Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Putting Lived Experience at the Centre: A Critical Review of Multidisciplinary, Person-Centred Mental Health Care
Authors Grattidge L ![]() , Haywood D, Hart NH
, Haywood D, Hart NH ![]() , Hamilton BE, Fossey E, Petrakis M, Castle DJ
, Hamilton BE, Fossey E, Petrakis M, Castle DJ
Received 1 February 2026
Accepted for publication 29 April 2026
Published 18 May 2026 Volume 2026:19 600579
DOI https://doi.org/10.2147/JMDH.S600579
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Laura Grattidge,1– 3 Darren Haywood,4– 8 Nicolas H Hart,4,9– 12 Bridget Elizabeth Hamilton,5,13,14 Ellie Fossey,15 Melissa Petrakis,5,15 David J Castle3,5
1Centre for Rural Health, University of Tasmania, Launceston, TAS, Australia; 2Manna Institute, Armidale, NSW, Australia; 3Tasmanian Centre for Mental Health Service Innovation, School of Medicine, University of Tasmania, Hobart, TAS, Australia; 4Human Performance Research Centre, INSIGHT Research Institute, Faculty of Health, University of Technology Sydney, Sydney, NSW, Australia; 5Department of Mental Health, St. Vincent’s Hospital Melbourne, Melbourne, VIC, Australia; 6Department of Psychiatry, Melbourne Medical School, Dentistry and Health Sciences, University of Melbourne, Melbourne, VIC, Australia; 7School of Population Health, Faculty of Health Sciences, Curtin University, Perth, WA, Australia; 8Centre for Mental Health and Brain Sciences, Department of Psychological Sciences, Swinburne University of Technology, Melbourne, VIC, Australia; 9Caring Futures Institute, College of Nursing and Health Sciences, Flinders University, Adelaide, SA, Australia; 10Cancer and Palliative Care Outcomes Centre, Faculty of Health, Queensland University of Technology, Brisbane, QLD, Australia; 11Exercise Medicine Research Institute, School of Medical and Health Sciences, Edith Cowan University, Perth, WA, Australia; 12Institute for Health Research, University of Notre Dame Australia, Perth, WA, Australia; 13The ALIVE National Centre, Medicine, Dentistry and Health Sciences, University of Melbourne, Melbourne, VIC, Australia; 14Centre for Mental Health Nursing, University of Melbourne, Melbourne, VIC, Australia; 15School of Primary and Allied Health Care, Faculty of Medicine, Nursing and Health Sciences, Monash University, Melbourne, VIC, Australia
Correspondence: David J Castle, Tasmanian Centre for Mental Health Service Innovation, School of Psychological Sciences University of Tasmania, Hobart, TAS, Australia, Email [email protected]
Purpose: Person-centred care is widely endorsed in mental health policy yet remains inconsistently enacted in multidisciplinary practice, particularly where services default to diagnostic dominance, risk management, and service-led priorities. This critical review examines what is required to operationalise person-centred, rights-based care across disciplines and settings, positioning lived and living experience as core expertise rather than a supplementary perspective and considering implications for suicide prevention.
Methods: A critical review of peer-reviewed and grey literature was undertaken, focusing on person-centred and multidisciplinary mental health care. Five commonly used approaches were compared: the Optimal Health Program, the Strengths Model, Open Dialogue, traditional case management, and Behaviour Support Planning. Models were examined against mechanisms consistently associated with high-quality care, including supported decision-making, shared formulation, relational continuity, lived experience leadership, integration of physical and social determinants of health, and management of coercion risk in acute settings.
Results: Alignment with person-centred, rights-based care was strongest when supported decision-making was routine rather than discretionary, care was relational and meaning-oriented and lived and living experience leadership was embedded with formal authority and resourcing. Approaches that are easier to standardise and scale were more likely to drift toward managerial and task-focused practices unless deliberately redesigned to protect agency, relational safety, and person-defined goals. These mechanisms were particularly important for suicide prevention and for people experiencing intersecting vulnerabilities, including trauma, disability, chronic physical illness, substance use, housing insecurity, family violence, racism, stigma, justice involvement, neurodivergence, and geographic isolation.
Conclusion: Rather than advocating a single branded model, this review supports a shift toward system-wide mechanisms and minimum standards that travel with the person across settings. Prioritising supported decision-making, shared formulation, relational continuity, equity-oriented responses, and lived and living experience governance offers a practical pathway to make person-centred care more consistent, accountable, and safer, particularly in acute, crisis, and rural contexts, to embed suicide prevention within everyday multidisciplinary practice.
Plain Language Summary: Mental health services often say they provide person-centred care. This means care should respect a person’s goals, values, and life context. In reality, many services still focus mainly on diagnosis, risk management, and system rules. This can leave people feeling unheard, especially during crisis or hospital care. This review explores what factors help multidisciplinary mental health teams (teams made up of different professions) deliver care that is genuinely led by the person.
To achieve this, research papers, policy documents, and practice frameworks were compared as to how well they support key elements of person-centred care. Five common approaches used in services, including programs focused on strengths, self-management, dialogue with families and networks, care coordination, and behaviour support planning, were additionally compared.
Findings highlight that good care does not depend on choosing the “right” branded model, rather a small set of practices that should happen everywhere. These include:
● Supporting people to make their own decisions, with help if needed
● Building shared understandings of a person’s experiences, strengths, and life situation, not just symptoms
● Maintaining trusting relationships across service changes
● Including people with lived and living experience in leadership roles
● Addressing physical health, housing, safety, and social connection as part of care
These practices are also critical for suicide prevention. When people feel listened to, respected, and involved in decisions, they are more likely to seek help early, talk about suicidal thoughts, and stay connected to support. When services protect these practices, people are more likely to feel respected, safe, and involved. Findings support system changes that make these person-centred practices standard, not optional.
Keywords: person-centred care, multidisciplinary teams, lived and living experience, recovery-oriented practice, mental health services, suicide prevention
Introduction
Person-centred care has become a dominant organising principle within contemporary mental health policy, service reform, and professional standards. Across jurisdictions, it is routinely used to signal commitments to recovery, autonomy, partnership, and holistic care. There is, however, growing recognition that the translation of person-centred principles into everyday multidisciplinary practice remains inconsistent and uneven.1,2 In many settings, care continues to be shaped primarily by service imperatives, diagnostic categorisation, and risk management frameworks, with limited attention to how power, language, and decision-making are negotiated within multidisciplinary teams.3,4 Further, across resource constrained public services, homogenised rather than personalised responses continue to grow, in the pursuit of efficiency.5
Person-centred care is also not universally defined or experienced. Its application is shaped by cultural understandings of identity, autonomy, and decision-making. Western individualised models may not align with collectivist or Indigenous perspectives that prioritise family, community, and connection to culture and land.6,7 Without explicit attention to these differences, person-centred care risks reinforcing dominant norms and failing to respond to diverse needs. Recent literature therefore emphasises culturally responsive and contextually grounded approaches.8,9
Multidisciplinary care is often positioned as inherently person-centred, yet the presence of multiple professional disciplines does not guarantee alignment with a person’s values, preferences, or lived realities. Evidence suggests that without explicit mechanisms for shared decision-making, relational continuity, and accountability to the person’s goals, multidisciplinary teams risk reproducing professional silos and hierarchical decision-making, even while adopting recovery-oriented or person-centred language.10,11 In practice, these dynamics are shaped by differences in disciplinary authority, language, and problem framing. For example, psychiatric perspectives may prioritise diagnosis, medication, and risk management, while social work and lived experience perspectives emphasise context, relationships, and structural determinants. Likewise, occupational therapy perspective may foreground everyday living and community participation,12 and nursing perspectives may attend to lay and embodied experiences and meaning making.13 When these approaches are not integrated, care can become fragmented or parallel, with decisions reflecting professional hierarchies rather than person-defined goals.2 Service users frequently describe not being heard and having their priorities overridden in favour of clinical or organisational imperatives.11,14 Examining how specific disciplines contribute to, and can actively shift, these dynamics is therefore critical. Understanding where power sits, how knowledge is valued, and how decisions are made across disciplines provides a practical pathway for addressing imbalances and strengthening genuinely person-centred multidisciplinary care.
Research is increasingly focusing on this gap between policy intent and lived and living experience. Studies show that people continue to report coercion, fragmentation, and limited involvement in care decisions despite system-level commitments to recovery.15–17 As a result, the literature is shifting from describing models of care to identifying the mechanisms required to embed person-centred practice, including supported decision-making, relational safety, and lived and living experience leadership.18,19 This review is written from an explicitly person-centred and lived and living experience-led position. Lived and living experience is conceptualised not as an adjunct perspective or supplementary workforce role, but as a core form of expertise that informs how mental health care is conceptualised, delivered, and evaluated.1,20 This position aligns with rights-based frameworks, including the United Nations Convention on the Rights of Persons with Disabilities, which emphasise autonomy, participation, and equality of knowledge between people who use services and professionals.18,21 The authorship team brings together disciplinary expertise from psychiatry, psychology, mental health nursing, occupational therapy, social work, exercise physiology, and lived and living experience leadership. This positionality is deliberate. Each author contributes deep discipline-specific knowledge of assessment, intervention, and system constraints, while also engaging critically with the limitations of discipline-led models when applied in isolation. The inclusion of lived and living experience leadership within the author group reflects an epistemological commitment to valuing experiential knowledge alongside professional and academic expertise, and to interrogating how multidisciplinary models are experienced by those who receive care, not only those who deliver it.22,23 Importantly, the review is not intended to promote a single preferred model of care. Instead, it synthesises peer-reviewed and grey literature on established person-centred and multidisciplinary models to examine how different approaches address, or fail to address, key elements consistently identified as central to high-quality mental health care. These include supported decision-making, relational continuity, lived and living experience leadership, integration of physical and social determinants of health, and mechanisms for multidisciplinary collaboration.18,19 By explicitly foregrounding author positionality and lived and living experience leadership, this review seeks to move beyond descriptive accounts of models toward a more critical examination of how person-centred care is enacted in practice. In doing so, it aims to support clinicians, service leaders, and policymakers to identify the principles, mechanisms, and conditions required for multidisciplinary mental health care that is not only coordinated but genuinely person-led, ethical, and responsive to the complexity of people’s lives.
There remains limited cross-disciplinary synthesis of how these mechanisms operate within real-world multidisciplinary care, particularly in acute and crisis settings where risk, time pressure, and system constraints are most pronounced. Existing literature tends to examine models or interventions in isolation, with less attention to how person-centred care is enacted across disciplines and settings, and what enables or constrains its implementation in practice.17,24 This review addresses this gap by focusing on the mechanisms that support or undermine person-centred multidisciplinary care across contexts. This includes a specific focus on how these mechanisms function as suicide prevention practices within everyday care, particularly in high-risk environments such as emergency departments, inpatient units, and rural or resource-constrained settings, where opportunities for early intervention are often missed.
Methods
Review Approach
This paper used a critical review approach to examine how person-centred care is conceptualised and enacted within multidisciplinary mental health practice. A purposive and theory-informed approach was taken to synthesise peer-reviewed and grey literature relevant to contemporary mental health systems, workforce design, and service reform. The review adopts a critical orientation, drawing on approaches that examine underlying assumptions, power dynamics, and gaps between policy intent and practice.25,26 This included consideration of how dominant diagnostic and risk-based frameworks shape care, and how alternatives such as supported decision-making and lived and living experience leadership are operationalised within practice.
This approach was selected because person-centred care, supported decision-making, and lived and living experience leadership cut across disciplines, settings, and policy domains, and are not well captured through narrowly defined intervention studies alone. A critical review using a narrative approach enables integration of empirical evidence, conceptual frameworks, implementation research, and lived and living experience scholarship, consistent with the multidisciplinary focus of this journal.
Review Questions
The review was guided by the following questions:
- How is person-centred care conceptualised within contemporary multidisciplinary mental health literature, and where do gaps emerge between policy intent and practice?
- What models of care are most commonly framed as person-centred in multidisciplinary mental health systems, and what assumptions do they make about power, agency, and decision-making?
- How do these models support or constrain supported decision-making, lived and living experience leadership, and attention to social and physical determinants of health?
- What are the implications for workforce design, governance, and service reform, particularly for people experiencing intersecting vulnerabilities?
Literature Sources and Selection
Peer-reviewed literature was identified through targeted searches of PubMed, PsycINFO, and Google Scholar using combinations of terms including person-centred care, recovery-oriented practice, supported decision-making, multidisciplinary mental health, lived and living experience, and peer workforce. Searches were iterative rather than exhaustive and refined as key themes emerged. Grey literature was intentionally included due to its central role in shaping mental health policy and practice. Sources included national and international policy documents, workforce guidelines, implementation reports, and frameworks published by organisations such as the National Mental Health Commission, Roses in the Ocean, Substance Abuse and Mental Health Services Administration, and the United Nations. Reference lists of key papers were hand-searched to identify additional relevant sources.
Models and Analytic Focus
Five models were selected for focused comparison: the Optimal Health Program, the Strengths Model, Open Dialogue, traditional case management, and Behaviour Support Planning approaches (to be further defined). These models were selected due to their prominence in the literature, widespread use across settings, and the way they reflect differing assumptions about personhood, agency, power, and multidisciplinary care. Analysis focused on features consistently identified as central to high-quality, person-centred and rights-based care, including supported decision-making, lived and living experience leadership, multidisciplinary integration, relational continuity, and attention to social and physical determinants of health, as well as their relevance to suicide prevention, including impacts on help-seeking, disclosure, engagement, and relational safety.
From Asylums to Autonomy: How Services Evolved (and Where They Stall)
Modern mental health systems were built through a series of reforms that aimed, at least in theory, to shift care from containment to community, and from paternalism to partnership. Deinstitutionalisation reduced reliance on long-stay asylums, expanded community-based services, and created new professional roles focused on psychosocial support, rehabilitation, and recovery.2 Contemporary mental health systems are often described as having progressed from institutional care to community-based, recovery-oriented, and person-centred models. While this trajectory is broadly accurate, it risks overstating the extent to which power, autonomy, and decision-making have genuinely shifted in practice. Under pressure, services can treat the person as the unit of care while sidelining relational networks, despite the centrality of trusted supporters to continuity, safety, and meaning-making.11,27 The historical evolution of mental health care from asylums, through deinstitutionalisation and community care, to the current recovery and person-centred era is summarised in Figure 1.
 |
Figure 1 From asylum to autonomy – the history of person centred care. |
Mental health reform has reshaped policy and service structures, yet people often continue to experience care as service-led rather than genuinely collaborative. Across reform phases, changes in settings have outpaced changes in ways of working, with diagnostic dominance, medico-legal risk frameworks, and organisational accountability continuing to privilege professional authority over personal knowledge.1,2,11
Despite the widespread adoption of recovery-oriented, person-centred and trauma-informed language, service logic frequently remains oriented toward risk management, throughput, and documentation rather than accountability to the person.1,27 As a result, multidisciplinary teams may function coherently while the person remains peripheral to decision-making.10 This pattern highlights that person-centred care is not primarily a matter of clinician attitude, but of system design. Supported decision-making therefore represents a necessary reframing of how power, choice, and responsibility are distributed across mental health systems, rather than an optional practice add-on.18,21,28,29 This is particularly evident in suicide prevention. System features such as fragmented care, repeated retelling of distress, and risk-driven interactions can compound vulnerability and disengagement. In contrast, continuity, relational safety, and shared understanding are associated with reduced suicide risk and improved post-crisis outcomes.30,31
Supported Decision-Making as the Foundational Spine
Supported decision-making is both a practical clinical approach and a rights-based commitment. It refers to the supports, adjustments, and relational conditions that enable people to make their own decisions about care, support, and risk, rather than decisions being made on the basis of professional authority, diagnosis, or contested assumptions about capacity.18,28,29,32 In mental health, it overlaps with shared decision-making33,34 but goes further, requiring services to actively ensure a person’s will and preferences are discoverable and actionable. It is not a single tool but a set of everyday practices using accessible language, offering balanced information about benefits and harms, checking understanding, inviting preferences, allowing time, and documenting decisions in ways that preserve narrative rather than reducing it to risk templates.33,35 It is also evident in team behaviour whether a person’s goals organise care or sit alongside a professionally driven plan. For multidisciplinary teams, supported decision-making functions as a shared governance principle, legitimising plural evidence and expertise, including medical, psychological, occupational, social, cultural, physical health, and lived and living experience knowledge. It reframes breakdowns in participation as gaps in support rather than non-compliance.18 A lived and living experience lens highlights its safety significance. People are more likely to disclose risk and return for care when they expect respect, transparency, and non-punitive responses to honesty.16,17,36 Supported decision-making is therefore not only an ethical requirement but a core suicide prevention mechanism. When people feel heard, respected, and able to influence decisions about their care, they are more likely to disclose suicidal distress, remain engaged with services, and seek help earlier, all of which are critical to reducing suicide risk.37
Why Tick-Box Diagnosis Fails Complex Lives
How mental health challenges are classified shapes assessment, formulation, treatment, and whose knowledge is prioritised. Categorical systems such as the Diagnostic and Statistical Manual of Mental Disorders (DSM) and International Classification of Diseases (ICD) provide shared language and administrative utility but have well-recognised limitations that can undermine person-centred multidisciplinary care.36,38 Comorbidity is common, raising questions about whether categories reflect distinct conditions or overlapping expressions of mental health challenges.39,40 There is also marked heterogeneity within diagnoses, with people sharing a label but having very different symptom profiles and needs.41 Tick-box approaches can narrow clinical curiosity and reinforce discipline-bound responses, particularly when physical symptoms such as sleep issues, appetite changes, and fatigue are some of the most commonly listed symptoms in the DSM and ICD.42,43 In multidisciplinary teams, diagnostic dominance can quietly create hierarchies of knowledge. Once a label is assigned, care may default to familiar pathways that prioritise symptom suppression over meaning, function, and social context. Diagnostic labels can also become identity-defining, justify coercion, or obscure complexity.
Dimensional and Formulation-Based Alternatives That Support Multidisciplinary Care
Dimensional approaches have emerged in response to the limitations of categorical diagnoses. One example is the Hierarchical Taxonomy of Psychopathology (HiTOP), which organises dimensional characteristics of mental health challenges into an empirically derived hierarchical structure.44–46 Although DSM frameworks remain more familiar, clinicians find HiTOP to be useful for formulation, treatment planning, and communication because it better reflects the complexity and overlap of real-world presentations.47
Another example is the International Classification of Functioning, Disability and Health (ICF).48 Developed to support interprofessional communication, the ICF offers less diagnostic detail than HiTOP but greater emphasis on functioning, participation, and interactions between personal, environmental, and social factors.48,49 This makes it particularly helpful for understanding people’s everyday lives, strengths, and contextual barriers in multidisciplinary care.
The value of these alternative approaches lies in enabling formulation that integrates symptoms, traits, strengths, vulnerabilities, and context. Shared formulation allows teams to hold what matters to the person, what is occurring biologically, and what is happening in their social world without collapsing complexity into a single label. This is especially important when integrating mental and physical health, and where substance use may be present.43 Dimensional and formulation-based approaches therefore better support personalised, collaborative care by focusing attention on what is most pressing, protective, and changeable for the person at a given time.
Multidisciplinary Processes That Keep Teams on Track with Supported Decision-Making
Before discussing models of care, it is important to recognise that settings may change, but ways of working often do not. Supported decision-making is shaped by team processes that operate across community services, primary care, tertiary mental health teams, emergency departments and inpatient units. Three process commitments are especially protective.
- Shared formulation as routine practice. This is a structured conversation that produces a single, evolving narrative, centred on the person’s goals and preferences, and explicit about uncertainty. It should include at least one deliberate prompt: “What does the person want, and what supports do they need to decide?”18
- Role clarity with anti-hierarchy guardrails. Multidisciplinary care fails when role boundaries are unclear and medical risk logic becomes the default tie-breaker. Teams need agreed rules for disagreement that prioritise the person’s will and preferences, and clear escalation pathways that do not automatically translate distress into control.
- Documentation that protects agency. Many services document risk exquisitely and preference poorly. Supported decision-making requires documentation that preserves the person’s narrative, choices, advance preferences, nominated supports, and specific adjustments that make participation possible.35 In practice, the systems that carry this information matter as much as the conversations. A beautifully collaborative plan that cannot be found at 2am in ED is not a plan.
These processes also reveal shifts needed in language and power. Whether the setting is a community NGO or a tertiary inpatient unit, teams can ask, are we talking about the person as an agent, or as a risk object? Are we inviting the person into decisions, or managing them around decisions?
Discipline Perspectives Within a Person-Centred Framework
Person-centred multidisciplinary care depends not simply on the presence of multiple disciplines, but on how disciplinary expertise is integrated and held accountable to the person’s goals, values, and lived realities. Each discipline carries its own epistemic habits and system pressures. The sections below highlight the distinctive contribution of each discipline to enabling agency, relational safety, and recovery, while keeping supported decision-making and shared formulation as the shared spine.
Psychiatry
Psychiatry brings essential expertise in diagnosis, medication stewardship, management of severe distress, and the interface between mental health, physical health, and neurobiology. In person-centred care, the key shift is from “psychiatry as the final arbiter” to “psychiatry as a partner in shared formulation and decision-making”. This includes using diagnostic language cautiously, acknowledging uncertainty, and treating medication as one tool among many rather than the default and sole intervention. Medication decisions are a high-stakes test of supported decision-making. Good psychiatric practice is transparent and iterative. It focuses on benefits and harms, outcomes that matter to the person, and support for preferences such as going slowly, trialing alternatives, or prioritising functioning over symptom reduction.35 Psychiatry also has a crucial role in reducing coercion by naming when restrictive practices are being driven by organisational anxiety rather than clinical necessity, and by championing advance statements, nominated persons, and decision supports as standard practice.18,50 These dynamics are particularly important in suicide prevention, where medication decisions, admission thresholds, and risk responses can shape whether a person experiences care as supportive or coercive. Collaborative, transparent approaches to risk and treatment planning are associated with improved engagement and reduced distress following crisis presentations.30
In multidisciplinary teams, there can be a tension about roles and responsibilities, with psychiatrists often seeing themselves as the clinical leaders; and it is the case that medicolegal responsibility ultimately rests with the psychiatrist. The art is for psychiatry to actively invite and perspectives from other disciplines, and to support decisions that integrate mental health, physical health, and substance use, rather than fragmenting care and threatening the integrity of team cohesion.
Psychology
Psychology is an evidence-based discipline focused on understanding cognition, emotion, and behaviour, and applying this knowledge to support mental health, wellbeing, and everyday functioning.51 In multidisciplinary mental health care, psychological practice emphasises individualised, theory-informed understandings of distress and recovery, translated into interventions responsive to each person’s context, values, and priorities.52 Psychologists contribute expertise in assessment, intervention, consultation, psychoeducation, advocacy, research, and evaluation.52,53 Practice is guided by ethical frameworks emphasising dignity, autonomy, and human rights, supporting collaborative, recovery-oriented, person-centred care and aligning with supported decision-making approaches where power, choice, and consent must be safeguarded.54
A core contribution of psychology is formulation. Psychological formulation provides a structured, hypothesis-driven synthesis of biological, psychological, and social influences on distress and functioning, supporting shared understanding of how difficulties develop and what may enable change.55 Although approaches vary, formulation is dynamic and person-centred, moving beyond diagnosis to situate symptoms within meaning, relationships, and social context, and supporting coordinated multidisciplinary decision-making.55
The therapeutic relationship is foundational. Strong working alliances characterised by trust, empathy, and collaboration are associated with improved engagement and outcomes, particularly for people with trauma histories.56 Trauma-informed principles are central to contemporary psychological practice, guided by commitments to safety, choice, collaboration, and empowerment, and oriented toward resilience rather than control.57 This extends beyond individual therapy to team practices and organisational culture, including psychological approaches to psychosis that attend to environmental and relational contributors to distress.58
Psychologists typically work within multidisciplinary teams where integration is essential. Assessments and formulations are shared to support coordinated planning and unified understandings of needs and goals.59 Psychologists contribute evidence-based perspectives in case conferences and joint decision-making while respecting other disciplines’ expertise, to align care and reduce fragmentation, particularly in complex systems. Through psychoeducation and consultation, psychologists also support teams to embed trauma-informed, recovery-oriented, and person-centred principles in everyday practice.53
Clinical Exercise Physiology
Clinical exercise physiology contributes to person-centred multidisciplinary mental health care by integrating physical health, functional capacity, and behaviour change within recovery-oriented systems. Exercise is recognised as an effective adjunctive treatment across common and severe mental health conditions. Meta-reviews and umbrella syntheses show exercise produces clinically meaningful reductions in depression, anxiety, and psychological distress,60–63 with additional benefits for cognition, social functioning, and psychosocial wellbeing in people living with severe mental illness.60,64 Exercise also operates synergistically with psychotherapy and pharmacotherapy as part of multimodal care.61,65 Mechanisms span neurobiological, psychological, and social domains, including neuroplasticity, inflammatory regulation, and enhanced self-efficacy.60
Physical and mental health are tightly interconnected. People living with mental illness experience markedly elevated cardiometabolic risk and a substantial life expectancy gap, driven by medication effects, sedentary behaviour, and inequitable access to preventive care.60,66 Exercise therefore addresses both mental health symptoms and preventable physical comorbidities, aligning with international recommendations to embed physical healthcare within mental health systems.66 This is particularly salient where metabolic conditions such as diabetes intersect with cognitive and functional impairments in severe mental illness.67
Clinical exercise physiologists apply exercise science in clinical contexts through comprehensive assessment, individualised prescription, and long-term self-management support. Professional standards emphasise person-centred care, accessibility, safety, and cultural responsiveness, positioning exercise as a therapeutic modality within chronic disease and mental health management.68,69 Behaviour change techniques are a core component of practice, supporting motivation, adherence, and sustained health behaviour change, particularly where low energy, amotivation, or cognitive challenges affect adherence to structured interventions.70,71
Within multidisciplinary teams, clinical exercise physiologists contribute expertise in safe activity prescription, physical health risk monitoring, and functional goal setting. Their inclusion strengthens shared formulation by addressing modifiable determinants of health and outcomes that people prioritise in everyday life, such as energy, sleep, confidence, and participation. This broadens recovery planning beyond symptom reduction and helps counter diagnostic dominance through attention to functional strengths and whole-person wellbeing.60,61 Despite robust evidence, exercise remains under-implemented in routine mental health services, underscoring the need for systematic integration of clinical exercise physiology within person-centred systems of care.60,66
Mental Health Nursing
As a specialist psychosocial field of nursing, mental health nursing brings relational person-centred care through the day-to-day interactions that constitute models of care and which determine whether a service is experienced as safe or coercive. Nursing practice is central to de-escalation, trauma-informed engagement, and bridging care across transitions. A foundational mental health nursing purpose is to create and maintain a therapeutic milieu that can facilitate patient recovery, a sense of safety and good interpersonal relationships.72 Interpersonal strategies include prioritising responses to requests, using verbal and non-verbal mirroring for emotional attunement, monitoring and responding to individual’s distress, offering self-soothing resources, facilitating relationships between consumers, and explaining and adjusting the environment and routines to better fit unique needs. Via fine-grained attention, mental health nurses facilitate in-the-moment moves towards recovery.
Achieving a milieu that is experienced by consumers as safe, therapeutic and supportive of recovery is challenging, expressly in environments where people’s experiences of crises are commonly associated with intense inner turmoil, fear and sense of alienation, and where legislated admission processes and confined spaces add distressing provocations, loss of freedom and autonomy.73 In acute settings in particular, nursing practice can either reinforce surveillance and compliance cultures or actively create conditions for supported decision-making. This is especially critical for suicide prevention in acute settings, where the quality of interpersonal interactions can influence whether individuals disclose ongoing risk or withdraw from care. Relational, trauma-informed nursing practices have been linked to reduced conflict, improved safety, and better post-discharge engagement.74,75
Mental health nurses engage in supported decision-making to uphold rights and specifically to redress harms of breaching human rights, when people are detained without consent. Practical mechanisms include truth telling, respectful language, offering genuine choices (even small ones) and collaborative safety planning. Consumer dissatisfaction with choice in treatment decisions in acute settings can reflect limited experience and investment of mental health nurses and others in supported decision making.76
Nurse-led interventions such as Safewards grow mutuality and relationships, helping ameliorate conflict and the associated trauma.77 But lived experience critiques highlight that power dynamics and coercion must be explicitly addressed for such models to be experienced as safe.78 Across settings, mental health nursing also plays a crucial role in medication monitoring and information provision, physical health screening, resources and support for self-care, and continuity of information among teams. When nursing documentation captures a person’s narrative, preferences, triggers, and early warning signs, it becomes a key carrier of supported decision-making into ED presentations and inpatient contexts, where continuity is otherwise fragile.79
Occupational Therapy
Occupational therapists work with individuals, families, groups, and communities to enable participation, support daily routines, and strengthen environmental and relational supports that make recovery possible.80–82 Occupations in daily life encompass how people care for themselves and others, experience enjoyment, sustain relationships, and contribute socially, culturally, and economically.83 This perspective centres everyday life rather than diagnosis, positioning participation as both a means and an outcome of care.
Occupational therapy draws on evidence that patterns of participation shape wellbeing and are disrupted by illness, social adversity, and structural inequality.81,84,85 Such disruption affects agency, identity, meaning, routines, roles, and relationships, all central to recovery.85,86 Consequences include restricted access to meaningful occupations, isolation, occupational imbalance, and exclusion driven by stigma and disadvantage.84,87 These disruptions are core to mental distress. Lived and living experience accounts similarly describe recovery as rebuilding participation, meaning, and belonging.88,89 Occupational therapy therefore understands people as citizens with biographies and social worlds,90 and attends to interactions between personal capacities and environmental conditions such as housing, resources, and structural barriers, resisting purely symptom-based explanations.84 However, occupational perspectives can be marginalised where biomedical and psychological models dominate.91
Mental health occupational therapy is intended to be individualised, occupation-focused, inclusive, and relational.92 Models emphasise client values, strengths, lived expertise, and partnership in decisions about priorities and participation.93,94 Enacting this within institutional systems is challenging where power structures constrain choice.95–97 Contemporary practice therefore emphasises collaborative, relational, and rights-based approaches, including power-sharing and cultural safety.98,99
In practice, occupational therapists use collaborative, action-oriented methods to build skills, solve practical problems, trial environmental changes, and embed strategies into daily routines to manage health impacts.100 Group-based practice is a distinctive contribution, supporting agency, belonging, and peer connection through shared meaningful activity.100,101 Co-design and co-facilitation with lived and living experience workforces further strengthen participation and connectedness. Within multidisciplinary systems, occupational therapy anchors person-centred care in the practical realities of everyday life.
Social Work
Social work is grounded in international human rights and social justice traditions, with practice aligned to the Universal Declaration of Human Rights.102 The global definition developed by the International Federation of Social Workers and the International Association of Schools of Social Work positions social work as both a practice-based profession and an academic discipline committed to social change, social cohesion, and the empowerment and liberation of people, underpinned by human rights, collective responsibility, and respect for diversity.103,104
In Australia, social work is guided by ethical commitments to dignity, human rights, and social justice, with practitioners working alongside individuals, families, groups, and communities.105 In mental health contexts, this includes enhancing wellbeing, addressing interpersonal and structural challenges, supporting social participation, confronting systemic barriers, and protecting people from oppression and abuse. Practice spans direct work, counselling, group and community work, advocacy, policy, research, supervision, and evaluation, all directed toward improving access to the social conditions that support recovery.105 A defining feature of social work is its long-standing commitment to strengths-focused practice, predating formal recovery-oriented frameworks.106–108 This approach shifts attention from deficit-based understandings of distress toward recognising people and environments as sources of capability and growth.109,110 Social workers collaborate with people to identify interests, skills, relationships, and assets, including housing, networks, confidence, and agency.111,112 The Strengths Model113 has been especially influential, framing strengths as coexisting with vulnerability and located in passions, skills, relationships, and environments, challenging “deficit dominance” and victim-blaming cultures in mental health services.113,114
Strengths-focused social work also critically engages with narrowly medicalised framings of distress. Recovery-oriented practice requires moving beyond disease-based narratives that individualise distress and obscure social, economic, cultural, and political influences.111,115 Social work brings a contextual, equity-oriented lens to multidisciplinary teams, foregrounding social determinants and structural conditions shaping recovery. Practitioners often navigate tensions between these commitments and statutory, risk, and compliance demands.116,117 Ethical practice in this context involves questioning constraining structures, using relational and empowerment-focused models, and exercising moral courage.118 Within multidisciplinary systems, social work anchors person-centred care in human rights, social context, and everyday realities, extending recovery beyond treatment to participation, inclusion, and justice.
Lived and Living Expertise
Increasingly, lived and living experience is recognised as central to suicide prevention and mental health reform. “Lived” experience of suicide emcompasses suicidal thoughts, surviving attempts, supporting someone in crisis, or bereavement, with “living” emphasising continuing impact and expertise over time.119 Lived and living experience is understood as expertise rather than anecdote, the capacity to translate personal and collective experience into practice-relevant knowledge that informs systems, professional practice, and outcomes. Meaningful integration requires power sharing, resourcing, and formal authority, not token consultation.19 Making lived experience leadership explicit responds to mental health systems that have historically prioritised professional authority, diagnosis, and risk management. Lived experience leadership re-centres safety, dignity, and recovery as defined from the inside, challenging practices that may unintentionally reproduce harm.11,16
Evidence indicates that peer and lived experience roles can improve engagement, hope, empowerment, and service experience when implemented with adequate organisational support.120,121 These benefits are not automatic. Role ambiguity, inadequate supervision, and expectations that lived experience workers assimilate into dominant clinical norms can dilute impact and increase workforce harm. Clear role definition, training, supervision, and organisational commitment are therefore essential.19,121
When effectively integrated, lived and living experience practitioners strengthen multidisciplinary care through complementary expertise. They enhance relational safety by modelling non-judgemental engagement and identifying when language or processes are experienced as coercive or dismissive.11,17 They enrich formulation by linking mental health challenges to meaning, identity, environment, and connection, and support supported decision-making by helping people prepare for appointments, articulate preferences, and navigate complex systems. Shared decision-making approaches are associated with improved decisional quality, therapeutic relationships, and recovery-oriented care planning.35,122
Lived and living experience expertise also broadens understandings of quality and safety. People consistently emphasise dignity, being believed, continuity, and avoidance of iatrogenic harm as central to safety, including suicide risk, help-seeking, and recovery following crisis. Embedding lived and living experience leadership in governance broadens what is measured to include relational safety, experiences of coercion, and barriers to help-seeking.16,17 These contributions are especially important in emergency and inpatient settings, where environments and interpersonal dynamics can compound distress, reinforcing the ward milieu as a shared clinical intervention.78
Strengths-based approaches bridge lived and living experience leadership and multidisciplinary care, with implementation dependent upon fidelity, supervision, and organisational culture.123 A lived and living experience lens strengthens accountability for how strengths are defined and whether services genuinely support people’s goals and identities. Occupational therapy research similarly highlights recovery as enacted through everyday doing, belonging, and routine, underscoring the importance of housing, structure, social connection, and meaningful activity.86,87 Lived and living experience practitioners often work in this terrain, aligning clinical plans with real-world living.
Lived and living experience is not limited to peer roles. Many clinicians have personal experiences of distress, and supported, ethical use of this can deepen empathy, authenticity, and therapeutic alliance when accompanied by appropriate boundaries and organisational support.124 Meaningful integration therefore requires deliberate workforce design, including clear role scopes, reflective supervision, career pathways, and safeguards against tokenism and emotional overexposure.19,125 These protections are especially important for those in dual roles, including clinicians who are also service users, and include choice about disclosure, boundary support, and prevention of unresourced lived and living experience labor.
Across disciplines, supported decision-making, relational practice, and shared formulation form the common foundation. Psychiatry, psychology, exercise physiology, nursing, occupational therapy, social work, and lived and living experience roles each contribute distinct knowledge that broadens care beyond symptom management to include meaning, participation, physical health, and social context. Person-centred care is strongest when these perspectives operate collaboratively rather than hierarchically, and when lived and living experience expertise holds formal authority within systems.
Models of Care Viewed Through Supported Decision-Making
Many services look for a single model to “solve” person-centred care. The literature suggests this is rarely how change happens. Instead, models work well when they embed the mechanisms already described, those of supported decision-making, shared formulation, relational continuity, lived experience leadership, and integration of physical and social determinants. In this paper, we compare five commonly referenced approaches: the Optimal Health Program (OHP), the Strengths Model, Open Dialogue, Traditional Case Management, and Behaviour Support Plan approaches. These models arise from different disciplinary traditions and service contexts, and are typically enacted through different mixes of professional expertise, which shapes how power, agency, and decision-making are operationalised. To keep the main text lean, we summarise model descriptions, disciplinary origins, and comparative features in Tables 1 and 2, intended to support reflection and service design rather than provide definitive rankings.
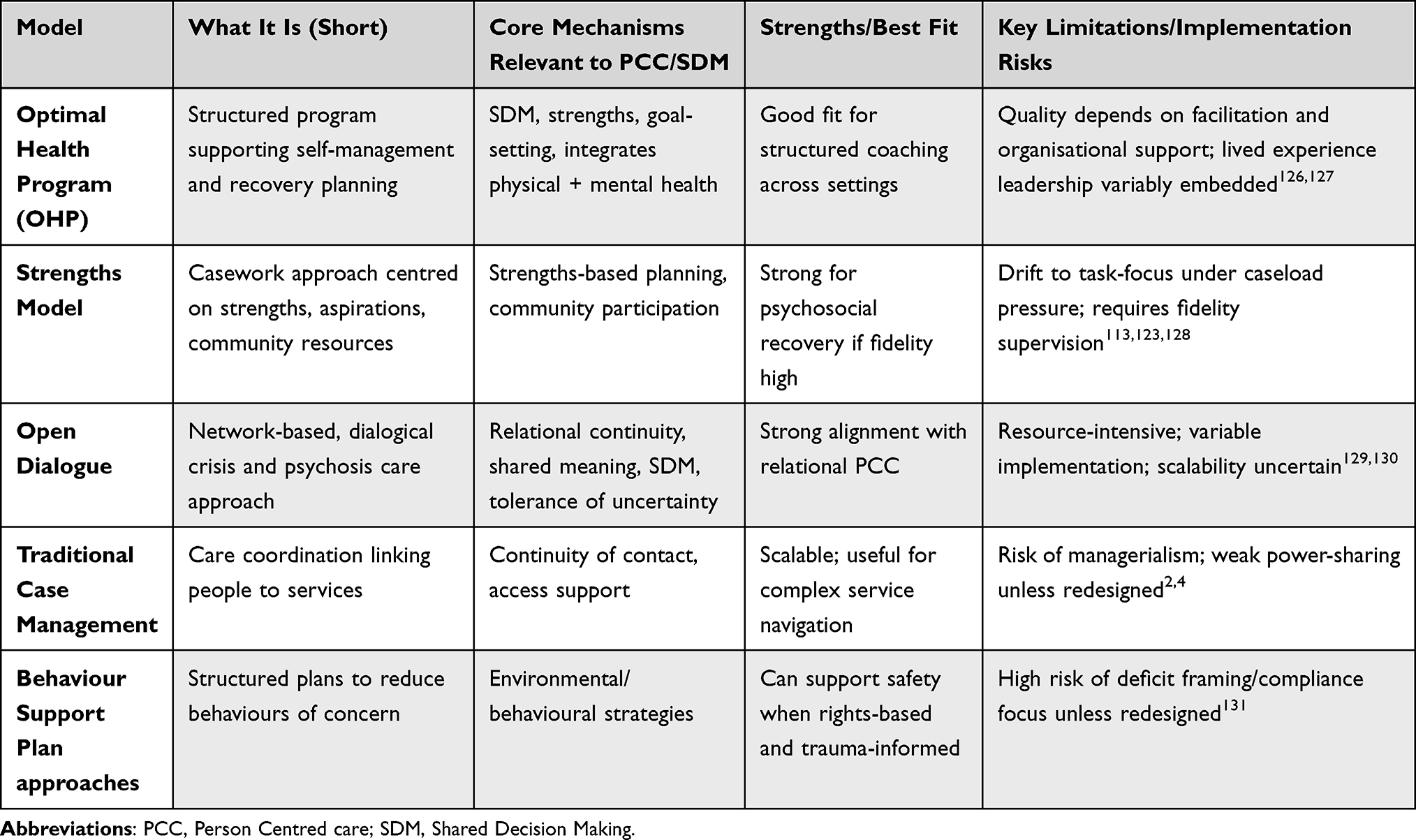 |
Table 1 Overview of Person-Centred Multidisciplinary Models |
 |
Table 2 Comparative Ratings of Models Against Person-Centred Mechanisms |
Relational and meaning-oriented models (notably Open Dialogue and OHP) tend to align strongly with person-centred care because they institutionalise collaborative conversation and tolerate uncertainty.126,127,129 The Strengths Model similarly centres capability and community participation, and higher fidelity implementation is associated with improved outcomes such as reduced hospitalisation.123,128 By contrast, more scalable coordination or behaviour-focused approaches can drift into managerialism unless explicitly redesigned to protect autonomy, meaning, and power sharing.2,4,131 Scalability is not the same as quality. Services can deliver activity without improving trust, agency, or recovery. These models persist for a reason. In resource-limited and high-demand systems, approaches such as case management provide structure, continuity of contact, and a practical way to coordinate care across fragmented services. Contemporary evidence continues to show that multidisciplinary case management and outreach models can support engagement, improve social functioning, and reduce service fragmentation, particularly for people with complex and ongoing needs.132,133 They can also offer a consistent point of contact within otherwise disjointed systems, which is critical where workforce capacity is stretched and service pathways are difficult to navigate. More recent evaluations suggest that outcomes are strongest where models are implemented with fidelity and adapted to context, rather than applied as rigid templates.134 In this sense, standardised approaches can function as stabilising infrastructure within overstretched systems. The issue, therefore, is not their presence, but how they are enacted. Without explicit attention to power sharing, supported decision-making, and person-defined goals, coordination can become task-focused rather than person-led. When these mechanisms are protected, scalable models can support person-centred care; when they are not, they risk reinforcing service-led practice. A useful practical conclusion is that services should adopt minimum standards that travel across settings, regardless of which model is “on the tin”. These include supported decision-making checkpoints, shared formulation routines, and explicit requirements for lived and living experience leadership in governance and transition planning.19
Social Context, Stigma, and the Politics of Who Gets to Be Heard
Person-centred care cannot be sustained without explicit attention to social context. Distress and decision-making are shaped by intersecting forms of stigma, including diagnostic stigma, cultural stigma, structural stigma embedded in policy and service design, and internalised stigma that constrains what people feel entitled to seek from care.11,43,135 These dynamics shape multidisciplinary practice by legitimising coercion, narrowing clinical curiosity, and obscuring the roles of trauma, disability, gender, racism, poverty, and family violence.2,3
When stigma and structural inequity are not directly addressed, person-centred language can coexist with service-led, risk-dominated practice, especially in acute and crisis settings.11,27 Diagnostic and risk frameworks are often treated as neutral, yet they can privilege professional authority over personal knowledge and marginalise lived and living experience perspectives on safety, dignity, and recovery.17,135 Genuinely person-centred multidisciplinary care therefore requires explicit social and equity competence, including culturally safe practice, recognition of intersectional disadvantage, and practical attention to the social and material conditions that make recovery possible, such as secure housing, income security, meaningful roles, community connection, and access to physical healthcare.115,136,137 While social work and occupational therapy are central to this work, responsibility is shared across teams. A treatment plan that ignores housing insecurity, food access, safety, or social exclusion is not person-centred care, but a partial intervention delivered as if it were sufficient.43,87
ED and Inpatient Environments: Making High-Risk Settings Safer and More Therapeutic
Emergency departments and inpatient units are the places where person-centred principles are most frequently compromised, often under the banner of safety. These environments are commonly characterised by noise, surveillance, lack of privacy, rapid consumer and staff turnover, bed pressure, and documentation systems that foreground risk over relationship. For people with trauma histories, disability, neurodivergence, or experiences of coercion, ED and inpatient settings can be re-traumatising and can reduce future help-seeking. A supported decision-making lens changes the clinical question in these settings. Instead of “how do we control risk?”, the question becomes “how do we reduce distress and increase agency quickly and safely?”. Practical steps include predictable communication, transparent rationale for decisions, genuine choices where possible, attention to sensory and environmental stressors, involvement of nominated supports with consent, and early planning for transition back to community care. Safewards and related approaches offer practical tools to reduce conflict, but consumer research indicates that power dynamics and coercion must be directly addressed to make wards feel safer.78 Multidisciplinary practice is especially important here because the drivers of crisis are often multi-layered and include medical issues, substance use, trauma, social stress, sleep deprivation, and despair. A person-centred ED or inpatient response therefore requires rapid access to multiple kinds of expertise, including lived and living experience practitioners who can support communication, de-escalation, and continuity. Services need to treat transitions as a core safety task. Many harms occur in the gaps: discharge without plan, handover without preferences, referral without follow-up. Minimum standards for supported decision-making and continuity should be strongest at these transition points.
What an Ideal Supported Decision-Making-Aligned Multidisciplinary Model Looks Like
Rather than advocating for a single branded model, we propose that services define and protect a small set of minimum elements that any person-centred multidisciplinary model should include. These elements are summarised in Table 3, alongside practical examples of how disciplines contribute and how lived and living experience expertise is embedded.
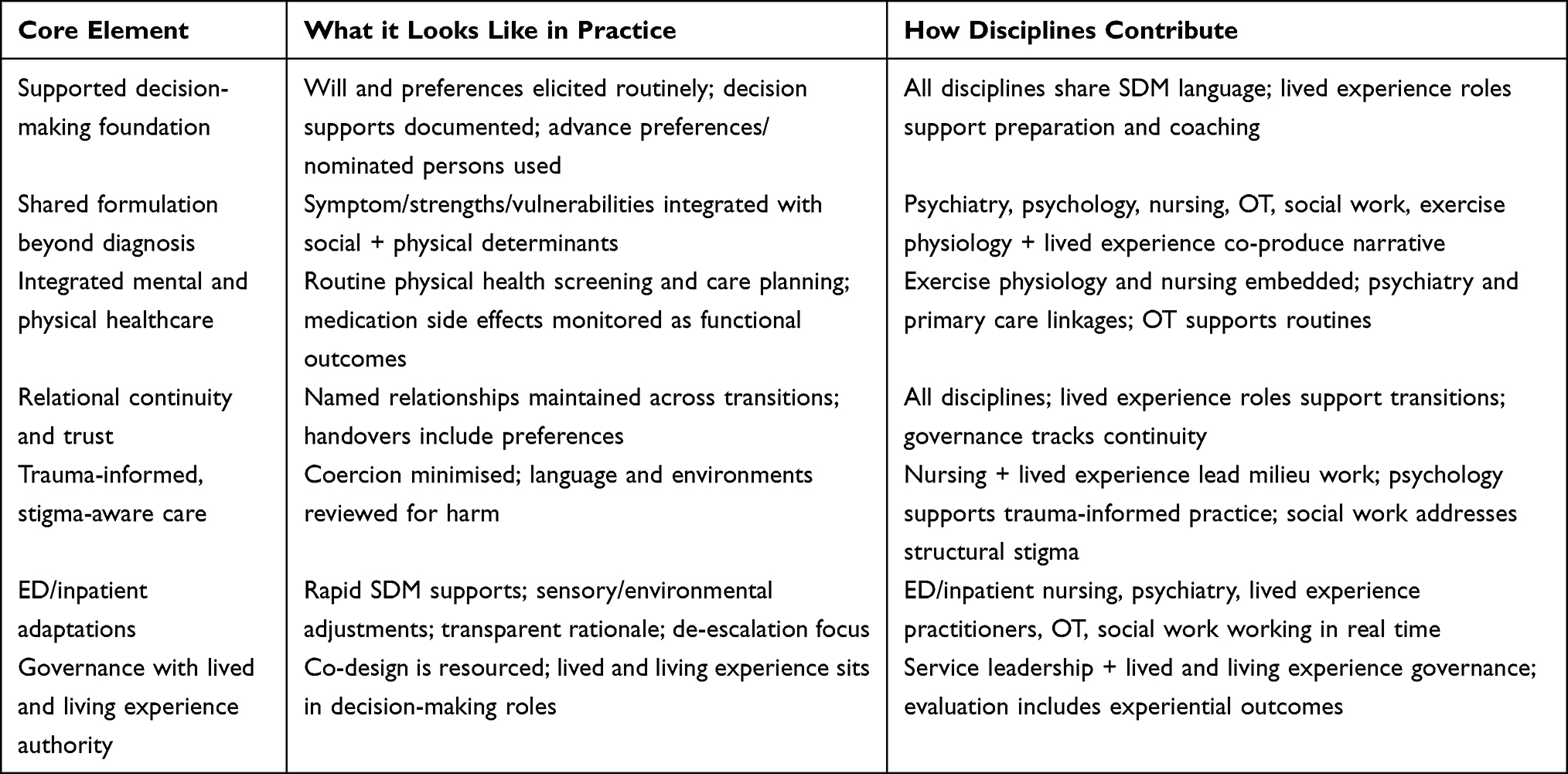 |
Table 3 Elements of an Ideal Supported Decision-Making-Aligned Multidisciplinary Model |
The value of this approach is twofold. First, it makes person-centred care measurable. Services can assess whether supported decision-making is routine, whether shared formulation is occurring, and whether lived and living experience leadership holds real authority. Second, it supports consistency across settings. People should not lose autonomy because the door they walked through happened to be that of an ED. Regardless of the model adopted, the shared formulation approach illustrated in Figure 2 offers a consistent foundation for multidisciplinary practice that remains person-led and aligned with supported decision-making.
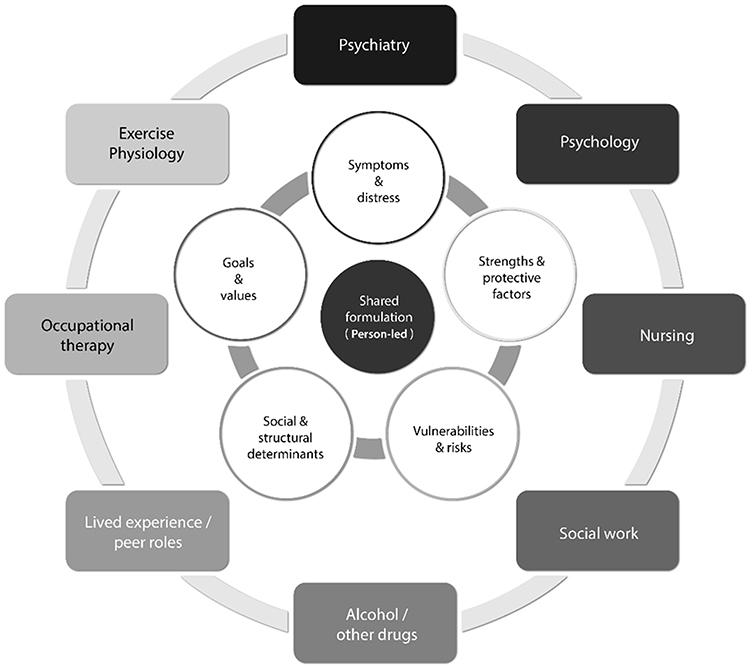 |
Figure 2 Shared formulation map – ideal supported decision-making/shared formulation-aligned multidisciplinary model. |
A person-led, multidisciplinary formulation needs to integrate symptoms and distress, strengths and protective factors, vulnerabilities and risks, social and structural determinants, and personal goals and values. Implementation will always involve compromise, particularly in rural and resource-constrained contexts. The point is not perfection. The point is protecting the mechanisms most closely linked to trust, safety, and recovery, those of supported decision-making, relational continuity, shared formulation, and attention to social and physical determinants.16,19
Discussion
Person-centred care is widely endorsed in mental health policy, yet its enactment in everyday multidisciplinary practice remains uneven. Often treated as a reform endpoint, it is readily displaced when diagnostic dominance, risk management, and service-led accountability structures shape care delivery. Across disciplines and settings, a consistent pattern emerges: person-centred care is not secured through model selection alone. It depends on protecting core mechanisms that redistribute power, enable supported decision-making, legitimise lived and living expertise, and integrate social and physical context into care, especially for people facing intersecting vulnerabilities in high-risk or resource-constrained environments. These findings have direct implications for suicide prevention. Rather than being confined to crisis response or specialised services, suicide prevention emerges here as an outcome of everyday practice: how people are listened to, how decisions are shared, and whether care feels safe, respectful, and continuous. This reframes suicide prevention as a whole-of-system responsibility embedded within person-centred multidisciplinary care, rather than a discrete intervention.138,139
Conceptualising Person-Centred Care in Multidisciplinary Systems
Person-centred care in multidisciplinary mental health is defined as care that respects preferences, values lived and living experience, and attends to broader life context rather than symptoms alone.1,117 Policy frameworks position it as central to recovery, autonomy, and partnership,21 a persistent gap remains between policy and practice. This gap reflects diagnostic dominance, risk management logics, and accountability systems that prioritise organisational demands over person-defined goals.2–4 In rural and regional settings, workforce scarcity, limited service options, and heightened risk aversion can further restrict choice, even where relationships are strong. Multidisciplinary care is often assumed to be inherently person-centred, but teams may reproduce professional hierarchies, with medical or organisational priorities overriding personal values, particularly in acute or high-risk contexts.10,11 This tension reflects system design rather than clinician intent, leaving person-centred care vulnerable to rhetorical rather than structural implementation.
Models Framed as Person-Centred and Assumptions About Power and Agency
Models described as person-centred, including those described above, rest on differing assumptions about power, agency, and decision-making. Relational and dialogical models such as Open Dialogue centre shared meaning-making, relational continuity, and tolerance of uncertainty, positioning expertise as distributed rather than professionally owned.129,130 Strengths-based approaches similarly emphasise capabilities, aspirations, and community participation, assuming agency is fostered by recognising what matters to people rather than defining need through deficit.113
Structured programs such as the Optimal Health Program foreground self-management, goal-setting, and integration of physical and mental health, but their person-centredness depends on facilitation quality, organisational support, and protected time for relational work.126,127 In contrast, traditional case management and behaviour-focused approaches often assume coordination or behaviour change can occur without redistributing decision-making power. These models risk drifting toward managerialism and compliance unless intentionally redesigned to safeguard agency and shared decision-making.2,4,131
Supported Decision-Making, Lived Experience Leadership, and Determinants of Health
Lived and living experience leadership strengthens person-centred practice when embedded with authority, resourcing, and role clarity. Peer and lived experience roles can improve engagement, hope, and relational safety, but only when supported through governance rather than positioned as symbolic additions.19,120,121 Attention to social and physical determinants shows a similar pattern: housing, physical health, substance use, and social exclusion are central to distress and recovery yet frequently marginalised in clinical and multidisciplinary planning.43,135
Advance choice mechanisms bridge rights-based supported decision-making. Advance statements and psychiatric advance directives can help preserve will and preferences during crisis or fluctuating capacity as well as strengthening autonomy, reducing conflict, and improving continuity.140 Embedding supported decision-making also means reliably mobilising the person’s chosen supporters during crisis and transitions, so autonomy is strengthened rather than displaced.16,18,21
Coercion is a key stress-test of person-centred care. Although justified in the name of safety, coercive practices are associated with reduced trust, heightened trauma, and diminished future help-seeking, particularly for people with histories of violence, institutionalisation, or discrimination.11,135 Reducing coercion requires coordinated action across staff capability, therapeutic milieu, organisational policy, and governance conditions that prioritise transparency, de-escalation, and supported decision-making.78
Implications for Workforce Design, Governance, and Reform
Workforce development requires explicit valuing and prioritisation of the core principles espoused here, to ensure person-centred is enacted in everyday clinical settings.3,10 It should be part of clinical supervision for all disciplines involved in the care of the mentally unwell.
Governance is equally critical. Embedding lived and living experience leadership with formal authority over service design, evaluation, and reform is a matter of accountability, not representation alone.19,141 Quality and safety frameworks must extend beyond clinical indicators to include relational and experiential outcomes such as dignity, transparency and continuity.16,17,27,142 A broader systems lens from public health and health economics further strengthens these findings. Public health literature emphasises that person-centred care cannot be achieved within service-level reform alone, but requires attention to upstream determinants, population need, and prevention-oriented investment.143,144 From a health economics perspective, current funding and commissioning models often prioritise throughput, short-term outputs, and crisis response over relational continuity and long-term outcomes, creating structural barriers to person-centred practice.145 Workforce shortages and maldistribution, particularly in rural and regional settings, further constrain the capacity of multidisciplinary teams to deliver relational, person-led care. These perspectives reinforce that the gap between person-centred policy and practice is not only clinical but systemic. Embedding supported decision-making, lived experience leadership, and multidisciplinary collaboration therefore requires alignment between service models and the policy, funding, and workforce structures that shape how care is delivered.146 These shifts are especially urgent for people facing intersecting vulnerabilities, including trauma, disability, chronic illness, substance use, housing insecurity, racism, stigma, and geographic isolation. The literature warns that person-centred care must be explicitly equity-oriented to avoid reproducing exclusion under recovery language.135,136 Future research should prioritise implementation studies on sustaining supported decision-making and shared formulation in resource-constrained, rural, and culturally diverse settings, with attention to how person-centred care travels across services, settings, and delivery modes.
Limitations
This review is grounded in lived and living experience leadership and recognises this as a critical form of expertise in mental health care. At the same time, this grounding reflects the perspectives within a relatively small authorship group and cannot represent the full breadth and diversity of lived and living experience. This experience is not singular; it is shaped by culture, identity, place, and interactions with systems over time. In particular, perspectives and knowledges of First Nations peoples, culturally and linguistically diverse communities, rural and remote populations, and others whose experiences are shaped by structural inequities are not comprehensively represented here. Ongoing work is needed to ensure a broader range of voices are meaningfully included and resourced in shaping mental health systems.
The perspectives presented herein also do not encompass all disciplines commonly involved in multidisciplinary mental health care. Notably, dietetics, general practice, pharmacy, speech pathology, cultural and Aboriginal health practitioners, and specialist alcohol and other drug roles are not represented within the authorship of this paper. Their contributions are essential to holistic, person-centred care, particularly where physical health, communication needs, cultural safety, and medication management are central.
As a critical review that used a narrative approach, this paper does not aim to provide exhaustive coverage of all relevant literature or models. The models included reflect those most visible in peer-reviewed and grey literature, particularly within English-language contexts, and those commonly implemented within contemporary mental health systems. This means the selection is shaped by what is most documented and accessible, as well as by the authors’ disciplinary and practice contexts. Other approaches, including those developed in non-Western or community-led contexts, may offer important additional insights that are not fully captured here.
The analysis is intended to support reflection, service design, workforce development, and policy discussion. It does not seek to make definitive claims about effectiveness or to privilege particular models, but rather to highlight the conditions and mechanisms that support more ethical, responsive, and person-led care.
Recommendations
Table 3 and Figure 1 translate this review’s findings into a concise set of system-level expectations to strengthen person-centred multidisciplinary mental health practice. Aimed at service leaders, policymakers, commissioners, and governance bodies, they guide service design, workforce development, quality and safety frameworks, and evaluation. While relevant to clinicians, their main leverage is organisational and systemic. Rather than promoting a single model, the recommendations presented in Table 4 define minimum mechanisms to be protected across settings, including community, primary care, tertiary services, emergency departments, and inpatient units. This is particularly important in rural and regional areas, where workforce limits, fragmentation, and distance can intensify power imbalances and weaken person-centred practice. The goal is to reduce variability in care, especially during crisis and transitions, and to ensure supported decision-making, lived and living experience leadership, and equity are treated as foundational.
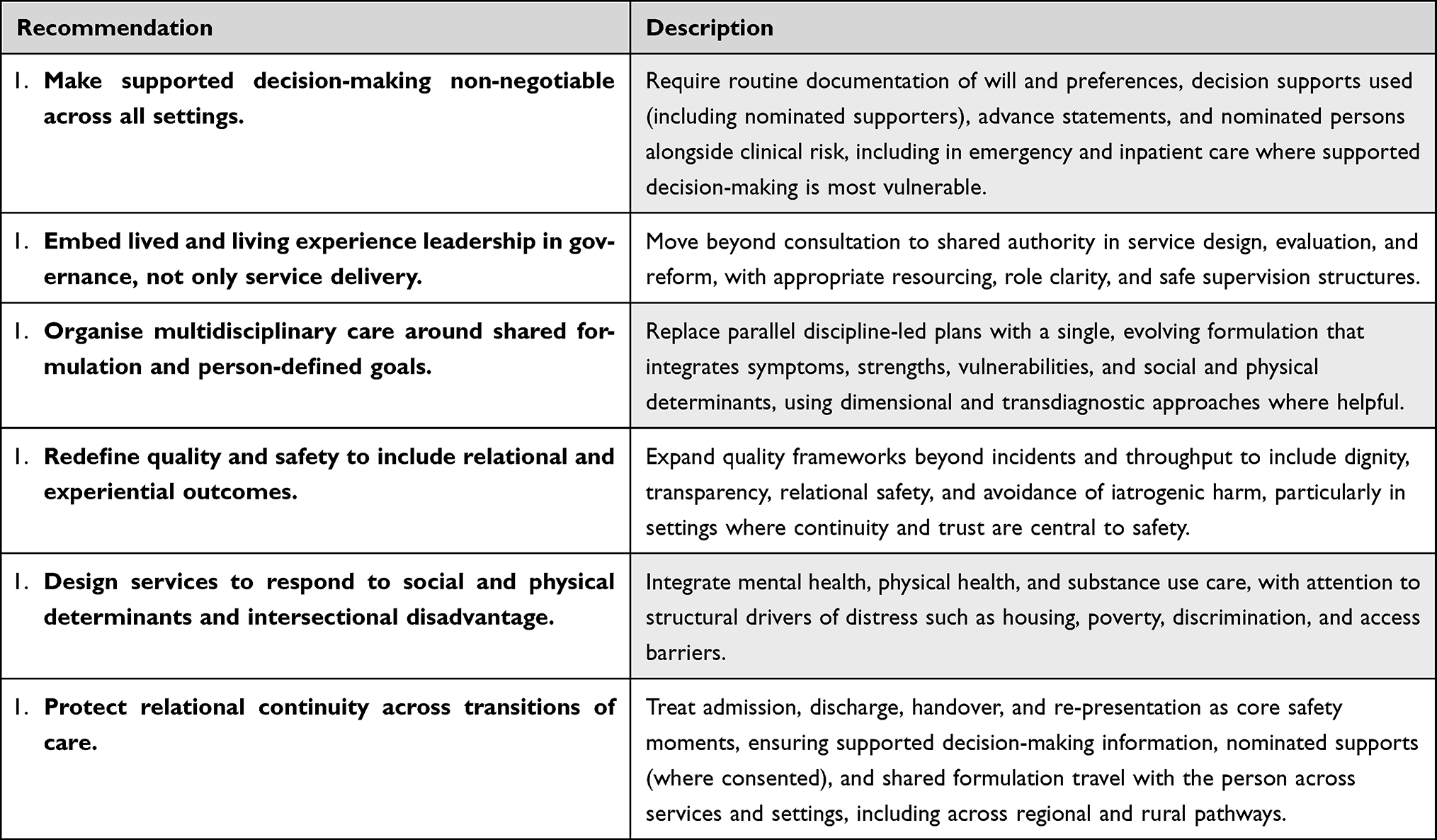 |
Table 4 Recommendations to Strengthen Person-Centred Multidisciplinary Practice |
Conclusion
Person-centred care depends not on new models but on system mechanisms that redistribute power, support agency, and centre lived realities. It is strongest where supported decision-making is routine, care is relational and meaning-focused, and lived and living experience leadership holds real authority. For policymakers and leaders, these mechanisms should be minimum standards across all settings, including emergency and inpatient care. This critical review shows how embedding supported decision-making, shared formulation, relational continuity, and lived experience leadership into system design shifts person-centred care from aspiration to practice, strengthening safety, trust, and recovery for people with complex needs and limited choices. Strengthening these mechanisms also offers a practical pathway for embedding suicide prevention within everyday care, through earlier engagement, safer care experiences, and sustained connection to support.
Abbreviations
AASW, Australian Association of Social Workers; ACSM, American College of Sports Medicine; AEP, Accredited Exercise Physiologist; APA, American Psychological Association; BSP, Behaviour Support Plan; CA, Capability Approach; CRPD, Convention on the Rights of Persons with Disabilities; DSM, Diagnostic and Statistical Manual of Mental Disorders; ED, Emergency Department; ESSA, Exercise & Sports Science Australia; G × E, Gene–Environment interaction; HiTOP, Hierarchical Taxonomy of Psychopathology; ICD, International Classification of Diseases; ICF, International Classification of Functioning, Disability and Health; IFSW, International Federation of Social Workers; IASSW, International Association of Schools of Social Work; MHHFA, Mental Health First Aid; NGO, Non-government organisation; OHP, Optimal Health Program; OT, Occupational Therapy/Occupational Therapist; PAR, Participatory Action Research; PCC, Person-centred care; SDM, Supported decision-making; SMI, Severe Mental Illness; UDHR, Universal Declaration of Human Rights; UN, United Nations; UNCRPD, United Nations Convention on the Rights of Persons with Disabilities; UTAS, University of Tasmania; UTS, University of Technology Sydney.
Acknowledgments
The authors acknowledge the people with lived and living experience of mental health challenges and suicidal distress whose insights and advocacy have shaped the principles discussed in this paper. Their leadership continues to guide efforts toward more respectful, safe, and person-led care. We also recognise multidisciplinary clinicians, peer workers, community organisations, and service leaders who work to provide relational, ethical care within complex and resource-constrained systems. Conversations and collaborations with colleagues and communities across clinical, academic, and service settings have informed the development of this work.
We acknowledge the ongoing efforts of service users, families, and communities who continue to advocate for more humane, just, and person-centred mental health systems.
Disclosure
The authors declare that this work reflects their professional and academic expertise in mental health research, clinical practice, workforce development, and lived and living experience leadership. Several authors are employed in clinical, academic, or service leadership roles within mental health services, universities, and health organisations, and some contribute to workforce development, service design, evaluation, or policy initiatives relevant to person-centred and multidisciplinary mental health care. These roles may be considered non-financial professional interests, as the authors are engaged in advancing approaches discussed in this review within their respective fields.
No author received specific funding, honoraria, or financial benefit for the preparation of this manuscript. NHH receives salary support from the National Health and Medical Research Council (NHMRC) Investigator Fellowship (APP2017080). DH receives salary support as a Chancellors Research Fellow; in addition, Dr David Castle reports potential conflicts of interest (past 3 years: March 2026): DC has received grant monies for research from NHMRC, MRFF, St Vincent’s Research Endowment Fund, Barbara Dicker Foundation, CIHR (Canada), Brain Canada, Servier, Boehringer Ingelheim, iNova; Travel Support and Honoraria for Talks and Consultancy from Servier, Seqirus, Lundbeck, Mindcafe, Psychscene, Inside Practice, Boeringher Ingelheim. He is a founder of the Optimal Health Program (OHP) and holds 50% of the IP for OHP; and is part owner (8%) of Clarity Healthcare. DC receives royalties for books from Allen and Unwin, Elsevier, Oxford University Press and Cambridge University Press. He is an advisor for Tryptamine Therapeutics, a psychedelics company. He does not knowingly have stocks or shares in any pharmaceutical company. The authors hold no patents, stock ownership, or commercial interests related to the models or frameworks discussed. The paper does not evaluate a proprietary product or commercial program. The authors have taken care to present a balanced, critical synthesis of the literature and to avoid promoting any single service, organisation, or branded model.
The authors report no other conflicts of interest in this work.
References
1. Slade M, Bird V, Clarke E, et al. Supporting recovery in patients with psychosis through care by community-based adult mental health teams (REFOCUS): a multisite, cluster, randomised, controlled trial. Lancet Psychiatry. 2015;2(6):503–23. doi:10.1016/S2215-0366(15)00086-3
2. Pilgrim D. Understanding Mental Health: A Critical Realist Exploration.
3. Morrison A. A manualised treatment protocol to guide delivery of evidence-based cognitive therapy for people with distressing psychosis: learning from clinical trials. Psychosis. 2017;9(9):271–281. doi:10.1080/17522439.2017.1295098
4. Hormazábal-Salgado R, Whitehead D, Osman AD, Hills D. Person-centred decision-making in mental health: a scoping review. Issues Mental Health Nurs. 2024;45(3):294–310. doi:10.1080/01612840.2023.2288181
5. Rehman Z, Real IPG. How intersectionality challenges the ‘one size fits all’ approach to global mental health. J Psychiat Mental Health Nurs. 2025;32(6):1359–1362. doi:10.1111/jpm.70031
6. Kirmayer LJ. Cultural competence and evidence-based practice in mental health: epistemic communities and the politics of pluralism. Soc Sci Med. 2012;75(2):249–256. doi:10.1016/j.socscimed.2012.03.018
7. Dudgeon P, Milroy H, Walker R. Working Together: Aboriginal and Torres Strait Islander Mental Health and Wellbeing Principles and Practice. 2017.
8. Truong M, Paradies Y, Priest N. Interventions to improve cultural competency in healthcare: a systematic review of reviews. BMC Health Serv Res. 2014;14:99. doi:10.1186/1472-6963-14-99
9. Aggarwal NK, Jarvis GE, Gómez-Carrillo A, Kirmayer LJ, Lewis-Fernández R. The cultural formulation interview since DSM-5: prospects for training, research, and clinical practice. Transcult Psych. 2020;57(4):496–514. doi:10.1177/1363461520940481
10. Happell B, Bennetts W, Tohotoa J, Wynaden D, Platania-Phung C. Promoting recovery-oriented mental health nursing practice through consumer participation in mental health nursing education. J Mental Health. 2019;28(6):633–639. doi:10.1080/09638237.2017.1294734
11. Rose D. The mainstreaming of recovery. J Mental Health. 2014;23(5):217–218. doi:10.3109/09638237.2014.928406
12. Christie L, Davys D, Cook PA. Service user perspectives on the value and effectiveness of occupational therapy following intervention for severe depression. Br J Occup Ther. 2026;89(2):83–93. doi:10.1177/03080226251363731
13. McSherry T, Loewenthal D, Cayne J. The implications of Kristeva’s notion of the abject in understanding the significance of therapeutic knowledge and practice in mental health nursing. J Psychiat Mental Health Nurs. 2015;22(1):82–88. doi:10.1111/jpm.12180
14. Nilsson E, Tjörnstrand C, Lindqvist D, Wetterling J, Lexén A, Bejerholm U. Turning to service users for the understanding of current and future mental health services in the development process of research and practice: a qualitative study. Health Expect. 2026;29(1):e70574. doi:10.1111/hex.70574
15. Byrne L, Roennfeldt H, O’Shea P. Identifying barriers to change: the lived experience worker as a valued member of the mental health team. 2017. Available from: https://mhcsa.org.au/wp-content/uploads/2021/12/Attachment-1-Identifying-barriers-to-change-The-lived-experience-worker-as-a-valued-member-of-the-mental-health-team-final-report.pdf.
16. Roennfeldt H, Glover H, Castles C, et al. We can do better: recommendations for mental health crisis care from people with lived experience. Emerg Med Austr. 2025;37(1):e14528. doi:10.1111/1742-6723.14528
17. Roennfeldt H, Hill N, Byrne L, Hamilton B. Exploring the lived experience of receiving mental health crisis care at emergency departments, crisis phone lines and crisis care alternatives. Health Expect. 2024;27(2):e14045. doi:10.1111/hex.14045
18. Szmukler G. “Capacity”, “best interests”, “will and preferences” and the UN convention on the rights of persons with disabilities. World Psychiatry. 2019;18(1):34–41. doi:10.1002/wps.20584
19. National Mental Health Commission. National Lived Experience (Peer) Workforce Development Guidelines; 2021.
20. Russo JSA. Searching for a Rose Garden: Challenging Psychiatry, Fostering Mad Studies. 2016.
21. United Nations. Convention on the Rights of Persons with Disabilities; 2006.
22. Byrne E, de Boer M. Epistemic injustice, medicine, and gender. The Oxford Handbook of Philosophy of Medicine. 2025;351.
23. Davidson G, Brophy L, Campbell J, Farrell S, Gooding P, O’brien A-M. An international comparison of legal frameworks for supported and substitute decision-making in mental health services. Int J Law Psych. 2015;44:30–40. doi:10.1016/j.ijlp.2015.08.029
24. Francis CJ, Hazelton M, Wilson RL. Supported decision-making interventions in mental healthcare: a systematic review of evidence on the outcomes for people with mental ill health. Health Expect. 2024;27(6):e70134. doi:10.1111/hex.70134
25. Grant MJ, Booth A. A typology of reviews: an analysis of 14 review types and associated methodologies. Health Info Libr J. 2009;26(2):91–108. doi:10.1111/j.1471-1842.2009.00848.x
26. Greenhalgh T, Thorne S, Malterud K. Time to challenge the spurious hierarchy of systematic over narrative reviews? Eur J Clin Invest. 2018;48(6):e12931. doi:10.1111/eci.12931
27. National Academies of Sciences E, and Medicine. Ending discrimination against people with mental and substance use disorders 2018.
28. United Nations Committee on the Rights of Persons with Disabilities. General Comment No. 1 (Article 12) 2014.
29. Dawson J. A realistic approach to assessing mental health laws’ compliance with the UNCRPD. Int J Law Psychiatry. 2015;40:70–79. doi:10.1016/j.ijlp.2015.04.003
30. Large MM, Ryan CJ, Carter G, Kapur N. Can we usefully stratify patients according to suicide risk? BMJ. 2017;359:j4627. doi:10.1136/bmj.j4627
31. Walter F, Carr MJ, Mok PLH, et al. Premature mortality among patients recently discharged from their first inpatient psychiatric treatment. JAMA Psychiatry. 2017;74(5):485–492. doi:10.1001/jamapsychiatry.2017.0071
32. United States Department of Health and Human Services. National Strategy for Suicide Prevention; 2024. https://www.ncbi.nlm.nih.gov/books/NBK604165/.
33. Elwyn G, Frosch D, Thomson R, et al. Shared decision making: a model for clinical practice. J Gen Intern Med. 2012;27(10):1361–1367. doi:10.1007/s11606-012-2077-6
34. Stiggelbout AM, Van der Weijden T, De Wit MP, et al. Shared decision making: really putting patients at the centre of healthcare. BMJ. 2012;344:e256. doi:10.1136/bmj.e256
35. Drake RE, Deegan PE, Rapp C. The promise of shared decision making in mental health. Psychiat Rehab J. 2010;34(1):7–13. doi:10.2975/34.1.2010.7.13
36. Lafrance MN, McKenzie-Mohr S. The DSM and its lure of legitimacy. Femin Psychol. 2013;23(1):119–140. doi:10.1177/0959353512467974
37. World Health Organization. Suicide. Available from: https://www.who.int/news-room/fact-sheets/detail/suicide.
38. First MB, Rebello TJ, Keeley JW, et al. Do mental health professionals use diagnostic classifications the way we think they do? A global survey. World Psychiatry. 2018;17(2):187–195. doi:10.1002/wps.20525
39. Newman DL, Moffitt TE, Caspi A, Silva PA. Comorbid mental disorders: implications for treatment and sample selection. J Abnormal Psychol. 1998;107(2):305. doi:10.1037/0021-843X.107.2.305
40. Kessler RC, Chiu WT, Demler O, Walters EE. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):617–627. doi:10.1001/archpsyc.62.6.617
41. Fried EI, Nesse RM. Depression is not a consistent syndrome: an investigation of unique symptom patterns in the STAR* D study. J Affective Disorders. 2015;172:96–102. doi:10.1016/j.jad.2014.10.010
42. Forbes MK, Neo B, Nezami OM, et al. Elemental psychopathology: distilling constituent symptoms and patterns of repetition in the diagnostic criteria of the DSM-5. Psycholog Med. 2024;54(5):886–894. doi:10.1017/S0033291723002544
43. Sartorious N. Comorbidity of mental and physical diseases: a main challenge for medicine of the 21st century. Shanghai Arch Psych. 2013;25(2):68. doi:10.3969/j.issn.1002-0829.2013.02.002
44. Kotov R, Cicero DC, Conway CC, et al. The Hierarchical Taxonomy of Psychopathology (HiTOP) in psychiatric practice and research. Psycholog Med. 2022;52(9):1666–1678. doi:10.1017/S0033291722001301
45. Kotov R, Krueger RF, Watson D, et al. The Hierarchical Taxonomy of Psychopathology (HiTOP): a dimensional alternative to traditional nosologies. J Abnormal Psychol. 2017;126(4):454. doi:10.1037/abn0000258
46. Kotov R, Krueger RF, Watson D, et al. The hierarchical taxonomy of psychopathology (HiTOP): a quantitative nosology based on consensus of evidence. Annual Rev Clin Psychol. 2021;17:83–108. doi:10.1146/annurev-clinpsy-081219-093304
47. Balling CE, South SC, Lynam DR, Samuel DB. Clinician Perception of the Clinical Utility of the Hierarchical Taxonomy of Psychopathology (HiTOP) System. Clin Psychol Sci. 2023;11:21677026221138818.
48. van der Veen S, Evans N, Huisman M, Welch Saleeby P, Widdershoven G. Toward a paradigm shift in healthcare: using the International Classification of Functioning, Disability and Health (ICF) and the capability approach (CA) jointly in theory and practice. Disability Rehabil. 2023;45(14):2382–2389. doi:10.1080/09638288.2022.2089737
49. Hemmingsson H, Jonsson H. An occupational perspective on the concept of participation in the international classification of functioning, disability and health—some critical remarks. Am J Occup Ther. 2005;59(5):569–576. doi:10.5014/ajot.59.5.569
50. Stavert J. Supported decision-making and paradigm shifts: word play or real change? Hypothesis and Theory. Front Psych. 2021. doi:10.3389/fpsyt.2020.571005
51. Walters GD. Psychology as the study of mind and behavior: two perspectives, one psychology. In: Advances in Psychology Research. Vol. 15. Nova Science Publishers; 2002:27–50.
52. Levant RF, Hasan NT. Evidence-based practice in psychology. Prof Psychol. 2008;39(6):658–662. doi:10.1037/0735-7028.39.6.658
53. Lukens EP, McFarlane WR. Psychoeducation as evidence-based practice: considerations for practice, research, and policy. Brief Treat Crisis Intervent. 2004;4(3):205–225. doi:10.1093/brief-treatment/mhh019
54. American Psychological Association. Ethical Principles of Psychologists and Code of Conduct; 2002.
55. Thrower Naomi E, Berry K, Johnston I, Morris L. Understanding the factors that contribute to creating a collaborative psychological formulation: a qualitative systematic review. Clin Psychol Psychother. 2024;31(3):e2998. doi:10.1002/cpp.2998
56. Ellis AE, Simiola V, Brown L, Courtois C, Cook JM. The role of evidence-based therapy relationships on treatment outcome for adults with trauma: a systematic review. J Trauma Dissociation. 2018;19(2):185–213. doi:10.1080/15299732.2017.1329771
57. Han HR, Miller HN, Nkimbeng M, et al. Trauma informed interventions: a systematic review. PLoS One. 2021;16(6):e0252747. doi:10.1371/journal.pone.0252747
58. Gianfrancesco O, Bubb VJ, Quinn JP. Treating the “E” in “G × E”: trauma-informed approaches and psychological therapy interventions in psychosis. Front Psych. 2019;10. doi:10.3389/fpsyt.2019.00009.
59. Pinheiro G, Alves J, Serra L. School leadership and organization in times of complexity: paths to a collaborative and regenerative school. Front Educ. 2025;10. doi:10.3389/feduc.2025.1657742.
60. Vancampfort D, Firth J, Stubbs B, et al. The efficacy, mechanisms and implementation of physical activity as an adjunctive treatment in mental disorders: a meta-review of outcomes, neurobiology and key determinants. World Psychiatry. 2025;24(2):227–239. doi:10.1002/wps.21314
61. Firth J, Solmi M, Wootton RE, et al. A meta-review of “lifestyle psychiatry”: the role of exercise, smoking, diet and sleep in the prevention and treatment of mental disorders. World Psychiatry. 2020;19(3):360–380. doi:10.1002/wps.20773
62. Singh B, Olds T, Curtis R, et al. Effectiveness of physical activity interventions for improving depression, anxiety and distress: an overview of systematic reviews. Br J Sports Med. 2023;57(18):1203–1209. doi:10.1136/bjsports-2022-106195
63. Clegg AJ, Hill JE, Mullin DS, et al. Exercise for depression. Cochrane Database Syst Rev. 2026;1(1). doi:10.1002/14651858.CD004366.pub7
64. Teychenne M, Sousa GM, Baker T, et al. Domain-specific physical activity and mental health: an updated systematic review and multilevel meta-analysis in a combined sample of 3.3 million people. Br J Sports Med. 2025;59:659–666. doi:10.1136/bjsports-2025-109806
65. Lederman OCJ, Fibbins H, Haywood D, et al. The role of exercise physiologists in mental health support and recovery: 2026 exercise and sport science Australia (ESSA) consensus statement. Br J Sports Med. 2026;60:568–582. doi:10.1136/bjsports-2025-110879
66. Firth J, Siddiqi N, Koyanagi A, et al. The Lancet Psychiatry Commission: a blueprint for protecting physical health in people with mental illness. Lancet Psychiatry. 2019;6(8):675–712. doi:10.1016/s2215-0366(19)30132-4
67. John AP, Mya T, Haywood D. Cognitive deficits among people with schizophrenia and prediabetes or diabetes. Acta psychiatrica Scand. 2024;149(1):65–76. doi:10.1111/acps.13627
68. ACoS M. ACSM’s Clinical Exercise Physiology. Lippincott Williams & Wilkins; 2019.
69. Accredited Exercise Physiologist Professional Standards for Accreditation. Exercise & Sports Science Australia (ESSA): 2021.
70. Haywood D, Mullan BA, Liddelow C, Rossell S, Castle D. A call for the increased education and use of behaviour change techniques in mental health services. Gen Hosp Psych. 2022;80:S0163–8343. doi:10.1016/j.genhosppsych.2022.11.002
71. Marques MM, Wright AJ, Corker E, et al. The behaviour change technique ontology: transforming the behaviour change technique taxonomy v1. Wellcome Open Res. 2023;8:308. doi:10.12688/wellcomeopenres.19363.1
72. Belsiyal CX, Rentala S, Das A. Use of therapeutic milieu interventions in a psychiatric setting: a systematic review. J Educ Health Promot. 2022;11:234. doi:10.4103/jehp.jehp_1501_21
73. Waldemar AK, Arnfred SM, Petersen L, Korsbek L. Recovery-oriented practice in mental health inpatient settings: a literature review. Psychiatric Serv. 2016;67(6):596–602
74. Cutcliffe JR, Stevenson C. Feeling our way in the dark: the psychiatric nursing care of suicidal people--a literature review. Int J Nurs Stud. 2008;45(6):942–953. doi:10.1016/j.ijnurstu.2007.02.002
75. Bowers L, Alexander J, Bilgin H, et al. Safewards: the empirical basis of the model and a critical appraisal. J Psychiat Mental Health Nurs. 2014;21(4):354–364. doi:10.1111/jpm.12085
76. James R, Maude P, Searby A. Clinician knowledge and attitudes of mental health advance statements in Victoria, Australia. Int J Mental Health Nurs. 2022;31(5):1164–1175. doi:10.1111/inm.13022
77. Dickens GL, Tabvuma T, Frost SA, Group SSS. Safewards: changes in conflict, containment, and violence prevention climate during implementation. Int J Mental Health Nurs. 2020;29(6):1230–1240. doi:10.1111/inm.12762
78. Kennedy H, Roper C, Randall R, et al. Consumer recommendations for enhancing the Safewards model and interventions. Int J Ment Health Nurs. 2019;28(2):616–626. doi:10.1111/inm.12570
79. Edan V, Brophy L, Hamilton B. To make another goal or to dream a different dream—a mixed method study of experiences of people using mental health advance care planning. Int J Mental Health Nurs. 2025;34(4):e70098. doi:10.1111/inm.70098
80. Kielhofner G. Conceptual Foundations of Occupational Therapy Practice. F. A. Davis Company; 2009.
81. Wilcock AA, Hocking C. An Occupational Perspective of Health.
82. Krupa T. Defining psychosocial practice in occupational therapy. In: Bruce & Borg’s Psychosocial Frames of Reference. Routledge; 2024:3–16.
83. Rudman DL, Aldrich R, Kiepek N. Evolving understandings of occupation. In: Promoting Occupational Participation: Collaborative Relationship-Focused Occupational Therapy. 2022:12–30.
84. Krupa T, Fossey E, Anthony WA, Brown C, Pitts DB. Doing daily life: how occupational therapy can inform psychiatric rehabilitation practice. Psychiatr Rehabil J. 2009;32(3):155–161. doi:10.2975/32.3.2009.155.161
85. Moll SE, Gewurtz RE, Krupa TM, Law MC, Larivière N, Levasseur M. “Do-Live-Well”: a Canadian framework for promoting occupation, health, and well-being. Can J Occup Ther. 2015;82(1):9–23. doi:10.1177/0008417414545981
86. Doroud N, Fossey E, Fortune T. Recovery as an occupational journey: a scoping review exploring the links between occupational engagement and recovery for people with enduring mental health issues. Aust Occup Ther J. 2015;62(6):378–392. doi:10.1111/1440-1630.12238
87. Fossey E, Doroud N, Harvey CA, et al. Contributions of a time use perspective in community mental health practice: a scoping review. Front Psychiatry. 2024;15:1461705. doi:10.3389/fpsyt.2024.1461705
88. Davidson L. Living Outside Mental Illness: Qualitative Studies of Recovery in Schizophrenia. New York University Press.; 2003.
89. Stuart SR, Tansey L, Quayle E, et al. Recovery narratives. J Ment Health. 2017;26(3):291–304. doi:10.1080/09638237.2016.1222056
90. Davidson L, Rakfeldt J, Strauss J. The Roots of the Recovery Movement in Psychiatry: Lessons Learned. 2010.
91. Ashby S, Gray M, Ryan S, James C. Maintaining occupation-based practice in Australian mental health practice: a critical stance. Br J Occup Ther. 2015;78(7):431–439. doi:10.1177/0308022614564168
92. Haracz K, Ennals P. Occupational therapy intervention in mental health should be individualised, occupation focussed, promote inclusion and occur in the context of an authentic relationship. Aust Occup Ther J. 2015;62(5):365–366. doi:10.1111/1440-1630.12230
93. Townsend EA, Polatajko HJ. Enabling Occupation.
94. Taylor RR, Bowyer P, Fisher G, Eds. Kielhofner’s Model of Human Occupation.
95. Townsend EA. Good Intentions Overruled. 1998.
96. Sumsion T, Law M. A review of evidence on the conceptual elements informing client-centred practice. Can J Occup Ther. 2006;73(3):153–162. doi:10.1177/000841740607300303
97. Arblaster K, Mackenzie L, Gill K, Willis K, Matthews L. Capabilities for recovery-oriented practice in mental health occupational therapy: a thematic analysis of lived experience perspectives. Br J Occup Ther. 2019;82(11):675–684. doi:10.1177/0308022619866129
98. Ryall J, Ritchie T, Butler C, Ryan A, Gibson C. Decolonising occupational therapy through a strengths-based approach. In: Occupational Therapy in Australia: Professional and Practice Issues.
99. Restall GJ, Egan MY. Collaborative relationship-focused occupational therapy: evolving lexicon and practice. Can J Occup Ther. 2021;88(3):220–230. doi:10.1177/00084174211022889
100. Scanlan J, Fossey E. Occupational Therapists. Mental Health and Collaborative Community Practice. Oxford University Press; 2021.
101. Zedel J, Chen S-P. Client’s experiences of occupational therapy group interventions in mental health settings: a meta-ethnography. Occup Ther Mental Health. 2021;37(3):278–302. doi:10.1080/0164212X.2021.1900763
102. United Nations. Universal Declaration of Human Rights. 1948. Available from: https://www.un.org/en/about-us/universal-declaration-of-human-rights.
103. International Federation of Social Workers. Global agenda for social work and social development 2020–2030. 2020. Available from: https://www.ifsw.org.
104. International Federation of Social Workers (IFSW). and the International Association of Schools of Social Work (IASSW). Global Definition Social Work. 2014. Available from. https://www.ifsw.org/what-is-social-work/global-definition-of-social-work/.:
105. Australian Association of Social Workers. Code of ethics. 2020. Available from: https://www.aasw.asn.au/document/item/1201.
106. Ramon S. Adult mental health in a changing international context: the relevance to social work. Brit J Soc Work. 2009;39(8):1615–1622. doi:10.1093/bjsw/bcp066
107. Brophy L, Bruxner A, Wilson E, Cocks N, Stylianou M. How social work can contribute in the shift to personalised, recovery-oriented psycho-social disability support services. Brit J Soc Work. 2015;45:i98–i116. doi:10.1093/bjsw/bcv094
108. Petrakis M, Brophy L, Lewis J, et al. Consumer measures and research co-production: a pilot study evaluating the recovery orientation of a mental health program collaboration. Asia Pacific J Soc Work. 2014;24:94–108. doi:10.1080/02185385.2014.885212
109. Petrakis M. Implementing the strengths model in a clinical mental health service. In:Francis A P, Pulla V, Clark M, Mariscal E S, Ponnuswami I, editors. Advancing Social Work in Mental Health Through Strengths-Based Practice.
110. Tse S, Tsoi EW, Hamilton B, et al. Uses of strength-based interventions for people with serious mental illness: a critical review. Int J Soc Psych. 2016;62(3):281–291. doi:10.1177/0020764015623970
111. Petrakis M, Aadam B. Social Workers. Mental Health and Collaborative Community Practice. Oxford University Press; 2020.
112. Hyde, Bowles, Pawar M, et al. Challenges of recovery-oriented practice in inpatient mental health settings – the potential for social work leadership. Asia Pacific Journal of Social Work and Development, Vol. 24, Nos. 1–2, 5–16. Asia Pac J Soc Work Dev. 2014;24:5–16. doi:10.1080/02185385.2014.885205
113. Rapp CA, Goscha RJ. The Strengths Model: Case Management with People with Psychiatric Disabilities. Oxford University Press; 2006.
114. Byrne L, Stratford A, Davidson L. The global need for lived experience leadership. Psychiatr Rehabil J. 2018;41(1):76–79. doi:10.1037/prj0000289
115. Burns JK. Mental health and inequity: a human rights approach to inequality, discrimination, and mental disability. Health Hum Rights. 2009;11(2):19–31.
116. Early Psychosis Guidelines Writing Group. Australian Clinical Guidelines for Early Psychosis; 2010.
117. Leamy M, Bird V, Le Boutillier C, Williams J, Slade M. Conceptual framework for personal recovery in mental health. Br J Psychiatry. 2011;199(6):445–452. doi:10.1192/bjp.bp.110.083733
118. Aadam B, Petrakis M. Ethics, Values, and Recovery in Mental Health Social Work Practice. In: Mental Health and Social Work (Social Work). Springer; 2020.
119. Roses in the Ocean. Lived experience of suicide. Available from: https://rosesintheocean.com.au/lived-experience-suicide/.
120. Repper J, Carter T. A review of the literature on peer support in mental health services. J Mental Health. 2011;20(4):392–411. doi:10.3109/09638237.2011.583947
121. Gillard S, Foster R, Gibson S, Goldsmith L, Marks J, White S. Describing a principles-based approach to developing and evaluating peer worker roles as peer support moves into mainstream mental health services. Ment Health Soc Incl. 2017;21:133–143. doi:10.1108/MHSI-03-2017-0016
122. Deegan PE, Drake RE. Shared decision making and medication management in the recovery process. Psychiat Serv. 2006;57(11):1636–1639. doi:10.1176/ps.2006.57.11.1636
123. Petrakis M, Wilson M, Hamilton B. Implementing the strengths model of case management: group supervision fidelity outcomes. Commun Mental Health J. 2013;49(3):331–337. doi:10.1007/s10597-012-9546-6
124. King AJ, Fortune TL, Byrne L, Brophy LM. Supporting the sharing of mental health challenges in the workplace: findings from comparative case study research at two mental health services. Int J Environ Res Public Health. 2021;18(23):12831. doi:10.3390/ijerph182312831
125. Krysinska K, Ozols I, Ross A, et al. Active involvement of people with lived experience of suicide in suicide research: a Delphi consensus study. BMC Psych. 2023;23(1):496. doi:10.1186/s12888-023-04973-9
126. Gilbert MM, Chamberlain JA, White CR, et al. Controlled clinical trial of a self-management program for people with mental illness in an adult mental health service - the Optimal Health Program (OHP). Aust Health Rev. 2012;36(1):1–7. doi:10.1071/ah11008
127. Ski CF, Thompson DR, Castle DJ. Trialling of an optimal health programme (OHP) across chronic disease. Trials. 2016;17(1):445. doi:10.1186/s13063-016-1560-5
128. Fukui S, Goscha R, Rapp CA, Mabry A, Liddy P, Marty D. Strengths model case management fidelity scores and client outcomes. Psychiat Serv. 2012;63(7):708–710. doi:10.1176/appi.ps.201100373
129. Freeman AM, Tribe RH, Stott JCH, Pilling S. Open Dialogue: a Review of the Evidence. Psychiat Serv. 2019;70(1):46–59. doi:10.1176/appi.ps.201800236
130. Mosse D, Pocobello R, Saunders R, Seikkula J, von Peter S. Introduction: open Dialogue around the world – implementation, outcomes, experiences and perspectives. Opinion. Front Psychol. 2023. doi:10.3389/fpsyg.2022.1093351
131. Spandler H, McKeown M. Exploring the case for truth and reconciliation in mental health services. Mental Health Rev J. 2017;22(2):83–94. doi:10.1108/MHRJ-01-2017-0011
132. Yamaguchi S, Usui K, Iwanaga M, et al. 10-year outcome trajectories of people with mental illness and their families who receive services from multidisciplinary case management and outreach teams: protocol of a multisite longitudinal study. BMJ Open. 2024;14(8):e085532. doi:10.1136/bmjopen-2024-085532
133. Dieterich M, Irving CB, Bergman H, Khokhar MA, Park B, Marshall M. Intensive case management for severe mental illness. Cochrane Database Syst Rev. 2017;1(1):Cd007906. doi:10.1002/14651858.CD007906.pub3
134. Giannios P, Chainey F, Degré C, Borduas Pagé S, Hudon A. Components and effectiveness of adult inpatient psychiatric rehabilitation programs: a scoping review. Healthcare. 2025;13(22):2971. doi:10.3390/healthcare13222971
135. Thornicroft G, Beecham J, Knapp MC. Costing psychiatric interventions. In: Measuring Mental Health Needs. Gaskell; 2001:220–224.
136. Crenshaw K. Mapping the margins: intersectionality, identity politics, and violence against women of color. Stanford Law Rev. 1991;43(6):1241–1299. doi:10.2307/1229039
137. Petrakis M, Lethborg C. An introduction to health and health services practice, and the social determinants of health. In: P M, editor. Social Work Practice in Health. Allen & Unwin; 2018:3–20.
138. National Mental Health Commission. National Safety and Quality Mental Health Standards; 2021.
139. World Health Organization. LIVE LIFE: an implementation guide for suicide prevention in countries. 2021. Available from: https://www.who.int/publications/i/item/9789240026629.
140. Torous J, Linardon J, Goldberg SB, et al. The evolving field of digital mental health: current evidence and implementation issues for smartphone apps, generative artificial intelligence, and virtual reality. World Psych. 2025;24(2):156–174. doi:10.1002/wps.21299
141. Roses in the Ocean. Lived Experience of Suicide Engagement Principles and Integration Framework; 2022.
142. Pirkis J, Dandona R, Silverman M, Khan M, Hawton K. Preventing suicide: a public health approach to a global problem. Lancet Public Health. 2024;9(10):e787–e795. doi:10.1016/s2468-2667(24)00149-x
143. World Health Organization. Guidance on community mental health services: Promoting person-centred and rights-based approaches. 2021. Available from: https://www.who.int/publications/i/item/9789240025707.
144. Gadsby EW, Wilding H. Systems thinking in, and for, public health: a call for a broader path. Health Promot Int. 2024;39(4). doi:10.1093/heapro/daae086
145. Office of Economic Co-operation and Development. A New Benchmark for Mental Health Systems: Tackling the Social and Economic Costs of Mental Ill-Health; 2021.
146. Chapman A, Buccheri A, Mohotti D, et al. Staff-reported barriers and facilitators to the implementation of healthcare interventions within regional and rural areas: a rapid review. BMC Health Serv Res. 2025;25(1):331. doi:10.1186/s12913-025-12480-8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.