attended school. More than 75.27% of respondents were married. The unemployment rate was less than 1.40%. The most common profession is farmers, which accounted for over 63.64%. The average household size was over 4. Poor or very poor health was reported by less than 47.21%.
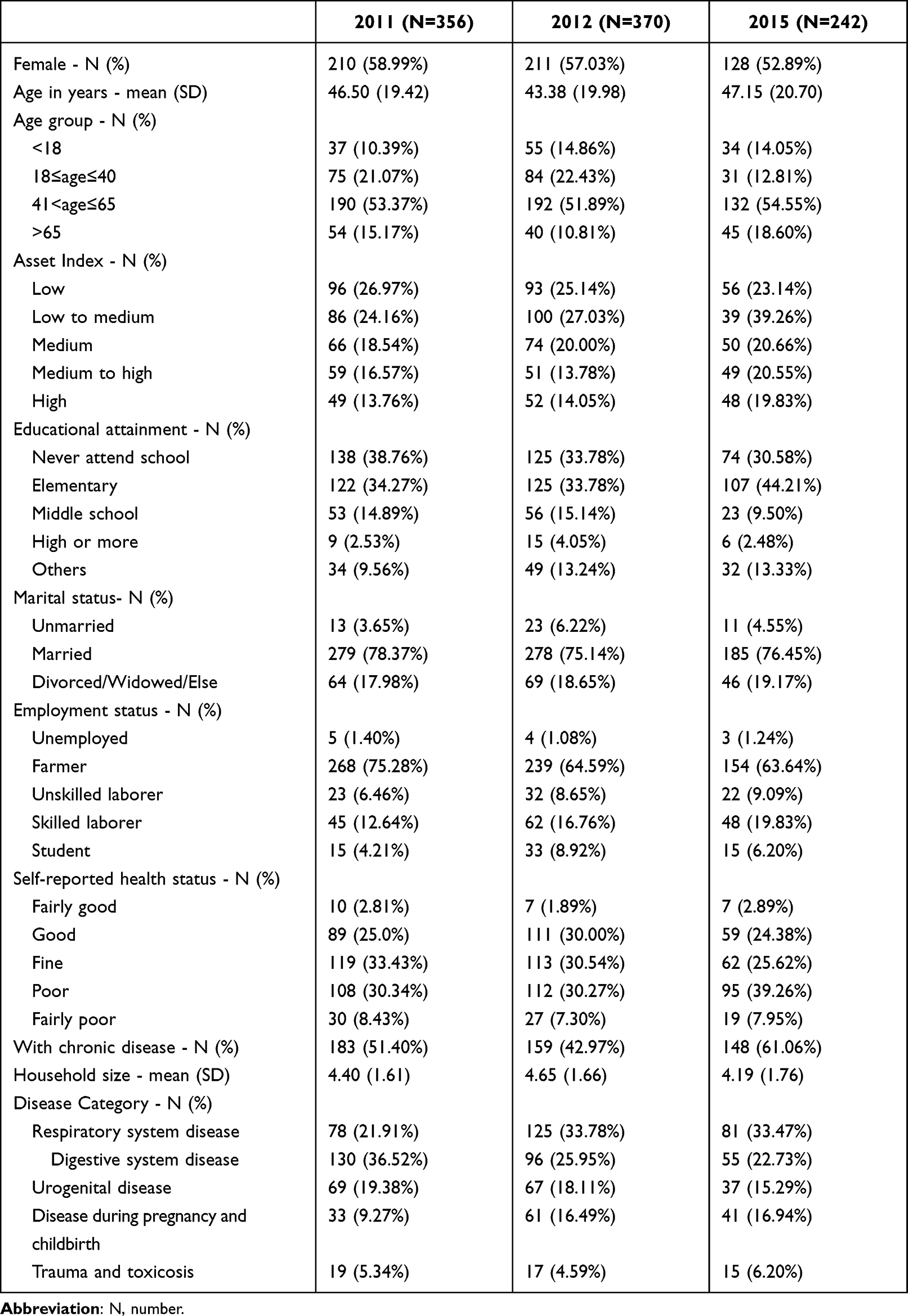 |
Table 1 Social-Demographic Characteristics of the Participants (N=968) |
Outpatient Care Quality Perceptions
Table 2 contains the ratings of the prior quality perception and the experienced quality perception. In the responses to the overall prior quality perception, compared to patients who retained at the same level of care (“retention”) or referred downward to lower tier public hospitals (“downward referral”), patients who sought higher level care (“upward referral”) rated lower score to the previously visited health care provider (P=0.025). Likewise, in the responses to the quality perception of the previously outpatient experience, compared to those who had retentions or downward referrals, patients who sought higher level care rated lower score to the previously visited provider (P<0.001).
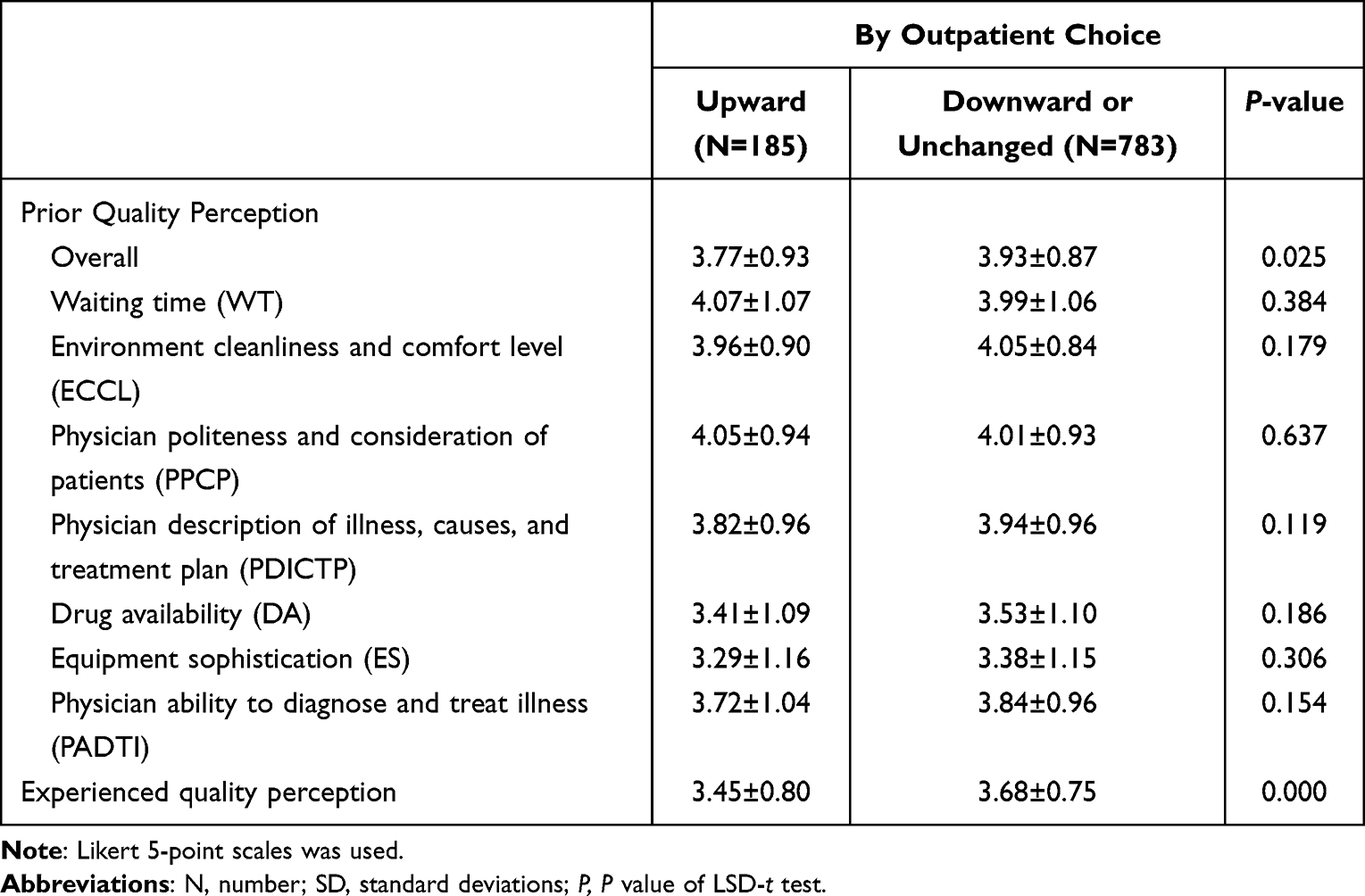 |
Table 2 Outpatient Care Quality Perceptions According to the Choice Outcome (N=968, Mean ± SD) |
Outpatients’ Choice of Health Facility
Table 3 presents the two outpatient choices we observed. For the first outpatient visit, 35.23% of the respondents sought outpatient care at village level, followed by 35.02% of the respondents sought outpatient care at county level or above, and 29.75% of the respondents sought outpatient care at township level. For the second visit, compared to the previous visit, 74.43% of the respondents stayed at the same tier health facilities, 6.49% of the respondents referred downward towards lower-tier health facilities, while 19.07% of the respondents referred upward towards higher tier health facilities.
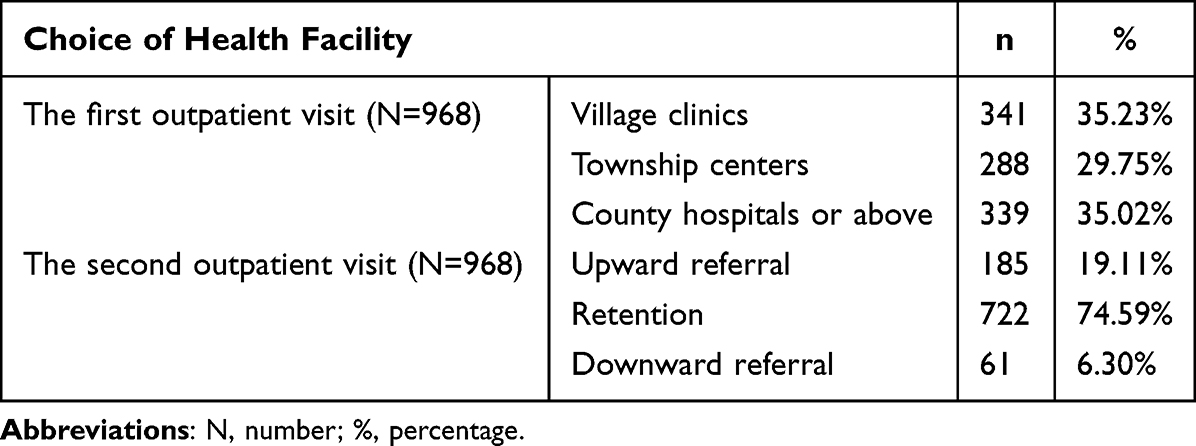 |
Table 3 The First and Second Choice of Health Facility of the Study Sample (N=968) |
Testing the Hypothesis
To validate the hypothetical relationships in the proposed research model, specifically, to determine whether prior quality perception predicted outpatients’ choice of public health facilities via outpatient experience, we followed Baron and Kenny’s procedure. The results are presented in Table 4.
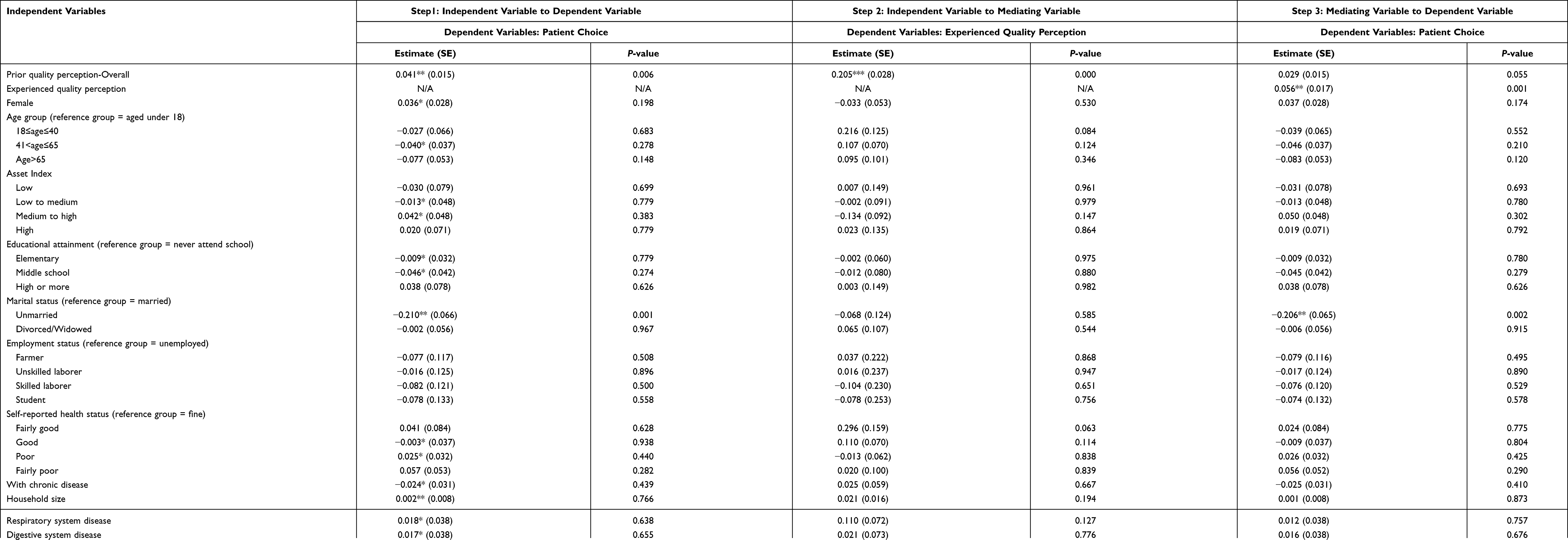 |
Table 4 The Relationships Among the Overall Prior Quality Perception of Outpatient Service, Experienced Quality Perception and the Patient Choice (N=968) |
In the first step, the results indicated that the overall prior quality perception of a health facility was a positive and significant predictor of patients’ retention at the same tier health facility or referral to lower-tier health facilities (β=0.041, P=0.006). In the second step, the results indicated that the prior quality perception of a health facility was positively and significantly associated with the experienced quality perception (β=0.205, P<0.001). In the third step, the results showed that, while the experienced quality perception of a health facility remained a positive and significant predictor of patients’ retention or downward referral (β=0.056, P=0.001), the prior quality perception did not (β=0.029, P=0.055). It was observed in the Sobel test that the experienced quality perception has a strong mediation effect on the relationship between prior quality perception and the choice outcome (z=2.985, P=0.003).
These results consistently suggest that the outpatient experience was likely to be a potential mediator of the effect of prior quality perception on outpatients’ choice outcome.
Mediation Effect of Outpatient Experience
We next disaggregate the effect of prior quality perception on the outpatients’ choice of health facility. The effect of the overall and the seven dimensions of prior quality perceptions was respectively disaggregated, using the KHB method. Table 5 presents the summary of the mediation analysis for the direct and indirect effect of the prior quality perceptions on outpatients’ choice outcome, with experienced quality perception as the mediating variable.
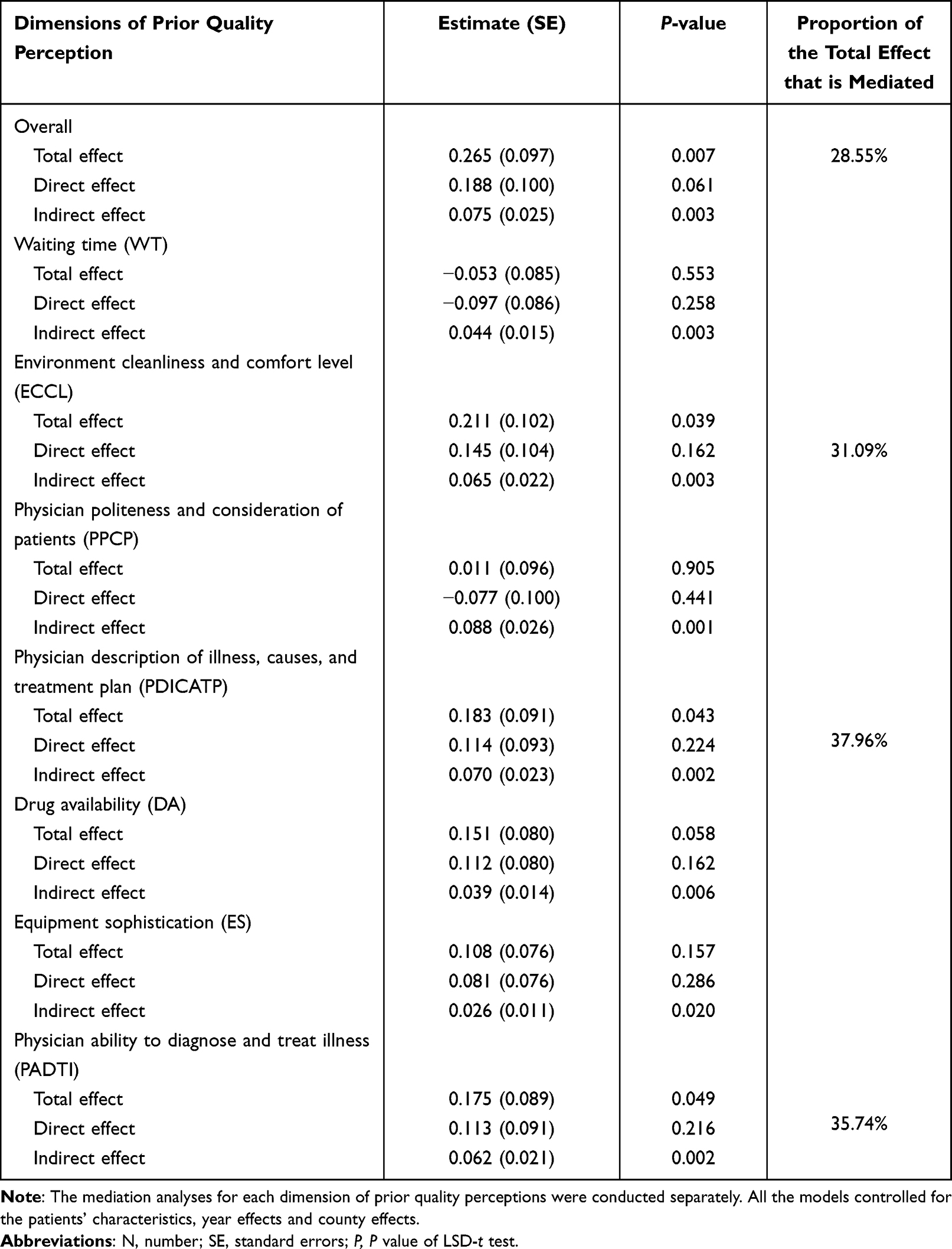 |
Table 5 Summary of Mediation Analysis Results for the Direct and Indirect Effect of Prior Quality Perceptions on Outpatients’ Choice Outcome with Experienced Quality Perception as the Mediating Variable (N=968) |
As shown in Table 5, among the seven dimensions of quality perceptions, only three dimensions- ECCL, PDICATP and PADTI, have positive effect on the outpatients’ choice of retention or downward referral (β=0.211, P=0.039; β=0.183, P=0.043; β=0.175, P=0.049). Furthermore, the above three dimensions’ effect on the outpatients’ choice outcome were fully mediated by the outpatient experience, in that the effect of these three dimensions were no longer significant (β=0.145, P=0.162; β=0.114, P=0.224; β=0.113, P=0.216) with the inclusion of experienced quality perception in the regression model. The KHB mediation analysis confirmed the existence of experienced quality perception as the mediator, the experienced quality perception explained respectively 28.55%, 31.09%, 37.96% and 35.74% of the total effect of the overall perceived quality, ECCL, PDICATP and PADTI.
Discussion
The study demonstrated that quality perception of outpatient service was a determinant of the behavioral intention to use public health facilities. This finding is consistent with some studies that show service quality perception was a predictor of patient choice,5,10 or patient satisfaction of service experience was an antecedent to behavioral intention.35,36 This finding provides the foundation for our subsequent mediation analysis.
We further found that the effect of quality perception on outpatients’ choice outcome was fully mediated by the outpatient experience, which are consistent with studies in other contexts that indicated “satisfaction of service experience” as a good mediating variable between quality perception and behavioral intention.11,37 This finding implies that improved quality perception could drive outpatients to stay at the same level of care or refer downward, but not without producing positive subjective feeling about the outpatient experience. In other words, the practice to improve the quality of primary care should also target the betterment of outpatient experience. If outpatients are satisfied with the quality of care received, they would be more likely to revisit the service provider or refer downward in the future. We speculate that the mediation effects under study should exist through three main mechanisms. Firstly, quality perception would affect the experience, and in return affected by the experience, so the relationship between quality perception and experience is dynamic and interactive. Secondly, the quality measures act on the health care providers could only affect patient behavior through contacting a doctor and having perceptions changed. Thirdly, service experience itself could help patients establish beliefs and attitudes towards health and disease, the beliefs and attitudes would have effect on the choice of provider.
As for the effect of different quality perception dimensions on the choice outcome, the mediation effect was significant for three particular dimensions, including the environment cleanliness and comfort level, the physician description, and the physician ability. These three quality perception dimensions affect the outpatients’ choice outcome positively and significantly, and the effects were also fully mediated by quality perception of outpatient experience. These findings suggest that outpatients cared about the environment, the informative communication, and the competency of physicians when choosing from public health facilities. In order to attract outpatients to seek care at VCs or THCs, policymakers need to implement measures to improve the patients’ appreciation of the environment, the doctor-patient informative communication and the physician’s ability at VCs or THCs. On the other hand, information on processes of care and various other dimensions at different health facilities should be provided to facilitate more appropriate decision making.
Our analysis has a number of limitations. First, the measurement of quality perceptions was based on patient self-report which may have been subject to recall bias, although interviewers were trained in techniques to assist accurate recall to minimize this risk. Second, “prior quality perception of a health facility level” and “experienced quality perception of a particular health facility”, were measured in the same survey and thus caused a measurement error. Third, we applied KHB method rather than traditional regressions to remove the potential mediator-outcome confounding and so as to more precisely disaggregate the direct and indirect effect. Still, the statistical associations found cannot be established as evidence for a causal interpretation under current study design, but as exploratory steps toward causality. Finally, the study was based largely in Ningxia, and heterogeneity across health systems and culture may preclude generalizability to other settings.
Conclusion
This research expands existing literature by providing evidence that outpatients’ quality perceptions significantly predicted their facility-level choice in rural China. And more specifically, positive quality perceptions regarding the health facility environment, doctor-patient communication, and physician ability—could contribute to minimizing upward referral via improvement in outpatient experience. This research also determines the vital role of outpatient experience connecting quality perceptions and the choice of provider.
Therefore, our research has clear implications that strategies should be developed as the health care systems have engaged in active pursuit for patient-centered care and primary care facilities are increasingly dependent on. Firstly, for the public, information on various dimensions of healthcare quality at different health facilities should be provided sufficiently to facilitate more appropriate decision-making. Secondly, for primary care providers, this study emphasized the importance of guaranteeing favorable health care experiences to direct access choices towards primary care facilities. Finally, dynamic understanding of patients’ quality perceptions about healthcare providers would strongly support health care quality management and policy-making.
Funding
This research was funded by National Natural Science Foundation of China (72074049) and National Office for Philosophy and Social Sciences (20ZDA072).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Li C, Chen Z, Khan MM. Bypassing primary care facilities: health-seeking behavior of middle age and older adults in China. Bmc Health Serv Res. 2021;21(1):895. doi:10.1186/s12913-021-06908-0
2. Li L, Fu H. China’s health care system reform: progress and prospects. Int J Health Plann Manage. 2017;32(3):240–253. doi:10.1002/hpm.2424
3. Zhou Z, Zhao Y, Shen C, Lai S, Nawaz R, Gao J. Evaluating the effect of hierarchical medical system on health seeking behavior: a difference-in-differences analysis in China. Soc Sci Med. 2021;268:113372. doi:10.1016/j.socscimed.2020.113372
4. Lin CW, Abdul SS, Clinciu DL, et al. Empowering village doctors and enhancing rural healthcare using cloud computing in a rural area of mainland China. Comput Methods Programs Biomed. 2014;113(2):585–592. doi:10.1016/j.cmpb.2013.10.005
5. Liu Y, Kong Q, Yuan S, van de Klundert J, Ciccozzi M. Factors influencing choice of health system access level in China: a systematic review. PLoS One. 2018;13(8):e0201887. doi:10.1371/journal.pone.0201887
6. World Health Orgnization. Quality in primary health care; 2018. Available from: https://www.who.int/docs/default-source/primary-health-care-conference/quality.pdf.
7. Papp R, Borbas I, Dobos E, et al. Perceptions of quality in primary health care: perspectives of patients and professionals based on focus group discussions. BMC Fam Pract. 2014;15(1):128. doi:10.1186/1471-2296-15-128
8. Sofaer S, Firminger K. Patient perceptions of the quality of health services. Annu Rev Public Health. 2005;26(1):513–559. doi:10.1146/annurev.publhealth.25.050503.153958
9. Khasimah AN, Normila MW. Perceptions of service quality and behavioral intentions: a mediation effect of patient satisfaction in the private health care in Malaysia. Int J Mark Stud. 2013;5(4). doi:10.5539/ijms.v5n4p15
10. Aljaberi MA, Juni MH, Al-Maqtari RA, et al. Relationships among perceived quality of healthcare services, satisfaction and behavioural intentions of international students in Kuala Lumpur, Malaysia: a cross-sectional study. BMJ Open. 2018;8(9). doi:10.1136/bmjopen-2017-021180
11. Goetz K, Jossen M, Rosemann T, Hess S, Brodowski M, Bezzola P, et al. Is patient loyalty associated with quality of care? Results of a patient survey over primary care in Switzerland. Int J Qual Health Care. 2018;31(3):199–204. doi:10.1093/intqhc/mzy142
12. Wu HC, Li T, Li MY. A study of behavioral intentions, patient satisfaction, perceived value, patient trust and experiential quality for medical tourists. J Qual Assur Hosp To. 2016;17(2):114–150. doi:10.1080/1528008x.2015.1042621
13. Ogbeide SA, Landoll RR, Nielsen MK, Kanzler KE. To go or not go: patient preference in seeking specialty mental health versus behavioral consultation within the primary care behavioral health consultation model. Fam Syst Health. 2018;36(4):513–517. doi:10.1037/fsh0000374
14. Nelson KM, Helfrich C, Sun HL, et al. Implementation of the patient-centered medical home in the veterans health administration associations with patient satisfaction, quality of care, staff burnout, and hospital and emergency department use. JAMA Intern Med. 2014;174(8):1350–1358. doi:10.1001/jamainternmed.2014.2488
15. Bockey AJ, Janda A, Braun C, et al. Patient satisfaction & use of health care: a cross-sectional study of asylum seekers in the Freiburg initial reception centre. Bmc Health Serv Res. 2020;20(1). doi:10.1186/s12913-020-05579-7
16. Jaber Hossain M, Islam A. Understanding perceived service quality and satisfaction. Perform Meas Metr. 2012;13(3):169–182. doi:10.1108/14678041211284713
17. Hu L, Ding H, Hu G, Wang Z, Liu S, Liu Y. How perceived quality of care affects outpatient satisfaction in China: a cross-sectional study of 136 tertiary hospitals. Inquiry. 2019;56:46958019895397. doi:10.1177/0046958019895397
18. Hailemeskal MB, Sereda Y, Latypov A, Kiriazova T, Avaliani N. Perceived quality of HIV care and client satisfaction across different service providers in Ukraine. Eur J Public Health. 2020;30(1):23–30. doi:10.1093/eurpub/ckz124
19. Taneja U. Brand image to loyalty through perceived service quality and patient satisfaction: a conceptual framework. Health Serv Manage Res. 2020;951484820962303. doi:10.1177/0951484820962303
20. Chanfreau-Coffinier C, Washington DL, Chuang E, et al. Exploring the association of care fragmentation and patient ratings of care quality: a mediation analysis of women Veterans’ experience with VA care. Health Serv Res. 2019;54(4):816–826. doi:10.1111/1475-6773.13153
21. Naik AD, Catic A. Achieving patient priorities: an alternative to patient-reported outcome measures (PROMs) for promoting patient-centred care. BMJ Qual Saf. 2021;30(2):92–95. doi:10.1136/bmjqs-2020-012244
22. Hocaoglu MB, Hepgul N, Tunnard I, et al. Towards patient-centred cancer care: cross-cultural validity and responsiveness of the Turkish Integrated Palliative care outcome scale. Health Qual Life Out. 2020;18(1). doi:10.1186/s12955-020-01535-5
23. Lee S, Gross SE, Pfaff H, Dresen A. Waiting time, communication quality, and patient satisfaction: an analysis of moderating influences on the relationship between perceived waiting time and the satisfaction of breast cancer patients during their inpatient stay. Patient Educ Couns. 2020;103(4):819–825. doi:10.1016/j.pec.2019.11.018
24. Lee W, Noh Y, Kang H, Hong SH. The mediatory role of medication adherence in improving patients’ medication experience through patient-physician communication among older hypertensive patients. Patient Prefer Adher. 2017;11:1119–1126. doi:10.2147/Ppa.S137263
25. Paddison CAM, Abel GA, Roland MO, Elliott MN, Lyratzopoulos G, Campbell JL. Drivers of overall satisfaction with primary care: evidence from the English General Practice Patient Survey. Health Expect. 2015;18(5):1081–1092. doi:10.1111/hex.12081
26. Rios-Martin MA, Folgado-Fernandez JA, Palos-Sanchez PR, Castejon-Jimenez P. The impact of the environmental quality of online feedback and satisfaction when exploring the critical factors for luxury hotels. Sustainability. 2020;12(1):299.
27. Statistics NHARBo. Ningxia Statistical Yearbook. China Statistical Publishing House; 2010.
28. Chen W, Zhu J. How to improve the efficiency and quality of basic healthcare: design and outcomes of capitation with pay-for-performance payment system reform in Ningxia. Chin J Health Policy. 2014;7(8):14–18. doi:10.3969/j.issn.1674-2982.2014.08.003
29. Anderson JG, Bartkus DE. Choice of medical care: a behavioral model of health and illness behavior. J Health Soc Behav. 1973;14(4):348–362. doi:10.2307/2136779
30. Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: conceptual, strategic, and statistical considerations. J Pers Soc Psychol. 1986;51(6):1173–1182. doi:10.1037//0022-3514.51.6.1173
31. Sobel M. Asymptotic confidence intervals for indirect effects in structural equation models. Sociol Methodol. 1982;13:290. doi:10.2307/270723
32. Karlson KB, Holm A, Breen R. Comparing regression coefficients between same-sample nested models using logit and probit: a new method. Sociol Methodol. 2012;42(1):286–313. doi:10.1177/0081175012444861
33. Christensen VT, Carpiano RM. Social class differences in BMI among Danish women: applying Cockerham’s health lifestyles approach and Bourdieu’s theory of lifestyle. Soc Sci Med. 2014;112:12–21. doi:10.1016/j.socscimed.2014.04.017
34. Mood C. Logistic regression: why we cannot do what we think we can do, and what we can do about it. Eur Sociol Rev. 2009;26(1):67–82. doi:10.1093/esr/jcp006
35. Tsai LY, Liou CF, Huang LH, Huang CY. Correlation between needs satisfaction and behavioral intentions of sexual health care. J Contin Educ Nurs. 2020;51(10):457–464. doi:10.3928/00220124-20200914-07
36. Ali S, Chessex C, Bassett-Gunter R, Grace SL. Patient satisfaction with cardiac rehabilitation: association with utilization, functional capacity, and heart-health behaviors (vol 11, pg 821, 2017). Patient Prefer Adher. 2017;11:1541. doi:10.2147/Ppa.S148901
37. Santouridis I, Trivellas P. Investigating the mediation effect of satisfaction on the service quality and customer loyalty link: empirical evidence from Greek Customers of internet shops. In C Ind Eng Eng Man. 2009;2227–2231. doi:10.1109/Ieem.2009.5373082
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.