Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
QT and P-wave dispersion during the manic phase of bipolar disorder
Authors Gurok MG ![]() , Korkmaz H
, Korkmaz H ![]() , Yıldız S, Bakış D
, Yıldız S, Bakış D ![]() , Atmaca M
, Atmaca M
Received 10 March 2019
Accepted for publication 10 June 2019
Published 3 July 2019 Volume 2019:15 Pages 1805—1811
DOI https://doi.org/10.2147/NDT.S208253
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Mehmet Gurkan Gurok,1 Hasan Korkmaz,2 Sevler Yıldız,1 Dilek Bakış,1 Murad Atmaca1
1Fırat University, School of Medicine, Department of Psychiatry, Elazig, Turkey; 2Fırat University, School of Medicine, Department of Cardiology, Elazig, Turkey
Background and aim: Patients with bipolar disorder (BD) are at increased risk for cardiovascular diseases and complications. This increased risk is considered to be associated with the autonomic nervous system (ANS) abnormalities. However, there is little or no documentation of the relationship between this increased risk and the phases of BD. In this study, we aimed to compare the changes in the QT dispersion (QTd) and P-wave dispersion (Pd), which are predictors of sudden cardiac death and atrial fibrillation, between the patients with manic BD and healthy controls.
Participants and methods: The study included a patient group of 44 patients (26 female and 18 male) that were hospitalized due to a diagnosis of manic BD and met the inclusion criteria, and a control group of 34 age- and gender-matched healthy individuals (21 female and 13 male) with no history of psychiatric and neurological disorders. The QTd and Pd values were determined in each participant by performing the standard 12-lead body surface electrocardiography (ECG).
Results: The principal electrocardiographic indicators including corrected maximum QT interval, corrected QT dispersion, and minimum P-wave duration significantly increased in the patient group compared to the control group (t=2.815, p<0.01; t=4.935, p<0.001; t=3.337, p<0.001, respectively).
Conclusion: The results indicated that patients with manic BD are at increased risk for cardiovascular autonomic dysfunction. Therefore, clinicians should be more careful about ECG changes and related possible cardiac conduction problems such as cardiac arrthythmias in patients with manic BD. Further longitudinal studies are needed to investigate BD and its phases (depression, mania, and hypomania) with regard to ANS and cardiac abnormalities.
Keywords: mania, bipolar disorder, QT dispersion, P-wave dispersion
Introduction
Bipolar disorder (BD) is a serious mental disorder characterized by recurrent attacks and high morbidity and mortality. There are three main phases that define the course of BP: depression, mania, and hypomania. Patients with BD can cycle between these phases and present completely normal or minimal symptoms.1 On the other hand, BD patients are at increased risk for diabetes mellitus (DM), metabolic syndrome, and cardiovascular disease (CVD).2 BD is associated with a decreased life expectancy of 8–12 years and CVD is one of the leading causes of this decrease.3 In patients with BD, the risk of mortality associated with CVD has been reported to be 8 times higher in patients younger than 40 years of age compared to the general population.4,5 Common risk factors for the increased mortality associated with CVD in BD patients include individual factors such as smoking, unhealthy diet, and lack of exercise, as well as psychotropic drugs and the potential metabolic processes involved in the pathophysiology of BD.6 Studies reporting on BD have primarily focused on the relationship between increased morbidity and mortality and the depressive phase of the disease.7,8 However, studies investigating the manic phase of BD, despite being limited in number, have indicated that the manic phase and manic symptoms are associated with the increased risk of mortality from CVD.6,7 This increase can be explained by the fact that the rates of mortality in BD are higher than those of another mood disorder, unipolar depression.9,10 Literature indicates that there are several hypotheses regarding the development of mania which are known as “noradrenergic activation hypothesis”, “noradrenergic/cholinergic imbalance hypothesis”, and “cholinergic insufficiency hypothesis”. Additionally, there are some other studies that postulate that BD is associated with sympathetic hyperactivity and there are some that investigate plasma norepinephrine concentration and its effect on the cardiovascular system.11,12 Most of these studies have indicated that patients with BD are likely to have increased sympathetic activity and increased heart rate variability (HRV) along with decreased parasympathetic activity, which suggests that autonomic factors may be effective in the development of manic episodes. On the other hand, there are some other studies specifically focusing on autonomic nervous system (ANS) abnormalities in BD13,14 and in the manic phase of BD.15 These studies have mainly considered CVD as a predictor of ANS functions, implicating that electrocardiography (ECG), which is a simple and noninvasive procedure, can provide information on the functions of ANS and its two branches (sympathetic and parasympathetic). In previous studies, ANS has been shown to be associated with numerous psychiatric disorders including depression, anxiety disorder, conversion disorder, and hypochondriasis.16–20 However, the exact effect of ANS abnormalities on the development of diseases remains to be elucidated.
Electrocardiography (ECG) is a widely used noninvasive cardiac imaging tool. The QT dispersion (QTd) on ECG indicates ventricular repolarization and depolarization. Increased QTd is an indicator of ventricular instability, which thus may lead to severe ventricular arrhythmia and sudden cardiac death.21,22 P-wave dispersion (Pd) is defined as the difference between the widest and the narrowest P-wave duration on ECG.23 Prolonged Pd interval is considered to be associated with abnormal electrical communication and to be an independent risk factor for atrial fibrillation.24 As they are directly related to the cardiac autonomic function, both QTd and Pd have a potential to predict ANS abnormalities.
It is commonly known that patients with psychiatric disorders have an increased risk for CVD. Based on this fact, QTd and Pd have been investigated in numerous psychiatric disorders including panic disorder, obsessive compulsive disorder (OCD), somatoform disorders, hypochondriasis, and schizophrenia.16–20 In addition, investigation of CVD in BD patients is highly important due to the fact that the manic phase of the disease has a more aggressive course and requires high-dose treatment compared to other psychiatric disorders and that the manic phase has been shown to be associated with ANS abnormalities. The aim of this study was to compare the QTd and Pd values between the patients with manic BD and healthy controls to shed light on the changes in QTd and Pd and on potential ANS abnormalities.
Materials and methods
The present study was conducted after approval by the Firat University School of Medicine Ethics Committee with the assignment number: 2017-17/13. All procedure are in accordance with the Helsinki Declaration. Also written informed consent was obtained from all healthy control subjects and patients. Additionally patients data confidentiality was strictly taken attention. The study included patients that were hospitalized at the Psychiatry clinic after being diagnosed with manic BD based on the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) criteria. As manic disorder requires inpatient hospitalization, the study retrospectively evaluated the medical records of the patients that were hospitalized in our inpatient clinic and underwent routine ECG evaluation. Meaningfully, since all the patients included in the study were hospitalized in the inpatient clinic, the easy access to all the medical records of the patients was a remarkable advantage for the study. As psychotropic drugs are likely to affect the ECG results, patients that had a primary diagnosis of BD or refused treatment and those who discontinued the drug therapy due to such reasons as treatment non-compliance were also included in the study. we have screened all patients who were hospitalized between January 2017 and June 2018. The number of patients were 61 but after exclusion criteria 44 met the inclusion criteria of the present study. As a result, medical records of 44 patients that received inpatient treatment at Firat University Medical School Psychiatry Department between January 2017 and June 2018 were retrospectively reviewed. In addition, a control group consisting of 34 healthy age- and gender-matched individuals with no history of psychiatric and neurological disorders was also included in the study.
Inclusion criteria for the patient group
The inclusion criteria for the patient group were as follows: an age of 18–65 years, a diagnosis of manic disorder based on the DSM-5 criteria, absence of comorbid psychiatric disorders and a neurological or serious systemic disease, absence of vasoactive medication or absence of regular use of psychoactive drugs (patients that had a primary diagnosis of BD, refused treatment, or discontinued the drug therapy), absence of alcohol or drug abuse (at least in the last 6 months), absence of a pathology in routine blood and biochemical tests (plasma lipids, fasting blood glucose, and liver and kidney function tests), absence of a history of cardiac failure, valvular heart disease, cardiomyopathy, myocardial infarction, and cardiovascular diseases such as bundle branch block and arrhythmia, absence of a history of bypass surgery, stent implantation, and pacemaker implantation, and normal blood pressure at rest.
Inclusion criteria for the control group
The inclusion criteria for the control group were as follows: an age of 18–65 years, absence of a history of an Axis-1 psychiatric disorder, absence of a history of medical treatment within the last 3 months, absence of serious neurological diseases (ie diseases that could affect the autonomic nervous system such as epilepsy) and systemic diseases (eg, DM), absence of a pathology in routine blood and biochemical tests (plasma lipids, fasting blood glucose, and liver and kidney function tests), absence of heart diseases (eg, hypertension) on cardiovascular examination and in patient history, and absence of valvular heart disease, ventricular hypertrophy, and structural heart disease on ECG examination.
Measurement of Qtd and Pd on ECG
Routine ECG monitoring was performed in the ECG room at the Psychiatry clinic. The room was quiet and isolated so that the ECG records were not affected by external factors. The recordings were performed when the participant reached adequate spontaneous respiration (after a 10-min waiting period), with the participant placed in the supine position and not allowed to speak during the ECG recording. All the participants underwent a routine standard 12-lead body surface ECG, recorded at a paper speed of 50 mm/s. Three leads were recorded simultaneously. One investigator blinded to patients’ clinical status measured the P and QT wave durations manually. To improve accuracy, measurements were performed with calipers and magnifying lens for defining the ECG deflection.25–27 The onset of P wave was defined as the junction between the isoelectric line and the start of P wave deflection, and the offset of the P waves as the junction between the end of the P wave deflection and the isoelectric line.28 Pmax in any of the 12-lead surface ECG was calculated and used as a marker of prolonged atrial conduction time. Pd, defined as the difference between Pmax and Pmin, was calculated from the 12-lead ECG. All QT interval measurements were performed manually with calipers. The QT interval was measured from the onset of the QRS complex to the end of the T wave, defined as the return to the T–P isoelectric line. QTd was defined as the maximal inter-lead difference in QT intervals. To achieve a precise evaluation, both QTc and QTd values were corrected using Bazett’s formula (corrected QT [cQT] = QT/√(R–R) interval).29
Statistical analysis
Data were analyzed using SPSS for Windows version 22.0 (Armonk, NY: IBM Corp.). Comparisons were performed using Student’s t-test and correlations were determined using Spearman’s Correlation Coefficient. In addition, analysis of covariance (ANCOVA) was also performed, with the left atrial (LA) size and heart rate accepted as covariates. A p-value of <0.05 was considered significant.
Results
The study included a patient group of 44 (26 female and 18 male) patients that met the inclusion criteria and a control group of age- and gender-matched 34 (21 female and 13 male) healthy individuals with no history of psychiatric and neurological disorders. Mean age was 31.8±8.77 years in the patient group and 36.12±12.35 years in the control group. No significant difference was found between the two groups with regard to age and gender (Table 1). With respect to ECG measurement, we found that the Pmin, QTcmax, and QTcd values of the patients were higher than those of healthy controls (t=3.337, p<0.001; t=2.815, p<0.01, t=4.935, p<0.001, respectively) (Table 1). However, the Pmax, Pd, and QTcmin values calculated for the patient group established no significant difference with those of the control group (p= 0.214; p= 0.204; p= 0.356, respectively) (Table 1). Additionally, Pearson’s correlation coefficient revealed no correlation between patient age and any cardiac parameter.
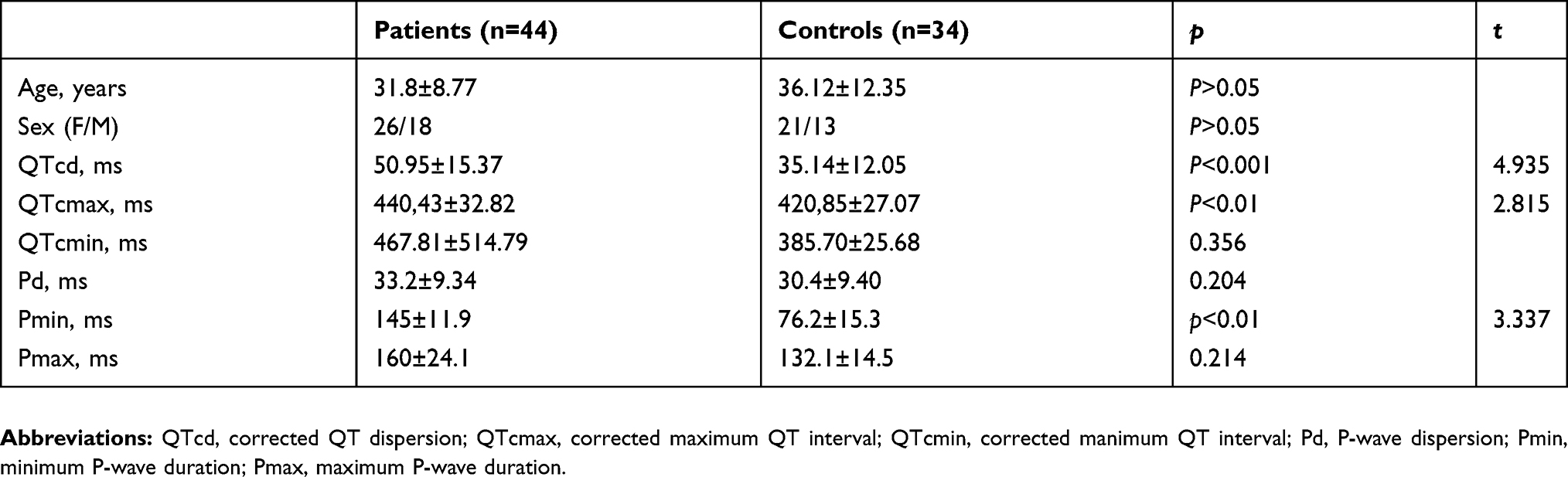 |
Table 1 Characteristics and cardiac parameters of patient and control groups |
Discussion
The results indicated that the principal electrocardiographic indicators including QTcmax, QTcd, and Pmin significantly increased in the patient group compared to the control group (t=2.815, p<0.01; t=4.935, p<0.001; t=3.337, p<0.001, respectively). Meaningfully, increased QTd has been reported to be an indicator of ventricular arrhythmia and subsequent sudden cardiac death and prolonged Pd interval is known to be associated with atrial fibrillation.21,22,24
Patients with BD are known to have an increased risk for CVD and CVD-related mortality. Mortality from CVD is considered to be associated with dyslipidemia, particularly low high-density lipoprotein (HDL) levels.30,31 Additionally, a number of biological factors have also been implicated in the relationship between BD and CVD, including inflammatory factors, oxidative stress, neurotrophic factors, and microvascular events.32 Inflammation and oxidative stress which have been linked with BD. Elevated oxidative stress and inflammation levels, are associated with BD as well as CVD.32 oksidatif Importantly, C-reactive protein, interleukin-6, and tumour necrosis factor-a are elevated in BD, and this proinflammatory markers are also implicated in the development of atherosclerosis.33,34 These studies support to the opinion that inflammation underlies the BD-CVD link.32–34 Additionally, Pompili et al.35 also proposed that there was a link between metabolic diseases (eg, stroke, atherosclerosis), bipolar disorder, and suicidal behavior. Importantly, stroke has been identified as a significant risk factor for both suicide and suicidal ideation especially among depressed patients.35
Literature reviews indicate that there is a large body of literature investigating cardiac repolarization abnormalities such as prolonged QTd interval in psychiatric disorders including OCD, panic disorder, and schizophrenia. However, there are a limited number of studies investigating QTd and Pd in BD.36,37 Additionally, a literature review specific to manic BD demonstrated that there has been no study investigating QTd and Pd in patients with manic BD. Kurt et al.36 classified euthymic BD patients based on the use of valproate and reported that the QTd values were significantly lower in the patient groups compared to the control group and also suggested that valproate may have a contributory effect on the stabilization of cardiac conduction. Another study evaluated 53 euthymic BD patients and revealed that lithium monotherapy increased the QTd, Pmin, and Pmax values in the patient group. The authors concluded that the use of lithium is associated with cardiac instability.37 In our study, all the patients were in the manic phase and the patients that had a primary diagnosis of BD or refused treatment, or discontinued psychotropic drugs due to such reasons as treatment non-compliance were also included in the study so as to rule out the possible effects of psychotropic drugs.
Autonomic nervous system (ANS) abnormalities have been extensively shown in BD patients and are considered to be associated with increased sympathetic activity and decreased parasympathetic activity.15 Accordingly, it is safe to assert that ANS abnormalities could be associated with various factors including individual factors, use of psychotropic drugs, and BD and its phases (including the manic phase). Additionally, they could also be related to cardiovascular events such as ventricular tachycardia, CVD, abnormal HRV, and sudden cardiac death.14 On the other hand, it has been reported that ANS dysregulation, which is associated with the cardiac system, is also associated with the medial prefrontal cortex and the amygdala and that the probable decrease in this cardiac ANS activity could be related to impulsivity and response inhibition, both of which often occur in the manic phase of BD.15,38 This association, considering the relationship between BD and its symptoms, is likely to increase the risk of ANS abnormalities (such as sympathetic hyperactivity) and CVD in the manic phase of BD. Taken together, all these notions suggest that the manic phase of BD can be an independent predictor of cardiovascular mortality in BD patients.6 In our study, the increased QTcd and Pmin values in our patients support the studies that advocate that patients with manic BD are at increased risk for cardiovascular events. Additionally, some other studies also proposed that the presence of a history of manic episodes is a biochemical risk factor for CVD,7,8,15 while Coello et al postulated that there is no difference between the manic phase and the other phases of BD with regard to CVD risk.3
Heart rate variability (HRV) is another parameter that could provide information regarding the association between ANS dysregulation and psychiatric diseases such as BD. Accumulating evidence suggests that there can be HRV-induced pathologies in BD patients.11,12,15,20 In addition, decreased HRV has been shown to be associated with increased risk of cardiac diseases and myocardial infarction.39,40 On the other hand, there is growing evidence suggesting that decreased HRV can be present in patients with serious psychiatric diseases such as schizophrenia, BD, and manic BD.41,42 Quintana et al.41 calculated HRV in patients with schizophrenia and BD compared them with those of healthy controls. The authors reported that HRV was significantly decreased in both patient groups compared to the healthy group and there was no difference between the two patient groups. The authors also noted that the patients with decreased HRV had increased overall and negative psychosis symptom severity irrespective of the diagnosis (ie schizophrenia or BD). Some other studies that investigated the relationship between manic BD and CVD reported that there can be cardiovascular events and ANS abnormalities specific to the manic phase of BD.6,7,15 Accordingly, the symptoms, biological processes, and the resulting risk of cardiovascular events specific to the manic phase of BD, as explicated by previous studies, seem to confirm the hypothesis of the present study. Therefore, it is advisable that patients should be more careful about cardiovascular events during the manic phase of BD, a phase characterized by psychotropic medication and individual problems such as sleep deprivation and nutritional problems.
Our study was limited in several ways. First, although we tried to rule out the confounding factors using the data obtained for the patient and control groups (given the fact that individual factors of the patients such as lifestyle features, physical activity patterns, and diet are likely to affect ECG parameters), there could have been unpredictable results in the study. Second, the present study had small sample size. Third, although we included patients that were not on active psychotropic drug therapy, the drugs that had been previously used by the patients might have affected the ANS features and the metabolic parameters of our patients. Finally we have not used a control group with any psychiatric disorder such as major depressive disorder and bipolar II disorder and we did not include considerable number of healty controls. This was another limitations
Conclusion
The results indicated that patients with manic BD are at increased risk for cardiovascular autonomic dysfunction. Therefore, clinicians should be more careful about ECG changes and related possible cardiac conduction problems such as cardiac arrthythmias in patients with manic BD. Further longitudinal studies are needed to investigate BD and its phases (depression, mania, and hypomania) with regard to ANS and cardiac abnormalities.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Eroğlu Zengin M, Özpoyraz N. Long term treatment in bipolar bisorder. Curr Approaches Psychiatry. 2010;2(2):206–236.
2. Young AH, Grunze H. Physical health of patients with bipolar disorder. Acta Psychiatr Scand Suppl. 2013;442:3–10. doi:10.1111/acps.12117
3. Coello K, Kjærstad HL, Stanislaus S, et al. Thirty-year cardiovascular risk score in patients with newly diagnosed bipolar disorder and their unaffected first-degree relatives. Aust N Z J Psychiatry. 2018;5:4867418815987. Epub ahead of print.
4. Goldstein BI, Schaffer A, Wang S, et al. Excessive and premature new-onset cardiovascular disease among adults with bipolar disorder in the US NESARC cohort. J Clin Psychiatry. 2015;76(2):163–169. doi:10.4088/JCP.14m09300
5. Westman J, Hallgren J, Wahlbeck K, et al. Cardiovascular mortality in bipolar disorder: a population-based cohort study in Sweden. BMJ Open. 2013;3(4):e002373. doi:10.1136/bmjopen-2012-002373
6. Murray DP, Weiner M, Prabhakar M, Fiedorowicz JG. Mania and mortality: why the excess cardiovascular risk in bipolar disorder? Curr Psychiatry Rep. 2009;11(6):475–480.
7. Wazen GLL, Gregório ML, Kemp AH, Godoy MF. Heart rate variability in patients with bipolar disorder: from mania to euthymia. J Psychiatr Res. 2018;99:33–38. doi:10.1016/j.jpsychires.2018.01.008
8. Fiedorowicz JG, Solomon DA, Endicott J, et al. Manic/hypomanic symptom burden predicts cardiovascular mortality with bipolar disorder in the collaborative depression study. Psychosom Med. 2009;71(6):598–606. doi:10.1097/PSY.0b013e3181acee26
9. Angst F, Stassen HH, Clayton PJ, Angst J. Mortality of patients with mood disorders: follow-up over 34–38 years. J Affect Disord. 2002;68(2–3):167–181. doi:10.1016/S0165-0327(01)00377-9
10. Osby U, Brandt L, Correia N, et al. Excess mortality in bipolar and unipolar disorder in Sweden. Arch Gen Psychiatry. 2001;58(9):844–850. doi:10.1001/archpsyc.58.9.844
11. Iacono WG, Lykken DT, Peloquin LJ, Lumry AE, Valentine RH, Tuason VB. Electrodermal activity in euthymic unipolar and bipolar affective disorders: a possible marker for depression. Arch Gen Psychiatry. 1983;40(5):557–565. doi:10.1001/archpsyc.1983.01790050083010
12. Lake CR, Pickar D, Ziegler MG, Lipper S, Slater S, Murphy DL. High plasma norepinephrine levels in patients with major affective disorder. Am J Psychiatry. 1982;139(10):1315–1318. doi:10.1176/ajp.139.10.1315
13. Goodwin FK, Ghaemi SN. Understanding manic-depressive illness. Arch Gen Psychiatry. 1998;55:23–25. doi:10.1001/archpsyc.55.1.23
14. Zahn TP, Nurnberger JI
15. Chang HA, Chang CC, Tzeng NS, Kuo TB, Lu RB, Huang SY. Heart rate variability in unmedicated patients with bipolar disorder in the manic phase. Psychiatry Clin Neurosci. 2014;68(9):674–682. doi:10.1111/pcn.12178
16. Tosu AR, Demir S, Yüksel Kaya MS, et al. Increased QT dispersion and P wave dispersion in major depressive disorder. Exp Clin Cardiol. 2013;18(2):110–112.
17. Atmaca M, Yavuzkir M, Izci F, et al. QT wave dispersion in patients with panic disorder. Neurosci Bull. 2012;28(3):247–252. doi:10.1007/s12264-012-1237-3
18. Yavuzkir MF, Atmaca M, Gurok MG, et al. P wave dispersion in obsessive-compulsive disorder. Indian J Psychiatry. 2015;57(2):196–199. doi:10.4103/0019-5545.158193
19. Izci F, Hocagil H, Izci S, Izci V, Koc MI, Acar RD. P-wave and QT dispersion in patients with conversion disorder. Ther Clin Risk Manag. 2015;26(11):475–480. doi:10.2147/TCRM.S81852
20. Atmaca M, Korkmaz H, Korkmaz SP. wave dispersion in patients with hypochondriasis. Neurosci Lett. 2010;485(3):148–150. doi:10.1056/NEJMra043430
21. Tran H, White CM, Chow MS, Kluger J. An evaluation of the impact of gender and age on QT dispersion in healthy subjects. Ann Noninvasive Electrocardiol. 2001;6(2):129–133.
22. Malik M, Batchvarov VN. Measurement, interpretation and clinical potential of QT dispersion. J Am Coll Cardiol. 2000;36(6):1749–1766.
23. Perzanowski C, Ho AT, Jacobson AK. Increased P-wave dispersion predicts recurrent atrial fibrillation after cardioversion. J Electrocardiol. 2005;38:43–46. doi:10.1016/j.jelectrocard.2004.09.008
24. Schocken K. The analysis of the normal QT interval. Exp Med Surg. 1955;13(3):258–260.
25. Davies LG, Ross IP. Abnormal P waves and paroxysmal tachycardia. Br Heart J. 1963;25(5):570–574. doi:10.1136/hrt.25.5.570
26. Friedman BH, Thayer JF. Anxiety and autonomic flexibility: a cardiovascular approach. Biol Psychol. 1998;49(3):303–323.
27. Snoeck J, Decoster H, Vrints C, et al. Predictive value of the P wave at implantation for atrial fibrillation after VVI pacemaker implantation. Pacing Clin Electrophysiol. 1992;15(11):2077–2083.
28. Waggoner AD, Adyanthaya AV, Quinones MA, Alexander JK. Left atrial enlargement. Echocardiographic assessment of electrocardiographic criteria. Circulation. 1976;54(4):553–557.
29. Robyns T, Willems R, Vandenberk B, et al. Individualized corrected QT interval is superior to QT interval corrected using the Bazett formula in predicting mutation carriage in families with long QT syndrome. Heart Rhythm. 2017;14(3):376–382. doi:10.1016/j.hrthm.2017.06.015
30. Taylor V, McKinnon MC, Macdonald K, et al. Adults with mood disorders have an increased risk profile for cardiovascular disease within the first 2 years of treatment. Can J Psychiatry. 2010;55(6):362–368. doi:10.1177/070674371005500605
31. Naiberg MR, Newton DF, Collins JE, et al. Elevated triglycerides are associated with decreased executive function among adolescents with bipolar disorder. Acta Psychiatr Scand. 2016;134(3):241–248. doi:10.1111/acps.12603
32. Goldstein BI. Bipolar disorder and the vascular system: mechanisms and new prevention opportunities. Can J Cardiol. 2017;33(12):1565–1576. doi:10.1016/j.cjca.2017.10.006
33. Tuomisto K, Jousilahti P, Sundvall J, Pajunen P, Salomaa V. C-reactive protein, interleukin-6 and tumor necrosis factor alpha as predictors of incident coronary and cardiovascular events and total mortality. A population-based, prospective study. Thromb Haemost. 2006;95(3):511–518.
34. Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med. 2005;352(16):1685–1695. doi:10.1056/NEJMra043430
35. Pompili M, Venturini P, Lamis DA, et al. Suicide in stroke survivors: epidemiology and prevention. Drugs Aging. 2015;32(1):21–29. doi:10.1007/s40266-014-0233-x
36. Kurt E, Emul M, Ozbulut O, et al. Is valproate promising in cardiac fatal arrhythmias? Comparison of P- and Q-wave dispersion in bipolar affective patients on valproate or lithium-valproate maintenance therapy with healthy controls. J Psychopharmacol. 2009;23(3):328–333. doi:10.1177/0269881108089594
37. Altinbas K, Guloksuz S, Caglar IM, Caglar FN, Kurt E, Oral ET. Electrocardiography changes in bipolar patients during long-term lithium monotherapy. Gen Hosp Psychiatry. 2014;36(6):694–697. doi:10.1016/j.genhosppsych.2014.07.001
38. Anticevic A, Brumbaugh MS, Winkler AM, et al. Global prefrontal and fronto-amygdala dysconnectivity in bipolar I disorder with psychosis history. Biol Psychiatry. 2013;73(6):565–573. doi:10.1016/j.biopsych.2012.07.031
39. Bigger J, Fleiss JL, Rolnitzky LM, Steinman RC. The ability of several short-term measures of RR variability to predict mortality after myocardial infarction. Circulation. 1993;88:927–934.
40. Kleiger RE, Miller JP, Bigger JT, Moss AJ. Decreased heart rate variability and its association with increased mortality after acute myocardial infarction. Am J Cardiol. 1987;59(4):256–262. doi:10.1016/0002-9149(87)90795-8
41. Quintana DS, Westlye LT, Kaufmann T, et al. Reduced heart rate variability in schizophrenia and bipolar disorder compared to healthy controls. Acta Psychiatr Scand. 2016;133(1):44–52. doi:10.1111/acps.12498
42. Henry BL, Minassian A, Paulus MP, Geyer MA, Perry W. Heart rate variability in bipolar mania and schizophrenia. J Psychiatr Res. 2010;44(3):168–176. doi:10.1016/j.jpsychires.2009.07.011
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.