Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
Public Awareness, Beliefs, And Attitudes Toward Bipolar Disorder In Saudi Arabia
Authors Alosaimi FD ![]() , AlAteeq DA
, AlAteeq DA ![]() , Bin Hussain SI, Alhenaki RS, Bin Salamah AA
, Bin Hussain SI, Alhenaki RS, Bin Salamah AA ![]() , AlModihesh NA
, AlModihesh NA
Received 17 March 2019
Accepted for publication 16 September 2019
Published 27 September 2019 Volume 2019:15 Pages 2809—2818
DOI https://doi.org/10.2147/NDT.S209037
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Fahad D Alosaimi,1 Deemah A AlAteeq,2 Sarah I Bin Hussain,3 Riham S Alhenaki,4 Abdullah A Bin Salamah,5 Noor Adnan AlModihesh1
1Department of Psychiatry, King Saud University, Riyadh, Saudi Arabia; 2College of Medicine, Princess Nourah Bint Abdulrahman University, Riyadh, Saudi Arabia; 3Department of Family Medicine and Polyclinics, King Faisal Specialist Hospital and Research Centre, Riyadh, Saudi Arabia; 4Department of Pediatrics, King Abdullah Specialized Children’s Hospital, KAMC, MNGHA, Riyadh, Saudi Arabia; 5Department of Family and Community Medicine, King Saud University, Riyadh, Saudi Arabia
Correspondence: Deemah A AlAteeq
College of Medicine, Princess Nourah Bint Abdulrahman University, P.O. Box 93949, Riyadh 11683, Saudi Arabia
Email [email protected]
Objectives: To examine public’s knowledge, beliefs, and attitudes toward bipolar disorder (BP) in Saudi Arabia (SA).
Methods: A cross-sectional survey was performed in 2016 in Riyadh, SA. The survey included sociodemographic characteristics and BP awareness scale.
Results: Of 416 participants, 49.5% had prior knowledge of BP, mainly from internet and social media, and 57% considered it to be common in SA. About half believed BP is caused by a neurophysiological or neurochemical imbalance and that it can be treated with psychiatric medications. Supernatural causes, weak faith, and weakness of character were considered causes of BP by 55%, 48%, and 40% of participants, respectively. Recreational activities and head bandaging by traditional therapists were considered viable treatment options by 55% and 41% of participants, respectively. Students and healthcare professionals scored significantly higher on awareness scale. Regarding attitude, a majority believed that persons with BP can work effectively (86%), have to pull themselves together to get over it (47%), and consider it a shame to mention that someone in a family is affected by BP (32%). Regarding relationships, 22% were not willing to maintain a friendship and 39.3% were not willing to marry someone with BP.
Conclusions: This study revealed suboptimal public awareness towards BP in SA. It identified several misconceptions and negative attitudes toward patients with BP. Further studies are needed to investigate potential public interventions to improve literacy of BP.
Keywords: bipolar disorder, awareness, literacy, attitudes, Saudi
Introduction
Bipolar disorder (BP) is a mental disorder that consists of manic/hypomanic and depressive episodes or manic episodes separated by periods of a stable mood. Manic episodes include elevated or irritable mood, hyperactivity, pressure of speech, inflated self-esteem, and a decreased need for sleep.1 Lifetime prevalence of BP is 1.0% for BP-I, 1.1% for BP-II, and 2.4% for subthreshold BP.2 BP is a debilitating disorder due to its early onset, severity, and chronicity.3 Moreover, there is huge caregivers’ burden related to patient behavior and patients’ and caregivers’ role dysfunction.4
The general public’s beliefs and attitudes toward mental illness may affect the level of care and treatment those with the illness receive.5 The public’s knowledge, beliefs, and attitudes toward BP are discussed extensively in the literature. A study in the United Kingdom explored the beliefs of lay people about the cause and treatment of BP. Brain’s chemical imbalance, drug use, emotional childhood trauma, and genetics were the most highly reported causes.6 A study in Spain7 on the opinions and beliefs about schizophrenia and BP found that 72% of the Spanish population endorsed psychological treatments as an effective therapeutic choice. This study also demonstrated prevalent concerns, including social rejection and lack of information and resources. Furthermore, more than half of participants in the first national survey of knowledge, attitudes, and behaviors toward BP in France8 cited stressful life events, lifestyle/environment, and drugs and alcohol abuse as the most important risk factors for BP, whereas one-quarter of participants selected genetic factors. Although both biomedical and psychosocial causes of BP were endorsed over fate causes by United Kingdom residents,9 this may not be same in other cultures that have supernatural beliefs.
In a Saudi Arabia, a misunderstanding of psychiatric disorders was demonstrated by the staff in general hospital.10 Poor knowledge and negative attitudes were reported by both doctors and patients in another Saudi general hospital, which negatively influenced the referral rates.11 A qualitative research conducted in Saudi primary healthcare centers has reported traditions, cultural norms as a main reason of stigma associated with psychiatric disorders. In addition, other significant reasons of stigma were reported, e.g. fear the reaction of psychiatric patients, lack of community awareness about psychiatric disorders and the role of psychiatrist, belief that psychiatric disorders cannot be cured, and that psychiatric disorders are hereditary. Whether patients will seek psychiatric help for BP also varies. The participants in the qualitative research have frequently mentioned seeking help from family or friends before consulting psychiatrist. On the other hand, going to “sheiks” (religious people) for Qur’an treatment was also reported.12 Regarding patients with BP, a study from Egypt conducted on patients with BP showed that 40.8% sought help from traditional healers before seeking psychiatric services.13 Other studies conducted in Saudi Arabia and Sudan have also reported patients with BP as being among visitors to traditional healers who interpret psychiatric disorders as being caused by spiritual and supernatural causes, e.g. jinn, evil eye, and witchcraft. This likely represents an important cause of delay in seeking psychiatric services, which may worsen the patients’ prognosis.14–17 Due to lack of data from Saudi Arabia, the objective of this study was to determine the public’s knowledge, beliefs, and attitudes toward BP.
Materials And Methods
Study Design
Data for this study were obtained using a cross-sectional survey during September and October, 2016. Ethical approval was obtained from the Institutional Review Board at the Faculty of Medicine at King Saud University in Riyadh, Saudi Arabia. Informed written consent was obtained from the participants after a detailed explanation of the aims of the study.
Sample Population
This study included both male and female, who are Arabic speakers over 17 years old currently living in Riyadh, Saudi Arabia. Survey participants under the age of 18 were permitted and approved by the Institutional Review Board at the Faculty of Medicine at King Saud University. People without the capacity to consent were excluded.
Recruitment
Eighteen medical students were trained to distribute the questionnaire to the residents of all regions of Riyadh (North, South, East, West). Medical students had small booths in shopping malls, public parks, hospitals, and on the walkway streets. Participants were selected conveniently.
Data Collection
A data collection tool was constructed from the literature on assessing mental health literacy in Arab regions.18–21 It was adapted mainly from a validated questionnaire which has been used in Saudi study on depression literacy with its parametrized answers.18 We chose items that assess BP awareness based on causes and treatments. We also added items that assess beliefs and attitudes toward people with BP. The questionnaire was translated into Arabic, approved by four psychiatrists, and then tested for both comprehension and readability by 20 subjects who were not included in the study. The time required to complete the survey was targeted to be around five minutes.
The final questionnaire consisted of the following sections: 1) sociodemographic characteristics including age, gender, marital status, nationality, educational level, and working status; 2) BP awareness based on: a) information had two items, b) sources of information used by participants were structured from none to eight potential sources (internet, social media, television, newspapers/magazines, leaflets/posters, hospitals/clinics, pharmacist/chemist, and relatives/friends/spouses), c) knowledge about the causes of BP had nine items, and d) knowledge about the treatment of BP had ten items; and 3) beliefs and attitudes toward patients with BP. Responses for BP awareness (Sections a–d) were either “yes” or “no”. Responses for beliefs and attitudes toward patients with BP were: “strongly agree,” “agree,” “neutral,” “disagree,” and “strongly disagree”. The scale of BP awareness was created from the sum of responses to the 21 items in Sections a, c, d. Positive responses were considered by answering “yes” to the positive statements: 2 items in section (a), 7 items in section (c), and 3 items in section (d). On the other hand, positive responses were considered by answering “no” to incorrect statements; 2 items in section (c) and 7 items in section (d). The 21 statements are illustrated in Table 1.
 |
Table 1 Percentages Of Positive Responses Toward Bipolar Awareness, Including Information And Knowledge (N=416) |
Statistical Analysis
Data were analyzed by using the Statistical Package for Social Studies (SPSS 22; IBM Corp., New York, NY, USA). Continuous variables were expressed as mean ± standard deviation (SD) and categorical variables were expressed as percentages. A Student’s t-test was used for continuous variables and the chi-square test was used for categorical variables. Because bipolar awareness score had a normal distribution, participants scoring more than or equal to the mean score of 12 points (~>70%) were defined arbitrary as bipolar literate.18 The differences in BP awareness were examined by sociodemographic characteristics, using BP awareness score ≤12 as a low awareness and BP awareness score >12 as a high awareness, which is illustrated in Table 2. Univariate and multivariate logistic regression models were used to calculate the odds ratio (OR) and its 95% confidence interval (CI). Low score (≤12) for BP awareness was used as an outcome (dependent variable) while sociodemographic variables were used as predictors (independent variables). Variables that were significant in univariate analysis were adjusted in multivariate analysis. A p-value <0.05 was considered statistically significant.
 |
Table 2 Univariate And Multivariate Logistic Regression Analysis To Predict Poor Bipolar Awareness Using Sociodemographic Characteristics (N=416) |
Results
Sociodemographic Characteristics
Of the 542 questionnaires distributed, 416 were completed (response rate of 76.75%). The demographic characteristics of the surveyed population are presented in Table 3.
 |
Table 3 Socio-Demographic Characteristics (N=416) |
BP Awareness Based On Information And Knowledge
Table 1 displays the positive responses from the 21-items scale provided by the participants on BP awareness based on information and knowledge about causes and treatments. Of the 416 participants, 50.5% had heard about BP, mainly from the internet (22.4%), social media (13%), and spouse/partner/relatives/friends (9.4%), while only 7% had heard it from clinics or hospitals. Moreover, 50% think that BP is common in Saudi Arabia. About half (45.2%) of the participants believed that neurophysiological or neurochemical imbalance is a cause of BP and 47.6% believed that psychiatric medications are a treatment for BP. In terms of BP origin, heredity or genetics was considered by 34.1% of participants and certain medical conditions were considered by 26% of them. Almost half of the participants believed that substance abuse is a cause of BP and most of them believed that smoking, having an occasional alcoholic drink, and amphetamine or hash use are not valid treatments to be used for BP (96.6%, 96.9%, and 97.4%, respectively). In addition, a traumatic life event, e.g., death of a close one, physical injury, theft, and other disaster, was considered as a cause of BP by 59.9% of the participants. Using brief counseling therapies (e.g. cognitive and/or behavioral therapies) was considered to be a treatment for BP by 44% of the participants. Less than half of the participants believed that weakness of character and a weak faith represented causes of BP, at 40.1% and 47.8%, respectively. Moreover, supernatural causes of BP were mentioned in addition to the provided scale, e.g. evil eye, magic, and jinn possessions at 19.2%, 18.8%, and 17.1%, respectively. On the other hand, prayer and faith-healing were mentioned as treatments for BP by 66.6% and 42.3% of the participants, respectively.
Differences In The Awareness Of BP Based On Sociodemographic Characteristics
Using univariate analysis, all sociodemographic characteristics except age and gender were significantly associated with low awareness (BP awareness score ≤12). In multivariate analysis adjusted for the significant variables in univariate analysis including marital status, nationality, educational level, career, health professional status, and monthly income, only career status and healthcare professional status were significantly associated with low awareness (Table 2). As indicated by adjusted odds ratios, students and healthcare professionals had significantly higher levels of awareness about BP (Table 2). Students earned significantly higher numbers of positive responses in seven items compared to the employed or unemployed participants. Three items were from the causes of BP: “Neurophysiologic or neurochemical imbalances,” “Medications,” and “Weak faith” (p-value <0.001, 0.005, and 0.013, respectively). The other four items were from the treatments of BP: “Psychiatric medications,” “Having an occasional alcoholic drink,” “Electroconvulsive therapy under psychiatrist supervision,” and “Hitting or choking by faith healer” (p-value <0.001, 0.049, <0.001, and 0.001, respectively). Healthcare professionals also showed significantly more positive responses on four items compared to non-healthcare professionals. “Neurophysiologic or neurochemical imbalances” and “Medications” were endorsed by 66.7% and 33.3% of healthcare professionals as causes of BP compared to 40.7% and 20.9% of non-healthcare professionals (p-value <0.001 and 0.023, respectively). “Psychiatric medications” and “Using brief counseling therapies” were endorsed by 62.5% and 55.6% of healthcare professionals as treatments for BP compared to 44.5% and 41.6% of non-healthcare professionals (p-value 0.005 and 0.030, respectively). In general, the level of awareness toward BP was not affected by the level of education. Nevertheless, compared with participants with lower education (high school or less), the participants with higher education (college and above) believed less that certain medical conditions may cause BP (22.3% versus 37.3%; p-value 0.003), believed more that certain medications may cause BP (25.7% versus 15.7%; p-value 0.039), and believed more that BP can be treated with psychiatric medications (50.7% versus 34.3%; p-value 0.004).
Attitudes And Beliefs About BP
For approaches to patients with BP, a substantial number (85.8%) believed that a person with BP can work effectively, 46.7% believed that patients with BP have to pull themselves together to get over it, and 31.8% considered it a shame to mention that someone in the family has BP. Regarding having a relationship with person with BP, 21.9% were not willing to maintain a friendship with someone with BP, 39.3% were not willing to marry a person who was previously diagnosed with BP, 19% were not willing to marry a person who has family members diagnosed with BP, and 16.8% would not consider telling their future spouse if they were diagnosed with BP (Table 4).
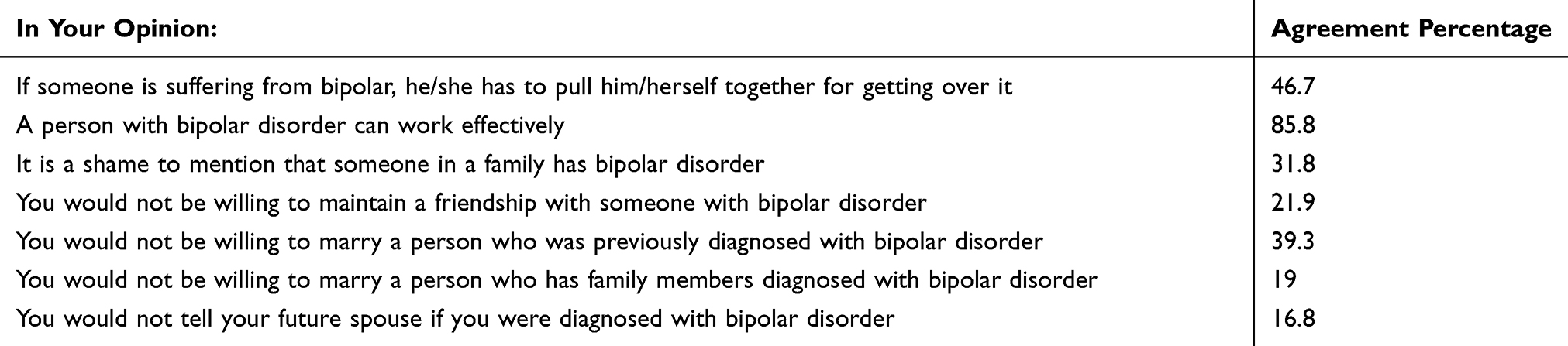 |
Table 4 Attitudes And Beliefs About Bipolar Disorder (N=416) |
Discussion
This study represents the first community-based survey of current public information, knowledge, beliefs, and attitudes toward BP in Saudi Arabia. This study showed that the internet and social media (35.4%) were major sources of information about BP, instead of clinics or hospitals (7%). This is not surprising as 77% of patients with BP reported using the internet to look up information about BP in an international multisite survey.22 Similarly, in the Arab world, there is a high interest in searching for online health information due to its fast and easy accessibility.23–25 However, the lack of reliable and credible Arabic online health information has led to improving the quality of the Arabic health web through launching the King Abdullah Bin Abdulaziz Arabic Health Encyclopedia website by the National Guard Health Affairs (NGHA), in collaboration with the Health On the Net Foundation (HON) and the World Health Organization (WHO). This Encyclopedia has multiple articles about mental health, including BP.26 Such certified websites need more advertisement on the internet to be used by the general population.
The causes of BP cited by the Saudi population in this study, in descending order, were: traumatic life event, unhealthy lifestyle, substance abuse, neurophysiological or neurochemical imbalance, and heredity or genetics. These results are similar to those found in the United Kingdom and France.6,8,9 On the other hand, the highly endorsed treatments for BP by the Saudi population were: psychiatric medications and brief counseling therapies, which are also similar to the United Kingdom and Spain.6,7,9
However, in our study, supernatural beliefs and weak faith were endorsed by half of the participants as causes of BP. Therefore, unsurprisingly, prayer and faith-healing were highly endorsed as a treatment for BP. Head bandaging by a traditional therapist was also a highly recognized treatment for BP. In this historical traditional method, a bandage is applied to the head, usually by wrap-around technique, that uses bony prominences as anchors or stays in order to treat mental illnesses.27 As per some traditional therapists’ claims, this will prevent any air from entering between the skin and the scalp which may cause headache and other neuropsychiatric and somatic complaints.28 Comparable findings from a study conducted in Saudi Arabia investigating the prevalence of psychiatric disorders among visitors to faith healers reported that 12.3% of participants attributed their psychiatric illnesses to evil eye, magic (5.5%), social and financial stress (16.5%), and 49.3% reported more than one of the aforementioned reasons. However, none of the participants attributed psychiatric illness to a biological reason. In the same study, the most commonly used treatment was the Holy Quran (95.9%) and using blessed water (71.3%).15 In an Egyptian study, 40.8% of the patients with BP sought traditional faith healers and, of those, 62.2% did so before seeking psychiatric services.13 Also, a study conducted in Sudan reported that 20.7% attributed their mental illness to jinn, 19.3% to Shiatan, 28.4% to evil spirits, and 43.7% to magic.14 The belief in supernatural causes could be explained by poor knowledge about psychiatric conditions, projections, and defense mechanisms from the patients and their relatives to blame their problem on an external influence (supernatural causes), to relieve their guilty feelings regarding their responsibility for their illness, and to avoid the stigma associated with mental disorders and psychiatric medications.17 As faith healers are highly appreciated and trusted by general population, we suggest to establish a mutually respectful relationship between mental health providers and faith healers, form a two-way dialogue to understand each other, in addition to licensing faith healers to formalize their practice, as well as educating them and promoting their training needs to recognize common psychiatric symptoms and refer in need patients to clinical care.15,17,29 These practitioners can also have a great impact on patients, so their role should not be neglected, and they should work in collaboration with the health mental system as per the WHO.30
In our study, we found that only 12.7% believe that ECT can treat BP despite it being a safe and highly effective tool to manage BP that is severe, treatment resistant, or occurs during pregnancy.31 Brief educational intervention has been found to improve ECT knowledge and attitudes toward ECT.32 Nevertheless, ECT, but not antidepressant medication utilization, is associated with global government expenditures on mental health. In Saudi Arabia, although the overall health budget has been increasing annually, there is still no independent budget for mental health.33
Although the mortality rate for serious mental illnesses, including BP, was not significantly associated with recreational activities,34 involvement in recreational activities was highly endorsed as a treatment for BP in our study. Also, almost half of the participants in our study believe that if someone has BP, he/she has to pull him/herself together to get over it. These results hint at the tendency of underestimating the seriousness of BP and blaming the patient for having the illness.
Adjusted estimates from our study showed that students and healthcare professionals had significantly higher awareness about BP, especially in terms of causes and treatments. Similar findings were reported by other studies that showed both psychiatrists and nurses had greater biopsychosocial understandings of mental illness than the lay public, likely from their training and experience.35 Another study showed that non-physician mental health clinicians were generally knowledgeable about BP but less knowledgeable about the pharmacotherapy for treating it.36 Also, a Saudi study found that males with lower levels of education and income were more likely to use faith-healing.37 It calls to attention the high rate of bachelor’s degrees in the sample (60%), which is comparable to the results of the demographic survey of Saudi Arabia that was done by the General Authority for Statistics in 2016, and showed that (52.7%) of Saudi population have high level of education (high school and above).38 The increased knowledge among students may be attributed to their frequent chatting, discussion, and file sharing on social network sites.39 These findings support the benefit of extending the training efforts of health clinicians (physician and non-physician)36 and of developing reliable information about BP for student and healthcare professionals on social networks using professional channels.
Although our study reflected the positive attitudes and beliefs about BP in terms of ability to work effectively (85.8%), a recent study conducted in Saudi Arabia on stigma in mood disorders found that 66% of people with BP were unemployed mainly due to psychiatric or medical problems.40 In the social domain, negative attitudes in our study included (in descending order): being unwilling to marry a person who was previously diagnosed with BP, considering it a shame to mention that someone in the family has BP, being unwilling to maintain a friendship with someone with BP, to marry a person who has family members diagnosed with BP, or to tell their future spouse if they were diagnosed with BP. These negative attitudes about marriage may be explained by believing in heredity or genetic causes of BP, which was endorsed by a third of the participants. Similarly, a previous qualitative research study in Saudi Arabia revealed that the widely held belief that psychiatric disorders were either hereditary or incurable was a reason behind their stigma. Other potential reasons for the stigma held by the Saudi community that may contribute to the negative attitudes found in our study include traditions, cultural norms, upbringing, lack of public awareness, and fear of aggression and violence from psychiatric patients (Koura et al, 2012). The experience of stigma in Saudi Arabia has affected patients with BP in terms of their quality of life (36%), ability to interact with family (24%), and ability to make or keep friends (20%). Patients with BP also think that the average person is afraid of someone with a serious mental illness (48%) and they try to avoid situations that may be stigmatizing (56%) (Alateeq et al, 2018). This may lead them to stop taking their medications prior to marriage – which is a stressful event – resulting in relapses during their honeymoon. Also, getting married in a conservative Islamic country like Saudi Arabia, where a man will usually marry a woman without a prior personal relationship, may lead people to not choose a future wife who has a psychiatric disorder. Eventually, this may contribute to a high rate of being spouseless among patients with psychiatric illnesses in Saudi Arabia.41 Moreover, higher levels of burden and depressed mood and lower levels of social support were associated with more perceived stigma among caregivers.42 Therefore, it is crucial to consider the caregivers of patients with BP in addition to the patients themselves.
Limitations
Although our study represents the first community-based survey of BP literacy among residents of the largest city in Saudi Arabia, we acknowledge a number of limitations. One of them is the convenient sampling of only one city in Saudi Arabia, which may limit generalizability of the study finding. Moreover, the cross-sectional design precludes making causal conclusions. Also, face validity was used as the main form of validity, which is a weak form of validity. It is subjective and cannot be quantified. Future studies should be longitudinal prospective ones, have a more representative samples, and use well-validated survey.
Conclusions
This study is the first national survey in Saudi Arabia to document some of the misconceptions in public information, knowledge, beliefs, and attitudes about BP. The internet and social media were the participant’s major sources of information, which highlights the need to support and improve the quality of and advertisement for Arabic online health information due to the fast and easily accessible nature of these sources. The impact of using social networking sites may also explain the high levels of awareness about BP’s causes and treatments among students and healthcare professions in addition to their training and experience. Although the general population showed positive responses about BP’s causes and treatments, supernatural beliefs are still predominant, which emphasizes the role of faith healers. Based on our findings, faith healers should be educated on the detection and treatment of mental diseases. When necessary, they can then refer patients to the mental health specialists and prevent any further delay in seeking help and appropriate treatment. Implementing a national community awareness program may raise the level of awareness through mass media communication strategies and schools’ curriculum resources.43–45 However, further studies are needed to investigate which potential public interventions will best improve the literacy of BP and other mental illnesses.
Acknowledgments
The authors would like to thank Dr. Mohammed Alangari and Dr. Abdulaziz Al-Muhanna for their great cooperation and participating in data collection. This research was funded by the Deanship of Scientific Research at Princess Nourah bint Abdulrahman University through the Fast-track Research Funding Program. The abstract of this study was presented as a poster in the 19th Annual Conference of the International Society for Bipolar Disorders, Washington DC, USA, and in the 25th European Congress of Psychiatry (EPA 2017), Florence, Italy. Mental health literacy in bipolar disorder: A cross-sectional survey in Saudi Arabia. Alosaimi F, et al. European Psychiatry, Volume 41, S418.
Disclosure
The authors report no conflicts of interest in this work.
References
1. WHO. Mental Disorders. WHO. 2017.
2. Merikangas KR, Akiskal HS, Angst J, et al. Lifetime and 12-month prevalence of bipolar spectrum disorder in the national comorbidity survey replication. Arch Gen Psychiatry. 2007;64(5):543–552. doi:10.1001/archpsyc.64.5.543
3. Ferrari AJ, Stockings E, Khoo JP, et al. The prevalence and burden of bipolar disorder: findings from the Global Burden of Disease Study 2013. Bipolar Disord. 2016;18(5):440–450. doi:10.1111/bdi.12423
4. Pompili M. Impact of living with bipolar patients: making sense of caregivers’ burden. World J Psychiatry. 2014;4(1):1. doi:10.5498/wjp.v4.i1.1
5. Jorm AF, Barney LJ, Christensen H, Highet NJ, Kelly CM, Kitchener BA. Research on mental health literacy: what we know and what we still need to know. Aust N Z J Psychiatry. 2006;40(1):3–5. doi:10.1111/j.1440-1614.2006.01734.x
6. Furnham A, Anthony E. Lay theories of bipolar disorder: the causes, manifestations and cures for perceived bipolar disorder. Int J Soc Psychiatry. 2010;56(3):255–269. doi:10.1177/0020764008095173
7. Ruiz MÁ, Montes JM, Correas Lauffer J, Álvarez C, Mauriño J, De Dios Perrino C. Opiniones y creencias sobre las enfermedades mentales graves (esquizofrenia y trastorno bipolar) en la sociedad española Opinions and beliefs of the. Rev Psiquiatr Salud Ment. 2012;5(2):98–106. doi:10.1016/j.rpsm.2012.01.002
8. Durand-Zaleski I, Scott J, Rouillon F, Leboyer M. A first national survey of knowledge, attitudes and behaviours towards schizophrenia, bipolar disorders and autism in France. BMC Psychiatry. 2012;12(1):128. doi:10.1186/1471-244X-12-128
9. Ellison N, Mason O, Scior K. Public beliefs about and attitudes towards bipolar disorder: testing theory based models of stigma. J Affect Disord. 2015;175:116–123. doi:10.1016/j.jad.2014.12.047
10. Shahrour TM, Rehmani RS. Testing psychiatric stigma in a general hospital in Saudi Arabia. Saudi Med J. 2009;30(10):1336–1339.
11. Alhamad AM, Al-Sawaf MH, Osman AA, Ibrahim IS. Differential aspects of consultation-liaison psychiatry in a Saudi hospital. II: knowledge and attitudes of physicians and patients. East Mediterr Heal J. 2006;12(3–4):324–330.
12. Koura M, Al-Dabal B, Al-Sowielem L. Qualitative research: stigma associated with psychiatric diseases. World Fam Med J Inc Middle East J Fam Med. 2012;10(6):44–47.
13. Assad T, Okasha T, Ramy H, et al. Role of traditional healers in the pathway to care of patients with bipolar disorder in Egypt. Int J Soc Psychiatry. 2015;61(6):583–590. doi:10.1177/0020764014565799
14. Sorketti EA, Zainal NZ, Habil MH. The characteristics of people with mental illness who are under treatment in traditional healer centres in Sudan. Int J Soc Psychiatry. 2012;58(2):204–216. doi:10.1177/0020764010390439
15. Alosaimi FD, Alshehri Y, Alfraih I, et al. Prevalence of psychiatric disorders among visitors to faith healers in Saudi Arabia. Pakistan J Med Sci. 2014;30(5):1077–1082. doi:10.12669/pjms.305.5434
16. Abdullah EK. Possession: is it real or fancy? Arab J Psychiatry. 1998;9(2):99–108.
17. Alsughayir MA. Public view of the “evil eye” and its role in psychiatry: a study in Saudi society. Arab J Psychiatry. 1996;7(2):152–160.
18. Siddiqui AR, Mahasin S, Alsajjan R, et al. Depression literacy in women attending university hospital clinics in Riyadh Saudi Arabia. Int J Soc Psychiatry. 2017;63(2):99–108. doi:10.1177/0020764016685346
19. Mansour A. High schoolers’ knowledge and attitudes about schizophrenia in Saudi Arabia. Alexandria Bull. 2008;44(3):316–319.
20. Bener A, Ghuloum S. Ethnic differences in the knowledge, attitude and beliefs towards mental illness in a traditional fast developing country. Psychiatr Danub. 2011;23(2):157–164. doi:10.1016/S0924-9338%2810%2971498-X
21. Bener A, Ghuloum S. Gender differences in the knowledge, attitude and practice towards mental health illness in a rapidly developing Arab society. Int J Soc Psychiatry. 2011;57(5):480–486. doi:10.1177/0020764010374415
22. Conell J, Bauer R, Glenn T, et al. Online information seeking by patients with bipolar disorder: results from an international multisite survey. Int J Bipolar Disord. 2016;4(1):17. doi:10.1186/s40345-016-0058-0
23. Abanmy NO, Al-Quait NA, Alami AH, Al-Juhani MH, Al-Aqeel S. The utilization of Arabic online drug information among adults in Saudi Arabia. Saudi Pharm J. 2012;20(4):317–321. doi:10.1016/j.jsps.2012.07.001
24. Buhi ER, Daley EM, Oberne A, Smith SA, Schneider T, Fuhrmann HJ. Quality and accuracy of sexual health information web sites visited by young people. J Adolesc Heal. 2010;47(2):206–208. doi:10.1016/j.jadohealth.2010.01.002
25. Bahkali S, Almaiman R, El-Awad M, Almohanna H, Khaled Al-Surimi MH. Exploring the impact of information seeking behaviors of online health consumers in the Arab World. Stud Health Technol Inform. 2016;226:279–282. doi:10.3233/978-1-61499-664-4-279
26. Altuwaijri MM. Empowering patients and health professionals in the Arab world: the King Abdullah bin Abdulaziz Arabic health encyclopedia on the web. Yearb Med Inform. 2011;6(1):125–130.
27. Dols MW. The treatment of the insane. J Muslim Ment Health. 2006;1(2):185–203. doi:10.1080/15564900600980830
28. Alwardani A. What are the symptoms of head air? Comprehensive Arabic encyclopedia, alternative and natural medicine.
29. Musyimi CW, Mutiso VN, Nandoya ES, Ndetei DM. Forming a joint dialogue among faith healers, traditional healers and formal health workers in mental health in a Kenyan setting: towards common grounds. J Ethnobiol Ethnomed. 2016;12(4):1–8. doi:10.1186/s13002-015-0075-6
30. Al-Rowais N, Al-Faris E, Mohammad AG, Al-Rukban M, Abdulghani HM. Traditional healers in Riyadh region: reasons and health problems for seeking their advice. A household survey. J Altern Complement Med. 2010;16(2):199–204. doi:10.1089/acm.2009.0283
31. Goodwin GM, Haddad PM, Ferrier IN, et al. Evidence-based guidelines for treating bipolar disorder: revised third edition recommendations from the British Association for Psychopharmacology. J Psychopharmacol. 2016;30(6):495–553. doi:10.1177/0269881116636545
32. Hoffman GA, McLellan J, Hoogendoorn V, Beck AW. Electroconvulsive therapy: the impact of a brief educational intervention on public knowledge and attitudes. Int Q Community Health Educ. 2018;38(2):129–136. doi:10.1177/0272684X17749939
33. Koenig HG, Al ZF, Sehlo MG, et al. Mental health care in Saudi Arabia : past, present and future. Open J Psychiatry. 2014;4(2):113–130. doi:10.4236/ojpsych.2014.42016
34. Hayes RD, Chang C-K, Fernandes AC, et al. Functional status and all-cause mortality in serious mental illness. PLoS One. 2012;7(9):e44613. doi:10.1371/journal.pone.0044613
35. Sun B, Fan N, Nie S, et al. Attitudes Towards People with Mental Illness among Psychiatrists, Psychiatric Nurses, Involved Family Members and the General Population in a Large City in Guangzhou, China. International Journal of Mental Health Systems. 2014:1–7.
36. Stein BD, Celedonia KL, Swartz HA, Burns RM, Sorbero MJ, Brindley RAFE. Psychosocial treatment of bipolar disorders: clinician knowledge, common approaches, and barriers to effective treatment. Psychiatr Serv. 2015;66(12):1361–1364. doi:10.1176/appi.ps.201400004.Psychosocial
37. Alosaimi FD, Alshehri Y, Alfraih I, et al. Psychosocial correlates of using faith healing services in Riyadh, Saudi Arabia: a comparative cross-sectional study. Int J Ment Health Syst. 2015;9(1):8. doi:10.1186/1752-4458-9-8
38. Demography Survey 2016. General Authority for statistics. 2016. Available from: https://www.stats.gov.sa/sites/default/files/en-demographic-research-2016_2.pdf.
39. Eid MIM, Al-jabri IM. Social networking, knowledge sharing, and student learning: the case of university students. Comput Educ. 2016;99:14–27. doi:10.1016/j.compedu.2016.04.007
40. Alateeq D, Aldaoud A, Alhadi A, Alkhalaf H, Milev R. The experience and impact of stigma in Saudi people with a mood disorder. Ann Gen Psychiatry. 2018;17(51):1–9. doi:10.1186/s12991-018-0221-3
41. Alosaimi FD, Alzain N, Asiri S, et al. Patterns of psychiatric diagnoses in inpatient and outpatient psychiatric settings in Saudi Arabia. Arch Clin Psychiatry. 2017;44(3):77–83. doi:10.1590/0101-60830000000124
42. Gonzalez JM, Perlick DA, Miklowitz DJ, et al. Factors associated with stigma among caregivers of patients with bipolar disorder in the STEP-BD study. Psychiatr Serv. 2007;58(1):41–48. doi:10.1176/ps.2007.58.1.41
43. Salerno JP. Effectiveness of universal school-based youth in the United States: a systematic abstract. J Sch Health. 2016;86:12. doi:10.1111/josh.12461
44. Petersen I, Lacko SE, Semrau M, et al. Promotion, prevention and protection: interventions at the population – and community – levels for mental, neurological and substance use disorders in low- and middle-income countries. Int J Ment Health Syst. 2016:1–13. doi:10.1186/s13033-016-0060-z
45. Sontag-padilla L, Dunbar M, Ye F, et al. Strengthening college students’ mental health knowledge, awareness, and helping behaviors: the impact of active minds, a peer mental health organization. J Am Acad Child Adolesc Psychiatry. 2018;(May):1–8. doi:10.1016/j.jaac.2018.03.019
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.