Back to Journals » Drug Design, Development and Therapy » Volume 19
Pyrotinib Plus Trastuzumab as an Effective Later-Line Therapeutic Strategy for HER2-Positive Metastatic Colorectal Cancer: Results from a Phase II Study
Authors Yang W ![]() , Zhang J, Wu G, Zhang W, Zhou A, Yang L, Sun Y
, Zhang J, Wu G, Zhang W, Zhou A, Yang L, Sun Y
Received 5 August 2025
Accepted for publication 14 November 2025
Published 21 November 2025 Volume 2025:19 Pages 10269—10280
DOI https://doi.org/10.2147/DDDT.S558378
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Manfred Ogris
Wenwei Yang,1,* Jing Zhang,1,* Guifu Wu,2,* Wen Zhang,1 Aiping Zhou,1 Lin Yang,1 Yongkun Sun1
1Department of Medical Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100021, People’s Republic of China; 2Department of Medical Oncology, Beijing Chaoyang District Sanhuan Cancer Hospital, Beijing, 100122, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yongkun Sun, Department of Medical Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Chaoyang District Panjiayuan Nanli No. 17, Beijing, 100021, People’s Republic of China, Email [email protected] Lin Yang, Department of Medical Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Chaoyang District Panjiayuan Nanli No. 17, Beijing, 100021, People’s Republic of China, Email [email protected]
Background: Dual human epidermal growth factor receptor 2 (HER2) blockade demonstrates promising yet limited clinical activity in HER2-positive metastatic colorectal cancer (mCRC). This study was initiated to evaluate the novel combination of trastuzumab (anti-HER2 monoclonal antibody) and pyrotinib (a pan-HER tyrosine kinase inhibitor) in this molecularly defined population.
Methods: This exploratory single-arm phase II trial enrolled HER2-positive mCRC patients refractory to standard first- and second-line therapies. Participants received intravenous trastuzumab (8 mg/kg loading dose on cycle 1 day 1, then 6 mg/kg every 3 weeks) plus oral pyrotinib 400 mg once daily in 21-day cycles. The primary endpoint was objective response rate (ORR).
Results: Between December 1, 2019, and March 31, 2025, 20 patients were enrolled, with 17 evaluable for efficacy. The objective response rate (ORR) was 23.5% (4 partial responses), and the disease control rate (DCR) reached 88.2%. Median progression-free survival (PFS) was 6.2 months (95% CI, 0.42– 11.98), and median overall survival (OS) was 21.1 months (95% CI, 15.84– 26.36). Responses occurred exclusively in RAS/BRAF wild-type patients (ORR 28.6%; DCR 92.9%), who showed significantly longer median PFS (8.5 vs 2.6 months; HR 0.32; P=0.008) and OS (22.6 vs 4.9 months; P=0.022) versus KRAS-mutant counterparts. Treatment-related adverse events (TRAEs) included diarrhea (75%), fatigue (40%), and nausea (35%). Diarrhea accounted for all grade 3 TRAEs (30%). No grade ≥ 4 TRAEs were observed.
Conclusion: Pyrotinib plus trastuzumab demonstrates clinically meaningful efficacy and a manageable safety profile in heavily pretreated HER2-positive metastatic colorectal cancer. These findings support advancing this regimen as a potential alternative in refractory HER2-positive mCRC, particularly in the RAS/BRAF wild-type subgroup.
Plain Language Summary: This phase II trial explored the novel dual HER2 blockade of oral pyrotinib plus trastuzumab in heavily pretreated HER2-positive metastatic colorectal cancer (mCRC). The regimen demonstrated clinically meaningful efficacy (ORR 23.5%, DCR 88.2%, median PFS 6.2 mo, OS 21.1 mo) with a manageable safety profile dominated by low-grade diarrhea. Crucially, all responses occurred in RAS/BRAF wild-type tumors, where outcomes were significantly superior (ORR 28.6%, PFS 8.5 mo, OS 22.6 mo) versus KRAS-mutant patients. These findings support advancing this regimen as a potential alternative in refractory HER2-positive mCRC, particularly in the RAS/BRAF wild-type subgroup.
Keywords: metastatic colorectal cancer, trastuzumab, pyrotinib, HER2, target therapy
Introduction
Colorectal cancer (CRC) ranks as the third most common malignant tumor and the second leading cause of cancer-related deaths worldwide.1 In China, the incidence and mortality of CRC have been increasing steadily, ranking second in incidence and fourth in mortality.2 Despite numerous advances in therapy, the prognosis for metastatic colorectal cancer (mCRC) patients remains poor, with a five-year survival rate of about 12%.3,4 In recent years, the molecular heterogeneity of CRC has been well recognized. A growing number of biomarker-driven treatments for mCRC have emerged, including those targeting deficient mismatch repair/microsatellite instability-high (dMMR/MSI-H), BRAF, neurotrophic tyrosine receptor kinase (NTRK), KRAS G12C, and human epidermal growth factor receptor 2 (HER2).5,6
HER2 is a transmembrane receptor tyrosine kinase encoded by the ERBB2 gene and activated by homodimerization or heterodimerization with other ERBB family members.7 HER2 protein overexpression is primarily caused by the ERBB2 gene amplification. In rare instances, HER2 point mutations may affect genomic regulatory regions, such as promoters or enhancers, indirectly modulating HER2 gene transcription and resulting in HER2 protein overexpression. HER2 overexpression or gene amplification is observed in 15–20% of breast cancer cases and about 20% of gastric cancer patients.8–10 In CRC cases, the frequency of HER2 overexpression or amplification is approximately 2–6.3%.11–13 The incidence of HER2 overexpression or amplification in CRC is associated with several factors. Firstly, HER2 overexpression/amplification is most commonly found in RAS/BRAF wild-type CRC, with an incidence of 5–14%.14 Secondly, the frequency of HER2 overexpression/amplification is influenced by the primary tumor location, with an increased incidence in left-sided CRC compared to right-sided CRC.15 HER2 overexpression also serves as a predictive marker. Several studies indicate that it confers increased risk of central nervous system (CNS) and ovarian metastases in CRC.16–18 Additionally, studies demonstrate that HER2 overexpression is associated with resistance to anti-EGFR (epidermal growth factor receptor) antibody therapy in RAS wild-type metastatic colorectal cancer.19,20 This association is currently under further evaluation in ongoing prospective studies. Regarding survival outcomes, HER2 overexpression is an established independent prognostic factor associated with poor survival in several cancers (eg, breast and gastric cancer).21 However, the prognostic value of HER2 overexpression in CRC continues to be debated.
HER2 is a promising therapeutic target in colorectal cancer. Current HER2-targeted therapies include monoclonal antibodies, tyrosine kinase inhibitors (TKIs), antibody drug conjugates (ADCs), and bispecific antibodies. Pivotal phase II trials, including HERACLES A study,22 MyPathway study,23 and MOUNTAINEER study,24 demonstrated the efficacy and safety of dual anti-HER2 blockade in HER2-positive mCRC. Recently, the DESTINY-CRC01 trial reported that anti-HER2 ADC trastuzumab deruxtecan (T-DXd) exhibits promising antitumor activity in refractory HER2-positive mCRC.25 These collective findings have led to the inclusion of four HER2-targeted regimens in the National Comprehensive Cancer Network (NCCN) guidelines: trastuzumab plus lapatinib, trastuzumab plus pertuzumab, trastuzumab plus tucatinib, and T-DXd. This integration marks a significant advancement in precision medicine for CRC treatment.
Pyrotinib is an oral, irreversible tyrosine kinase inhibitor (TKI) that potently targets EGFR, HER2, and HER4. Pyrotinib has been approved in China for the treatment of breast cancer patients,26,27 and has demonstrated superior efficacy to lapatinib in breast cancer patients with brain metastases.28 Furthermore, the antitumor effect of pyrotinib has been validated in additional solid tumors, including lung and gastric cancer.29,30
Due to the frequent development of trastuzumab resistance, combining it with other anti-HER2 agents possessing complementary mechanisms has emerged as a promising approach. Lapatinib, a reversible EGFR/HER2 TKI, blocks downstream signaling and results in cell-surface accumulation of inactive HER2, which is then targeted for downregulation and degradation by trastuzumab. Consequently, this combination yields synergistic efficacy.31 Given this mechanistic basis, the novel regimen of trastuzumab plus pyrotinib represents a potential alternative with anticipated clinical benefit for mCRC.
This phase II study aimed to evaluate the efficacy and safety of pyrotinib plus trastuzumab in patients with HER2-positive mCRC refractory to standard treatment.
Patients and Methods
Study Design
This investigator-initiated single-arm phase II study was conducted at Cancer Hospital Chinese Academy of Medical Sciences. This study aims to investigate the efficacy and safety of combining pyrotinib with trastuzumab in third-line or later treatment for patients with HER2-positive mCRC. Patients with HER2-positive metastatic colorectal cancer who are refractory to first-line and second-line treatment and have not received any anti-HER2 treatment are eligible. All enrolled patients received an intravenous infusion of trastuzumab at an 8 mg/kg loading dose on day 1, followed by 6 mg/kg, and an oral administration of pyrotinib at 400 mg per day in a 21-day treatment cycle. Dose reductions or delays were allowed for severe adverse events (≥ grade 3 nonhematological or grade 4 hematological toxicity). Treatment was continued until RECIST-defined or clinical disease progression, unacceptable toxicity, patient withdrawal, or investigator decision to terminate treatment.
The study adhered to the Declaration of Helsinki and Good Clinical Practice guidelines. Written informed consent was obtained from all participants. The Ethics Committee of Cancer Hospital Chinese Academy of Medical Sciences approved this study. This study was registered on the Chinese Clinical Trial Registry website (registration number ChiCTR2000028711).
Patient Eligibility
Key inclusion criteria comprised: (1) histologically confirmed metastatic colorectal cancer with HER2 positivity, defined as: immunohistochemistry (IHC) 3+ according to HERACLES diagnostic criteria,22 or ERBB2 gene amplification by fluorescence in situ hybridization (FISH) (ERBB2/CEP17 ratio ≥ 2.0),32 or next-generation sequencing (NGS). (2) metastatic CRC diagnosed by computed tomography (CT) and/or magnetic resonance imaging (MRI) (AJCC 8th edition); (3) at least one measurable lesion per Response Criteria Evaluation in Solid Tumors (RECIST) version 1.1; (4) Eastern Cooperative Oncology Group Performance Status (ECOG PS) of 0 to 2; (5) age ≥ 18 years; (6) disease progression or intolerance to standard first-line and second-line systemic treatment; (7) adequate organ function; (8) estimated life expectancy ≥ 3 months.
The main exclusion criteria: (1) Known hypersensitivity to pyrotinib, trastuzumab, or any of its excipients; (2) prior treatment with pyrotinib, trastuzumab, or any other HER2-targeted agent; (3) symptomatic central nervous system metastases; (4) Inability to swallow oral medications or presence of clinically significant gastrointestinal disorders affecting drug absorption; (5) active gastrointestinal bleeding within 4 weeks before enrollment; (6) major surgery or significant anti-tumor therapy within 4 weeks before enrollment (excluding diagnostic biopsy); (7) history of another primary malignancy within the past 5 years (except adequately treated non-melanoma skin cancer, carcinoma in situ, or other malignancies treated with curative intent without recurrence); (8) severe concurrent diseases or medical conditions; (9) pregnancy, lactation, or refusal to use effective contraception in patients of childbearing potential; (10) any other conditions unsuitable for participation in the trial by the investigator.
Study Endpoints
The primary endpoint was the investigator-assessed objective response rate (ORR) per RECIST version 1.1, defined as the proportion of patients achieving a best overall response of a complete response (CR) or partial response (PR). Secondary endpoints were disease control rate (DCR), progression-free survival (PFS), overall survival (OS), and safety. DCR is defined as the proportion of patients achieving CR, PR, or stable disease (SD). PFS was defined as the time from the first study treatment dose to the earliest occurrence of disease progression per RECIST v1.1 or death from any cause, and OS was defined as the time from first study treatment dose to death from any cause. Safety was assessed through the incidence and severity of adverse events (AEs), graded according to the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0.
Efficacy and Safety Assessment
Tumor assessment was evaluated at baseline (within 28 days before treatment initiation) and every two cycles (approximately every 6 weeks) or as clinically necessary, using CT, MRI, and/or positron-emission tomography (PET-CT). The response was assessed by the investigator per RECIST version 1.1. The efficacy analysis population consisted of patients who received at least one treatment cycle and underwent at least one post-baseline tumor assessment.
Safety assessments were conducted in all patients who received at least one dose of the study medication from the first dose through 30 days after the last dose. The left ventricular ejection fraction was measured at baseline, every 6 weeks during treatment, and at the end of treatment. AEs were graded per CTCAE version 5.0.
Statistical Analyses
This was a single-arm, exploratory phase II trial. The sample size was determined based on practical and statistical considerations for signal detection. Given the exploratory nature of this study and the limited historical controls for HER2-positive mCRC, we aimed to enroll 20–30 evaluable patients. This sample size provides a 95% confidence interval of approximately ±20% around the observed ORR, which was deemed sufficient for an initial assessment of the treatment’s activity.
Baseline characteristics, efficacy, and safety data were summarized using descriptive statistics. Continuous variables are reported as medians with ranges, while categorical variables are expressed as frequencies and percentages. The confidence interval (CI) for the proportion was calculated using the normal approximation method. The Kaplan-Meier method was used to analyze the median follow-up duration and survival endpoints, reported as medians with 95% CI. Survival curves were generated accordingly. The confidence intervals were calculated using the Clopper-Pearson exact method. Subgroup analyses for ORR were performed using logistic regression models, while PFS and OS subgroup analyses were analyzed using the Log rank test. All statistical analyses were conducted using SPSS 29.0 (IBM Corp., Armonk, NY, United States) and GraphPad Prism 10 (GraphPad Software, Inc). Statistical significance was defined as two-sided p < 0.05.
Results
Patient Characteristics
Between December 1, 2019, and March 31, 2025, a total of 20 patients were enrolled. Baseline demographic and clinical characteristics of all patients are summarized in Table 1. The cohort had a median age of 56.5 years (range, 43–70), with 7 females (35%) and 13 males (65%). Primary tumors were predominantly left-sided (90%), comprising 7 sigmoid colon and 11 rectal cancers. The two right-sided tumors included one ascending colon and one transverse colon cancer. Fifteen patients (75%) presented with metastases in two or more organs. HER2 expression status, as determined by IHC, revealed HER2 3+ tumors in 16 patients and HER2 2+/FISH+ tumors in 4 patients. Among 16 patients assessed by FISH or NGS, HER2 amplification was confirmed in all cases; one patient concurrently exhibited HER2 amplification and mutation. Baseline RAS/BRAF gene status testing was conducted in 19 patients, identifying 17 patients with RAS/BRAF wild-type status and two with KRAS mutations. All 17 patients assessed for microsatellite status exhibited proficient mismatch repair/microsatellite stability (pMMR/MSS).
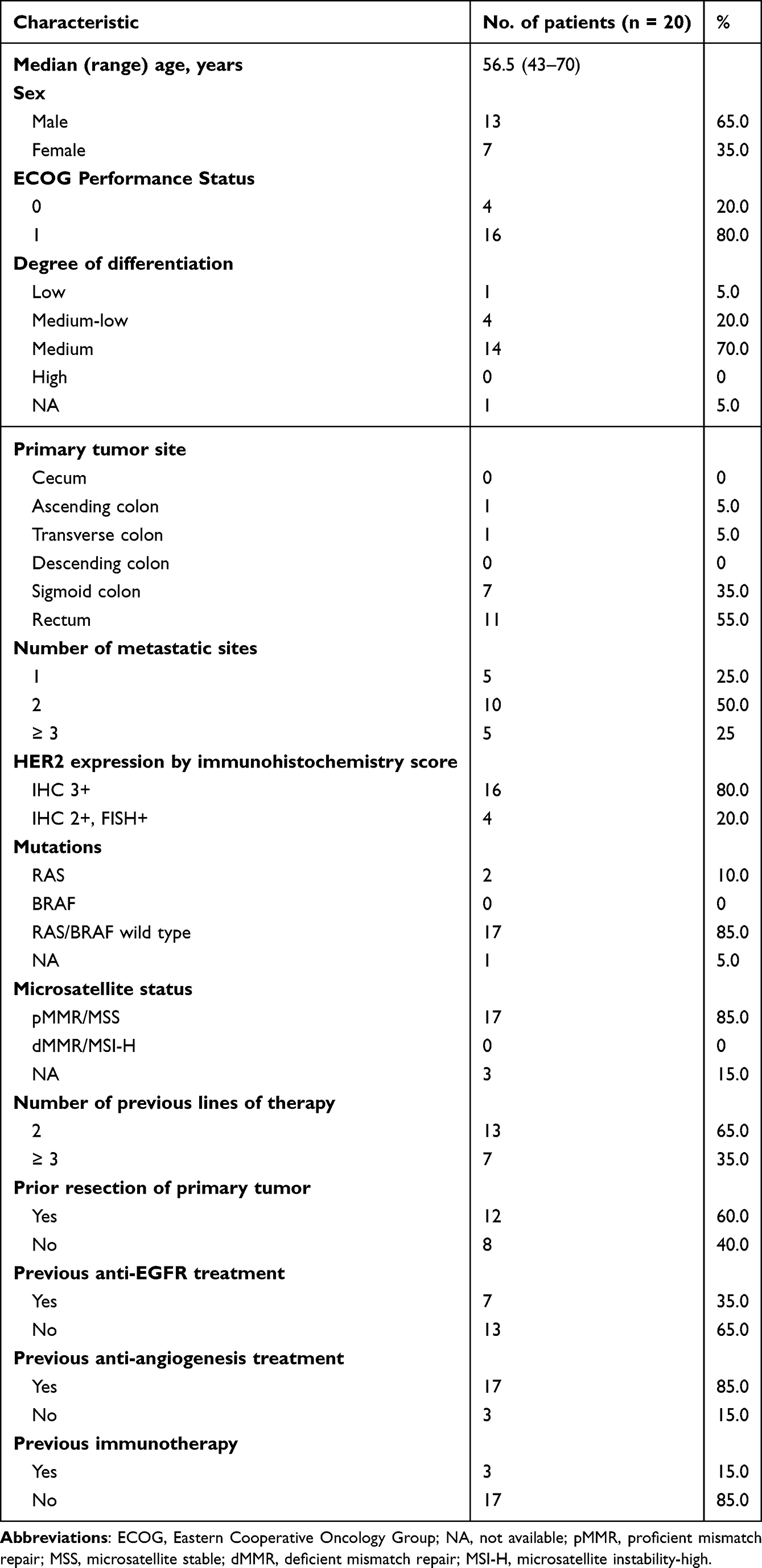 |
Table 1 Baseline Characteristics |
Regarding prior therapies, the cohort was heavily pretreated, with 7 patients (35%) receiving ≥3 prior systemic regimens. Primary tumor resection (radical or palliative) was performed in 12 patients (60%). Previous anti-EGFR monoclonal antibody therapy (cetuximab) was administered to 7 patients (35%), while bevacizumab exposure occurred in 17 patients (85%). Notably, 3 patients (15%) had received prior immune checkpoint inhibitors (ICIs).
Efficacy
As of March 31, 2025, 20 patients had been enrolled, with 17 being evaluable for efficacy. One patient withdrew informed consent within 6 weeks; two discontinued trastuzumab therapy from cycle 2 due to myocardial infarction and allergy in cycle 1, respectively. The median number of cycles administered was 7 (range, 1–17). Four patients (23.5%) achieved a partial response (PR), and 11 patients (64.7%) had stable disease (SD). The ORR and DCR were 23.5% (95% CI, 0.010–0.460) and 88.2% (95% CI, 0.712–1.053), respectively (Table 2). Two (11.8%) patients developed clinically detected tumor progression at the first radiological assessment.
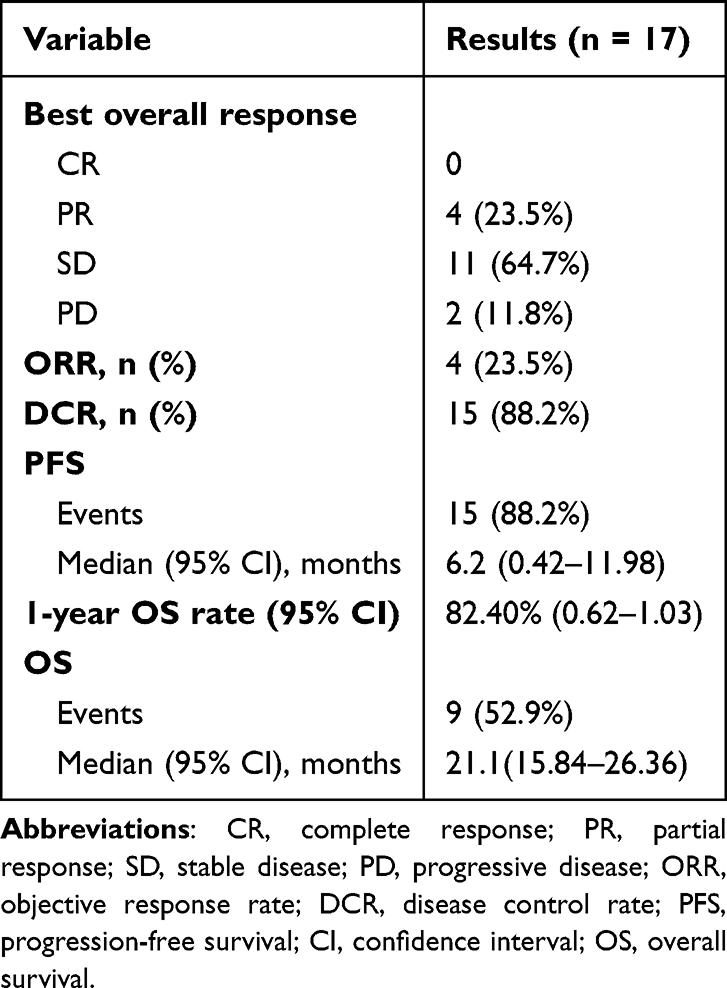 |
Table 2 Summary of Efficacy Outcomes |
As of the cutoff date, the median follow-up was 21.5 months (95% CI, 14.12–28.88). The median PFS was 6.2 months (95% CI, 0.42–11.98) (Table 2 and Figure 1A). As of the data cutoff date, 9 patients (52.9%) had died, the 1-year overall survival (OS) rate was 82.4% (95% CI, 0.62–1.03), and the median OS reached 21.1 months (95% CI, 15.84–26.36) (Table 2 and Figure 1B).
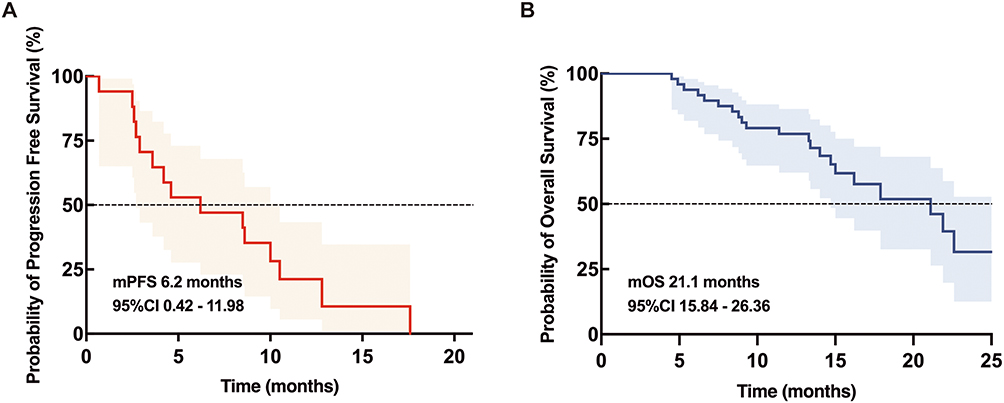 |
Figure 1 Analysis of Survival Outcomes. The figure presents Kaplan-Meier curves for (A) progression-free survival and (B) overall survival. Abbreviations: mPFS, median progression-free survival; mOS, median overall survival; CI, confidence interval. |
Safety
All patients were evaluable for safety assessment. Overall, 18 patients (90%) experienced TRAEs of any grade, with grade 3/4 TRAEs reported in 6 patients (30%). The most common TRAEs were diarrhea (75%), fatigue (40%), and nausea (35%). All six grade 3 events consisted of diarrhea. One patient with a history of coronary artery disease experienced a grade 2 myocardial infarction after cycle 1 treatment (asymptomatic and cardiac enzymes are minimally abnormal, and no evidence of ischemic ECG changes). Treatment interruption or pyrotinib dose reduction was required in 8 patients (40%), attributed to diarrhea (n=7) and fatigue (n=1). Treatment suspension or dose reduction of pyrotinib occurred in 8 (40%) patients, resulting from diarrhea in seven patients and fatigue in one patient. No grade 4/5 TRAEs occurred. Table 3 shows the most common TRAEs.
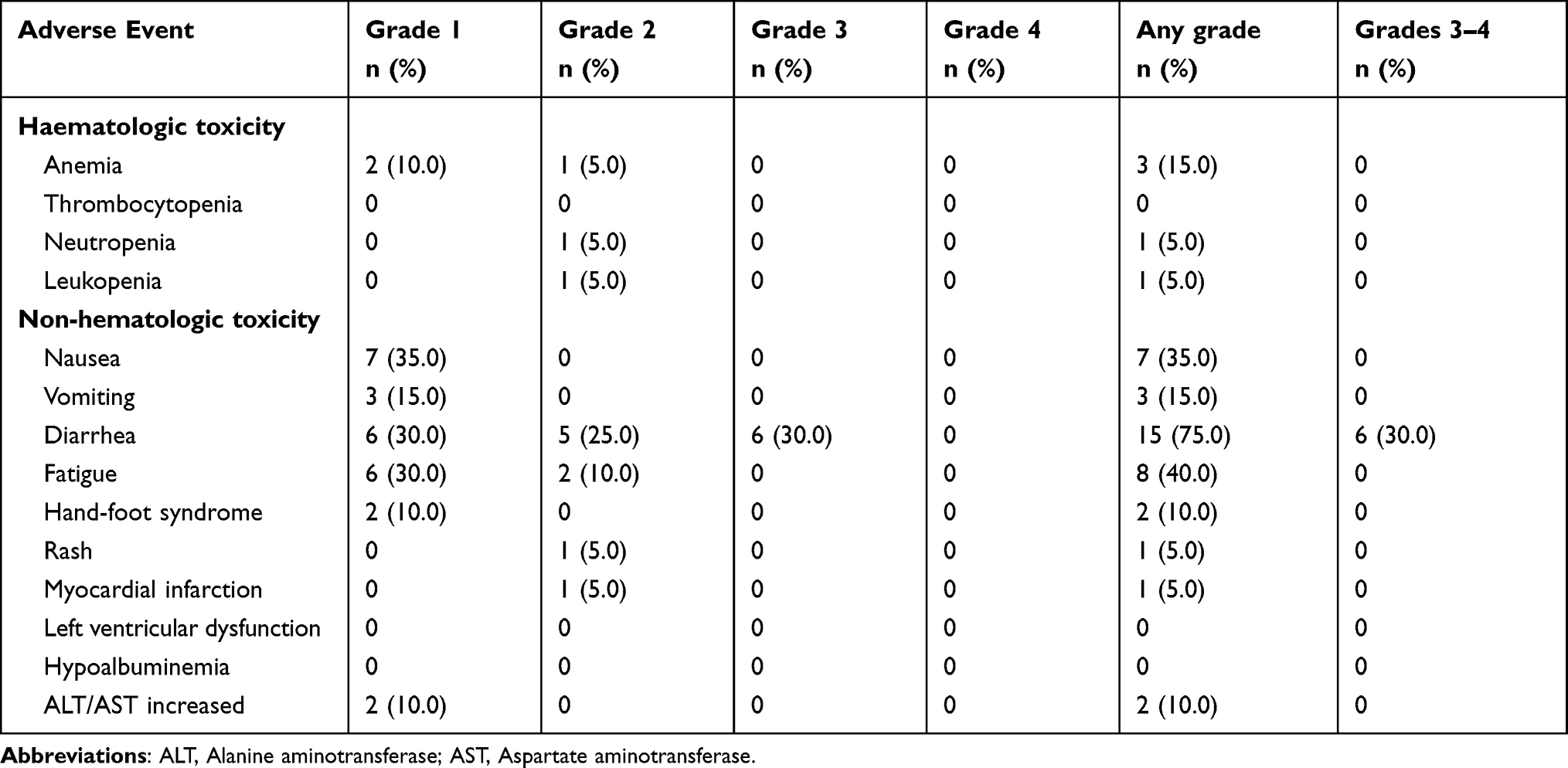 |
Table 3 Most Common Treatment-Related Adverse Events (Maximum Grade per Patient per Event) |
Exploratory Analyses
Among the 17 patients evaluable for efficacy, 2 harbored KRAS mutations, 14 were RAS/BRAF wild-type, and the gene status of 1 patient was unknown. Objective responses were exclusively observed in RAS/BRAF wild-type patients, whereas the two KRAS-mutant patients achieved SD as their best response. In the RAS/BRAF wild-type subgroup, the ORR was 28.6% and the DCR was 92.9%. As shown in Figure 2, compared to KRAS-mutant CRC patients, those with RAS/BRAF wild-type CRC exhibited significantly longer median PFS (8.5 vs 2.6 months; P = 0.0081) and median OS (22.6 vs 4.9 months; P = 0.022). Univariate logistic analysis revealed no significant associations between clinical variables and ORR in HER2-positive RAS/BRAF wild-type CRC patients (all P > 0.05) (Supplementary Table S1).
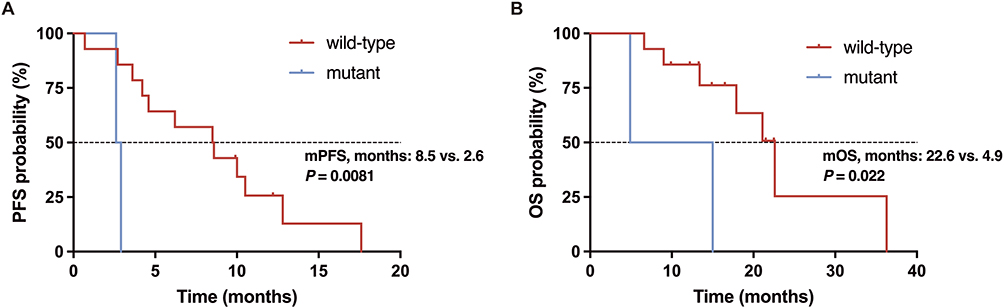 |
Figure 2 Subgroup analysis based on RAS/BRAF mutation status. (A) Kaplan-Meier curves of PFS for patients of different RAS/BRAF mutation status. (B) Kaplan-Meier curves of OS for patients of different RAS/BRAF mutation status. |
Discussion
Colorectal cancer ranks among the most prevalent gastrointestinal malignancies. Recent advances in precision medicine concepts and diagnostic techniques have progressively heightened clinical interest in HER2-positive CRC. Developing a unified diagnostic criterion for HER2 positivity in CRC has been challenging due to the low prevalence of HER2-positive cases. While tumor cell staining is objectively observable, the positivity threshold (cut-off value) is a clinically defined parameter, the selection of which is directly influenced by the intended therapeutic approach. Valtorta et al identified highly homogeneous HER2 expression patterns in CRC (distinct from gastric cancer) through IHC/FISH analysis of 1000 specimens, with >50% tumor cell overexpression in most positive cases.32 Consequently, the study defined HER2 positivity in CRC as either: (1) HER2 IHC 3+ in >50% of tumor cells, or (2) HER2 IHC 2+ with HER2/CEP17 ratio ≥2 in >50% of tumor cells—establishing the HERACLES criteria. In 2020, a study comparing ToGA gastric criteria with HERACLES in CRC showed almost identical positivity rates (2.9% vs 2.6%), confirming HER2 expression homogeneity.33 These data suggest the gastric cancer threshold (>10% IHC 3+ cells) may be clinically applicable for CRC HER2 testing.
Although HER2 alterations occur in only 5–10% of CRC cases, the large absolute number of CRC patients renders precision therapeutic strategies for this subgroup critically significant for improving clinical outcomes. Preclinical and early clinical data suggest dual HER2 blockade may confer clinical benefit in HER2-positive colorectal cancer. In the present study, we investigated the antitumor activity of trastuzumab plus pyrotinib in patients with HER2-positive mCRC who progressed on second-line standard therapy.
In recent years, HER2-overexpressed/amplified mCRC has emerged as a key focus in clinical research. Multiple therapeutic strategies have been evaluated in patients who failed standard therapy, including: Trastuzumab plus lapatinib (HERACLES-A),34 Trastuzumab plus pertuzumab (MyPathway),23 Trastuzumab plus tucatinib (MOUNTAINEER),24 Trastuzumab deruxtecan (DESTINY-CRC01),35 Pertuzumab plus T-DM1 (HERACLES-B),36 etc. In the HERACLES-A trial, trastuzumab plus lapatinib achieved a 28% ORR, median PFS of 4.7 months, and median OS of 10.0 months in chemotherapy-refractory, HER2-positive/KRAS wild-type mCRC patients.34 The MyPathway trial evaluated trastuzumab plus pertuzumab in HER2-positive mCRC, demonstrating a 32% ORR. Subgroup analysis revealed significantly inferior outcomes in KRAS-mutant versus wild-type patients: median PFS (1.4 vs 5.3 months) and median OS (8.5 vs 14.0 months).23 These findings support prioritizing dual anti-HER2 therapy for HER2-amplified mCRC with RAS/BRAF wild-type status. Similarly, our study demonstrated significantly superior efficacy and survival outcomes in RAS/BRAF wild-type versus KRAS-mutant mCRC patients: ORR 28.6% vs 0, median PFS 8.5 vs 2.6 months, and median OS 22.6 vs 4.9 months. Notably, both KRAS-mutated mCRC patients failed to respond to trastuzumab plus pyrotinib therapy, achieving only stable disease.
Recent phase II trials—MOUNTAINEER24 and DESTINY-CRC0135—demonstrated significant anti-tumor activity in pretreated HER2-positive RAS/BRAF wild-type mCRC. These findings supported the inclusion of two novel regimens in NCCN guidelines: trastuzumab plus tucatinib (a highly selective HER2 TKI) and T-DXd (an ADC linking trastuzumab to a topoisomerase I inhibitor payload). These small-sample phase II studies were all explorative and reported heterogeneous efficacy outcomes. Among HER2-positive RAS/BRAF wild-type patients, ORR ranges from 10% to 45%, mPFS ranges from 3.1 to 8.2 months, and mOS from 11 to 24.1 months.
In China, efficacy data on anti-HER2 therapy for HER2-positive colorectal cancer remain limited. According to the NCCN guidelines, the 2020 Chinese Society of Clinical Oncology (CSCO) Guidelines for Diagnosis and Treatment of Colorectal Cancer incorporated recommendations for anti-HER2 therapy in the third-line or later treatment of CRC. Pyrotinib, a China-developed pan-HER TKI, selectively inhibits HER1, HER2, and HER4 tyrosine kinases. PHOEBE trial results confirmed pyrotinib’s advantage over lapatinib when combined with capecitabine for HER2-positive metastatic breast cancer improved ORR (79% vs 57%), nearly tripled median PFS (18.1 vs 7.0 months), and significantly reduced risk of death (HR 0.36)—these outcomes position pyrotinib as a more potent anti-HER2 TKI.27 A case report documented prolonged PFS with pyrotinib monotherapy in a heavily pretreated HER2-positive mCRC patient.37 Collectively, these findings position trastuzumab plus pyrotinib as a promising therapeutic strategy for heavily pretreated HER2-positive mCRC, potentially addressing the unmet need in third-line and beyond settings.
In recent years, two phase II trials preliminarily verified pyrotinib-trastuzumab efficacy in HER2-positive mCRC. A multicenter study38 demonstrated an ORR of 22.2% with acceptable safety, while the HER2-FUSCC-G trial39 reported higher antitumor activity (ORR 50.0%; median PFS 7.53 months; OS 16.8 months), collectively confirming the regimen’s therapeutic potential. The results of the present study demonstrated an ORR of 23.5% in the overall cohort and 28.6% in the RAS wild-type subgroup, aligning with previously reported efficacy of dual anti-HER2 therapies. These results further support the clinical application of trastuzumab plus pyrotinib in later-line treatment for HER2-positive mCRC patients.
The safety profile in our cohort aligned with established pyrotinib toxicity data. Diarrhea was the most frequent grade 3 TRAE (30%), effectively managed through dose reduction. One patient with pre-existing coronary artery disease experienced a grade 2 myocardial infarction following the first dose. Given the patient’s cardiovascular history, a definite link between the study drug and myocardial infarction could not be established. Two previous similar studies investigating trastuzumab plus pyrotinib reported grade 3–4 diarrhea incidences of 65% and 25%, respectively.38,39 Broader experience from pyrotinib-based trials across solid tumors shows this toxicity occurring in 16.7–45% of patients.27,40,41 In the future, prophylactic loperamide administration is recommended during pyrotinib-containing regimens to mitigate the incidence and severity of treatment-related diarrhea in clinical practice.
The clinical utility of anti-HER2 therapy in later-line treatment for HER2-positive mCRC has been established. In the future, anti-HER2 therapy may extend to neoadjuvant, adjuvant, and first-line settings for colorectal cancer patients with HER2 amplification or overexpression. This strategic shift is being evaluated in the MOUNTAINEER-3 study—a randomized Phase III trial comparing first-line trastuzumab + tucatinib + mFOLFOX6 versus standard of care (mFOLFOX6 plus cetuximab or bevacizumab) in RAS wild-type, HER2-positive mCRC.42 Positive outcomes may establish HER2-targeted regimens as frontline therapy, embodying precision oncology principles throughout the cancer care continuum. Furthermore, the combined assessment of HER2 amplification with other biomarkers may significantly improve therapeutic outcomes in CRC. Previous studies indicated that HER2 positivity correlates with limited efficacy of anti-EGFR therapies. Therefore, integrating HER2 and RAS/BRAF mutation testing can identify patients likely resistant to anti-EGFR agents and guide personalized treatment strategies. Furthermore, HER2 crosstalk with other signaling pathways warrants further investigation to elucidate potential synergistic therapeutic effects.
Deeper mechanistic insights into HER2 signaling in CRC drive the development of novel targeted agents as a priority research trajectory. Zanidatamab (ZW25), a bispecific anti-HER2 antibody engaging both trastuzumab and pertuzumab binding epitopes, has demonstrated clinical activity in a Phase I study43 and is under evaluation in phase II trials (NCT02892123; NCT03929666). ZW49, an ADC linking zanidatamab to an auristatin payload, shows potent preclinical efficacy and is being assessed in an ongoing phase I trial (NCT03821233). HER2-targeted immunotherapeutic strategies are under investigation. These include combination regimens with anti-HER2 therapies and immune checkpoint inhibitors (NCT05493683, NCT05333809, NCT05193292), as well as cellular therapy (eg, chimeric antigen receptor (CAR) T cells,44 CAR macrophages,45 and natural killer (NK) cells).46
In terms of limitations, first, the absence of a control arm and limited sample size restrict subgroup comparisons across HER2 profiles or other oncogenes. Validation of pyrotinib-trastuzumab efficacy in HER2-positive mCRC and population selection requires larger controlled studies. Second, clinical data for HER2-mutated (non-amplified) mCRC are absent—only one case with dual HER2 mutation/amplification was observed. Despite preclinical sensitivity in PDX models,47 anti-HER2 efficacy in pure HER2-mutated disease remains unverified clinically. Third, during the COVID-19 pandemic, patient enrollment was slow, prolonging the study timeline (December 2019 to March 2025) and causing significant patient follow-up challenges. Furthermore, post-hoc subgroup analyses (unplanned per protocol) yield exploratory insights needing prospective confirmation.
In conclusion, the trastuzumab and pyrotinib regimen was well-tolerated and demonstrated promising antitumor activity in HER2-positive mCRC, particularly in RAS/BRAF wild-type patients. This dual anti-HER2 therapy may offer an alternative option and warrants further investigation.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, Yongkun Sun, upon reasonable request.
Acknowledgment
We thank all participants and medical personnel involved in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by National High Level Hospital Clinical Research Funding and Beijing Hope Run Special Fund of Cancer Foundation of China (LC2022A10) and Beijing Xisike Clinical Oncology Research Foundation (Y-HR2019-0285).
Disclosure
The authors declare that they have no conflict of interest.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Han B, Zheng R, Zeng H, et al. Cancer incidence and mortality in China, 2022. J Natl Cancer Cent. 2024;4(1):47–53. doi:10.1016/j.jncc.2024.01.006
3. Miller KD, Nogueira L, Mariotto AB, et al. Cancer treatment and survivorship statistics, 2019. CA Cancer J Clin. 2019;69(5):363–385. doi:10.3322/caac.21565
4. Xi Y, Xu P. Global colorectal cancer burden in 2020 and projections to 2040. Transl Oncol. 2021;14(10):101174. doi:10.1016/j.tranon.2021.101174
5. Strickler JH, Yoshino T, Graham RP, Siena S, Bekaii-Saab T. Diagnosis and treatment of ERBB2-positive metastatic colorectal cancer: a review. JAMA Oncol. 2022;8(5):760–769. doi:10.1001/jamaoncol.2021.8196
6. Ruan DY, Wu HX, Xu Y, et al. Garsorasib, a KRAS G12C inhibitor, with or without cetuximab, an EGFR antibody, in colorectal cancer cohorts of a phase II trial in advanced solid tumors with KRAS G12C mutation. Signal Transduct Target Ther. 2025;10(1):189. doi:10.1038/s41392-025-02274-z
7. Hynes NE, Lane HA. ERBB receptors and cancer: the complexity of targeted inhibitors. Nat Rev Cancer. 2005;5(5):341–354. doi:10.1038/nrc1609
8. Yan M, Parker BA, Schwab R, Kurzrock R. HER2 aberrations in cancer: implications for therapy. Cancer Treat Rev. 2014;40(6):770–780. doi:10.1016/j.ctrv.2014.02.008
9. Bruni S, Mauro FL, Proietti CJ, et al. Blocking soluble TNFα sensitizes HER2-positive breast cancer to trastuzumab through MUC4 downregulation and subverts immunosuppression. J Immunother Cancer. 2023;11(3):e005325. doi:10.1136/jitc-2022-005325
10. Ebert K, Haffner I, Zwingenberger G, et al. Combining gene expression analysis of gastric cancer cell lines and tumor specimens to identify biomarkers for anti-HER therapies-the role of HAS2, SHB and HBEGF. BMC Cancer. 2022;22(1):254. doi:10.1186/s12885-022-09335-4
11. Cancer Genome Atlas Network. Comprehensive molecular characterization of human colon and rectal cancer. Nature. 2012;487(7407):330–337. doi:10.1038/nature11252
12. Sawada K, Nakamura Y, Yamanaka T, et al. Prognostic and predictive value of HER2 amplification in patients with metastatic colorectal cancer. Clin Colorectal Cancer. 2018;17(3):198–205. doi:10.1016/j.clcc.2018.05.006
13. Ross JS, Fakih M, Ali SM, et al. Targeting HER2 in colorectal cancer: the landscape of amplification and short variant mutations in ERBB2 and ERBB3. Cancer. 2018;124(7):1358–1373. doi:10.1002/cncr.31125
14. Punt CJ, Koopman M, Vermeulen L. From tumour heterogeneity to advances in precision treatment of colorectal cancer. Nat Rev Clin Oncol. 2017;14(4):235–246. doi:10.1038/nrclinonc.2016.171
15. Salem ME, Weinberg BA, Xiu J, et al. Comparative molecular analyses of left-sided colon, right-sided colon, and rectal cancers. Oncotarget. 2017;8(49):86356–86368. doi:10.18632/oncotarget.21169
16. Cavanna L, Seghini P, Di Nunzio C, et al. Gastric cancer with brain metastasis and the role of human epidermal growth factor 2 status. Oncol Lett. 2018;15(4):5787–5791. doi:10.3892/ol.2018.8054
17. Martin AM, Cagney DN, Catalano PJ, et al. Brain metastases in newly diagnosed breast cancer: a population-based study. JAMA Oncol. 2017;3(8):1069–1077. doi:10.1001/jamaoncol.2017.0001
18. Li JL, Lin SH, Chen HQ, et al. Clinical significance of HER2 and EGFR expression in colorectal cancer patients with ovarian metastasis. BMC Clin Pathol. 2019;19:3. doi:10.1186/s12907-019-0085-8
19. Raghav K, Loree JM, Morris JS, et al. Validation of HER2 amplification as a predictive biomarker for anti-epidermal growth factor receptor antibody therapy in metastatic colorectal cancer. JCO Precis Oncol. 2019;3:1–13. doi:10.1200/PO.18.00226
20. Yonesaka K, Zejnullahu K, Okamoto I, et al. Activation of ERBB2 signaling causes resistance to the EGFR-directed therapeutic antibody cetuximab. Sci Transl Med. 2011;3(99):99ra86. doi:10.1126/scitranslmed.3002442
21. Chen N, He L, Zou Q, Deng H. HER2 targeted therapy in colorectal cancer: current landscape and future directions. Biochem Pharmacol. 2024;223:116101. doi:10.1016/j.bcp.2024.116101
22. Sartore-Bianchi A, Trusolino L, Martino C, et al. Dual-targeted therapy with trastuzumab and lapatinib in treatment-refractory, KRAS codon 12/13 wild-type, HER2-positive metastatic colorectal cancer (HERACLES): a proof-of-concept, multicentre, open-label, Phase 2 trial. Lancet Oncol. 2016;17(6):738–746. doi:10.1016/S1470-2045(16)00150-9
23. Meric-Bernstam F, Hurwitz H, Raghav KPS, et al. Pertuzumab plus trastuzumab for HER2-amplified metastatic colorectal cancer (MyPathway): an updated report from a multicentre, open-label, phase 2a, multiple basket study. Lancet Oncol. 2019;20(4):518–530. doi:10.1016/S1470-2045(18)30904-5
24. Strickler JH, Cercek A, Siena S, et al. Tucatinib plus trastuzumab for chemotherapy-refractory, HER2-positive, RAS wild-type unresectable or metastatic colorectal cancer (MOUNTAINEER): a multicentre, open-label, phase 2 study. Lancet Oncol. 2023;24(5):496–508. doi:10.1016/S1470-2045(23)00150-X
25. Siena S, Di Bartolomeo M, Raghav K, et al. Trastuzumab deruxtecan (DS-8201) in patients with HER2-expressing metastatic colorectal cancer (DESTINY-CRC01): a multicentre, open-label, phase 2 trial. Lancet Oncol. 2021;22(6):779–789. doi:10.1016/S1470-2045(21)00086-3
26. Ma F, Ouyang Q, Li W, et al. Pyrotinib or lapatinib combined with capecitabine in HER2-positive metastatic breast cancer with prior taxanes, anthracyclines, and/or trastuzumab: a randomized, phase II study. J Clin Oncol. 2019;37(29):2610–2619. doi:10.1200/JCO.19.00108
27. Xu B, Yan M, Ma F, et al. Pyrotinib plus capecitabine versus lapatinib plus capecitabine for the treatment of HER2-positive metastatic breast cancer (PHOEBE): a multicentre, open-label, randomised, controlled, Phase 3 trial. Lancet Oncol. 2021;22(3):351–360. doi:10.1016/S1470-2045(20)30702-6
28. Zhu W, Wu J, Cui M, Zhang L. Durable clinical benefit from pyrotinib combined with carboplatin in HER2-positive relapsed breast cancer previously treated with taxanes, anthracyclines, and trastuzumab. Ann Palliat Med. 2020;9(5):3684–3689. doi:10.21037/apm-20-1363
29. Zhou C, Li X, Wang Q, et al. Pyrotinib in HER2-mutant advanced lung adenocarcinoma after platinum-based chemotherapy: a multicenter, open-label, single-arm, phase II study. J Clin Oncol. 2020;38(24):2753–2761. doi:10.1200/JCO.20.00297
30. Li X, Gu X, Xu J, et al. Sustained clinical benefit of pyrotinib combined with capecitabine rescue therapy after trastuzumab resistance in HER2-positive advanced gastric cancer: a case report. Onco Targets Ther. 2021;14:3983–3989. doi:10.2147/OTT.S310421
31. Waks AG, Martínez-Sáez O, Tarantino P, et al. Dual HER2 inhibition: mechanisms of synergy, patient selection, and resistance. Nat Rev Clin Oncol. 2024;21(11):818–832. doi:10.1038/s41571-024-00939-2
32. Valtorta E, Martino C, Sartore-Bianchi A, et al. Assessment of a HER2 scoring system for colorectal cancer: results from a validation study. Mod Pathol. 2015;28(11):1481–1491. doi:10.1038/modpathol.2015.98
33. Liu F, Ren C, Jin Y, et al. Assessment of two different HER2 scoring systems and clinical relevance for colorectal cancer. Virchows Arch. 2020;476(3):391–398. doi:10.1007/s00428-019-02668-9
34. Tosi F, Sartore-Bianchi A, Lonardi S, et al. Long-term clinical outcome of trastuzumab and lapatinib for HER2-positive metastatic colorectal cancer. Clin Colorectal Cancer. 2020;19(4):256–262.e2. doi:10.1016/j.clcc.2020.06.009
35. Yoshino T, Di Bartolomeo M, Raghav K, et al. Final results of DESTINY-CRC01 investigating trastuzumab deruxtecan in patients with HER2-expressing metastatic colorectal cancer. Nat Commun. 2023;14(1):3332. doi:10.1038/s41467-023-38032-4
36. Sartore-Bianchi A, Lonardi S, Martino C, et al. Pertuzumab and trastuzumab emtansine in patients with HER2-amplified metastatic colorectal cancer: the phase II HERACLES-B trial. ESMO Open. 2020;5(5):e000911. doi:10.1136/esmoopen-2020-000911
37. Li HS, Yang LL, Zhang MY, Cheng K, Chen Y, Liu JY. Remarkable response of EGFR- and HER2-amplified metastatic colon cancer to pyrotinib after failed multiline treatments: a case report and literature review. Front Oncol. 2020;10:548867. doi:10.3389/fonc.2020.548867
38. Fu X, Ying J, Yang L, et al. Dual targeted therapy with pyrotinib and trastuzumab for HER2-positive advanced colorectal cancer: a phase 2 trial. Cancer Sci. 2023;114(3):1067–1074. doi:10.1111/cas.15660
39. Chang J, Xu M, Wang C, et al. Dual HER2 targeted therapy with pyrotinib and trastuzumab in refractory HER2 positive metastatic colorectal cancer: a result from HER2-FUSCC-G study. Clin Colorectal Cancer. 2022;21(4):347–353. doi:10.1016/j.clcc.2022.07.003
40. Song Z, Li Y, Chen S, et al. Efficacy and safety of pyrotinib in advanced lung adenocarcinoma with HER2 mutations: a multicenter, single-arm, phase II trial. BMC Med. 2022;20(1):42. doi:10.1186/s12916-022-02245-z
41. Xuhong J, Qi X, Tang P, et al. Neoadjuvant pyrotinib plus trastuzumab and chemotherapy for stage I-III HER2-positive breast cancer: a phase II clinical trial. Oncologist. 2020;25(12):e1909–e1920. doi:10.1002/onco.13546
42. Strickler JH, Bekaii-Saab T, Cercek A, et al. MOUNTAINEER-03 phase III study design: first-line mFOLFOX6 + tucatinib + trastuzumab for HER2+ metastatic colorectal cancer. Future Oncol. 2025;21(3):303–311. doi:10.1080/14796694.2024.2441101
43. Meric-Bernstam F, Beeram M, Hamilton E, et al. Zanidatamab, a novel bispecific antibody, for the treatment of locally advanced or metastatic HER2-expressing or HER2-amplified cancers: a Phase 1, dose-escalation and expansion study. Lancet Oncol. 2022;23(12):1558–1570. doi:10.1016/S1470-2045(22)00621-0
44. Xu J, Meng Q, Sun H, et al. HER2-specific chimeric antigen receptor-T cells for targeted therapy of metastatic colorectal cancer. Cell Death Dis. 2021;12(12):1109. doi:10.1038/s41419-021-04100-0
45. Sloas C, Gill S, Klichinsky M. Engineered CAR-macrophages as adoptive immunotherapies for solid tumors. Front Immunol. 2021;12:783305. doi:10.3389/fimmu.2021.783305
46. Li HK, Hsiao CW, Yang SH, et al. A novel off-the-shelf trastuzumab-armed NK cell therapy (ACE1702) using antibody-cell-conjugation technology. Cancers. 2021;13(11).
47. Kavuri SM, Jain N, Galimi F, et al. HER2 activating mutations are targets for colorectal cancer treatment. Cancer Discov. 2015;5(8):832–841. doi:10.1158/2159-8290.CD-14-1211
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.