")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 14
Psychotropic drug therapy in patients in the intensive care unit - usage, adverse effects and drug interactions: a review
Authors Shafiekhani M , Mirjalili M , Vazin A
Received 1 June 2018
Accepted for publication 2 August 2018
Published 28 September 2018 Volume 2018:14 Pages 1799—1812
DOI https://doi.org/10.2147/TCRM.S176079
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Mojtaba Shafiekhani, Mahtabalsadat Mirjalili, Afsaneh Vazin
Department of Clinical Pharmacy, Faculty of Pharmacy, Shiraz University of Medical Sciences, Shiraz, Iran
Abstract: Managing psychological problems in patients admitted to intensive care unit (ICU) is a big challenge, requiring pharmacological interventions. On the other hand, these patients are more prone to side effects and drug interactions associated with psychotropic drugs use. Benzodiazepines (BZDs), antidepressants, and antipsychotics are commonly used in critically ill patients. Therefore, their therapeutic effects and adverse events are discussed in this study. Different studies have shown that non-BZD drugs are preferred to BZDs for agitation and pain management, but antipsychotic agents are not recommended. Also, it is better not to start antidepressants until the patient has fully recovered. However, further investigations are required for the use of psychotropic drugs in ICUs.
Keywords: critical care, delirium, sedation, antipsychotics, benzodiazepines
Introduction
Comorbidities are prevalent among critically ill patients admitted to intensive care units (ICUs), and several pharmacological and non-pharmacological treatments are usually required to manage these complications.1 One of the most important issues is to manage psychiatric complications that can be accomplished by pharmacological interventions.2 According to Gilbert et al study, agitation and delirium occur in 60% and 80% of patients in the ICU, respectively, and there is a direct relationship between the incidence of these complications with mortality rate, duration of mechanical ventilation, and medical costs.3
The need for appropriate sedative drugs in these patients as well as managing multiple psychiatric disturbances, including insomnia, pain, agitation, and delirium have caused unavoidable administration of a wide range of psychotropic agents in this ward.3 Treating agitation and delirium even gets more difficult in patients with drug abuse who develop withdrawal symptoms on abstinence from the drug.4 At the same time, psychotropic drugs should be carefully selected, since patients are at high risk of adverse drug–drug interactions. In this respect, we can mention several adverse events like arrhythmias, extrapyramidal symptoms (EPS), and even increased mortality rate due to inappropriate use of drugs or drug–drug interactions.5,6
This review article describes and compares pharmacological properties, clinical indications, and adverse drug effects of commonly used psychotropic drugs in ICUs, including benzodiazepines (BZDs), antidepressants, antipsychotics, and some other sedative agents.
BZDs
Pharmacology
BZDs are generally administered for critically ill patients to manage agitation.2 The proportion of gamma-Aminobutyric acid (GABA) receptors interacting with BZDs is responsible for the wide range of clinical effects: 20%, 30%–50%, and at least 60% interaction cause anxiolysis, sedation, and hypnosis, respectively.7 Different pharmacological and pharmacokinetic properties of BZDs are shown in Table 1.8–11
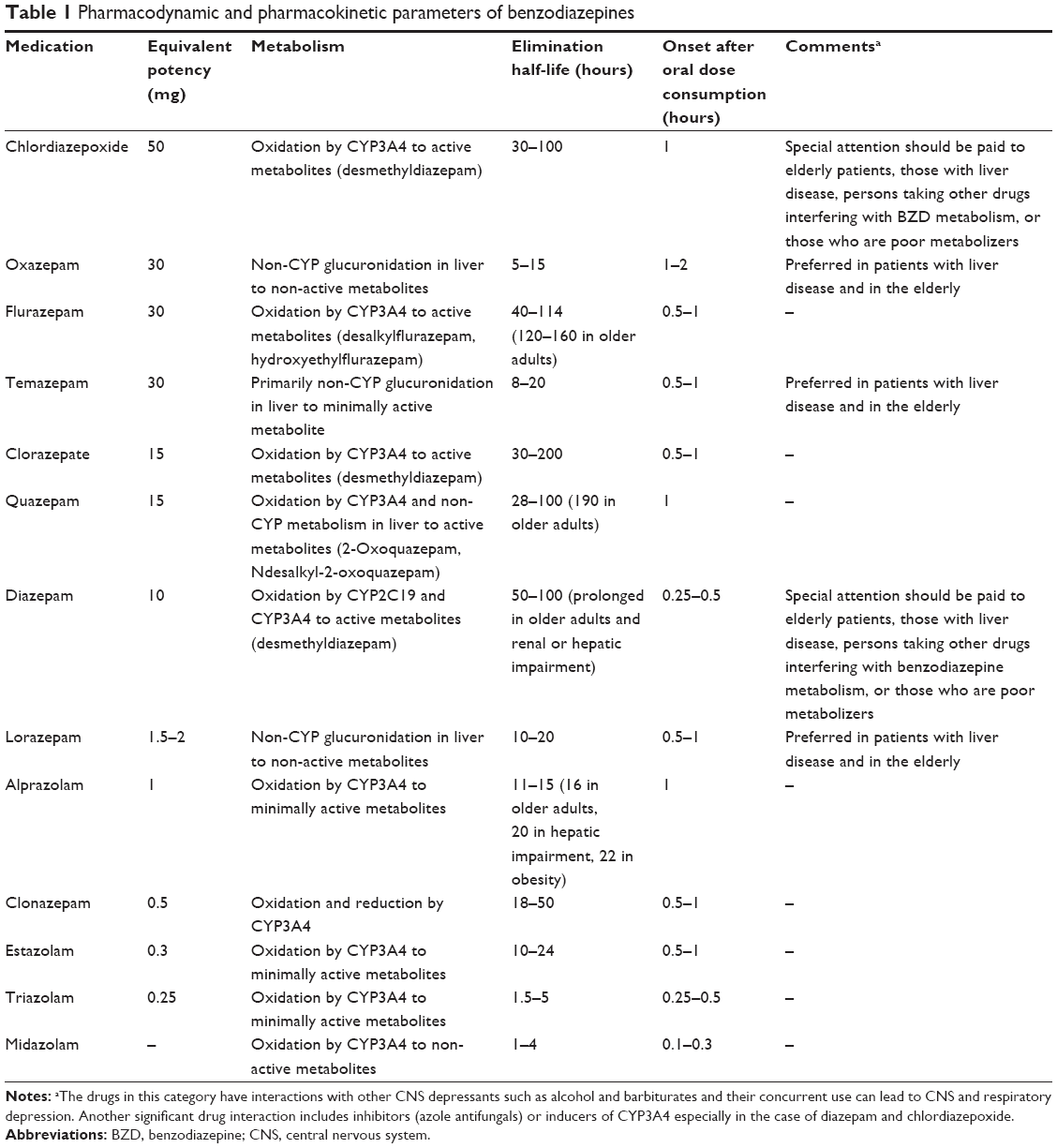 | Table 1 Pharmacodynamic and pharmacokinetic parameters of benzodiazepines |
Clinical indications
BZDs are generally administered for critically ill patients, not only to achieve a state of deep sedation and amnesia but even in the case of a need for an anxiolytic effect. BZDs have hypnotic, anticonvulsant, and muscle relaxant effects that may be desirable in selected ICU patients.12
Midazolam and lorazepam are common BZDs that are best suited for sedation in the ICUs due to the possibility of intermittent or continuous infusion administration, and having short duration of action. Since diazepam cannot be administered by continuous infusion, it is not a suitable choice for sedation. Midazolam and diazepam are more lipid soluble than lorazepam; therefore, they have faster onset of action (2–5 minutes vs 5–20 minutes) following intravenous (IV) infusion and larger volume of distribution.13 Consequently, more attention should be given to the accumulation of midazolam active metabolites, especially in obese and elderly patients by continuous infusion.14
Several studies have compared continuous infusion of midazolam vs lorazepam for sedating critically ill patients, which mostly concluded that midazolam is the preferred choice for short-term sedation, while lorazepam is suggested for long-term sedation.15,16
Adverse effects
The incidence of adverse drug events associated with BZDs, such as respiratory suppression, reduced blood pressure, and delirium, especially in combination with opioids,17 undermine the usage of these drugs for sedation.18,19 According to a study, nearly 80% of critically ill patients receiving mechanical ventilation experience delirium, which costs 4–16 billion USD in the USA.20 So far, different causes have been identified for delirium in ICU, including use of sedatives, especially BZDs and prolonged physical immobilty.2 Long-term BZD usage and their abrupt discontinuation lead to withdrawal syndrome with symptoms including agitation, anxiety, insomnia, and hyperactive delirium.21
It is worth mentioning that special care should be given to patients receiving prolonged and continuous infusion of lorazepam since there is high risk of poisoning with the solvent of these drugs, propylene glycol, which is characterized by metabolic acidosis with high anion gap and renal dysfunction.22,23
Conclusion
Due to risk of delirium associated with BZDs and its role on prolonging ICU length of stay, the 2013 Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit suggest a non-BZD agent for sedation in critically ill patients.16
Antipsychotics
Pharmacology
There are two main types of antipsychotics according to their mechanism of action: first generation, typical or conventional antipsychotics; and second generation or atypical ones.24
First-generation antipsychotics have high affinity for dopamine (D2) receptors, while the second generation are known as serotonin receptors antagonists (5HT2A).24 Drugs in these two categories differ from one other in some pharmacologic properties, and their affinity to different receptors as shown in Table 2.25–27
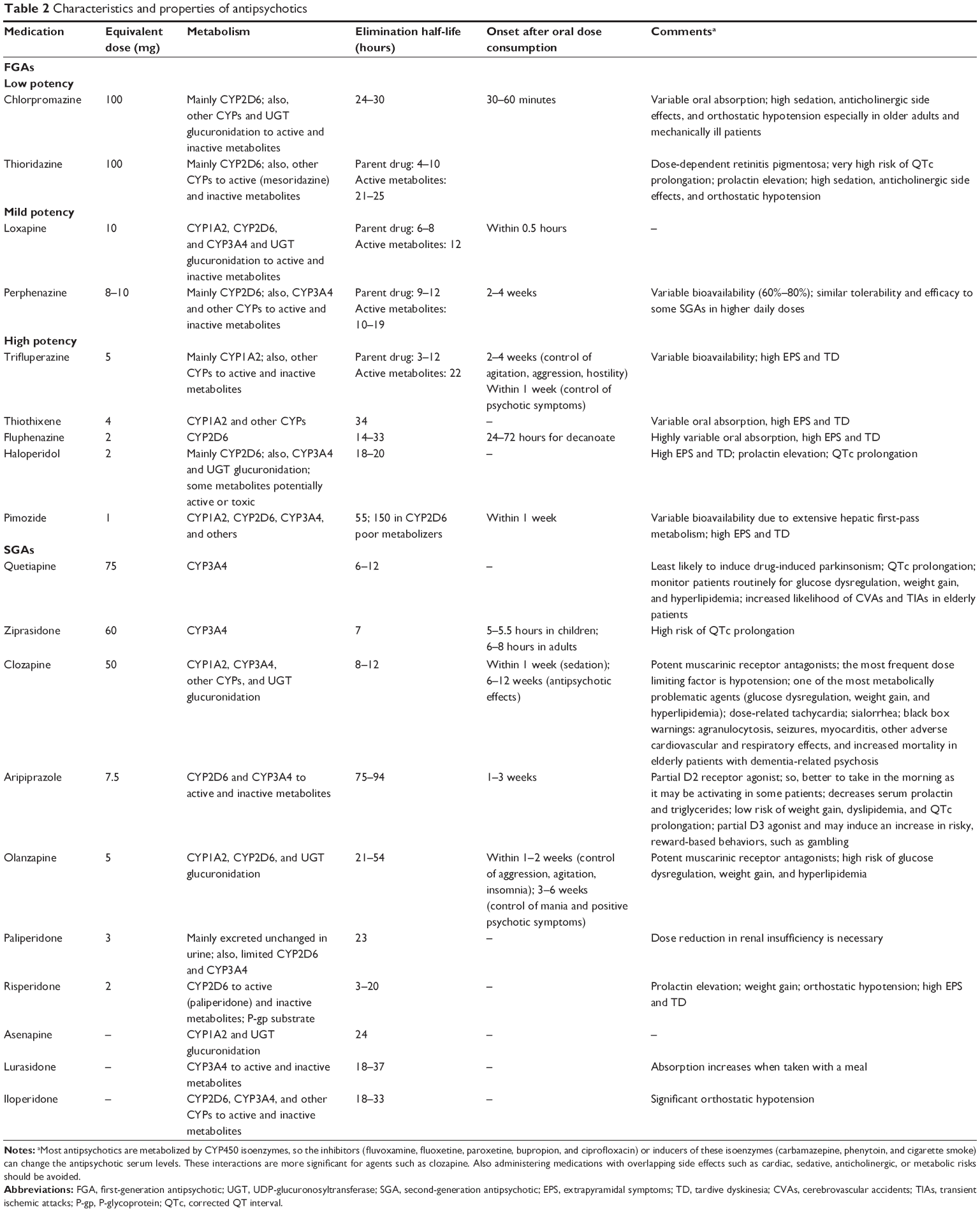 | Table 2 Characteristics and properties of antipsychotics |
Clinical indications
Antipsychotics are mainly used to treat schizophrenia and other psychotic disorders.28 Managing acute agitation and delirium in ICU is one of the most important indications of these drugs.29
Several studies on the effectiveness of Haloperidol injection to treat hyperactive delirium were published in recent years.30 Due to high risk of EPS associated with haloperidol, other typical antipsychotic drugs of this category such as chlorpromazine were studied. Then, different studies were conducted on the efficacy of atypical antipsychotics including quetiapine, olanzapine, and risperidone, but results failed to show the superiority of one of these drugs in treating delirium.31,32
For instance, in one study that evaluated the effect of low-dose haloperidol in comparison with atypical antipsychotics, such as olanzapine and risperidone, no significant difference was observed. However, the incidence of adverse effects including EPS was higher in patients receiving haloperidol. Although atypical antipsychotic agents are not superior to haloperidol, it is suggested to administer these drugs due to their less adverse effects. This is suggested for patients receiving high-dose haloperidol (>4.5 mg/day) for treating delirium, but we should also consider that these drugs are more expensive.31 In recent years, studies on control and prevention of delirium in critically ill patients could not prove the efficacy and safety of antipsychotic agents.
Antipsychotics treatment duration and appropriate time to discontinue these drugs were other important issues, considered in some studies. For example, in the Modifying the Incidence of Delirium trial, all the patients received their antipsychotic agents, and these drugs were discontinued when patients were delirium-free for 48 hours, but this study did not find a direct relationship between treatment with antipsychotics and duration of delirium.31 The significance of this issue is lack of timely drug discontinuation and even if patient is discharged with these drugs, it would lead to drug interaction due to unnecessary antipsychotic agents in drug regimen of polypharmacy patients, as well as increasing medical costs. Jasiak et al study estimated that cost of continued unnecessary treatment with atypical antipsychotic medication was 2,255.35 USD.33 In another study, it was shown that patients receiving BZDs for a longer period in ICU were more likely to be discharged with a new antipsychotic agent, which could cause higher rate of adverse drug reactions (ADRs) in polypharmacy patients.34
Adverse effects
First-generation drugs are more likely to produce EPS due to more potent inhibition of D2 receptors. The EPS side effects mostly occur when the patient is taking high dosage of typical antipsychotics. Those symptoms include akathisia, acute dystonic reaction (more often in young male patients), parkinsonism (more in old females), and tardive dyskinesia (in patients who receive first-generation antipsychotic for a long period of time).35 Also, low potent first-generation drugs such as chlorpromazine and thioridazine have more anticholinergic effects than the high potent ones including haloperidol, fluphenazine, and trifluoperazine. Accordingly, clozapine and olanzapine as second-generation drugs have the most anticholinergic and sedative effects.36 Hence, special attention should be given to these pharmacologic differences and side effects when selecting a drug from this category.
In a prospective study in 2016, it was observed that 18% of patients with delirium who were receiving antipsychotics experienced ADRs, half of which were severe or harmful including corrected QT interval (QTc) prolongation (10%), drowsiness (20%), ventricular tachycardia (10%), fever (10%), and neutropenia (10%). Severe and harmful adverse reactions were mainly observed in receiving first-generation antipsychotic drugs.6
Also, in one study that evaluated the incidence of QTc prolongation in critically ill patients, haloperidol, amiodarone, and levofloxacin were among the main causes of QTc prolongation.5 Furthermore, the most common drug interactions leading to QTc prolongation, haloperidol, was among the first five frequently prescribed drugs in patients.3
One concerning issue is the incidence of torsades de pointes in patients receiving antipsychotics, especially patients with risk factors such as hypokalemia and hypomagnesemia.37 However, this risk was higher in patients receiving IV haloperidol; some torsades de point cases were reported due to the use of atypical antipsychotics, such as ziprasidone and risperidone.38 Even though there are not ample amount of evidence, related mortality and morbidity are significant and should be considered when administering these drugs.
The incidence of ADRs and drug interactions with typical antipsychotics, particularly haloperidol which is commonly administered in the ICUs, led to use of atypical antipsychotics.
A multicenter prospective study was conducted to evaluate the efficacy and safety of treatment with quetiapine in critically ill patients. Shorter delirium duration, less agitation, and reduced need to haloperidol was observed among patients receiving quetiapine (50 mg by mouth (PO) every 12 hours which was increased every 24 hours up to 200 mg every 12 hours) in comparison with placebo, but there was no significant difference in the incidence of QTc prolongation and EPS.32
In one study, acute hyperglycemia independent from other glucose elevation factors in patients treated with quetiapine was considered as an adverse effect.39
Conclusion
Although typical antipsychotics such as haloperidol have been extensively used to prevent delirium, it seems that the data for using atypical antipsychotic agents are promising. In summary, according to what was mentioned so far in terms of efficacy and safety of antipsychotics in clinical practice guideline for managing delirium in ICUs (2013), atypical antipsychotics are not recommended to prevent delirium (level of recommendation: −2C).16
Antidepressants
Pharmacology
Selective serotonin reuptake inhibitors (SSRIs) selectively block the reuptake of serotonin at presynaptic neuronal junction, while selective serotonin–norepinephrine reuptake inhibitors (SNRIs) inhibit the reuptake of both norepinephrine and serotonin.40 Different pharmacologic and pharmacokinetic properties of these drugs are shown in Table 3.27,41–45
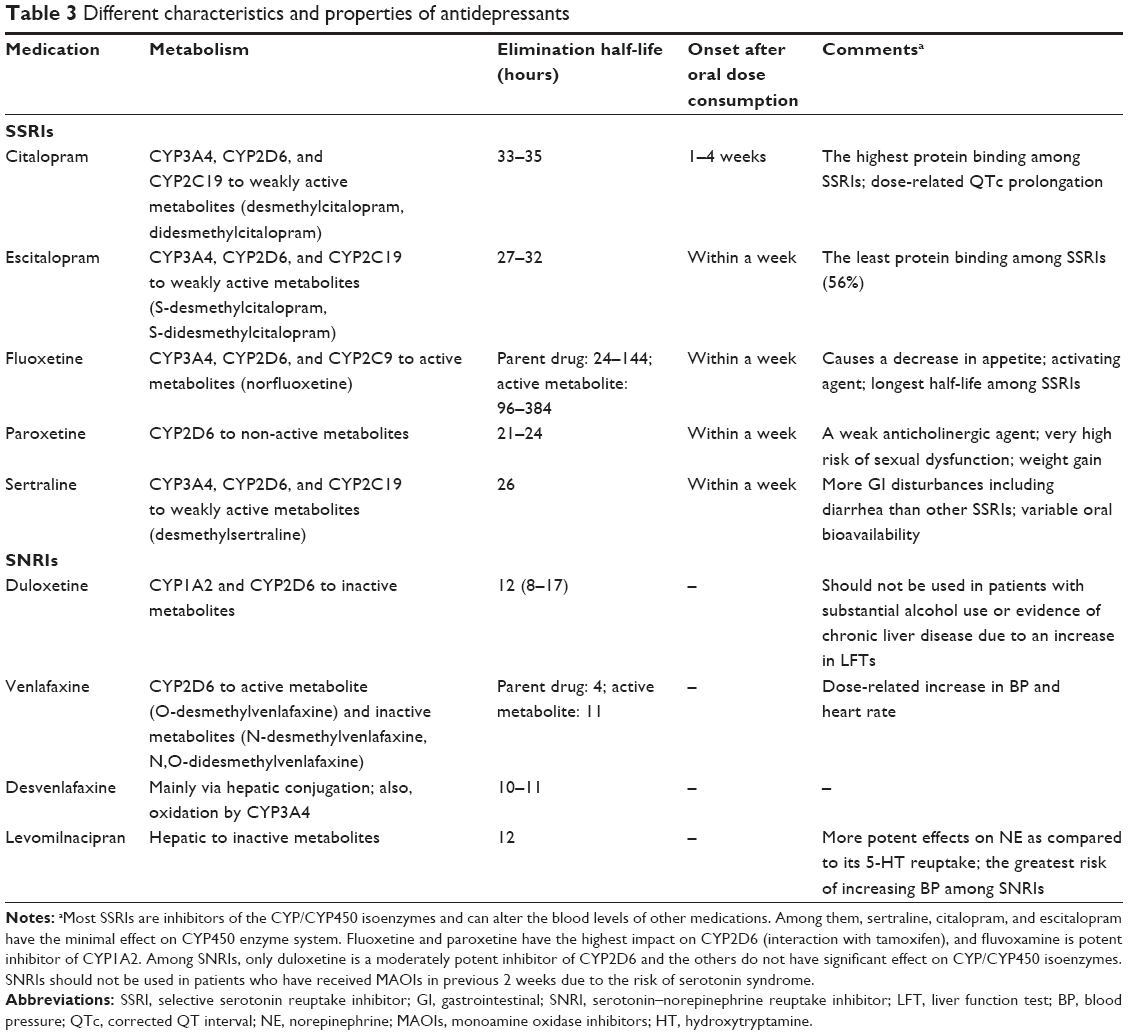 | Table 3 Different characteristics and properties of antidepressants |
Clinical indications
Antidepressants have been approved for some conditions such as depression, anxiety, neuropathic pains, and fibromyalgia; their use is often limited in ICU.40 Nearly 17% of patients in ICU have SSRI or SNRI in their medication history list on admission.46 Therefore, with regard to the increasing consumption of these drugs, continuation of taking these medications during admission is an important issue. Abrupt discontinuation of SSRI/SNRI drugs can lead to withdrawal syndrome in critically ill patients, attenuate the patient’s psychiatric condition like depression, and have a negative impact on the patient’s recovery in critically ill settings.47 Several points should be considered regarding continuation or initiating of SSRI/SNRI therapy which are described in the next section.
Adverse effects
Due to the effect of serotonin inhibitors on platelet functions, special attention should be given to upper gastrointestinal and preoperative bleeding.48,49 Risk of bleeding increases, especially when used concurrently with antiplatelet agents and common anticoagulants like aspirin or warfarin.49 On the other hand, drugs affecting serotonin reuptake are considered as a factor causing or exacerbating delirium in critically ill patients.50
Serotonin syndrome is one of the important ADRs associated with the use of drugs affecting serotonin reuptake, caused by excessive activation of postsynaptic serotonin receptors.51 This syndrome’s manifestation, such as altered mental status, neuromuscular irritability and autonomic instability are due to its impact on central nervous system (CNS).52 In one study, the incidence of this adverse reaction in ICU was estimated to be 39%.53 This syndrome can occur due to overdose with single serotonin agents, but most of the severe cases are because of interaction between two or more drugs increasing serotonin transmission. Drugs that so have shown to interact with SSRI/SNRI agents and can cause serotonin syndrome include linezolid, meperidine, tramadol, and dextromethorphan.54,55
Another risk in using SSRI in ICUs is higher risk of vasospasm followed by aneurysmal subarachnoid hemorrhage, and current use of statins can increase the risk of this adverse effect.56
Other adverse effect of SNRI/SSRI use in ICU includes fever, known as drug fever.57
Conclusion
The response to the question whether SSRI/SNRI agents should be discontinued, tapered off, or be continued in critically ill patients requires further investigations. Kelly et al study indicated that it is better to hold these drugs in acutely critically ill patients and when they become stable, start them again after psychiatric consultation.46
Alpha2 agonists
Pharmacology
Alpha2 adrenergic stimulation leads to adenylate cyclase inhibition and subsequently a decrease in cyclic adenosine monophosphate (cAMP) production.58 Reduction of cAMP level and efflux of potassium through an activated channel causes hyperpolarization of excitable membranes that prevents neurons activation. Alpha2 adrenergic stimulation prevents calcium from entering the nerve terminals, responsible for exertion of a very powerful inhibition of adrenergic tone.59
Dexmedetomidine, clonidine, methyldopa, and guanabenz are examples of alpha2 receptor agonists. Among them, dexmedetomidine is commonly used for conscious sedation in critically ill patients. The characteristics of these drugs are shown in Table 4.16,26,60,61
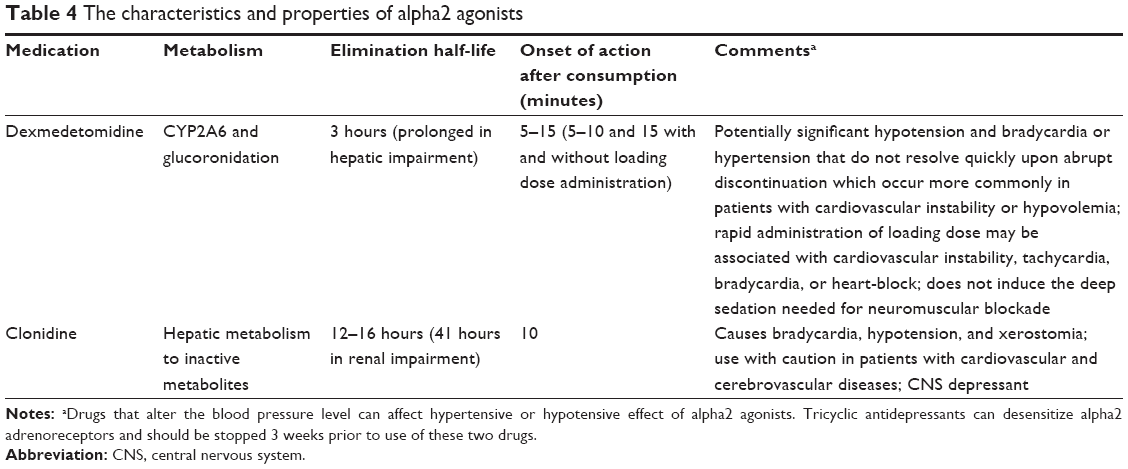 | Table 4 The characteristics and properties of alpha2 agonists |
Clinical indications
Alpha2 receptor agonist indication mainly depend on their effects in CNS. These effects include sedation, analgesia, anesthetic sparing, and sympatholytic properties.62
Clonidine is an imidazoline compound, which is a selective alpha-2-agonist with selective ratio of 200/1 for alpha2/alpha1.63 This drug is used in conditions such as high blood pressure, migraine, menopause flushing, and alcohol withdrawal syndrome.64,65 Clonidine has dose-related effects such as sedation, anxiolysis, and analgesia and can reduce the need for other anesthetic drugs and opioids in ICUs.66
Clonidine is an ideal agent for sedation in ICUs due to its minimal respiratory suppression and insignificant effects on respiratory rate, PaCO2, and SpO2.67,68 Nowadays in Europe, clonidine is one of the most popular drugs for sedation in ICUs.69
Dexmedetomidine is a newer and more selective alpha2 receptor agonist (with eight times more affinity to α2 receptors than clonidine) with sympatholytic, sedative, analgesic (opioid sparing), anxiolytic, and anesthetic drug-sparing effects and, of note, without respiratory depression.70–72 In clinical trials on dexmedetomidine, this drug showed to reduce the duration of mechanical ventilation in comparison with midazolam.73 Also, patients receiving dexmedetomidine were aroused more easily and had lower rates of postoperative delirium than those using propofol and midazolam.74
Dexmedetomidine is only used as IV infusion. All patients should be under continuous cardiac monitoring during treatment period. Also, non-mechanically ventilated patients should be monitored for respiration.75
Dexmedetomidine has a half-life of 2 hours. Its maximum dose is 1.4 μg/kg·hour, and due to transient hypertension, loading dose is not recommended.75 In the USA, dexmedetomidine is approved for infusion of up to 1 day only in mechanically ventilated patients. It is the only approved drug in the USA for inducing sedation in non-mechanically ventilated patients.76
According to a meta-analysis conducted in 2014, dexmedetomidine was associated with reduced incidence of delirium, agitation, confusion as well as shorter ICU stay, and extubation in comparison with other sedative agents.77
Considering its lack of effect on respiratory drive, being only available as IV formulation, requiring cardiovascular monitoring during infusion period and the high cost, researchers have attempted to develop strategies to switch from dexmedetomidine to enteral clonidine.78,79 In this regard, an observational pilot study was conducted on critically ill patients who had sustained agitation and were treated with dexmedetomidine to reach a Sedation Agitation Scale (SAS) score of 3–4.
If patients showed appropriate response (SAS: 3–4) between 12 and 24 hours, while being hemodynamic stable, dexmedetomidine would be switched to clonidine (0.2–0.5 mg every 6 hours PO). Finally, it was observed that the efficacy and safety of clonidine for sedation induction was not statistically different from dexmedetomidine, but this change from dexmedetomidine to oral clonidine could reduce drug cost 819–2,338 USD per patient within the 3 months of study period.80
Adverse effects
Bradycardia, hypotension, and xerostomia are considered as side effects of clonidine.81 These side effects, rebound hypertension and tachycardia following sudden cessation of clonidine after prolonged usage, have led to the development of other alpha2 agonists, such as dexmedetomidine.82 Hence, according to the latest guidelines in ICU settings, clonidine is considered as one of the agents for treating delirium and as second-line agent for inducing sedation.16
Dexmedetomidine causes dose-dependent bradycardia, hypertension, or hypotension. These effects are clinically relevant in those patients in whom hemodynamic conditions rely on augmented sympathetic stimulation and vasoconstriction, for example, those with fixed stroke volume and hypovolemic status, on rate-reducing drugs (beta blockers or digitalis).83 These side effects can be omitted by omitting loading dose or slowly incrementing infusion rate.
Conclusion
As mentioned before, according to Pain, Agitation, and Delirium management guideline which was released in 2013, it is recommended to use non-BZD strategies, such as dexmedetomidine instead of BZDs to prevent delirium. Also, dexmedetomidine is considered as an agent that can prevent delirium in ICU setting (level of recommendation: +2B).16
Others
Propofol and ketamine are sedative hypnotic drugs used for sedation in ICUs, but their usage is limited.84
Propofol
Pharmacology
It is a GABAergic IV anesthetic used to sedate the agitated critically ill patients.85 Propofol inhibits acetylcholine release in the hippocampus and prefrontal cortex through its effect on GABA receptors. It also acts through α2-adrenoreceptor and inhibits the N-Methyl-D-aspartate (NMDA) subtype of glutamate receptor. Propofol is not an analgesic agent. It has a potent antiemetic action, probably due to a decrease in serotonin levels through its action on GABA receptors in the area postrema.86–89 Table 5 shows pharmacokinetic and pharmacologic characteristics of propofol and ketamine.90,91
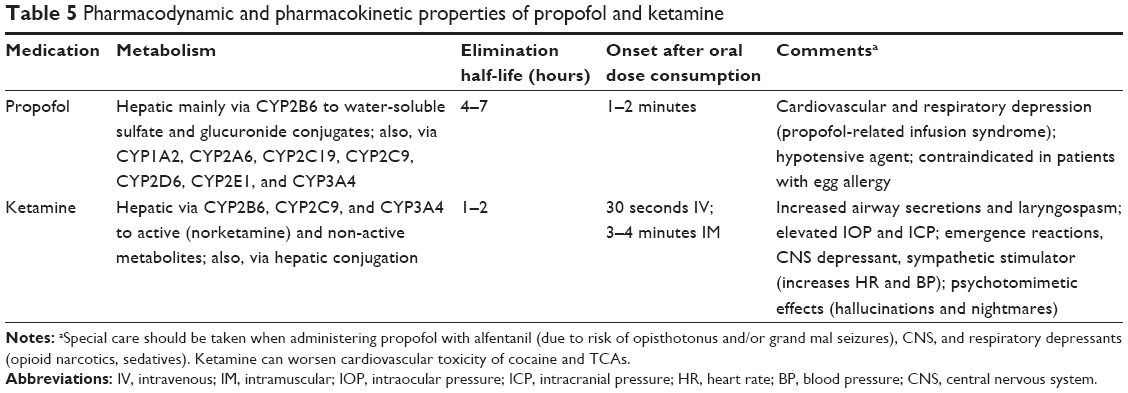 | Table 5 Pharmacodynamic and pharmacokinetic properties of propofol and ketamine |
Clinical indications
Propofol is considered as a drug of choice due to its rapid onset, rapid awakening, and antiemetic effects.92 In recent years, usage of this agent to induce and maintain sedation in critically ill patients has been controversial.
Many studies have evaluated and compared propofol with other sedative agents in terms of efficacy, safety, and inducing sedation. For example, in a retrospective study that compared propofol-based vs dexmedetomidine-based sedation in cardiac surgery patients, they concluded that patients sedated with dexmedetomidine were extubated faster than patients receiving propofol. Also, the length of hospital stay in dexmedetomidine-based group was shorter than propofol-based group.93 However, according to one review article published in the New England Journal of Medicine,94 there was no difference in the duration of mechanical ventilation and ICU stay between patients receiving propofol and dexmedetomidine.
In another meta-analysis study that evaluated the efficacy and harmful effect of propofol vs midazolam, they concluded that propofol was superior to midazolam for sedating mechanically ventilated critically ill patients.95
In a multicenter ICU database analysis that evaluated 3,000 patients admitted to an ICU, lower rate of mortality, shorter duration of mechanical ventilation, and earlier discharge were observed in patients receiving propofol infusions in comparison with those using lorazepam or midazolam.96 However, it seems that more data from comparative trials with current sedation guideline studies are required to confirm these results.
Adverse effects
The vasodilatory effect of this drug is responsible for severe hypotension in some patients, especially those with cardiac dysfunction or hemodynamic instability.97 When bolus injection of this drug is required, it should be infused according to the patient’s blood pressure.98 The incidence of hypertriglyceridemia is rare, but it mostly occurs with high propofol continuous infusion rate or when the patient is receiving parenteral nutrition formulations containing lipid.99 Especially this side effect should be considered in patients who are older and have a longer ICU stay which can be further complicated by the development of pancreatitis.100
Propofol-related infusion syndrome (PRIS) is an unusual and serious adverse effect of long-term propofol infusion. Its clinical symptoms include acute refractory bradycardia progressing to asystole, metabolic acidosis rhabdomyolysis of both skeletal and cardiac muscle, hyperlipidemia, and enlarged or fatty liver.101 It usually occurs with doses more than 67 μg/kg·min and infusions longer than 48 hours.102 Concurrent use of glucocorticoids, catecholamine infusion, high fat, and low carbohydrate intake are other risk factors for developing PRIS.103 The incidence of PRIS is <1%, but if it occurs, it has high mortality rate. Consequently, it is suggested to check triglyceride levels, serum lactate, and creatine kinase in patients receiving propofol. Hence, discontinuation of propofol and supportive care can treat PRIS.104
Conclusion
Altogether, the results of conducted studies on propofol show that this agent is favorable when rapid sedation and rapid awakening are desired; stopping the infusion can reverse the sedative effects, usually within 1 hour and often within 15 minutes but should pay attention to the patient’s hemodynamic condition and the incidence of adverse events.82,92
Ketamine
Pharmacology
Ketamine is an IV anesthetic which has been used since 1975 due to its different pharmacological properties, such as sedation, somatic analgesia, sympathetic nervous system stimulation, and bronchodilation.105 Ketamine is a phencyclidine derivative that competitively inhibits NMDA as well as sigma opioid receptors.106
Ketamine passes through blood–brain barrier very swiftly and its onset and duration are close to 1 and 10–15 minutes, respectively.107
Clinical indications
Induction of dissociative anesthesia in which the patient is nonresponsive to nociceptive stimulators, while the eyes are open and reflexes remain, is considered as a unique characteristic of ketamine.107 Due to sympathomimetic hemodynamic effects that can lead to vasoconstriction and positive inotropic actions, ketamine is an attractive choice for inducing sedation in sepsis.108 Thus, it seems to be a safer choice than midazolam, etomidate, and propofol for inducing sedation in septic shock among critically ill patients.109 Also, due to its bronchodilatory property, it is an appropriate choice for inducing sedation in asthma attacks and bronchoconstriction.110 Continuous infusion of ketamine and propofol can provide adequate and safe sedation for short time (<24 hours) in critically ill patients.111
In one study, it was stated that ketamine is a favorable choice in patients with intracranial hypertension who are under mechanical ventilation,112 but today it is believed that in patients with increased intracranial pressure (ICP), the depth of sedation is more important than selecting a sedative agent for managing these patients.113 In addition, it has been observed that low dose of ketamine (60–120 μg/kg·hour) with BZDs or particularly opioids can have beneficial effects for critically ill patients. The reason is as follows: the necessary effects of ketamine occur in lower doses in comparison with psychotropic effects. Thus, appropriate analgesic effects occur in lower doses without being concerned about its psychiatric adverse events, which is observed less frequently with BZDs and opioids.114 Unlike opioids that cause ileus, ketamine does not inhibit bowel motility, thus constipation occurs less frequently.115 Additionally, ketamine reduces opioid-induced hyperalgesia; hence, the patients require less dose of opioids.116
Adverse effects
Increase in saliva secretion is an adverse effect of ketamine, which might lead to laryngospasm, requiring suctions or premedication with atropine in patients under ventilation.117 However, psychoactive effects of ketamine (vivid hallucination, confusion, and delirium) have threatened its status as a safe sedative agent.118 On the other hand, due to the effect of ketamine on intraocular pressure, it is recommended to limit its usage in patients with open glaucome.119
Conclusion
According to the above-mentioned studies, ketamine is now considered as an agent for rapid sequence intubation (RSI), and we need more clinical studies to evaluate its safety in critically ill patients.
Summary
Controlling psychiatric problems in critically ill patients is an important issue. Their poor management can lead to attenuation of patients’ settings and affect their recovery. On the other hand, using psychotropic drugs might increase the risk of drug–drug interactions or ADRs. Therefore, selecting appropriate psychotropic drugs for critically ill patients is a crucial challenge.
Further studies are required on the efficacy and safety of psychotropic drugs, but the results of several studies have shown that it is better to use non-BZD drugs instead of BZDs to control agitation and pain. In this regard, cost is an important factor. The use of BZDs should be limited (as well as barbiturate) in patients with head trauma, intracranial hemorrhages, or epilepsy to prevent increase of ICP. If it is necessary to use BZDs, they should be given in the lowest possible dose for the shortest duration to prevent adverse effects.
Alpha2 agonists, such as dexmedetomidine are preferred over BZDs for inducing sedation, because they can prevent delirium in ICU setting.
Propofol has a rapid onset of action and recovery, but the incidence of adverse events is high. Ketamine is a favorable choice for RSI; however, it causes psychological complications in a dose-dependent manner.
Antipsychotic agents, either first generation or second generation, are not recommended, but it seems that atypical antipsychotics are associated with less ADRs when used to treat delirium. Nonetheless, special care should be given to patients prone to arrhythmias (ie, patients with history of arrhythmias and patients receiving proarrhythmogenic agent).
The use of antidepressants is often limited in ICU, and their administration is only recommended when the patients are in stable condition.
Acknowledgment
The authors wish to thank Mr H Argasi at the Research Consultation Center of Shiraz University of Medical Sciences for his invaluable assistance in editing this manuscript.
Author contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Hipp DM, Ely EW. Pharmacological and nonpharmacological management of delirium in critically ill patients. Neurotherapeutics. 2012;9(1):158–175. | ||
Reade MC, Finfer S. Sedation and delirium in the intensive care unit. N Engl J Med Overseas Ed. 2014;370(5):444–454. | ||
Gilbert B, Morales JR, Searcy RJ, Johnson DW, Ferreira JA. Evaluation of neuroleptic utilization in the intensive care unit during transitions of care. J Intensive Care Med. 2017;32(2):158–162. | ||
Sabetian G, Farid Z, Khalili F, et al. Implementation of a protocol to control pain, agitation and delirium in the patients admitted to intensive care unit with opioid drug dependency: A feasibility study. Biomed Res. 2017;28(8):3666–3671. | ||
Beitland S, Platou ES, Sunde K. Drug-induced long QT syndrome and fatal arrhythmias in the intensive care unit. Acta Anaesthesiol Scand. 2014;58(3):266–272. | ||
Hale GM, Kane-Gill SL, Groetzinger L, Smithburger PL. An evaluation of adverse drug reactions associated with antipsychotic use for the treatment of delirium in the intensive care unit. J Pharm Pract. 2016;29(4):355–360. | ||
Amrein R, Hetzel W, Hartmann D, Lorscheid T. Clinical pharmacology of flumazenil. Eur J Anaesthesiol Suppl. 1988;2:65–80. | ||
Davidson JR. Pharmacotherapy of generalized anxiety disorder. J Clin Psychiatry. 2001;62(Suppl 11):461–502. | ||
Offidani E, Guidi J, Tomba E, Fava GA. Efficacy and tolerability of benzodiazepines versus antidepressants in anxiety disorders: a systematic review and meta-analysis. Psychother Psychosom. 2013;82(6):355–362. | ||
Chouinard G, Lefko-Singh K, Teboul E. Metabolism of anxiolytics and hypnotics: benzodiazepines, buspirone, zoplicone, and zolpidem. Cell Mol Neurobiol. 1999;19(4):533–552. | ||
Bostwick JR, Gardner KN. Anxiety Disorder. Applied Therapeutics: The Clinical Use of Drugs. 11th ed. In: Koda-Kimble MA, Young LY, editors. Philadelphia: Lippincott Williams & Wilkins; 2018:1731–1862. | ||
Devlin JW, Roberts RJ. Pharmacology of commonly used analgesics and sedatives in the ICU: benzodiazepines, propofol, and opioids. Crit Care Clin. 2009;25(3):431–449. | ||
Swart EL, Zuideveld KP, de Jongh J, Danhof M, Thijs LG, Strack van Schijndel RM. Population pharmacodynamic modelling of lorazepam- and midazolam-induced sedation upon long-term continuous infusion in critically ill patients. Eur J Clin Pharmacol. 2006;62(3):185–194. | ||
Swart EL, Zuideveld KP, de Jongh J, Danhof M, Thijs LG, Strack van Schijndel RM. Comparative population pharmacokinetics of lorazepam and midazolam during long-term continuous infusion in critically ill patients. Br J Clin Pharmacol. 2004;57(2):135–145. | ||
Gommers D, Bakker J. Medications for analgesia and sedation in the intensive care unit: an overview. Critical Care. 2008;12(Suppl 3):S4. | ||
Barr J, Fraser GL, Puntillo K, et al. Clinical practice guidelines for the management of pain, agitation, and delirium in adult patients in the intensive care unit. Crit Care Med. 2013;41(1):263–306. | ||
Devlin JW, Roberts RJ. Pharmacology of commonly used analgesics and sedatives in the ICU: benzodiazepines, propofol, and opioids. Anesthesiol Clin. 2011;29(4):567–585. | ||
Thomason JWW, Shintani A, Peterson JF, Pun BT, Jackson JC, Ely EW. Intensive care unit delirium is an independent predictor of longer hospital stay: a prospective analysis of 261 non-ventilated patients. Critical Care. 2005;9(4):R375. | ||
Fraser GL, Devlin JW, Worby CP, et al. Benzodiazepine versus nonbenzodiazepine-based sedation for mechanically ventilated, critically ill adults: a systematic review and meta-analysis of randomized trials. Crit Care Med. 2013;41(9):S30–S38. | ||
Collinsworth AW. A Bundled Care Process For The Prevention Of Delirium In Patients In The Intensive Care Unit: Implementation Strategies And Uptake, Impact On Patient Outcomes, And Cost-effectiveness [dissertation]. New Orleans, LA: Tulane University; 2015. | ||
Awissi DK, Lebrun G, Fagnan M, Skrobik Y. Regroupement de Soins Critiques, Réseau de Soins Respiratoires, Québec, Critiques Rdes, Réseau de Soins Respiratoires, RdeS. Alcohol, nicotine, and iatrogenic withdrawals in the ICU. Crit Care Med. 2013;41(9 Suppl 1):S57–S68. | ||
Hansen L, Lange R, Gupta S. Development and evaluation of a guideline for monitoring propylene glycol toxicity in pediatric intensive care unit patients receiving continuous infusion lorazepam. J Pediatr Pharmacol Ther. 2015;20(5):367–372. | ||
Wilson KC, Reardon C, Theodore AC, Farber HW. Propylene glycol toxicity: a severe iatrogenic illness in ICU patients receiving IV benzodiazepines: a case series and prospective, observational pilot study. Chest. 2005;128(3):1674–1681. | ||
Leucht S, Corves C, Arbter D, Engel RR, Li C, Davis JM. Second-generation versus first-generation antipsychotic drugs for schizophrenia: a meta-analysis. Lancet. 2009;373(9657):31–41. | ||
Silvia RJ, Dufrense RL, Ellison JC. Schizophrenia. In: Koda-Kimble MA, Young LY, editors. Applied Therapeutics: The Clinical Use of Drugs. 11th ed. Philadelphia: Lippincott Williams & Wilkins; 2018:1780–1812. | ||
Lieberman JA, Stroup TS, Mcevoy JP, et al. Effectiveness of antipsychotic drugs in patients with chronic schizophrenia. N Engl J Med. 2005;353(12):1209–1223. | ||
By the American Geriatrics Society 2015 Beers Criteria Update Expert Panel. American Geriatrics Society 2015 Updated Beers Criteria for Potentially Inappropriate Medication Use in Older Adults. J Am Geriatr Soc. 2015;63(11):2227–2246. | ||
Miyamoto S, Duncan G, Marx C, Lieberman J. Treatments for schizophrenia: a critical review of pharmacology and mechanisms of action of antipsychotic drugs. Mol Psychiatry. 2005;10(1):79–104. | ||
Debiasi EM, Akgün KM, Pisani M, editors. Awake or Sedated: trends in the evaluation and management of agitation in the intensive care unit. Seminars in Respiratory and Critical Care Medicine. Stuttgart: Thieme Medical Publishers; 2015. | ||
Wang W, Li HL, Wang DX, et al. Haloperidol prophylaxis decreases delirium incidence in elderly patients after noncardiac surgery: a randomized controlled trial. Crit Care Med. 2012;40(3):731–739. | ||
Girard TD, Pandharipande PP, Carson SS, et al. Feasibility, efficacy, and safety of antipsychotics for intensive care unit delirium: the MIND randomized, placebo-controlled trial. Crit Care Med. 2010;38(2):428–437. | ||
Devlin JW, Roberts RJ, Fong JJ, et al. Efficacy and safety of quetiapine in critically ill patients with delirium: a prospective, multicenter, randomized, double-blind, placebo-controlled pilot study. Crit Care Med. 2010;38(2):419–427. | ||
Jasiak KD, Middleton EA, Camamo JM, Erstad BL, Snyder LS, Huckleberry YC. Evaluation of discontinuation of atypical antipsychotics prescribed for ICU delirium. J Pharm Pract. 2013;26(3):253–256. | ||
Rowe AS, Hamilton LA, Curtis RA, et al. Risk factors for discharge on a new antipsychotic medication after admission to an intensive care unit. J Crit Care. 2015;30(6):1283–1286. | ||
Frontera JA. Delirium and sedation in the ICU. Neurocrit Care. 2011;14(3):463–474. | ||
Peluso MJ, Lewis SW, Barnes TR, Jones PB. Extrapyramidal motor side-effects of first- and second-generation antipsychotic drugs. Br J Psychiatry. 2012;200(5):387–392. | ||
Wildstein S, Karim I, Goldin M. QTc Prolongation and Torsades de Pointes. In: Manu P, Suarez RE, Barnett BJ, editors. Handbook of Medicine in Psychiatry. Washington DC: American Psychiatric Pub; 2015:24. | ||
Hasnain M, Vieweg WV. QTc interval prolongation and torsade de pointes associated with second-generation antipsychotics and antidepressants: a comprehensive review. CNS Drugs. 2014;28(10):887–920. | ||
Bishara A, Phan SV, Young HN, Liao TV. Glucose disturbances and atypical antipsychotic use in the intensive care unit. J Pharm Pract. 2016;29(6):534–538. | ||
Lee YC, Chen PP. A review of SSRIs and SNRIs in neuropathic pain. Expert Opin Pharmacother. 2010;11(17):2813–2825. | ||
Nierenberg AA, Ostacher MJ, Huffman JC, Ametrano RM, Fava M, Perlis RH. A brief review of antidepressant efficacy, effectiveness, indications, and usage for major depressive disorder. J Occup Environ Med. 2008;50(4):428–436. | ||
Preskorn SH. Clinically relevant pharmacology of selective serotonin reuptake inhibitors. Clin Pharmacokinet. 1997;32(Supplement 1):1–21. | ||
Wynn G, Sandson EA. Psychiatry. In: Wynn GH, Oesterheld JR, Cozza KL, Armstrong SC, editors. Clinical Manual of Drug Interaction Principles for Medical Practice. American Psychiatric Publishing Inc.; 2009:423. | ||
Spina E, Trifirò G, Caraci F. Clinically significant drug interactions with newer antidepressants. CNS Drugs. 2012;26(1):39–67. | ||
Angelini MC. Depressive disorders. In: Koda-Kimble MA, Young LY, editors. Applied Therapeutics: The Clinical Use of Drugs. 11th ed. Philadelphia: Lippincott Williams & Wilkins; 2018:1813–1833. | ||
Kelly JM, Rubenfeld GD, Masson N, Min A, Adhikari NKJ. Using selective serotonin reuptake inhibitors and serotonin-norepinephrine reuptake inhibitors in critical care: a systematic review of the evidence for benefit or harm. Crit Care Med. 2017;45(6):e607–e616. | ||
Bienvenu OJ, Colantuoni E, Mendez-Tellez PA, et al. Depressive symptoms and impaired physical function after acute lung injury: a 2-year longitudinal study. Am J Respir Crit Care Med. 2012;185(5):517–524. | ||
Anglin R, Yuan Y, Moayyedi P, Tse F, Armstrong D, Leontiadis GI. Risk of upper gastrointestinal bleeding with selective serotonin reuptake inhibitors with or without concurrent nonsteroidal anti-inflammatory use: a systematic review and meta-analysis. Am J Gastroenterol. 2014;109(6):811–819. | ||
Mahdanian AA, Rej S, Bacon SL, Ozdin D, Lavoie KL, Looper K. Serotonergic antidepressants and perioperative bleeding risk: a systematic review. Expert Opin Drug Saf. 2014;13(6):1–10. | ||
Kogoj A. Selective serotonin reuptake inhibitors-induced delirium: a case review. Psychiatr Danub. 2014;26(3):0–280. | ||
Isbister GK, Buckley NA. The pathophysiology of serotonin toxicity in animals and humans: implications for diagnosis and treatment. Clin Neuropharmacol. 2005;28(5):205–214. | ||
Boyer EW, Shannon M. The Serotonin Syndrome. N Engl J Med Overseas Ed. 2005;352(11):1112–1120. | ||
Pedavally S, Fugate JE, Rabinstein AA. Serotonin syndrome in the intensive care unit: clinical presentations and precipitating medications. Neurocrit Care. 2014;21(1):108–113. | ||
Debellis RJ, Schaefer OP, Liquori M, Volturo GA. Linezolid-associated serotonin syndrome after concomitant treatment with citalopram and mirtazepine in a critically ill bone marrow transplant recipient. J Intensive Care Med. 2005;20(6):303–305. | ||
das PK, Warkentin DI, Hewko R, Forrest DL. Serotonin syndrome after concomitant treatment with linezolid and meperidine. Clin Infect Dis. 2008;46(2):264–265. | ||
Singhal AB, Topcuoglu MA, Dorer DJ, Ogilvy CS, Carter BS, Koroshetz WJ. SSRI and statin use increases the risk for vasospasm after subarachnoid hemorrhage. Neurology. 2005;64(6):1008–1013. | ||
Kam PC, Chang GW. Selective serotonin reuptake inhibitors. Pharmacology and clinical implications in anaesthesia and critical care medicine. Anaesthesia. 1997;52(10):982–988. | ||
Hayashi Y, Maze M. Alpha 2 adrenoceptor agonists and anaesthesia. Br J Anaesth. 1993;71(1):108–118. | ||
Svensson TH, Bunney BS, Aghajanian GK. Inhibition of both noradrenergic and serotonergic neurons in brain by the alpha-adrenergic agonist clonidine. Brain Res. 1975;92(2):291–306. | ||
Hafermann M, Grgurich P, Marshal J. Care of the critically ill adults. In: Koda-Kimble MA, Young LY, editors. Applied Therapeutics: The Clinical Use of Drugs. 11th ed. Philadelphia: Lippincott Williams & Wilkins; 2018:1205–1217. | ||
Vaughan BR, Kleber HD. Opioid detoxification. In: Galanter M, Kleber HD, Brady KT, editors. The American Psychiatric Publishing Textbook of Substance Abuse Treatment. 5th ed. Washington, DC: American Psychiatric Publishing Inc.; 2015. | ||
Patel SB, Kress JP. Sedation and analgesia in the mechanically ventilated patient. Am J Respir Crit Care Med. 2012;185(5):486–497. | ||
Pichot C, Ghignone M, Quintin L. Dexmedetomidine and clonidine: from second- to first-line sedative agents in the critical care setting? J Intensive Care Med. 2012;27(4):219–237. | ||
Spies CD, Dubisz N, Neumann T, et al. Therapy of alcohol withdrawal syndrome in intensive care unit patients following trauma: results of a prospective, randomized trial. Crit Care Med. 1996;24(3):414–422. | ||
Gold MS, Redmond DE, Kleber HD. Clonidine blocks acute opiate-withdrawal symptoms. Lancet. 1978;2(8090):599–602. | ||
Liatsi D, Tsapas B, Pampori S, Tsagourias M, Pneumatikos I, Matamis D. Respiratory, metabolic and hemodynamic effects of clonidine in ventilated patients presenting with withdrawal syndrome. Intensive Care Med. 2009;35(2):275–281. | ||
Hall JE, Uhrich TD, Ebert TJ, Sedative ET. Sedative, analgesic and cognitive effects of clonidine infusions in humans. Br J Anaesth. 2001;86(1):5–11. | ||
Bailey PL, Sperry RJ, Johnson GK, et al. Respiratory effects of clonidine alone and combined with morphine, in humans. Anesthesiology. 1991;74(1):43–48. | ||
Jamadarkhana S, Gopal S. Clonidine in adults as a sedative agent in the intensive care unit. J Anaesthesiol Clin Pharmacol. 2010;26(4):439. | ||
Mantz J, Josserand J, Hamada S. Dexmedetomidine: new insights. Eur J Anaesthesiol. 2011;28(1):3–6. | ||
Bajwa S, Kulshrestha A. Dexmedetomidine: an adjuvant making large inroads into clinical practice. Ann Med Health Sci Res. 2013;3(4):475–483. | ||
Kemp KM, Henderlight L, Neville M. Precedex: is it the future of cooperative sedation? Nursing. 2008;38:7–8. | ||
Riker RR, Shehabi Y, Bokesch PM, et al. Dexmedetomidine vs midazolam for sedation of critically ill patients: a randomized trial. JAMA. 2009;301(5):489–499. | ||
Jakob S, Ruokonen E, Grounds R, et al. Dexmedetomidine for long-term sedation investigators: dexmedetomidine vs midazolam or propofol for sedation during prolonged mechanical ventilation: two randomized controlled trials. JAMA. 2012;307(11):1151–1160. | ||
Keating GM. Dexmedetomidine: a review of its use for sedation in the intensive care setting. Drugs. 2015;75(10):1119–1130. | ||
Food U. Drug Administration b. Sunland Nut and Seed Product Recalls. Available from: http://www.fda.gov/Safety/Recalls/MajorProductRecalls/SunlandNutSeedProductRecalls/default htm. Accessed May 5, 2018. | ||
Pasin L, Landoni G, Nardelli P, et al. Dexmedetomidine reduces the risk of delirium, agitation and confusion in critically Ill patients: a meta-analysis of randomized controlled trials. J Cardiothorac Vasc Anesth. 2014;28(6):1459–1466. | ||
Dasta JF, Kane-Gill SL, Pencina M, et al. A cost-minimization analysis of dexmedetomidine compared with midazolam for long-term sedation in the intensive care unit. Crit Care Med. 2010;38(2):497–503. | ||
Bioc JJ, Magee C, Cucchi J, et al. Cost effectiveness of a benzodiazepine vs a nonbenzodiazepine-based sedation regimen for mechanically ventilated, critically ill adults. J Crit Care. 2014;29(5):753–757. | ||
Gagnon DJ, Riker RR, Glisic EK, Kelner A, Perrey HM, Fraser GL. Transition from dexmedetomidine to enteral clonidine for ICU sedation: an observational pilot study. Pharmacotherapy. 2015;35(3):251–259. | ||
Roberts DJ, Haroon B, Hall RI. Sedation for critically ill or injured adults in the intensive care unit. Drugs. 2012;72(14):1881–1916. | ||
Hart GR, Anderson RJ. Withdrawal syndromes and the cessation of antihypertensive therapy. Arch Intern Med. 1981;141(9):1125–1127. | ||
Barbani F, Angeli E, De Gaudio AR. Intravenous sedatives and analgesics. In: De Gaudio AR, Romagnoli Stefano, editors. De Gaudio AR, Romagnoli Stefano. Critical Care Sedation. Springer; 2018:69–101. | ||
Hendrickx JF, Eger EI, Sonner JM, Shafer SL. Is synergy the rule? A review of anesthetic interactions producing hypnosis and immobility. Anesth Analg. 2008;107(2):494–506. | ||
Marik PE. Propofol: therapeutic indications and side-effects. Curr Pharm Des. 2004;10(29):3639–3649. | ||
Kikuchi T, Wang Y, Sato K, Okumura F. In vivo effects of propofol on acetylcholine release from the frontal cortex, hippocampus and striatum studied by intracerebral microdialysis in freely moving rats. Br J Anaesth. 1998;80(5):644–648. | ||
Kushikata T, Hirota K, Yoshida H, Kubota T, Ishihara H, Matsuki A. Alpha-2 adrenoceptor activity affects propofol-induced sleep time. Anesth Analg. 2002;94(5):1201–1206. | ||
Lingamaneni R, Birch ML, Hemmings HC. Widespread inhibition of sodium channel-dependent glutamate release from isolated nerve terminals by isoflurane and propofol. Anesthesiology. 2001;95(6):1460–1466. | ||
Cechetto DF, Diab T, Gibson CJ, Gelb AW. The effects of propofol in the area postrema of rats. Anesth Analg. 2001;92(4):934–942. | ||
Farington EA, Buck ML. Care of the critically ill child. In: Koda-Kimble MA, Young LY, editors. Applied Therapeutics: The Clinical Use of Drugs. 11th ed. Philadelphia: Lippincott Williams & Wilkins; 2018. | ||
Tietze KJ, Fuchs B. Sedative-analgesic medications in critically ill adults: Properties, dosage regimens, and adverse effects. Waltham, MA: UpToDate Inc.; 2018. Available from: https://www.uptodate.com/contents/sedative-analgesic-medications-in-critically-ill-adults-properties-dosage-regimens-and-adverse-effects?search=sedative%20analgesic&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1. Accessed April 15, 2018. | ||
Jacobi J, Fraser GL, Coursin DB, et al. Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adult. Crit Care Med. 2002;30(1):119–141. | ||
Curtis JA, Hollinger MK, Jain HB. Propofol-based versus dexmedetomidine-based sedation in cardiac surgery patients. J Cardiothorac Vasc Anesth. 2013;27(6):1289–1294. | ||
Reade MC, Finfer S. Sedation and delirium in the intensive care unit. N Engl J Med Overseas Ed. 2014;370(5):444–454. | ||
Walder B, Elia N, Henzi I, Romand JR, Tramèr MR. A lack of evidence of superiority of propofol versus midazolam for sedation in mechanically ventilated critically ill patients: a qualitative and quantitative systematic review. Anesthesia & Analgesia. 2001;92(4):975–983. | ||
Fong JJ, Kanji S, Dasta JF, Garpestad E, Devlin JW. Propofol associated with a shorter duration of mechanical ventilation than scheduled intermittent lorazepam: a database analysis using Project IMPACT. Ann Pharmacother. 2007;41(12):1986–1991. | ||
Girard TD, Kress JP, Fuchs BD, et al. Efficacy and safety of a paired sedation and ventilator weaning protocol for mechanically ventilated patients in intensive care (Awakening and Breathing Controlled trial): a randomised controlled trial. Lancet. 2008;371(9607):126–134. | ||
Burns V, Peitz G. 897: Dexmedetomidine Vs. Propofol. Crit Care Med. 2018;46(1):432. | ||
Bowdle A, Richebe P, Lee L, Rostomily R, Gabikian P, Hypertriglyceridemia GP. Hypertriglyceridemia, lipemia, and elevated liver enzymes associated with prolonged propofol anesthesia for craniotomy. Ther Drug Monit. 2014;36(5):556–559. | ||
Dönmez A, Arslan G, Pirat A, Demirhan B. Is pancreatitis a complication of propofol infusion? Eur J Anaesthesiol. 1999;16(6):367–370. | ||
Bray RJ. Propofol infusion syndrome in children. Paediatr Anaesth. 1998;8(6):491–499. | ||
Schroeppel TJ, Fabian TC, Clement LP, et al. Propofol infusion syndrome: A lethal condition in critically injured patients eliminated by a simple screening protocol. Injury. 2014;45(1):245–249. | ||
Fodale V, La Monaca E. Propofol infusion syndrome. Drug Saf. 2008;31(4):293–303. | ||
Roberts RJ, Barletta JF, Fong JJ, et al. Incidence of propofol-related infusion syndrome in critically ill adults: a prospective, multicenter study. Critical Care. 2009;13(5):R169. | ||
Kurdi MS, Theerth KA, Deva RS. Ketamine: Current applications in anesthesia, pain, and critical care. Anesth Essays Res. 2014;8(3):283. | ||
Sleigh J, Harvey M, Voss L, Denny B. Ketamine – More mechanisms of action than just NMDA blockade. Trends in Anaesthesia and Critical Care. 2014;4(2–3):76–81. | ||
Morgan CJA, Curran HV. The Independent Scientific Committee on Drugs (ISCD) Ketamine use: a review. Addiction. 2012;107(1):27–38. | ||
Yoon SH. Concerns of the anesthesiologist: anesthetic induction in severe sepsis or septic shock patients. Korean J Anesthesiol. 2012;63(1):3–10. | ||
Jabre P, Combes X, Lapostolle F, et al. Etomidate versus ketamine for rapid sequence intubation in acutely ill patients: a multicentre randomised controlled trial. Lancet. 2009;374(9686):293–300. | ||
Goyal S, Agrawal A. Ketamine in status asthmaticus: A review. Indian J Crit Care Med. 2013;17(3):154. | ||
Badrinath S, Avramov MN, Shadrick M, Witt TR, Ivankovich AD. The use of a ketamine-propofol combination during monitored anesthesia care. Anesth Analg. 2000;90(4):858–862. | ||
Bar-Joseph G, Guilburd Y, Tamir A, Guilburd JN. Effectiveness of ketamine in decreasing intracranial pressure in children with intracranial hypertension. J Neurosurg Pediatr. 2009;4(1):40–46. | ||
Hijazi Y, Bodonian C, Bolon M, Salord F, Boulieu R. Pharmacokinetics and haemodynamics of ketamine in intensive care patients with brain or spinal cord injury. Br J Anaesth. 2003;90(2):155–160. | ||
Bowdle TA, Radant AD, Cowley DS, Kharasch ED, Strassman RJ, Roy-Byrne PP. Psychedelic effects of ketamine in healthy volunteers: relationship to steady-state plasma concentrations. Anesthesiology. 1998;88(1):82–88. | ||
Kronenberg RH. Ketamine as an analgesic: parenteral, oral, rectal, subcutaneous, transdermal and intranasal administration. J Pain Palliat Care Pharmacother. 2002;16(3):27–35. | ||
Joly V, Richebe P, Guignard B, et al. Remifentanil-induced postoperative hyperalgesia and its prevention with small-dose ketamine. Anesthesiology. 2005;103(1):147–155. | ||
Kye YC, Rhee JE, Kim K, et al. Clinical effects of adjunctive atropine during ketamine sedation in pediatric emergency patients. Am J Emerg Med. 2012;30(9):1981–1985. | ||
Pomarol-Clotet E, Honey GD, Murray GK, et al. Psychological effects of ketamine in healthy volunteers. Phenomenological study. Br J Psychiatry. 2006;189(2):173–179. | ||
Smith M, Barletta M, Diehl K, Hofmeister E, Franklin S. Effect of propofol and ketamine–diazepam on intraocular pressure in healthy premedicated dogs. Vet Anaesth Analg. 2017;44(5):1262.e12–e12. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.