Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 12
Public Perception and Viewpoints of Dental Radiograph Prescriptions and Dentists’ Safety Protection Practice
Authors Al Faleh W ![]() , Bin Mubayrik A
, Bin Mubayrik A ![]() , Al Dosary S
, Al Dosary S ![]() , Almthen H, Almatrafi R
, Almthen H, Almatrafi R
Received 16 September 2020
Accepted for publication 10 November 2020
Published 17 November 2020 Volume 2020:12 Pages 533—539
DOI https://doi.org/10.2147/CCIDE.S281851
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Wafa Al Faleh,1 Azizah Bin Mubayrik,1 Sarah Al Dosary,1 Haifa Almthen,2 Razan Almatrafi2
1Oral Medicine and Diagnostic Science Department, King Saud University, Riyadh, Saudi Arabia; 2College of Dentistry, King Saud University, Riyadh, Saudi Arabia
Correspondence: Azizah Bin Mubayrik
Oral Medicine and Diagnostic Science Department, College of Dentistry, King Saud University, 3680 - King Saud University Unit No. 3ar, Riyadh 12372− 7453, Kingdom of Saudi Arabia
Email [email protected]
Purpose: The exposure of patients to ionizing radiation used in dentistry comes with a subtle risk of a stochastic effect, but there is tremendous benefit obtained from radiographic investigation for diagnosis, management, and monitoring of the treatment offered.
Aim: The aim of this study was to assess the viewpoint of the population concerning the prescriptions and practices in dentistry associated with dental radiographs and the safe use of ionizing radiation in dental clinics.
Patients and Methods: Validated and pretested structured self-administered questionnaires with 11 items were used. An electronic version of the questionnaire was created using Google Forms and distributed online through social media outlets. A total of 437 patients completed the questionnaire which contains questions about their demographic data and their perception of the practice of dentistry regarding hazard from dental radiographs. The collected data were analyzed statistically.
Results: Up to 88.6% of the study participants underwent dental radiography for various dental treatments. A majority of them relied on the dentist for the type of requested radiograph, 40% of them reported that dentist never explained the hazards associated with radiography. More than half of the participants (55%) never or hardly ever asked about safety measures before undergoing radiography. Most of the participants approved of radiography and never refrained.
Conclusion: There is a spectrum of perceptions by the population. Continuous patient education is recommended to enhance awareness regarding this matter. Community perception assists in correcting wrong beliefs and ensuring improvement.
Keywords: knowledge, radiation hazards, dental radiography, perception, safety and protection
Introduction
Human beings are constantly exposed to numerous kinds of ionizing radiation, both natural background radiation and artificial radiation. X-rays are one of the big families of ionizing radiations that are frequently used for therapeutic and diagnostic purposes in both medicine and dentistry. In dentistry, radiography plays a central role in diagnosis, planning for or managing pathological conditions in the oral and maxillofacial region. Despite the small amount of all radiation that comes from dental radiography, there is still some risk.1
Patients during dental treatment are definitely exposed to diagnostic x-rays. Although the level of exposure is lower than that encountered in the medical field, the frequent exposure might carry an innate risk from radiation exposure that cannot be ignored. Biological hazards are classified based on probability of occurrence into deterministic and stochastic effects.2 Deterministic effects are those effects in which the severity of the response is proportional to the dose; once the threshold dose reached the effect will occur in the exposed individual. On the other hand, stochastic effects develop at random and depend on the law of chance. There is no threshold dose, and even a minute dose could cause these harmful biological effects. Cancer and genetic mutations are examples of a stochastic effect in which the probability of occurrence increases with the degree of exposure to ionizing radiation, but the exposures do not influence the severity of the effect.2 The importance of these effects has led the International Commission on Radiological Protection (ICRP) to introduce the “effective dose” concept as a measure of the risk from various radiographical evaluations.3
The effective dose was developed to measure the dose in relation to the possibility of induction of harm due to stochastic effects.4 The increased incidence of cancer in the head and neck area and health effects have been associated with the exposure to dental radiography as reported by some investigators.5–7
In an attempt to determine the effective dose and safety from various types of dental radiography in the head and neck, several studies have been conducted to measure the effective dose from different kinds of intraoral and extraoral radiography and concluded that the effective dose exceeds that which was estimated previously.7,8 However, there is no clear evidence of the threshold dose beyond which patients are definitely exposed to risk from dental radiography. Thus, a reduction of the effective dose is recommended.7–9 The guiding concept is known as the “as low as reasonably achievable” (ALARA) principle, in which each patient should receive the correct imaging exam, at the right time, with the appropriate radiation dose.8–10
Patients might have questions and concerns about safety during dental imaging procedures. Some of this information can be misleading, confusing, or incorrect; therefore, patients might refuse to undergo radiography based on the information they received via social media or the incorrect information they received from non-professional personnel. Moreover, patients might be unaware of the need for investigations by dentists to properly diagnose and treat the disease, which will affect the outcome of the dental treatment. Only a few studies in the reviewed English literature have investigated the perception and views of the general population.11 Thus, this study aimed to investigate the perception and viewpoints of a sample from the general population about the hazards of dental radiography and the practice of frequently requesting radiography in dentistry.
Materials and Methods
This cross-sectional study was designed and conducted to study the perception and viewpoints of the population regarding hazards associated with prescribed dental radiography and practice before any radiographic procedures. A structured self-administered questionnaire was designed based on the reviewed literature. The questionnaire was developed in Arabic in the form of multiple-choice questions on the hazards of ionizing radiation and protective measures used by dentists.
Before distributing the questionnaire through social media the institutional ethical committee approval was obtained, and a pilot study was first carried out on 40 participants with different characteristics to assess its clarity and feasibility. Participation in the study was voluntary.
The content of the questionnaire validated by oral radiologist before distribution to the population. The questionnaire consisted of three parts: the cover page with a consent form, request for cooperation, study explanation, importance, and instructions. The second part included socio-demographic questions such as age, gender, marital status, occupation, and level of education. It also had a part asking about the last dental visit, whether or not radiographs were taken or not and if the dental care center was private practice, governmental, or an academic institution. The third part was designed to assess the perception and attitude of participants toward the dental radiography prescription and x-ray using the Likert scale.
Statistical Analysis
The data were collected and analyzed, then summarized and presented in tables. All statistical analyses were performed with the Statistical Package for Social Sciences program (version 22). Descriptive statistics like frequency distributions were performed. T-tests were used to determine the association between previous radiographs and perception and attitude. The one-way ANOVA test and post hoc analysis were used to measure the relationship between level of education and perception with P-values ≤0.05 was considered statistically significant.
Results
A total of 437 completed questionnaires were received. More than half (58.1%) of the respondents were aged 40 or below. More than three-quarters (75.1%) of the sample had attained at least college level of education. More than half of the study participants (56.52%) were either unemployed or students; with the working-class individuals constituting the smallest group which represented 36.4% of the sample who are working in non-health-related sectors. The distribution of the socio-demographic characteristics of the participants is shown in Table 1.
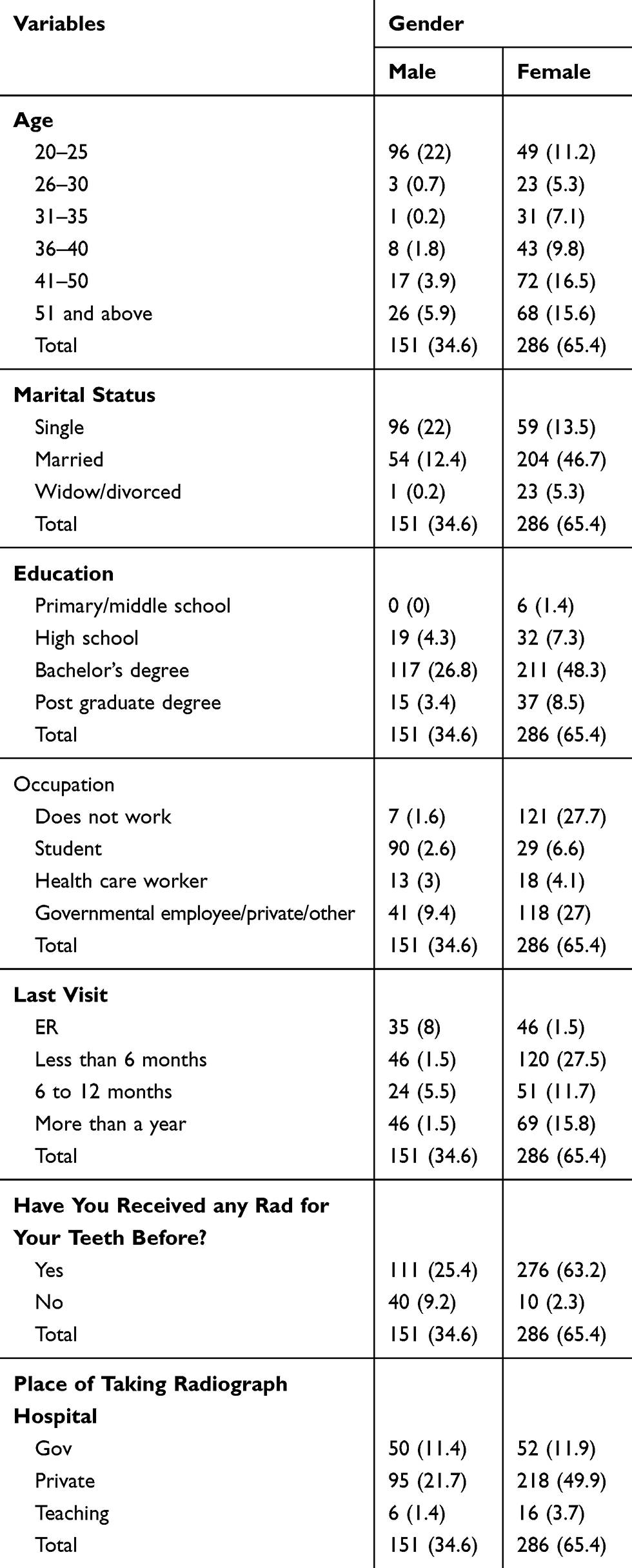 |
Table 1 Socio-Demographic Characteristics of the Sample |
Table 2 shows the perceptions and attitudes of the study participants toward different aspects of a radiographic prescription and practice by their dentist. More than half of the study population (51.7%) stated that they gave a history and underwent clinical examination are either often or always preformed before radiographs are taken. Moreover, almost 40% of the respondents indicated that their dentists never explained the hazards associated with radiography to them. However, almost one-third of the participants (28.4%) reported that they have never asked about radiographic safety measures. Furthermore, a majority of the dentists (67.2%) either always or frequently explained the results. A majority of the study participants did not abstain from radiography because of it is potential hazards.
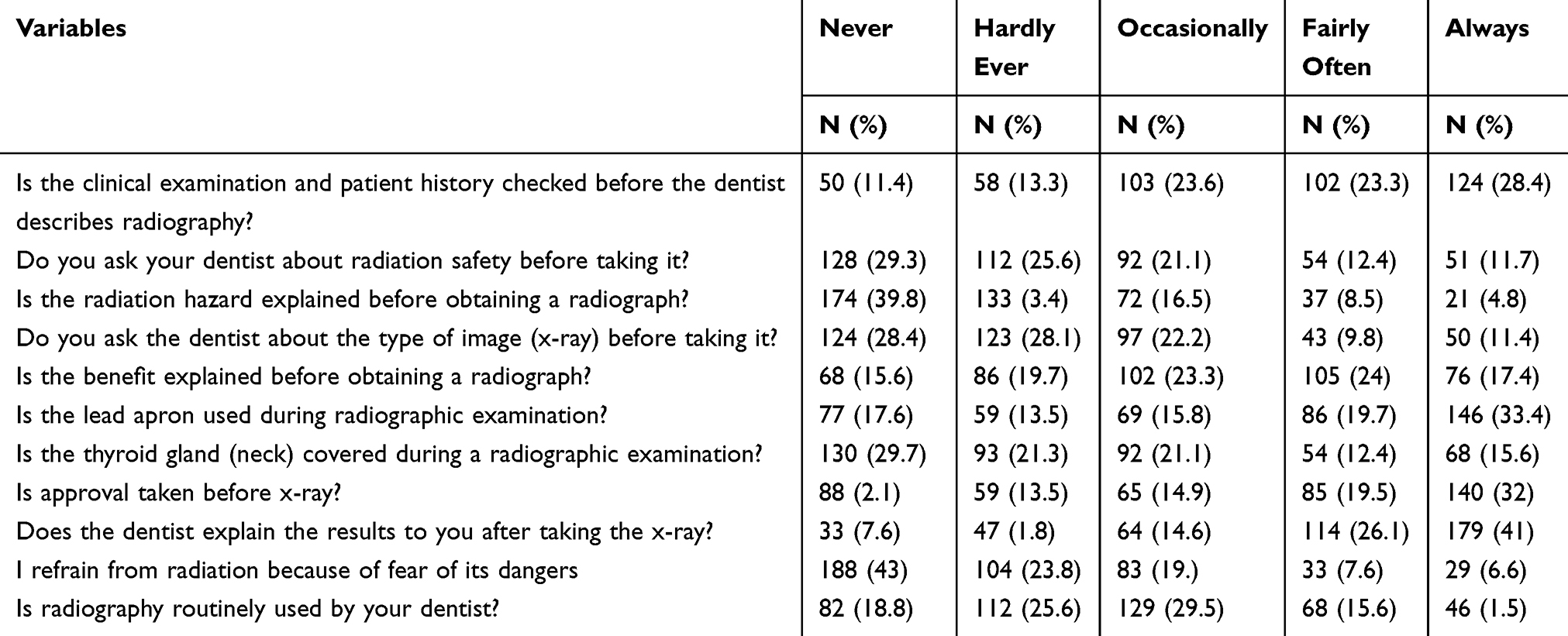 |
Table 2 Perception and Attitude of the Respondents Regarding Different Aspects of a Radiographic Prescription and Practice by Their Dentist |
Clinical examination and patient history before taking radiographs were significantly associated with age at p = 0.043. The Tukey’s test indicated the most significant difference was between the 36–40 and 41–50 years age groups, with the latter were agreeing less that clinical history and examination was performed before radiography.
There was also a significant difference in the age groups regarding if radiation hazards were explained prior to obtaining radiographs or not. Tukey post hoc analysis showed that a significant difference exists between those in the 20–25 years age group and those in the 31–35 years age group. Similarly, students and singles agreed significantly more than governmental employee and married individuals about radiation hazards being explained to them, with P-values of p = 0.009 and p = 0.012, respectively. Respondents with previous radiographs were more to ask the dentist about radiation hazards was significantly associated with age (p = 0.020), previous radiographs (p = 0.012), and whether the individual being treated at governmental, private or teaching hospital (p = 0.012). The Tukey post hoc analysis indicated that significantly more respondents treated in teaching hospitals asked questions about hazards than those in private hospitals. The hazards were also explained to them significantly more (p = 0.023).
The level of education and marital status were significantly associated with the question related to the routine use of radiographs in the visited dental clinic (p = 0.038 and p = 0.003, respectively). Respondents who had attended high school agreed more than those with bachelor’s degrees.
Participants with frequent dental visits (less than 6 months) agreed significantly more that lead aprons were used during radiation exposure than those who presented only for emergency treatments. The significant results are summarized in Tables 3 and 4.
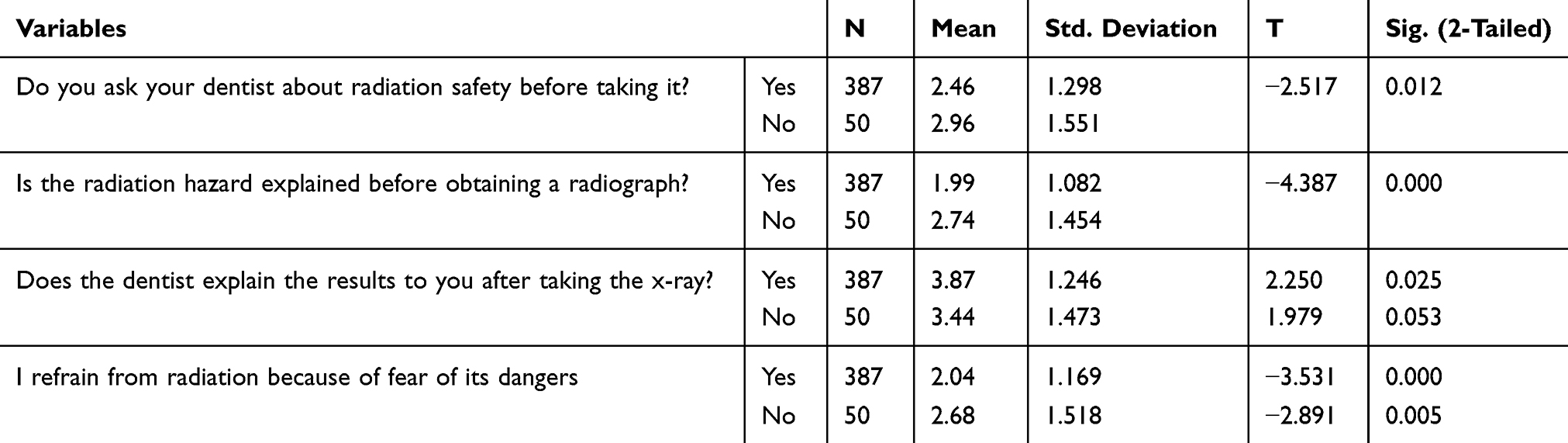 |
Table 3 T-Test of Analysis of the Association Between Previous Radiographs and Perception and Attitude |
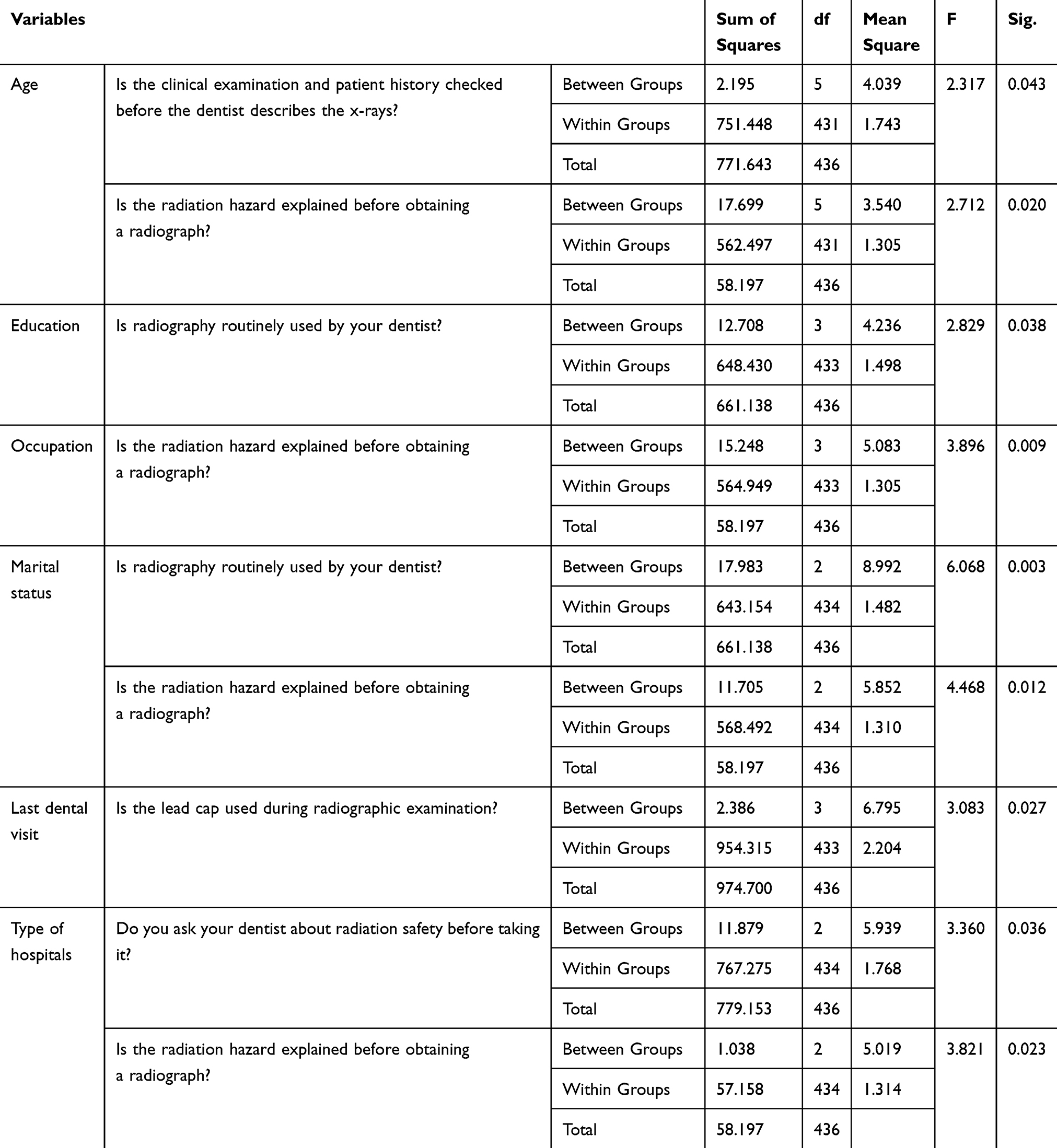 |
Table 4 Association of Sample Characteristics with Perception and Attitudes Using ANOVA Test |
Discussion
Radiation hazard is never considered zero, but when this procedure will benefit the treatment outcome, dentists have to ensure that the amount of radiation received outweighs the risk. The amount of radiation received by patients cannot be compared between individuals receiving different treatments; however, the dose is dependent on the type of imaging and how frequently it is used by the dentist. This investigation was designed to explore the population perspectives about radiographic hazards, prescription, attitude, and anxiety in the dental clinics.
Diagnostic imaging is one of the elements of a large strategy plotted to treat patients successfully. Exposure of the patients to ionizing radiation used in dentistry carry a subtle risk of a stochastic effect that may lead to cancer or genetic mutations but there are tremendous benefits derived from radiographic investigations for diagnosis, management, and monitoring the improvement of treatments offered. Certain amounts of radiation are inevitably delivered to patients during dental treatment. Despite the indispensable role of imaging in dentistry, it still has the potential to cause harmful effects. However, there are dangers associated with the use of the various imaging modalities frequently used in dental treatment. This danger is not comparable to the risk associated with other activities in daily life. In Saudi Arabia, the average dose the population was exposed to from natural background radiation was estimated by Al ammar in 2008, where he studied the amount of radiation from the soil in Riyadh and found that the annual effective radiation dose was calculated to be 0.14 mSv y−1.12
A majority of the general population have access to dental information if they have concerns or doubts either through social media or websites of dental universities and hospitals, or private websites of dentists from different specialties. In the past, patients preferred to extract the tooth when they started to have pain due to several factors, among them their socio-economic status or difficulty accessing dental clinics. However, these behaviors have been changed with increased education and awareness of the population and prefer to keep their teeth to maintain function and esthetics by seeking dental treatment for the restoration of decayed teeth or periodontitis or other craniofacial complications to lower the risk of tooth mortality and maintain a healthy dental status. This tendency of going for a preventive approach increases the frequency of use of ionizing radiation to optimize treatment outcomes.
After careful clinical examination and to formulate proper treatment plans, dentists frequently need further investigation to confirm their clinical findings by requesting various imaging modalities. With good practice, dentists must adhere to ALARA principles when requesting any imaging modalities it is recommended to use the lowest possible radiation doses required to produce the desired diagnostic image. In this study, the majority of respondents declared that clinical examination was conducted before performing any imaging modalities. Also, the dentist explained the result of the requested radiograph, which is the same finding reported by Purmal et al.13
Our investigation demonstrated that radiography is not used on a regular basis, but it will be requested depending on clinical need. This might also indicate the adherence of dentists to ALARA. Likewise, observing the relationship between the radiation dose and risk estimated for each imaging procedure and the benefit obtained from the radiographic image obtained.14
Although several methods of protection15–17 have been applied to reduce the radiation dose to patients, among them using digital or fastest films, use of lead aprons, use of rectangular collimators, adjustment of the exposure factor based on the task still required some concern from patients regarding the hazards of ionization radiation used in dentistry. In this study, more than half of the patients that never asked their dentist about the safety of procedures used. This could be attributed to the trust the patients had for their dentist. They believed that their dentists would never subject patients to unnecessary radiation that will not contribute to treatment or diagnosis. It could also be because the patients did not have any idea about these safety measures. Up to 70% reported that lead aprons were used before any radiographic procedures. In this study, we are not aware whether or not the lead aprons used by various dental clinics covered the thyroid gland to justify the 50% of participants that did not use the thyroid collar during radiographic examination. Also, panoramic radiography is the most requested radiograph by dentists. It is a frequently prescribed screening procedure by many dentists during initial visits. Thyroid collars are not recommended in panoramic radiography since it will obscure the anterior area and lead to error and poor diagnostic images.
The perception of dental care by the population and safety protection methods implemented in the majority of dental clinics visited by the patients included in this study explained why the majority of the participants approved of radiographic procedures and never refrained from any procedure suggested by the dentist due to fear of dangerous effects of radiation.
Almost 40% of the respondents indicated that hazards were never explained to them by their dentists, which could be due to the limited time the dentist spent with the patients, or the fact that they concentrated on the treatment. Nevertheless, 4.8% of respondents reported that the dentist explained the hazards to them before taking radiographs. Therefore, dentist must educate the patients about the hazards of dental radiography and describe the benefit versus the risk, while reassuring the patients. If patients have any fear of exposure to dental radiation, the dentist has the responsibility to alleviate this fear.
In general, we cannot overemphasize the importance of the development of a good perception, and thus, acceptable awareness about the importance of imaging procedures to optimize the treatment outcomes. The dentist and oral radiologist must take some time to educate and inform patients about the hazards associated with x-ray and the different methods implemented to reduce these hazards. Scientific information regarding radiation doses delivered in dentistry might be disseminated improperly through the media to the public. With increased awareness of the population of the benefits of radiography, taking radiographs will improve the treatment outcome. In this study, 64.7% of the participant said that the dentist explained the benefit of taking radiographs, and this justified the use of specific procedures for specific tasks.
This investigation indicated that age, level of education, and marital status were associated with the perception of radiation hazards. Similarly, individuals treated in teaching hospitals were more prone to ask questions about the risks associated with radiography. Moreover, previous radiographs increase the concerns about the hazards associated with radiography. This is the first study to demonstrate such a relationship.
Overall, it seems that a reasonable percentage of participants’ value dentists’ practice of taking radiographs. Since a good percentage indicated a clinical screening, explanations of the clinical benefits, results, and obtaining the approval of patients before prescribing. Correcting the community perception assists in correcting wrong beliefs and ameliorating the practice of dentistry.
Conclusion
Our investigation revealed a reasonable perception and practice of dentists with respect to ionizing radiation. Yet, more emphasis needs to be laid on educating the population about hazards and protection, since perception was related to being exposed to dental radiography and several demographic variables. This might give the impression of perception built on experience.
Data Sharing Statement
Data are available and can be provided upon request.
Ethics Approval and Informed Consent
Ethical approval was obtained from Research Ethics Committee, Deanship of Scientific Research, King Saud University, Riyadh, Saudi Arabia. (IRB#E-20-4896CDRC No. FR0548235). Participation was voluntary, and written consent were obtained prior to contribution. This study was conducted in accordance with the Declaration of Helsinki.
Consent for Publication
We consent to that the details of any images, videos, recordings, etc. can be published, and that the persons providing consent have been shown the article contents to be published.
Acknowledgments
The author would like to express deepest thanks to the Researchers Support and Services Unit at King Saud University for their editorial assistance.
Funding
This research project was supported by a grant from the “Research Center of the Female Scientific and Medical Colleges”, Deanship of Scientific Research, King Saud University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. UNSCEAR. Source and Effect of Ionizing Radiation: United Nations Scientific Committee on the Effect of Atomic Radiation(UNSCEAR 2000). New York: United Nations; 2000.
2. White SC, Pharoah MJ. Oral Radiology-E-Book: Principles and Interpretation. Elsevier Health Sciences; 2014.
3. International Commission on Radiological Protection. 1990 Recommendations of the International Commission on Radiological Protection: Adopted by the Commission in November 199. New York: Pergamon; 1991.
4. Gibbs SJ. Effective dose equivalent and effective dose: comparison for common projections in oral and maxillofacial radiology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000;90(4):538–545. doi:10.1067/moe.2000.109189
5. Preston-Martin S, White SC. Brain and salivary gland tumors related to prior dental radiography: implications for current practice. J Am Dent Assoc. 1990;120(2):151–158. doi:10.14219/jada.archive.1990.0026
6. Preston-Martin S, Thomas DC, White SC, et al. Prior exposure to medical and dental x-rays related to tumors of the parotid gland. Natl Cancer Inst. 1988;80(12):943–949. doi:10.1093/jnci/80.12.943
7. Hwang SY, Choi ES, Kim YS, et al. Health effects from exposure to dental diagnostic X-ray. Environ Health Toxicol. 2018;33(4):e2018017. doi:10.5620/eht.e2018017
8. Ludlow JB, Davies-Ludlow LE, White SC. Patient risk related to common dental radiographic examinations: the impact of 2007 international commission on radiological protection recommendations regarding dose calculation. J Am Dent Assoc. 2008;139(9):1237–1243. doi:10.14219/jada.archive.2008.0339
9. Ludlow JB. Dose and risk in dental diagnostic imaging: with emphasis on dosimetry of CBCT. Korean J Oral Maxillofac Radiol. 2009;39(4):175–184.
10. ICRP Publication 105. Radiation protection in medicine. Ann ICRP. 2007;37(6):1–63. doi:10.1016/j.icrp.2008.07.001
11. Ashok NG, Kumar VJ. Patients perception on dental radiographs: a questionnaire-based study. Int J Orofac Biol. 2017;1:28–31.
12. Alaamer AS. Assessment of human exposures to natural sources of radiation in soil of Riyadh, Saudi Arabia. Turkish J Eng Environ Sci. 2008;32:229–234.
13. Purmal K, Alam MK, Nambiar P. Patients’ perception on dental radiographs. Int Med J. 2013;20(2):235–238.
14. Rushton VE, Horner K. The use of panoramic radiology in dental practice. J Dent. 1996;24(3):185–201. doi:10.1016/0300-5712(95)00055-0
15. Okano T, Sur J. Radiation dose and protection in dentistry. Jpn Dent Sci Rev. 2010;46(2):112–121. doi:10.1016/j.jdsr.2009.11.004
16. Horner K. Review article: radiation protection in dental radiology. Br J Radiol. 1994;67(803):1041–1049. doi:10.1259/0007-1285-67-803-1041
17. Gibbs SJ, Pujol A
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.