Back to Journals » Patient Preference and Adherence » Volume 20
Public Knowledge, Attitudes, and Practices Toward Obesity and Anti-Obesity Medications in Palestine: A Cross-Sectional Study
Authors Albarghouthy HM ![]() , Abdallah TW, Salahaldin MM, Mashni LI, Abukeshek A, Hallak H
, Abdallah TW, Salahaldin MM, Mashni LI, Abukeshek A, Hallak H ![]()
Received 8 September 2025
Accepted for publication 20 December 2025
Published 21 January 2026 Volume 2026:20 566117
DOI https://doi.org/10.2147/PPA.S566117
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Ramón Morillo-Verdugo
Heba M Albarghouthy,* Tala W Abdallah,* Mohammed M Salahaldin, Loae I Mashni, Abdullah Abukeshek, Hussein Hallak
Faculty of Medicine, Al-Quds University, Abu-Deis, Jerusalem, Palestine
*These authors contributed equally to this work
Correspondence: Heba M Albarghouthy, Email [email protected]
Background: Obesity is a rising public health concern in Palestine and is increasingly recognized as a chronic disease requiring long-term management. Understanding knowledge, attitudes, and practices (KAP) related to obesity and anti-obesity medications is essential for improving prevention and treatment efforts. This study assessed KAP levels and awareness of anti-obesity medications among overweight and obese Palestinian adults.
Methods: A cross-sectional survey was conducted between September and December 2024 using a validated electronic questionnaire distributed through social media platforms. Overweight and obese adults aged 18– 80 years were invited to participate.
Results: Among 380 respondents, 85% demonstrated good knowledge of obesity, 65.5% showed positive attitudes, and 50.5% reported good practices. Awareness of anti-obesity medications was high (75.8%), although only 8% had used them.
Conclusion: Despite strong knowledge and generally positive attitudes toward obesity management, practical engagement in healthy behaviors remains suboptimal. Public-health programs and educational interventions are needed to bridge the gap between awareness and effective practice, including better integration of evidence-based pharmacologic options.
Keywords: awareness, practice, weight loss, obesity, anti-obesity, Palestine
Introduction
Obesity is a major global health concern and is widely recognized as a chronic, relapsing condition that results from a complex interaction of biological, behavioral, socioeconomic, and environmental factors.1 According to the National Institutes of Health (NIH) and the World Health Organization (WHO), obesity is defined as a Body Mass Index (BMI) of 30 kg/m2 or higher. It is strongly associated with numerous comorbidities, including cardiovascular diseases, type 2 diabetes, hypertension, certain cancers, sleep apnea, osteoarthritis, fatty liver disease, and mental-health disorders such as depression and anxiety.2 These interconnected complications highlight the urgent need for effective and sustainable obesity-management strategies.
Recent global estimates indicate that obesity rates continue to rise, with projections suggesting that by 2025, obesity prevalence will reach 18% among men and 21% among women worldwide.3 The Eastern Mediterranean Region bears a disproportionately high burden, with some of the highest obesity-related mortality rates reported globally. Furthermore, recent regional data suggest that 66–75% of adults and 25–40% of children in Arab countries are overweight or obese.1 In Palestine, obesity is increasingly prevalent, with higher rates observed among urban populations, particularly among women (49.1% in urban vs 36.8% in rural settings).4
Although lifestyle modification remains the cornerstone of obesity treatment, its effectiveness is often modest, typically achieving only 3–10% weight loss, with a high likelihood of weight regain.3 Consequently, alternative interventions—including pharmacotherapy and bariatric surgery—have gained increasing attention for their potential to promote long-term weight control.5 Advances in pharmacotherapy have led to the approval of several medications for chronic weight management, including semaglutide, liraglutide, phentermine–topiramate, orlistat, and naltrexone–bupropion. Semaglutide, in particular, has demonstrated the greatest efficacy, achieving up to 10% body-weight reduction compared to placebo.1 Despite this progress, public understanding of these medications remains limited, and misconceptions about their safety and effectiveness persist.
Given the rising availability of anti-obesity medications and the increasing demand for simple and rapid weight-loss solutions, it is critical to assess public knowledge, attitudes, practices, and awareness regarding both obesity and the use of these therapies. However, evidence from Palestinian and broader Arab populations remains scarce, underscoring the need for research addressing this gap.6–12
Therefore, this study aimed to evaluate knowledge, attitudes, practices, and awareness related to obesity and anti-obesity medications among overweight and obese Palestinian adults.
Methods
Study Design and Setting
A cross-sectional, web-based survey was conducted between September and December 2024 across the northern, central, and southern regions of the West Bank, Palestine. Data were collected using a validated electronic questionnaire distributed via social media platforms, public community groups, and nutrition-focused forums. The survey targeted overweight and obese adults aged 18–80 years.
Consent to Participate
Participation in this study was voluntary. On the first page of the online questionnaire, participants were presented with an informed consent statement outlining the study purpose, procedures, confidentiality, and the right to withdraw at any time. Only individuals who provided electronic consent by selecting “I agree to participate” were able to proceed to the questionnaire. Responses were collected anonymously, and no identifying information was recorded.
Sampling and Participants
Participants were recruited using convenience sampling through online dissemination. The sampling frame included Palestinian adults residing in the West Bank. Inclusion criteria were: (1) Palestinian nationality, (2) age 18–80 years, and (3) self-reported BMI ≥ 25 kg/m2. Individuals who were non-Palestinian, underweight or normal weight (BMI < 25 kg/m2), outside the age range, or who provided incomplete BMI information were excluded.
Because recruitment occurred online, the sample is subject to potential self-selection bias, with possible over-representation of younger and more educated participants.
Sample Size
The required sample size was estimated using Slovin’s formula (n = N / [1 + Ne2]) based on a West Bank population of approximately 3.2 million adults (Palestinian Central Bureau of Statistics, 2023),13 with a 95% confidence interval and a 5% margin of error. The minimum calculated sample was 400 participants. To ensure adequate representation and account for incomplete responses, 620 individuals were invited; 380 completed the questionnaire and met the inclusion criteria.
Questionnaire Development and Validation
A self-developed questionnaire was constructed following a review of prior KAP studies on obesity and anti-obesity medications.1–5 The initial version was prepared in English, then translated into Arabic through a forward–backward translation process by bilingual experts. Content validity was assessed by two statisticians and two public-health specialists. A pilot study of 28 overweight or obese adults was conducted to evaluate clarity and reliability. Cronbach’s alpha coefficients ranged between 0.76 and 0.78 across scale domains, indicating acceptable internal consistency.
The final questionnaire included six sections:
- Demographics (age, gender, residence, education level, employment status, marital status, health-sector background, family history of obesity, height, weight, and past weight-loss strategies).
- Knowledge of obesity (definitions, causes, risks, complications).
- Attitudes toward obesity as a chronic condition.
- Weight-management practices.
- Opinions regarding obesity and its management.
- Awareness of anti-obesity medications, including mechanism of action, eligibility, effectiveness, and side effects.
Variables and Scoring
Knowledge: Correct = 1 point; incorrect = 0. “Good knowledge” defined as > 8/16 correct items; “poor knowledge” ≤ 8/16.
Attitude: Categorized using mean scores: positive (3.67–5.00), neutral (2.34–3.66), poor (<2.34).
Practice: Good practice = > 5/11 correct items; poor practice = ≤ 5/11.
Awareness of anti-obesity medications: Good awareness = > 5/11 correct; poor awareness = ≤ 5/11.
BMI was calculated from self-reported height and weight; this represents a potential measurement limitation.
Ethical Considerations
Ethical approval was obtained from the Al-Quds University Research Ethics Committee (Reference: 460/REC/2024). All procedures performed in this study involving human participants were in accordance with the ethical standards of the national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Bias Control and Missing Data
To reduce recall and social-desirability bias, the questionnaire ensured anonymity, avoided leading questions, and presented items in random order. Only complete responses were included in the analysis (complete-case approach). No imputation was performed.
Statistical Analysis
Data were analyzed using IBM SPSS Statistics version 27. Descriptive statistics (frequencies, percentages, means, and standard deviations) were used to summarize participant characteristics and KAP measures. Normality was assessed using both the Kolmogorov–Smirnov and Shapiro–Wilk tests.
Independent t-tests and one-way ANOVA were used to examine group differences when assumptions of normality and homogeneity of variance were met. When assumptions were violated, non-parametric alternatives (Mann–Whitney U and Kruskal–Wallis tests) were applied. Effect sizes (Cohen’s d or η2) were reported where applicable.
Multivariate regression analyses were conducted to identify independent predictors of knowledge, attitudes, practices, and awareness, adjusting for key confounders including age, gender, education level, and health-sector affiliation. Statistical significance was set at p < 0.05.
Results
Participant Characteristics
Of the 380 participants, 54.7% were females and 45.3% were males. Most respondents were aged 26–40 years (37.6%) or above 40 years (36.3%). A majority were married (61.8%), lived mainly in the northern West Bank (33.9%), and held a university-level education (85.8%). Most participants were employed (63.9%) or students (18.2%), and 72.4% were not affiliated with the health sector. Additionally, 58.7% were overweight and 30.5% had Class I obesity, while fewer fell into Class II or III obesity. Most participants (72.6%) had attempted weight loss in the previous year, and among them, only 20.5% maintained weight loss for more than a year. (Table 1)
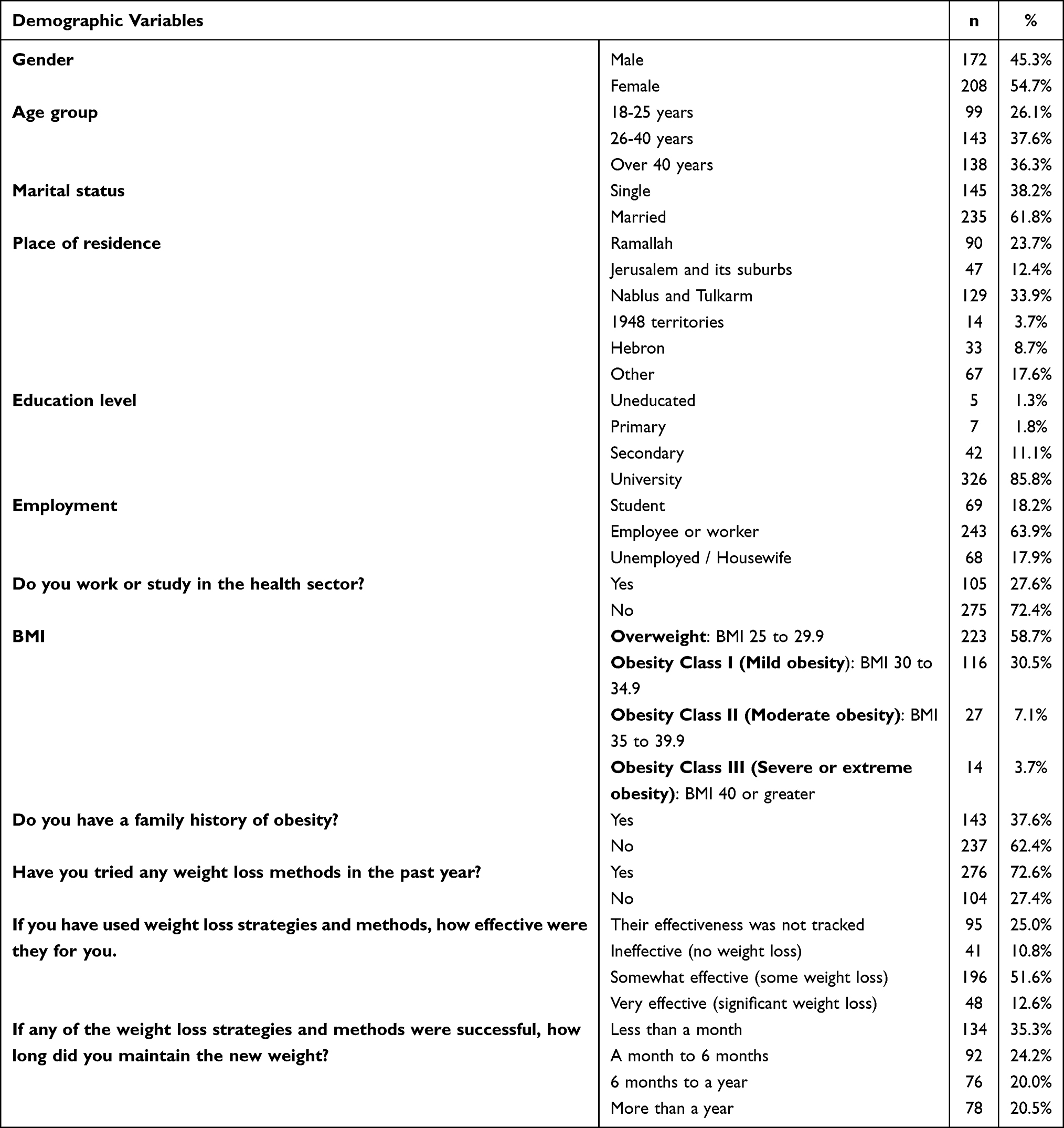 |
Table 1 Demographic Variables of the Participants (n=380) |
Knowledge of Obesity
A total of 85% of participants demonstrated good knowledge, while 15% had poor knowledge. (Figure 1)
 |
Figure 1 Distribution of knowledge levels among participants. Participants were categorized as having good knowledge (≥8 correct answers) or poor knowledge (<8) based on the median score. |
The mean correct response rate was 68.2%. Most participants correctly identified poor diet (91.1%) and lack of physical activity (90.8%) as major causes of obesity. Awareness of complications was high for cardiovascular disease (78.4%) and hypertension (72.9%), but lower for chronic kidney disease (37.6%) and cancer risk (41.1%). (Table 2)
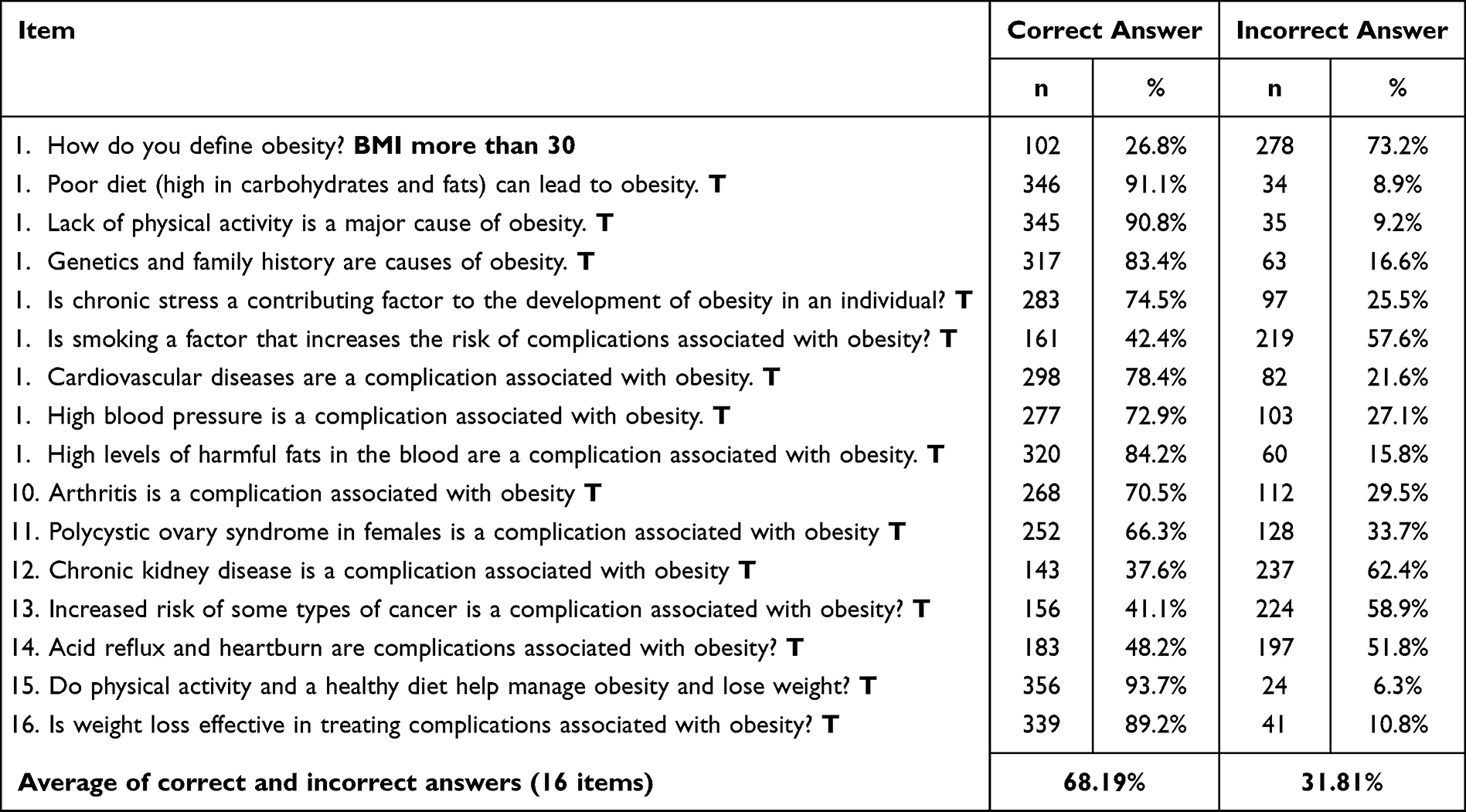 |
Table 2 Frequency and Percentages of Each Item Toward the Obesity Knowledge (n=380) |
Attitudes Toward Obesity
Overall, 65.5% of participants had a positive attitude toward obesity as a chronic condition, while 34.5% exhibited a neutral attitude. (Figure 2)
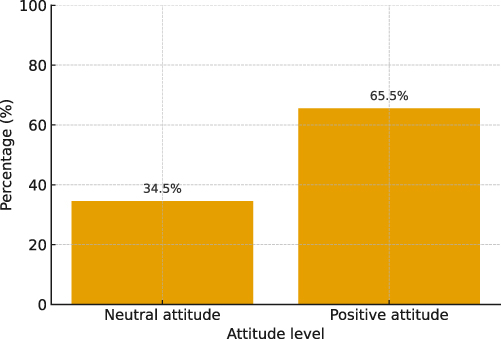 |
Figure 2 Distribution of attitude levels among participants. Attitudes were categorized as positive (3.67–5.00) or neutral (2.34–3.66) according to mean attitude scores. |
The total mean attitude score was 3.74 (SD = 0.36). Participants strongly agreed that obesity is a public health issue requiring management (Mean = 4.62) and expressed willingness to reduce calorie intake and increase physical activity. Mixed attitudes were noted regarding the use of anti-obesity medications and bariatric surgery. (Table 3)
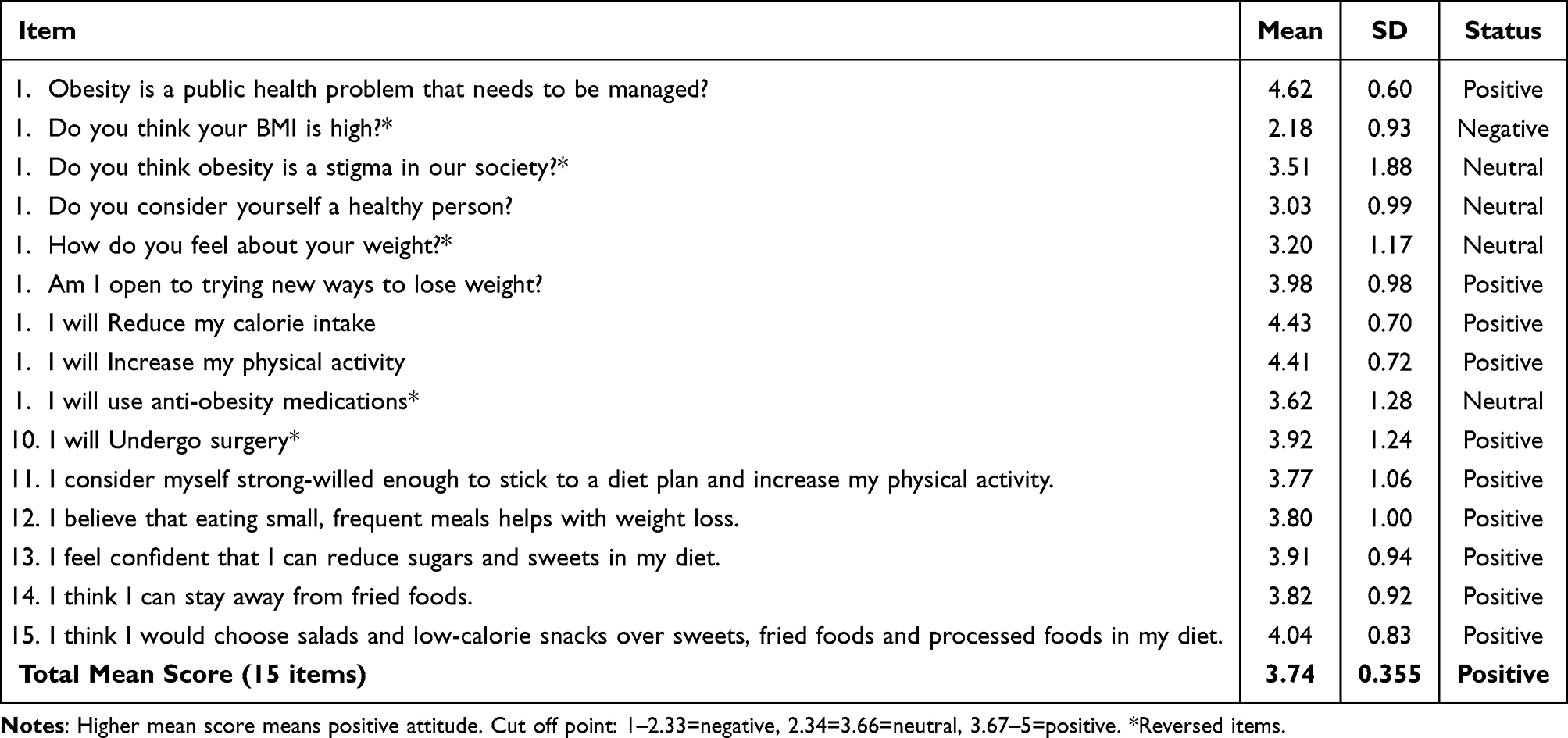 |
Table 3 Mean Score for Each Item Toward the Attitude of Participants About Obesity (n=380) |
Obesity-Related Practices
Overall, 50.5% demonstrated good practices, while 49.5% had poor practices. (Figure 3)
 |
Figure 3 Distribution of practice levels among participants. Practices were classified as good (>5 correct answers) or poor (≤5) based on the median practice score. |
Positive behaviors included avoiding excessive fast food (72.9%) and avoiding food close to bedtime (65.5%). However, unfavorable behaviors were common, such as skipping meals followed by overeating (54.5%), eating while watching screens (55.0%), and staying up late (60.5%). Only 42.6% engaged in daily physical activity, and 43.4% sought professional advice. (Table 4)
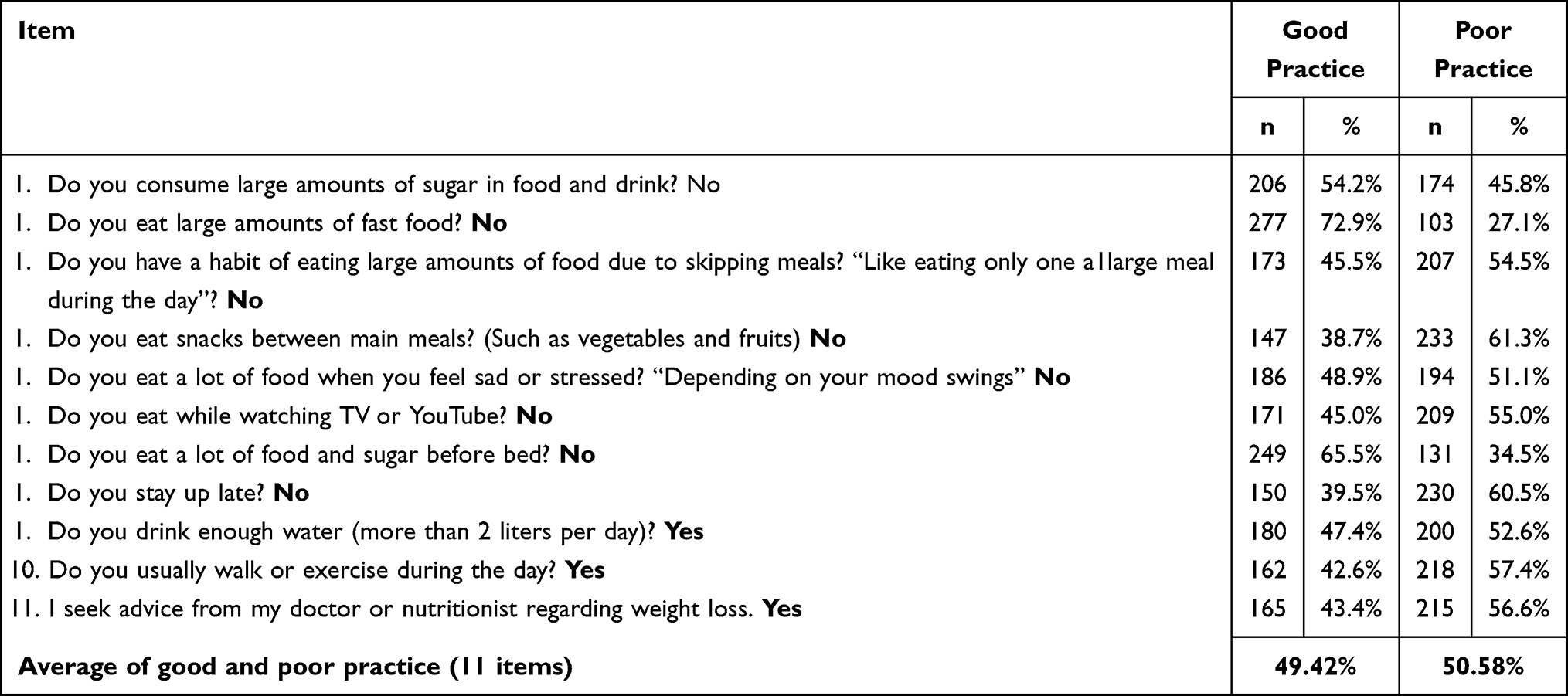 |
Table 4 Frequency and Percentages of Each Item Toward Practice Among Participants (n=380) |
Awareness of Anti-Obesity Medications (AOMs)
A total of 75.8% were aware of anti-obesity medications, while 24.2% were not. (Figure 4)
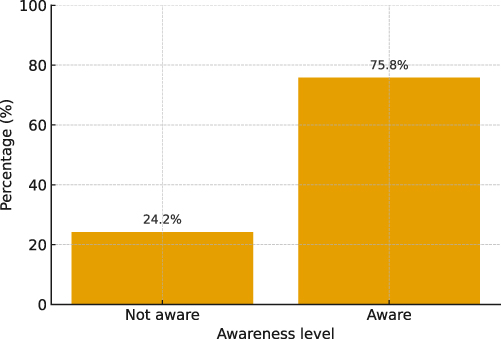 |
Figure 4 Distribution of awareness levels regarding anti-obesity medications among participants. Awareness was classified as good (>5 correct answers) or poor (≤5) based on the median awareness score. |
Most participants recognized appetite-suppressing mechanisms (90.3%) and enhanced satiety (82.6%), and 78.4% believed medications were not effective without diet and exercise. However, only 23.4% correctly identified BMI ≥ 30 kg/m2 as the eligibility criterion. Awareness of potential risks such as pancreatitis and thyroid tumors exceeded 70%. (Table 5)
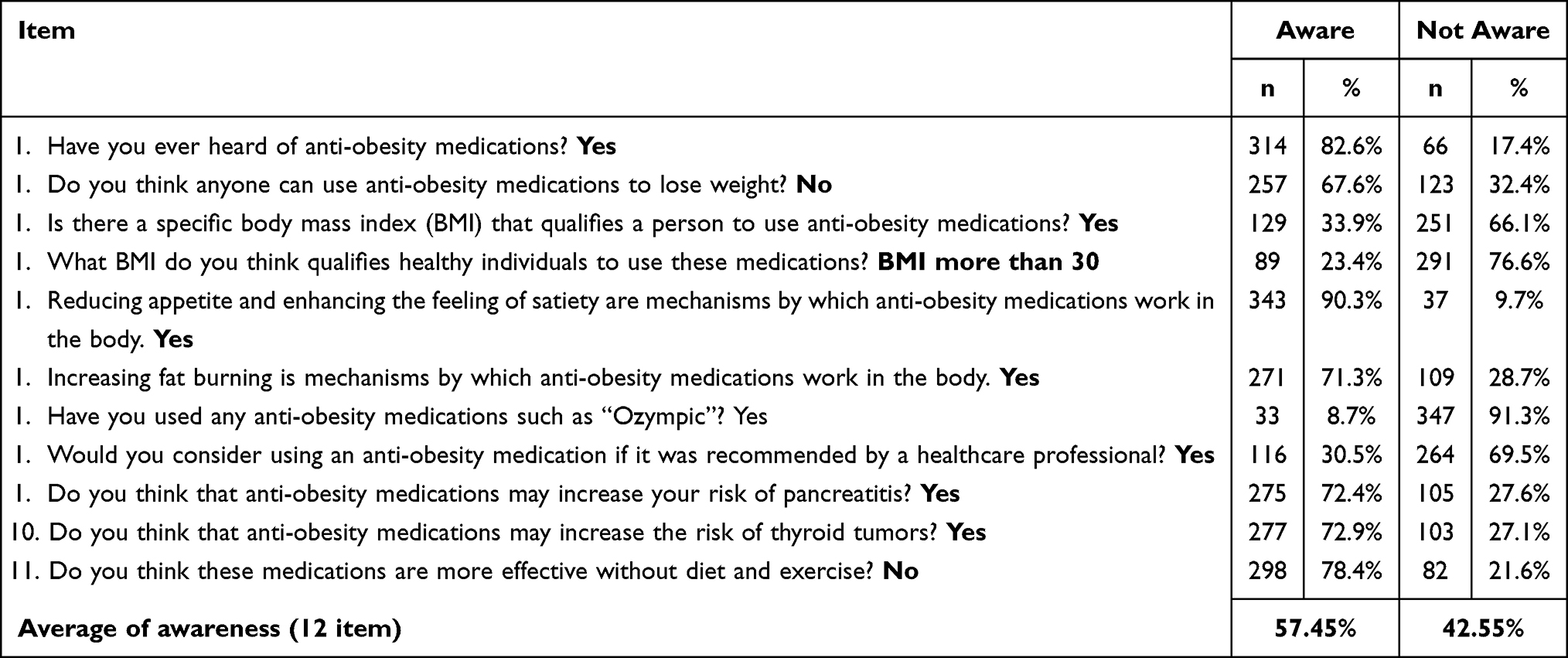 |
Table 5 Frequency and Percentages of Each Item Toward the Awareness of Obesity (n=380) |
Opinions on Obesity and AOMs
Around 23.2% first learned about slimming medications from the internet, while 11.6% heard about them from healthcare providers. Side effects were the most common concern (83.9%), followed by doubts regarding long-term effectiveness (28.9%) and cost (24.7%). About one-third reported no daily physical activity, and 12 participants had used Ozempic. (Tables 6 and 7)
 |
Table 6 Opinion Related Information Among Participants (n=380) |
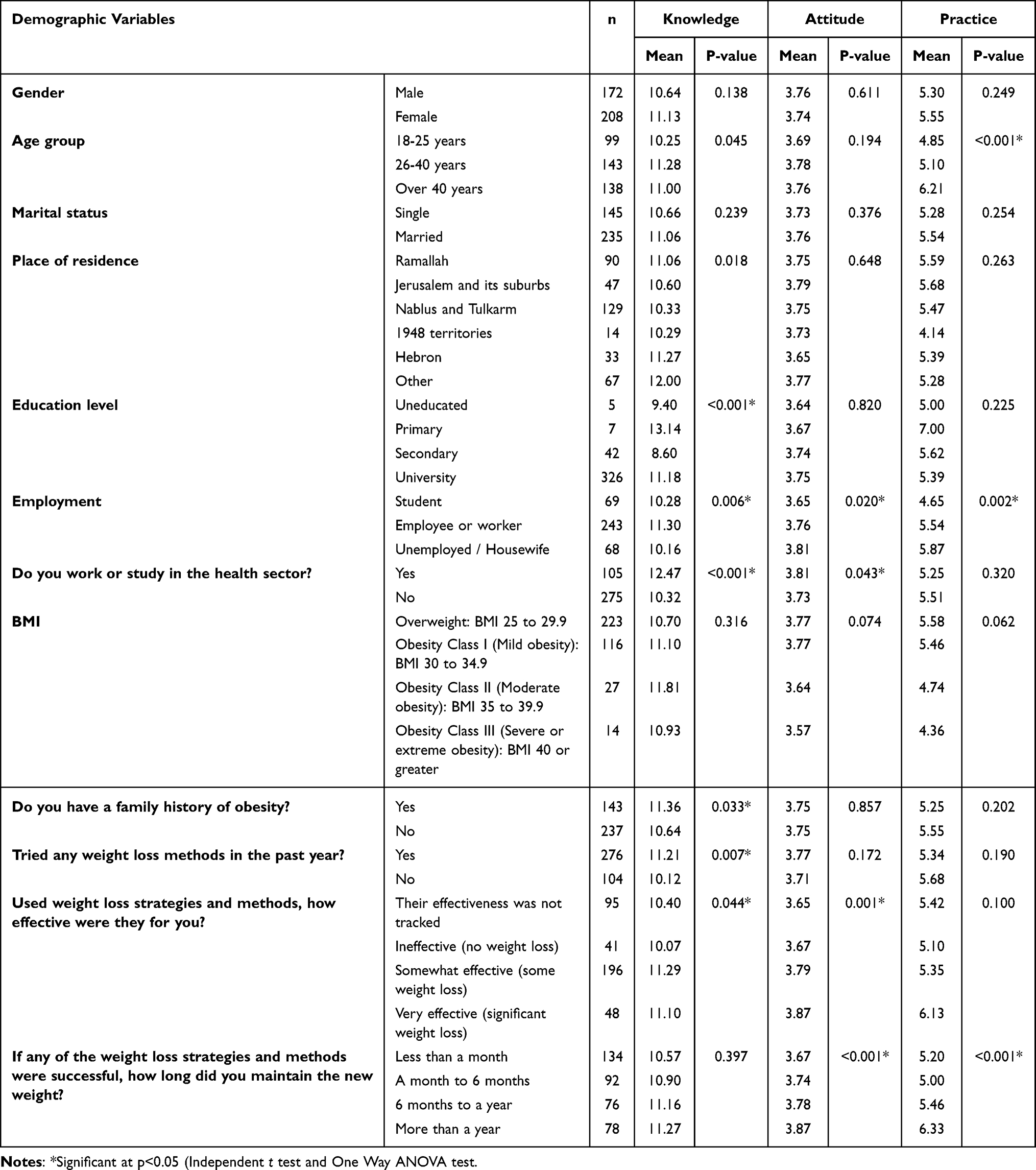 |
Table 7 Differences Between Demographic Variables in Term of Both Knowledge, Attitude and Practice Scores (n=380) |
Group Differences Across Characteristics
Significant differences in knowledge were observed across age groups, education level, health-sector involvement, family history of obesity, and recent weight-loss attempts.
Attitude scores were significantly higher among health-sector workers/students and those who experienced effective weight-loss outcomes.
Older participants (> 40 years) and those maintaining weight loss for > 1 year demonstrated significantly better practice scores. (Table 7)
Correlation Analysis
Awareness was positively correlated with knowledge (r =0.349) and weight-loss strategy effectiveness (r =0.158).
Practice correlated positively with age (r =0.257) and weight-loss maintenance duration (r =0.158), and negatively with BMI (r = –0.138).
Attitude correlated positively with weight-loss strategy effectiveness (r =0.207) and maintenance duration (r =0.206), but negatively with BMI (r = –0.131).
Knowledge correlated positively with education level (r =0.141) and weight-loss strategy effectiveness (r =0.116). (Table 8)
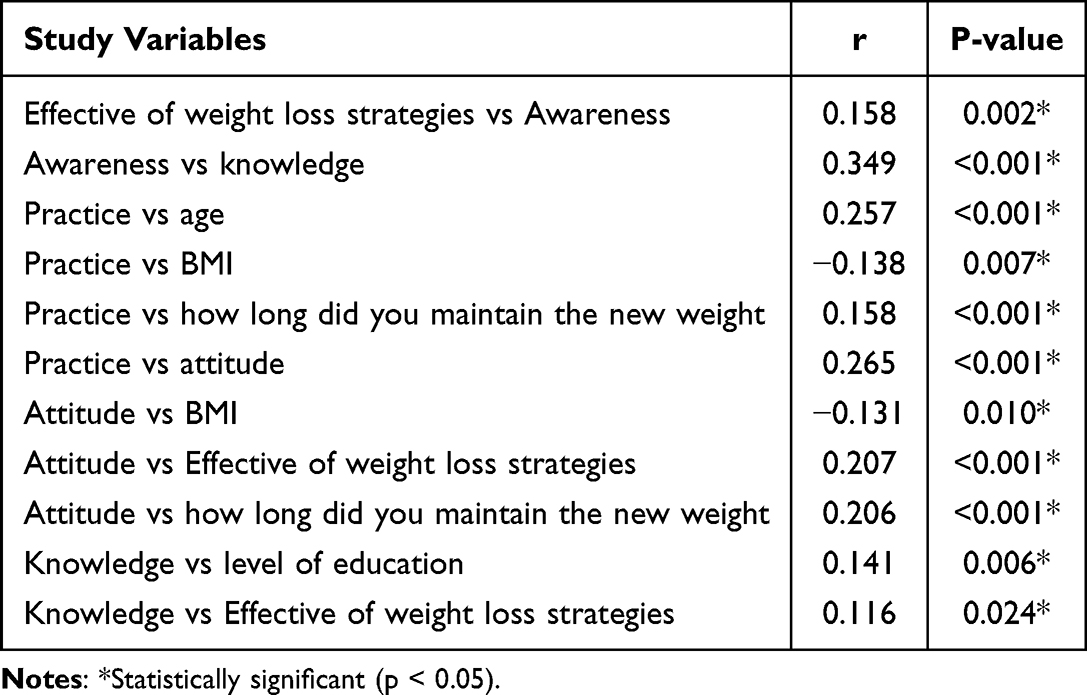 |
Table 8 Correlation Between Study Variables |
Discussion
This study provides updated insights into the knowledge, attitudes, practices, and awareness related to obesity and anti-obesity medications (AOMs) among overweight and obese Palestinian adults. Overall, the findings reflect a regional pattern commonly observed in Middle Eastern populations: relatively high knowledge and generally positive attitudes, contrasted with suboptimal practices and low uptake of pharmacological treatments.
Knowledge
Participants demonstrated high awareness of common causes and complications of obesity. Recognition of dietary and physical inactivity factors was similar to findings from Saudi Arabia, where the majority also recognized these contributors.1 However, awareness of less familiar complications—such as cancer—was limited, contrasting with higher cancer-related awareness reported in Pakistan2 and the ACTION-IO multicountry cohort.3 These gaps suggest a need for enhanced public-health messaging emphasizing long-term and less visible risks.
A major deficit involved defining obesity using BMI thresholds, with only a minority identifying BMI ≥ 30 kg/m2. This diverges from Sharaf et al’s findings in Saudi Arabia,4 where awareness of obesity definitions was considerably higher. Educational attainment strongly predicted knowledge levels, supporting evidence from the United States showing that higher education enhances health literacy and comprehension of chronic disease concepts.5
Participants working in health sectors scored higher, consistent with similar findings from Bahrain, where healthcare workers had better basic obesity literacy.13 Participants with a family history of obesity and prior weight-loss attempts also demonstrated better knowledge, consistent with evidence suggesting that personal or familial exposure improves health-related awareness.14
Attitudes Toward Obesity
Attitudes toward obesity management were largely positive, with strong willingness to reduce caloric intake and increase physical activity. These trends agree with Puhl and Heuer’s findings15 and regional data showing increasing acceptance of obesity as a chronic condition requiring structured management.1
However, societal stigma toward obesity was less prominent than in Western countries, where stigma is more explicitly recognized.16 Cultural perceptions of body weight in Arab populations may explain these differences.
Health-sector workers and individuals who achieved meaningful weight loss displayed more positive attitudes, supporting literature demonstrating that exposure to health information and successful experiences foster positive perceptions of weight management.17 Mixed feelings toward AOMs and bariatric surgery mirrored findings from India and Bahrain, where populations consistently preferred lifestyle-based interventions and expressed concerns about cost, side effects, and accessibility.13,18
Neutral self-perception findings reflected similar patterns in Saudi Arabia, Mexico, and Gaza, where weight misperception is common and strongly influences health-seeking behavior.1,4,19 Consistent with previous research, higher BMI was associated with less favorable attitudes, while effective weight-loss strategies and longer maintenance duration correlated positively with attitudes.17
Practices
Despite good knowledge and generally positive attitudes, practices were nearly evenly split between good and poor. This knowledge–practice gap has been widely documented in regional obesity studies.4 Although avoidance of fast food and late-night eating was common, sedentary behaviors and irregular eating patterns remained highly prevalent—findings consistent with both global patterns17 and evidence from India and Bahrain highlighting the role of sedentary lifestyle in weight gain.13,18
Participants over 40 demonstrated better practices, whereas prior Saudi research found no significant association with age.1 Homemakers showed better practices than students, possibly due to more structured daily routines and fewer academic demands. Long-term weight-loss maintenance emerged as a strong predictor of healthier practices, aligning with studies that emphasize behavioral reinforcement and self-efficacy as key determinants of sustained weight control.17
Underutilization of professional support was consistent with Bahrain’s findings, which attribute this to insufficient structured weight-management services and reliance on non-specialist advice.13
Awareness of Anti-Obesity Medications (AOMs)
Awareness of AOMs was relatively high, comparable to results from Almughais et al in Saudi Arabia,1 although gaps in understanding eligibility criteria persisted. As in Sharaf et al’s findings,4 participants understood general mechanisms but had limited knowledge of clinical thresholds for prescribing AOMs.
Social media was the dominant information source, reflecting its expanded role in shaping health perceptions regionally and globally. However, fears regarding side effects were exceptionally high—much higher than reported in Saudi Arabia1—which may reflect public mistrust, cultural caution toward pharmaceuticals, or lack of accessible medical counseling.
Awareness of risks such as pancreatitis and thyroid tumors aligned with findings from Waghmare et al,18 though awareness did not necessarily translate into willingness to use medications. Only a minority expressed willingness to take AOMs even if recommended by a healthcare professional, mirroring global literature describing stigma and misconceptions surrounding pharmacological obesity treatments.3,18
Use of AOMs was very low (8.7%), contrasting with higher usage reported in Saudi Arabia.2 This gap is likely explained by the absence of Ministry of Health approval for GLP-1 agonists in Palestine and lack of insurance coverage—key determinants of accessibility also identified in OECD obesity reports.20
Study Limitations
This study has several limitations. The use of an online self-administered questionnaire may introduce selection bias and limit participation among individuals with limited internet access. Self-reported height and weight may have resulted in measurement bias. The cross-sectional design prevents establishing causal relationships between variables. Additionally, individuals with a previous history of obesity but a current BMI < 25 kg/m2 were excluded, limiting insights into the experiences of those who successfully maintained weight loss. Finally, although the sample size was adequate, it may not fully represent all Palestinian subpopulations.
Recommendations
Based on the study findings, several evidence-informed strategies may help improve knowledge, attitudes, and practices related to obesity management in Palestine.First, implementing structured community-based educational programs focused on obesity risk factors, early identification, and long-term health consequences may enhance public understanding. Expanding accessible online health-education resources is recommended, given that social media was the most frequently reported source of information.At the clinical level, integrating standardized counseling on nutrition, physical activity, and weight-management strategies within primary care settings may strengthen patient engagement. Training healthcare providers in updated obesity-management guidelines, including indications for anti-obesity medications, could further support evidence-based care.At the policy level, improving access to safe and effective pharmacotherapies—such as recently approved GLP-1 receptor agonists—may support individuals who do not respond adequately to lifestyle modifications. Ensuring affordability through governmental or insurance coverage should also be considered.Finally, future interventions may benefit from developing multi-sectoral initiatives that encourage physical activity and promote supportive environments conducive to long-term weight control.
Conclusion
Participants in this study demonstrated generally high levels of knowledge and positive attitudes toward obesity, yet these did not consistently translate into effective weight-management practices. Although awareness of anti-obesity medications was relatively high, actual utilization remained very limited. These findings underscore the need for targeted educational interventions, improved clinical counseling, and greater access to evidence-based pharmacological treatments to support effective obesity management in Palestine.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
Heba M Albarghouthy and Tala W Abdallah are co-first authors for this study. Mohammed M Salahaldin, Loae I Mashni, Abdullah Abukeshek, and Hussein Hallak are co-second authors for this study. The authors declare that they have no competing interests in this work.
References
1. Almughais ES, Alshehri MH, Alsatti M, et al. Awareness and perception of anti-obesity medications among Al-Ahsaa, Riyadh, and Hail in Saudi Arabia populations. Cureus. 2023;15(6):e40425. doi:10.7759/cureus.40425
2. Mahmood S, Najjad MKR, Ali N, Yousuf N, Hamid Y. Predictors of obesity among post-graduate trainee doctors working in a tertiary care hospital of the public sector in Karachi, Pakistan. J Pak Med Assoc. 2018;60(9):758–13.
3. Vázquez-Velázquez V, Laviada-Molina H, García-García E, Sandoval-Diez E, Mancillas-Adame L. Perceptions, attitudes, and barriers to obesity care in Mexico: data from the ACTION-IO study. Obesity. 2021;29(2):317–326. doi:10.1002/oby.23077
4. Sharaf ES, Al-shalabi BT, Althani GF. Obesity self-management: knowledge, attitude, practice, and pharmaceutical use among healthy obese individuals in Saudi Arabia. Int J Fam Community Med. 2021;5(4):110–121. doi:10.15406/ijfcm.2021.05.00232
5. Beydoun MA, Wang Y. Sociodemographic disparities in the dietary behaviors of U.S. adults. Am J Prev Med. 2009;36(2):104–111. doi:10.1016/j.amepre.2008.09.018
6. Alqarni SS. A review of prevalence of obesity in Saudi Arabia. J Obes Eat Disord. 2016;2(2):25. doi:10.21767/2471-8203.100025
7. Anwar M, Hussain M, Sarwar H, et al. Association of pharmacological treatments for obesity with weight loss and adverse events. Int J Soc Sci Manag. 2018;5(3):187–191. doi:10.3126/ijssm.v5i3.20609
8. Yanovski SZ, Yanovski JA. Association of pharmacological treatments for obesity with weight loss and adverse events: a systematic review and meta-analysis. JAMA. 2014;311(1):74–86. doi:10.1001/jama.2013.281361
9. Abdul-Rahim HF, Holmboe-Ottesen G, Stene LC, et al. Obesity in a rural and an urban Palestinian West Bank population. Int J Obes. 2003;27(1):140–146. doi:10.1038/sj.ijo.0802160
10. Safaei M, Sundararajan EA, Driss M, Boulila W, Shapi’i A. A systematic literature review on obesity: causes and consequences and reviewing machine learning approaches. Comput Biol Med. 2021;136:104754. doi:10.1016/j.compbiomed.2021.104754
11. Palestinian Central Bureau of Statistics. Palestinian population estimates, Mid-2023. 2023.
12. Moorthy SBR, Subbaiahgari H, Sibbala P, et al. Study of the knowledge, attitudes, and practices of individuals regarding obesity. Int J Adv Med. 2022;9(7):783–788. doi:10.18203/2349-3933.ijam20221276
13. Al-Ghawi A, Uauy R. Study of the knowledge, attitudes, and practices of physicians towards obesity management in primary health care in Bahrain. Public Health Nutr. 2009;12(10):1791–1798. doi:10.1017/S1368980008004564
14. Galan-Lopez P, Sanchez-Oliver AJ, Ries F, Gonzalez-Jurado JA, Qiu J. Influence of family history on the level of physical activity and obesity in adolescents. Int J Environ Res Public Health. 2020;17(5):1538. doi:10.3390/ijerph17051538
15. Puhl RM, Heuer CA. Obesity stigma: important considerations for public health. Am J Public Health. 2010;100(6):1019–1028. doi:10.2105/AJPH.2009.159491
16. Schwartz MB, Chambliss HO, Brownell KD, Blair SN, Billington C. Weight bias among health professionals specializing in obesity. Obes Res. 2003;11(9):1033–1039. doi:10.1038/oby.2003.142
17. Teixeira PJ, Carraca EV, Markland D, Silva MN, Ryan RM. Exercise, physical activity, and self-determination theory: a systematic review. Int J Behav Nutr Phys Act. 2012;9(78):78. doi:10.1186/1479-5868-9-78
18. Waghmare V, Pathak S, Das S, et al. Assessment of knowledge, attitude, and practices regarding obesity and associated disorders among young adults. Int J Physiol. 2019;7(1):108–112. doi:10.5958/2320-608X.2019.00023.4
19. Frontiers in Public Health. Prevalence of overweight, obesity, and associated factors among healthcare workers in the Gaza Strip, Palestine: a cross-sectional study. Front Public Health. 2023. doi:10.3389/fpubh.2023.1129797
20. OECD. The heavy burden of obesity: economic and health impacts. Organisation for Economic Co-operation and Development; 2020.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.