Back to Journals » Patient Preference and Adherence » Volume 20
Public Perceptions of Ethical and Professional Practice in Jordanian Community Pharmacies: A Cross-Sectional Study
Authors Jarad OF, Hasan HE ![]() , Khabour OF
, Khabour OF ![]() , Alzoubi KH
, Alzoubi KH ![]() , Al-Delaimy WK
, Al-Delaimy WK
Received 3 November 2025
Accepted for publication 13 February 2026
Published 18 March 2026 Volume 2026:20 578660
DOI https://doi.org/10.2147/PPA.S578660
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Ramón Morillo-Verdugo
Ola F Jarad,1,* Hisham E Hasan,1,* Omar F Khabour,2 Karem H Alzoubi,3 Wael K Al-Delaimy4
1Department of Clinical Pharmacy, Faculty of Pharmacy, Jordan University of Science and Technology, Irbid, Jordan; 2Department of Medical Laboratory Sciences, Faculty of Applied Medical Sciences, Jordan University of Science and Technology, Irbid, Jordan; 3Department of Pharmaceutical Sciences, College of Pharmacy, QU Health, Qatar University, Doha, Qatar; 4Herbert Wertheim School of Public Health and Human Longevity Science, University of California, San Diego, La Jolla, CA, USA
*These authors contributed equally to this work
Correspondence: Omar F Khabour, Department of Medical Laboratory Sciences, Faculty of Applied Medical Sciences, Jordan University of Science and Technology, Petra Street, Irbid, 22110, Jordan, Tel +960790453765, Email [email protected]
Background: Ethical and professional pharmacy practice is fundamental to supporting patient safety and trust. Despite advances in Good Pharmacy Practice (GPP), evidence from developing systems indicates gaps in ethical performance. This study aimed to assess the ethical dimensions of community pharmacists’ practice in Jordan from the public’s perspective, focusing on counseling quality, privacy, autonomy, and fairness.
Methods: A cross-sectional survey was conducted among 710 community pharmacy clients across Jordan using a validated questionnaire measured five ethical domains and an attitude scale. Composite scores for patient satisfaction, ethical conduct, and pharmacist attitude were calculated. Descriptive statistics and logistic regression were used to identify demographic predictors.
Results: Participants were predominantly female (57.9%) and from central Jordan (69.6%). Mean domain scores were: history-taking (51.3 ± 34.3), counseling (60.3 ± 29.6), privacy (67.8 ± 26.1), autonomy (60.2 ± 36.6), and justice (86.5 ± 24.0). Counseling was strongest for medication use and timing but weakest for safety aspects—adverse effects (41.4%), storage (40.1%), and drug interactions (31.7%). Justice and professionalism received the highest perception scores, while privacy and autonomy received moderate ratings. Gender (female) and south region predicted higher satisfaction and ethical perception (p < 0.05).
Conclusion: Community pharmacists in Jordan were perceived as demonstrating strong fairness and professionalism, but gaps remain in safety-oriented counseling and privacy assurance. These findings highlight areas where communication practices, privacy infrastructure, and ethics-oriented training may warrant further attention. Strengthening these areas could contribute to supporting patient trust and the ethical quality of community pharmacy services.
Keywords: pharmaceutical ethics, community pharmacy, patient counselling, professional conduct, patient-centered care, Jordan
Introduction
Pharmaceutical care has evolved from a product-centered activity to a patient-centered professional practice that emphasizes responsibility for the outcomes of drug therapy and the ethical relationship between pharmacists and patients.1,2 The modern pharmacist is expected not only to ensure the correct supply of medicines but also to act as a therapeutic partner, providing counseling, monitoring adherence, and safeguarding patient welfare. This transformation, reflected in the Pharmacists’ Patient Care Process (PPCP) framework endorsed by the Joint Commission of Pharmacy Practitioners, integrates clinical competence, communication, and ethical accountability throughout the patient journey.3,4
Pharmacy ethics are traditionally grounded in the principles of autonomy, beneficence, non-maleficence, justice, and confidentiality.5,6 These principles define the pharmacist’s professional obligations to respect patient choice, act for their benefit, avoid harm, treat individuals fairly, and maintain privacy/confidentiality. Ethical excellence, however, extends beyond rule compliance—it requires recognizing each patient as a moral partner and enabling informed, trust-based decisions.7 Thus, the moral quality of pharmaceutical care is revealed not merely in adherence to codes, but in the pharmacist’s ability to communicate effectively, respect privacy, safeguard patient dignity, and engage patients in shared decision-making.
Globally, regulatory bodies such as the World Health Organization (WHO) and the International Pharmaceutical Federation (FIP) have embedded ethical performance within the concept of Good Pharmacy Practice (GPP), emphasizing the pharmacist’s duty to ensure safety, privacy, and counseling quality in every encounter.8 However, evidence suggests that community pharmacists, particularly in developing and transitional health systems, continue to face ethical and professional challenges. Studies from many countries report incomplete counseling, limited privacy, and conflicts between commercial pressures and professional integrity.9–11 These systemic factors need to reinforce ethical accountability and patient-centered practice within evolving pharmacy services.
In Jordan, community pharmacies represent the most accessible component of the health-care system, often serving as patients’ first and sometimes only point of contact. Pharmacists play a central role in medication supply, patient education, and health promotion. Yet, despite these responsibilities, prior studies have identified significant variability in counseling standards, privacy provisions, and ethical awareness.12 Many pharmacies lack dedicated counseling areas, documentation systems, or standardized consent procedures, raising concerns about compliance with both local and international ethical benchmarks. Moreover, as pharmacy practice modernizes through digital technologies, new ethical challenges—ranging from data protection and online professionalism to algorithmic transparency in AI-assisted dispensing—have been recognized in the literature, further broadening the scope of professional ethical responsibility.13
Educational frameworks in Jordan and across the region have begun to integrate ethics and professional communication into pharmacy curricula.14,15 However, translation of classroom ethics into real-world practice remains inconsistent. Practical competencies—such as obtaining medication histories, discussing adverse effects, and ensuring patient privacy—are often under-reinforced after graduation. Previous studies have emphasized that these clinical and ethical competencies are inseparable; ethical care must manifest through everyday communication, documentation, and follow-up.16–18
From a clinical perspective, effective ethical communication directly influences medication adherence and health outcomes. A recent review on ethical guides highlighted that adherence is contingent on understanding, trust, and the quality of pharmacist–patient dialogue.19 When counseling is superficial or privacy is compromised, ethical lapses translate into therapeutic inefficiency. Conversely, adherence and safety improve when pharmacists act as empathetic communicators and moral agents within the care process. GPP frameworks are internationally associated with promoting the rational use of medicines, enhancing service quality, and strengthening patient safety. However, the ethical and professional dimensions of these standards remain underexplored from the patient perspective, particularly in developing settings.
Despite these international advances, empirical evidence examining the ethical and professional dimensions of community pharmacy practice from the patient perspective remains limited in the Middle East.20–22 A comprehensive assessment encompassing counseling quality, privacy, autonomy, fairness, and overall professional conduct is therefore warranted. Accordingly, the present study aims to evaluate the ethical dimensions of pharmaceutical care provided by community pharmacists in Jordan, as perceived by the general public. It provides an evidence base to inform efforts aimed at strengthening ethical quality and patient trust in community pharmacy practice in Jordan, aligned with international frameworks.
Materials and Methods
Study Design and Setting
This was a cross-sectional study conducted between September 2024 and February 2025 to assess the ethical dimensions of pharmaceutical care provided by community pharmacists in Jordan. The study evaluated patients’ satisfaction, perception of ethical and professional practices, and attitudes toward pharmacists as healthcare providers. Data was collected through a structured self-administered questionnaire distributed online via Google Forms® and shared through social media platforms and community networks. The questionnaire was originally designed in English and then translated into Arabic to suit the local population. A forward–backward translation procedure was applied to ensure linguistic and conceptual equivalence.
Study Population and Sampling
The study targeted adults residing in Jordan who had visited a community pharmacy within the preceding two weeks. Inclusion criteria were age ≥18 years, permanent resident of Jordan, ability to provide informed consent, and a recent pharmacy interaction. Participants who were healthcare professionals but not acting as patients, or who provided incomplete responses, were excluded.
A sample size of 385 was calculated using the Raosoft® calculator with a 95% confidence level and 5% margin of error for the Jordanian adult population. To improve representativeness, the sample was increased by 45% to account for non-response and stratification. The final dataset included 710 valid responses, exceeding the minimum requirement. Participants represented all three main geographical regions: north, middle, and south of Jordan.
Because the survey was administered online, eligibility criteria were based on self-report and could not be independently verified. Participants were informed that the questionnaire should be completed only once, and no incentives were offered. In addition, to prevent duplicate responses, in the “Google Forms” setting, the choice “limit to 1 response” was selected. While the use of multiple distribution channels was intended to broaden participation, the sampling approach was non-probabilistic and convenience-based; therefore, potential selection bias should be considered when interpreting the findings.
Instrument Development
The questionnaire (Supplementary file, Appendix 1) was developed based on previous literature addressing ethical pharmacy practice and adapted to the Jordanian context.23–25 It comprised four sections: first; demographic and health-related information (age, gender, region of residence, education, monthly income, smoking status, chronic diseases, and employment in the medical field), as these factors may influence the frequency of pharmacy encounters, expectations of counseling, or sensitivity to privacy and medication safety communication, second; patient satisfaction and counseling quality (assessed through 14 items related to the pharmacist’s explanation of medication use, dosage, timing, meals, duration, adverse effects, drug interactions, and storage conditions), third; ethical and professional practices (measured using 9 items addressing privacy, autonomy, informed consent for substitution or near-expiry medicines, fairness, and respect in service), finally; attitude toward pharmacists (evaluated using six 5-point Likert-scale statements regarding trust, professionalism, and perceived need for pharmacist training). Monthly income categories were defined with reference to national household income and expenditure indicators reported by the Jordan Department of Statistics (dosweb.dos.gov.jo), supporting the cutoff of 650 JD that used to distinguish respondents earning above versus below the national average income level. The instrument was validated by an expert panel of three pharmacy academics and one biostatistician for content relevance and clarity. A pilot test (n = 25) confirmed comprehension and internal consistency. Cronbach’s alpha coefficients were satisfactory for the major domains (α = 0.81, 0.79, and 0.66), acknowledging the multidimensional nature of ethical practice constructs.
Scoring System
Responses were coded numerically for analysis. Binary items (Yes/No) were scored as 1 and 0, respectively, while domain scores (History, Counseling, Privacy, Autonomy, Justice) were calculated as the percentage of affirmative responses per participant, normalized to a 0–100 scale. Composite indices were then derived: patient satisfaction score (combining history and counseling items), ethical/professional score (combining privacy, autonomy, and justice items), and attitude score (average of six Likert-scale items, rescaled to 0–100). Higher scores indicated better perceived performance or attitudes.
Data Management and Statistical Analysis
Data was exported to IBM SPSS Statistics® (Version 30.0) for processing and analysis. Descriptive statistics (frequencies, means, and standard deviations) were used to summarize demographic characteristics and domain scores. Normality was assessed, and depending on the distribution, comparisons between categorical groups were performed using independent t-tests or one-way ANOVA tests. To identify predictors of high satisfaction, ethical perception, and attitude, composite scores were dichotomized at their mean values. For regression analyses, composite scores were dichotomized at the sample mean to represent relatively higher versus lower perceived performance within this study population. This approach was chosen to facilitate interpretation of associations, although it may reduce statistical efficiency; therefore, findings are interpreted as relative differences rather than absolute thresholds. Binary logistic regression was then performed to estimate odds ratios (ORs) and 95% confidence intervals (CIs). Independent variables included demographic characteristics, health status indicators, and professional background variables. Model diagnostics included assessment of multicollinearity using variance inflation factors (VIF), evaluation of model calibration with the Hosmer–Lemeshow goodness-of-fit test, and estimation of overall explanatory performance using Nagelkerke’s R2 and classification accuracy. No problems were detected, and all indicated an acceptable fit. Statistical significance was set at p < 0.05.
Ethical Considerations
The study protocol was reviewed and approved by the Institutional Review Board (IRB) of Jordan University of Science and Technology (JUST) before initiation under approval number (63/170/2024). All participants provided informed electronic consent prior to participation by selecting a checkbox confirming voluntary agreement and the right to withdraw at any time on the first page of the online questionnaire. Responses were collected anonymously, and no personal identifiers were retained. Data were stored securely and used solely for research purposes. The study adhered to the Declaration of Helsinki and local ethical standards by the King Abdullah University Hospital (KAUH) for research involving human participants.
Results
Demographic Characteristics
A total of 710 participants were included in the analysis. The mean age of respondents was 32.2 ± 11.4 years, ranging from 18 to 80 years. Females represented 57.9% (n = 411) of the sample, and 42.1% (n = 299) were males. Most participants resided in the Middle region of Jordan (69.6%), followed by the North (18.3%) and South (12.1%). Over half of the participants held a bachelor’s degree (53.9%), and 8.9% held a postgraduate degree. Approximately 74.8% reported monthly incomes below 650 JD, 38.6% were current smokers, and 32.3% worked in the medical field. Hypertension (14.5%) and diabetes mellitus (13.0%) were the most common chronic conditions. Table 1 provides the detailed descriptive statistics of respondents’ sociodemographic and clinical characteristics.
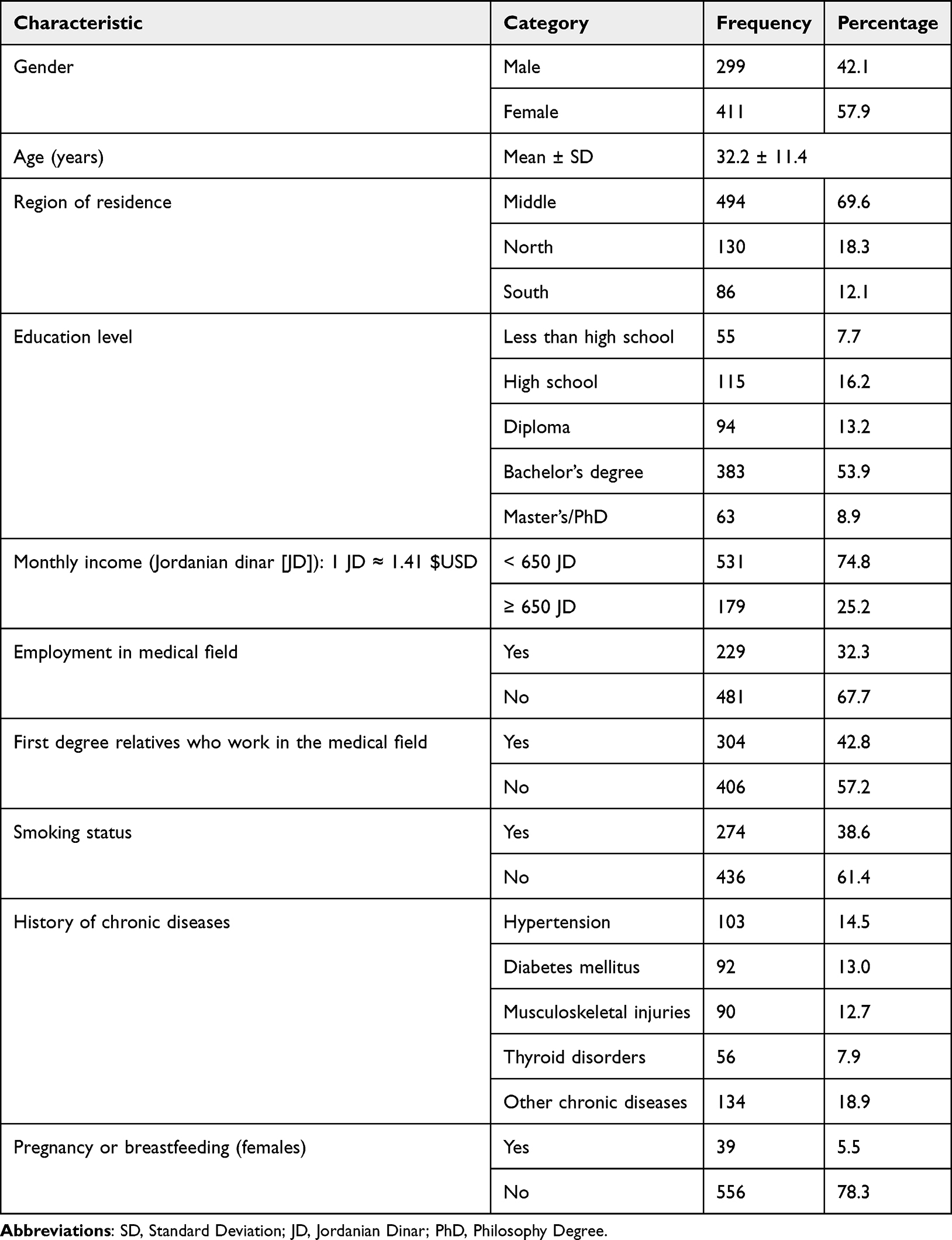 |
Table 1 Sociodemographic Characteristics of Participants (n = 710) |
Composite Outcome Scores
Table 2 shows the mean percentage scores for each ethical domain assessed in the survey instrument. Composite outcome scores are calculated from normalized domain means. The three normalized composite scores were moderate patient satisfaction (56.1 ± 27.1), positive ethical/professional considerations (75.9 ± 19.0), and positive pharmacist attitude (76.7 ± 12.1). These results indicate higher mean scores for ethical/professional considerations and pharmacist attitude than for patient satisfaction.
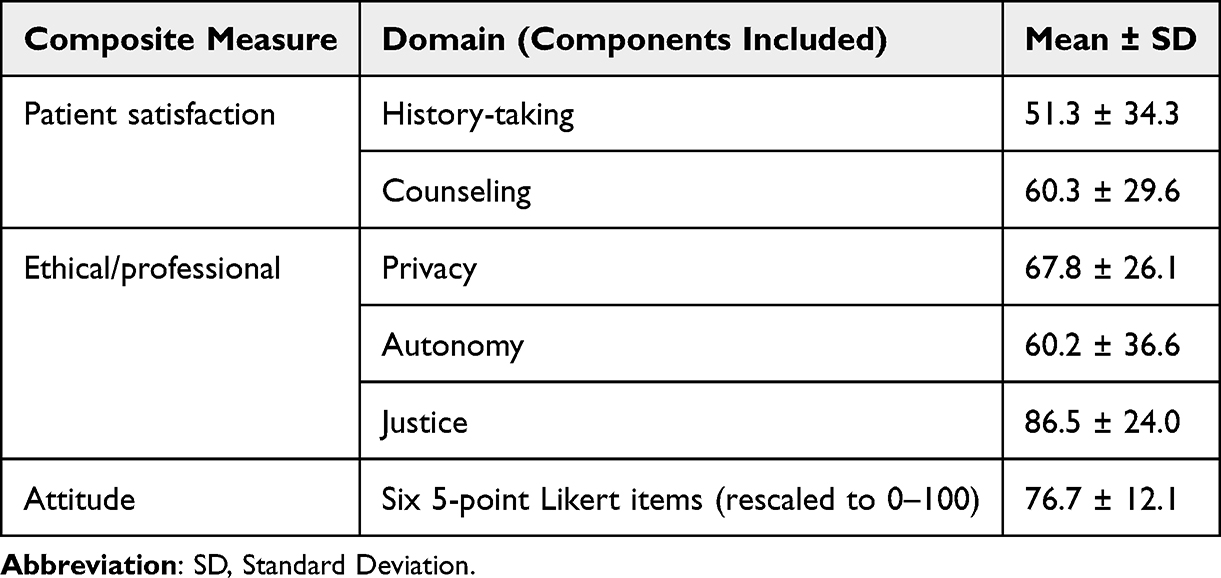 |
Table 2 Descriptive Statistics of Ethical Domain Scores (0–100 Scale) |
Figure 1 illustrates the proportion of participants who reported receiving counseling on specific aspects of care from community pharmacists, including (Supplementary file, Appendix 2) history-taking (Table A1), counseling content (Tables A2 and A3), privacy (Table A4), autonomy (Table A5), justice (Table A6), and perceptions of pharmacist attitude (Table A7). Response patterns varied across domains. The highest counseling frequency was reported for basic administration guidance (blue bars). In contrast, counseling deficiencies were most notable for safety-oriented information (red bars). Gender and geographic region significantly predicted satisfaction and ethical perception (p < 0.05). Detailed results are shown in Tables 3–5 and Table A8 (Supplementary file, Appendix 2). Model diagnostics confirmed a good fit for all logistic regressions, indicating adequate explanatory power and no multicollinearity among predictors. However, as this study employed a cross-sectional design, all associations reported represent correlations rather than causal relationships between patient characteristics and ethical perceptions.
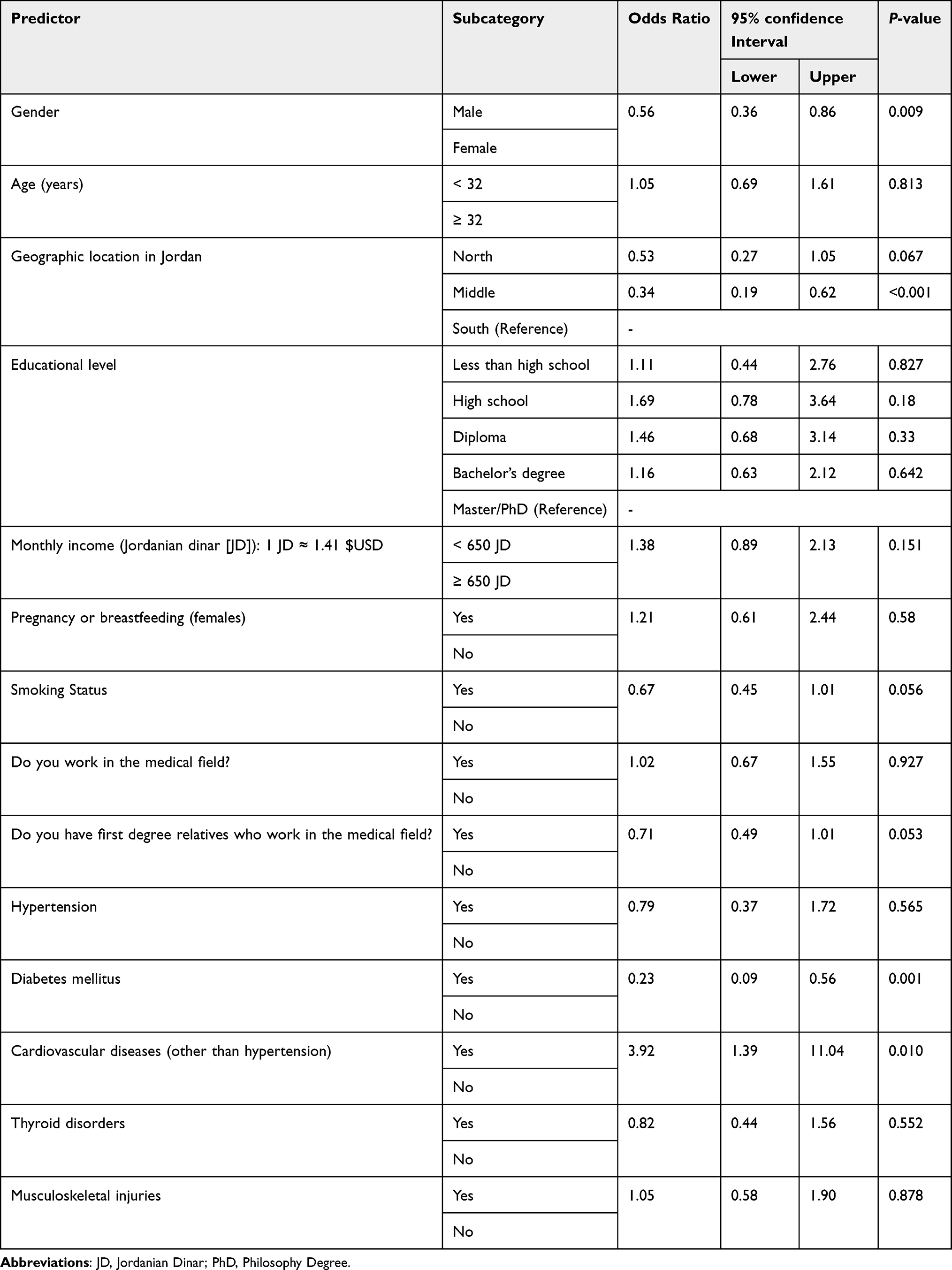 |
Table 3 Logistic Regression for Predictors of High Patient Satisfaction |
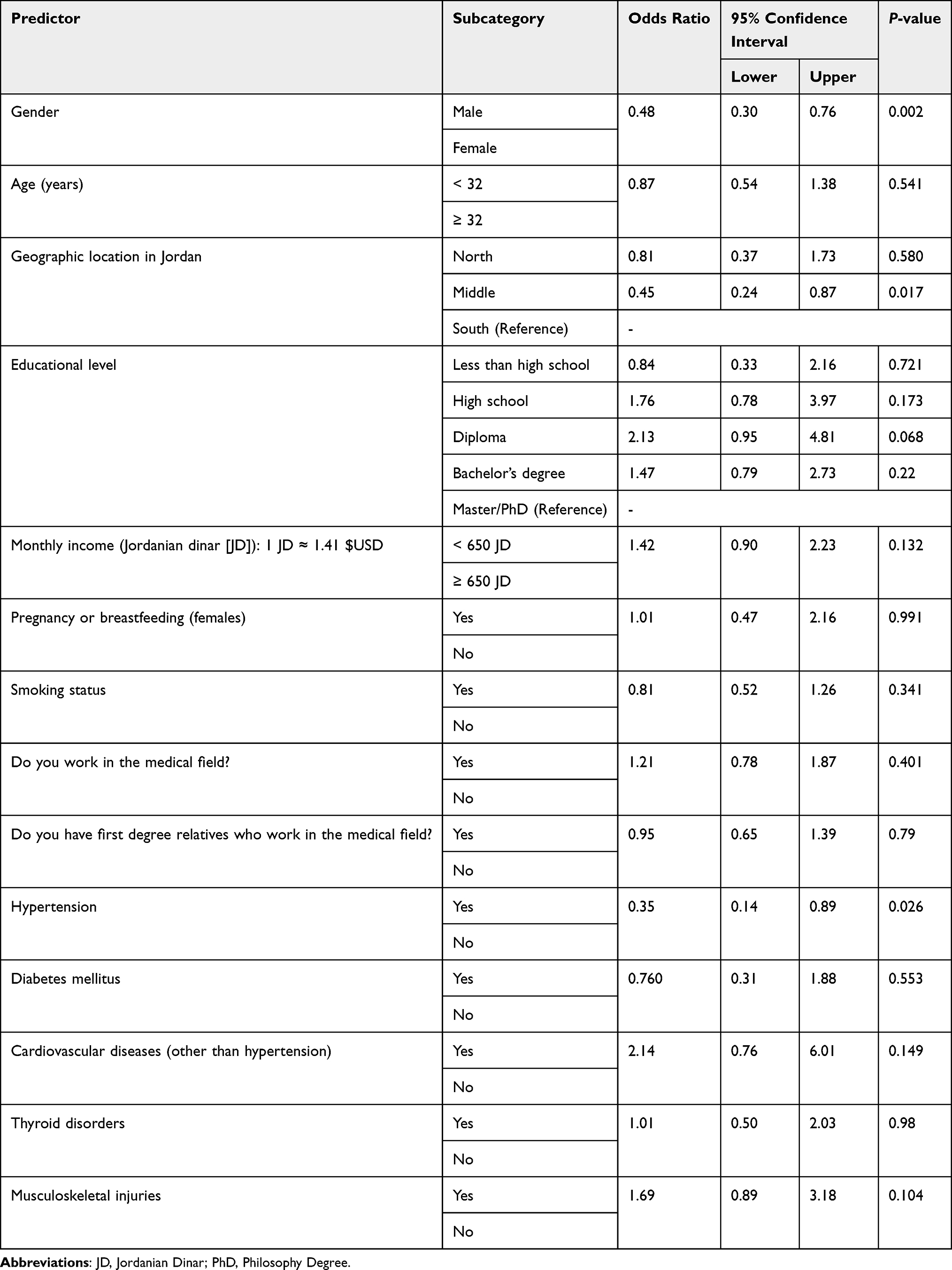 |
Table 4 Logistic Regression for Predictors of Positive Ethical/Professional Considerations |
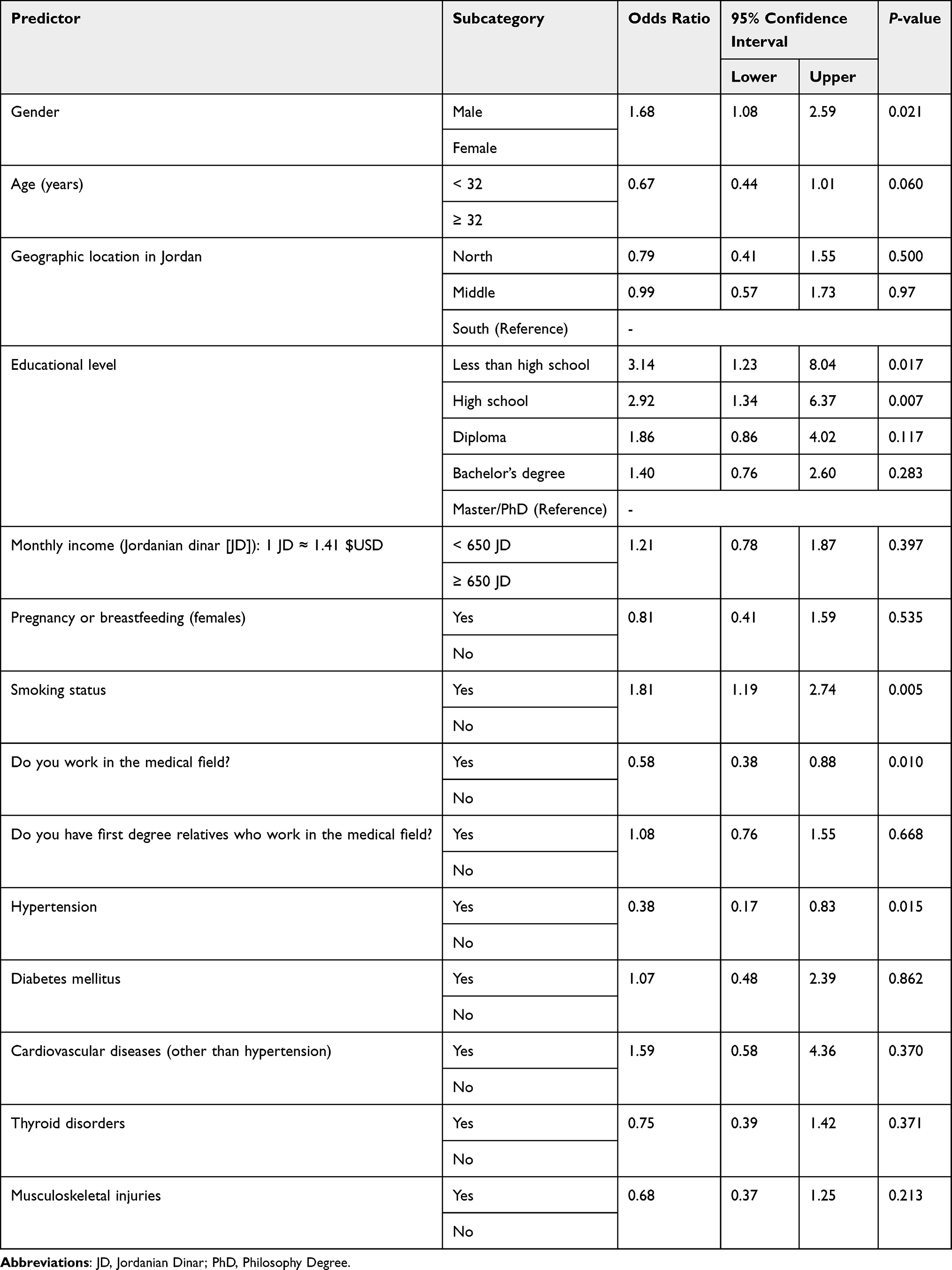 |
Table 5 Logistic Regression for Predictors of Positive Pharmacist Attitude |
 |
Figure 1 Counseling components reported by patients in community pharmacies. Red bars are items that scored less than 50%. Blue bars are items that scored more than 50%. |
Predictors of Patient Satisfaction
Table 3 summarizes the predictors of high patient satisfaction (scores ≥ mean). Binary logistic regression showed that gender and region as significant predictors. Male participants were less likely to report high satisfaction compared with females (OR = 0.56, 95% CI 0.36–0.86, p = 0.009). Respondents from the Middle region of Jordan demonstrated lower odds of satisfaction compared with those from the South (OR = 0.34, 95% CI 0.19–0.62, p < 0.001). No statistically significant associations were observed for age, education, income, smoking, or other chronic diseases, except for diabetes (OR = 0.23, 95% CI 0.09–0.56, p = 0.001) and cardiovascular disease (OR = 3.92, 95% CI 1.39–11.04, p = 0.010) after adjustment.
Predictors of Ethical and Professional Perception
Table 4 presents the predictors of high perception of pharmacists’ ethical and professional conduct (≥ mean score). Gender and regional remained statistically significant predictors. Male participants were less likely to report high ethical practice perception compared with females (OR = 0.48, 95% CI 0.30–0.76, p = 0.002). Similarly, participants residing in the Middle region were less likely to report high ethical practice perception than those in the South (OR = 0.45, 95% CI 0.24–0.87, p = 0.017). Age, education, income, and medical-field employment were not significant predictors. However, comorbid patients with hypertension were less likely to report high ethical practice perception (OR = 0.35, 95% CI 0.14–0.89, p = 0.026).
Predictors of Pharmacists’ Attitude Perception
For pharmacist attitude, a significant gender effect was observed: males were more likely to rate pharmacist attitudes positively (OR = 1.68, 95% CI 1.08–2.59, p = 0.021). Education level may also influenced perceptions—participants with less than 12th-grade education (OR = 3.14, 95% CI 1.23–8.04, p = 0.017) and those with 12th-grade education (OR = 2.92, 95% CI 1.34–6.37, p = 0.007) were more likely to report positive attitudes compared with university postgraduates. Smokers were more likely to rate pharmacist attitudes positively (OR = 1.81, 95% CI 1.19–2.74, p = 0.005), whereas participants employed in the medical field were less likely to do so (OR = 0.58, 95% CI 0.38–0.88, p = 0.010). Patients with hypertension were again less likely to report positive attitudes (OR = 0.38, 95% CI 0.17–0.83, p = 0.015). No other demographic or clinical variables were statistically significant. Table 5 summarizes the predictors of high pharmacist attitude perception.
Discussion
This study assessed the ethical dimensions of pharmaceutical care in Jordan as perceived by community pharmacy public patients. The findings demonstrate a generally positive evaluation of community pharmacists’ professionalism, fairness, and accessibility, but identify persistent deficiencies in counseling, documentation, and privacy assurance. The domains of justice and privacy achieved the highest mean scores, while counseling and history-taking were notably lower, reflecting a gap between ethical intent and clinical communication. Gender and regional disparities were statistically significant: female participants reported higher satisfaction, and southern regions perceived higher ethical and professional conduct than those in central or northern areas. These results correspond with previous regional investigations in Jordan and neighboring countries, which described similar counseling deficiencies, limited privacy measures, and uneven service standards across community pharmacy settings.9,10,12 Collectively, these findings suggest that perceived gaps in ethical and professional practice may be influenced not only by individual behaviors but also by systemic, educational, and infrastructural factors.
Community pharmacists in Jordan continue to serve as first-contact healthcare providers who must navigate complex ethical decisions despite limited diagnostic authority. As described in contemporary pharmacy ethics literature, the ethical pharmacist transcends the traditional “product-centered dispenser” role to become a clinical problem solver—capable of symptom assessment, evidence-based decision-making, and timely referral.7,26 Most patients present with undifferentiated symptoms rather than formal diagnoses; thus, ethical practice begins with empathetic communication and clinical reasoning that safeguard both autonomy and safety.
Pharmacy ethics are traditionally anchored in the principles of autonomy, beneficence, non-maleficence, justice, and confidentiality. The current findings indicate that participants perceived stronger performance in justice and fairness than in autonomy and beneficence, as reflected in limited counseling on adverse reactions, drug interactions, and storage instructions. This observation is consistent with earlier Jordanian reports describing similar counseling gaps in both over-the-counter and prescription settings.27,28 This pattern suggests greater emphasis on equitable service delivery than on in-depth patient-centered counseling, which may limit opportunities for informed decision-making and optimal medication use.
In the Jordanian sociocultural context, professional ethical expectations in healthcare are often shaped by broader moral and religious traditions that emphasize responsibility, dignity, fairness, trust, and protection from harm. Such enduring moral frameworks may influence how patients understand professional accountability and respectful ethical conduct in pharmacy practice. Within this context, the observed pattern—high ratings for fairness and professionalism alongside weaker perceptions of privacy and safety-related counseling—may reflect structural and practice-related constraints rather than differences in moral intent. Previous literature has emphasized that ethical care in pharmacy is closely linked to communication quality, where adequate explanation, patient engagement, and respect for confidentiality support autonomy, trust, and safe medication use.7,29 Limited counseling or insufficient privacy may therefore affect how patients experience ethical and professional care, highlighting the importance of strengthening communication practices within community pharmacy settings.
The relatively low score for privacy likely reflects structural and environmental barriers rather than moral indifference. Many Jordanian pharmacies lack designated private counseling spaces or confidentiality protocols, as similarly reported in previous studies.11,30 Time constraints and commercial pressures within community pharmacies may also contribute to this pattern. Privacy breaches violate the contextual dimension of clinical ethics, where shared moral responsibility depends on social settings and environmental design as much as personal virtue in practice.31 Therefore, improving the physical and organizational infrastructure for confidential counseling may thus be considered an ethical priority.
Islamic tradition strongly endorses scientific practice and patient care, which situates pharmacotherapy as a religiously sanctioned act of preserving life.32,33 Therefore, promoting ethical perception among Jordanian pharmacists can be interpreted as an act of stewardship—integrating humanitarian, religious, and clinical responsibilities. Within this broader moral discourse, pharmacist-led evidence-based symptom management and patient triage in community settings are legitimized.34 Similarly, ethical excellence is judged by intent and trust: dispensing without adequate counseling—particularly when driven by commercial motives—undermines both, whereas transparent communication fulfills them. Such perspectives do not replace contemporary biomedical ethics but may shape how professional duties are understood and valued locally. Integrating structured modules on Islamic medical fiqh within pharmacy curricula could therefore reinforce professional conscience alongside modern and relevant biomedical ethics rather than secular codes alone.35
Effective pharmacist–patient communication is not only a moral expectation but also a determinant of adherence and therapeutic success.36 Adherence is built on trust and understanding, with outcomes often influenced by ethical interaction. Deficits in counseling on adverse effects and storage conditions observed in this study may thus contribute to non-adherence and therapeutic failure, transforming ethical lapses into clinical risk. The Pharmacists’ Patient Care Process (PPCP) aligns closely with this study’s evaluated domains: history-taking (collect/assess), autonomy (plan/decision-sharing), counseling (implement), justice (follow-up fairness), and privacy (context).3,16,37 Deficiencies in any stage may interrupt this ethical continuum of care. Moreover, the absence of documentation—a key accountability mechanism—weakens both legal and moral responsibility. Ethical care, therefore, cannot be separated from clinical performance.
Gender, regional, and health-status differences further illustrate how personal experience may shape ethical perception and satisfaction. Female respondents’ higher satisfaction may have received more empathetic or communicative interactions, while rural or southern pharmacies— often resource-limited settings where patients may lack ready access to physicians with lower patient volumes—may allow for longer consultations and continuity of care. Patients with chronic conditions such as hypertension and diabetes reported lower satisfaction with counseling quality, which may be related to their higher frequency of pharmacy visits and greater familiarity with expected standards of care. Standardized or non-individualized counseling approaches may produce dissatisfaction or “service fatigue”, suggesting the need for tailored, ongoing communication strategies in chronic disease management.38 Ultimately, these findings suggest that structural workload and resource constraints mediate ethical performance more profoundly than demographic factors alone.
In this study, the perceived patient attitude toward pharmacists scored relatively high, aligning with previous Jordanian research reporting strong public trust in community pharmacists as accessible healthcare professionals.27,39 However, heterogeneity was evident in perceptions: male participants and those with lower educational levels tended to rate pharmacists’ attitudes more favorably, while respondents employed in medical fields expressed somewhat more critical views—perhaps reflecting higher expectations for clinical and ethical performance. Interestingly, hypertension was negatively associated with positive attitude perception, possibly pointing to the importance of tailored communication for chronic-disease populations, whose frequent pharmacy interactions may shape their long-term expectations of professionalism.
Beyond interpersonal conduct, ethical performance is also shaped by systemic and environmental contexts. The regional disparities observed in this study mirror reports from Saudi Arabia, the UAE, Lebanon, and Iran, where high urban workload, fragmented patient records, limited oversight, commercial pressure/profit, and inadequate staffing have been linked to ethical erosion.40–44 These findings suggest that ethical quality may be influenced by system-level factors: if work environments reward speed and sales over counseling time, opportunities for patient-centered ethical practice may become constrained rather than reflecting individual intent.30 In Jordan, many pharmacists work extended hours under space limitations, which can make individualized counseling more difficult. Achieving ethical competence may therefore benefit from supportive regulation and improved practice infrastructure. Without enforcing WHO/FIP GPP standards—such as mandatory private counseling areas and records documentation—ethical principles risk remaining aspirational.
To strengthen ethical pharmacy practice, ethics education may benefit from evolving beyond theoretical instruction toward applied competency. Current curricula in the MENA region often emphasize moral philosophy while neglecting clinical reasoning, communication, and documentation skills.13,45–49 Incorporating case-based learning and simulation exercises, as recommended by the American College of Clinical Pharmacy (ACCP), would enhance moral reasoning and relational competence.50
At the policy level, integrating ethical indicators into national accreditation and inspection frameworks could be considered. National regulatory and professional bodies (eg, Jordan Pharmacists Association, Ministry of Health, and Jordan Food and Drug Administration) may consider incorporating measures such as privacy audits, requiring private counseling/consultation areas as a licensing requirement, counseling checklists, random regulatory inspections, and informed-consent templates into GPP enforcement.
Continuous professional development focused on ethics, communication, and patient safety may also play an important role. Furthermore, as digital health expands, emerging ethical challenges—such as data privacy, algorithmic bias, and digital consent—will likely require attention through proactive governance and updated ethical codes.13 Embedding ethical evaluation within the WHO five-dimension adherence model—patient, therapy, condition, system, and socioeconomic factors—could link ethics to measurable outcomes.51 Such approaches may help transforming ethics from abstract idealism into a quality-assurance metric and reduces reliance on individual moral judgment alone.
Limitations and Future Directions
The present study’s strengths include its geographically diverse sample and a reliability-tested instrument aligned with international ethical standards. Nevertheless, limitations include its cross-sectional design and reliance on online self-reported perceptions, which may introduce recall, selection, or social desirability bias. The modest internal consistency of the privacy domain suggests the need for broader item development to capture both behavioral and infrastructural aspects of confidentiality. Future studies should adopt mixed-methods or multilevel designs that integrate patient and pharmacist perspectives. They should explicitly measure drug expiry management, commercial incentives, or prescribing behaviors to better understand the occurrence and ethical perceptions surrounding conflicts of interest and unsupervised practice within community pharmacies. Qualitative interviews could elucidate the underlying factors influencing ethical decision-making, including economic incentives, workload, or lack of facilities. Additionally, longitudinal studies could assess whether targeted ethical training and infrastructure changes translate into measurable improvements in patient outcomes and trust.
As with many online surveys, verification of eligibility criteria relied on self-report. Although it is not possible to independently confirm individual pharmacy encounters, community pharmacy use is widespread within the general population. The risk of duplicate submissions was considered low. The use of social media as a dissemination tool may introduce selection bias toward individuals who are more digitally engaged. Nevertheless, the sample may overrepresent individuals who are younger, more educated, or more health-aware, and this should be considered when interpreting the findings. Finally, the use of percentage-based composite scores and mean-based dichotomization may have reduced statistical efficiency and obscured within-group variability. Although this approach facilitated interpretation of relative differences in perceptions, future research could retain continuous composite measures or apply latent variable modeling to preserve information and explore perception gradients more precisely.
Conclusion
Ethical pharmacy practice in Jordan demonstrates strong foundations in fairness and professionalism, but appears to face challenges related to communication, privacy, and infrastructure. Counseling, privacy, satisfaction, and autonomy—core dimensions of ethical care—may benefit from further strengthening through potential improvements in training, workflow organization, and supportive policy frameworks. Gender, region, and chronic disease status were associated with differences in these perceptions, suggesting that patient experience is shaped by both individual and contextual factors. As global pharmacy practice continues to evolve toward more digital and patient-centered models, embedding ethics within the pharmaceutical care process, quality accreditation, and national training programs may help reinforce patient rights and professional accountability. Ultimately, ethical excellence in pharmacy is not compliance with rules but the consistent, compassionate exercise of professional judgment in every patient interaction—an act that unites scientific precision with moral and religious purpose.
AI Use in the Writing Process
During the preparation of this manuscript, the authors used ChatGPT-5.2 Plus to assist with language and grammar editing. The AI tool was not used to generate original scientific content, analyze data, or draw conclusions. All work and final decisions were performed by the authors, who take full responsibility for the integrity and accuracy of this work.
Data Sharing Statement
The data that was used and analyzed in this study will be available from the corresponding author.
Acknowledgement
The authors would like to thank Jordan University of Science and Technology for its support.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas, took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported by funds from Fogarty International Center (NIH: R25TW010026-01).
Disclosure
The authors declare that there is no conflict of interest.
References
1. Wang Y, Rao Y, Yin Y, Li Y, Lin Z, Zhang B. A bibliometric analysis of global trends in the research field of pharmaceutical care over the past 20 years. Front Public Health. 2022;10:980866. doi:10.3389/fpubh.2022.980866
2. Grabenweger R, Völz D, Weck C, Hau P, Paal P, Bumes E. Spirituality in professional patient-centered care for adults with primary brain tumors: an exploratory scoping review. J Religion Health. 2025;64(3):2165–15. doi:10.1007/s10943-024-02161-x
3. Olson AW, Vaidyanathan R, Stratton TP, Isetts BJ, Hillman LA, Schommer JC. Patient-centered care preferences & expectations in outpatient pharmacist practice: a three archetype heuristic. Res Soc Administrative Pharm. 2021;17(10):1820–1830. doi:10.1016/j.sapharm.2021.02.005
4. Roosan D, Wu Y, Tatla V, et al. Framework to enable pharmacist access to health care data using blockchain technology and artificial intelligence. J Am Pharm Assoc. 2022;62(4):1124–1132. doi:10.1016/j.japh.2022.02.018
5. Shea M. The ethics of clinical ethics. HEC forum. 2025;37(3):389–410. doi:10.1007/s10730-024-09544-3
6. Herzanych VM, Badyda AY, Buletsa NV, Svyshcho VY. Ethical and legal principles of biomedical research. Wiadomosci Lekarskie. 2025;78(4):943–948. doi:10.36740/WLek/203907
7. Seedhouse D. People-Centred Pharmacy: Ethical Challenges in Everyday Practice. John Wiley & Sons; 2025.
8. Kusynová Z, van den Ham HA, Leufkens HGM, Mantel-Teeuwisse AK. Longitudinal study of good pharmacy practice roles covered at the annual world pharmacy congresses 2003-2019. J Pharm Policy Pract. 2022;15(1):94. doi:10.1186/s40545-022-00482-4
9. Jairoun AA, Al-Hemyari SS, Shahwan M, et al. Top unresolved ethical challenges and dilemmas faced by community pharmacists in providing pharmaceutical care: drawing the line between ethical challenges and the quality of the pharmaceutical care. Res Soc Administrative Pharm. 2022;18(10):3711–3713. doi:10.1016/j.sapharm.2022.05.009
10. Esmalipour R, Larijani B, Mehrdad N, Ebadi A, Salari P. The ethical challenges in pharmacy practice in community pharmacies: a qualitative study. Saudi Pharm J. 2021;29(12):1441–1448. doi:10.1016/j.jsps.2021.11.003
11. Wernecke K, Nadolny S, Schildmann J, Schiek S, Bertsche T. Ethical conflicts in patient care situations of community pharmacists: a cross-sectional online survey. Int J Clin Pharm. 2024;46(6):1500–1513. doi:10.1007/s11096-024-01797-9
12. Akour A, Halloush S, Nusair MB, Barakat M, Abdulla F, Al Momani M. Gaps in pharmaceutical care for patients with mental health issues: a cross-sectional study. Int J Clin Pharm. 2022;44(4):904–913. doi:10.1007/s11096-022-01391-x
13. Hasan HE, Jaber D, Khabour OF, Alzoubi KH. Ethical considerations and concerns in the implementation of AI in pharmacy practice: a cross-sectional study. BMC Med Ethics. 2024;25(1):55. doi:10.1186/s12910-024-01062-8
14. Al-Delaimy WK, Alzoubi K, Khabour O, Jaber S. Research ethics education program in Jordan: achievements and challenges. J Empirical Res Human Res Ethics. 2025;15562646251331757. doi:10.1177/15562646251331757
15. Alnahar SA, AL-Rawashdeh AI, Makhzoomy AK, Bates I. What is needed to reform pharmacy education in Jordan: an exploratory study based on a multi-stakeholder perspective. Pharm Educ. 2022;22(4):63–72. doi:10.46542/pe.2022.224.6372
16. Pharmacy ACoC. Standards of practice for clinical pharmacists. J Am College Clin Pharm. 2023;6(10):1156–1159. doi:10.1002/jac5.1873
17. Hayakawa M, Kizaki H, Yanagisawa Y, et al. Development of a novel person-centered question prompt list to talk with your pharmacists in Japanese community pharmacies: focus group and Delphi method. J Pharm Health Care Sci. 2025;11(1):87. doi:10.1186/s40780-025-00494-7
18. Bloom TJ, Kebodeaux C, Munger M, Smith MD, Stutz M, Wagner J. A narrative review of pharmacy identity and the PharmD experiment. Am J Pharm Educ. 2025;89(2):101351. doi:10.1016/j.ajpe.2024.101351
19. Hasan HE. Review of ethics in pharmacy practice: a practical guide. In: Sullivan DM, C. Douglas C, Anderson JWC, editors. Ethics in Pharmacy Practice: A Practical Guide. Switzerland: Springer Nature; 2021. ISBN 978–3-030–72171-8.
20. Alghamdi KS, Petzold M, Ewis AA, Alsugoor MH, Saaban K, Hussain-Alkhateeb L. Public perspective toward extended community pharmacy services in sub-national Saudi Arabia: an online cross-sectional study. PLoS One. 2023;18(10):e0280095. doi:10.1371/journal.pone.0280095
21. Owusu YB, Abouelhassan R, Awaisu A. Evaluation of patient safety culture in community pharmacies in Qatar. Int J Clin Pract. 2021;75(5):e14055. doi:10.1111/ijcp.14055
22. Alsaleh FM, Abahussain EA, Altabaa HH, Al-Bazzaz MF, Almandil NB. Assessment of patient safety culture: a nationwide survey of community pharmacists in Kuwait. BMC Health Serv Res. 2018;18(1):884. doi:10.1186/s12913-018-3662-0
23. Fino LB, Basheti IA, Chaar BB. Exploring ethical pharmacy practice in Jordan. Sci Engineer Ethics. 2020;26(5):2809–2834. doi:10.1007/s11948-020-00231-3
24. Basheti IA, Mhaidat NM, Alqudah R, Nassar R, Othman B, Mukattash TL. Primary health care policy and vision for community pharmacy and pharmacists in Jordan. Pharm Pract. 2020;18(4):2184. doi:10.18549/PharmPract.2020.4.2184
25. Salari P, Namazi H, Abdollahi M, et al. Code of ethics for the national pharmaceutical system: codifying and compilation. J Res Med Sci. 2013;18(5):442–448.
26. Blenkinsopp A, Duerden M, Blenkinsopp J. Symptoms in the Pharmacy: A Guide to the Management of Common Illnesses and Disease Prevention. John Wiley & Sons; 2025.
27. Naser AY, Abu Sbeat BS. Satisfaction with community pharmacies services in Jordan: a cross-sectional study. Saudi Pharm J. 2022;30(11):1646–1651. doi:10.1016/j.jsps.2022.09.007
28. Al-Taani GM, Ayoub NM. Assessment of satisfaction of attendees of healthcare centers in Jordan with community pharmacy services of pharmacies they usually use. PLoS One. 2024;19(7):e0305991. doi:10.1371/journal.pone.0305991
29. Tindall WN, Beardsley RS, Kimberlin CL. Communication skills in pharmacy practice. A practical guide for students and practitioners. Am J Hospital Pharm. 1990;47(4):944–947.
30. Owens CT, Baergen R. Pharmacy practice in high-volume community settings: barriers and ethical responsibilities. Pharmacy. 2021;9(2). doi:10.3390/pharmacy9020074
31. Varkey B. Principles of clinical ethics and their application to practice. Med Princ Pract. 2021;30(1):17–28. doi:10.1159/000509119
32. Ghaly M. Islamic ethical perspectives on life-sustaining treatments. Eastern Mediterranean Health J. 2022;27(8):557–559. doi:10.26719/emhj.22.044
33. Aissaoui Y, Charif F, Bencharfa B, Bouchama A, Myatt I, Belhadj A. End-of-life care in Moroccan ICUs: ethical challenges, practices, and perspectives of intensivists. BMC Med Ethics. 2025;26(1):135. doi:10.1186/s12910-025-01271-9
34. Bulus Y, Abiola T. Evidence-based practice adherence and medical error reduction: an Islamic ethical perspective. Iman Med J. 2025;11(1).
35. Wijianto DW, Nurinnafi’a AMU, Luthfitah A, Firdaus MW, Suryandaru S, Febriani RE. Implementation of islamic ethics in pharmaceutical services: a literature review approach. Solo Int Collab Pub Soc Sci Human. 2023;1(03):181–188. doi:10.61455/sicopus.v1i03.64
36. Schoenthaler A, Knafl GJ, Fiscella K, Ogedegbe G. Addressing the social needs of hypertensive patients: the role of patient–provider communication as a predictor of medication adherence. Circ Cardiovasc Qual Outcomes. 2017;10(9):e003659. doi:10.1161/CIRCOUTCOMES.117.003659
37. DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey LM. Pharmacotherapy: a pathophysiologic approach. 2014.
38. Iroegbu C, Tuot DS, Lewis L, Matura LA. The influence of patient-provider communication on self-management among patients with chronic illness: a systematic mixed studies review. J Adv Nurs. 2025;81(4):1678–1699. doi:10.1111/jan.16492
39. Mukattash TL, Bazzi NH, Nuseir KQ, Jarab AS, Abu-Farha RK, Khdour MR. Pharmaceutical care in community pharmacies in Jordan: a public survey. Pharm Pract. 2018;16(2):1126. doi:10.18549/PharmPract.2018.02.1126
40. Easwaran V, Almeleebia TM, Mantargi MJS, et al. Patient safety culture in the southern region of Saudi Arabia: a survey among community pharmacies. Healthcare. 2023;11(10):1416.
41. Mohamed S, Palaian S, Alomar M, M M-A-A. A national survey on community pharmacists’ perception, practice and perceived barriers towards pharmaceutical care services in the United Arab Emirates. J Pharm Policy Pract. 2025;18(1):2523936. doi:10.1080/20523211.2025.2523936
42. Alameddine M, Bou-Karroum K, Hijazi MA. A national study on the resilience of community pharmacists in Lebanon: a cross-sectional survey. J Pharm Policy Pract. 2022;15(1):8. doi:10.1186/s40545-022-00406-2
43. Alameddine M, Bou-Karroum K, Kassas S, Hijazi MA. A profession in danger: stakeholders’ perspectives on supporting the pharmacy profession in Lebanon. PLoS One. 2020;15(11):e0242213. doi:10.1371/journal.pone.0242213
44. Iranmanesh M, Yazdi-Feyzabadi V, Mehrolhassani MH. The challenges of ethical behaviors for drug supply in pharmacies in Iran by a principle-based approach. BMC Med Ethics. 2020;21(1):84. doi:10.1186/s12910-020-00531-0
45. Nahar P, Unicomb L, Lucas PJ, et al. What contributes to inappropriate antibiotic dispensing among qualified and unqualified healthcare providers in Bangladesh? A qualitative study. BMC Health Serv Res. 2020;20(1):656. doi:10.1186/s12913-020-05512-y
46. Ahmed WS, Nebeker C. Assessment of research ethics education offerings of pharmacy master programs in an Arab nation relative to top programs worldwide: a qualitative content analysis. PLoS One. 2021;16(2):e0238755. doi:10.1371/journal.pone.0238755
47. Ahmed WS, Ahmed A, Alzoubi KH, Nebeker C. Perceptions of pharmacy graduate students toward research ethics education: a cross-sectional study from a developing country. Sci Engineer Ethics. 2022;28(6):47. doi:10.1007/s11948-022-00406-0
48. ElKhalifa D, Hussein O, Hamid A, Al-Ziftawi N, Al-Hashimi I, Ibrahim MIM. Curriculum, competency development, and assessment methods of MSc and PhD pharmacy programs: a scoping review. BMC Med Educ. 2024;24(1):989. doi:10.1186/s12909-024-05820-5
49. Alameri M, Al-Taani G, Alsous M, Shilbayeh S, Al Mazrouei N. Attitude and awareness toward general and professional ethics among pharmacists and pharmacy students: a cross-sectional study from Jordan. Healthcare. 2025;13(13). doi:10.3390/healthcare13131556
50. McBane S, Alavandi P, Allen S, et al. Overview of implementation and learning outcomes of simulation in pharmacy education. J Am College Clin Pharm. 2023;6(5):528–554. doi:10.1002/jac5.1784
51. Peh KQE, Kwan YH, Goh H, et al. An adaptable framework for factors contributing to medication adherence: results from a systematic review of 102 conceptual frameworks. J Gen Intern Med. 2021;36(9):2784–2795. doi:10.1007/s11606-021-06648-1
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.