Back to Journals » Infection and Drug Resistance » Volume 19
Pulmonary Abscess, Endophthalmitis, and Lumbar Spine Infection Attributable to Invasive Klebsiella pneumoniae Liver Abscess Syndrome: A Case Report
Received 30 September 2025
Accepted for publication 2 February 2026
Published 27 March 2026 Volume 2026:19 569282
DOI https://doi.org/10.2147/IDR.S569282
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hemant Joshi
Fengjian Li, Xueyan Chen
Department of Clinical Laboratory Medicine, The People’s Hospital of Longhua, Shenzhen, Guangdong, People’s Republic of China
Correspondence: Xueyan Chen, Department of Clinical Laboratory Medicine, The People’s Hospital of Longhua, Jianshe Road No. 38, Longhua District, Shenzhen, Guangdong, 518109, People’s Republic of China, Email [email protected]
Background: Invasive Klebsiella pneumoniae Liver Abscess Syndrome (IKLAS) represents a serious multisite infection primarily triggered by a hypervirulent strain of Klebsiella pneumoniae. Among Asian patients with diabetes, these bacteria are relatively prevalent and have the potential to cause organ abscesses or sepsis. When patients present with multiple concurrent infections, their treatment becomes significantly more complex, necessitating a comprehensive diagnostic and therapeutic strategy. Instances of complex and severe infection cases are infrequently reported. Early detection of infections, selection of appropriate antibiotics, and proactive management of diabetes and related complications are critical determinants of patient prognosis.
Case Presentation: A 52-year-old Chinese man with a history of type 2 diabetes mellitus arrived at the emergency department with fever and chills, and he was subsequently diagnosed with a pyogenic liver abscess accompanied by a pulmonary infection, exhibiting clinical signs of sepsis. The patient received intravenous administrations of vancomycin and piperacillin-tazobactam for anti-infection and subcutaneous insulin for managing hyperglycemia. Ultrasound imaging was employed to guide a percutaneous procedure for liver puncture and drainage. During treatment, he developed invasive Klebsiella pneumoniae liver abscess syndrome, complicated with osteomyelitis, lung abscesses, and endophthalmitis. He achieved complete recovery following a two-month treatment regimen that included ultrasound-guided percutaneous transhepatic drainage, vitrectomy, and anti-infective therapy.
Conclusion: This case suggests that clinicians should consider the possibility of invasive liver abscess syndrome caused by hypervirulent Klebsiella pneumoniae when treating diabetic patients who present with fever in the emergency setting. Targeted intravenous antibiotic therapy, glycemic control, and percutaneous abscess drainage play an essential role in managing invasive Klebsiella pneumoniae liver abscess syndrome.
Keywords: invasive Klebsiella pneumoniae liver abscess syndrome, lung abscesses, osteomyelitis, endophthalmitis, antibiotic therapy
Introduction
Liver abscesses, defined as localized accumulations of pus within the liver, constitute a common intrahepatic infection typically caused by bacteria, parasites, or fungi. Liver abscesses are generally classified into two types: pyogenic liver abscesses (PLAs) and amebic liver abscesses. Klebsiella pneumoniae (K. pneumoniae), Escherichia coli, and Staphylococcus aureus are commonly identified as the primary pathogens implicated in the development of PLA.1 Currently, two predominant pathogenic variants of KP have been identified: the classical strain and the hypervirulent strain. Invasive Klebsiella pneumoniae liver abscess syndrome (IKLAS) refers to a clinical condition in which a hypervirulent K. pneumoniae-induced pyogenic liver abscess (PLA) is accompanied by secondary complications outside the liver, including endophthalmitis, meningitis, necrotizing fasciitis, and spondylodiscitis, which is a rapidly progressive, life-threatening condition associated with a high mortality rate.2 The incidence of IKLAS is significantly higher in Asian countries compared to Western nations, and in 1986, the first report emerged from Taiwan documenting hypervirulent K. pneumoniae as the causative agent of a diverse array of infections.2,3 The prevalence of diabetes in China has been steadily increasing over the years,4 and several studies have indicated that diabetes constitutes a risk factor for the development of IKLAS.5 We have observed that the rising prevalence of hypervirulent K. pneumoniae, particularly in recent years, has substantially complicated the treatment protocols for this disease. Herein, we present a rare case of IKLAS caused by hypervirulent K. pneumoniae that resulted in osteomyelitis, lung abscesses, and endophthalmitis. The patient underwent an extended course of antibiotic therapy in combination with surgical intervention and glycemic control, ultimately achieving recovery.
Case Representation
A 52-year-old Chinese male with type 2 diabetes mellitus presented with a fever of unknown origin lasting nine days, accompanied by chills, cough, and expectoration, and was subsequently referred to our emergency department (ED) due to unconsciousness on April 23, 2024. He also experienced eye discomfort without any accompanying changes in his vision. His vital signs were stable, except for an elevated temperature (38.1°C). He had been diagnosed with type 2 diabetes mellitus (T2DM) five years prior and was consistently managed with metformin and insulin therapy. In the ED, a blood culture specimen was obtained, and the laboratory test findings are summarized in Table 1. The initial assessment identified septic shock in conjunction with suboptimal glycemic control associated with diabetes mellitus.
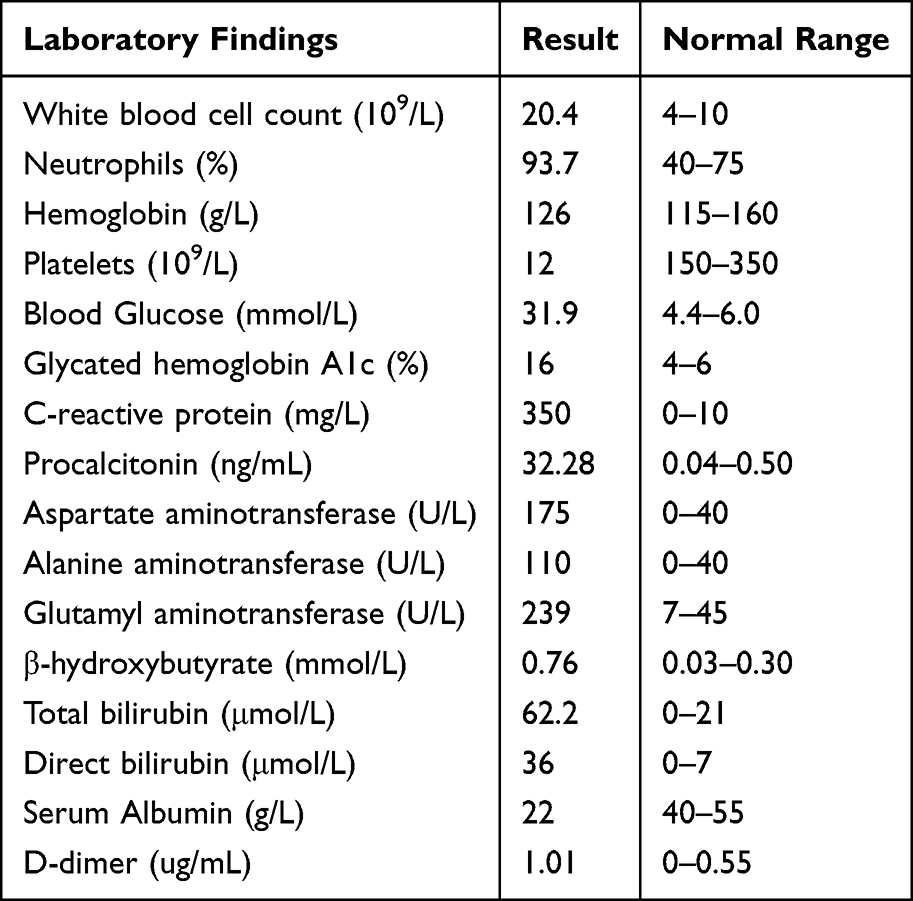 |
Table 1 Laboratory Findings of the Patient |
The imaging evaluation revealed no detectable abnormalities within the brain. A plain CT scan of the chest and abdomen revealed multiple nodules and cavitations in both lungs, suggesting primarily infectious lesions and hematogenous lung abscesses (Figure 1A). Additionally, low-density, space-occupying lesions were observed in segments 4/8 and 5/8 of the liver, measuring 75 mm × 60 mm and 45 mm × 35 mm, respectively, raising consideration for a liver abscess (Figure 1B). The patient received intravenous vancomycin (0.5 g every 12 hours for 4 days) and piperacillin-tazobactam (4.5 g every 8 hours for 4 days), along with albumin and platelet infusions to help curb disease progression, and subcutaneous insulin to manage hyperglycemia. Five days after initiating anti-infection and supportive treatment, the patient’s platelet count increased to 110×109/L, thereby facilitating an ultrasound-guided percutaneous liver puncture and catheter drainage procedure for the liver abscess. K. pneumoniae was identified using the microbial culture (Figure 2A and B), which was also isolated from blood and throat swab samples. The combination of hyperglycemia (31.9 mmol/L) and a liver abscess diameter of ≤5.8 cm is strongly associated with a high probability of IKLAS.4 Polymerase Chain Reaction (PCR) confirmed the K1 serotype (magA-positive). The virulence gene iroB in KP was detected using multiplex-targeted amplification combined with high-throughput sequencing, resulting in 40,857 reads. Additional virulence genes associated with hvKP, such as peg-344 with 6475 reads, iucA with 14,051 reads, rmpA with 10,152 reads, and rmpA2 with 9376 reads, were detected. Drug susceptibility testing confirmed fully susceptible K. pneumoniae (Table 2). The treatment regimen was switched to Meropenem (0.5 g q8h, i.v. D for 14 days) based on Antimicrobial Susceptibility Testing (AST) Report, showing a notable reduction in inflammatory markers, and he gradually regained full consciousness. Given that the patient’s temperature (37.5°C) remained elevated and the decrease in inflammatory markers was below expectations, meropenem was replaced with piperacillin-tazobactam (4.5 g q8h, i.v. D for 10 days), as recommended by the clinical pharmacist.
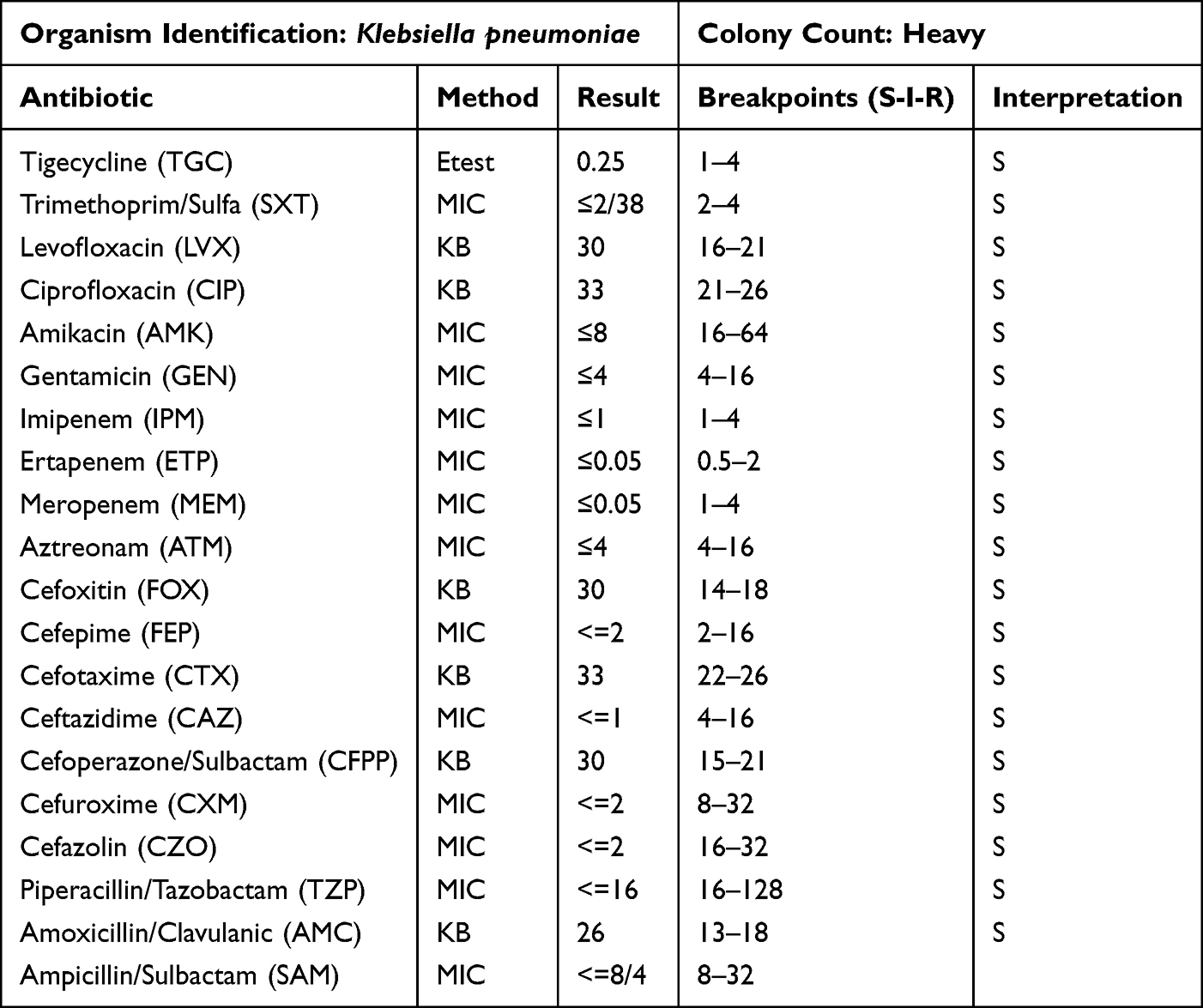 |
Table 2 Antimicrobial Susceptibility Test Report |
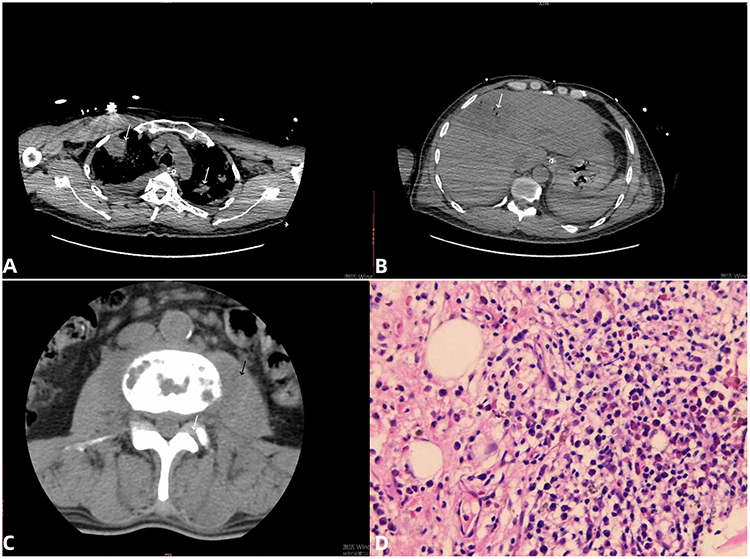 |
Figure 1 (A) CT scan of the chest revealed multiple nodules and cavitations in both lungs. (white arrows). (B) Low-density, space-occupying lesions were observed in segments 4/8 and 5/8 of the liver (white arrows). (C) The vertebral bodies exhibit bone destruction (white arrows) adjacent to an enlarged psoas muscle (black arrows). (D) The bone biopsy findings were consistent with a diagnosis of chronic osteomyelitis. (Hematoxylin and eosin staining× 400). |
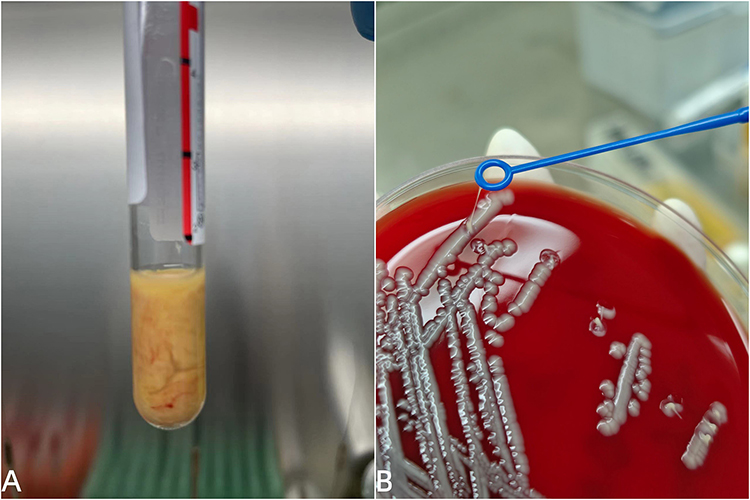 |
Figure 2 (A) Pus drained by ultrasound-guided percutaneous liver puncture. (B) Klebsiella pneumoniae isolates from pus were cultured on sheep blood agar, and the String test was positive, forming a line at least 5 mm in length. |
Despite receiving appropriate and targeted antibiotic treatment, He complained of progressively worsening ocular discomfort and developed blurred vision in both eyes on May 20, 2024. He was diagnosed with bilateral endophthalmitis, an obstruction of the left lacrimal system, and secondary glaucoma in the left eye, recommending surgical intervention. To achieve optimal outcomes following ocular vitrectomy, the anti-infection treatment protocol was modified to incorporate ceftazidime-avibactam sodium (2.5 g q8h, i.v. D for 10 days) and levofloxacin (0.1g qd, po. D for 10 days), administered both preoperatively and postoperatively, in combination with levofloxacin eye drops. He exhibited bilateral blurred vision accompanied by reduced pain, demonstrating sensitivity to light reflection in the right eye and a delayed response in the left eye, after surgical intervention. His body temperature consistently remained within the normal range for 5 consecutive days, which prompted his transfer to the Infectious Diseases Department on May 29, 2024.
Owing to lower back pain and extensive edema in the subcutaneous tissues of the waist region, he experienced substantial limitations in ambulation in the Infectious Diseases Department. A lumbar spine CT revealed abnormal signal changes in the L3 and L4 vertebral bodies as well as in the paravertebral soft tissue, with involvement of the L3/4 intervertebral disc, suggestive of tuberculosis on June 5, 2024 (Figure 1C). To identify the cause of infection, the patient underwent a percutaneous biopsy of the bone lesions in the lumbar vertebral body, performed in collaboration with the Department of Orthopedics. Analysis of the biopsy tissue using next-generation metagenomic sequencing confirmed KP infection with 10 reads. The pathological examination of biopsies from vertebral lesions revealed chronic osteomyelitis (Figure 1D). The patient presented with impaired immune function and developed multiorgan infection, and the identification of the KP-associated virulence gene iroB supported a diagnosis of IKLAS. The patient did not exhibit indications for surgery, so the conservative anti-infection therapy was maintained. His antimicrobial regimen was subsequently modified to incorporate ceftazidime-avibactam sodium (4.5 g q8h, i.v. D) and levofloxacin (0.5 g qd, i.v.D) on June 16, 2024. Following the diagnostic and treatment procedures described, the patient’s inflammation markers decreased, and multiple blood cultures returned negative for bacteria. Upon re-examination of the chest, abdomen, and lumbar spine CT scans, a notable improvement in the lesions was observed compared to previous studies, leading to the patient’s discharge on July 6, 2024. He was advised to continue oral levofloxacin for ongoing anti-infective therapy. During the one-year follow-up period, he achieved complete recovery, with no evidence of recurrence noted. Figure 3 illustrates the treatment procedure.
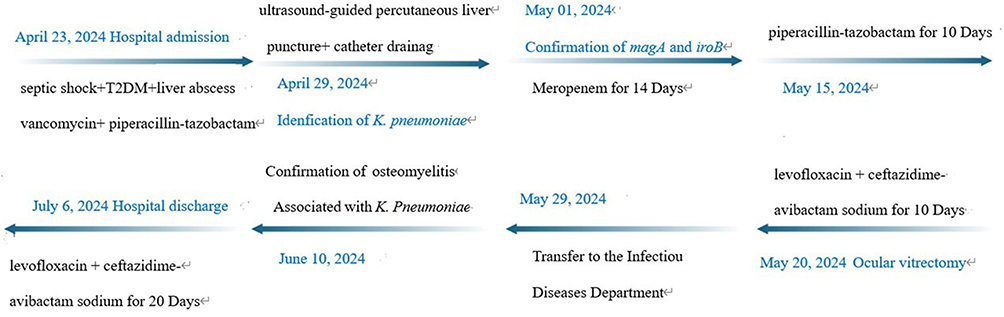 |
Figure 3 Patient Treatment Timeline. |
Discussion
We successfully managed a case of IKLAS attributed to K. pneumoniae harboring the virulence gene iroB, secondary to inadequate glycemic control. Polymerase chain reaction (PCR) detection of the magA gene confirmed that the strain belonged to the K1 serotype. In K. pneumoniae, a high level of virulence is closely linked to the presence of K1/K2 serotypes, a hypermucoviscosity phenotype, and the expression of the magA gene.6 For instance, the K1/K2 serotypes and magA gene expression do not possess the capsular sugar residues that macrophages typically recognize;7 hypermucoviscosity enhances the organism’s resistance to serum killing initiated by the complement system.8 Consequently, some individuals with K. pneumoniae-induced PLA exhibit symptoms of IKLAS. In aged mice, the reduction in intestinal macrophages leads to lower levels of growth arrest-specific 6 (Gas6). As a result, K. pneumoniae can more easily penetrate the intestinal lining and later move into the liver, which could account for the increased incidence of K. pneumoniae infections in older subjects.9 This phenomenon has also been observed in our clinical practice.
There are instances when the route of infection for PLA is not well understood, leading to its classification as a cryptogenic infection. Data from China indicate that the primary cause of PLA has transitioned from biliary origins to a cryptogenic basis, while K. pneumoniae has now supplanted Escherichia coli as the chief bacterial culprit.10 In recent times, the incidence of IKLAS has been on the rise globally, particularly within the Asia–Pacific region, and was initially identified in Taiwan during the 1980s, where it is linked with considerable morbidity and mortality.2,3 IKLAS is most commonly associated with endophthalmitis, meningitis, and brain abscess, and other clinical manifestations may include psoas abscess, lung abscess, spondylodiscitis, and septic pulmonary emboli.11 IKLAS are typically characterized by a singular bacterial infection that is often accompanied by multiple extrahepatic sites of involvement, with the majority of patients lacking a previous history of biliary tract disease.12
The key surface antigens in Klebsiella spp. are the capsular polysaccharide (known as the K antigen) and lipopolysaccharide (which includes the O antigen), which play a critical role as virulence factors in K. pneumoniae.13 The hypervirulence observed in K. pneumoniae can be attributed to the presence of its chromosomes, large virulence plasmids, or a combination of both.14 To sustain metabolism and support growth in iron-deficient conditions, these bacteria produce siderophores that help them extract the essential nutrient.15 Hypermucoviscosity represents a key virulence element, and strains exhibiting this property tend to demonstrate increased tolerance toward peripheral blood mononuclear cells.16 Another notable characteristic of hypervirulent Klebsiella pneumoniae is its production of colibactin, which replicates more rapidly in malnourished hosts and demonstrates increased virulence.1 IKLAS often presents with ambiguous signs and symptoms and may mimic other conditions, which increases the risk of misdiagnosis. Individuals with weakened immune systems, such as those suffering from diabetes, cancer, liver or biliary diseases, and recipients of organ transplants, are particularly vulnerable to this condition. Literature has reported that individuals with diabetes experienced liver abscesses at a rate more than three times higher than that of healthy individuals.17 Hyperglycemia impairs essential immune functions, including phagocyte adhesion, neutrophil function, chemotaxis, phagocytosis, and bactericidal activity, which ultimately weakens the body’s ability to eliminate bacterial pathogens and heightens the severity of infections.18 Accordingly, diligent oversight and regulation of blood glucose levels might be essential in diabetic patients with IKPLA to potentially avert the onset of severe metastatic infections.4 Blood glucose levels serve as reliable risk factors for predicting IKLAS.
The patient in this case underwent a percutaneous liver puncture with drainage and commenced anti-infective treatment using vancomycin combined with piperacillin-tazobactam. Laboratory cultures from both blood and drainage fluid confirmed the presence of non-drug-resistant K. pneumoniae. During the course of anti-infection treatment, the patient developed a liver abscess caused by K. pneumoniae, along with involvement of other organs, ultimately leading to a diagnosis of IKLAS. To ensure diagnostic accuracy, we sent the abscess drainage fluid to a tertiary hospital for comprehensive analysis of virulence genes. Similar cases have been documented in the literature,1 and a key distinguishing factor is that the reported case was not tested for virulent genes. When patients with liver abscesses exhibit additional clinical symptoms, clinicians should suspect an infection with hypervirulent Klebsiella pneumoniae and perform imaging studies to identify any hidden infectious foci, thereby enabling a more targeted antibiotic treatment strategy. Management of PLA typically involves draining the abscess, either through percutaneous or open surgical methods, while promptly administering the appropriate antibiotics. Thanks to significant strides in interventional radiology and minimally invasive surgery, percutaneous drainage has gained widespread adoption and now serves as an effective means of controlling the source of liver abscesses. In this case, the patient benefited from prompt ultrasound-guided percutaneous drainage combined with extended antibiotic therapy. Moreover, rigorous regulation of blood glucose levels significantly contributed to enhanced recovery from the disease.
Conclusion
The patient experienced favorable outcomes from the administration of targeted intravenous broad-spectrum antibiotics, strict regulation of blood glucose levels using intensive insulin therapy, and timely percutaneous drainage of the abscess. Apart from blurred vision, the patient reported no additional symptoms and maintained independent self-care. In clinical settings, when patients with diabetes and liver abscesses exhibit additional clinical symptoms, clinicians should suspect an infection with hypervirulent Klebsiella pneumoniae and perform imaging studies to identify any hidden infectious foci, thereby enabling a more targeted antibiotic treatment strategy. This report aims to enhance clinician awareness regarding IKLAS. The management of IKLAS fundamentally relies on the use of targeted intravenous antibiotics combined with percutaneous abscess drainage.
Abbreviation
IKLAS, invasive Klebsiella pneumoniae liver abscess syndrome.
Ethical and Consent Statements
The patient has provided written consent for the disclosure of case details and any related images. Consequently, these details can be published without the need for institutional approval.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study did not receive any external funding.
Disclosure
The authors state that no conflicts of interest are associated with this study.
References
1. Gui YG, Shou ST, Jiang Y, Wang QL. Treatment of liver abscess caused by Klebsiella pneumoniae with multi-site infection: a case report. J Med Case Rep. 2025;19(1):428. doi:10.1186/s13256-025-05511-9
2. Siu LK, Yeh KM, Lin JC, Fung CP, Chang FY. Klebsiella pneumoniae liver abscess: a new invasive syndrome. Lancet Infect Dis. 2012;12(11):881–7. doi:10.1016/S1473-3099(12)70205-0
3. Liu YC, Cheng DL, Lin CL. Klebsiella pneumoniae liver abscess associated with septic endophthalmitis. Arch Intern Med. 1986;146(10):1913–1916. doi:10.1001/archinte.1986.00360220057011
4. Feng CY, Zhang LW, Liu T, Jiang SF, Li XM, Di J. Establishment and verification of invasion syndrome prediction model in patients with diabetes complicated with Klebsiella pneumoniae liver abscess. Zhonghua Yi Xue Za Zhi. 2024;104(12):956–962. doi:10.3760/cma.j.cn112137-20231019-00813
5. Yoon JH, Kim YJ, Jun YH, et al. Liver abscess due to Klebsiella pneumoniae: risk factors for metastatic infection. Scand J Infect Dis. 2014;46(1):
6. Yu WL, Ko WC, Cheng KC, et al. Association between rmpA and magA genes and clinical syndromes caused by Klebsiella pneumoniae in Taiwan. Clin Infect Dis. 2006;42(10):1351–1358. doi:10.1086/503420
7. Lin JC, Chang FY, Fung CP, et al. High prevalence of phagocytic-resistant capsular serotypes of Klebsiella pneumoniae in liver abscess. Microbes Infect. 2004;6(13):1191–1198. doi:10.1016/j.micinf.2004.06.003
8. Alvarez D, Merino S, Tomas JM, Benedí VJ, Albertí S. Capsular polysaccharide is a major complement resistance factor in lipopolysaccharide O side chain-deficient Klebsiella pneumoniae clinical isolates. Infect Immun. 2000;68(2):953–955. doi:10.1128/IAI.68.2.953-955.2000
9. Tsugawa H, Ohki T, Tsubaki S, et al. Gas6 ameliorates intestinal mucosal immunosenescence to prevent the translocation of a gut pathobiont, Klebsiella pneumoniae, to the liver. PLoS Pathog. 2023;19(6):e1011139. doi:10.1371/journal.ppat.1011139
10. Luo M, Yang XX, Tan B, et al. Distribution of common pathogens in patients with pyogenic liver abscess in China: a meta-analysis. Eur J Clin Microbiol Infect Dis. 2016;35(10):1557–1565. doi:10.1007/s10096-016-2712-y
11. Iwadare T, Kimura T, Sugiura A, et al. Pyogenic liver abscess associated with Klebsiella oxytoca: mimicking invasive liver abscess syndrome. Heliyon. 2023;9(11):e21537. doi:10.1016/j.heliyon.2023.e21537
12. Choby JE, Howard-Anderson J, Weiss DS. Hypervirulent Klebsiella pneumoniae clinical and molecular perspectives. J Intern Med. 2020;287(3):283–300. doi:10.1111/joim.13007
13. Russo TA, Olson R, Fang CT, et al. Identification of biomarkers for differentiation of hypervirulent Klebsiella pneumoniae from classical K. pneumoniae. J Clin Microbiol. 2018;56(9):e00776–18. doi:10.1128/JCM.00776-18
14. Kamau E, Allyn PR, Beaird OE, et al. Endogenous endophthalmitis caused by ST66-K2 hypervirulent Klebsiella pneumoniae, United States. Emerg Infect Dis. 2021;27(8):2215–2218. doi:10.3201/eid2708.210234
15. Page MGP. The role of Iron and siderophores in infection, and the development of siderophore antibiotics. Clin Infect Dis. 2019;69(Suppl 7):S529–37. doi:10.1093/cid/ciz825
16. Lee IR, Sng E, Lee KO, et al. Comparison of diabetic and non-diabetic human leukocytic responses to different capsule types of Klebsiella pneumoniae responsible for causing pyogenic liver abscess. Front Cell Infect Microbiol. 2017;7:401. doi:10.3389/fcimb.2017.00401
17. Liao WI, Sheu WH, Chang WC, Hsu CW, Chen YL, Tsai SH. An elevated gap between admission and A1C-derived average glucose levels is associated with adverse outcomes in diabetic patients with pyogenic liver abscess. PLoS One. 2013;8(5):e64476. doi:10.1371/journal.pone.0064476
18. Gu L, Wang Y, Wang H, Xu D. Analysis of clinical and microbiological characteristics of invasive Klebsiella pneumoniae liver abscess syndrome. BMC Infect Dis. 2025;25(1):626. doi:10.1186/s12879-025-10981-9
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.