")
Back to Journals » Clinical Interventions in Aging » Volume 13
Quality of life and psychological consequences in elderly patients after a hip fracture: a review
Authors Alexiou KI, Roushias A , Varitimidis SE, Malizos KN
Received 26 August 2017
Accepted for publication 28 November 2017
Published 24 January 2018 Volume 2018:13 Pages 143—150
DOI https://doi.org/10.2147/CIA.S150067
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Walker
Konstantinos I Alexiou,1 Andreas Roushias,2 Sokratis E Varitimidis,1 Konstantinos N Malizos1
1Department of Orthopaedic Surgery and Musculoskeletal Trauma, Medical School, University of Thessaly, Larissa, Greece; 2Orthopaedic Department, Apollonion Private Hospital, Nicosia, Cyprus
Abstract: Fractures due to fragility of the bone around the hip joint have become a major public health issue, presenting with an increasing incidence due to the growth of the elderly population. The purpose of this review was to evaluate the impact of hip fractures on the quality of life (QoL), health status (HS), functioning, and psychological parameters, and factors influencing the outcome and the appropriate interventions for improvement of elderly patients. A systematic electronic search of the relevant literature was carried out using the CINAHL, Cochrane, EMBASE, Medline (OvidSP), and PubMed databases spanning the time period from their establishment up to January 2017. Forty-nine randomized controlled trials or prospective cohort studies reporting the QoL and psychological outcomes were assessed by using standardized questionnaires. Patients with a hip fracture who were older than 65 years, were included in the analysis. In the majority of elderly patients, the hip fracture seriously affected physical and mental functioning and exerted a severe impact on their HS and health-related QoL (HRQoL). Moreover, most of the patients did not return to prefracture levels of performance regarding both the parameters. The levels of mental, physical, and nutritional status, prior to the fracture, comorbidity, and female gender, in addition to the postoperative pain, complications, and the length of hospital stay, were the factors associated with the outcome. Psychosocial factors and symptoms of depression could increase pain severity and emotional distress. For the displaced femoral neck fractures, the treatment with total hip arthroplasty or hemiarthroplasty, when compared to the treatment with internal fixation, provided a better functional outcome. Supportive rehabilitation programs, complemented by psychotherapy and nutritional supplementation prior to and after surgery, provided beneficial effects on the HS and the psychosocial dimension of the more debilitated patients’ lives. Lack of consensus concerning the most appropriate HRQoL questionnaires to screen and identify those patients with more difficulties in the psychosocial functions, demonstrates the necessity for further research to assess the newer outcome measurement tools, which might improve our understanding for better care of patients with hip fractures.
Keywords: hip fractures, quality of life, psychological outcomes, elderly, health status
Introduction
Fragility fractures around the hip joint are common serious injuries presenting a substantially increasing incidence along with the growth and aging of the population.1–3 Many fit and active elderly individuals after a hip fracture lose their independent mobility after a hip fracture, whereas the frailer patients may lose their independent living at home. The most frail patients with an already-distressing health status (HS) become further debilitated by pain, loss of mobility, and inability to cater for themselves.4–6 The mortality after the hip fracture in the first 30 days remains high (8%–10%), and in the first year also, it is around 20%–28%, although only one third of that is directly attributable to the fracture itself.7–11
An accidental fall of an older person occurs most commonly at home, sustaining a fracture around the hip joint, either with preexisting medical problems or even without any problems. This is the beginning of a health care journey involving not only many specialists dealing with the problems (eg, surgeons, physicians, and physiotherapists), but also services from the family, the social workers, and carers. Previous frailty and dependency further complicate both the patient’s outcome and the demand for care. Nowadays, hip fractures have become a uniquely challenging global health problem with significant socioeconomic consequences for the patients and their families and health care budgets.12 The financial cost of managing such patients is significantly high, reaching a mean life cost up to £64.000/patient (UK National Report 2013) or up to $8 billion/year in the USA; this is directly proportional to a number of variables, including the length of hospital stay, timing of surgery, availability of specialized orthopedic–geriatric units, and access to rehabilitation after the hospitalization.
An increasing number of studies on hip fractures focus not only on the socioeconomic aspects involved in the management of these patients, but also on the high rates of morbidity and mortality. In addition, these studies consider many other outcome variables, mainly on the special measures needed to improve the physical, mental, emotional functioning and the postoperative social well-being. After the surgical treatment of a hip fracture, patient-reported outcome tools are required in order to assess not only the impact, but also the efficacy of all medical and surgical interventions, on the HS and the health-related quality of life (HRQoL) of the individuals.
The aims of this systematic review were 1) to estimate the impact of a hip fracture on the QoL and the psychological status of the patient; 2) to identify and describe the factors influencing the status of general health and functioning of the patients; and 3) to identify appropriate interventions for improving the overall functioning after a hip fracture in the elderly.
Materials and methods
A systematic literature search through the electronic databases CINAHL, Cochrane, EMBASE, Medline (OvidSP), and PubMed was carried out, using the keywords “hip fracture,” “health status,” “psychological status,” and “health-related quality of life.” All relevant studies conducted up to January 2017 were retrieved, but only 49 studies were fulfilled the inclusion criteria and, thus, were analyzed in this systematic review.
Inclusion criteria
The inclusion criteria were the following: 1) the patients diagnosed with low-energy traumatic pertrochanteric or intertrochanteric fracture of the proximal femur or the femoral neck; 2) studies investigating QoL and psychological outcomes after hip fracture in the elderly (>65 years), managed with or without surgery; 3) the HS and the HRQoL measured with a standardized questionnaire such as the HRQoL, Short Form (SF)-36, SF-12, EuroQol (EQ)-5D, and Barthel; 4) the articles available in full-text format; and 5) the studies published in the English language. Reviews, case reports, abstracts from congresses, comments, editorials, guidelines, letters, protocols, and papers with incomplete data were excluded from the final analysis.
Two authors reviewed the title and abstract of each article, after the literature search. When eligibility was unclear from the title and abstract, the full text of the article was obtained and evaluated. The quality of the methodology for each study was independently assessed by two of the authors (KA and SV), using a list of 17 specific established criteria developed for reviewing QoL studies for systematic reviews.13–18 If there were any disagreements, they were solved by consensus from all the authors. Insufficiently described items were assigned with 0, whereas the ones clearly presented received 1. “High-quality” studies were assigned, which satisfied at least 70% of the criteria received with 1 point, while “low-quality” studies were considered those which satisfied <50% of the criteria and “moderate-quality” studies were those whose total attainable points were between 50% and 70%.15–19 The quality assessment described above was ranked according to Peeters et al’s criteria.20
Data extraction
Two authors (KA and SV) extracted the data by collecting information on the study design and the population enrolled. In addition, they evaluated demographics, follow-up period, outcome measures, and results. Factors affecting the QoL and psychological status of elderly patients after hip fracture and additional interventions, which could improve physical and psychosocial functioning of these patients, were also identified. The outcome measures employed were 1) the reliable and valid 36-Item Short Form Health Survey (SF-36), with its 36 items covering seven health components: the general HS, the physical function, the physical and emotional role limitation, the mental health, the body pain, the vitality, and the social functioning; 2) the EQ-5D with five domains assessing mobility, the ability to self-care and to do usual daily routine activities, assessment of pain and/or discomfort, and anxiety/depression; 3) The Barthel scale/Barthel ADL index: an ordinal scale with ten variables to measure performance and mobility in activities of daily living (ADL). Each performance item on this scale is rated with a given number of points assigned to each level or ranking; and 4) the SF-12, which is a shortened version of the SF-36, including 12 questions and covers eight dimensions: general health, physical functioning, physical role, body pain, vitality, social functioning, emotional role, and mental health.
Results
Study characteristics and methodological quality
According to the quality assessment of all the included studies, based on Peeters et al’s review,20 a moderate mean quality score was 11 (SD =2.1), ranging from 6 to 15. Twenty of the included studies were randomized controlled trials (RCTs), and 29 were prospective cohort studies. The size of the samples analyzed ranged from 61 to 33,152 patients. The age range of the cohorts was 72–84 years, and the length of follow-up ranged from 6 weeks to 4 years. For the assessment of the outcomes, the studies analyzed in this review had used the SF-12 and SF-36 (one study); SF-12 and Barthel (three studies); SF-12 and EQ-5D questionnaire (three studies); SF-36 and Barthel (one study); EQ-5D and Barthel (seven studies); SF-36 and EQ-5D questionnaire (three studies); SF-12, SF-36, and EQ-5D questionnaire (one study); and SF-36, Barthel, and EQ-5D questionnaire (one study).
QoL and psychological status among patients with a hip fracture
There was a unanimous conclusion that, during the first months after a hip fracture, the physical functioning of all the patients was seriously affected, with a subsequent detrimental impact on the HS and the HRQoL, both of which showed an incomplete recovery in the majority of patients. Only four of the studies reported a complete recovery based on the prefracture levels of the HRQoL and the HS.21–24 In particular, Mariconda et al found that the prefracture functional status was regained by 57% of the patients, Hansson et al reported that 29% of the patients regained their previous mobility, while the proportional percentage in Van Balen et al’s study was quoted 18% and Comans et al’s study 11%.21–24 In addition, most of the greatest recovery takes place within the first 6 months as documented by 12 studies,25–36 while some improvement in the physical status is observed up to a year postoperatively. The SF-36 score was used in eleven articles,31,34,36–40,43,44,54,66 the SF-12 score in five articles,29,44,67–69 the EQ-5D score in 21 articles,12,21,22,25,26,28,32,33,38,40,43–45,47,48,53,57–61 and the Barthel index score in 19 articles.21–23,29,38,44,50–53,55–57,60–63,65,67
Factors associated with the HS the HRQoL and functioning:
Femoral neck fractures (FNF)
A number of factors such as comorbidity, female gender, and undernutrition have been found as related to the low physical HS and a low psychosocial functioning of the patient prior to the fracture. They have also been clearly associated with a negative impact on the HRQoL and the HS, after the surgical treatment, and were associated with longer duration of hospital stay, severe postoperative pain perception, and complications.21,22,37–42,46,47,49,51–53 It was shown in seven studies that cognitive dysfunction (eg, dementia) also had a negative impact on the QoL after a hip fracture.39,40,45,48,54–56 The importance of preserving the normal anatomy of the hip as a predictor for HS was demonstrated in a study by Tidermark et al.57 The undisplaced healed FNF type after the surgical treatment with internal fixation (IF) significantly influenced the overall functioning and HRQoL of the patients toward regaining the prefracture levels of HS, when compared to patients with healed displaced FNF after IF.
The surgical treatment options for this subset of patients were compared in four studies53,57–59 (Table 1). Tidermark et al compared the group of patients treated with the total hip arthroplasty (THA), who regained a better HS, to those treated with IF at 4-month (p<0.005) and 1-year (p<0.05) follow-ups. Most of this difference was attributed to the lower complication rate in THA group (4% vs 34% for the IF group).60 The difference in the first year, though, seems to equalize at 2 years postoperatively.
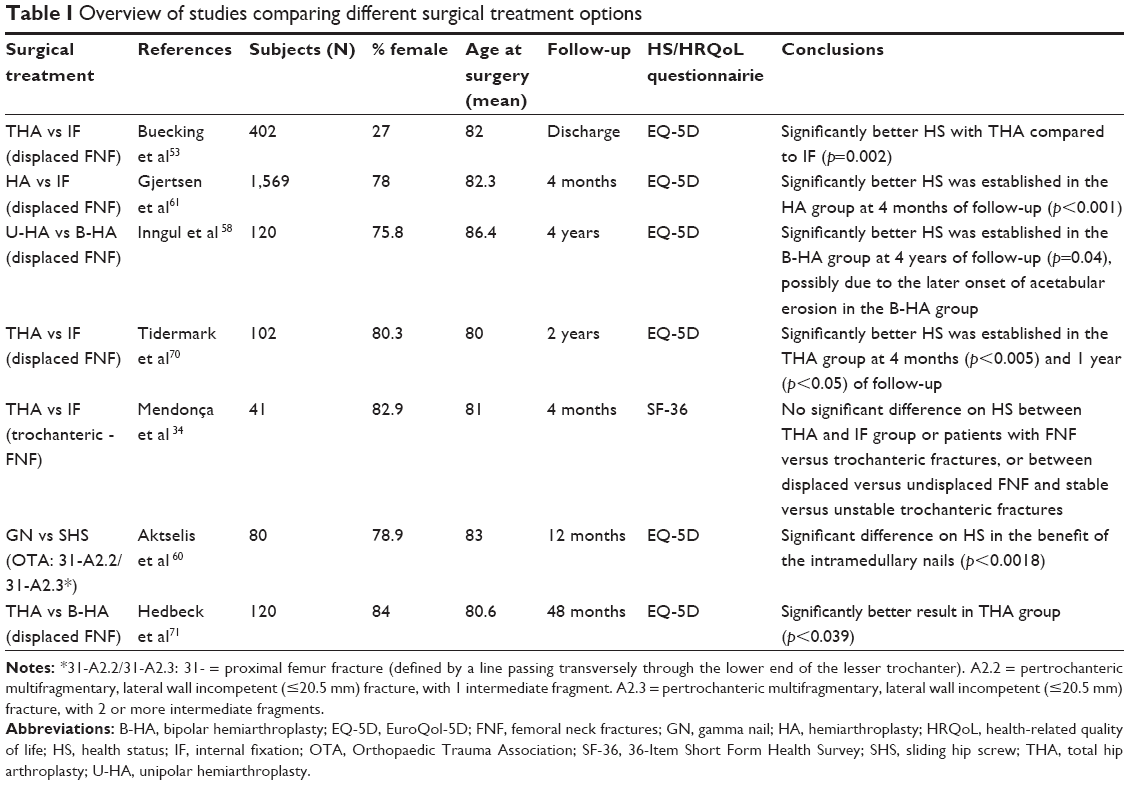 | Table I Overview of studies comparing different surgical treatment options |
Hemiarthroplasty has also been compared with IF and was demonstrated as to be a superior treatment alternative with a significant difference of the HS in two other studies.60,61 However, we could say that these findings are not strictly comparable because they refer to different types of fractures. The studies comparing unipolar with bipolar hemiarthroplasty for the treatment of FNF have shown no significant difference in HRQoL between the two treatment options. Inngul et al58 showed that the bipolar hemiarthroplasties result in better HRQoL 2 years after surgery as compared to the unipolar ones. Another study has focused on comparing hemiarthroplasty with THA and demonstrated significantly better HRQoL in the THA group after 2 years follow-up, suggesting THA as the preferred treatment for the displaced FNF in all active elderly patients.59
Pertrochanteric hip fractures
The types of IF methods, ie, intramedullary gamma nails and sliding hip screws in the management of pertrochanteric hip fractures, were compared by Aktselis et al. The authors demonstrated a significant difference in HS after fixation with the intramedullary gamma nails (p<0.0018).60 Mendonça et al,34 utilizing the SF-36 scores for all the scales, reported no significant difference when comparing the outcomes between the patients with stable versus unstable trochanteric fractures, femoral neck versus trochanteric fractures, or displaced versus undisplaced FNF.
Interventions for improving the overall functioning after a hip fracture
Supportive rehabilitation programs and HS/HRQoL
Hip fracture patients’ care in specifically organized geriatric units has been investigated by Prestmo et al38 and Taraldsen et al,25 who found it less costly and more effective than that in orthopedic care units. Patients treated with comprehensive geriatric care during hospitalization had improved physical behavior and independent living as compared to those treated with the orthopedic care. Significant emphasis has been placed on the rehabilitation, counseling, and supportive programs for home care. In six RCTs and in three cohort studies, the authors reported significant improvements in most measured components of HS and HRQoL when supportive programs were already applied prior to discharge and were subsequently continued as home rehabilitation programs.25,29,38,62–65,67,69 For the community-dwelling older adults with a hip fracture, Zidén et al62,63 suggest the initiation of “home rehabilitation” programs in the early phase, prior to discharge, and focusing on the enhancement of self-efficacy and training for daily activities. They showed improved balance, confidence, physical activity, and a significantly higher degree of independence at 1-year postdischarge. Hagsten et al35 also indicated that the individualized occupational training improved the ability to perform independent ADL and appeared to speed up the recovery. Muscle strength training has also been tested by Sylliaas et al67,69 with a 12-week progressive program which included four exercises performed at 80% of maximum capacity. Measurements taken with the SF-12, the Nottingham Extended ADL (NEADL) scale, and the Berg Balance Scale; the sit-to-stand test; timed up-and-go test; maximal gait speed; and 6-minute walk test after 12 weeks of intervention seemed to improve strength and endurance at 1-year postdischarge and resulted in better self-reported NEADL and self-rated HS after a hip fracture.
Psychological counseling and HS/HRQoL
A number of studies39,45,48,54,56 reported that psychosocial factors and symptoms of depression could increase the severity of pain and the emotional distress of the patients. Early, upon admission, the identification of a patient and application of counseling throughout the perioperative and postoperative courses could improve the patients’ pain perception and their overall HS, particularly for those patients who receive a low score on the SF-36 evaluation scale. Most importantly, Liu et al43 reported that when a family caregiver’s mental health was “poor,” the patient recovering after a hip fracture surgery was more likely to reach a poor outcome.
Nutritional status and HS/HRQoL
The nutritional status of hip fracture patients has also been investigated in a study by Hoekstra et al28 who compared hip fracture patients with a control group of patients who received multidisciplinary nutritional care and, after 3 months, demonstrated a significant reduction in EQ-5D index scores among the hip fracture patients compared with the control group (p=0.004). At 3 months, significantly fewer patients in the intervention group were classified as malnourished or at a risk of malnutrition, indicating an improvement in their HRQoL.
Discussion
It is generally accepted that hip fractures in elderly population have a detrimental effect on all aspects of their life. In this systematic review, the collected studies investigated the impact of a hip fracture on elderly patient’s (>65 years old) HS and examined factors positively or negatively influencing the HRQoL. The outcome measurement scores most commonly employed were the EQ-5D, followed by SF-36, Barthel index, and SF-12. All the above outcome measurement tools do not give a clear HS score, but rather serve as an indication of the physical, emotional, and social functioning of the patient and not the patients’ internal experiences.
A hip fracture in an elderly patient does not only affect mobility over a period of several months but also, most importantly, results in high mortality within the first few months and the first year. For all fracture types – independently of the country where the study was conducted – the QoL was reduced significantly after the fracture compared with that of the prefracture status. A number of variables, including the physical and psychosocial functioning of the patient prior to the fracture, the psychological state, multiple comorbidities including psychiatric conditions, female gender, malnutrition, unstable extracapsular fractures, postoperative pain, increased length of hospital stay, and postoperative complications, have a negative effect on the outcome, namely deteriorating a patient’s general HS and functioning and, finally, leading to mortality. When examining the QoL between different countries, significant differences in the QoL after a hip fracture were found, indirectly and partially reflecting to a certain degree the effect of socioeconomic conditions and the health care services in each country on the outcome.
The methodological quality of most studies was moderate. In a number of studies, the follow-up was too short (4–6 months), considering that the time period is inadequate for most patients to achieve a complete recovery. Inevitably, the higher rate of mortalities, mainly for those with the lowest scores at baseline, involved the patients who died in the early period after the hip fracture, and thus, they were not included in the study. In most series, these patients die prior to discharge from the hospital and they are not included in the analysis for the HRQoL, providing thus a more favorable outcome.
The interpretation of the findings of this review should be understood within the context that aging is a risk factor for most chronic disease conditions with a range of comorbidities and their consequences and gradual decline in the physical capacity and function in many aspects. This is definitely influencing the results in particular when the follow-up is longer. Understanding the mechanisms of aging in this particular population with fragility-related hip fractures further improves the outcome of this condition and may lead to most appropriate interventions.
Conclusion
A hip fracture in an elderly patient exerts a severe impact on the physical, mental, and psychosocial aspects of a patient’s life, and it is detrimental for his/her QoL. The recovery of the general HS to the prefracture levels experienced before the fracture is lengthy, and a relatively high number of patients do not manage to reach those levels or even survive. Optimizing nutritional status and the general HS prior to and after surgery, and as well as applying supportive rehabilitation programs both at the specializing facilities and at home, is recommended after surgery for the improvement in patient’s general health and the overall functioning. Currently, there is no consensus for as to which the HRQoL questionnaires should be employed to screen and identify patients with psychosocial difficulties in the psychosocial dimensions. Some studies advise providing them an adjusted psychological counseling during the hospital stay and afterwards, when it is necessary. It is the authors’ impression that, besides HS questionnaires, further research is required to improve and assess outcome measurements, which might be able to obtain better insights into the subjective experiences of the patient’s psychological status and his/her perception on the quality of living life. This may lead to an improved comprehensive management algorithm for the treatment of patients with hip fractures.
Disclosure
The authors report no conflicts of interest in this work.
References
Bergstrom U, Johnson H, Gustafson Y, Pettersson U, Stenlund H, Svensson O. The hip fracture incidence curve is shifting to the right. Acta Orthop. 2009;80(5):520–524. | ||
Cooper C, Campion G, Melton LJ 3rd. Hip fractures in the elderly: a worldwide projection. Osteoporos Int. 1992;2(6):285–289. | ||
Schurch MA, Rizzoli R, Mermillod B, Vasey H, Michel JP, Bonjour JP. A prospective study on socioeconomic aspects of fracture of the proximal femur. J Bone Miner Res. 1996;11(12):1935–1942. | ||
Hallberg I, Rosenqvist AM, Kartous L, Lofman O, Wahlstrom O, Toss G. Health-related quality of life after osteoporotic fractures. Osteoporos Int. 2004;15(10):834–841. | ||
Pande I, Scott DL, O’neill TW, Pritchard C, Woolf AD, Davis MJ. Quality of life, morbidity, and mortality after low trauma hip fracture in men. Ann Rheum Dis. 2006;65(1):87–92. | ||
Peterson MG, Allegrante JP, Cornell CN, et al. Measuring recovery after a hip fracture using the SF-36 and Cummings scales. Osteoporos Int. 2002;13(4):296–302. | ||
Johnell O, Kanis JA. An estimate of the worldwide prevalence, mortality and disability associated with hip fracture. Osteoporos Int. 2004;15(11):897–902. | ||
Keene GS, Parker MJ, Pryor GA. Mortality and morbidity after hip fractures. BMJ. 1993;307(6914):1248–1250. | ||
Vestergaard P, Rejnmark L, Mosekilde L. Increased mortality in patients with a hip fracture-effect of pre-morbid conditions and post-fracture complications. Osteoporos Int. 2007;18(12):1583–1593. | ||
Valizadeh M, Mazloomzadeh S, Golmohammadi S, Larijani B. Mortality after low trauma hip fracture: a prospective cohort study. BMC Musculoskelet Disord. 2012;13:143. | ||
Leibson CL, Tosteson AN, Gabriel SE, Ransom JE, Melton LJ. Mortality, disability, and nursing home use for persons with and without hip fracture: a population-based study. J Am Geriatr Soc. 2002;50(10):1644–1650. | ||
Marques A, Lourenço O, da Silva JA; Portuguese Working Group for the Study of the Burden of Hip Fractures in Portugal. The burden of osteoporotic hip fractures in Portugal: costs, health related quality of life and mortality. Osteoporos Int. 2015;26(11):2623–2630. | ||
Gill TM, Feinstein AR. A critical appraisal of the quality of quality-of-life measurements. JAMA. 1994;272(8):619–626. | ||
Den Oudsten BL, Van Heck GL, De Vries J. Quality of life and related concepts in Parkinson’s disease: a systematic review. Mov Disord. 2007;22(11):1528–1537. | ||
Mols F, Vingerhoets AJ, Coebergh JW, van de Poll-Franse LV. Quality of life among long-term breast cancer survivors: a systematic review. Eur J Cancer. 2005;41(17):2613–2619. | ||
Scholten-Peeters GG, Verhagen AP, Bekkering GE, et al. Prognostic factors of whiplash-associated disorders: a systematic review of prospective cohort studies. Pain. 2003;104(1–2):303–322. | ||
Moons P, Van Deyk K, Budts W, De Geest S. Caliber of quality-of-life assess-ments in congenital heart disease: a plea for more conceptual and methodological rigor. Arch Pediatr Adolesc Med. 2004;158(11):1062–1069. | ||
Kuijpers T, van der Windt DA, van der Heijden GJ, Bouter LM. Systematic review of prognostic cohort studies on shoulder disorders. Pain. 2004;109(3):420–431. | ||
Ariens GA, van Mechelen W, Bongers PM, Bouter LM, van der Wal G. Physical risk factors for neck pain. Scand J Work Environ Health. 2000;26(1):7–19. | ||
Peeters CM, Visser E, van de Ree CL, Gosens T, Den Oudsten BL, De Vries J. Quality of life after hip fracture in the elderly: a systematic literature review. Injury. 2016;47(7):1369–1382. | ||
Mariconda M, Costa GG, Cerbasi S, et al. Factors predicting mobility and the change in activities of daily living after hip fracture: a 1-year prospective cohort study. J Orthop Trauma. 2016;30(20):71–77. | ||
Hansson S, Rolfson O, Akesson K, Nemes S, Leonardsson O, Rogmark C. Complications and patient-reported outcome after hip fracture. A consecutive annual cohort study of 664 patients. Injury. 2015;46(11):2206–2211. | ||
Van Balen R, Essink-Bot ML, Steyerberg E, Cools H, Habbema DF. Quality of life after hip fracture: a comparison of four health status measures in 208 patients. Disabil Rehabil. 2003;25(10):507–519. | ||
Comans TA, Peel NM, Gray LC, Scuffham PA. Quality of life of older frail persons receiving a post-discharge program. Health Qual Life Outcomes. 2013;11:58. | ||
Taraldsen K, Thingstad P, Sletvold O, et al. The long-term effect of being treated in a geriatric ward compared to an orthopaedic ward on six measures of free-living physical behavior 4 and 12 months after a hip fracture – a randomized controlled trial. BMC Geriatr. 2015;15:160. | ||
Griffin XL, Parsons N, Achten J, Fernandez M, Costa ML. Recovery of health-related quality of life in a United Kingdom hip fracture population. The Warwick Hip Trauma Evaluation–a prospective cohort study. Bone Joint J. 2015;97-B(3):372–382. | ||
Tarride JE, Burke N, Leslie WD, et al. Loss of health related quality of life following low-trauma fractures in the elderly. BMC Geriatr. 2016;16:84. | ||
Hoekstra JC, Goosen JH, de Wolf GS, Verheyen CC. Effectiveness of multidisciplinary nutritional care on nutritional intake, nutritional status and quality of life in patients with hip fractures: a controlled prospective cohort study. Clin Nutr. 2011;30(4):455–461. | ||
Sylliaas H, Thingstad P, Wyller TB, Helbostad J, Sletvold O, Bergland A. Prognostic factors for self-rated function and perceived health in patient living at home three months after a hip fracture. Disabil Rehabil. 2012;34(140):1225–1231. | ||
Tidermark J, Zethraeus N, Svensson O, Tonkvist H, Ponzer S. Femoral neck fractures in the elderly: functional outcome and quality of life according to EuroQol. Qual Life Res. 2002;11(5):473–481. | ||
Peterson MG, Allegrante JP, Cornell CN, et al. Measuring recovery after a hip fracture using the SF-36 and Cummings scales. Osteoporos Int. 2002;13(4):296–302. | ||
Ekström W, Miedel R, Ponzer S, Hedstrom M, Samnegard E, Tidermark J. Quality of life after a stable trochanteric fracture – a prospective cohort study on 148 patients. J Orthop Trauma. 2009;23(1):39–44. | ||
Ekström W, Nemeth G, Samnegard E, Dalen N, Tidermark J. Quality of life after a subtrochanteric fracture: a prospective cohort study on 87 elderly patients. Injury. 2009;40(4):371–376. | ||
Mendonça TM, Silva CH, Canto RS, Morales NM, Pinto RM, Morales RR. Evaluation of the health-related quality of life in elderly patients according to the type of hip fracture: femoral neck or trochanteric. Clinics (Sao Paulo). 2008;63(5):607–612. | ||
Hagsten B, Svensson O, Gardulf A. Health-related quality of life and self-reported ability concerning ADL and IADL after hip fracture: a randomized trial. Acta Orthop. 2006;77(1):114–119. | ||
Shyu Y, Chen MC, Liang J, Lu JF, Wu CC, Su JY. Changes in quality of life among elderly patients with hip fracture in Taiwan. Osteoporos Int. 2004;15(2):95–102. | ||
Rohde G, Haugeberg G, Mengshoel AM, Moum T, Wahl AK. Two-year changes in quality of life in elderly patients with low-energy hip fracture. A case-control study. BMC Musculoskelet Disord. 2010;11:226. | ||
Prestmo A, Hagen G, Sletvold O, et al. Comprehensive geriatric care for patients with hip fractures: a prospective, randomized, controlled trial. Lancet. 2015;385(9978):1623–1633. | ||
Romeo R, Knapp M, Banerjee S, et al. Treatment and prevention of depression after surgery for hip fracture in older people: cost-effectiveness analysis. J Affect Disord. 2011;128(3):211–219. | ||
Borgström F, Lekander I, Ivergård M, et al. The International Costs and Utilities Related to Osteoporotic Fractures Study (ICUROS) – quality of life during the first 4 months after fracture. Osteoporos Int. 2013;24:811–823. | ||
Crotty M, Unroe K, Cameron ID, Miller M, Ramirez G, Couzner L. Rehabilitation interventions for improving physical and psychosocial functioning after hip fracture in older people. Cochrane Database Syst Rev. 2010;(1):CD007624. | ||
Smith TO, Hameed YA, Cross JL, Henderson C, Sahota O, Fox C. Enhanced rehabilitation and care models for adults with dementia following hip fracture surgery. Cochrane Database Syst Rev. 2015;(6):CD010569. | ||
Liu HY, Yang CT, Cheng HS, Wu CC, Chen CY, Shyu YI. Family caregivers’ mental health is associated with postoperative recovery of elderly patients with hip fracture: a sample in Taiwan. J Psychosom Res. 2015;78(5):452–458. | ||
Orive M, Aguirre U, Garcia-Gutierrez S, et al. Changes in health-related quality of life and activities of daily living after hip fracture because of a fall in elderly patients: a prospective cohort study. Int J Clin Pract. 2015;69(4):491–500. | ||
Daniels AH, Daiello LA, Lareau CR, et al. Preoperative cognitive impairment and psychological distress in hospitalized elderly hip fracture patients. Am J Orthop (Belle Mead NJ). 2014;43(7):E146–E152. | ||
Oh ES, Li M, Fafowora TM, et al. Preoperative risk factors for postoperative delirium following hip fracture repair: a systematic review. Int J Geriatr Psychiatry. 2015;30(9):900–910. | ||
Gjertsen JE, Baste V, Fevang JM, Furnes O, Engesæter LB. Quality of life following hip fractures: results from the Norwegian hip fracture register. BMC Musculoskelet Disord. 2016;17:265. | ||
Cristancho P, Lenze EJ, Avidan MS, Rawson KS. Trajectories of depressive symptoms after hip fracture. Psychol Med. 2016;46(7):1413–1425. | ||
Si L, Winzenberg TM, de Graaff B, Palmer AJ. A systematic review and meta-analysis of utility-based quality of life for osteoporosis-related conditions. Osteoporos Int. 2014;25(8):1987–1997. | ||
Dyer SM, Crotty M, Fairhall N, et al. A critical review of the long-term disability outcomes following hip fracture. BMC Geriatr. 2016;16:158. | ||
Walters S, Khan T, Ong T, Sahota O. Fracture liaison services: improving outcomes for patients with osteoporosis. Clin Interv Aging. 2017;12:117–127. | ||
Roth T, Kammerlander C, Gosch M, Luger TJ, Blauth M. Outcome in geriatric fracture patients and how it can be improved. Osteoporos Int. 2010;21(Suppl 4):S615–S619. | ||
Buecking B, Struewer J, Waldermann A, et al. What determines health-related quality of life in hip fracture patients at the end of acute care? – a prospective observational study. Osteoporos Int. 2014;25(2):475–484. | ||
Gambatesa M, D’Ambrosio A, D’Antini D, et al. Counseling, quality of life, and acute postoperative pain in elderly patients with hip fracture. J Multidiscip Healthc. 2013;6:335–346. | ||
Samuelsson B, Hedstrom MI, Ponzer S, et al. Gender differences and cognitive aspects on functional outcome after hip fracture – a 2 years’ follow-up of 2,134 patients. Age Ageing. 2009;38(6):686–692. | ||
Givens JL, Sanft TB, Marcantonio ER. Functional recovery after hip fracture: the combined effects of depressive symptoms, cognitive impairment, and delirium. J Am Geriatr Soc. 2008;56(6):1075–1079. | ||
Tidermark J, Zethraeus N, Svensson O, Tornkvist H, Ponzer S. Quality of life related to fracture displacement among elderly patients with femoral neck fractures treated with internal fixation. J Orthop Trauma. 2002;16(1):34–38. | ||
Inngul C, Hedbeck CJ, Blomfeldt R, Lapidus G, Ponzer S, Enocson A. Unipolar hemiarthroplasty versus bipolar hemiarthroplasty in patients with displaced femoral neck fractures: a four-year follow-up of a randomised controlled trial. Int Orthop. 2013;37(12):2457–2464. | ||
Beaupre LA, Jones CA, Johnston DW, Wilson DM, Majumdar SR. Recovery of function following a hip fracture in geriatric ambulatory persons living in nursing homes: prospective cohort study. J Am Geriatr Soc. 2012;60(7):1268–1273. | ||
Aktselis I, Kokoroghiannis C, Fragkomichalos E, et al. Prospective randomised controlled trial of an intramedullary nail versus a sliding hip screw for intertrochanteric fractures of the femur. Int Orthop. 2014;38(1):155–161. | ||
Gjertsen JE, Vinje T, Lie SA, et al. Patient satisfaction, pain, and quality of life 4 months after displaced femoral neck fractures: a comparison of 663 fractures treated with internal fixation and 906 with bipolar hemiarthroplasty reported to the Norwegian Hip Fracture Register. Acta Orthop. 2008;79(5):594–601. | ||
Zidén L, Frandin K, Kreuter M. Home rehabilitation after hip fracture. A randomized controlled study on balance confidence, physical function and everyday activities. Clin Rehabil. 2008;22(12):1019–1033. | ||
Zidén L, Kreuter M, Frändin K. Long-term effects of home rehabilitation after hip fracture – 1-year follow-up of functioning, balance confidence, and health-related quality of life in elderly people. Disabil Rehabil. 2010;32(1):18–32. | ||
Hawley S, Javaid MK, Prieto-Alhambra D, et al. Clinical effectiveness of orthogeriatric and fracture liaison service models of care for hip fracture patients: population-based longitudinal study. Age Ageing. 2016;45(2):236–242. | ||
Beaupre LA, Cinats JG, Senthilselvan A, Scharfenberger A, Johnston DW, Saunders LD. Does standardized rehabilitation and discharge planning improve functional recovery in elderly patients with hip fracture? Arch Phys Med Rehabil. 2005;86(12):2231–2239. | ||
Shyu YI, Chen ML, Chen MC, Wu CC, Su YJ. Postoperative pain and its impact on quality of life for hip-fractured older people over 12 months after hospital discharge. J Clin Nurs. 2009;18(5):755–764. | ||
Sylliaas H, Brovold T, Wyller TB, Bergland A. Prolonged strength training in older patients after hip fracture: a randomised controlled trial. Age Ageing. 2012;41(2):206–212. | ||
Moerman S, Vochteloo AJ, Tuinebreijer WE, Maier AB, Mathijssen NM, Nelissen RG. Factors associated with the course of health-related quality of life after a hip fracture. Arch Orthop Trauma Surg. 2016;136(7):935–943. | ||
Sylliaas H, Brovold T, Wyller TB, Bergland A. Progressive strength training in older patients after hip fracture: a randomised controlled trial. Age Ageing. 2011;40(2):221–227. | ||
Tidermark J, Ponzer S, Svensson O, Söderqvist A, Törnkvist H. Internal fixation compared with total hip replacement for displaced femoral neck fractures in the elderly. A randomised, controlled trial. J Bone Joint Surg Br. 2003;85(3):380–388. | ||
Hedbeck CJ, Enocson A, Lapidus G, et al. Comparison of bipolar hemiarthroplasty with total hip arthroplasty for displaced femoral neck fractures: a concise four-year follow-up of a randomized trial. J Bone Joint Surg Am. 2011;93(5):445–450. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.