Back to Journals » Journal of Pain Research » Volume 19
Psychometric Properties of a Smartphone Application for Measuring Shoulder Active Range of Motion in Individuals with and without Shoulder Pain and Mobility Deficits
Authors Aafreen A ![]() , Khan AR
, Khan AR ![]() , Ahmad A
, Ahmad A ![]() , Alshehre YM
, Alshehre YM ![]() , Alshehri MM
, Alshehri MM ![]() , Shaphe MA
, Shaphe MA ![]() , Aldhahi MI
, Aldhahi MI ![]()
Received 13 November 2025
Accepted for publication 7 March 2026
Published 18 March 2026 Volume 2026:19 581403
DOI https://doi.org/10.2147/JPR.S581403
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor King Hei Stanley Lam
Aafreen Aafreen,1 Abdur Raheem Khan,2 Ausaf Ahmad,3 Yousef M Alshehre,1 Mohammed M Alshehri,4 Mohammad Abu Shaphe,4 Monira I Aldhahi5
1Department of Health Rehabilitation Sciences, Faculty of Applied Medical Sciences, University of Tabuk, Tabuk, Saudi Arabia; 2Department of Physiotherapy, Integral University, Lucknow, India; 3Department of Community Medicine, Kalyan Singh Government Medical College Bulandshahr, Bulandshahr, UP, India; 4Physical Therapy department, College of Nursing and Health Sciences, Jazan University, Jazan, Saudi Arabia; 5Department of Rehabilitation Sciences, College of Health and Rehabilitation Sciences, Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia
Correspondence: Abdur Raheem Khan, Department of Physiotherapy, Integral University, Lucknow, India, Email [email protected]
Background: Shoulder pain and mobility deficits impact functional capacity, necessitating the use of reliable tools to assess active range of motion (AROM) for evaluation and monitoring outcomes. This study evaluated the psychometric properties of a smartphone application (PhysioMaster) for measuring shoulder AROM in individuals with and without shoulder pain and mobility deficits.
Methods: This cross-sectional study included a cohort of 90 participants, comprising 45 individuals with and 45 without shoulder pain and mobility deficits, recruited through convenience sampling from the Physiotherapy Outpatient Department at Integral University, Lucknow. The participants were aged 20– 50 years. Measurements of AROM, including flexion, extension, abduction, external rotation, and internal rotation, were performed using the PhysioMaster application. The readings were compared using a universal goniometer (gold standard). Reliability and criterion validity assessments were conducted by three physical therapists. We calculated the intraclass correlation coefficients (ICC), standard error of measurement (SEM), and minimal detectable change (MDC), and conducted a Bland–Altman analysis to evaluate the agreement between the measurements.
Results: The PhysioMaster application demonstrated excellent intra-rater reliability (ICC ≥ 0.944) and good-to-excellent inter-rater reliability (ICC ≥ 0.742) for most movements, although the reliability was slightly reduced for abduction and external rotation in the group without pain, with one isolated measurement showing poor reliability due to sample homogeneity. The criterion validity was high (ICC ≥ 0.944), except for abduction and external rotation in pain-free individuals, which ranged from 0.742 − 0.886. Biases were minimal (< 1°), with 95% confidence intervals (CIs) including zero. The SEM and MDC ranged from 1.1 °to 2.6 °and 2.9° to 4.7°, respectively.
Conclusion: The PhysioMaster smartphone application demonstrated robust psychometric properties for evaluating shoulder AROM in young and middle-aged adults (aged 20– 50 years) with and without mild-to-moderate shoulder pain and mobility deficits. Within this population, the application serves as a valid and reliable alternative the universal goniometer.
Keywords: psychometric properties, smartphone application, shoulder AROM, shoulder mobility deficits, universal goniometer
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Goyal has been published for this article.
Introduction
Shoulder active range of motion (AROM) is important for diagnosing pain and mobility deficits, monitoring rehabilitation progress, and evaluating treatment efficacy.1 Traditional tools, such as handheld goniometers and inclinometers, are frequently used in clinical practice owing to their popularity. Nevertheless, their measurement accuracy and reliability may be limited by inter- and intra-rater variability, which can produce inconsistencies in the evaluation process.2 The limitations associated with these traditional tools have prompted the use of more objective approaches, including smartphone applications that employ built-in sensors.3 These applications often utilize smartphone accelerometers and gyroscopes to provide digital angle measurements, potentially reducing the subjective errors associated with manual goniometry.4 The integration of smartphone technology into clinical assessment tools offers significant advantages, including enhanced objectivity, cost-effectiveness, and ease of access, making them increasingly viable for widespread adoption.5,6 However, despite the growing popularity of these digital tools, it remains crucial to rigorously validate their psychometric properties against established standards to ensure their accuracy and reliability in diverse clinical populations.7 This rigorous validation is essential to confirm their utility across various conditions and patient demographics, ensuring that the measurements are consistent and clinically meaningful.2,8 The assessment of shoulder joint mobility is also advantageous for identifying structural impairment, understanding functional limitations, and guiding clinical decision-making across different patient groups.9 The precise quantification of shoulder AROM is essential because of its biomechanical complexity, which involves the coordinated movement of the glenohumeral and scapulothoracic articulations. This complexity creates significant challenges in accurately assessing using traditional tools.10 Conventional measurements, including goniometry, are frequently used in the initial, dynamic, and final stages of assessment to document the data.11 Despite their widespread use, the reliability of traditional goniometric measurements can be compromised by factors such as inconsistent anatomical landmark identification, varied examiner experience, and subjective interpretation of endpoints.12 These limitations emphasize the need to develop more objective and reliable methods for assessing the joint range of motion.2 Consequently, smartphone applications incorporating machine learning offer a promising solution for the automated and objective assessment of the range of motion, addressing the limitations of traditional methods.13,14
The literature review revealed a notable gap in the current research, as the psychometric properties of the PhysioMaster smartphone application for assessing shoulder AROM in individuals with and without shoulder pain and mobility deficits have not yet been reported in the literature. Although several studies have examined various tools and applications, the psychometric properties of the PhysioMaster application remain to be established.15–17 To address this gap, this study aimed to determine the psychometric properties of the PhysioMaster smartphone application in individuals with and without shoulder pain and mobility deficits. We hypothesized that this application would demonstrate robust psychometric properties for measuring shoulder AROM in both populations. This investigation is particularly relevant given that an accurate AROM assessment is essential for effective clinical decision-making, especially considering the complex biomechanics of the shoulder joint.16 Furthermore, the validation of such smartphone applications is essential for advancing cost-effective, accessible, and efficient clinical assessments, enabling tailored rehabilitation strategies, and accurately monitoring treatment outcomes.18,19
Materials and Methods
Study Design
This study employed a cross-sectional design to assess the psychometric properties of the PhysioMaster application, adhering to the Guidelines for Reporting Reliability and Agreement Studies and COnsensus-based Standards for the Selection of Health Measurement INstruments (COSMIN) recommendations.20
The shoulder joint was selected as the primary focus of this investigation due to its complex biomechanics and high clinical relevance, which present unique challenges for accurate objective assessment. Shoulder pain and mobility deficits are common musculoskeletal disorders. The multiplanar movement of the glenohumeral joint and scapulothoracic rhythm pose challenges for measurement. AROM is preferred over PROM for several reasons. AROM reflects functional capacity, including muscle strength, motor control, and pain tolerance, all of which are critical for rehabilitation. AROM assessment can be conducted independently, thereby enhancing the use of smartphone applications in rehabilitation.
Study Setting
Participants with shoulder pain were recruited between January and July 2024 at the Department of Physiotherapy and Orthopaedics at the Integral Hospital and Research Centre, part of the Integral University in Lucknow, Uttar Pradesh, India. Participants without shoulder pain were recruited from the Integral University.
Participants
The sample size was calculated using the following formula to estimate the minimum sample size required to detect a significant Intraclass Correlation Coefficient (ICC) in psychometric property studies:
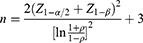
where ρ is the expected ICC (0.60), Z1−α/2, is the z-score corresponding to the significance level (1.96 for α = 0.05), and Z1−β is the z-score for the desired power (0.84, 80% power). The calculation yielded a minimum sample size of 90 participants. Participants were recruited using convenience sampling methods.21,22 The total number of participants in this study was 90, and who were split evenly into two groups: 45 participants with shoulder pain and mobility deficits (Group A) and 45 healthy individuals without shoulder pain and mobility deficits (Group B).
Participants aged 20–50 years were included to represent young and middle-aged adults of both gender, who are the most common demographic seeking intervention for shoulder pain and mobility deficits related to occupational, recreational and daily activities. This age range was chosen to minimize the confounding effects of age-related degenerative changes seen in older adults and to ensure the biomechanical stability of shoulder motion during measurement.23
They also needed to be able to walk independently and have normal or corrected-to-normal hearing and vision. Group A included individuals with shoulder pain and mobility deficits for a minimum of one month. Eligibility was limited to those with mild to moderate shoulder pain (VAS score 2–6/10) because participants with severe pain (VAS >7/10) show protective behaviors that alter movement patterns and confound reliability; individuals with mild to moderate pain can complete full ROM assessment; and this pain range represents common clinical presentation in outpatient department. Capsular pattern restriction (external rotation > abduction >internal rotation) was assessed based on the difficulty in performing daily activities (overhead activity, dressing, grooming, and reaching). ADL difficulty was evaluated through patient interviews using activity assessments, self-reported limitation severities, and clinical observations during examinations. Although we did not use a validated disability questionnaire as an inclusion criterion, functional limitations were clinically verified in this study. The VAS was used for pain characterization and inclusion classification, with scores excluded from psychometric analysis.
For Group B, the inclusion criteria were the absence of any history of shoulder pain or mobility deficit. The exclusion criteria were shoulder surgery, upper extremity surgery or injury within the past 12 months, recent interventions, cardiovascular or neurological disorders, cognitive impairment, vestibular or neuromuscular issues, and systemic arthritic conditions.
Ethical Approval
This study was approved by the Institutional Ethics Committee of the Integral University, Lucknow, India (reference number: IEC/IIMSR/2024/99). The study was conducted in accordance with the 1964 Declaration of Helsinki, and all participants provided written informed consent before the study began.24
Procedure
Each participant underwent a comprehensive evaluation that included demographic information and assessment of shoulder AROM. Pain intensity was measured using a visual analogue scale (VAS) for inclusion in Group A; however, these scores were not included in the final analysis. AROM was assessed using the PhysioMaster smartphone application and a universal goniometer to evaluate reliability and criterion validity across both groups.
Prior to testing, the participants were asked to remove watches, upper-body accessories, or tight clothing that could interfere with shoulder movements or device placement. Five shoulder movements (flexion, extension, abduction, external rotation, and internal rotation) were demonstrated to ensure familiarity with the procedure. A standardized body position was used throughout the study to minimize variability.
For flexion, extension, and abduction, the participants stood upright with their feet at shoulder width, arms relaxed at their sides, and their gaze directed forward. The smartphone was secured to the distal humerus using an armband. For external and internal rotation, the participants lay supine with the shoulder abducted at 90°, elbow flexed at 90°, and forearm in a neutral position. In this setup, a smartphone was attached to the elbow using an armband.
Before the measurement, a warm-up consisting of five repetitions of each movement was performed to reduce fatigue and enhance consistency. The participants were instructed to execute the movements in their usual, natural way. Each AROM movement was measured three times, and the mean value was used for analysis. The testing followed a fixed sequence, and the reliability was assessed within hours.25
The PhysioMaster application, developed by Trinus Laboratory, is a smartphone-based tool that utilizes integrated magnetometer and accelerometer sensors to measure the joint range of motion.26 The device was placed on the distal segment of the limb, and the motion trajectories were recorded.4 Proprietary algorithms process raw data to accurately calculate joint angles and offer portable and precise measurement methods.3
All measurements were conducted using identical smartphone devices (iPhone 13, iOS 17.7, integrated gyroscope, and accelerometer sensors) to eliminate inter-device variability. Prior to each measurement session, all devices were calibrated using the internal calibration protocol of the PhysioMaster application, with calibration verified by maintaining the measurement tolerance within ±1°. The use of a single smartphone model enhanced measurement consistency and reproducibility.
The selection of the PhysioMaster application for this study was based on several practical and methodological considerations of the app. Primarily, the application is freely accessible on both Android and iOS platforms, facilitating clinical implementation. Additionally, unlike many proprietary devices, PhysioMaster does not require costly subscriptions or specialized equipment beyond a standard smartphone and armband. Furthermore, its user interface is intuitive and requires minimal training compared with more complex motion analysis systems. The authors declare no financial relationships or conflicts of interest with regards to the application developers.
In contrast, the universal goniometer, a conventional mechanical tool, measures joint angles by aligning its arms with the anatomical landmarks of the proximal and distal segments, thereby providing a visual reading of angular displacement.27,28 Standardized positioning and landmark identification were used to ensure consistency in all the goniometric measurements.25
The AROM was measured in the standing (for flexion, extension, and abduction) and supine (for internal and external rotation) positions.29 Smartphone placement and measurement protocols were consistently applied to all the participants.30
Three physical therapy professionals underwent three hours of training to standardize goniometer and smartphone application use. They practiced identifying anatomical landmarks and performed shoulder AROM measurements on each other to ensure the technique’s consistency and accuracy. This rigorous training process aimed to minimize measurement variability and enhance the internal validity of the collected data.2 This meticulous training process is critical, as inter-rater reliability is a common challenge in goniometry, with reported errors ranging from 5° to 10°, even among experienced clinicians.7
Reliability and Validity Procedures
To assess inter- and intra-rater reliability, three examiners independently measured AROM using a smartphone application in separate rooms, blinded to each other’s measurements. Each examiner was accompanied by a paired observer to assist with data recording.
Each examiner recorded three repetitions per movement, rotating the rooms clockwise so that each participant was evaluated by all examiners. For criterion validity, the same protocol was applied, using a universal goniometer. This design facilitated a comprehensive comparison between the smartphone application and the gold-standard goniometer while also evaluating measurement consistency among different raters and over time.
Statistical Analysis
Descriptive statistics (mean ± SD) were used to summarize the participant characteristics (age, gender, height, weight, and body mass index (BMI)). The Kolmogorov–Smirnov test was used to assess the normality of the data. Independent t-tests and chi-square tests were used to compare the characteristics of the groups. ICCs with 95% confidence intervals (CIs) were used to evaluate interrater and intrarater reliability, classified as excellent (≥0.90), good (0.75–0.89), fair (0.50–0.74), or poor (<0.50). The standard Error of Measurement (SEM) was calculated as SEM = SD × √(1 – ICC), and the Minimal Detectable Change (MDC) was calculated as MDC = 1.96 × √2 × SEM. Criterion validity was assessed using the Pearson’s correlation coefficients. All analyses were performed using SPSS 16.0 (SPSS, Chicago, IL, USA).
Results
Table 1 presents the demographic characteristics of the participants in Groups A and B. The mean age of participants in Group A was significantly higher than that of Group B (31.96 ± 8.61 vs. 26.07 ± 3.24 years, p < 0.001). Similarly, a statistically significant difference was observed in BMI, with Group A showing a higher mean BMI compared to Group B (24.91 ± 2.84 vs. 23.80 ± 2.31 kg/m2, p = 0.04).
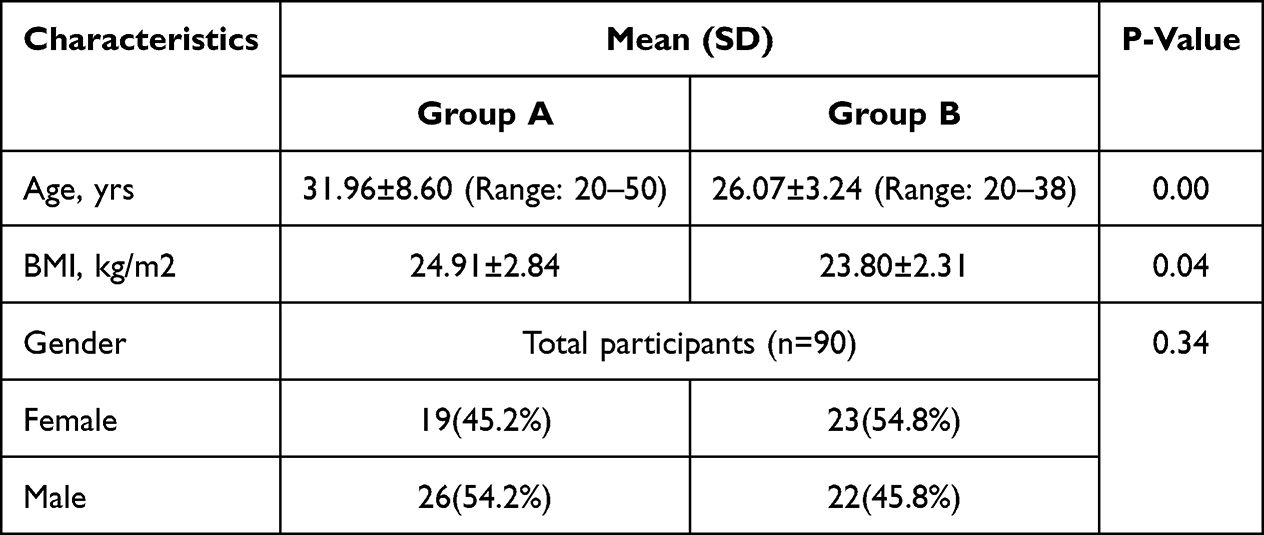 |
Table 1 Demographic Characteristics of Study Participants |
With respect to gender distribution, 45.2% of females were in Group A and 54.8% in Group B, whereas 54.2% of males were in Group A and 45.8% in Group B. The difference in gender distribution between the two groups was not statistically significant (p = 0.34).
Table 2 summarizes the inter-rater reliability of the smartphone application for AROM measurements by Raters 1, 2, and 3 in Groups A and B. Group A exhibited, excellent interrater reliability was observed across all movements, with intraclass correlation coefficients (ICCs) ranging from 0.966 to 0.998. The standard error of measurement (SEM) and minimal detectable change (MDC) values remained low, indicating high measurement precision. In Group B, the ICCs were slightly lower but still demonstrated good to excellent reliability (ranging from 0.799 to 0.971), with flexion and extension showing the highest consistency among raters. Overall, the findings support a strong inter-rater agreement, particularly in Group A, suggesting that the smartphone application provides reliable measurements across different raters.
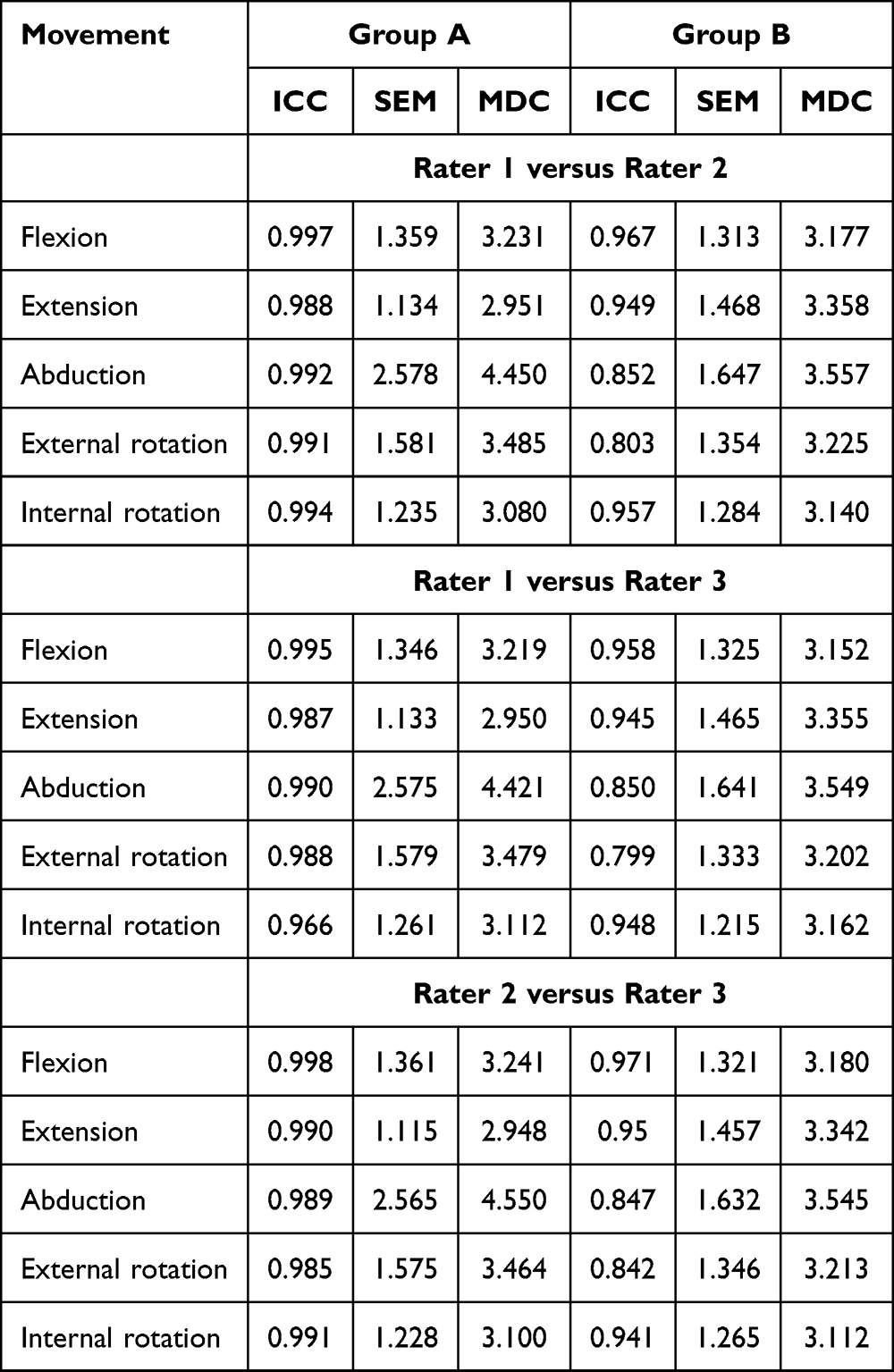 |
Table 2 Inter-Rater Reliability of Smartphone Application by Rater 1, Rater 2 and Rater 3 for Group A and Group B |
Table 3 demonstrates strong intra-rater reliability for each rater across the three measurement sets (Set 1, Set 2, and Set 3), for smartphone-based AROM measurements, with predominantly excellent (≥0.90) ICCs for raters and movements in Group A, indicating high repeatability despite pain-related variability. In Group B, reliability was mostly good to excellent, although outliers, such as Rater 2 abduction (ICC=0.032), suggested minor inconsistencies, possibly due to low variability in the norms. Low SEM/MDC values confirmed clinical precision, complementing the inter-rater excellence in Table 3 and affirming the app’s overall reliability.
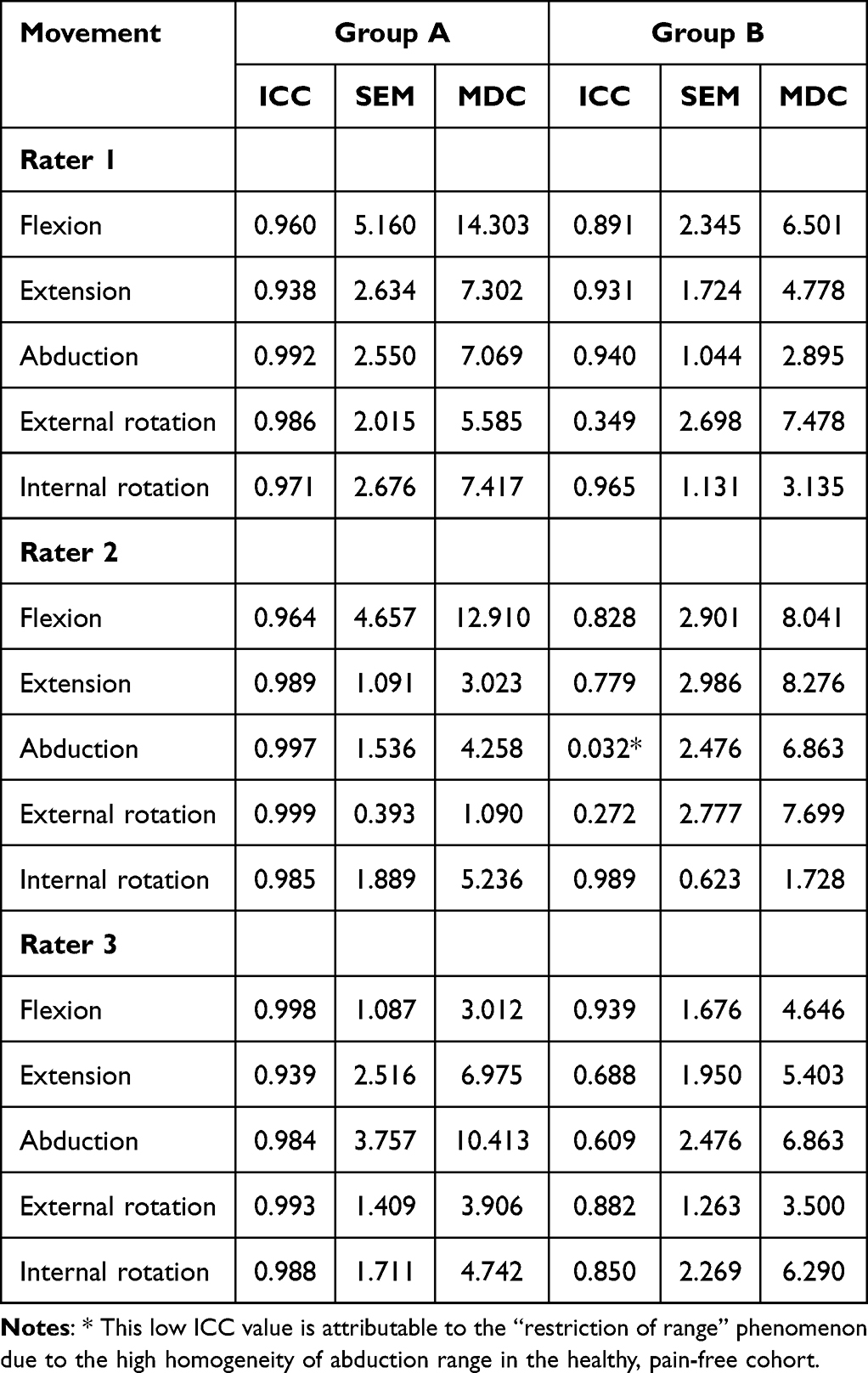 |
Table 3 Intra-Rater Reliability of Smartphone Application by Rater 1, Rater 2, and Rater 3 for Groups A and B |
Table 4 presents the criterion validity of the smartphone application by comparing the AROM measurements from raters 1, 2, and 3 with those obtained using a goniometer in groups A and B. In group A, excellent validity was observed across all movements, with ICCs ranging from 0.984 to 0.999, and low SEM and MDC values indicating high agreement and measurement precision. In Group B, the validity remained acceptable, with ICCs ranging from 0.798 to 0.985. Flexion and internal rotation showed the strongest agreement with the goniometer values across all raters, whereas slightly lower ICCs were noted for external rotation and abduction in Group B. Overall, these findings support the criterion validity of the smartphone application, particularly in Group A.
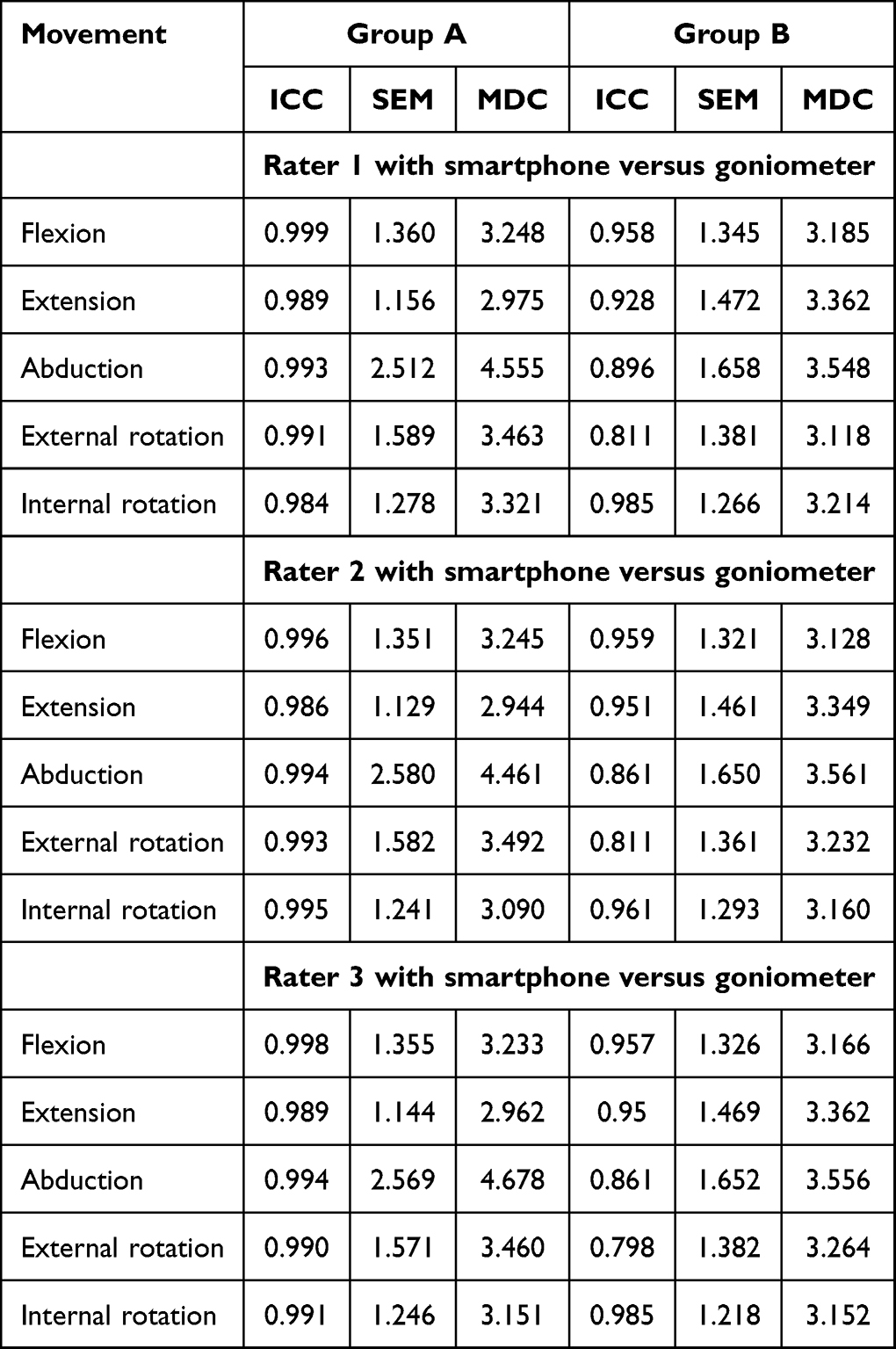 |
Table 4 Criterion Validity Measured by Rater 1, Rater 2 and Rater 3 with Smartphone versus Goniometer for Group A and Group B |
Table 5 presents the results of the Bland–Altman analysis comparing the AROM measurements obtained using the smartphone application with those obtained using the universal goniometer in Group A and Group B across all raters. In both groups, the mean bias values for all movements were small, ranging from approximately −0.67° to 0.97°, indicating minimal systematic differences between the two measurement methods. The 95% confidence intervals (CIs) for the limits of agreement were narrow across most movements, suggesting good agreement between smartphone and goniometer measurements. Group A generally showed slightly tighter limits and less variability than Group B. Overall, the Bland–Altman results support the clinical agreement and interchangeability of the smartphone application with the traditional goniometer across all raters and shoulder movements (Figure 1).
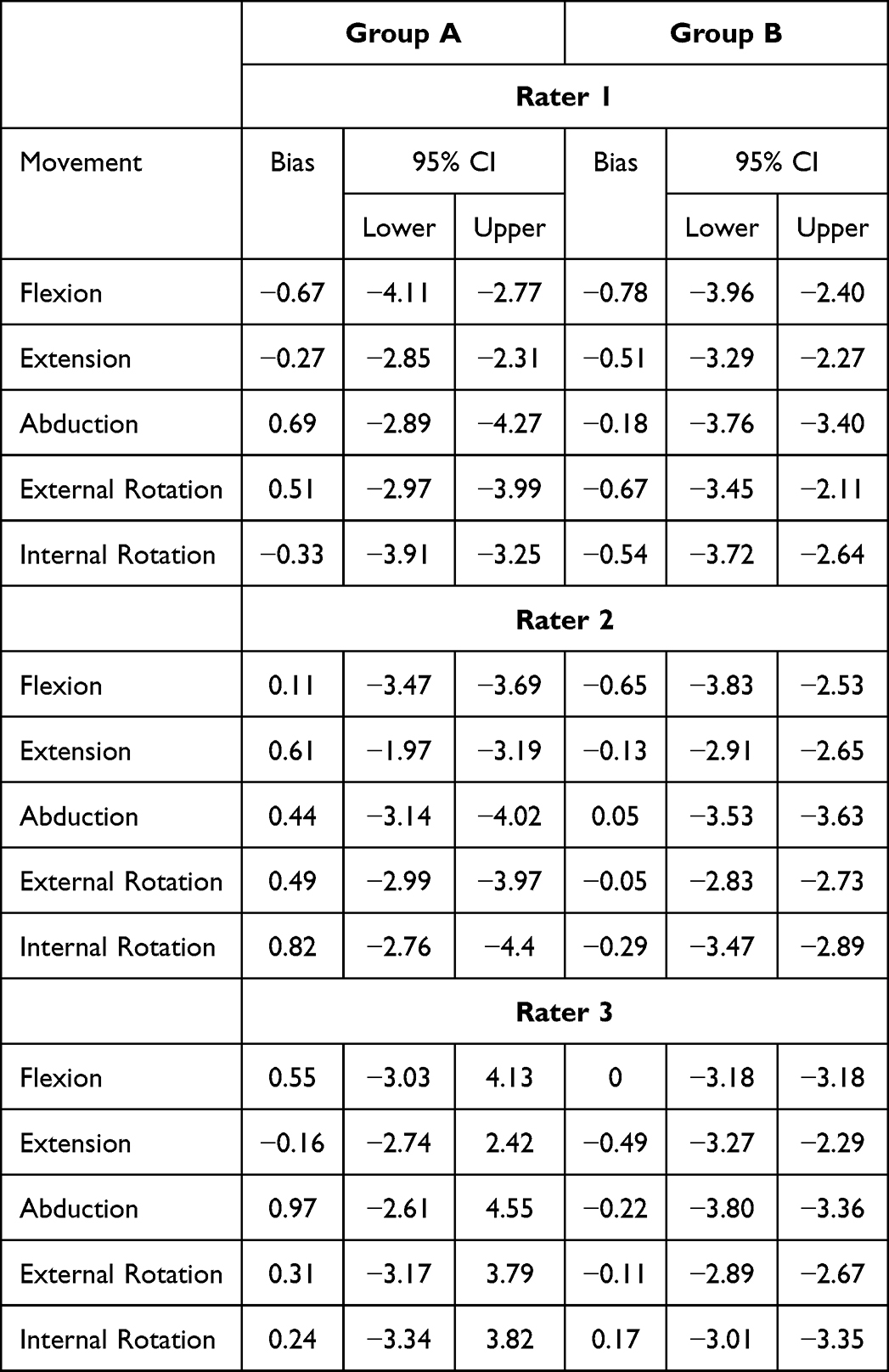 |
Table 5 Bland-Altman Analysis: Smartphone versus Universal Goniometer |
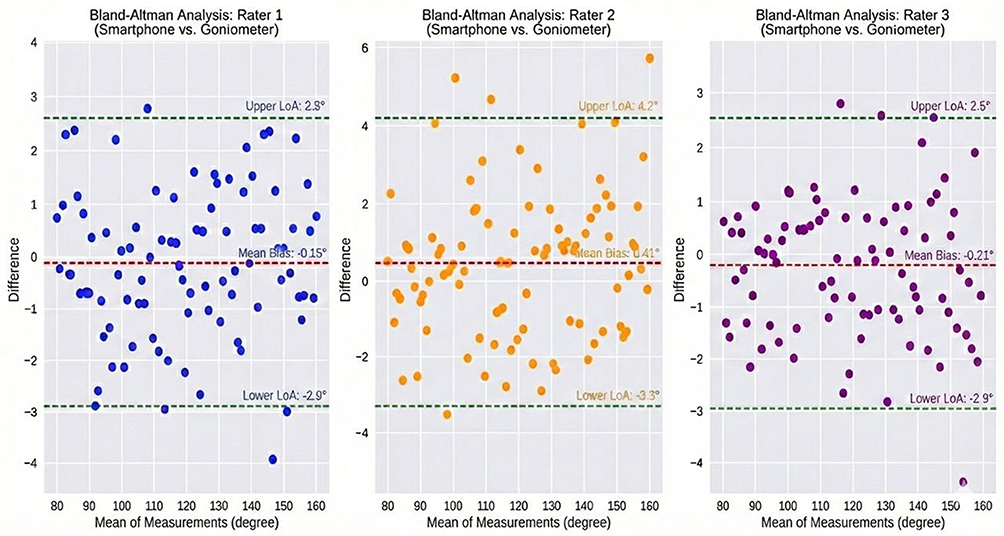 |
Figure 1 Bland–Altman Plot indicating mean difference and 95% limits of agreement between measurements from the smartphone application (PhysioMaster) and goniometer for shoulder active range of motion (°) in Group A and B. |
Discussion
This study aimed to evaluate the psychometric properties, specifically inter- and intra-rater reliability, criterion validity, and agreement of the smartphone application (PhysioMaster) for assessing shoulder AROM in individuals with and without shoulder pain and mobility deficits. The findings indicate that the smartphone application (PhysioMaster) consistently demonstrated good to excellent inter-and intra-rater reliability, as well as criterion validity, in individuals with and without shoulder pain and mobility deficits, supporting its clinical applicability in shoulder AROM assessments. Bland–Altman analysis further confirmed the agreement between the smartphone application (PhysioMaster) and the universal goniometer, with small biases and narrow limits of agreement.
Consistent with this hypothesis, ICCs across both groups were in the good to excellent range, accompanied by low standard errors of measurement (SEM) and minimal detectable change (MDC). These psychometric properties indicate that the smartphone application (PhysioMaster) is sensitive to clinically meaningful differences in shoulder AROM measurements. These results further underscore the accuracy of the PhysioMaster application in detecting subtle variations in shoulder AROM, making it reliable for both clinical use and patient self-monitoring purposes. Previous research supports the reliability and validity of smartphone-based goniometry for measuring the range of motion, with studies reporting good agreement with traditional methods and high inter-rater reliability.9,12,31,32
Group comparisons revealed demographic differences that may have influenced the results. Specifically, Group A participants were significantly older and had higher BMIs than Group B participants. Although gender distribution did not differ significantly, previous research has shown that age and BMI may affect shoulder biomechanics and ROM reliability due to variations in joint flexibility and muscle function.10,33 These variables may have contributed to the more consistent measures observed in Group A. In contrast, the younger age and lower BMI in Group B might indicate a cohort with potentially greater joint flexibility or different pain compensation strategies, which could affect the consistency of AROM measurements.34
This study extends the existing literature by confirming the reliability and validity of smartphone-based and digital inclinometers for assessing joint mobility.35 These tools offer practical advantages over traditional goniometry, which is subject to examiner skill and interrater variability. By including both symptomatic and asymptomatic individuals and implementing a standardized rater training protocol, this study enhanced internal validity and increased generalizability beyond that of studies limited to healthy cohorts or single-rater designs. However, it is important to acknowledge that the accuracy of smartphone goniometers can be influenced by the quality of the inertial sensors within the device, with older smartphone models potentially yielding less reliable measurements than newer ones.33 Moreover, device-specific errors in accelerometry and gyroscopes, even within modern smartphones, can introduce measurement inaccuracies that require careful consideration and potential calibration to ensure data integrity.33
While the application generally demonstrated good reliability, a notable exception was observed in Group B for Rater 2’s abduction measurements (ICC = 0.032). This isolated lack of reliability likely results from the “restriction of range” phenomenon, where the high homogeneity of abduction values in healthy, pain-free participants artificially depresses the ICC calculation. Importantly, despite this statistical anomaly, the absolute measurement error (SEM) for this measurement remained low (as shown in Table 3), confirming that the issue is primarily a statistical consequence of sample homogeneity rather than an indication of poor clinical precision. Additionally, the large arc of motion during full abduction in healthy individuals may have introduced soft tissue artifacts or minor sensor displacement which were not present in the restricted movements of the symptomatic group. In contrast, symptom-related motion constraints in Group A likely produced more predictable and consistent movement patterns, thereby enhancing the reproducibility of measurements. These findings are consistent with those of previous studies indicating that restricted motion due to pain or pathology may reduce within-subject variability, thereby improving reliability.2 Minor inconsistencies in Group B, particularly during abduction and external rotation, may also result from challenges in maintaining consistent device placement or accurately identifying anatomical landmarks through soft tissue. Additional factors, such as reduced scapular stabilization, disturbances in scapulohumeral rhythm, muscular imbalances, or lower examiner alertness during pain-free assessments, could have contributed to these discrepancies.35–37
This study provides new insights into the clinical utility of smartphone-based tools in settings where access to traditional instruments or experienced clinicians may be limited. The integration of such applications aligns with broader trends in digital health, offering adaptable and user-friendly options for both clinicians and patients. In addition to reducing the clinical workload, these tools enable patients to track their rehabilitation progress and contribute objective data to support collaborative clinical decision-making.
While previous research has shown that smartphone applications can consistently measure shoulder mobility, this study emphasizes the need for tool-specific validation.3,12 Performance variability across applications remains a concern, underscoring the importance of psychometric analyses tailored to each tool.38,39 The PhysioMaster application addresses the ongoing need for accessible, reliable, and cost-effective measurement solutions, particularly considering the limitations associated with traditional goniometry.
However, this study had some limitations. The generalizability of these findings is constrained by the single-center recruitment. In addition, this study assessed only AROM; passive mobility and functional assessments were not included in the study. Furthermore, intra-rater reliability was evaluated over a short-term interval, and all raters were professional clinicians, which may not fully reflect their performance in real-world clinical settings. We used a single smartphone model to ensure validity; however, validation may be required for other models with different sensors and systems. Clinicians should exercise caution when applying these findings to other devices without prior validation. Future studies should explore the impact of rater experience and extend the validation to a broader range of clinical populations and settings. Longitudinal studies are also needed to assess the responsiveness of the PhysioMaster application over time, particularly in term of monitoring rehabilitation outcomes. Further research could incorporate machine learning to enhance landmark detection, reduce user-dependent variability and evaluate the performance of the tool across diverse age groups and cultural contexts. Additionally, the establishment of standardized protocols for device positioning and measurement procedures will be critical for improving the reliability and facilitating cross-study comparisons.
Conclusion
The findings of this study demonstrate that the PhysioMaster smartphone application is a valid and reliable tool for measuring the active range of motion of the shoulder in young and middle-aged adults (20–50 years) with or without mild- to- moderate shoulder pain and mobility deficits. The application showed excellent inter-rater reliability and strong criterion validity compared with the universal goniometer, with minimal measurement error and strong agreement across raters and measurement sets. These results support the clinical utility of this application as a practical, accessible, and accurate alternative to traditional goniometry. Its portability and ease of use make it particularly valuable in outpatient settings, remote assessments, and tele-rehabilitation programs. Future studies should explore its responsiveness to changes over time, its application in broader clinical populations, and functional movement assessments.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Ethical Committee of Integral University, Lucknow, India (reference number: IEC/IIMSR/2024/99).
Data Sharing Statement
The data presented in this study are available upon reasonable request from the corresponding author.
Acknowledgments
We would like to thank Princess Nourah bint Abdulrahman University for supporting this project through Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2026R286), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia. The authors are also grateful to the Faculty of Medicine and Health Sciences, Integral University, India, for the scientific support to this research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2026R286), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Disclosure
The authors declare no conflicts of interest. The funders had no role in the study design, data collection, data analysis, data interpretation, manuscript writing, or decision to publish the results.
References
1. Kelley MJ, Shaffer MA, Kuhn JE, et al. Shoulder pain and mobility deficits: adhesive capsulitis. J Orthop Sports Phys Ther. The Journal of Orthopaedic and Sports Physical Therapy. 2013;43(5):A1–13. doi:10.2519/jospt.2013.0302
2. Riddle DL, Rothstein JM, Lamb RL. Goniometric reliability in a clinical setting. Shoulder measurements. Phys Ther. 1987;67(5):668–673. doi:10.1093/ptj/67.5.668
3. De Baets L, van der Straaten R, Matheve T, Timmermans A. Shoulder assessment according to the international classification of functioning by means of inertial sensor technologies: a systematic review. Gait Posture. 2017;57:278–294. doi:10.1016/j.gaitpost.2017.06.025
4. Kaszyński J, Baka C, Białecka M, Lubiatowski P. Shoulder range of motion measurement using inertial measurement unit–concurrent validity and reliability. Sensors. 2023;23(17):7499. doi:10.3390/s23177499
5. Mohammad WS, Elattar FF, Elsais WM, AlDajah SO. Validity and Reliability of a Smartphone and Digital Inclinometer in Measuring the Lower Extremity Joints Range of Motion. Monten J Sports Sci Med. 2021;10(2). doi:10.26773/mjssm.210907
6. Aafreen A, Khan A, Ahmad A, et al. Clinimetric properties of a smartphone application to measure the craniovertebral angle in different age groups and positions. Heliyon. 2023;9(9):e19336. doi:10.1016/j.heliyon.2023.e19336
7. Pereira LC, Rwkabayiza S, Lécureux E, Jolles BM. The knee smartphone-application goniometer is a more reliable tool than the standard goniometer in acute orthopaedic settings. Physiotherapy. 2015;101:e1192–3. doi:10.1055/s-0036-1584184
8. Ganokroj P, Sompornpanich N, Kerdsomnuek P, Vanadurongwan B, Lertwanich P. Validity and reliability of smartphone applications for measurement of Hip rotation, compared with three‐dimensional motion analysis. BMC Musculoskelet Disord. 2021;22(1):166. doi:10.1186/s12891-021-03995-2
9. Kiatkulanusorn S, Luangpon N, Srijunto W, et al. Analysis of the concurrent validity and reliability of five common clinical goniometric devices. Sci Rep. 2023;13(1):20931. doi:10.1038/s41598-023-48344-6
10. Fleisig GS, Slowik JS, Daggett M, Rothermich MA, Cain Jr EL, Wilk KE. Active range of motion of the shoulder: a cross-sectional study of 6635 subjects. JSES Int. 2023;7(1):132–137. doi:10.1016/j.jseint.2022.09.008
11. Gliga AC, Neagu N, Szabo DA. Optimising the validity of shoulder range of motion evaluation: a comparative study. BRAIN. 2020;11:101. doi:10.18662/BRAIN/11.4SUP1/158
12. Shishani Y, Flocken J, Gobezie R. What Is the Accuracy of Shoulder Range of Motion Measurements on Physical Exam? Open J Orthoped. 2015;5(9):264–276. doi:10.4236/ojo.2015.59036
13. Moreira R, Teles A, Fialho R, et al. Can human posture and range of motion be measured automatically by smart mobile applications? Med Hypotheses. 2020;142:109741. doi:10.1016/j.mehy.2020.109741
14. Kusunose M, Inui A, Nishimoto H, et al. Measurement of shoulder abduction angle with posture estimation artificial intelligence model. Sensors. 2023;23(14):6445. doi:10.3390/s23146445
15. Riddle DL, Rothstein JM, Lamb RL. Goniometric reliability in a clinical setting. Shoulder Measurements Phys Ther. 1987;67(5):668–673. doi:10.1093/ptj/67.5.668
16. Correll S, Field J, Mickevicius G, Hutchinson H, Smoot B, Fitzsimmons A. Reliability and Validity of the Halo Digital Goniometer for Shoulder Range of Motion in Healthy Subjects. Int J Sports Phys Ther. 2018;13(4):707–714.
17. Rigoni M, Gill S, Babazadeh S, et al. Assessment of Shoulder Range of Motion Using a Wireless Inertial Motion Capture Device—A Validation Study. Sensors. 2019;19(8):1781. doi:10.3390/s19081781
18. Aafreen KA, Ahmad A, Khan AR, et al. Clinimetric properties of a smartphone application to measure the craniovertebral angle in different age groups and positions. Heliyon. 2023;9(9):e19336. doi:10.1016/j.heliyon.2023.e19336
19. Aldon-Villegas R, Ridao-Fernandez C, Torres-Enamorado D, Chamorro-Moriana G. How to assess shoulder functionality: a systematic review of existing validated outcome measures. Diagnostics. 2021;11(5):845. doi:10.3390/diagnostics11050845
20. Gagnier JJ, Lai J, Mokkink LB, Terwee CB. COSMIN reporting guideline for studies on measurement properties of patient-reported outcome measures. Qual Life Res. 2021;30(8):2197–2218. doi:10.1007/s11136-021-02822-4
21. Walter SD, Eliasziw M, Donner A. Sample size and optimal designs for reliability studies. Stat Med. 1998;17(1):101–110. doi:10.1002/(sici)1097-0258(19980115)17:1<101::aid-sim727>3.0.co;2-e
22. Bujang MA, Baharum N. A simplified guide to determination of sample size requirements for estimating the value of intraclass correlation coefficient: a review. Arch Orofac Sci. 2017;12(1):1–11.
23. Gill TK, Shanahan EM, Tucker GR, Buchbinder R, Hill CL. Shoulder range of movement in the general population: age and gender stratified normative data using a community-based cohort. BMC Musculoskelet Disord. 2020;21(1):676. doi:10.1186/s12891-020-03665-9
24. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053.
25. Hanks J, Myers B. Validity, reliability, and efficiency of a standard goniometer, medical inclinometer, and builder’s inclinometer. Int J Sports Phys Ther. 2023;18(4):989–996. doi:10.26603/001c.83944
26. Wadhwa M, Panchwan M, Arunmozhi R, Verma V, Singh S, Singh Sr S. Reliability and Criterion Validity of PhysioMaster Application for the Measurement of Cervical Range of Motion in Healthy Individuals. Cureus. 2024;16(11):e73723. doi:10.7759/cureus.73723
27. Dhage P, Naqvi WM, Arora SP, Kulkarni C. A reliability test for its efficacy in smartphone application for computing joint range of motion: a research protocol. Res Square. 2021. doi:10.21203/rs.3.pex-1551/v1
28. Hamersma DT, Hofste A, Rijken NH, of Rohé MR, Oosterveld FG, Soer R. Reliability and validity of the Microgate Gyko for measuring range of motion of the low back. Musculoskelet Sci Pract. 2020;45:102091. doi:10.1016/j.msksp.2019.102091
29. Tveitå EK, Ekeberg OM, Juel NG, Bautz-Holter E. Range of shoulder motion in patients with adhesive capsulitis; intra-tester reproducibility is acceptable for group comparisons. BMC Musculoskelet Disord. 2008;9(1):49. doi:10.1186/1471-2474-9-49
30. Shimizu H, Saito T, Shimoura K, et al. Validity and reliability of a smartphone application for self-measurement of active shoulder range of motion in a standing position among healthy adults. JSES Int. 2022;6(4):655–659. doi:10.1016/j.jseint.2022.04.005
31. Roldán-Jiménez C, Martin-Martin J, Cuesta-Vargas AI. Reliability of a smartphone compared with an inertial sensor to measure shoulder mobility: cross-sectional study. JMIR mHealth uHealth. 2019;7(9):e13640. doi:10.2196/13640
32. Cuesta-Vargas Á, Roldán‐Jiménez C. Validity and reliability of arm abduction angle measured on smartphone: a cross-sectional study. BMC Musculoskelet Disord. 2016;17(1):93. doi:10.1186/s12891-016-0957-3
33. Tombak Y. Do Comorbidities and Body Mass Index Influence Shoulder Pain, Disability and Joint Range of Motion? J Clin Med Kaz. 2024;21(4):52–58. doi:10.23950/jcmk/14973
34. Holzgreve F, Maurer-Grubinger C, Isaak J, et al. The acute effect in performing common range of motion tests in healthy young adults: a prospective study. Sci Rep. 2020;10(1):21722. doi:10.1038/s41598-020-78846-6
35. Soeters R, Damodar D, Borman N, et al. Accuracy of a smartphone software application compared with a handheld goniometer for measuring shoulder range of motion in asymptomatic adults. Orthop J Sports Med. 2023;11(7):23259671231187297. doi:10.1177/23259671231187297
36. Morrissey D, Morrissey MC, Driver W, King JB, Woledge RC. Manual landmark identification and tracking during the medial rotation test of the shoulder: an accuracy study using three-dimensional ultrasound and motion analysis measures. Man Ther. 2008;13(6):529–535. doi:10.1016/j.math.2007.07.009
37. Møller M, Attermann J, Myklebust G, et al. The inter-and intrarater reliability and agreement for field-based assessment of scapular control, shoulder range of motion, and shoulder isometric strength in elite adolescent athletes. Phys Ther Sport. 2018;32:212–220. doi:10.1016/j.ptsp.2018.04.005
38. Van den Hoorn W, Lavaill M, Cutbush K, Gupta A, Kerr G. Comparison of shoulder range of motion quantified with mobile phone video-based skeletal tracking and 3D motion capture—preliminary study. Sensors. 2024;24(2):534. doi:10.3390/s24020534
39. Kaur V, Makhija M, Phadke V. Reliability and concurrent validity of smartphone clinometer application for measuring scapular rotations in subjects with and without shoulder pain. J Sport Rehabil. 2023;32(8):926–931. doi:10.1123/jsr.2023-0005
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.