Back to Journals » Psychology Research and Behavior Management » Volume 16
Purpose Orientation and Its Protective Effect on Self-Esteem Among Chinese Depressive Patients: A Comparative Study
Received 15 August 2023
Accepted for publication 11 November 2023
Published 22 December 2023 Volume 2023:16 Pages 5197—5207
DOI https://doi.org/10.2147/PRBM.S435433
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Dannuo Lyu,1 Xiaosong Gai,1,2 Yanfeng Zhong3
1School of Psychology, Northeast Normal University, Changchun, Jilin Province, People’s Republic of China; 2Research Center of Mental Health Education in Northeast Normal University, Key Research Institute of Humanities and Social Science in Universities in Jilin Province, Changchun, Jilin Province, People’s Republic of China; 3Changchun Sixth Hospital, Changchun, Jilin Province, People’s Republic of China
Correspondence: Xiaosong Gai, Northeast Normal University, Nanling Street, Changchun City, Jilin Province, 130024, People’s Republic of China, Tel +86 186 4307 2597, Email [email protected]
Purpose: Although previous studies have confirmed that purpose in life may negatively predict depressive symptoms, focusing on the intensity of purpose without focusing on content may ignore significant individual differences. This study explores differences in purpose orientations between depressive patients and healthy population to examine the relationship between the purpose content and self-esteem, one of the symptoms of depression. In addition, the moderating role of purpose orientations in the relationship between depression and self-esteem was analyzed to verify the protective effect of purpose orientation on self-esteem.
Patients and Methods: The study utilized the questionnaire approach. The Purpose Orientation Scale (Self and Forced Rating) and the Rosenberg Self-Esteem Scale were administered to the participants. The study recruited 73 depressive patients using convenience sampling. Moreover, using random sampling, 146 participants matched based on depressive patients’ demographics were selected as a healthy population in a 1:2 ratio.
Results: The results showed that: 1) depressive patients valued all four types of purpose orientations to a lesser extent compared to healthy population, both depressive patients and healthy population valued family well-being and personal growth to a greater extent than personal well-being and social promotion. 2) Depressive patients reported lower self-esteem than healthy people. 3) All four types of Purpose orientations positively correlated with self-esteem in depressive patients, while only personal well-being positively correlated with self-esteem in healthy population. Family well-being and social promotion moderated the predictive effect of depression on self-esteem.
Conclusion: The above results imply that prosocial purpose orientations may attenuate the harmful effects of depression on self-esteem. Additionally, intervention focusing on enhancing depressive patients’ purpose in life (especially prosocial purpose) could be helpful.
Keywords: purpose in life, meaning in life, self-esteem, hopelessness, prosocial
Introduction
Depression has become a significant public health problem. According to the survey, the detection rate of depression risk among Chinese is as high as 10.6%,1 and the weighted lifetime prevalence of major depressive disorder reached 3.4%.2 Numerous related studies have found that depression impairs patients’ social functioning and physical and mental health and increases the risk of death due to its high relapse and suicide rates.3 The lifetime prevalence of suicidal ideation and attempted suicide in Chinese depressive patients was 53.1% and 23.7%, respectively. Psychopathological research on depression has been a popular topic in clinical psychology recently. Following the call to identify protective factors for depression, we tested whether the purpose in life and its content would be related to self-esteem, one of the symptoms of depression. Specifically, we compared the importance depressive patients and healthy people placed on each purpose orientation and examined whether each purpose orientation might play a moderating role in predicting depression on self-esteem.
Purpose in Life and Depression
Meaning in life is a stable resource for maintaining well-being and avoiding hopelessness.4 According to the Hopelessness Theory,5,6 hopelessness is a sufficient condition for depression,7 and helplessness is a necessary component of hopelessness. Other factors such as absence of meaning are also contributing causes of depression. The search for and the presence of meaning in life is an essential process in psychological development, and the absence of meaning can lead to mental health problems. Previous research found that lack of meaning in life is one of the causes of depression.8
The level of meaning depends on the extent to which people have a purpose in life.8–11 Purpose in life, has been defined as having goals and a sense of direction that gives meaning to one’s life and existence,12 which drives individuals to accomplish things that are meaningful to the self and society.13,14 Purpose in life, one of the six components of well-being in the Six-factor Model of Psychological Well-being,12 has been viewed as a high-level psychological construct that can be used to explain why and how people stay healthy and happy.15–17 Research has shown that people with a sense of purpose experience higher positive emotions, hope,18 and happiness.19 Purpose in life directly and negatively predicted levels of hopelessness20 and played an important mediating role between mood dysregulation and hopelessness.21 A meta-analytic study found that higher levels of purpose in life were significantly related with lower levels of depression, and the mean weighted effect size between purpose in life and depression was r = −0.49.22 A recent study found that having a sense of purpose in life was a protective factor against depression during the COVID-19 pandemic.23 Hence, purpose in life is a psychological resource in the face of adversity, and its absence is a cause of depression. To summarize, we propose Hypothesis 1: depressive patients value each purpose orientation less than healthy population.
Purpose Orientation and Depression
However, most of the instruments used in previous research about the relationship between purpose and depression only measure the intensity of purpose without focusing on the content of purpose,23 which may ignore significant individual differences.24 This study focused on purpose orientation, defined as the content of one’s life purpose, which was found to lead to different patterns of living and to be differentially related to well-being.25 Precisely, research confirms that prosocial purpose orientations are more adaptive and associated with higher well-being.26 For instance, prosocial purpose orientations predicted creativity, personal growth, and integrity27 and were associated with greater psychological resilience.28 People focusing on family-centered purpose orientations showed greater happiness and fewer negative life events after two years. In contrast, people focusing on self-centered purpose orientations showed lower happiness levels at follow-up29 and were associated with a sustained decline in lifetime life satisfaction.30 Concerning depression, Prager et al found that patients with depression were less likely to value transcendent goals (for example, upholding human values and ideals and concern for human rights) than a healthy population.31 However, the study had a small sample size and did not use a rigorous matching method. Therefore, to control for irrelevant variables in this study, the demographic variables of the depressive patients and the healthy population were rigorously matched in the present study. Thus, we propose Hypothesis 2: regarding the order of purpose orientations, depressive patients gave less weight to prosocial purpose orientations than healthy population.
Self-Esteem, Purpose, and Depression
Self-esteem reflects the gap between a person’s perceived actual and ideal selves.32 Patients with depression feel hopeless and helpless to reduce the gap between their actual and ideal selves. According to the Hopelessness Theory, when an adverse event occurs, depressive patients anticipate that others will achieve an outcome they feel hopeless about. Furthermore, when depressive patients make adverse inferences about their self-worth, the negative traits (they feel helpless to change) are critical to the overall self-concept, leading to decreased self-esteem.5 Moreover, self-esteem as defined by the DSM-5 is one of the core symptoms of depression.33 Empirically a meta-analysis of 77 studies on the relationship between depression and self-esteem confirmed the negative prediction of depression on self-esteem.34 Thus, we propose Hypothesis 3: depressive patients have lower levels of self-esteem than healthy population.
However, the relationship between depression and self-esteem may be limited by purpose in life. Previous research found a relationship between self-esteem and purpose in life. Such as, purpose in life was found to be a strong predictor of self-esteem,35 whereas instability in self-esteem was associated with unclear purpose.36 In addition, low self-esteem in depressive patients was associated with hopelessness, but purpose in life can provide hope.18,19 And prosocial purpose orientations tend to be more adaptive, its protective effect on self-esteem may be more prominent in depressive patients. Qualitative research found that students who defined their purpose as contributing to society showed higher self-worth and confidence in realizing their potential.37 Empirical studies have also found that people who are committed to contributing to the world beyond themselves have higher levels of self-esteem.38 To summarize, the study proposes the Hypothesis 4: Purpose orientations, especially prosocial purposes, may attenuate the detrimental effects of depression on self-esteem.
The Present Study
Previous research on purpose and depression has examined only the intensity of purpose without focusing on content, whereas prosocial purpose is more adaptive than other purpose. Therefore, we aimed to examine the relationship between purpose content and depression by comparing the intensity and order of purpose orientations in depressive patients and healthy people. In addition, depression leads to lower self-esteem, and purpose in life positively predicts self-esteem levels. Therefore, in order to test whether purpose orientation is a protective factor for self-esteem in depressive patients, the study examined the relationship between each purpose orientation and self-esteem within two groups, depressive patients and healthy people, respectively, and further examined the moderating role of purpose orientation in the negative prediction of self-esteem by depression.
On this basis, the study aimed to examine the following four hypotheses: (1) Depressive patients value each purpose orientation less than healthy population; (2) Regarding the order of purpose orientations, depressive patients gave less weight to prosocial purpose orientations than healthy population; (3) Depressive patients have lower levels of self-esteem than healthy population; (4) Purpose orientations, especially prosocial purposes, may attenuate the detrimental effects of depression on self-esteem.
Materials and Methods
Participants
The sample for this study comprised both depressive patients and healthy people. We recruited 73 participants, using convenience sampling, who were diagnosed with clinical depression and were being treated for depression as outpatients in a hospital in Jilin Province. The diagnosis of depressive patients was consistent with the DSM-V diagnostic criteria. We recruited 2507 healthy people using convenience sampling. Using random sampling, we selected 146 participants as the healthy population sample as the control group, with a ratio of healthy people to depressive people of 2:1. The demographic variables of the depressive patients and the healthy population were strictly matched.
In total, there were 219 participants in this study, including 73 depressive patients and 146 healthy people. Age ranged from 13 to 66 years old, with a mean age of 21.77±10.01 years. To test the validity of the matching method, we compared the demographic variables between the two groups. There was no significant difference in age between depressive patients (M=21.85, SD=10.23) and the healthy population (M=21.73, SD=9.93, t(140.41)=.083, p=0.93). Similarly, there were no significant differences between the two groups regarding gender, level of education, residence, and occupation, as shown in Table 1. The results provide support for the validity of the matching method.
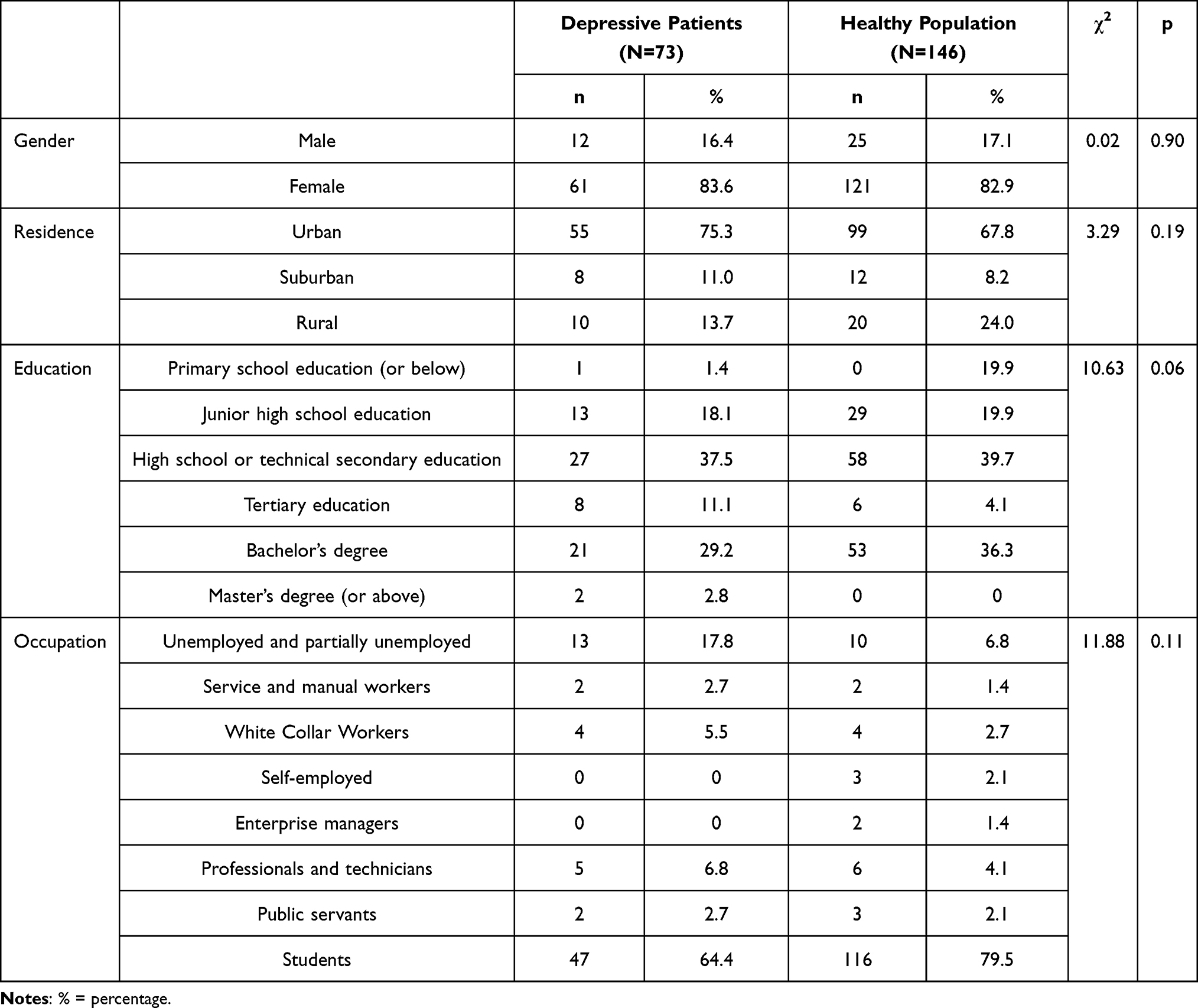 |
Table 1 Differences in Demographics Between Depression Inpatients and a Healthy Population |
The study complies with the Declaration of Helsinki. The study protocol has been approved by the Ethics Committee of the School of Psychology, Northeast Normal University (Reference No. 2021033). In this study, participants gave informed verbal consent before completing the questionnaire, and those under the age of 18 had the consent of a parent or legal guardian.
Research Design
At the outpatient unit of the hospital, using convenience sampling, the study recruited 87 depressive patients to complete paper questionnaires. Using convenience sampling, 2873 healthy participants from Jilin Province were recruited to complete online questionnaires distributed on the WJX platform (https://www.wjx.cn). We used lie detection questions to reduce social desirability, and ultimately 73 depressive patients and 2507 participants with mean scores greater than or equal to three were retained as usable data. Out of 2507 healthy participants, we randomly selected 146 as the control group for the depressive group. Using a depressive patient as an example, the following is our matching process. First, we filtered out healthy people who matched the demographics of this depressive patient; Second, we randomly selected two people from the filtered healthy people. To avoid getting duplicate data, healthy people who have already been selected will be excluded from the next filter.
Measures
The Youth Purpose Orientations Scale25 was used to measure purpose orientations. The scale is present in two forms, the Youth Purpose Orientation Scale-Self Rating (YPOS-SR) and the Youth Purpose Orientation Scale-Forced Choice (YPOS-FC). The scale measures four purpose orientations. YPOS-SR measures the intensity and order of each purpose orientation, while YPOS-FC only measures the order of purpose orientation.
The YPOS-SR is composed of 19 items measuring four purpose orientations, family well-being (eg, Having a happy family), social promotion (eg, Making society a better place), personal growth (eg, Having a satisfying job), and personal well-being (eg, Living a colorful life). YPOS-SR is a 5-point Likert scale ranging from 1 (extremely unimportant) to 5 (extremely important), with higher scores indicating greater importance of the orientation. Cronbach’s alpha coefficients39 of the four purpose orientations were as follows, family well-being (α = 0.809), social promotion (α = 0.906), personal growth (α = 0.894), and personal well-being (α = 0.912). A confirmatory factor analysis (CFA) was performed using Mplus with model fit indices of X2/df = 2.790, CFI = 0.919, TLI = 0.903, RMSEA = 0.091, and SRMR = 0.061.
Similarly, the YPOS-FC measures the four purpose orientations. The scale asks participants which purpose orientation they value more by comparing purpose orientations to each other. For example, the scale asks “What you seek in life is? (A) To live a colorful life or (B) To make society a better place. Each of the two purpose orientations is compared three times as a set, using different items. The two-by-two comparisons between the four purpose orientations makes a total of six sets of 18 items. Level of importance is calculated through the highest to lowest scores of each purpose orientation. Since every two purpose orientations are compared three times, the probability of a participant choosing the same purpose orientation three times in a random response is 25%. The average probability of a participant choosing the same purpose orientations three times in each set of comparison in this study is 56.5%, higher than the random level of 25%. Therefore, the scale is considered to have good reliability.
The Rosenberg Self-Esteem Scale was used to measure the level of self-esteem.32 The questionnaire consists of 10 items and has a one-factor structure. The questionnaire is scored on a 4-point Likert scale ranging from 1(strongly disagree) to 4(strongly agree). Items 3, 5, 8, 9, and 10 are reverse-scored. Chinese scholars pointed out that item 8 has cultural differences between Chinese and Western cultures and should be deleted or changed to positive scoring,40 so item 8 was positively scored. Higher scores indicate higher levels of participants’ self-esteem. The Cronbach alpha coefficient39 for this scale in this study was 0.743. A confirmatory factor analysis (CFA) was performed using Mplus with model fit indices of X2/df = 2.576, CFI = 0.950, TLI = 0.934, RMSEA = 0.085, and SRMR = 0.047.
Analysis
All statistical analyses were performed using IBM SPSS version 25.0 software. First, we analyzed the self-report data of purpose orientation using an independent samples t-test to compare differences in the intensity of purpose orientation between depressive and healthy populations. We also used independent samples t-tests to compare differences in self-esteem levels between the two groups. Second, we present the ordering of purpose orientation by the two groups using forced-choice data. We further analyzed the self-rating data for purpose orientation using paired sample t-tests to obtain rankings within each group. Finally, we used the Pearson correlation to test the relationship between purpose orientation (self-rating) and self-esteem for each group. PROCESS MACRO 3.4.1 Model 1 was used to test the moderating effects of purpose orientations (self-rating) on the depression-self-esteem interaction.
Common Method Bias Test
Since questionnaires were used in this study, Harman’s single-factor test was used to test common method bias. This technique assumes that if there is a significant amount of common method bias, either (a) a single factor emerges from factor analysis or (b) a general factor accounts for most covariance among measures.41 The results showed that the variance contribution rate of the first common factor was 24.80%, which was lower than the critical value of 40%, so there is no serious systematic error from using the same measurement method.
Results
Using an independent samples t-test to compare differences in the intensity of purpose orientation between depressive and healthy populations. Based on the results of the self-report questionnaire, the depressive patients had significantly lower scores on all four purpose orientations, as shown in Table 2, which was consistent with Hypothesis 1.
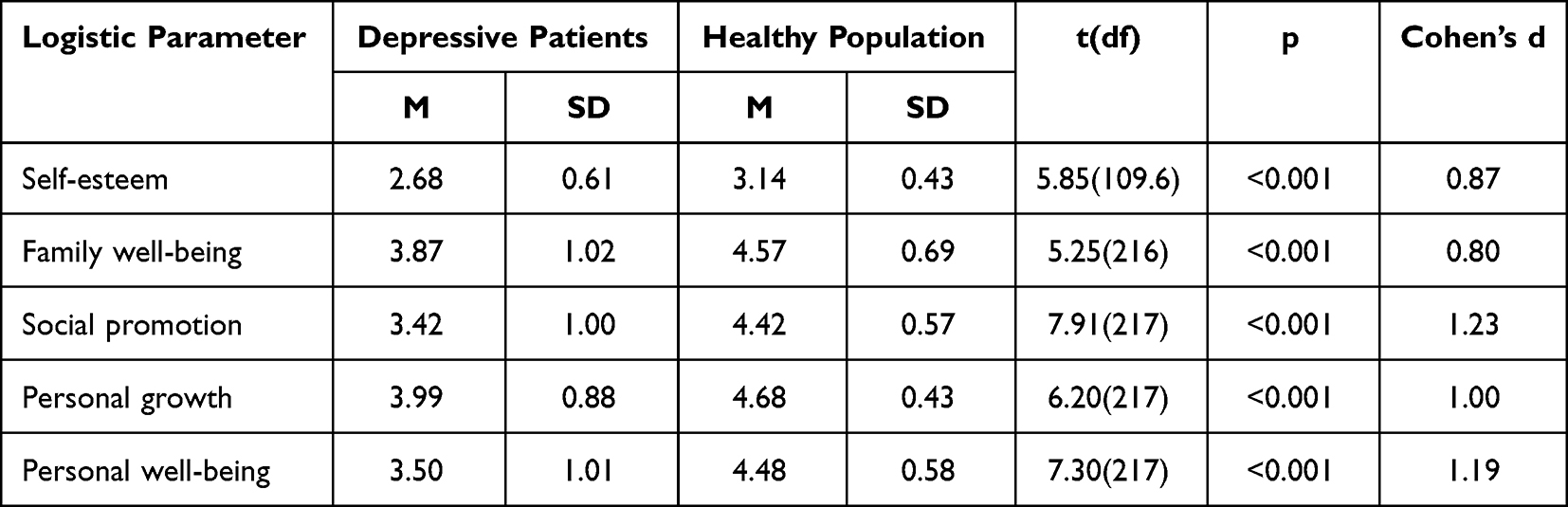 |
Table 2 Difference in Self-Esteem and Purpose Orientations (Self-Rating) Across the Two Groups |
Moreover, to compare the order of importance participants placed on each purpose orientation within the two groups, descriptive statistic was used. Based on the results of the forced-choice questionnaire, both groups attached the greatest importance on family well-being (depressive patients: M = 6.20, SD = 2.49; healthy population: M = 6.23, SD = 2.55), followed by personal growth (depressive patients: M = 5.60, SD = 2.08; healthy population: M = 5.03, SD = 1.91), personal well-being (depressive patients: M = 4.17, SD = 2.30; healthy population: M = 4.05, SD = 2.18), and least importance was social promotion (depressive patients: M = 2.03, SD = 2.01; healthy population: M = 2.69, SD = 2.43).
Additionally, based on the results of the self-report questionnaire, a paired sample t-test results showed that within the depressive group, participants placed significantly more importance on family well-being than on social promotion (t(72) = 4.15, p < 0.001, Cohen’s d = 0.49) and personal well-being (t(72) = 3.04, p = 0.003<0.01, Cohen’s d = 0.36). Also, within the depressive group, participants placed significantly more importance on personal growth than on social promotion (t(72)=5.37, p < 0.001, Cohen’s d = 0.63). Similarly, in the healthy population, participants significantly valued family well-being (t(144) = 2.52, p = 0.01<0.05, Cohen’s d = 0.21) and personal growth (t(144) = 6.59, p < 0.001, Cohen’s d = 0.55,) more than social promotion. The results of both the self-report and forced-choice questionnaires indicated that the two groups ranked purpose orientation similarly, which is inconsistent with Hypothesis 2.
The self-esteem levels of the two groups were compared using an independent samples t-test. As shown in Table 2, the depressive patients had significantly lower self-esteem levels than the healthy population, which is consistent with Hypothesis 3.
To test whether purpose orientation protects the level of self-esteem in depressive patients, we first examined the correlation between purpose orientation (self-rating) and self-esteem within the groups. The results of Pearson’s correlation showed that, in the healthy population group, only personal well-being was significantly correlated with self-esteem. However, in the depressive patients’ group, all purpose orientations were significantly associated with self-esteem, as shown in Table 3.
 |
Table 3 Correlation Analysis Between Purpose Orientation (Self-Rating) and Self-Esteem |
Process macro (Model 1) was used to test whether each purpose orientation (self-rating) moderated whether depression was a predictor of self-esteem (Hypothesis 3). Whether or not a person suffers from depression was a categorical dummy coded variable (depression = 0; healthy = 1). Also, purpose orientations and self-esteem levels, as continuous variables, were standardized before entering the model. The results indicated that family well-being and social promotion both played a moderating role in the relationship between depression and self-esteem (see Table 4).
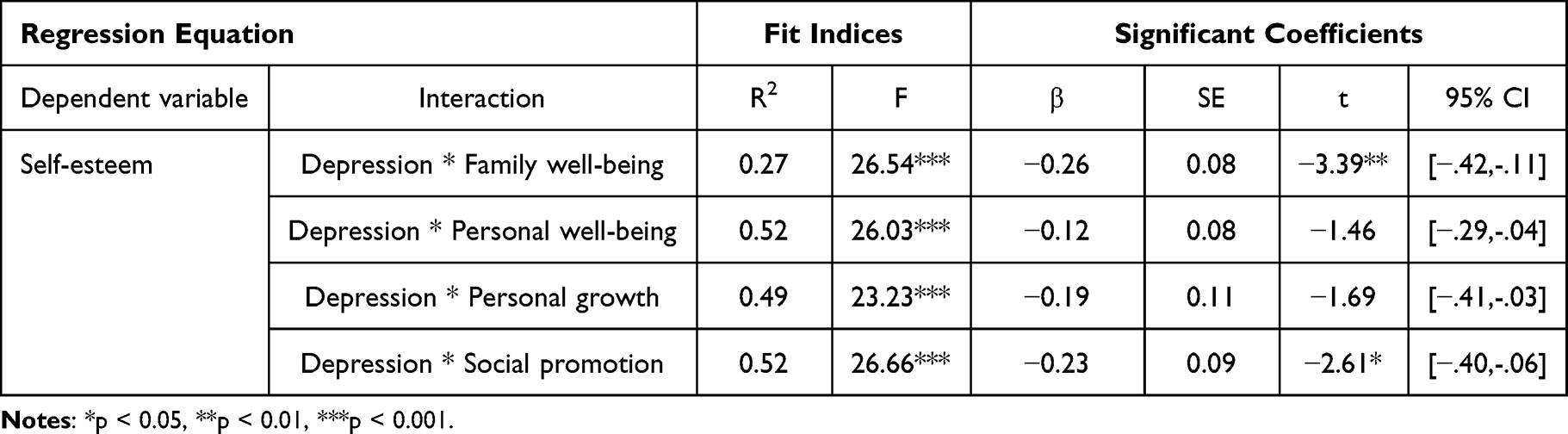 |
Table 4 Predictors of the Interaction Between Depression and Each Orientation on Self-Esteem |
The moderating effects were further explored using simple slope analyses. Family well-being was further coded into M -/+ 1SD. When family well-being was low (M-1SD), depression significantly predicted self-esteem levels (β = 0.55, SE = 0.09, p < 0.001). The prediction weakened as family well-being increased. When family well-being was high (M+1SD), depression no longer had a significant predictive effect on self-esteem (β = 0.14, SE = 0.09, p = 0.13>0.05) (see Figure 1a). In the same manner, social promotion was further analyzed. When social promotion was low (M-1SD), depression was a significant predictor of self-esteem levels (β = 0.44, SE = 0.11, p < 0.001). As social promotion increased the prediction effect of depression was weaker. When social promotion was high (M+1SD), depression was no longer a significant predictor of self-esteem (β = 0.04, SE = 0.11, p = 0.72>0.05) (see Figure 1b). Prosocial purposes attenuate the detrimental effects of depression on self-esteem, which is consistent with Hypothesis 4.
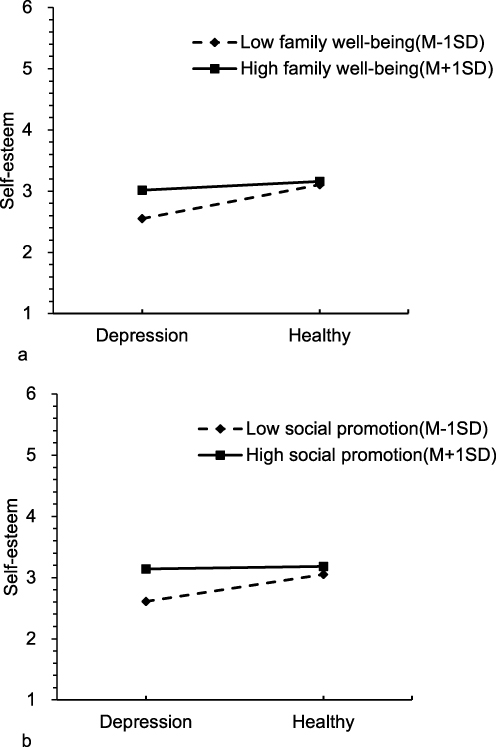 |
Figure 1 (a) Relationship between depression and self-esteem at high and low levels of family well-being; (b) Relationship between depression and self-esteem at high and low levels of social promotion. |
Discussion
Purpose Orientations’ Value
The study found that the depressive patients rated less intensely purpose orientations compared to the healthy population, consistent with Hypothesis 1. Previous research focused on diminished interest as symptoms of depression (for instance, appetite),33 the present study uncovered a deeper diminished interest. The depressive patients group attached low importance on all purpose orientations. Previous studies found that lack of purpose predicted an increase in depressive symptoms two months later.42 In contrast, increased identification with purpose predicted increased life satisfaction and decreased depressive symptoms.43
Inconsistent with Hypothesis 2, the study found that the depressive patients and the healthy population ranked purpose orientations similarly, although the depressive patients rated less intensely purpose orientations. Both groups valued family well-being and personal growth to a greater extent, compared to personal well-being and social promotion. Family well-being was the most frequently selected, while social promotion was the most frequently abandoned purpose orientations. Even though these results partially reject Hypothesis 2, they provide an understanding of purpose orientations’ value in the Chinese context. First, these results showed that family has an important role in the Chinese culture.44 Second, the results are consistent with studies on sources of meaning. Previous studies found that although sources of meaning are very complex45 and vary widely,31 family (as a source of meaning) satisfies people’s need for a sense of belonging46 and is a strong and important source of meaning in life.47 Finally, these results are also consistent with Fei’s concept of “The Differential Mode of Association”.48 Chinese social relationships are centered around the inner circle of the social network followed by the macro-society. Thus, in the Chinese context, whether individuals suffer from depression or not, family well-being will be of greatest importance while social promotion will be of least importance.
Purpose Orientations as Protective Factors
Consistent with Hypothesis 3, 4, Although the depressive patients had significantly lower levels of self-esteem than the healthy population, individuals with depression link their purpose orientations with self-esteem to a higher extent than individuals not suffering from depression. In the depressive patients group, all four purpose orientations positively correlated with self-esteem, whereas in the healthy population only personal well-being positively correlated with self-esteem. This might be explained through the hopelessness and helplessness individuals suffering from depression feel toward their actual and ideal selves. On the one hand, individuals suffering from depression assume they have no hope of achieving the outcomes others can achieve5 and have a highly conditioned self-worth. On the other hand, individuals suffering from depression experience more negative affect than healthy population, have more negative perceptions of themselves, and feel helpless to change.5 Purpose in life is the basis of personal coherence, an expression of core values and interests. It provides a psychological framework for goal-seeking that can facilitate depressive patients’ coherent understanding of who they are.15 Additionally, purpose in life may play a protective role in the face of negativity.49 For example, it has been found that even when experiencing high levels of negative affect, people with high levels of purpose still report high levels of life satisfaction.35 In a healthy population, however, there is no difference in the extent to which individuals value family well-being, social promotion, and personal growth regardless of self-esteem levels. Individuals with high self-esteem perceive themselves as more entitled to a good life. Thus, only personal well-being was positively associated with self-esteem levels in a healthy population.
Consistent with Hypothesis 3, Family well-being and social promotion can be considered a psychological resource that moderates the detrimental effects of depression on self-esteem. The difference in self-esteem levels between the two groups was no longer significant when the patients valued family well-being and social promotion. Previous research found that prosocial behavior was negatively associated with depressive symptoms for any age group.50,51 Prosocial behavior is an important socialization process in human development and is essential to people’s physical and mental health and social development. The definition of purpose in life also emphasizes the prosocial component, suggesting that purpose makes people want to make a difference in the world and contribute to something more important than themselves.14 When individuals view engaging in prosocial behaviors as having a purpose in life, they perceive having something to accomplish in the world as meaningful beyond their self-interest. Moreover, engaging in prosocial behavior directed to a purpose in life motivates individuals to engage in relevant activities both in the present and in the future.52 As a result, individuals with prosocial purposes are more likely to maintain a good psychological state.26–28
Additionally, previous research has shown that interventions that help people commit to and pursue a purpose can significantly reduce an individual’s depression.53 The above findings imply that focusing on prosocial purpose may lead to better outcomes in interventions that help depressive patients to commit to and pursue a purpose in life.
Limitations
Finally, the study has the following limitations. First, the measurement tool used in this study only examined the level of importance attached to each purpose orientation and the dimension of presence-search could be included in the measurement model in future studies. Second, the study was cross-sectional, and future studies could use cross-lagged panel, experimental, and intervention designs to examine the causal relationship between purpose orientations and depressive symptoms.
Conclusion
Although depressive patients have a lower intensity of purpose orientation than healthy people, both populations ranked the importance of purpose orientations in the same order, placing greater importance on family well-being and personal growth and lesser importance on personal well-being and social promotion. Although depression leads to a decline in self-esteem, purpose orientation can play a protective role. Specifically, all four purpose orientations were significantly and positively associated with self-esteem in depressive patients, whereas only personal well-being was significantly and positively associated with self-esteem in healthy population. Moreover, Family well-being and social promotion played a moderating role in the interaction between depression and self-esteem. In summary, this study implicated that intervention focusing on enhancing depressive patients’ purpose in life (especially prosocial purpose) could alleviate the symptoms of depression.
Ethics Approval
All participants gave informed consent prior to their inclusion in the study. The study design was approved by the Ethics Committee of School of Psychology, Northeast Normal University.
Acknowledgments
Thanks to all the participants and volunteers who provided support for this study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
We declare that there is no conflict of interest.
References
1. Huang Y, Wang Y, Wang H, et al. Prevalence of mental disorders in China: a cross-sectional epidemiological study. Lancet Psychiatry. 2019;6(3):211–224. doi:10.1016/S2215-0366(18)30511-X
2. Fu XL, Zhang K. Report on National Mental Health Development in China (2021-2022). Beijing: SOCIAL SCIENCES ACADEMIC PRESS (CHINA); 2022.
3. Kessler RC, Bromet EJ. The epidemiology of depression across cultures. Annu Rev Public Health. 2013;34(1):119–138. doi:10.1146/annurev-publhealth-031912-114409
4. Frankl VE. Man’s Search for Meaning. New York: Simon and Schuster; 1963.
5. Abramson LY, Metalsky GI, Alloy LB. Hopelessness depression: a theory-based subtype of depression. Psychol Rev. 1989;96(2):358–372. doi:10.1037/0033-295X.96.2.358
6. Abramson LY, Garber J, Edwards NB, et al. Expectancy changes in depression and schizophrenia. J Abnorm Psychol. 1978;87(1):49–74. doi:10.1037/0021-843X.87.1.49
7. Metalsky GI, Joiner TE, Hardin TS, et al. Depressive reactions to failure in a naturalistic setting: a test of the hopelessness and self-esteem theories of depression. J Abnorm Psychol. 1993;102(1):101–109. doi:10.1037/0021-843X.102.1.101
8. Steger MF, Frazier P, Oishi S, et al. The meaning in life questionnaire: assessing the presence of and search for meaning in life. J Couns Psychol. 2006;53(1):80–93. doi:10.1037/0022-0167.53.1.80
9. Steger MF; Meaning in life. Oxford Handbook of Positive Psychology.
10. Steger MF, Kashdan TB. The unbearable lightness of meaning: well-being and unstable meaning in life. J Posit Psychol. 2013;8(2):103–115. doi:10.1080/17439760.2013.771208
11. Huo JY, Wang XQ, Steger MF, et al. Implicit meaning in life: the assessment and construct validity of implicit meaning in life and relations with explicit meaning in life and depression. J Posit Psychol. 2019. 15:500–518.
12. Ryff CD. Psychological well-being revisited: advances in the science and practice of eudaimonia. Psychother Psychosom. 2014;83(1):10–28. doi:10.1159/000353263
13. Sharma G, Yukhymenko-Lescroart MA. A framework for cultivating purpose as a pedagogy of care. Ital J Educ Techno. 2022. 30:65–74.
14. Malin H, Ballard PJ, Damon W. Civic purpose: an integrated construct for understanding civic development in adolescence. Hum Dev. 2015;58(2):103–130. doi:10.1159/000381655
15. Kashdan TB, Mcknight PE. Origins of purpose in life: refining our understanding of a life well lived. Psihologijsk Psychol. 2009;18(2):303–316.
16. Hill PL, Burrow AL, Sumner R. Addressing important questions in the field of adolescent purpose. Child Dev Perspect. 2013;7(4):232–236. doi:10.1111/cdep.12048
17. Lan GR, Lee HY, Gai XS. Purpose in life: a psychological construct that indicates positive development. Adv Methods Pract Psychol Sci. 2017;25(12):2192–2202. doi:10.3724/SP.J.1042.2017.02192
18. Burrow AL, Hill PL. Purpose as a form of identity capital for positive youth adjustment. Dev Psychol. 2011;47(4):1196–1206. doi:10.1037/a0023818
19. Hill PL, Sumner R, Burrow AL. Understanding the pathways to purpose: examining personality and well-being correlates across adulthood. J Posit Psychol. 2014;9(3):227–234. doi:10.1080/17439760.2014.888584
20. Garcia-Alandete J, GALLEGO-PÉREZ JF, Esteban P. Purpose in life and hopelessness: an empirical study. Univ Psychol. 2009;8(2):447–454.
21. García-Alandete J, Gallego Hernández de Tejada B, Pérez Rodríguez S, et al. Meaning in life among adolescents: factorial invariance of the purpose in life test and buffering effect on the relation between emotional dysregulation and hopelessness. Clin Psychol Psychother. 2018;26(1):24–34. doi:10.1002/cpp.2327
22. Boreham ID, Schutte NS. The relationship between purpose in life and depression and anxiety: a meta analysis. J Clin Psychol. 2023;2023:23576.
23. Echeverria I, Peraire M, Penadés D. Purpose in life and character strengths as predictors of health sciences students’ psychopathology during the COVID-19 pandemic. Front Psychiatry. 2022;13. doi:10.3389/fpsyt.2022.932249
24. Damon W, Bronk KC. Taking ultimate responsibility. In: Gardner H, editor. Responsibility at Work: How Leading Professionals Act (or Don’t Act) Responsibly. San Francisco: Jossey-Bass; 2007:21–42.
25. Wang H, Gai XS, Lee SL. Development and validation of the youth purpose orientation scale among Chinese sample. Psychol Res Behav Manag. 2022;15:3485–3496. doi:10.2147/PRBM.S377052
26. Bronk KC, Finch WH. Adolescent characteristics by type of long-term aim in life. Appl Dev Sci. 2010;14(1):35–44. doi:10.1080/10888690903510331
27. Hill PL, Burrow AL, Brandenberger JW, et al. Collegiate purpose orientations and well-being in early and middle adulthood. J Appl Dev Psychol. 2010;31(2):173–179. doi:10.1016/j.appdev.2009.12.001
28. Mariano JM, Vaillant GE. Youth purpose among the ‘greatest generation’. J Posit Psychol. 2012;7(4):281–293. doi:10.1080/17439760.2012.686624
29. Salmela-Aro K, Nurmi J-E. Goal contents, well-being, and life context during transition to university: a longitudinal study. International Journal of Behavioral Development. 1997;20(3):471–491. doi:10.1080/016502597385234
30. Cross S, Markus H. Possible selves across the life span. Hum Dev. 1991;34(250):230–255. doi:10.1159/000277058
31. Prager E, Bar-Tur L, Abramowici I. The sources of meaning profile (somp) with aged subjects exhibiting depressive symptomatology. Clin Gerontol. 1997;17(3):25–39. doi:10.1300/J018v17n03_04
32. Rosenberg M. Society and the Adolescent Self-Image. Princeton, NJ: Princeton University Press; 1965.
33. American Psychiatric Association. DSM-5 Diagnostic and Statistical Manual of Mental Disorders.
34. Sowislo JF, Orth U. Does low self-esteem predict depression and anxiety? A meta-analysis of longitudinal studies. Psychol Bull. 2013;139(1):213–240. doi:10.1037/a0028931
35. Diener E, Fujita F, Tay L, et al. Purpose, mood, and pleasure in predicting satisfaction judgments. Soc Indic Res. 2012;105(3):333–341. doi:10.1007/s11205-011-9787-8
36. Paradise AW, Kernis MH. Self-esteem and psychological well-being: implications of fragile self-esteem. J Soc Clin Psychol. 2002;21(4):345–361. doi:10.1521/jscp.21.4.345.22598
37. Sharma G, De Alba E. Sense of purpose among female students belonging to minority ethnic and Buddhist backgrounds. J Coll Charact. 2018;19(2):137–151. doi:10.1080/2194587X.2018.1445644
38. Sharma G, Yukhymenko-Lescroart M, Sanchez T. Examining the role of life purpose in high school students’ self-esteem through structural equation modelling. Heliyon. 2023;9(9):e19614. doi:10.1016/j.heliyon.2023.e19614
39. Cronbach LJ. Coefficient alpha and the internal structure of tests. Psychometrika. 1951;16(3):3):297–334. doi:10.1007/BF02310555
40. Yan Y, Xie XC, Gai XS, et al. Assessment results of the Rosenberg Self-Esteem (RSSE) in middle school and college students in China. Chin Mental Health J. 2021;35(10):863–868.
41. Podsakoff PM, MacKenzie SB, Lee JY, Podsakoff NP. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol. 2003;88(5):879–903. doi:10.1037/0021-9010.88.5.879
42. Mascaro N, Rosen DH. Existential meaning’s role in the enhancement of hope and prevention of depressive symptoms. J Pers. 2005;73(4):985–1013. doi:10.1111/j.1467-6494.2005.00336.x
43. Chen H, Cheng C. Developmental trajectory of purpose identification during adolescence: links to life satisfaction and depressive symptoms. J Adolesc. 2020;80:10–18. doi:10.1016/j.adolescence.2020.01.013
44. Jin SH, Zheng JJ, Xin ZY. The structure and characteristics of contemporary Chinese values: the structure and characteristics of contemporary Chinese values. Acta Psychol. 2009;41(10):1000–1014. doi:10.3724/SP.J.1041.2009.01000
45. Steger MF, Shim Y, Rush BR, et al. The mind’s eye: a photographic method for understanding meaning in people’s lives. J Posit Psychol. 2013;8(6):530–542. doi:10.1080/17439760.2013.830760
46. Lambert NM, Stillman TF, Hicks JA, et al. To belong is to matter: sense of belonging enhances meaning in life. Pers Soc Psychol Bull. 2013;39(11):1418–1427. doi:10.1177/0146167213499186
47. Lambert NM, Stillman TF, Baumeister RF, et al. Family as a salient source of meaning in young adulthood. J Posit Psychol. 2010;5(5):367–376. doi:10.1080/17439760.2010.516616
48. Fei XT. From the Soil: The Foundations of Chinese Society. Berkeley, CA: University of California Press; 1992.
49. Schaefer SM, Morozink Boylan J, van Reekum CM, et al. Purpose in life predicts better emotional recovery from negative stimuli. PLoS One. 2013;8(11):e80329. doi:10.1371/journal.pone.0080329
50. Kim J, Pai M. Volunteering and trajectories of depression. J Aging Health. 2009;22(1):84–105. doi:10.1177/0898264309351310
51. Sarid O, Melzer I, Kurz I, et al. The effect of helping behavior and physical activity on mood states and depressive symptoms of elderly people. Clin Gerontol. 2010;33(4):270–282. doi:10.1080/07317115.2010.502105
52. Yuen M, Lee QA, Kam J, et al. Purpose in life: a brief review of the literature and its implications for school guidance Programs. J Psychol Couns Sch. 2015;27(1):55–69. doi:10.1017/jgc.2015.18
53. Robatmili S, Sohrabi F, Shahrak MA, et al. The effect of group logotherapy on meaning in life and depression levels of Iranian students. Int J Adv Couns. 2014;37(1):54–62. doi:10.1007/s10447-014-9225-0
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.