Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Qualitative Focus Group Study Examining Perceptions of the Community’s Important Health Issues, Health Care Needs and Perceived Barriers to Access Among Arabic Speaking Primary Care Clients in the State of Qatar
Authors Al-Kuwari MG ![]() , Al Abdulla S
, Al Abdulla S ![]() , Abdulla M, Mohammed AM
, Abdulla M, Mohammed AM ![]() , Haj Bakri A
, Haj Bakri A ![]() , Shaikhan F, Buhaddoud H
, Shaikhan F, Buhaddoud H
Received 22 October 2020
Accepted for publication 21 December 2020
Published 28 April 2021 Volume 2021:14 Pages 961—971
DOI https://doi.org/10.2147/JMDH.S288194
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mohamed Ghaith Al-Kuwari,1 Samya Al Abdulla,2 Maha Abdulla,1 Azza Mustafa Mohammed,1 Ahmad Haj Bakri,1 Fahad Shaikhan,3 Hanan Buhaddoud1
1Strategy Planning and Health Intelligence, Primary Health Care Corporation, Doha, Qatar; 2Operations, Primary Health Care Corporation, Doha, Qatar; 3Preventative Health – Health Protection, Primary Health Care Corporation, Doha, Qatar
Correspondence: Azza Mustafa Mohammed Tel +974 40270065
Email [email protected]
Objective: This study is a part of the Primary Health Care Corporation’s (PHCC) Health Needs Assessment (HNA) Initiative. It focuses on identifying perceptions of Arabic speaking primary care clients regarding community’s major health issues, their experiences in utilizing health services, and the barriers that limit their access to health care in the State of Qatar.
Study Setting and Design: A total of 10 focus groups sessions were conducted at different PHCC’s health centers between October of 2019 and March of 2020. Sessions were distributed to cover all PHCC’s three geographical regions. Data were analyzed using thematic analysis.
Participants: A total of 89 adult Arabic speaking individuals were recruited. Participants included were in the age groups (18– 69), native Arabic speaker, and registered at one of the PHCC’s health centers with a valid health card at time of recruitment.
Results: Areas investigated included perceptions of the community’s health issues, needed health services, and perceived barriers to health care. Priority health issues identified were chronic non-communicable diseases, mental health, timely access to care, cultural competency of delivered services, and integration and coordination across health care settings and sectors. Participants were able to identify socioeconomic and environmental factors such as the need for health and wellness interventions at schools that affects the health of the individual and the community. The importance of raising the community’s awareness about health-related issues and availability of health services was highlighted by study participants.
Conclusion: Collecting qualitative data provides an opportunity to examine people’s perceptions, and motivations and engage the whole community. This process is very important for strategic planning of health services. The study attempts to fill the knowledge gap and should be linked to health policy and the development of socially and culturally appropriate health programs.
Keywords: primary care, qualitative research, PHCC, health needs assessment, Qatar
Introduction
The state of Qatar is a peninsula located along the coast of the Arabian gulf1 with a total population of 2,666,938, as of August 2019.1,2 Qatar has a dynamic population that includes 94 different nationalities.3 Qatari citizens account for around 10.5% of the total population.2,3 Although the English language is widely used, Arabic is the official language of the country.1
Qatar has experienced significant economic and demographic growth over the past years.4 The population growth, recent industrialization and lifestyle shift have led to changes in health care demands.4 To meet these challenges, the country worked on advancing health care system and increased health care spending per capita to become among the highest in the Middle East.4,5 Health services are accessible to Qatar’s entire population with full “Coverage of preventive and curative health care, both physical and mental, taking into account the differing needs of men, women and children”.6,7
The Primary Health Care Corporation (PHCC) is the public primary care provider in the State of Qatar. The PHCC provides a wide range of preventative and curative services through 27 health centers distributed across the three regions of the country. In 2018, the PHCC started gradual implementation of the Family Medicine model of care, and all patients were automatically assigned to a named family doctor supported by a multidisciplinary team along with integrated electronic medical records of all patients.8 Moreover, it is committed to developing and providing patient centered care where patients, families and communities are considered equal partners and they are actively engaged in the design of health services.7
This study is a part of the PHCC’s Community Health Needs Assessment (HNA) Initiative to provide reliable data on the prevalence, and modifiable risk factors of Non-Communicable Diseases (NCDs) among primary care patients.2 This project is the first health needs assessment conducted by the PHCC. In addition, it is the first to combine quantitative and qualitative methods to examine important health issues at the primary care level. In 2012, the Ministry of Public Health conducted the WHO STEPS survey to establish a comprehensive epidemiological profile of the population on the national level.9 However, to the best of our knowledge, there is no existing studies that examined patients’ experiences and their awareness of priority health issues at the primary care level in Qatar.
Our study’s purpose is to collect in depth qualitative data through focus groups discussions. The gathered information will give complementary insights into primary care clients’ perception of important community health issues, their experiences and expectations of health services, and their perceived barriers to healthcare access. The findings will help in bridging the knowledge gap, developing socially and culturally appropriate health improvement plans and creating programs that are most relevant to patients.10 Not to mention that participatory needs assessment in local communities using focus groups generates a sense of ownership and creates a partnership which improves the trust between the community and health care providers.11,12
Objectives
- Describe study participants perceptions of the most important community health issues and concerns.
- Determine the perceptions of primary care clients of unmet health care needs.
- Identify contributing factors that impact primary care client’s access to health services.
Methods
Study Design
The number of focus groups was guided by theme saturation and the “criterion of informational redundancy”.9 We planned 10 focus groups to be conducted in two cycles. Each cycle included 5 focus groups each of them covered a different demographic group. It was agreed that after the completion of the two cycles the study team will evaluate the data collected and decide if more focus group sessions are needed. However, after conducting 10 focus group sessions with a total of 89 participants, it was decided that data saturation has been reached and information collected became repetitive as no new themes were emerging.
Designing the focus groups to target different demographic groups helped us to achieve across group theme saturation and conducting 2 sessions for each demographic group was essential to ensure within group theme saturation.
Demographic groups covered were (female, male, population aged (18–34) years old, population aged ≥35 years old).
The design of the focus groups followed a structured format where specific interview open-ended questions were asked at each group. This format was used to make certain that all important topics were covered in all groups, not to mention that it helped us in comparing information between groups to ensure thematic saturation.
Study Setting
The focus groups were conducted at the PHCC’s Health centers as it is familiar to participant populations. Focus groups sites were selected based on recommendations from regional directors of the operations’ team at PHCC and the choice was determined based on the size of the center and type of population it serves. Sessions were distributed to cover all PHCC three geographical regions with three sessions conducted in the central region, three in the Northern region, and four in the Western Region (Table 1).
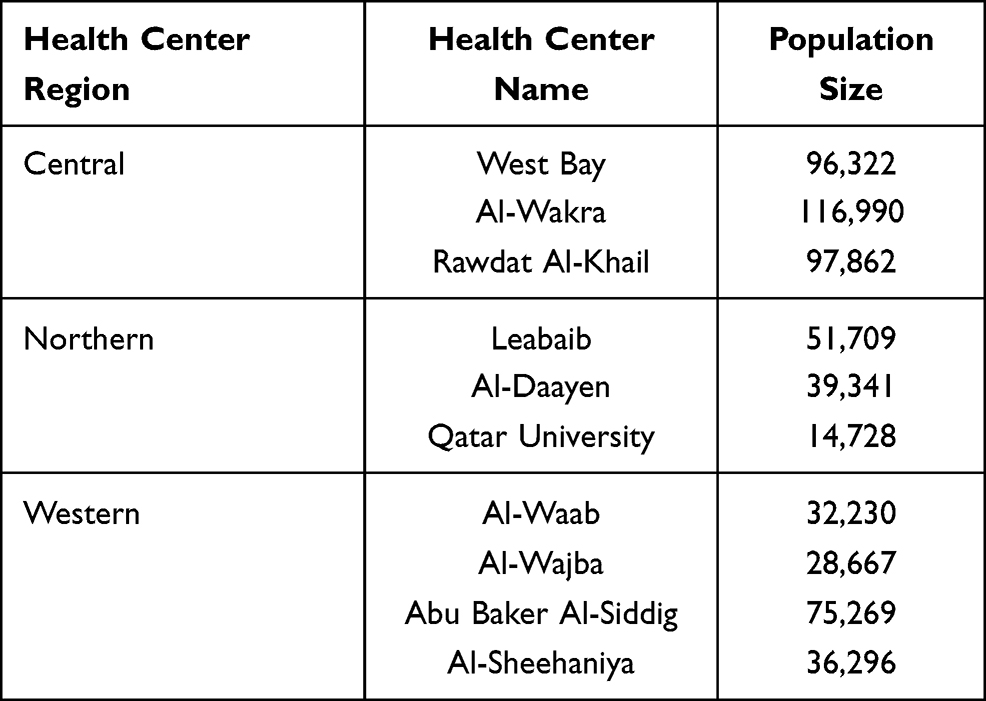 |
Table 1 Health Centers at Which Focus Groups Were Held and the Size of Population It Serves |
Group Structure and Facilitation
Each focus group lasted for approximately 2 hours which is a significant time frame that allowed in depth discussions. The focus groups sessions were facilitated by trained Arabic speaking moderates to ensure that the questions will be delivered in a unified and clear language to reduce chances of questions’ misinterpretation by the participants. A facilitator guide was developed by the study team, and the moderators were trained based on it. A script was developed for the moderators to guide and unify the discussion. They used the script along with a presentation that explained the purpose of the focus group, went over the focus group rules, and reinforced the confidentiality of all the information shared.
Study Population
All participants were recruited by health centers’ staff. They were selected to participate if they met inclusion and exclusion criteria. The selected focus groups sites were contacted and asked to provide a list of potential participants. The list was extracted from the electronic system. In addition, we emphasized diversity in nationality, and family composition in recruitment. The list of participants suggested by the health center staff were then screened for eligibility by the study team. Recruitment staff at health centers made direct phone calls to potential participants. And, official invitations were sent via emails to those expressed interest in attending.
Inclusion Criteria
- Age groups of (18–69).
- Self-identified as Arabic-speaking, and Arabic is their first language.
- Have a valid health card and is registered at one of the PHCC health centers, preferring participants that have accessed PHCC health centers in the last 12 months.
Exclusion Criteria
- Do not fit in the age cohort (≥70).
- Did not access PHCC health centers for more than 3 years prior to the study date.
- Arabic is not their first language. This is important to reduce bias due to questions misunderstanding or misinterpretation.
Sample
Convenience sampling was used as the sampling methods. In addition, we used purposeful sampling and identified participants based on recommendations from health centers’ staff. The middle east is a conservative region, part of the cultural norms is that people can be hesitant about asking questions, commenting on or challenging other participants’ points of views as it might be perceived as a sign of impoliteness,13 that posed a challenge for recruiting people to the sessions. We wanted to make sure that at least some of the participants will have the ability to communicate their health experiences and opinions in an articulate, and reflective manner.14 It was agreed that each session should have a maximum of 3 information rich cases to control for researcher bias. The “information rich cases” were identified by health centers staff through the help of local community leaders.
Consent
The study was part of health Needs Assessment project that was approved by the Managing Director, and the Corporate Strategy Implementation group (CSIG) at PHCC on April 2019. The project was exempt from IRB review as it was decided that the research presents no more than minimal risk to subjects. However, investigators prepared an oral presentation that included core information about the study, possible risks and confidentiality information that was shared with the subjects at the beginning of the sessions. Verbal informed consent was obtained from participants at each session, as per PHCC informed consent policy. In addition, participants were reminded that the information discussed during the focus group should not be shared and remain confidential.
Data Collection and Analysis
All sessions were conducted between October of 2019 and March of 2020, and all of them were conducted in Arabic. All sessions were recorded using audio recording device after taking permission from participants at the time of recruitment as well as the beginning of the sessions. All audio recordings were destroyed after transcription. In addition, two individuals from the study team took written notes during the sessions. Audio recordings were transcribed verbatim in Arabic and then translated to English by the analysis team, all of them are bilingual, with help of a lay translator that works at PHCC. The translation was checked independently by three of the study team. The data was analyzed manually using thematic analysis. We used the interview questions (Table 2) as a framework to be able to organize the data before starting the process of coding. The transcripts were read multiple times to ensure familiarity with the data and concepts. A line by line analysis was conducted and the data was coded using inductive coding. Then, the codes were further analyzed and grouped into categories. Following it the coding themes were identified. Themes identified in each focus group were compared to the whole data set and themes that did not have enough data to support them, recurred less than three times across all focus groups, were excluded.
 |
Table 2 Focus Group Interview Questions |
Results
Description of Participants
Ten focus groups were conducted with a total of 89 participants Table 3. Each focus group had between 5 and 12 participants, with a median of 9 participants. The participants ages ranged from 20 to 65 years old. The mean age of participants was 42 years old. 54% of participants were males, and 46% were females. Qatari participants represented 46% of all participants. Out of all Non-Qatari participants (n=48), Egyptians represented 23% (n=11), followed by Jordanians at 21% (n=10), Sudanese 17% (n=8), Syrian 15% (n=7), Palestinians 10% (n=5), and Yemenis 6% (n=3). The rest of the participants were from UAE, Iraq, Algeria and Oman. Although research team emphasized diversity in family structure in recruitment, the data in relation to family composition was not documented through the study.
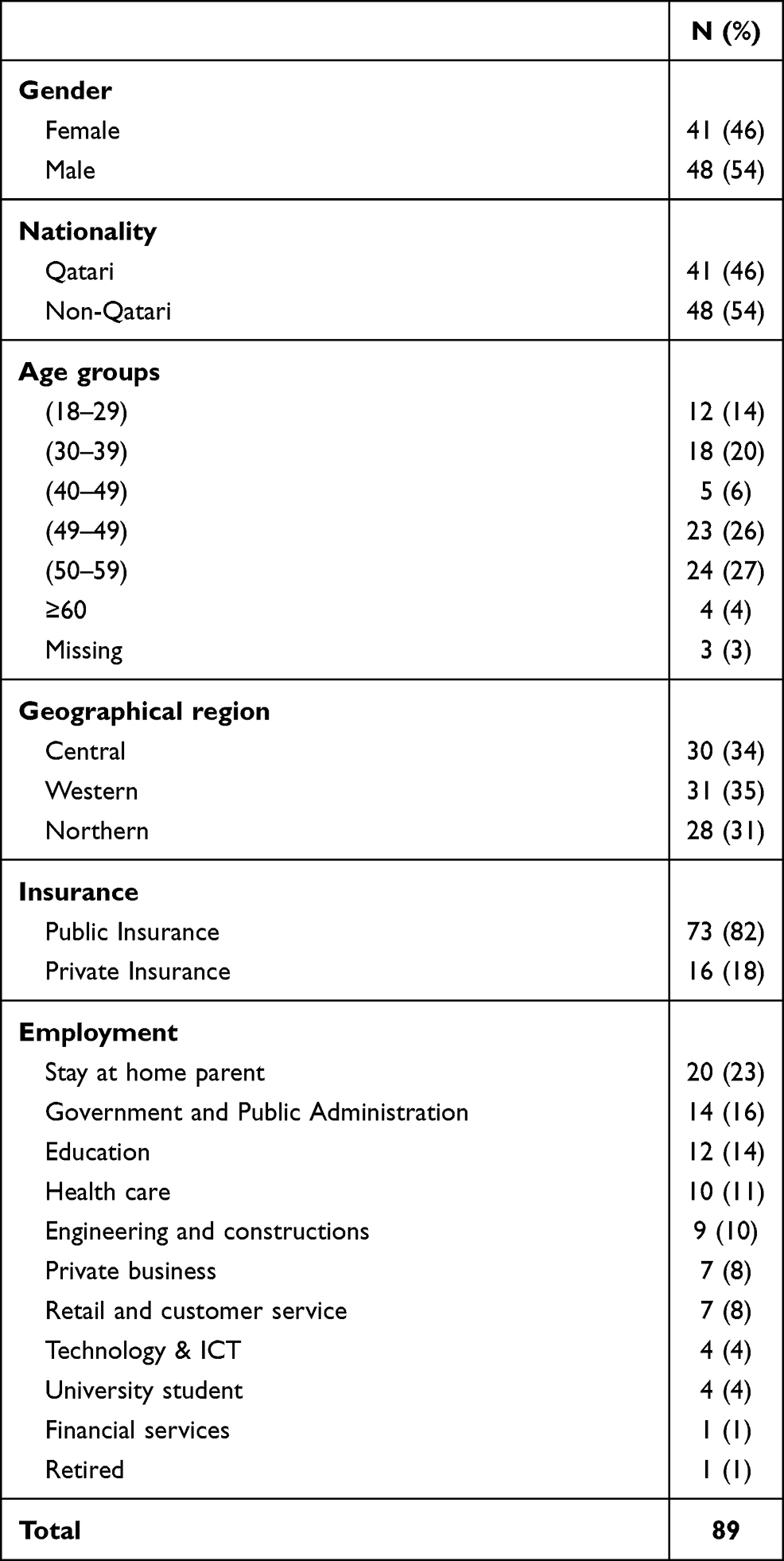 |
Table 3 Participant Demographics |
Themes
Community’s Health Needs and Concerns
- Overweight and obesity: participants identified overweight and obesity as a major community health problem especially its increase among children. They relate the obesity issue to the changing lifestyle of families with many leading a sedentary or inactive lifestyle combined with unhealthy nutrition and eating habits of fast and junk food.
I think we need to change our food culture, my nieces and nephews are overweight, because they don’t move a lot, most households have house help and kids don’t have to do any chores or clean their rooms. They spend most of the day playing with electronics. Even when their parents decide to reward them, they take them out to the mall to have a fast food meal. (Female, Qatari participant)
I noticed that most of the drinks and snacks in the health center vending machine are unhealthy. (Female, Non-Qatari participant)
- Chronic non-communicable diseases: diabetes and hypertension were identified as health threats. Participants were concerned about increasing diabetes rates among adults and children. They expressed concerns about the lack of awareness about childhood diabetes among families and schools.
Obesity is a big problem. People eat a lot of sweets and fatty food. A lot of the people are having diabetes now, and they resort to weight loss surgeries to get rid of it. (Female, Qatari participant)
- Mental health and substance abuse: mental health illness along with the mental health stigma were noted as a major health concern. Participants mentioned that they rarely seek mental or emotional support from a professional because of fear of stigma. They also spoke about the lack of awareness of mental health illness and its symptoms and linking it to religion, and not understanding that it is a disease. In fact, some of the participants expressed that they believe that people with strong faith will not be affected by mental illness.
My sister got depressed after she gave birth, me and my mother were very tough on her, we refused to send her for psychiatry services, and we helped her through “rogya”, and it worked for her. (Female Qatari participant)
I don’t feel comfortable asking for a mental health appointment because when I go to the front desk, they will ask me what type of appointment do you have, I can’t say I am coming for the mental health appointment. (Male Qatari participant)
- Limited number of trained health professionals in schools: according to participants, most schools have one school nurse that do not deal with chronic diseases such as diabetes, mental illness, or disability. They mentioned that there is a need for more counselors and wellness coaches to support emotional and mental wellbeing of the students. Finally, more teachers should be trained to identify mental health symptoms among children and adolescents.
There is a shortage in school nurses, they only prescribe “Panadol”. Some schools have one nurse for 700–800 students. (Male, Qatari participant)
Sometimes we refer students to hospitals for minor problems that can be handled at the school if we had trained providers. I think this burdens the system. (Female, Non-Qatari participant)
- Psychosocial stress: participants expressed that factors such as job insecurity, limited promotions, and long working hours especially in the private sector are significant contributors to their stress.
Fast life pace is affecting people’s mental health and increasing their stress. We are exposed to negative news and news of wars all day. (Female, Non-Qatari participant)
- Built environment concerns: this include increasing the pedestrian-friendly areas with walking trails, physical fitness facilities, and more parks or green spaces in all neighborhoods.
I used to walk daily in my old neighborhood, since I moved to my current neighborhood I can’t walk because it doesn’t have pedestrian or bicycles paths for children. (Female Non-Qatari participant)
We are working with the municipality council to install gym stations at the public park in our area just like the ones at aspire park, so people can do exercise. (Male, Qatari participant)
New health center’s buildings have swimming pools and gyms, unlike old health centers. (Male, Qatari participant)
Health Care Needs
- Healthcare co-ordination: participants voiced that co-ordination of medical care was very important especially for those with multiple morbidities as they receive their care from multiple health providers. In general, they faced difficulty navigating the system firstly in getting diagnosed because of the long waiting times for tests and specialized appointments. Secondly, they faced challenges after patients got discharged from secondary care because of the lack of communication and information exchange between different health providers. They suggested hiring case managers that work collaboratively with the patient and their care givers to help them navigate the health system and better co-ordinate their care.
Patients who travel abroad for treatment face challenges when the patient returns back. We were referred to a special committee to coordinate our patient’s care and we ended up waiting for months for appropriate referrals and appointments. (Male, Qatari participant)
- Community based health education programs: participants highlighted the need for more initiatives that raise people awareness and expand their knowledge about prevention and educate them about health in community settings.
Raising the awareness is very important, I’ve attended a workshop that our local health center held at my workplace about the risks of unhealthy nutrition and drinks with high sugar content such as Pepsi, and after it I decided to stop drinking these drinks. (Male, Non-Qatari participant)
- Telecommunication with physicians: participants expressed interest in getting online medical consultations through medical apps accessed in smartphones or desktops. According to them, It will be an efficient way to reduce the number of personal appointments. This will be particularly helpful for patients with chronic conditions that constantly need to monitor their health.
I saw an app when I traveled abroad and the patient can access his medical records through it, book appointments, or ask for information. (Female, Qatari participant)
I have Diabetes, and whenever I need an information about managing my diseases or my medications, I communicate with a doctor in the USA through an app instead of having to go to the health center, book an appointment and spend a long time only to ask for information, I think this will save my time, and free appointments for people in more need. (Male, Qatari participant)
- Improving patients access to their medical records: some participants noted challenges when they tried to access their medical records. They think that it is essential for patients, especially those with multiple conditions that see multiple health care providers, to access their full records.
I am aware of “My-health”, but when I accessed it, it didn’t have all the information I needed. I had to go to the health center and pay an extra fee to get a print of my records. (Male, Qatari participant)
- Increasing access to dietetics/nutrition, physiotherapy, and geriatric services: participants, especially those living outside of Doha noted the need for more clinics that offer geriatric rehabilitation services and pediatric physiotherapists that can help children with special needs. In addition, they expressed their needs for more clinics that offer prenatal, and women care.
A lot of people in the community suffer from obesity and diabetes. We need obesity clinics that runs every day on both shifts. (Male, Qatari participant)
- Expansion of worksite wellness programs to improve behavioral risk factors such as sedentary lifestyle smoking, and unhealthy nutrition.
- Sources of health-related information: most of the participants used Google search engine as their main source of their medically relevant information. Although using the Internet as a main source of medical information is an international trend, there are “multiple studies reporting the lack of accuracy and reliability of internet for obtaining the information”.11 Other sources mentioned by participants were family members and friends followed by doctors.
Health Care Experiences and Barriers to Access
- Timely access to care: participants expressed concerns about the difficulty in getting timely appointments, especially for dental services which leads to limited accommodation of patients with urgent problems. In addition, Qatari patients’ perception is that they are disadvantaged when it comes to availability of appointments, and they think they are not being prioritized.
I took my daughter to a private dental clinic, payed more money out of pocket, but it’s better than having to wait for an appointment. (Male, Qatari participant)
I wonder if we are being prioritized in getting medical services! (Female, Qatari participant)
- Physician-patient communication: participants did not feel that doctors spend enough time with their patients. They mentioned that a lot of physicians at the health centers do not speak Arabic which highly affects the patient-doctor communication and the quality of care. Moreover, participants expressed concerns that physicians spent a big amount of the consultation’s time typing on their computers.
The patients don’t just need medication; they need advice and guidance from their doctor. The doctors don’t spend enough time with the patient as they are occupied with writing on the computers and other patients keep knocking on the door. (Male, Qatari participant)
My last visit the doctor only spoke English, my English is not very good, and I couldn’t understand what he was saying, he went outside the room and brought a nurse to help translate for him. (Male, Non-Qatari participant)
- Patient’s awareness of availability of health services: most of the focus groups participants knew about the Family Medicine Model implemented at all PHCC health centers (80%, n=71). However, only (14%, n=12) knew the name of their assigned family physician. In general, they were not fully aware of the family physician role or scope of service. Some of the participants tended to confuse “family physicians” with “general practitioners”. While almost all participants were aware of cancer screening services offered at PHCC, more than half of them were not aware that PHCC offers mental health, or home health care services.
I don’t understand why I have to see the family physician if I came with an eye complaint, for example. This process wastes the patient’s time. I think they need to invest funds in hiring more needed practitioners, such as dentists, we have to wait for months for a dental appointment. (Male, Non-Qatari participant)
- Front desk customer service: participants noted the need for a sensitive front desk staff that treat patients with respect and help maintain a patient friendly environment. In general, they were not satisfied with front desk staff at the health centers. The front desk staff were perceived as being unhelpful and insensitive to patient’s needs. In addition, male participants mentioned that most front desk staff are women. The limited number of male receptionists can be inconvenient for male patients.
The staff at the reception desks watch videos or talk on their phones and ignore the patients. (Male, Qatari participant)
- Appointment booking through phone or call center (107): participants acknowledged that using the (107) booking services made the process much easier, however, they expressed concerns about the level of training of the respondents as some of them were not fully aware of the available services, and some of the participants received wrong appointments at a different clinic than the one they have requested.
- Factors affecting people with disabilities’ access to care: participants discussed factors that compromised people with disabilities access to care. The need for longer appointments, shortage of specialized staff, and community stigma were some of the factors identified by them.
I work with deaf people, if sign language interpretation services were available at all centers, the patients can come to the center alone without the need to bring a family member, currently they have to come with someone to interpret for the doctor, and that can improve their privacy. (Female, Qatari participant)
Some families keep their special needs children at home and not allow them to go out or socialize. (Female, Qatari participant)
Discussion
To our knowledge, this is the first study that explored the perception of Arabic speaking primary care clients of the most important community health issues, their health care needs, their experiences with health services, and their perceived barriers to healthcare access. One of main principles of Qatar’s national strategy is community empowerment. It focuses on building a system that acknowledge patients as individuals and value their health experiences.15 Collecting qualitative data provides an opportunity to examine people’s perceptions, and motivations and engage the whole community. This process is very important for strategic planning of health services. It is particularly necessary for understanding perceived barriers to health care utilization and improving access to services.16
When asked about the most significant health issues in the community, participants identified obesity, especially childhood obesity, and type 2 diabetes as major community concerns. Qatar has one of the highest prevalence’s of childhood obesity when compared to the Gulf Corporation Countries (GCC).17 “The prevalence for overweight and obesity in children aged 5–9 years in Qatar was recently reported as 18.3% and 18.2%, respectively”.17 And, recent estimates project an increase in type 2 diabetes prevalence by 43% by 2050.18
In addition, mental health illness was also among major problems identified by participants. Previous research shows that around 20% of people attending primary care have at least one mental health condition.19,20 Moreover, our study participant’s perceptions about mental health were consistent with recent research conducted among university students in Qatar where 39.6% of Qatari subjects believed that “mental illness is the result of possession of evil spirits”.21 Our findings support the need for service design that decreases stigma and recognizes that religious and cultural beliefs can influence patient’s health-care seeking behavior.22
One of unique findings in our study was that participants were able to identify some of the socioeconomic and environmental factors that affects the health of the individual and the community. Participants identified factors such as neighborhood design, and workplace stress as alarming community concerns. In addition, the need for health and wellness interventions at schools and workplaces was highlighted in the sessions. They realize that improving the places we live, learn, and work in can enhance the health of the whole community and support change of unhealthy behaviors.23,24
Our study also demonstrates some of the perceived barriers to accessing and utilizing health services. The inability to obtain timely access to services, and the difficulty of getting timely appointments especially to dental services was one of the highlighted barriers. It has been reported that many of the GCC countries including Qatar are still facing challenges with shortage of health care workers25 especially dentists. According to the annual statistical report produced by PHCC in 2019,26 there is a 1.5 dentist per 10,000 registered PHCC population26 which is less than 1:1000 ratio recommended by the WHO.27
In addition, our results show that participants had negative perceptions regarding the physician’s use of computers during medical consultations. They thought that it affected the duration of the visits and interrupted their communication with the physician. As the use of Clinical Information System (CIS) and electronic medical records has been established recently in Qatar,28 we could not find studies that explored the impact of using it on patient’s satisfaction and on doctor-patient interaction. A recent study conducted in Saudi Arabia in primary care settings concluded that the use of electronic medical records did not affect the overall patient’s satisfaction or their communication with doctors.29 However, there is existing evidence that shows that the use of computers can negatively impact the psychological, and emotional communication between physicians and their patients.29 Such challenges can be avoided by constant training of providers and system improvements.
Another interesting finding was that telecommunication with health care providers was perceived to help with providing faster medical care and shortening waiting times. Comparable findings were reported by Ashfaq et al30 as they reported that E-health is cost effective, permits earlier interventions and can be used as a tool to deliver global medical care.
Arabic speaking participants also expressed difficulty accessing health services because of the language barrier. In Qatar, a lot of the primary care physicians do not speak Arabic. An explanation of this is that Qatar and neighboring GCC countries are heavily dependent on expatriate health care professionals and there is a shortage of nationally trained health care providers.25 This can cause cultural and language challenges and might compromise patients’ safety and their access to quality care.31
The importance of raising the community’s awareness about health-related issues and availability of services has been reported in other studies.32,33 Van den Broucke32 reported that people with lower awareness are less likely to partake in health screening initiatives, embrace health promoting behaviors, or use preventative services. Our results clearly highlighted the need to enhance the community’s awareness of the full range of services available at primary care health centers. In addition, it shed light on the gaps in perception of the basic role of the family medicine physicians and the scope of their practice when compared to “general practitioners”. A “general practitioner” in Qatar is a licensed physician who completed one year of post-graduate training34 unlike family doctors that complete a longer postgraduate specialized training. The confusion can negatively affect patients’ trust in family physicians’ medical expertise35 which might lead them to skip primary care and seek medical care at secondary and tertiary care hospitals.35,36
Respondent groups favored health care models that supports smooth transitioning between different providers across health care settings.37 Moreover, they identified the need for diversified programs with multidisciplinary teams that combine medical, nutrition, physiotherapy, and social services and recognize the health needs of vulnerable populations such as individuals with special needs.37,38
Strengths and Limitations of This Study
- We collected in-depth qualitative data with 89 participants sharing wide ranging point of views about their perceptions and experiences. There are limited studies in Qatar that investigated patients’ views in primary care.
- The focus groups were conducted in two cycles. Each cycle included 5 sessions and each of them covered a separate demographic group. Data collection continued until theoretical saturation was reached. However, as the data was analyzed manually we did not explore findings particular to each demographic group.
- Although the facilitators were Arabic speakers which reduced the chances of misinterpretation of the questions, targeting Arabic speaking clients excluding Non-Arabic speaking ones can affect the generalizability of the results.
- We used non-random sampling, purposeful sampling and identified “information-rich cases” based on recommendations from health centers’ staff which is prone to researcher bias, and it also limits the extrapolation of findings.
Conclusion
This study was completed as part of the Primary Health Care Corporation’s (PHCC) Community Health Needs Assessment (HNA) initiative. The findings yielded new insights into the perceptions of Arabic speaking primary care clients regarding important health issues in the community, health care needs and experiences, as well as barriers to health care access. It highlights facets of health needs not related directly to the health service as it offers a wider look into social and environmental factors affecting the health of the Arabic speaking individuals and their surrounding community. The results from this paper take the literature forward in filling the knowledge gap and it provides valuable information to assist the development of socially and culturally appropriate health programs.
Further activities can be explored to raise the community’s awareness about existing health services and programs at the primary care level. And, further research is needed to examine the relationship between the perceptions and needs of primary care clients and their demographic characteristics. We recommend that the results of this study should be linked to health policy development and service design at the primary care level in the State of Qatar.
Data Sharing Statement
No additional data are available.
Ethics Approval
The study was part of health Needs Assessment project that was approved by the Managing Director, and the Corporate Strategy Implementation group at PHCC on April 2019. The project was exempt from IRB approval as it was deemed a low-risk epidemiological activity.
Consent for Publication
Written informed consent was waived. All participants provided oral informed consent at each session for this research, which included publication of anonymized responses. This consent process was approved by ethics committee. The research was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
Open Access funding provided by the Qatar National Library. The authors acknowledge the Operations department at PHCC, the members of the Technical Advisory Group (TAG) for providing support during the planning of the project, and managers and staff of health centers (Al Wakra, West Bay, Al Daayen, Al Wajba, Al Waab, Abu Baker Al Siddig, AlSheehanya, Rawdat Al Khail, Leabaib and Qatar-University).
Funding
The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclosure
The authors reported no conflicts of interest for this work.
References
1. Hukoomi (Qatar e-government). About Qatar; 2020. Available from: https://portal.www.gov.qa/wps/portal/about-qatar.
2. Al Kuwari MG, Al Abdulla S, Abdulla M, et al. Qatar’s primary health care health needs assessment 2019; 2020. Available from: https://www.phcc.gov.qa/assets/phcc/HealthNeedsAssessment.pdf.
3. Priya Dsouza Communications. Population of Qatar by nationality - 2019 report; 2020. Available from: https://priyadsouza.com/population-of-qatar-by-nationality-in-2017/.
4. Sharkey T. Mental health strategy and impact evaluation in Qatar. BJPsych Int. 2017;14(1):18–21. doi:10.1192/s2056474000001628
5. World Health Organization. Country profile Qatar. Available from: https://www.who.int/countries/qat/en/.
6. General Secretariat for Development Planning. Qatar National Vision 2030; 2008. Available from: https://www.psa.gov.qa/en/knowledge/Documents/QNV2030_English_v2.pdf.
7. Primary Health Care Corporation. Primary health care corporation corporate strategic plan 2019 – 2023; 2019. Available from: https://phcc.qa/portal_new/admin/images/documents/2019/Corporate%20Strategic%20Plan%202019-2023%20English.pdf.
8. Ministry of Public Health. Family medicine model for integrated and high quality care; 2020. Available from: https://www.moph.gov.qa/english/strategies/Supporting-Strategies-and-Frameworks/PrimaryHealthCareFoundationStrategy/Pages/family-medicine-model-for-integrated-and-high-quality-care.aspx.
9. Haj Bakri A, Al Thani A. Qatar stepwise report, 2012 chronic diseases risk factor surveillance; 2020. Available from: https://www.who.int/ncds/surveillance/steps/Qatar_2012_STEPwise_Report.pdf.
10. Bani IA. Journal of family & community medicine. Health Needs Assess. 2008;15(1):13–20.
11. Leung FH, Savithiri R. Spotlight on focus groups. Can Fam Physician. 2009;55(2):218–219.
12. Sandru C. Participatory needs assessment in local communities. methodological aspects. Bull Transil Univ Brasov Series II. 2014;7:97–104.
13. Hawamdeh S, Raigangar V. Qualitative interviewing: methodological challenges in Arab settings. Nurse Res. 2014;21(3):27–31. doi:10.7748/nr2014.01.21.3.27.e357
14. Palinkas LA, Horwitz SM, Green CA, Wisdom JP, Duan N, Hoagwood K. Purposeful sampling for qualitative data collection and analysis in mixed method implementation research. Adm Policy Ment Health. 2015;42(5):533–544. doi:10.1007/s10488-013-0528-y
15. Ministry of Public Health. National Health Strategy 2018–2022; 2018. Available from: https://www.moph.gov.qa/Admin/Lists/PublicationsAttachments/Attachments/54/NHS.pdf.
16. Pieh-Holder K, Goldschmidt C, Young P. Qualitative needs assessment: healthcare experiences of underserved populations in Montgomery County, Virginia, USA. Rural Remote Health. 2012;12:1816.
17. Choudhury S, Omar O, Arora T, et al. Qatar obesity reduction study (QORS): report on a pilot school-based nutrition education campaign in Qatar. J Child Obes. 2018;S2:007.
18. Awad SF, O’Flaherty M, Critchley J, Abu-Raddad LJ. Forecasting the burden of type 2 diabetes mellitus in Qatar to 2050: a novel modeling approach. Diabetes Res Clin Pract. 2018;137:100–108. doi:10.1016/j.diabres.2017.11.015
19. Bener A, Abou-Saleh MT, Dafeeah EE, Bhugra D. The prevalence and burden of psychiatric disorders in primary health care visits in qatar: too little time? J Fam Med Prim Care. 2015;4(1):89–95. doi:10.4103/2249-4863.152262
20. Qatar Ministry of Public Health. Summary national mental health & wellbeing strategic framework 2019–2022. Available from: https://www.moph.gov.qa/english/strategies/Supporting-Strategies-and-Frameworks/SummaryNationalMentalHealthFramework2019-2022/Pages/default.aspx.
21. Zolezzi M, Bensmail N, Zahrah F, Khaled SM, El-Gaili T. Stigma associated with mental illness: perspectives of university students in Qatar. Neuropsychiatr Dis Treat. 2017;13:1221–1233. doi:10.2147/NDT.S132075
22. Alzubaidi H, Mc Namara K, Browning C, Marriott J. Barriers and enablers to healthcare access and use among Arabic-speaking and Caucasian English-speaking patients with type 2 diabetes mellitus: a qualitative comparative study. BMJ Open. 2015;5(11):e008687. doi:10.1136/bmjopen-2015-008687
23. Healthypeople 2020. Social determinants of health; 2020. Available from: https://www.healthypeople.gov/2020/topics-objectives/topic/social-determinants-of-health.
24. Girgis L, Van Gurp G, Zakus D, et al. Physician experiences and barriers to addressing the social determinants of health in the Eastern Mediterranean Region: a qualitative research study. BMC Health Serv Res. 2018;18:614. doi:10.1186/s12913-018-3408-z
25. Sheikh JI, Cheema S, Chaabna K, Lowenfels AB, Mamtani R. Capacity building in health care professions within the Gulf cooperation council countries: paving the way forward. BMC Med Educ. 2019;19(1):83. doi:10.1186/s12909-019-1513-2
26. Primary Health Care Corporation: a strategy planning & health intelligence directorate initiative. Annual statistical report; 2019. Available from: https://www.phcc.qa/portal_new/admin/images/2020/PHCC%20Annual%20Statistical%20Report%202019.pdf.
27. WHO. Density of physicians (total number per 1000 population, latest available year). Available from: https://www.who.int/gho/health_workforce/physicians_density/en/.
28. Hamad Medical Corporation. Qatar’s World-first Implementation of Electronic Patient Medical Records Highlighted at HIMSS Conference and Exhibition; 2017. Available from: https://www.hamad.qa/EN/news/2017/December/Pages/Qatars-World-first-Implementation-of-Electronic-Patient-Medical-Records-Highlighted-at-HIMSS-Conference-and-Exhibition.aspx.
29. Wali RM, Alqahtani RM, Alharazi SK, et al. Patient satisfaction with the implementation of electronic medical Records in the Western Region, Saudi Arabia, 2018. BMC Fam Pract. 2020;21:37. doi:10.1186/s12875-020-1099-0
30. Ashfaq A, Memon SF, Zehra A, et al. Knowledge and attitude regarding telemedicine among doctors in Karachi. Cureus. 2020;12(2):e6927. doi:10.7759/cureus.6927
31. Abdelrahim H, Elnashar M, Khidir A, et al. Patient perspectives on language discordance during healthcare visits: findings from the extremely high-density Multicultural State of Qatar. J Health Commun. 2017;22(4):355–363. doi:10.1080/10810730.2017.1296507
32. Van den Broucke S. Health literacy: a critical concept for public health. Arch Public Health. 2014;72(1):10. doi:10.1186/2049-3258-72-10
33. Seymour J. The impact of public health awareness campaigns on the awareness and quality of palliative care. J Palliat Med. 2018;21(S1):S30–S36. doi:10.1089/jpm.2017.0391
34. Ministry of Public Health. Guidelines for physicians; 2020. Available from: http://www.qchp.org.qa/en/Documents/Guidelines%20for%20Physicians.pdf.
35. Elagi A, Jaber BA, Wassly A, Ahmed R, Bosily F. Public’s perception and satisfaction on the role and services provided by family physicians in Saudi Arabia: a cross-sectional study. J Fam Med Prim Care. 2019;8(10):3282–3286. doi:10.4103/jfmpc.jfmpc_621_19
36. Liu X, Tan A, Towne SD
37. WHO. Continuity and coordination of care, A practice brief to support implementation of the WHO Framework on integrated people-centred health services. Available from: https://apps.who.int/iris/bitstream/handle/10665/274628/9789241514033-eng.pdf?ua=1.
38. Williams MD, Asiedu GB, Finnie D, et al. Sustainable care coordination: a qualitative study of primary care provider, administrator, and insurer perspectives. BMC Health Serv Res. 2019;19(1):92. doi:10.1186/s12913-019-3916-5
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.