Back to Journals » Patient Preference and Adherence » Volume 19
Psychosocial Determinants of Antidepressant Adherence Among Hungarian Adults: A Cross-Sectional Online Survey
Authors Boruzs K ![]() , Dombrádi V
, Dombrádi V ![]() , Bíró K
, Bíró K
Received 22 August 2025
Accepted for publication 26 November 2025
Published 18 December 2025 Volume 2025:19 Pages 4153—4166
DOI https://doi.org/10.2147/PPA.S562457
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ramón Morillo-Verdugo
Klára Boruzs, Viktor Dombrádi, Klára Bíró
Institute of Health Economics and Management, Faculty of Economics and Business, University of Debrecen, Debrecen, Hungary
Correspondence: Klára Boruzs, Institute of Health Economics and Management, Faculty of Economics and Business, University of Debrecen, Böszörményi út 138, Debrecen, H-4032, Hungary, Tel +36 52 508 444 68033, Email [email protected]
Purpose: Depression is a significant public health concern in Hungary, contributing to disability, reduced productivity, and impaired quality of life.
Patients and Methods: A nationwide online survey (14 May– 11 June 2025) was followed by multiple linear regression analyses to explore links between patients’ socio-demographic factors and their scores on the Beliefs about Medicines Questionnaire and Beck Anxiety Inventory. The main focus of the study was on participants’ adherence to prescribed antidepressant treatment assessed using the Medication Adherence Report Scale. Adults over 18 taking GP-prescribed antidepressants were included. This was a cross-sectional observational study based on self-reported survey data.
Results: The sample consisted of 213 participants. The participants who smoked were less adherent to their prescribed antidepressant regimen (coef=− 1.445; p=0.038). In contrast, individuals reporting satisfaction with their general practitioner exhibited higher adherence levels (coef=1.609; p=0.033). Monthly collection of antidepressant prescriptions was associated with better adherence than less frequent collection intervals—specifically every two months (coef=5.106; p=0.001), every three months (coef=3.900; p=0.016), or less often (coef=3.887; p=0.013). General beliefs about medicine influence antidepressant adherence: perceiving them as harmful (coef=− 2.404; p=0.001) or overused (coef=− 1.197; p=0.002) reduces adherence, while viewing antidepressants as necessary enhances it (coef=1.531; p=0.001).
Conclusion: Medication adherence is influenced by patients’ beliefs, smoking status, anxiety levels, and satisfaction with care. Enhancing treatment continuity requires addressing these areas.
Keywords: depression, antidepressant, medication adherence, surveys and questionnaires
Introduction
Depression, defined as a persistent low mood and/or diminished interest or pleasure in activities over an extended period, can affect individuals regardless of age, gender, or socioeconomic status. However, certain groups are at elevated risk. As previously highlighted, people in early adulthood in the European Union are at increased risk of depression.1
In 2019, an estimated 970 million people worldwide—approximately one in eight individuals—were living with a mental disorder, anxiety and depression being the most commonly reported conditions.2 The onset of the COVID-19 pandemic in late 2019 led to a substantial rise in these conditions, preliminary data indicate a notable surge within a single year, with anxiety disorders rising by 26% and major depressive disorders by 28%.3
Risk factors significantly associated with depression include being female, feelings of loneliness, low level of education, financial difficulties, poor housing conditions, health and sleep problems, mental illness, stressful life events, lack of social support, stress, academic or personal problems, and excessive smartphone use.4
The highest prevalence rates of chronic depression in Europe were observed in Luxembourg, Denmark, Croatia, Germany, Sweden, and Portugal, with each country reporting figures between 10.0% and 12.2%. In contrast, significantly lower rates—at or below 4.0%—were recorded in Hungary, Ireland, Greece, Malta, Bulgaria, and Romania.5 In 2019, 7.2% of adolescents in the European Union reported experiencing chronic depression in the 12 months prior to the survey.5
The differences in the prevalence of depression across the European Union are due to complex social, health and cultural factors. Socio-economic factors such as income inequality, poverty, unemployment and low education levels increase the risk of depression, while a stable economic background and an inclusive education system reduces it.6 High unemployment rates can lead to economic insecurity and loss of identity, which increases the risk of depression (eg Portugal).7,8 Access to healthcare is also key: countries with well-funded, widely available mental health services, such as the Netherlands or Sweden, have lower rates of untreated depression.9 Cultural and social norms play a prominent role: where mental illnesses are stigmatized, underreporting and delay in seeking help are more common, while stronger family and community support can act as a protective factor to reduce the severity and persistence of depression (eg, Sweden, Lithuania, the Netherlands).10 Cultural stigma also plays an important role: in parts of Eastern and Southern Europe, shame about mental illness hinders help-seeking, and depression is often hidden behind physical symptoms.11 Gender roles and expectations about emotional expression also influence the recognition and reporting of symptoms: women are more likely to talk about their problems, while men often suppress them.12
The comparability of international prevalence data is limited by methodological differences, such as the type of measurement instruments used, differences in diagnostic criteria, the method of data collection (self-report vs clinical interview), and the demographic composition of the samples and sampling procedures. All of these affect the reliability and generalizability of the data.13
An earlier study explored the correlation between economic development and the prevalence of mental health disorders in four Central European countries: Poland, Czechia, Slovakia, and Hungary. Between 2000 and 2018, the prevalence of mental disorders showed an upward trajectory in most of the examined countries, except for Hungary, where a declining pattern was identified. Nonetheless, the standardized mortality rate attributed to mental disorders rose across all four countries. Hungarian data indicate that, although the overall prevalence remained relatively stable, the incidence declined, while mortality rates and the prescription of psychotropic medications both showed an upward trend. This paradox may indicate hidden morbidity: many mental disorders may remain unrecognized or untreated, especially in vulnerable groups (eg the unemployed, the elderly, rural residents).14 The lower number of new diagnoses may be due to limited access to psychiatric care, underreporting due to stigmatization, and weakening screening capacity in primary care. International comparisons (eg Eurostat, WHO) are further complicated by differences in measurement methods, especially the limitations of self-reported data.5
A survey of adults in Mozambique found that depression and anxiety were more common in women, especially in those with low socioeconomic status and unemployment. Men reported symptoms at much lower rates. Education and rural residence had different effects on mental health between genders. Vulnerable groups – the elderly, the divorced, Muslim women and those with limited resources – require special attention in mental health policy interventions.15
Several effective strategies exist for managing mental disorders, such as consulting mental health professionals, primary care providers, or faith-based support networks. Evidence-based treatments, including cognitive behavioral therapy and psychotherapy, have proven effective for mild to moderate depression. While antidepressants can be helpful, they are not recommended as first-line treatments for mild depression, especially for children and adolescents. Despite the availability of cost-effective interventions, a substantial gap persists between those who need mental healthcare and those who actually receive it. In addition, the gravity of depression as a public health problem has been highlighted by the recent global pandemic.16
Medication adherence is often low for many medical and psychiatric conditions, posing a significant challenge to achieving positive therapeutic outcomes. Explanatory models that examine beliefs about illness and treatment suggest that individuals’ beliefs significantly influence whether they take their medication as prescribed.17 In the context of psychopharmacology, adherence to medication is a complex phenomenon influenced by health-related attitudes and psychological characteristics, such as self-efficacy and sense of control, as well as family support.18,19 The medication possession ratio (MPR) method was used to assess medication adherence, with a score below 80% considered non-adherence. The main predictors of non-adherence were urban residence, use of tricyclic antidepressants, and presence of pain. Adherence improved with age, while female gender, institutional care, multiple medications, and comorbidities were protective factors. The MPR is a useful tool for identifying and monitoring non-adherent patients.20
In Hungary, medication adherence among people living with depression is extremely low: between 2012 and 2015, adherence to antidepressants was only 20.3% in Hungary, significantly lower than the European average. The 20.3% adherence rate means that approximately 80% do not follow antidepressant treatment properly – that is, 8 out of 10 patients do not switch or do not take the medication properly, which can lead to recurrence of symptoms, chronicity, and an increased burden on the healthcare system.21
The link between income inequality and depression is confirmed by several European studies. For example, a 2023 study in nine high-income European countries showed that socioeconomic differences contribute significantly to the concentration of depressive symptoms.22
Despite its widespread prevalence, depression remains challenging to treat, with antidepressant therapy leading to remission in no more than 60% of cases. In 2022, Iceland reported the highest level of antidepressant use among European countries, amounting to 157.3 Defined Daily Doses (DDD) per 1000 population. Between 2010 and 2020, all European countries—with the exception of Denmark—experienced a rise in antidepressant consumption, although the extent of this increase varied significantly across nations. Notably, Estonia, Latvia, and the United Kingdom reported growth rates exceeding 100%. Multiple factors contribute to the increased use of antidepressants, notably enhanced awareness and identification of depressive disorders, alongside the expansion of clinical indications for their application.23–25
The target group of the study was working-age adults, as in their case, discontinuation of drug therapy may not only have health consequences, but also have a direct impact on their ability to work and thus their participation in the labor market. Lack of therapeutic adherence in this population may represent an increased risk of losing work, which has relevant consequences from a social and economic perspective.26
The selection of variables was guided by two complementary theoretical models: The Necessity–Concerns Framework (NCF) and the Health Belief Model (HBM). The NCF emphasizes the balance between patients’ sense of need and concerns about taking medication, which directly affects adherence. The HBM offers a broader perspective on individual health risk perception, benefits and barriers to action, and external stimuli that motivate behavior. Based on the two models, variables such as perceived need for medication, concerns about side effects, perceived health risks, self-efficacy, workplace expectations and social support were included.27
Taking these notions into account, this study aimed to investigate the possible psychosocial factors influencing adherence of Hungarian adult patients taking antidepressant medication.
Materials and Methods
Data Collection and Study Settings
Between 14 May and 11 June, 2025, SZLEM Service L.P., a private Hungarian company, conducted an online national survey among Hungarian adults (18 and older).
The market research panel (egeszsegpanel.hu) is a cohort of patients who registered preliminary and gave consent to process their personal data for market research purposes. The panel is a good mix of respondents all over Hungary (by age, gender, region, type of settlement, education level). From this panel those patients were selected who indicated having depression. All these patients were invited to take part in the survey. No personal data was collected and all data was stored and analyzed without any personal identification variable guaranteeing participant anonymity.
Before participating, individuals signed an informed consent form that outlined the purpose and procedures of the study and were assured that their involvement was completely voluntary. The informed consent process adhered to the Ministerial Decree governing research involving human participants in Hungary. They also received written documentation explaining the goals of the research and were assured that their involvement was completely voluntary.
Additionally, any personal data managed by the research panel, based on prior consent for communication purposes, were kept entirely separate from survey responses, ensuring that the individuals’ answers could not be traced back to them under any circumstances.
The survey instrument comprised 24 demographic items, 11 items from the Beliefs about Medicines Questionnaire (BMQ), 8 items assessing background variables (BG), 5 items from the Medication Adherence Report Scale (MARS-5), and 21 items from the Beck Depression Inventory (BDI).
The study had sociodemographic characteristics, including age, sex, education, NUTS 2 (Nomenclature of territorial units for statistics) regional classification, town size (based on population), marital status, perceived financial status, being a healthcare worker, and perceived health condition. Participants’ financial circumstances were categorized, based on self-assessment, into three groups: good or very good, fair, and bad or very bad. Education was classified as primary, secondary, or tertiary (college or university). The results of the BMQ (Beliefs about Medicines Questionnaire) and BAI (Beck Anxiety Inventory) scales served as independent (input) variables, while the MARS-5 (Medication Adherence Report Scale) score was analyzed as a dependent (output) variable.
The survey took approximately 8 minutes to complete and was administered through an anonymous online questionnaire.
Study Design & Sampling
This is an observational study. The study design was a cross-sectional, web-based survey, with inclusion and exclusion criteria being adults aged 18 years or older who reported taking at least one relevant antidepressant medication at the time of completion.
Of the 2,199 individuals invited to participate in the study, 863 opened the invitation email. Among them, 689 initiated the survey, and 677 provided informed consent. Following eligibility screening, 280 participants of the total invited sample met the inclusion criteria and completed the full survey.
All questions except the open-ended one asking about the specific medication were closed and compulsory to answer. 67 respondents were excluded from the analysis due to not-eligible answers (no or wrong answer) to the open-ended question asking about the specific antidepressant medication. It was a self-completion questionnaire. For validation we asked the name(s) of the prescription drug(s) taken for treating depression unaided. Those were excluded who could not give a valid answer for this question. Given the final sample size (N=213), the study had sufficient precision to detect at least moderate associations for the main predictors (two-sided α=0.05).
The Beliefs About Medicines Questionnaire
The Beliefs about Medicines Questionnaire (BMQ), developed by Horne, Weinman, and Hankins in 1999, is a well-established psychometric tool used to assess individuals’ cognitive perceptions about medication. It is comprised of two major sections: the BMQ-General and the BMQ-Specific. The BMQ-General evaluates people’s beliefs regarding medicines as a whole, focusing on themes of harm and overuse. For instance, individuals may be asked to consider statements such as whether they believe medicines do more harm than good, whether natural remedies are perceived as safer alternatives, or whether doctors rely too heavily on prescribing medications.28 The BMQ-General is a brief questionnaire that measures people’s general beliefs about medicines. It includes two subscales: General-Harm, which assesses the belief that medicines are harmful, and General-Overuse, which evaluates the idea that doctors overprescribe medications.29
On the other hand, the BMQ-Specific assesses an individual’s beliefs about their prescribed medication. This component distinguishes between two dimensions, necessity and concerns. The necessity dimension probes the extent to which a patient believes their medication is essential to maintaining their current health status. In contrast, the concern dimension captures apprehensions about the medication, such as fears of long-term side effects, dependency, or the medication’s impact on daily life.28
The BMQ has been validated multiple times30–35 and widely adapted across various patient populations and cultural settings, including Hungarian.36,37
To measure attitudes about medications, we used a standardized version of the Beliefs about Medicines Questionnaire (BMQ). The instrument contains several subscales that assess individual beliefs about the necessity of medications, concerns about possible side effects, and general perceptions of medications. Each item is rated on a five-point Likert scale (1 = strongly disagree, 5 = strongly agree), and the subscale score is calculated by summing the responses to the given item.38
The Specific–Necessity subscale contains five items and measures the belief in the personal necessity of medication; its score range is 5–25, where higher scores indicate stronger beliefs about the importance of taking medications. The Specific–Concerns subscale consists of six items and assesses concerns about the side effects and long-term consequences of medications; its score range is 6–30, where higher scores indicate greater concern. The General–Overuse subscale has four items and measures the belief that doctors prescribe medications too often (score range: 4–20). The General–Harm subscale also has four items and assesses beliefs about the general harmfulness or addictiveness of medications (score range: 4–20). Higher scores on the Concerns, Overuse, and Harm scales indicate more negative, sceptical attitudes toward medications, while higher scores on the Necessity scale reflect positive, intrinsic motivation for medication.28
The Hungarian BMQ-Specific scale validated by Boruzs et al showed good psychometric properties: the Cronbach’s alpha value of the “Need” subscale was 0.84, while that of the “Concerns” scale was 0.78, indicating adequate internal consistency. The two-factor structure was confirmed by factor analysis, and the correlations between the individual items were also adequate. The culturally adapted version of the questionnaire, tested on a targeted patient group, proved to be a reliable measuring instrument for examining attitudes towards medication taking.36
The Medication Adherence Report Scale
The Medication Adherence Report Scale (MARS-5) is a widely used self-report instrument developed to assess how consistently patients follow their prescribed medication regimens. It was introduced by Horne et al as part of a broader effort to understand the psychological and behavioral factors influencing medication adherence. The MARS-5 consists of five items that reflect common patterns of non-adherence, such as forgetting to take medication, altering the dose, or intentionally skipping doses. Each item is rated on a five-point Likert scale ranging from “always” to “never,” with higher scores indicating better adherence. The total score ranges from 5 to 25, calculated by adding up the responses to each item. A higher score indicates better self-reported adherence, ie, fewer inappropriate medication behaviors. A score of 25 indicates perfect adherence, while a score of 23–24 indicates moderate adherence, and a score of 22 or less indicates low adherence.38
Using the commonly applied threshold of MARS-5 ≥ 20 to define adherence, the median score of 20.0 suggests that at least 50% of respondents were adherent. Precise adherence rates could be calculated from the raw data by determining the proportion of participants scoring ≥ 20.39
This tool is particularly valued for its brevity, ease of use, and applicability across a range of chronic conditions and treatment contexts. It has been employed in numerous studies to identify patients at risk of poor adherence and to evaluate the effectiveness of interventions aimed at improving medication-taking behavior.40
This instrument was translated into Hungarian for patients with inflammatory bowel disease.41
Beck Anxiety Inventory (BAI)
The Beck Anxiety Inventory (BAI) is a self-report questionnaire designed to assess the severity of anxiety in individuals. Comprising 21 items, it uses a Likert-type format where each symptom is rated on a scale that reflects increasing levels of distress. This scale is ordinal in nature, meaning the values reflect a ranked order but not necessarily equal intervals between them. Respondents indicate how much each symptom has bothered them over the past week, with response options typically ranging from “not at all” to “severely.” The cumulative score provides a general measure of anxiety intensity, which can be categorized into minimal, mild, moderate, or severe levels.42
This questionnaire was translated into Hungarian and was used among patients in family practice.43
Respondents rate each item on a four-point scale, where 0 indicates “not at all” and 3 indicates “severely” typical symptoms. The total score ranges from 0 to 63, calculated by adding up the responses to each item. A higher score reflects a greater presence of anxiety symptoms. The interpretation is made according to the following categories: 0–7 points indicate minimal, 8–15 points indicate mild, 16–25 points indicate moderate, while 26–63 points indicate severe anxiety.44
Data Analysis
Only those taking antidepressant medication prescribed by their general practitioner and who completed all relevant items in the BMQ, the MARS-5 and BAI were included in the statistical analysis. Categorical variables were expressed as frequency (%), and continuous variables were expressed as mean, standard deviation (SD), median and interquartile range (IQR). Cronbach’s alpha was calculated for all three instruments to assess the reliability of each subscale. If the alpha value was greater than 0.70, the internal reliability was considered acceptable.45
A multiple linear regression was conducted to investigate the association between socio-demographic characteristics and the subscale scores of both the BMQ and the BAI. The outcome of the study was patients’ adherence to taking their antidepressant medication, utilizing MARS-5, which measures how consistently study participants take their antidepressant as prescribed by their doctor. The outcomes were expressed as regression coefficients along with their respective 95% confidence intervals (CI). In the multivariate linear regression analyses, all measured variables were included as covariates regardless of their univariate associations, in order to obtain adjusted estimates that account for potential confounding. The included covariates were: sex, age, education, marital status, type of residence, healthcare worker status, self-perceived health status, self-perceived financial status, smoking status, alcohol consumption, satisfaction with the GP, and redemption frequency of antidepressant medication. These variables were selected a priori based on theoretical relevance and previous literature on medication adherence and healthcare satisfaction. Model diagnostics were performed, including the assessment of multicollinearity, residual normality, and homoscedasticity. No multicollinearity was detected, while mild non-normality and heteroscedasticity were addressed by using robust standard errors. Explained variance ranged between R2=0.19–0.33 (adjusted R2=0.13–0.27) across models.
Statistical significance was determined at a threshold of p<0.05. All analyses were performed using STATA version 13 (StataCorp LLC, College Station, TX, USA).
The total scores from the questionnaires were treated as continuous variables in the statistical analyses. This allowed for the full range of values of the scales to be considered and ensured that variance was preserved when examining relationships. The scores of the individual scales (eg, BMQ, MARS-5, BAI) were therefore included in the correlation and regression analyses in numerical form rather than in categories. Internal consistency (Cronbach’s alpha) was computed on the full analytic sample for all psychometric scales (Supplementary Table S1).
The survey was hosted and data was collected on VOXCO Microsoft Azure server at highest security. No personal data was collected during the survey and all data was stored and analyzed without any personal identification variables.
Results
Demographic Profile
The sample consisted of 213 participants (Table 1), of which 63% were women and 37% men. Most participants had completed secondary education (65%), while 29% held a tertiary (college or university) degree, and 6% had only primary education. Regarding marital status, 59% were married or in a relationship, and 41% fell into other categories. A majority of participants (79%) lived in urban areas, while 21% resided in rural regions. Only 8% were healthcare workers. In terms of health perceptions, 62% rated their health as excellent, very good, or good, and 38% considered their health poor or bad. Financial status was generally perceived as less favorable, with 84% reporting fair to very bad conditions, and only 16% rating their finances as very good or good. Smoking and alcohol consumption were common among respondents, 49% smoked and 73% consumed any amount of alcohol. Satisfaction with general practitioners was relatively high, with 62% expressing satisfaction.
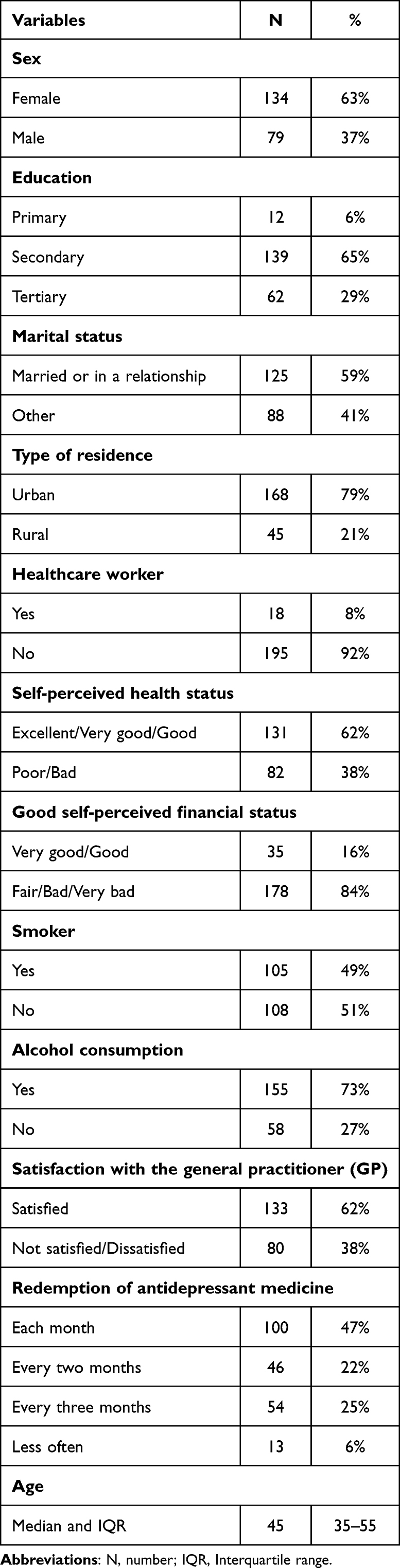 |
Table 1 Demographic Data of the Respondents |
Regarding antidepressant medication redemption, 47% filled prescriptions monthly, 22% every two months, 25% every three months, and 6% less frequently. The median age of respondents was 45 years, with an interquartile range of 35 to 55 years. The most frequently reported antidepressants or related medications were Frontin/Alprazolam, Xanax/Alprazolam and Rivotril/ Clonazepam, followed by Scippa/Sertraline, Rexetin/Paroxetine and Velaxin/Venlafaxine. A list of self-reported drugs is provided in Supplementary Table S2.
Descriptive Statistics
The BAI scores among participants averaged 22.23 with a standard deviation of 15.22, indicating a broad range of anxiety levels across the sample (Table 2). The average score on MARS-5 was 19.1 (SD=5.19), reflecting moderate adherence behaviors. Based on established cut-offs, 26.3% (N=56) of participants showed low adherence (<16), 18.8% (N=40) showed medium adherence (16–19), and 54.9% (N=117) showed high adherence (≥20). BMQ-General beliefs reflected moderate concern about overuse (mean=3.63, SD=0.91) and potential harm (mean=3.36, SD=0.85). BMQ-Specific beliefs demonstrated a nearly balanced perception of necessity (mean=3.26, SD=0.85) and concern (mean=3.22, SD=0.83). Cronbach’s alpha values for all scales exceeded 0.70, confirming good internal consistency (range: 0.773–0.953). Bivariate Spearman correlations between the main continuous variables are shown in Supplementary Table S1. MARS-5 scores were positively associated with BMQ-Specific Necessity (rho = 0.16, p = 0.022) and negatively associated with BMQ-Specific Concerns (rho = –0.18, p = 0.010), BMQ-General Overuse (rho = –0.19, p = 0.006), and BMQ-General Harm (rho = –0.37, p < 0.001). Intercorrelations among the BMQ subscales ranged from weak to moderate, with the strongest relationship observed between General Harm and General Overuse (rho = 0.68, p < 0.001).
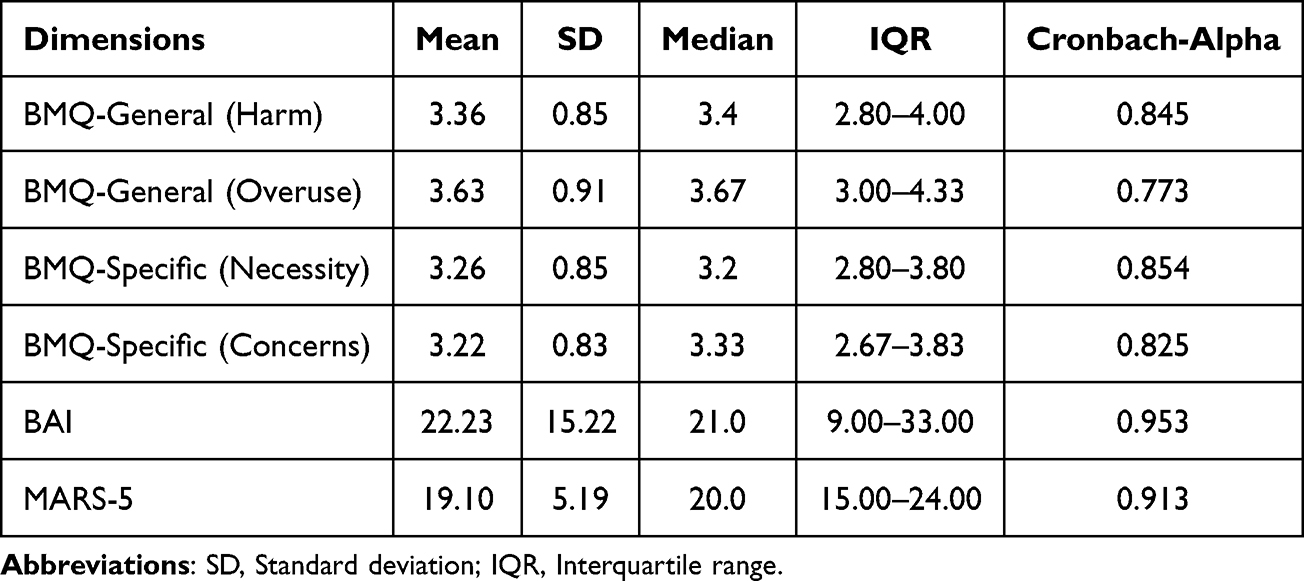 |
Table 2 Descriptive Statistics and Reliability Coefficients for Psychometric Scales |
Multivariate Analyses
Several differences were identified, which were not significant regarding the association between socio-demographic variables and adherence, measured with MARS-5 (Table 3). For example, among those surveyed, women are more adherent to antidepressant medication than men, meaning that they are more likely to stick to their medication (coef=1.408; p=0.053). Compared to those with primary education, those with higher education (secondary and tertiary) were less adherent, meaning that those with a lower level of education were more adherent to their medication (Secondary: coef=−0.830; p=0.590; Tertiary: coef=−0.841; p=0.610). Furthermore, those who were married or in a relationship were more adherent to antidepressant medication than those who were not married. (coef=0.693; p=0.326). Smoking was negatively associated with antidepressant medication adherence, with smokers showing significantly lower adherence (coef=–1.445, p=0.038). Participants who were satisfied with their GP (coef=1.609; p=0.033) were significantly more adherent to their medication than those who were not satisfied. Compared with monthly redemption as reference, patients who redeemed their antidepressant every two months, every three months, or less often had higher adherence scores (coef=5.106, 95%, p=0.001; coef=3.900, p=0.016; and coef=3.887, p=0.013; respectively).
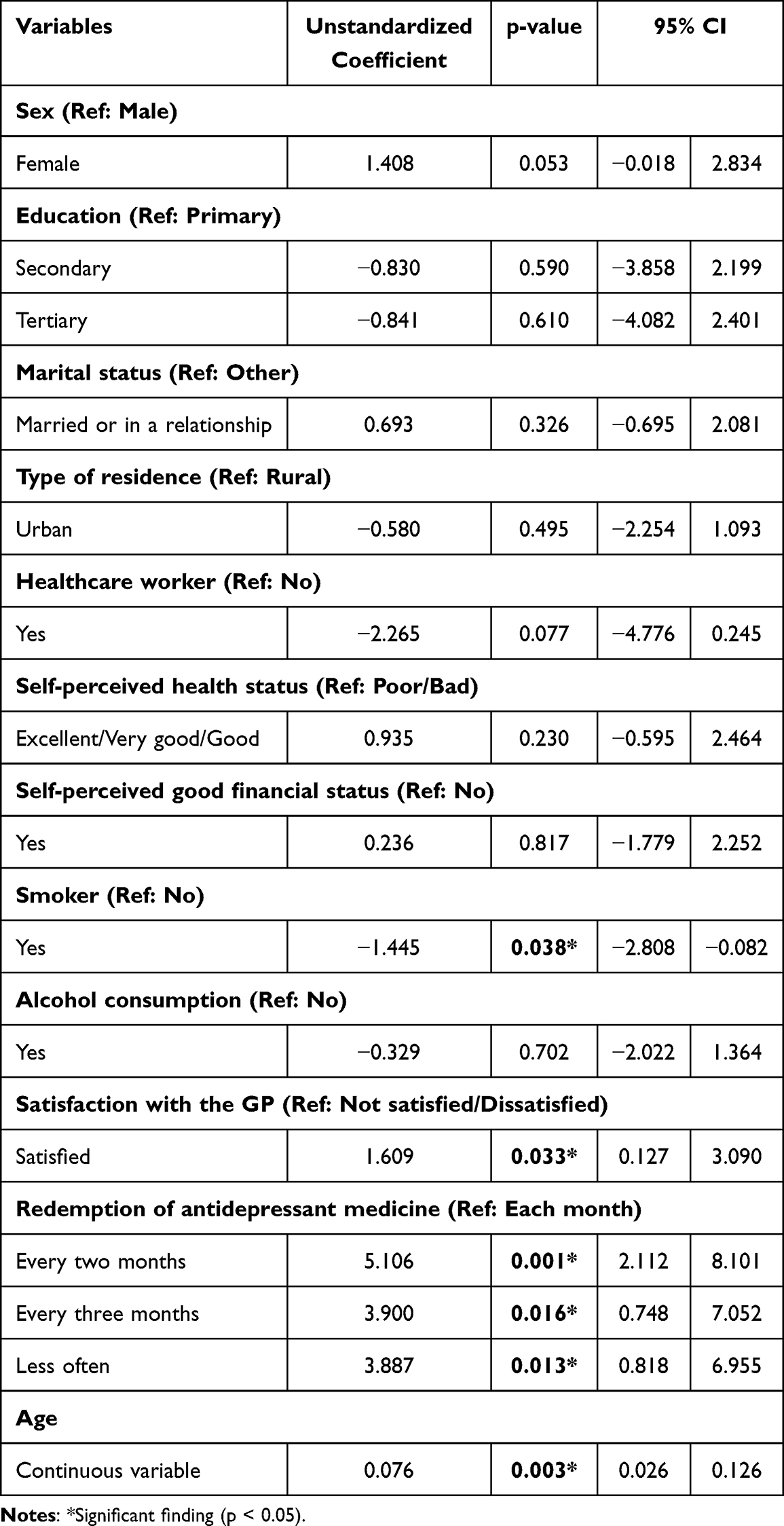 |
Table 3 Multivariate Analysis of the Association Between Socio-Demographic Variables and MARS-5 |
When each psychometric dimension was added separately to the base model adjusted for all potential confounding variables, several consistent and significant associations were observed. The analysis shows that individuals who believe medicines overall are generally harmful (coef=−2.404; p<0.001) or overused (coef=−1.197; p=0.002) tend to have significantly lower antidepressant adherence (Table 4). Conversely, those who view their antidepressant medication as necessary exhibit higher adherence (coef=1.531; p=0.001). Concerns about antidepressant medications were also related to lower adherence, though the effect was more modest (coef=−0.900; p=0.038). Additionally, higher scores on the Beck Anxiety Inventory were associated with slightly lower adherence (coef=−0.050; p=0.031).
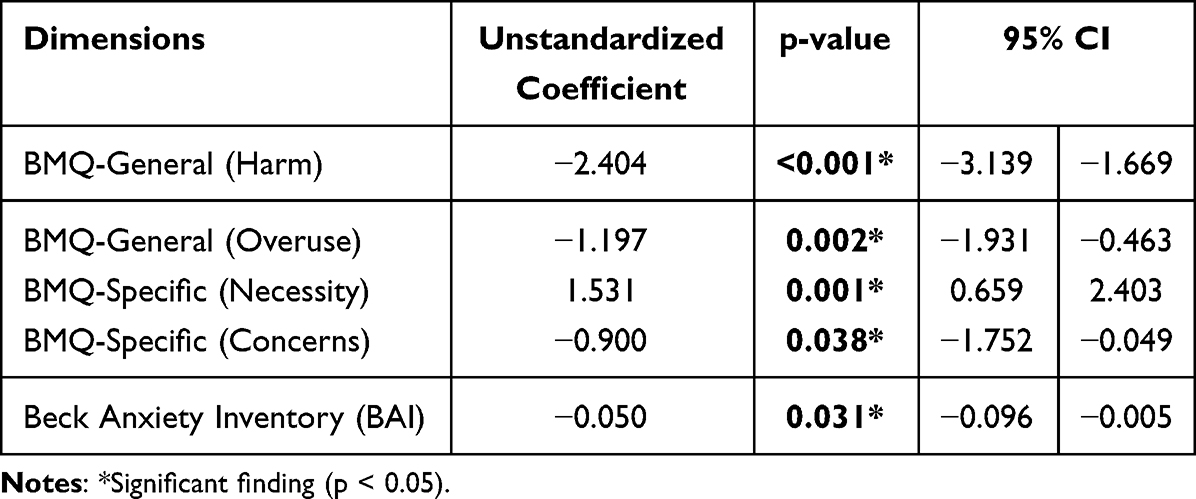 |
Table 4 Patients’ Adaptation to Taking Antidepressants Based on the Multivariate Analyses Adjusted for Socio-Demographic Variables |
Discussion
The current study explores the various psychosocial factors influencing antidepressant medication adherence among Hungarian adults.
Approximately half of all patients fail to follow their prescribed medication regimens, a factor linked to poorer health outcomes and increased healthcare costs.46 According to the Necessity-Concerns Framework, personal beliefs surrounding medication significantly influence adherence. In line with this, UK Clinical Adherence Guidelines advocate for actively exploring and incorporating patients’ individual perceptions of their medication during consultations.46
A systematic review and meta-analysis of studies have found the same results as our research, that the Necessity-Concerns Framework offers a valuable model for interpreting patients’ opinions about their prescribed medications. By considering patients’ beliefs and concerns about the necessity of treatment, healthcare professionals can improve their prescribing practices. This approach will facilitate more meaningful patient involvement in treatment decisions and promote better adherence to prescribed therapies.27
A study conducted in the Unites States made the same finding as our research, that the intensity of depressive symptoms and specific concerns about antidepressant use were closely related to patients’ self-reported behavior. These findings indicate that primary care physicians need to go beyond prescribing instructions to inform patients about the immediate and long-term effects of treatment, and explain the mechanism of action, and clarify that antidepressants are not addictive.17
The current research also confirmed the results of a study done in Tenerife, Spain: among the Hungarian adult respondents, there was no strong correlation between therapy adherence and sociodemographic characteristics. Instead, the patients’ individual attitudes, beliefs, and relationship to medication proved to be a determining factor in consistent treatment adherence. Patients who adhered to therapy were typically less concerned about the adverse effects of medications and reported fewer side effects, all of which facilitated greater cooperation in the treatment recommended by the doctor.46
While depression severity appeared to influence adherence, the nature of this relationship, whether direct or shaped by interactions with other variables, remains uncertain. Additionally, the presence of side-effects was closely linked to adherence, particularly in the context of frequent polypharmacy.47
Results from a study using the MARS-5 questionnaire showed a significant rate of non-adherence to medication in general, with many patients discontinuing medication on their own. An equally significant proportion of participants admitted to forgetting their doses. The results suggest that medication may have only a limited impact on patients’ emotional, psychological and physical health. In addition, a significant proportion of respondents reported experiencing stigma or prejudice related to medication.48
In our study, we examined specific psychosocial variables that may be associated with medication adherence. Factors included beliefs about medications, satisfaction with treatment, smoking status, and anxiety levels. However, certain clinical variables, such as severity of depression, presence of comorbidity, and duration of treatment, were not examined.
Beliefs about medications were measured using the Beliefs about Medicines Questionnaire (BMQ). Results suggest that high need scores promote adherence, while high worry scores may be predictive of nonadherent behavior. The scale provides insight into internalized attitudes that can be influenced by targeted education or counselling.28,46
Satisfaction with the general practitioner is positively associated with adherence and long-term persistence. This variable can also be interpreted as an indirect indicator of therapeutic alliance and patient-centered care.49,50
Smoking status serves as a behavioral marker related to health risk perception, self-regulation, and lifestyle patterns. Patients who smoke are often associated with lower levels of adherence and poorer health outcomes.51,52 According to a study, adherence to antidepressant medications is lower among smokers than among non-smokers, and although this association is not statistically significant, the trend is also observed for other medications. Smokers are generally less likely to adhere to recommended preventive care and medication use, which not only worsens health outcomes but may also result in additional costs for employers. Therefore, raising awareness and targeting care gaps among smokers may be an important part of a comprehensive public health strategy.53
The quality of the patient-physician relationship has a positive impact on medication adherence. When patients perceive a strong, trusting relationship with their physician, they are more likely to follow treatment instructions. Empathy and effective communication play a key role in increasing patient engagement in their therapy, which can lead to better health outcomes in the long term.54
Anxiety levels were measured using the Beck Anxiety Inventory (BAI). Higher anxiety scores may negatively impact adherence to therapy, particularly through avoidance behaviors, forgetfulness, or an excessive focus on somatic symptoms.54,55
Overall, based on our results we can recommend the following interventions for patients taking antidepressant medication: (1) Since attitudes influence medication adherence, it is important to take these into account and take actions to improve. (2) As depressed patients have a slightly worse adherence, it is important that the doctor closely monitors not only the severity of the illness, but also the medication habits of the patients; (3) this is even more true for smokers and younger people. (4) Finally, it is also recommended to improve the doctor-patient relationship, as this also influences medication adherence.56–58 Based on our findings, more frequent meetings can contribute to the adherence of patients, therefore one specific suggestion might be that the prescription period of antidepressants should be re-evaluated and shortened.
The results of the study outline a practical recommendation to routinely assess medication-related beliefs in everyday care, as they directly affect patient cooperation and therapeutic decisions. In addition, it is important to ensure the continuity of the GP relationship, which facilitates the development of trust, the monitoring of psychosocial factors over time, and the possibility of personalized interventions. These elements may contribute to improving long-term adherence and strengthening patient-centered care.
The current research has some limitations worth highlighting. Although the initial aim was to analyze a representative sample within the Hungarian adult population, restricting the population to participants who were taking antidepressant medication, as outlined in the descriptive statistics, compromised that representativeness. As a result, the extent to which these findings can be generalized to the entire population is uncertain. Additionally, the items addressing financial and health status relied on subjective self-assessment, which may have introduced individual bias into the responses. Also, data were gathered after the COVID-19 pandemic, which may have impacted participants’ views on pharmacological treatment and the environmental factors influencing depression self-management.58,59
The impact of belief in harm on adherence is not only statistically relevant, but also deeply connected to patient trust, cultural attitudes, and healthcare communication. This is a point where quantitative results and patient experiences intersect.28
Various facets of doctor–patient communication, including patient satisfaction with doctor–patient communication, the specific content discussed, the style of communication, the comprehensive communication skills of doctors, and the duration of these conversations, were scrutinized. In general, the results suggest a promising link between effective doctor–patient communication and increased medication adherence and blood pressure control.60
Limitations
The limitations of the research were as follows: selection bias due to online panel (excludes digitally limited or illiterate adults; self-reported measures (risk of recall/social desirability bias); cross-sectional design (no causal inference); absence of antidepressant type/dose stratification and lack of adjustment for depression severity or comorbid anxiety–depression overlap. The study has several methodological limitations that may affect the interpretability of the results. The use of an online panel may result in selection bias by excluding adults with digital limitations or low literacy skills. Self-report measures are at risk of recall bias and socially desirable responding. The cross-sectional design does not allow for the investigation of causal relationships. Another limitation is that the study did not stratify by type and dose of antidepressants, and there was no adjustment for depression severity or anxiety-depression comorbidity. There were no illiterate participants.
Conclusion
The current study has identified that attitude to medication, depression level, smoking and doctor-patient relationship significantly are associated with adherence to antidepressant medication. In order to improve adherence, and thus the mental health of depressed patients, it is important that possible future interventions take these factors into account.
Redeeming antidepressants at least monthly is strongly associated with better adherence.
Based on the results provided, it is clear that monthly medication rotation is strongly associated with better adherence. The positive and significant coefficients indicate that patients who rotate their medications monthly are significantly more likely to adhere to the prescribed treatment than those who do so less frequently.
In practical terms, this means that regular, monthly medication rotation not only helps to follow the therapeutic process, but also probably reflects more conscious patient behaviour, better control and greater commitment. In contrast, less frequent rotations – for example, every two or three months – increase the risk of non-adherence, either due to forgetfulness or lack of motivation.
This suggests that regular redemption not only help follow the therapeutic process, but also probably reflects more conscious patient behavior, better control and greater commitment.
A practical recommendation of this study is to routinely assess medication-related beliefs in everyday care, as they directly affect patient cooperation and therapeutic decisions. Ensuring continuity of care is key to building trust, monitoring psychosocial factors over time, and implementing personalized interventions. Together, these factors can help promote long-term adherence and strengthen patient-centered care.
Ethical Approval
The study was conducted in accordance with the principles of the Declaration of Helsinki (World Medical Association). Ethical approval was obtained from the Scientific Research and Ethics Committee of the Medical Research Council in Hungary (approval number: BM/4912-3/2025). All participants received written information and provided informed consent prior to participation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Depressive disorder (depression). Available from: https://www.who.int/news-room/fact-sheets/detail/depression.
2. World Health Organization. Mental disorders. Available from: https://www.who.int/news-room/fact-sheets/detail/mental-disorders.
3. Gautam S, Jain A, Chaudhary J, Gautam M, Gaur M, Grover S. Concept of mental health and mental well-being, its determinants and coping strategies. Indian J Psychiatry. 2024;66(Suppl 2):S231–S244. doi:10.4103/indianjpsychiatry.indianjpsychiatry
4. Nour MO, Alharbi KK, Hafiz TA, et al. Prevalence of depression and associated factors among adults in Saudi Arabia: systematic review and meta-analysis (2000–2022). Depress Anxiety. 2023;2023:8854120. doi:10.1155/2023/8854120
5. Eurostat. Mental well-being and social support statistics. Available from: https://ec.europa.eu/eurostat/statistics-explained/index.php?oldid=569192&utm.
6. Rai D, Zitko P, Jones K, Lynch J, Araya R. Country- and individual-level socioeconomic determinants of depression: multilevel cross-national comparison. Br J Psychiatry. 2013;202(3):195–203. doi:10.1192/bjp.bp.112.112482.Epub
7. Economist impact. Depression in Europe: building resilience through awareness, improved access, integrated care, and parity of esteem. 2022. Available from: https://impact.economist.com/projects/depression-in-europe/files/janssen-depression_in_europe_report.pdf.
8. OECD (2023). Health at a Glance: Europe 2023. Mental health report: transforming mental health for all. Available from: https://www.oecd.org/en/publications/2023/11/health-at-a-glance-2023_e04f8239/full-report/mental-health_af4ca002.html.
9. la Torre J A-D, Vilagut G, Ronaldson A, et al. Prevalence and variability of depressive symptoms in Europe: update using representative data from the second and third waves of the European Health Interview Survey (EHIS-2 and EHIS-3). Lancet Public Health. 2023;8(11):e889–e898. doi:10.1016/S2468-2667(23)00220-7
10. Oblak L. Public mental health stigma and suicide rates across Europe. Front Public Health. 2025;13:1554072. doi:10.3389/fpubh.2025.1554072
11. Juhász G, Eszlari N, Pap D, Gonda X. Cultural differences in the development and characteristics of depression. Neuropsychopharmacol Hung. 2012;14(4):259–265.
12. Hagen D, Goldmann E. Gender differences in depression across Europe: a systematic review of cross-national studies. Eur J Public Health. 2019;29(Suppl 4):
13. Arias-de la Torre J, Vilagut G, Ronaldson A, et al. Prevalence and variability of current depressive disorder in 27 European countries: a population-based study. Lancet Public Health. 2021;6:e729–e738. doi:10.1016/S2468-2667(21)00047-5
14. Szőllősi GJ, Boruzs K, Karcagi-Kováts A, et al. Investigation of the relationship between incidence of mental disorders and economic growth among the Visegrad countries. Front Public Health. 2022;10:982716. doi:10.3389/fpubh.2022.982716
15. Antabe R, Antabe G, Sano Y, Batung E. Prevalence and socio-demographic correlates of probable depression and anxiety symptoms in Mozambique: a secondary data analysis. Plos Ment Health Prev. 2025;39:200440. doi:10.1371/journal.pmen.0000169
16. World Health Organization. Mental health: strengthening our response. Available from: https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-response.
17. Brown C, Battista DB, Bruehlman R, et al. Beliefs about antidepressant medications in primary care patients: relationship to self-reported adherence. Med Care. 2005;43(12):1203–1207. doi:10.1097/01.mlr.0000185733.30697.f6
18. Semahegn A, Torpey K, Manu A, Assefa N, Tesfaye G, Ankomah A. Psychotropic medication non-adherence and its associated factors among patients with major psychiatric disorders: a systematic review and meta-analysis. Syst Rev. 2020;9(1):17. doi:10.1186/s13643-020-1274-3
19. Marrero RJ, Fumero A, de Miguel A, Peñate W. Psychological factors involved in psychopharmacological medication adherence in mental health patients: a systematic review. Patient Educ Couns. 2020;103(10):2116–2131. doi:10.1016/j.pec.2020.04.030
20. Pedrosa-Naudín MA, Gutiérrez-Abejón E, Herrera-Gómez F, Fernández-Lázaro D, Álvarez FJ. Non-adherence to antidepressant treatment and related factors in a region of Spain: a population-based registry study. Pharmaceutics. 2022;14(12):2696. doi:10.3390/pharmaceutics14122696
21. Harsha NAY. Determinants of primary nonadherence to prescribed medications among adults in Hungary [PhD thesis]. Debrecen: University of Debrecen; 2020.
22. McElroy B, Walsh E. A happy home? Socio-economic inequalities in depressive symptoms and the role of housing quality in nine European countries. BMC Public Health. 2023;23(1):2203. doi:10.1186/s12889-023-17070-z
23. Statista. Depression in Europe - statistics & facts. Available from: https://www.statista.com/topics/12402/depression-in-europe/#topicOverview.
24. World Health Organization. Depressive disorder (depression). Available from: https://www.who.int/news-room/fact-sheets/detail/depression.
25. Data Pandas. Depression rates by country. Available from: https://www.datapandas.org/ranking/depression-rates-by-country.
26. Kornder N, Donner-Banzhoff N, Staudt I, Grede N, Becker A, Viniol A. Trials evaluating drug discontinuation: a scoping review sub-analysis focusing on outcomes and research questions. BMC Med Res Methodol. 2025;25(146). doi:10.1186/s12874-025-02597-z
27. Horne R, Chapman SCE, Parham R, Freemantle N, Forbes A, Cooper V. Understanding patients’ adherence-related beliefs about medicines prescribed for long-term conditions: a meta-analytic review of the necessity-concerns framework. PLoS One. 2013;8(12):e80633. doi:10.1371/journal.pone.0080633
28. Horne R, Weinman J, Hankins M. The beliefs about medicines questionnaire: the development and evaluation of a new method for assessing the cognitive representation of medication. Psychol Health. 1999;14:1–24. doi:10.1080/08870449908407311
29. Verhagen PA. Beliefs about medicine questionnaire. J Physiother. 2018;64(1):60. doi:10.1016/j.jphys.2017.04.006
30. Krauskopf K, Federman AD, Kale MS, et al. Chronic obstructive pulmonary disease illness and medication beliefs are associated with medication adherence. COPD. 2015;12:151–164. doi:10.3109/15412555.2014.922067
31. Topp M, Vestbo J, Mortensen EL. Psychometric properties of the COPD-specific beliefs about medicine questionnaire in an outpatient population: a Rasch-analysis. Chronic Obstr Pulm Dis. 2016;3:748–757. doi:10.15326/jcopdf.3.4.2016.0134
32. Otero ME, van den Reek JMPA, van de Kerkhof PCM, et al. Beliefs about medicines in patients with psoriasis treated with methotrexate or biologics: a cross-sectional survey study. Acta Derm Venereol. 2019;99:386–392. doi:10.2340/00015555-3108
33. Mostafavi F, Najimi A, Sharifirad G, Golshiri P. Beliefs about medicines in patients with hypertension: the instrument validity and reliability in Iran. Mater Sociomed. 2016;28:298–302. doi:10.5455/msm.2016.28.298-302
34. McCulley C, Katz P, Trupin L, et al. Association of medication beliefs, self-efficacy, and adherence in a diverse cohort of adults with rheumatoid arthritis. J Rheumatol. 2018;45(12):1636–1642. doi:10.3899/jrheum.171339
35. Bermingham M, Hayden J, Dawkins I, et al. Prospective analysis of LDL-C goal achievement and self-reported medication adherence among statin users in primary care. Clin Ther. 2011;33:1180–1189. doi:10.1016/j.clinthera.2011.07.007
36. Boruzs K, Dombrádi V, Sándor J, et al. Cross-cultural adaptation and lingual validation of the beliefs about medicines questionnaire (BMQ)-specific for cholesterol lowering drugs in the Visegrad countries. Int J Environ Res Public Health. 2020;17(20):7616. doi:10.3390/ijerph17207616
37. Boruzs K, Fekete Z, Dombrádi V, et al. Differences in beliefs about cholesterol-lowering medications among the Visegrad Group countries: a cross-sectional study. Front Public Health. 2021;9:645043. doi:10.3389/fpubh.2021.645043
38. Horne R, Weinman J. Self-regulation and self-management in asthma: exploring the role of illness perceptions and treatment beliefs in explaining non-adherence to preventer medication. Psychol Health. 2002;17(1):17–32. doi:10.1080/08870440290001502
39. Thompson K, Kulkarni J, Sergejew AA. Reliability and validity of a new medication adherence report scale (Mars) for the psychoses. Schizophr Res. 2000;42(3):241–247. doi:10.1016/S0920-9964(99)00130-9
40. Psychiatry. Medication Adherence Report Scale (Mars): a full guide for researchers and clinicians. 2025. Available from: https://resref.com/medication-adherence-report-scale-mars-a-full-guide-for-researchers-and-clinicians/.
41. Dohos D, Váradi A, Farkas N, et al. Hungarian linguistic, cross-cultural, and age adaptation of the patient satisfaction with health care in inflammatory bowel disease questionnaire (CACHE) and the medication adherence report scale (Mars). Children. 2022;9(8):1143. doi:10.3390/children9081143
42. Sheperis C, Drummond R, Jones K. Assessment Procedures for Counselors and Helping Professionals.
43. Rózsa S, Szádóczky E, Füredi J. Psychometric properties of the Hungarian version of the shortened beck depression inventory. Psychiatr Hung. 2001;16(4):379–397. doi:10.1080/08870440290001502
44. Headway. Compliance and documentation. How to use the beck anxiety inventory and interpret scores. 2025. Available from: https://headway.co/resources/beck-anxiety-inventory#what-is-the-beck-anxiety-inventory.
45. Nunnally JC. Psychometric Theory.
46. Thorneloe RJ, Griffiths CEM, Ashcroft DM, Cordingley L. The challenges of assessing patients’ medication beliefs: a qualitative study. BMC Health Serv Res. 2017;17:119. doi:10.1186/s12913-017-2020-y
47. De Las Cuevas C, Peñate W, Sanz EJ. Risk factors for non-adherence to antidepressant treatment in patients with mood disorders. Eur J Clin Pharmacol. 2014;70(1):89–98. doi:10.1007/s00228-013-1582-9
48. Lekic L, Pavlović B, Emina K. Adherence and medication adherence rating scale (Mars). Int J Innov Sci Res Technol. 2021;6(11):210–217.
49. Dicker R, Hodge B. The influence of the therapeutic alliance on treatment adherence. In: Pediatric Nonadherence. Cham: Springer; 2024:167–181.
50. Abukari K, Petrucka PM. A literature-based study of patient-centered care and communication in nurse-patient interactions: barriers, facilitators, and the way forward. BMC Nurs. 2021;20:158. doi:10.1186/s12912-021-00684-2
51. DiMatteo MR, Lepper HS, Croghan TW. Depression is a risk factor for noncompliance with medical treatment: meta-analysis of the effects of anxiety and depression on patient adherence. Arch Intern Med. 2000;160(14):2101–2107. doi:10.1001/archinte.160.14.2101
52. Schnoll RA, Lerman C. Current and emerging pharmacotherapies for treating tobacco dependence. Expert Opin Emerg Drugs. 2006;11(3):429–444. doi:10.1517/14728214.11.3.429
53. Sherman BW, Lynch WD. The association of smoking with medical treatment adherence in the workforce of a large employer. Patient Prefer Adherence. 2014;8:477–486. doi:10.2147/PPA.S60927
54. Beck AT, Epstein N, Brown G, Steer RA. An inventory for measuring clinical anxiety: psychometric properties. J Consult Clin Psychol. 1988;56(6):893–897. doi:10.1037/0022-006X.56.6.893
55. Perche PO, Singh R, Cook MK, et al. The patient-physician relationship and adherence: observations from a clinical study. J Drugs Dermatol. 2023;22(8):838–839. doi:10.36849/jdd.7103
56. Palmer GA, Dahlstrom A, Kingwell A, Van Sickle J. Beck Anxiety Inventory. Zeigler-Hill V, Shackelford TK. editors. Encyclopedia of Personality and Individual Differences. Springer. 2017. doi:10.1007/978-3-319-28099-8_5-1 :pp. 1–4
57. Zhang R, Lu X, Wu W, Shang X. Why do patients follow physicians’ advice? The influence of patients’ regulatory focus on adherence: an empirical study in China. BMC Health Serv Res. 2019;19:301. doi:10.1186/s12913-019-4127-9
58. Yang G, Zuo Y, Cheng H, Zhang L. How environmental perception influence depression and anxiety: the mediating role of social interaction. BMC Public Health. 2025;25(1):1216. doi:10.1186/s12889-025-21627-5
59. Gao YI, Shen LX, Hou XM, Si SP, Zhu HH, Shi ZL. The factors influencing self-management in patients with depression: a qualitative research from China. BMC Psychiatry. 2025;25(1):48. doi:10.1186/s12888-025-06489-w
60. Zeng J, Gao Y, Hou C, Liu T. The impact of doctor-patient communication on medication adherence and blood pressure control in patients with hypertension: a systematic review. PeerJ. 2024;12:e18527. doi:10.7717/peerj.18527
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.