Back to Journals » Infection and Drug Resistance » Volume 19
Purulent Pericarditis Caused by Polymicrobial Periodontal Pathogens (Tannerella forsythia, Fusobacterium nucleatum, and Porphyromonas gingivalis): A Case Report and Literature Review
Received 4 February 2026
Accepted for publication 15 June 2026
Published 19 June 2026 Volume 2026:19 598156
DOI https://doi.org/10.2147/IDR.S598156
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Bao-Hua Wei, Hong-Ju Da
Department of Emergency Medicine, The First Hospital of Lanzhou University, Gansu, People’s Republic of China
Correspondence: Bao-Hua Wei, Department of Emergency Medicine, The First Hospital of Lanzhou University, Gansu, People’s Republic of China, Email [email protected]
Background: Purulent pericarditis is a rare, life-threatening infection, most commonly caused by bacteria such as Staphylococcus aureus. We report an exceptional case of hematogenously disseminated infection probably originating from the oral cavity, highlighting a novel pathogen profile.
Case Presentation: We report a 66-year-old male with no history of periodontal disease or oral procedures presented with purulent pericarditis and a concomitant subphrenic abscess. Metagenomic next-generation sequencing (mNGS) of pericardial fluid revealed a polymicrobial infection with three periodontal pathogens: Tannerella forsythia, Fusobacterium nucleatum, and Porphyromonas gingivalis. The patient was treated with pericardiocentesis, targeted antibiotics, and organ support, resulting in clinical stabilization.
Conclusion: This case provides clinical evidence that a consortium of periodontal pathogens can disseminate hematogenously to cause severe metastatic infections in sterile sites, even in individuals without overt oral disease. It underscores the need to consider occult oral origins in infections of unknown source and illustrates the value of comprehensive molecular diagnostics in identifying fastidious organisms, although it remains undetermined whether both conditions were secondary to the same source.
Keywords: purulent pericarditis, subphrenic abscess, Tannerella forsythia, Fusobacterium nucleatum, Porphyromonas gingivalis, mNGS
Introduction
Purulent pericarditis is a rare, life-threatening infection of the pericardium that necessitates diagnostic and therapeutic approaches distinct from those for viral or idiopathic pericarditis.1,2 Although the incidence of this condition has significantly decreased since the introduction of antibiotics, purulent pericarditis remains associated with a high mortality rate, primarily due to delays in diagnosis and the occurrence of complications.3
Typical purulent pericarditis is commonly caused by pathogens such as Staphylococcus aureus and Streptococcus pneumoniae.4,5
To our knowledge, based on a thorough review of the available literature, this appears to be the first reported case of purulent pericarditis attributed to the concurrent infection with three recognized periodontal pathogens: Tannerella forsythia, Fusobacterium nucleatum, and Porphyromonas gingivalis. This specific polymicrobial etiology involving this exact combination of pathogens has not been commonly described in the context of purulent pericarditis.
Case Presentation
A 66-year-old man arrived at the emergency department with a four-hour history of sudden, tearing pain in left side of his chest. This was accompanied by profuse sweating, chest tightness, and shortness of breath. He had initially been evaluated at a local hospital, where an electrocardiogram (ECG) and tests for troponin-I and D-dimer came back unremarkable. Suspecting acute coronary syndrome, the medical team administered a loading dose of aspirin (300 mg) and clopidogrel (300 mg) orally; however, his chest pain persisted. He was subsequently transferred to our center for further management.
The patient’s medical history includes a cerebral infarction and a cholecystectomy. He has a smoking history of two packs per day and denies any history of hypertension, diabetes, trauma, or drug allergies.
Upon admission, his vital signs were stable, with a body temperature of 36.6°C, blood pressure of 124/71 mmHg, respiratory rate of 18 breaths per minute, and heart rate of 93 beats per minute. The patient appeared alert but lethargic. Lung auscultation revealed bilateral coarse breath sounds, and cardiac auscultation detected no pathological murmurs or pericardial friction rub.
Initial laboratory investigations revealed leukocytosis characterized by neutrophilic predominance, with a white blood cell count of 9.85 × 109/L and neutrophil percentage at 86.5%. A simultaneous assessment of inflammatory markers indicated an elevated C-reactive protein level of 33 mg/L. The electrocardiogram (ECG) was non-diagnostic. However, contrast-enhanced computed tomography (CT) of the chest and abdomen demonstrated a small pericardial effusion alongside a subphrenic mass (illustrated in Figure 1a and b).
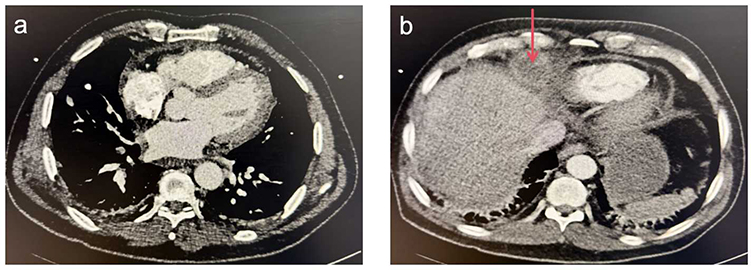 |
Figure 1 (a) Contrast-enhanced computed tomography showing a small amount of pericardial effusion. (b) Contrast-enhanced computed tomography showing a subphrenic mass (red arrow). |
While under observation in the emergency department, the patient received empirical antimicrobial and analgesic therapy, resulting in partial alleviation of chest pain over the subsequent 15 hours. Nevertheless, the clinical status of the patient deteriorated, as evidenced by the onset of fever (38.0°C), somnolence, tachycardia, and hypotension (77/54 mmHg).
Repeat diagnostic evaluations confirmed the progression of the clinical condition. The ECG displayed widespread ST-segment elevation. Subsequent laboratory tests indicated pronounced leukocytosis (15.17 × 109/L) with sustained neutrophilia (84.7%) and a significant elevation in C-reactive protein levels (207.23 mg/L). Furthermore, evidence of hyperkalemia (7.00 mmol/L), metabolic acidosis (pH 7.32), and acute hepatic and renal impairment was noted, with elevated alanine aminotransferase (308 U/L), total bilirubin (44.6 μmol/L), and creatinine (165 μmol/L) levels. An urgent transthoracic echocardiogram revealed a moderate-to-large circumferential pericardial effusion accompanied by impaired biventricular function (as depicted in Figure 2). In light of the critical presentation, a multidisciplinary consultation was convened, and the patient was urgently admitted to the intensive care unit.
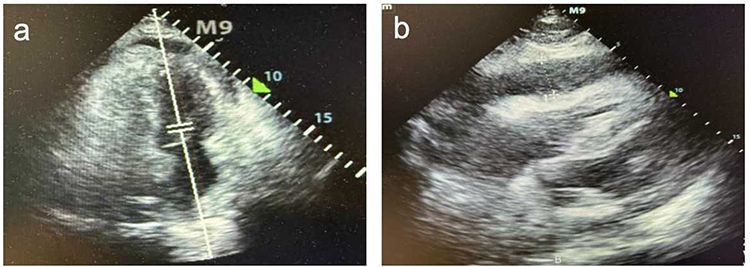 |
Figure 2 Transthoracic echocardiogram. (a) Apical 4-chamber image demonstrating a large pericardial effusion. (b) Subcostal image demonstrating early right ventricular diastolic collapse in the context of the large circumferential effusion. |
Upon admission, the patient was initiated on empirical antimicrobial therapy, consisting of piperacillin-tazobactam 4.5 g every 6 hours and moxifloxacin 0.4 g once daily. The patient underwent tracheal intubation for respiratory support and received continuous renal replacement therapy. Given the clinical presentation characterized by fever, pericardial effusion, and the subphrenic mass, the initial differential diagnosis included tuberculous pericarditis, autoimmune disorders (such as systemic lupus erythematosus), malignancies (including lymphoma or metastatic cancer), and other pyogenic bacterial infections. On the 1st day of hospitalization, a diagnostic pericardiocentesis was performed, yielding 300 mL of purulent, yellow, turbid fluid. Analysis of the effusion revealed significant biochemical markers indicative of infection: markedly low glucose (0.05 mmol/L), elevated white blood cell count (5400 cells/μL), increased protein (50.6 g/L), elevated lactate dehydrogenase levels (5056 U/L), and a positive mucin clot test. Collectively, these findings conclusively established a diagnosis of purulent pericarditis.
To investigate common pathogens, pericardial fluid and blood samples were sent for comprehensive bacterial, fungal, and mycobacterial cultures, all of which yielded negative results. A multidisciplinary team (MDT) discussed the CT findings and concluded that the mass observed in the right subphrenic area was likely an abscess. This conclusion was supported by characteristic imaging features, which included rim enhancement and a well-defined fluid collection. The lesion measured approximately 4.1×3.8 cm. The team also hypothesized that the purulent pericarditis might have resulted from the direct extension of this subphrenic infection. On the 10th day of hospitalization, given the negative results from conventional cultures and the complexity of the case, there was an urgent need for a more sensitive and rapid diagnostic approach to guide targeted therapy. As a result, the pericardial effusion was sent for mNGS analysis. CT-guided percutaneous drainage of the subphrenic mass was performed, and the fluid obtained was purulent, yellow, and turbid. The patient’s symptoms of cardiac tamponade improved significantly. On the 11th day of hospitalization, follow-up echocardiography revealed only a small amount of residual pericardial effusion. Since the drainage tube was no longer patent and could not facilitate further drainage, it was removed after a total of 1000 mL of purulent fluid had been drained.
On the 14th day of hospitalization, the mNGS findings identified the causative organisms as T. forsythia (15.4%), F. nucleatum (6.3%), and P. gingivalis (5.2%). Based on these results, the empirical antibiotic regimen of piperacillin-tazobactam and moxifloxacin was changed to targeted therapy with cefoperazone-sulbactam, administered intravenously at a dosage of 3g every 12 hours. A subsequent specialized oral examination revealed poor oral hygiene characterized by significant dental plaque and calculus. A repeat echocardiogram showed a small amount of pericardial effusion with fibrin formation and impaired biventricular diastolic function. Given the patient’s stabilized condition, the tracheal tube was successfully extubated.
On hospital day 21, the patient was discharged in stable condition. Although his renal function had not fully recovered, he was advised to follow up with the nephrology department and to undergo regular echocardiographic surveillance. The detailed timeline of clinical presentation, diagnostic workup, and therapeutic interventions is summarized in Table 1.
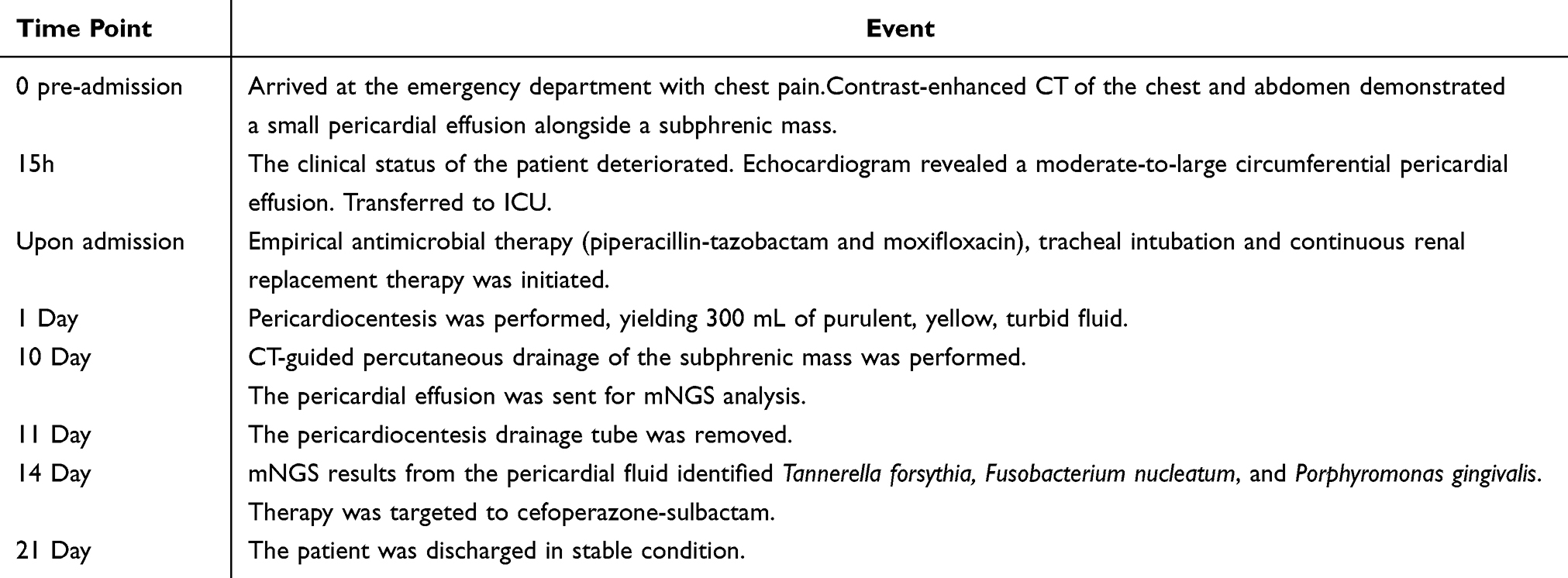 |
Table 1 Timeline of Key Clinical Events |
Discussion
Purulent pericarditis is an acute infection of the pericardium, characterized by the presence of purulent effusion, most often caused by bacterial pathogens and, in some cases, fungal pathogens.2,6 Once a significant contributor to infectious disease mortality, it has become quite rare, representing less than 1% of cases of acute pericarditis.2 Nevertheless, its mortality rate remains alarmingly high, ranging from 20% to 30%, primarily due to diagnostic delays attributed to non-specific symptoms, as well as two major complications: rapid effusion leading to cardiac tamponade and the progression of fibrinous organization to constrictive pericarditis.6–8
Typically, purulent pericarditis occurs secondary to the spread of infection from adjacent sites (such as pneumonia or empyema), hematogenous dissemination (as seen in sepsis or endocarditis), direct contamination (due to surgery or trauma), or in individuals with compromised immune systems.4
The present case, driven by the periodontal pathogens T. forsythia, F. nucleatum, and P. gingivalis, highlights the unique diagnostic challenges posed by atypical microorganisms. The isolation of this specific anaerobic triad is noteworthy. T. forsythia, F. nucleatum, and P. gingivalis are obligate anaerobic, gram-negative rods native to the oral cavity.9–11 Research in animal models has demonstrated that a single bacterial species does not induce abscess formation; rather, the combination of T. forsythia, F. nucleatum, and P. gingivalis is responsible for abscess development.12 This indicates that these three bacterial species exhibit synergistic effects. Two of these members, P. gingivalis and T. forsythia, form the core of the “red complex”, a consortium strongly linked to periodontal diseases.11 P. gingivalis is particularly recognized for its immune evasion strategies through gingipains, which may facilitate persistent bacteremia.13 F. nucleatum, often regarded as a bridging pathogen within oral biofilms, possesses adhesins such as FadA that enable the invasion of endothelial cells, potentially explaining its spread through the bloodstream to distant sites.9,11 The identification of these classic periodontal pathogens in a patient without overt symptoms of periodontitis suggests that hematogenous spread may occur through mechanisms such as subclinical dysbiosis and low-grade inflammation that can microscopically compromise the gingival epithelial barrier, and/or transient bacteremia induced by routine daily activities that may introduce bacteria into circulation.14–16 Their simultaneous presence at a distant sterile site strongly supports the hypothesis of coordinated translocation from a periodontal niche, emphasizing the oral microbiome as a possible reservoir for systemic infections.13
Conventional microbiological methods complicate this issue. Standard cultures often exhibit low sensitivity for fastidious anaerobes,17 frequently leading to “culture-negative” purulent pericarditis. As demonstrated in this study, a definitive diagnosis relied on advanced molecular techniques.18 Metagenomic next-generation sequencing (mNGS) played a crucial role, directly identifying pathogens that conventional methods failed to detect and establishing a link between the infection and a likely oral source.
The multidisciplinary team proposed that the purulent pericarditis resulted from the direct spread of a subphrenic abscess. However, since the pus from the subphrenic region was not subjected to mNGS testing, a definitive etiological conclusion could not be established. While the direct contiguous spread from the subphrenic abscess was deemed the most likely cause, it is also essential to consider the alternative possibility of hematogenous spread originating from a periodontal source. T. forsythia, F. nucleatum, and P. gingivalis have been shown to induce bacteremia and contribute to metastatic infections, revealing a synergistic role in abscess formation and systemic spread.9,13,14 Therefore, it is plausible that transient bacteremia from a periodontal site could result in concurrent seeding of both the pericardium and subphrenic space. This case highlights a critical clinical consideration: the detection of such periodontal pathogens in any sterile site should raise suspicion for a potential hidden oral source and necessitate further evaluation for additional metastatic foci.
The precise route of dissemination from the oral cavity to the pericardium in this case remains uncertain. Both direct extension from the adjacent subphrenic abscess and hematogenous spread are plausible, though neither can be definitively proven based on the available evidence.
To our knowledge, two cases of pericarditis caused by Fusobacterium nucleatum have been documented,19,20 but this appears to be a rare reported case of cardiac infection specifically linked to the periodontal pathogen triad of T. forsythia, F. nucleatum, and P. gingivalis. The underreporting of T. forsythia can likely be attributed to its fastidious nature, its role in polymicrobial infections, and historical diagnostic challenges.11,21 This case underscores the significance of molecular tools, such as mNGS, in identifying fastidious pathogens. It highlights the necessity of incorporating these diagnostic methods early in the evaluation of culture-negative or atypical infections. Additionally, it strongly suggests that a silent oral source should be considered in case of pericarditis of unknown origin, emphasizing the importance of a comprehensive dental assessment. Ultimately, this finding reinforces the concept that oral health is a crucial aspect of systemic wellness and positions the management of periodontal disease as a potential strategy for preventing focal non-oral infections.
This case report has several limitations, the most notable of which is the lack of a formal periodontal examination and diagnosis following discharge. As a result, we cannot definitively confirm whether active periodontitis is the primary source of the issue. However, there are several compelling pieces of circumstantial evidence that support this hypothesis. Firstly, the identification of the classic periodontal pathogen triad (T. forsythia, F. nucleatum, P. gingivalis) from both sterile sites is highly specific; these organisms are rarely found as part of the normal flora outside of deep periodontal pockets.9,13,17 Secondly, the specialized oral examination conducted during hospitalization provided objective documentation of poor oral hygiene characterized by significant dental plaque and calculus (degree 2), which acts as a critical prerequisite and major risk factor for periodontitis.18,22 While this finding does not replace a formal periodontal charting, it does offer a plausible anatomical and ecological environment for the pathogens in question. Therefore, although definitive confirmation of the source is lacking, the combination of microbiological and clinical evidence suggests a probable periodontal origin. This situation highlights a practical challenge in managing critically ill patients, as comprehensive dental evaluations are often postponed during acute management. Our experience emphasizes the necessity of documenting the oral health status during hospitalization and ensuring mandatory dental follow-up as part of the discharge plan for such cases. This approach is essential for confirming the source and guiding long-term preventive care. Furthermore, despite the molecular identification of periodontal pathogens, the inability to conduct concurrent oral microbiological sampling prevents us from definitively establishing causality between oral colonization and the metastatic cardiac infection.
While metagenomic next-generation sequencing (mNGS) proved instrumental in elucidating the polymicrobial etiology in this culture-negative case, it is essential to recognize the inherent limitations associated with this technology. Firstly, the potential for environmental or reagent contamination must be critically assessed. Secondly, the clinical significance of the relative abundance percentages yielded by mNGS can be ambiguous. For instance, a low-abundance signal may still reflect the presence of a true pathogen, as evidenced by the identification of Porphyromonas gingivalis in our case. Furthermore, it is important to note that mNGS detects microbial DNA but cannot intrinsically distinguish between active infection, colonization, or the presence of non-viable organisms. Thus, correlating the results with the clinical presentation—in this case, our patient with purulent pericarditis—is critical for accurately interpreting pathogenicity. Finally, a significant limitation of mNGS is its failure to provide conventional antimicrobial susceptibility data. This shortcoming necessitated the selection of empirical broad-spectrum antimicrobial therapy directed against anaerobic and oral flora, informed by both the identified pathogens and established clinical guidelines.
Conclusion
Patients with purulent pericarditis often present initially to the emergency department.23–26 The effective management of this condition requires prompt recognition by emergency physicians, with the definitive diagnosis achieved in collaboration with cardiologists. This teamwork enables the development of an appropriate treatment plan and helps prevent complications.27 This case offers compelling clinical evidence that a consortium of periodontal pathogens can lead to severe metastatic infections in sterile sites, even in individuals without evident oral disease. It highlights the importance of considering hidden oral origins in infections of unknown source and demonstrates the value of comprehensive molecular diagnostics in identifying elusive organisms.
AI Statement
We acknowledge the use of ChatGPT (OpenAI) for assistance with English language editing during manuscript preparation.
Statement of Consent
Written informed consent was obtained from the patient for the publication of this case report. Institutional review board approval was not required for this single-patient case report, and all identifying details have been removed to maintain confidentiality.
Acknowledgments
We thank all the participants for providing the available data.
Funding
No funding was received for this study.
Disclosure
Neither of the authors has any conflict of interest to disclose for this work.
References
1. Chiabrando JG, Bonaventura A, Vecchié A, et al. Management of acute and recurrent pericarditis. J Am Coll Cardiol. 2020;75(1):76–7. doi:10.1016/j.jacc.2019.11.021
2. Schulz-Menger J, Collini V, Gröschel J, et al. 2025 ESC guidelines for the management of myocarditis and pericarditis. Eur Heart J. 2025;46(40):3952–4041. doi:10.1093/eurheartj/ehaf192
3. Klacsmann PG, Bulkley H, Hutchins GM. The changed spectrum of purulent pericarditis. Am J Med. 1977;63:666–673. doi:10.1016/0002-9343(77)90150-4
4. Sagristà-Sauleda JA, Barrabés J, Permanyer-Miralda G, Soler-Soler J. Purulent pericarditis: review of a 20-year experience in a general hospital. J Am Coll Cardiol. 1993;22(6):1661–1665. doi:10.1016/0735-1097(93)90592-O
5. Pankuweit S, Ristić AD, Seferović PM, Maisch B. Bacterial Pericarditis. Am J Cardiovasc Drugs. 2005;5(2):103–112. doi:10.2165/00129784-200505020-00004
6. Augustin P, Desmard M, Mordant P, et al. Clinical review: intrapericardial fibrinolysis in management of purulent pericarditis. Crit Care. 2011;15(2):220. doi:10.1186/cc10022
7. Cremer PC, Klein AL, Imazio M. Diagnosis, risk stratification, and treatment of pericarditis: a review. JAMA. 2024;332(13):1090. doi:10.1001/jama.2024.12935
8. Adler Y, Ristić AD, Imazio M, et al. Cardiac tamponade. Nat Rev Dis Primers. 2023;9(1):36. doi:10.1038/s41572-023-00446-1
9. Han YW. Fusobacterium nucleatum: a commensal-turned pathogen. Curr Opin Microbiol. 2015;23:141–147. doi:10.1016/j.mib.2014.11.013
10. How KY, Song KP, Chan KG. Porphyromonas gingivalis: an overview of periodontopathic pathogen below the gum line. Front Microbiol. 2016;7. doi:10.3389/fmicb.2016.00053
11. Sharma A. Virulence mechanisms of Tannerella forsythia. Periodontology 2000. 2010;54(1):106–116. doi:10.1111/j.1600-0757.2009.00332.x
12. Takemoto T, Kurihara H, Dahlen G. Characterization of Bacteroides forsythus isolates. J Clin Microbiol. 1997;35(6):1378–1381. doi:10.1128/jcm.35.6.1378-1381.1997
13. Holt SC, Ebersole JL. Porphyromonas gingivalis, Treponema denticola, and Tannerella forsythia: the ‘red complex’, a prototype polybacterial pathogenic consortium in periodontitis. Periodontology 2000. 2005;38(1):72–122. doi:10.1111/j.1600-0757.2005.00113.x
14. Hajishengallis G. Periodontitis: from microbial immune subversion to systemic inflammation. Nat Rev Immunol. 2015;15(1):30–44. doi:10.1038/nri3785
15. Tomás I, Diz P, Tobías A, Scully C, Donos N. Periodontal health status and bacteraemia from daily oral activities: systematic review/meta-analysis. J Clinic Periodontology. 2012;39(3):213–228. doi:10.1111/j.1600-051X.2011.01784.x
16. Figuero E, Sánchez-Beltrán M, Cuesta-Frechoso S, et al. Detection of periodontal bacteria in atheromatous plaque by nested polymerase chain reaction. J Periodontol. 2011;82(10):1469–1477. doi:10.1902/jop.2011.100719
17. Tanner ACR, Izard J. Tannerella forsythia, a periodontal pathogen entering the genomic era. Periodontology 2000. 2006;42(1):88–113. doi:10.1111/j.1600-0757.2006.00184.x
18. Marsh PD. Dental plaque as a biofilm and a microbial community – implications for health and disease. BMC Oral Health. 2006;6(1):S14. doi:10.1186/1472-6831-6-S1-S14
19. Kearney A, Knoll B. Myopericarditis associated with Fusobacterium nucleatum-caused liver abscess. Infect Dis. 2015;47(3):187–189. doi:10.3109/00365548.2014.969306
20. Truant AL, Menge S, Milliorn K, Lairscey R, Kelly MT. Fusobacterium nucleatum pericarditis. J Clin Microbiol. 1983;17(2):349–351. doi:10.1128/jcm.17.2.349-351.1983
21. Stefanopoulos PK, Kolokotronis AE. The clinical significance of anaerobic bacteria in acute orofacial odontogenic infections. Oral Surg Oral Med Oral Pathol Oral Radiol. 2004;98(4):398–408. doi:10.1016/j.tripleo.2004.01.016
22. Akcalı A, Lang NP. Dental calculus: the calcified biofilm and its role in disease development. Periodontology 2000. 2018;76(1):109–115. doi:10.1111/prd.12151
23. Huang B, Yeh JK. Eikenella corrodens and Parvimonas micra purulent pericarditis following oral fish bone impaction: a case report. BMC Infect Dis. 2025;25(1):232. doi:10.1186/s12879-025-10624-z
24. Yamaguchi H, Nagasaki K, Kobayashi H. Purulent Pericarditis due to Pneumococcal bacteremia caused by acupuncture: an autopsy case report. Internal Medicine. 2023;62(6):939–943. doi:10.2169/internalmedicine.0102-22
25. Hori K, Arai R, Kuwana T, et al. Purulent Pericarditis and Septic Shock Caused by Nontypeable Haemophilus Influenzae in an Immunocompromised Patient: a Case Report. IDR. 2025;18:3199–3205. doi:10.2147/IDR.S530643
26. Steffen C, Sägmüller J, Schöneburg D, et al. Pyopericardium with cardiac tamponade caused by pyogenic liver abscess: a case report. J Med Case Rep. 2025;19(1):7. doi:10.1186/s13256-024-05014-z
27. Bouriche F, Toro A, Negre V, Yvorra S. Acute Pericarditis: aetiologic diagnosis and practical aspect of the management. Curr Prob Cardiol. 2021;46(4):100769. doi:10.1016/j.cpcardiol.2020.100769
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.