Back to Journals » Psychology Research and Behavior Management » Volume 15
Psychological Resilience as the Mediating Factor Between Stigma and Social Avoidance and Distress of Infertility Patients in China: A Structural Equation Modeling Analysis
Authors Zhao Q, Huangfu C, Li J, Liu H, Tang N
Received 18 December 2021
Accepted for publication 10 February 2022
Published 22 February 2022 Volume 2022:15 Pages 391—403
DOI https://doi.org/10.2147/PRBM.S354803
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Qing Zhao,1,* Chaoji Huangfu,2,* Junzheng Li,2 Huihui Liu,1 Nan Tang1
1School of Nursing, Lanzhou University, Lanzhou, Gansu, 730010, People’s Republic of China; 2Department of Infectious Disease Prevention and Control, Center for Disease Control and Prevention, Western Theater Command, Lanzhou, Gansu, 730020, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Nan Tang, Tel +86-18793111027, Email [email protected]
Background: Stigma, social avoidance and distress may seriously affect the quality of life of infertility patients. Psychological resilience has been proved to effectively combat psychological stress. This study aimed to explore the mediating role of psychological resilience between stigma and social avoidance and distress (SAD) in females with an unfulfilled wish for a child.
Methods: Stigma Scale, Social Avoidance and Distress Scale (SADS), and Psychological Resilience Scale were used to evaluate 266 females with infertility. Structural equation model was used to test the mediating effect of psychological resilience on the relationship between stigma and SAD.
Results: The SADS, stigma scores, and psychological resilience scores of 266 females with infertility were 13.36 ± 5.77, 77.84 ± 16.91, and 58.84 ± 12.24 points, respectively. The stigma scores were positively correlated with SADS, and negatively correlated with psychological resilience scores. The psychological resilience scores were negatively correlated with SADS. Psychological resilience played a partially mediating role between the stigma and SAD of infertility patients, and the mediating effect accounted for 25.5% of the total effect.
Conclusion: Psychological resilience had a partial mediating effect on the relationship between stigma and SAD, and could reduce the negative effect of stigma on the development of SADS. Therefore, positive psychological interventions improving psychological resilience might help to reduce stigma and improve SAD in infertility patients.
Keywords: infertility, stigma, psychological resilience, social avoidance and distress, mediating effect
Introduction
Infertility is a reproductive system disease and defined by failure to conceive after 1 year of unprotected regular sexual intercourse. Patients who have never been pregnant are called primary infertility.1 The secondary infertility is defined as follows: one partner in a couple has had at least one successful conception in the past, and is the incapability to conceive now.2 Previous study indicated that some external factors such as environmental pollution, life pressure and food safety, and some internal factors such as the increase of average childbearing age and the change of lifestyle will lead to the increase in the prevalence rate.3 Meanwhile, the prevalence of infertility in the world is rising, while the prevalence of infertility in China is expected to rise from 16.4% in 2019 to 18.2% in 2023.4,5 Infertility and related treatment process will bring serious psychological pressure to infertility patients and their families.
Patients with infertility in different cultures tend to experience a wide range of negative emotions, including anxiety, depression, stigma, social avoidance and distress (SAD).6–8 Stigma is a source of chronic stress, which may reduce the self-esteem and self-efficacy of infertile patients, and reduce their quality of life.9,10 SAD refers to people’s persistent and significant avoidance tendency to social interaction, as well as negative emotions and distress under social environment.11 Sometimes, having no children makes infertile patients be commented on and even criticized by the outside world, which leads to SAD.12 A study of 432 infertile women in the United States indicated that infertile people felt strongly stigmatized when they found themselves being talked about infertility by others, which further resulted in SAD.13
Stigma is defined as a negative sense of social difference from others, which makes these people excluded and isolated, have negative self-cognition, and show self-blame and self-derogation.14,15 Stigma could be divided into 3 different types including experienced stigma, perceived stigma and self-stigma. Experienced stigma is known as an external stigma, perceived stigma and self-stigma belong to internal stigma.16,17 Stigmatized persons may internalize perceived prejudices and develop negative feelings about themselves. This study aimed to investigate the individual perception and identification of discrimination among infertility females.18 Stigma is very common in infertile patients, and it is believed to be one of the most common features of the disease.19 Individuals with high levels of stigma are more likely to lack positive coping measures and have higher levels of social anxiety.17,20 Stigma can lead to inferiority, loneliness, self-blame and self-derogation in interpersonal communication.21 Infertile patients often take the form of self-closure and marginalization to avoid social activities, and then appear to be a more serious SAD phenomenon.13,22
Psychological resilience refers to people’s resilience in the face of difficulties and setbacks, which is a dynamic process affected by life events and challenges.23 The patients with low levels of psychological resilience tend to adopt avoidance methods to cope with difficulties. On the contrary, people with higher psychological resilience tend to have stronger positive social orientation, and can actively participate in social activities.24 In the face of adversity or stress events, patients with high levels of psychological resilience can have a good attitude to accept the incurability of the disease, and can actively face other people’s discrimination, rejection and disgust, have less negative emotions and less stigma.25 There are many positive impacts of psychological resilience such as maintaining function, subjective well-being, motivation for activity, and improving the quality of life.26 In addition, psychological resilience plays an important defensive role in the face of difficulties, and it is related with patients’ social adaptability, quality of life, negative emotion, disease stigma.27,28
Stigma could affect the level of individual psychological resilience, and it plays an important role in the construction of individual psychological resilience. The psychological resilience of low stigma patients is significantly higher than that of high stigma patients.29,30 Resilience is negatively associated with infertility-specific and general distress in women with fertility in the United States.31 For infertile couples in Germany, resilience can be considered as an unspecific protective factor against infertility-specific distress and impaired quality of life.28 Lower resilience and higher avoidance were believed to be predictors of distress and anxiety during pregnancy.32 Therefore, there is a close relationship among stigma, SAD, and psychological resilience. Meanwhile, individuals with higher psychological resilience tend to have a strong positive social orientation ability, and can participate in social activities with a positive attitude.
Therefore, this study aimed to explore the influencing relationships among stigma, SAD, and psychological resilience in infertile patients. We also tried to understand the potential influence of psychological resilience on the formation of stigma, SAD of infertile patients. Understanding the influencing relationship among stigma, SAD, and psychological resilience might help to make psychological resilience-related intervention measures to help improve patients’ stigma, SAD, and finally help patients better integrate into society and participate in normal social activities with a positive attitude. This study is also helpful for medical staff to understand the causes of patients’ social avoidance and distress, and solve the problem from the perspective of positive factors of patients. In addition, the findings of this study indicate that medical staff should pay more attention to patients’ emotional response, and help patients to reduce stigma for the improvement of social ability.
In this study, we propose the following assumptions: (1) Both stigma and psychological resilience affect the SAD level of infertility patients; (2) Psychological resilience could mediate the relationship between stigma and SAD. In order to test the above hypothesis, we analyzed the relationship among stigma, psychological resilience, and SAD in infertile patients, and explored the possible mediating role of psychological resilience in stigma and SAD. This study might provide a new strategy for the psychological intervention of infertile patients.
Methods and Materials
Participants and Procedure
From November 2020 to March 2021, the infertile women taking ART treatment in the reproductive clinic of the first hospital of Lanzhou University were selected using convenience sampling method. The convenience sampling method was performed as follows: All patients who met the inclusion criteria and signed informed consent were selected for investigation in this study. The study has been approved by the Ethical Committee of Nursing School, Lanzhou University. This study was performed according to the Declaration of Helsinki for Medical Research involving Human Subjects. The inclusion criteria of this study: (1) female patients diagnosed as infertility using WHO diagnostic criteria (Infertility is clinically described as a disease of the reproductive system defined by the failure to achieve a clinical pregnancy after 12 months or more of regular unprotected sexual intercourse);1 (2) patients voluntarily participate in this study and were able to understand the survey content; (3) married females (Unmarried females with infertility are prohibited from receiving assisted reproductive technology in China). The exclusion criteria of this study were set as described previously:19,33 (1) patients with disturbance of consciousness and mental illness; (2) patients were unable to fill in the questionnaires; (3) patients with severe physical or chronic diseases, such as (1) Severe heart, brain or kidney diseases; (2) Severe mental disorders; (3) Severe organic diseases in the reproductive or endocrine system. A total of 278 infertile patients were enrolled in this research. All participants have signed informed consent and agreed to participate in this research.
This study is a cross-sectional study. A face-to-face interview was conducted among the infertility patients in the hospital by the trained investigators. The researchers introduced the purpose and significance of this study directly to the participants. After obtaining their signed informed consents, 4 kinds of questionnaires, including General information questionnaire, Social avoidance and distress scale (SADS), The Infertility Stigma Scale (ISS), and Connor-Davidson resilience scale (CD-RISC), were sent out on the spot and collected on the spot. A total of 278 questionnaires were distributed, 12 invalid questionnaires were eliminated, and 266 valid questionnaires were recovered, with an effective response rate of 95.7%. The effective response rate = (valid questionnaires/total distributed questionnaires) × 100%. If the questionnaire was viewed as either (1) Missing answers to the questionnaire; (2) Wrong answers to the questionnaire (For example, more than one answers for the non-multiple choice questions); (3) The options checked in the whole questionnaire are the same; or (4) The options checked in the whole questionnaire are regular, the questionnaire was considered as an “invalid questionnaire”.
In order to protect the personal information of infertile patients, this study is an anonymous survey, which reduces the impact of common methods on data results in a certain extent. Meanwhile, Harman single-factor analysis was used to test the common method bias, and we found that the cumulative percentage of the first factor was 12.98%, which was less than the critical value of 40%. Therefore, this study was not affected by the common method bias.
Questionnaire and Measurement
General Information Questionnaire
A self-made general information questionnaire was made and designed by the research team after literature review and expert consultation. The demographic characteristics and disease-related details of patients are included in this general information questionnaire, which contains age, nationality, residence place, educational level, occupation, per capita monthly income, marriage history, time of infertility, causes of infertility, presence or absence of biological children, type of infertility, source of birth pressure, treatment history, etc. “Have you ever been treated” was defined as “yes”, if the participants had received assisted reproductive technologies, traditional Chinese medicine treatment, or western medicine treatment.
SADS
SADS was firstly designed by Watson and Friend,11 and the Chinese version was revised by Peng et al34,35 SADS totally contains 28 items (Social avoidance: 14, social distress: 14) and 2 dimensions. SADS is mainly used to measure the avoidance tendency and distress experience of subjects in social situations. The scale was scored by “yes/no” answer method, with a score range of 0–28. Higher score suggests serious SAD. Items 1, 3, 4, 6, 7, 9, 12, 15, 17, 19, 22, 25, 27 and 28 are reverse scoring items. The Cronbach’s α coefficient was 0.837, and the test–retest reliability was 0.793. SADS has been widely used in many kinds of studies including social anxiety36 and intellectual disabilities populations,37 and social phobia.37 SADS is characterized by good structural validity, compatibility validity and discriminant validity, and it could be used to effectively measure the subjective emotional experience and behavior changes of individuals with social difficulties. The score-level range was listed as follows: 0–10 (Low level); 11–20 (Middle level); ≧21 (High level).
The Infertility Stigma Scale (ISS)
The ISS designed by Fu et al17 is mainly used to measure the stigma of females with infertility. ISS contains 27 items and 4 dimensions including family stigma, public stigma, social withdrawal, and self-devaluation. Likert 5 level scoring method was used in this ISS, with a score range of 27–135 points. The total score of 27–63 points indicated that the level of stigma was low, 64–100 points indicated that the level of stigma was moderate, and 101–135 points indicated that the level of stigma was severe. The higher the score, the higher the level of stigma. The Cronbach’s α coefficient was 0.77~0.94, and the test–retest reliability was 0.91. ISS has good construct validity, reliability and validity. ISS has been widely used in the study of infertility.15,17,19 The score-level range was listed as follows: 27–63 (Low level); 64–100 (Middle level); 101–135 (High level).
Connor- Davidson Resilience Scale (CD-RISC)
The CD-RISC designed by Connor and Davidson38 in 2003 is a universal scale for evaluating individual psychological resilience. The Chinese version of CD-RISC was translated and revised by Chinese scholar Xiaonan Yu et al.39 The scale includes three dimensions: tenacity (13 items), strength (8 items) and optimism (4 items). Likert 5-level scoring method was used in this CD-RISC, with a score range of 0–100 points. The score of ≤25 is very poor, 26 ~ 50 is poor, 51 ~ 75 is average, 76 ~ 100 is good. The Cronbach’s α coefficient of Chinese version was 0.952, content validity was 0.91, and the split-half reliability was 0.894. All the measurement tools have been endorsed by the developers of the scales. CD-RISC is the most widely used scale to study psychological resilience. The Chinese version of CD-RISC has been widely applied in the populations of infertility,40 tumor,41 and stroke.42 The Chinese version of CD-RISC has shown good reliability and validity. The Cronbach’s alpha coefficient of the Chinese version of CD-RISC was 0.943 in this study. The score-level range was listed as follows: ≧25 (Very bad); 25–50 (Bad); 51–75 (Normal); 76–100 (Good).
Statistical Analysis
EpiData 3.1 Chinese version was used as input data. SPSS 25.0 software was used to analyze the data, and measurement data was presented using  . Counting data were presented using frequency and percentage. Two independent sample t-test and one-way analysis of variance (ANOVA) were used to compare the difference of SAD among categorical variables. Pearson correlation analysis was used to explore the correlation among stigma, psychological resilience, and SAD in infertile patients. Multiple regression analysis was performed to explore the predictors of SAD and test the mediating effect of psychological resilience on the relationship between stigma and SAD. SAD was used as a dependent variable. The independent variables were entered into three steps as follows: Step 1: demographic characteristics of patients; Step 2: stigma; and Step 3: psychological resilience. If the regression coefficient of stigma to the SAD was significant and decreased from step 2 to step 3, there was a partial mediated effect. If the regression coefficient was not statistically significant (P > 0.05), a complete mediating role of psychological resilience was indicated. In addition, the Structural Equation Model (SEM) was used to confirm the mediating effect of psychological resilience on the relationship between stigma and SAD, which was analyzed by Amos 23.0. The model fitted with the SEM criteria (χ2/df < 3, GFI > 0.90, AGFI > 0.90, NFI > 0.90, IFI >0.90, TLI > 0.90, CFI >0.90, and RMSEA < 0.08) according to previous publications.43,44 Bootstrapping sampling is a method for evaluating statistical precision, and it is a statistical process that can resample a single dataset to create a distribution of datasets, where bootstrap sampling distributions are created by sampling repeatedly with replacement from the original dataset.45 A bias-corrected and accelerated 95% CI (BCa 95% CI) for each a*b product was examined. All analyses were performed using SPSS version 25.0 and Amos 23.0 statistical software for Windows. Statistical significance was defined as P < 0.05 (two-tailed). The results were presented as mean± standard deviation in this study.
. Counting data were presented using frequency and percentage. Two independent sample t-test and one-way analysis of variance (ANOVA) were used to compare the difference of SAD among categorical variables. Pearson correlation analysis was used to explore the correlation among stigma, psychological resilience, and SAD in infertile patients. Multiple regression analysis was performed to explore the predictors of SAD and test the mediating effect of psychological resilience on the relationship between stigma and SAD. SAD was used as a dependent variable. The independent variables were entered into three steps as follows: Step 1: demographic characteristics of patients; Step 2: stigma; and Step 3: psychological resilience. If the regression coefficient of stigma to the SAD was significant and decreased from step 2 to step 3, there was a partial mediated effect. If the regression coefficient was not statistically significant (P > 0.05), a complete mediating role of psychological resilience was indicated. In addition, the Structural Equation Model (SEM) was used to confirm the mediating effect of psychological resilience on the relationship between stigma and SAD, which was analyzed by Amos 23.0. The model fitted with the SEM criteria (χ2/df < 3, GFI > 0.90, AGFI > 0.90, NFI > 0.90, IFI >0.90, TLI > 0.90, CFI >0.90, and RMSEA < 0.08) according to previous publications.43,44 Bootstrapping sampling is a method for evaluating statistical precision, and it is a statistical process that can resample a single dataset to create a distribution of datasets, where bootstrap sampling distributions are created by sampling repeatedly with replacement from the original dataset.45 A bias-corrected and accelerated 95% CI (BCa 95% CI) for each a*b product was examined. All analyses were performed using SPSS version 25.0 and Amos 23.0 statistical software for Windows. Statistical significance was defined as P < 0.05 (two-tailed). The results were presented as mean± standard deviation in this study.
Results
Demographic Characteristics
The demographic characteristics are presented in Table 1. The average age of the infertile women was 31.39 ± 4.30 years old. 43.2% of the infertile women have been suffering from infertility for 2–5 years, and 42.9% of them have been diagnosed with infertility, and the time after diagnosis was less than one year. Around 69.9% of the infertile women had treatment experience before, and 38.3% of them have been married for less than 3 years. About 80.1% of them currently have no biological children, and 49.2% of them are primary infertility. Among the 266 women we investigated, 59% of the causes of infertility came from women, 13.6% from men, 16.9% from both husband and wife, and 10.5% belonged to unexplained infertility. About 59.8% of the infertile women have “big” or “very big” pressure from others.
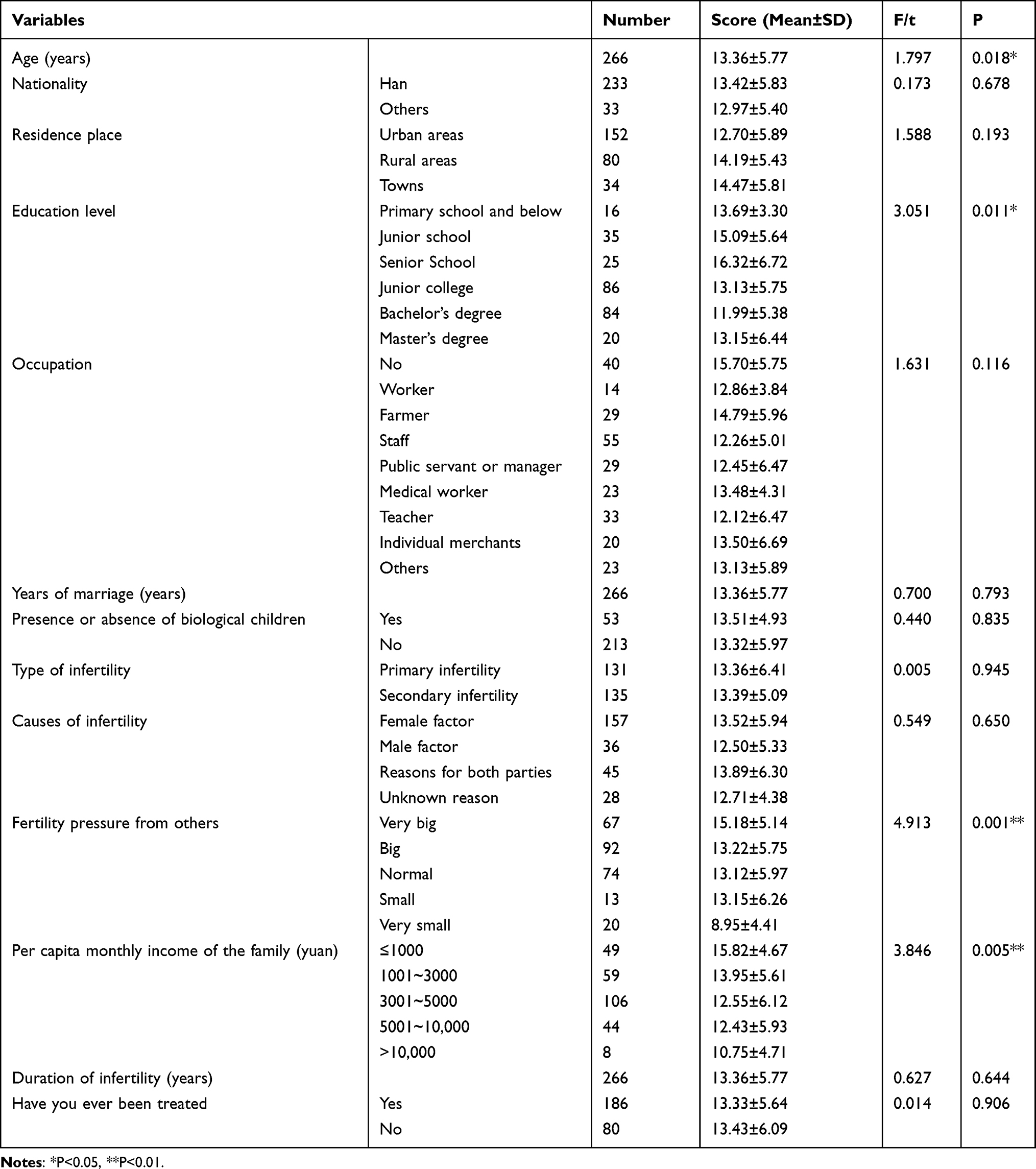 |
Table 1 Univariate Analysis of Social Avoidance and Distress Score of Infertile Women (n = 266) |
Univariate Analysis of SAD in Infertile Patients
The data of univariate analysis indicated that significant differences in SAD could be observed among patients in terms of different education levels, fertility stress levels, and per capita monthly income (Table 1). However, no statistical differences were observed in terms of age, nationality, residence place, occupation, years of marriage, presence or absence of biological children, type of infertility, duration of infertility, have you ever been treated, and causes of infertility between different groups (Table 1).
The Scores of Stigma, SAD, and Psychological Resilience of Infertility Patients
The total score of SADS was 13.36 ± 5.77, which was in the middle level. The scores of each dimension are listed in Table 2. The score of social avoidance of infertile women was 6.80 ± 2.97 and the social distress was 6.56 ± 3.38, which was in the middle level. The total score of ISS was 77.84 ± 16.91, which were in the middle levels. In addition, the scores of CD-RISC were 58.84 ± 12.24, which was in the low level (Table 2).
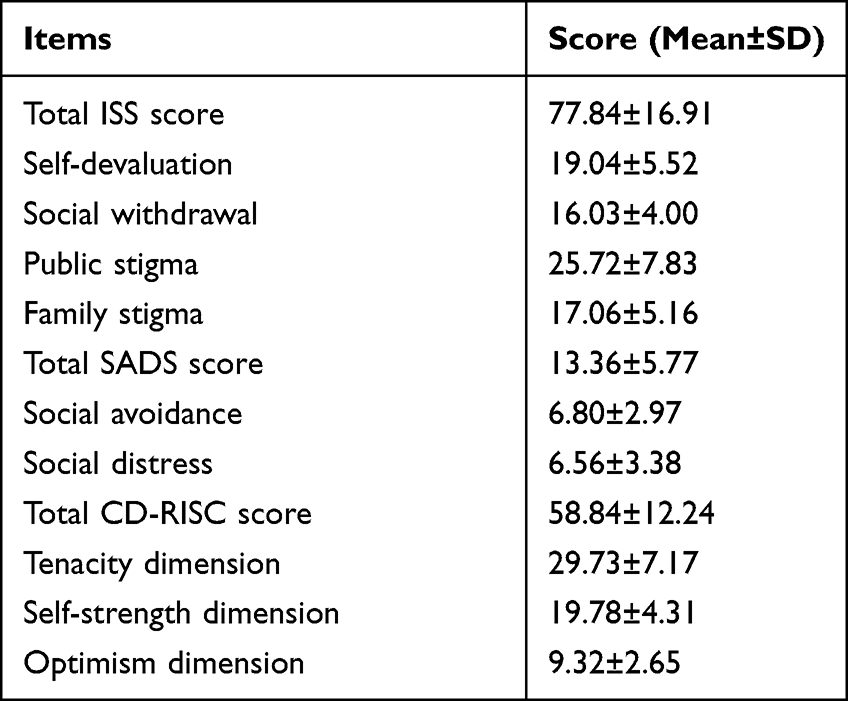 |
Table 2 The Scores of Different Dimensions of Infertile Women (n = 266) |
Correlation Between Stigma and Psychological Resilience and SAD
Significant positive correlation between stigma and social avoidance (r = 0.308, P <0.01), social distress (r = 0.257, P < 0.01), SAD (r = 0.309, P <) was observed (Table 3). Stigma was negatively correlated with psychological resilience (r = −0.405, P < 0.01). In addition, psychological resilience was remarkably negatively correlated with social avoidance (r = −0.340, P < 0.01), social distress (r = −0.331, P < 0.01), SAD (r = −0.369, P < 0.01) (Table 3). With the increase in stigma score, the score of SADS also increased (Figure 1A), while with the increase in psychological resilience score, the degree of SADS gradually decreased (Figure 1B). These data indicated that stigma was positively correlated with SADS in infertile women, and psychological resilience was negatively correlated with SADS, which was in consistent with the results of Table 3.
 |
Table 3 Correlation Between Stigma and Psychological Resilience and Social Avoidance and Distress |
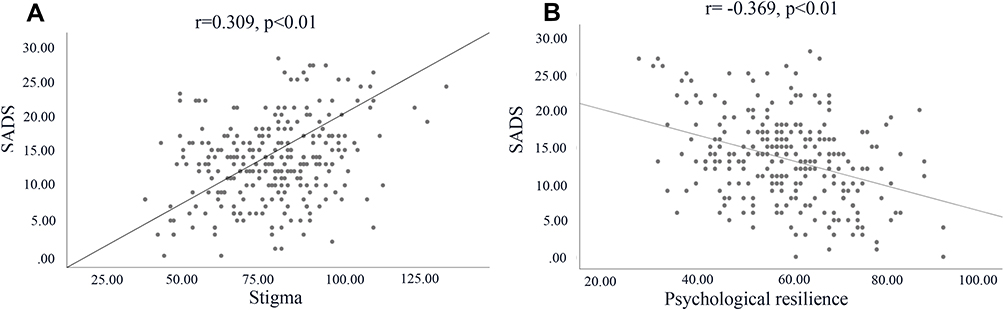 |
Figure 1 Correlation analysis between stigma and psychological resilience and SADS. (A) The correlation analysis between stigma and SADS; (B) the correlation analysis between psychological resilience and SADS. Abbreviation: SADS, social avoidance and distress scale. |
Mediating Effect of Psychological Resilience on Stigma, SAD in Infertile Patients
According to the correlation analysis between psychological resilience and stigma, SAD and stigma might exert a direct effect on SAD, and psychological resilience might be the mediating factor of stigma and SAD. Amos 23.0 software was used to build a structural equation model to verify the hypothesis above. Stigma (self-devaluation, social withdrawal, public stigma, family stigma) was set as independent variables, psychological resilience (tenacity, strength, optimism) was set as mediating variables, and SAD was set as dependent variables. The hypothesized mediation model between stigma and SAD is illustrated in Figure 2A.
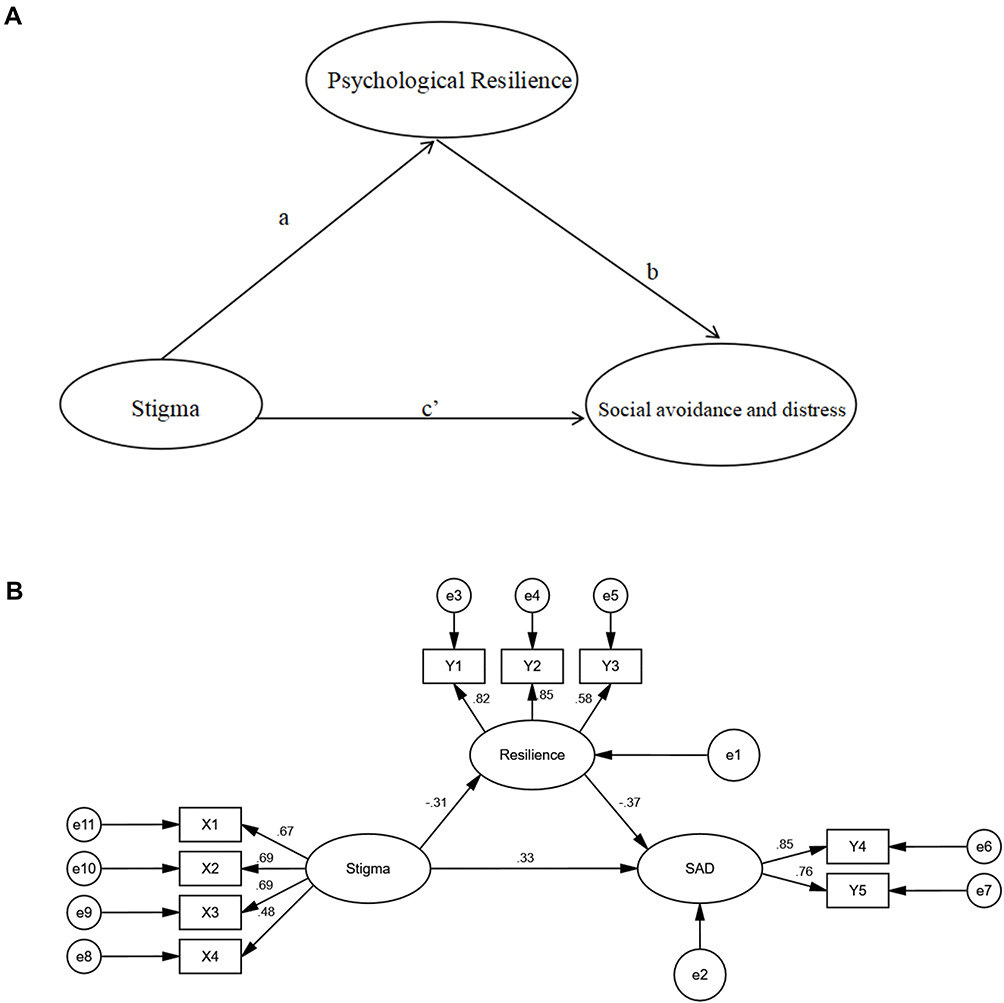 |
Figure 2 Mediating role of psychological resilience between stigma, social avoidance and distress. (A) Hypothesized mediation model (a, b, and c’ = unstandardized regression coefficients): indirect effect = a*b; direct effect = c′; total effect c = sum of indirect and direct effect = a*b + c’; (B) the structural equation model of the mediating role of psychological resilience between stigma, social avoidance and distress (X1: self-devaluation; X2: social withdrawal; X3: public stigma; X4: family stigma; Y1: tenacity dimension; Y2; self-strength dimension; Y3: optimism dimension Y4: social avoidance; Y5: social distress; ellipse: the latent variables; Rectangle: the observed variables; black arrow: the endogenous variable; SAD is the endogenous latent variable; stigma is the exogenous latent variable; resilience is the mediator variable; e1 and e2 are the equation error, and e3-e11 is the measure error). Abbreviation: SAD, social avoidance and distress. |
The mediating role of psychological resilience in the association between stigma and SAD is shown in Figure 2B. The results of mediation analyses showed that the significance of the direct, indirect and total effects in a mediation model was indicated in Table 4 and Figure 2B. The model shows that the stigma of infertile women has a negative predictive effect on psychological resilience (β = −0.312, P < 0.01), and that psychological resilience has a negative predictive effect on SAD (β = −0.373, P < 0.01), stigma has a direct positive predictive effect on SAD (β = 0.338, P < 0.01), there is a positive mediating effect between stigma and SAD in women with infertility, and the mediating effect is 0.116, accounting for 25.5% of the total effect.
 |
Table 4 Psychological Resilience in the Mediating Effect Model Between Stigma, Social Avoidance and Distress |
The results of mediation analyses also showed that the total effect (path c) of stigma on SAD was significant (β= 0.454, P < 0.001). Moreover, when psychological resilience was modeled as a mediator, the path coefficient of stigma on SAD decreased significantly (c’ = 0.338, P < 0.01). The bias-corrected and accelerated bootstrap test indicated that psychological resilience significantly mediated the relationship between stigma and SAD (a*b = 0.116, BCa 95% CI: 0.046∼0.254). The empirical 95% CI did not consist of zero, indicating that psychological resilience partially mediated the relationship between stigma and SAD (Table 4).
The model presented in Figure 2B was fully supported by all standard goodness-of-fit indices (χ2/df < 3, GFI = 0.958, AGFI = 0.921, NFI = 0.934, IFI = 0.965, TLI = 0.947, CFI = 0.964, and RMSEA = 0.063) (Table 5). Thus, stigma directly affected SAD and also influenced SAD indirectly by the mediating pathway of psychological resilience. The above results have proved the hypothesis, which was mentioned in the article.
 |
Table 5 Fitting Indicators of the Structural Equation Model of Social Avoidance and Distress, Psychological Resilience and Stigma of Infertility Patients |
Discussion
The total score of SAD was 13.36±5.77, which was close to the medium level. We compared our data with another infertility study46 in China, and found that Chinese women with infertility have higher levels of SAD compared with healthy Chinese women. The SAD level of infertile patients with lower education level (below senior high school) was higher than that of with higher education level (above junior college). This might be explained by the reason that patients with higher education level have a higher level of disease awareness and are more likely to accept the fact of infertility. Therefore, infertility patients with higher education are more likely to take a positive attitude to social interaction, and the degree of SAD is relatively low.47 In addition, the SAD level of infertile patients with higher monthly income was lower. Women with higher income may balance their attention to infertility through their work and career, and have higher levels of disease perception and control. They might have more psychological adjustment skills and methods to help them alleviate negative emotions and maintain normal social activities.19,48 Infertility patients with very low reproductive pressure scored the lowest in SAD, while infertility patients with very high reproductive pressure scored the highest in SAD. It might be explained by the reason that social attention from the outside world will make infertile women more sensitive, and they do not want to be asked about having children by relatives or friends. Therefore, they tend to take an evasive attitude towards all kinds of social activities, which leads to a serious degree of SAD.49
The above results suggest that clinical medical staff should pay more attention to the infertility patients with low education level, low income and greater social pressure, and give them targeted psychological counselling. In the process of medical treatment, medical staffs should create a friendly environment, help them expand their social support system to obtain more emotional and spiritual support, reduce their perceived emotional or social isolation, and then reduce their SAD level, so that infertility patients can cooperate with infertility treatment with a better attitude and the outcome of assisted reproduction could be improved. In a recent study, social pressure during pregnancy among Malian women in West Africa is a more significant predictor of depressive symptoms than the infertility status itself.8 Therefore, future research should measure the social pressure of pregnancy using a simple and psychometrically sound instrument, the 5-item, 3-point Likert Social Pressure for Pregnancy Scale.8 Results from this understudied concept of social pressure in pregnancy may advance research and clinical practice in the infertility area.
Studies have shown that females with an unfulfilled wish for a child have different degrees of stigma, and the stigma mainly derives from themselves, families, friends, relatives, classmates, and society.14 Stigma could cause some negative effects on infertility patients, such as anxiety, depression, low self-esteem, decreased life satisfaction, social isolation, and social avoidance.50 The experience of stigma seriously affected the ability of patients to work, seek outside help and communicate with others.18,51,52 This study confirmed the direct predictive effect of stigma on SAD. The intermediary test results showed that the total effect of stigma on SAD was 0.454. Stigma not only had a direct effect on SAD (β = 0.338, p < 0.01 but also indirectly affected SAD through psychological resilience. The stigma of infertility patients was mainly reflected in self-derogation and social withdrawal, which are the potential mechanisms of SAD.17 SAD behaviors were related to negative emotions, stigma and social discrimination.53 Individuals with a high level of stigma are more likely to adopt negative coping styles, such as closing themselves and unwilling to communicate with family and friends, which further aggravates their loneliness and SAD in social life.34,54,55
Psychological resilience is an important predictor of mental health.56 Individuals with a high level of psychological resilience have some qualities, such as tenacity, self-improvement and optimism. They could actively and effectively deal with the adverse effects of infertility, actively seek help and social support, and properly avoid the sources of stress.56,57 They tend to show more positive social-oriented behaviors.40 In this study, we demonstrated that psychological resilience might play a positive role in coping with stress and adversity in infertile patients. Psychological resilience can help patients effectively cope with the adverse effects of disease and buffer the adverse effects of negative emotions, so as to play a buffer function in SAD of infertile patients. As a mediator, this may be the underlying mechanism of psychological resilience. Therefore, improving the stigma and resilience of infertility patients through psychological intervention may be an effective strategy to increase their psychological adaptability and reduce SAD. In order to improve the social ability of infertile patients, the following suggestions were put forward. (1) The positive factors (psychological capital, psychological resilience, subjective well-being) of patients should be actively explored to reduce stigma, SAD; (2) Psychological intervention (mindfulness therapy, group cognitive therapy, rational emotional behavior therapy) can guide patients to face the disease with a positive attitude, reduce or eliminate negative emotions, treat other people’s discrimination and exclusion correctly, learn to accept themselves, reduce stigma and improve social skills.
A few limitations exist in the present study. Firstly, the cross-sectional design in this study cannot establish causal relationships among study variables. Secondly, only one hospital was selected, and the sample source was relatively limited. Multi-center and large sample research are needed to validate the conclusions of this study. Finally, the results of this study might be limited by unmeasured confounders.
Stigma was highly associated with SAD, whereas psychological resilience was negatively associated with SAD. Stigma can directly affect SAD in infertility patients and can also indirectly affect SAD through psychological resilience. Psychological resilience plays a positive role in alleviating the psychological problems of patients and could reduce the negative effect of stigma on the development of SAD. Stigma and psychological resilience are potentially changeable factors and also important targets to improve the SAD of infertility patients.
Conclusion
This study firstly studied the relationship between stigma, psychological resilience, and SAD in infertile patients systematically. The mediating role of psychological resilience between stigma and SAD was firstly reported. During the treatment process, medical staff should find out the stigma of infertility patients over time, take targeted psychological intervention measures, to improve psychological resilience level and alleviate SAD. Clinical medical workers should give culturally appropriate psychological counselling to infertility patients, promote their affirmation of self-value, guide them to find their own advantages, and then integrate into normal social activities. This study might provide a new strategy for the psychological intervention of infertile patients.
Abbreviations
SADS, social avoidance and distress scale; SAD, social avoidance and distress; ISS, The Infertility Stigma Scale; CD-RISC, Connor-Davidson resilience scale; ANOVA, one-way analysis of variance; SEM, Structural Equation Model.
Data Sharing Statement
Data supporting this study have been presented in the manuscript, and the data could be obtained from the corresponding author.
Ethics Approval and Consent to Participate
The study has been approved by the Ethical Committee of Nursing School, Lanzhou University. This study was performed according to the Declaration of Helsinki for Medical Research involving Human Subjects. All patients signed informed consent.
Consent for Publication
All authors agree the publication of this manuscript.
Author Contributions
CH and NT conceived and designed the study; NT, QZ, JL, and HL conducted the survey, NT, CH, and QZ analyzed the data and wrote the paper. All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval for the version to be published, and agree to be accountable for all aspects of the work.
Funding
The study was funded by the Research project of School of Nursing, Lanzhou University (LZUSON202009).
Disclosure
The authors declare that they have no conflict of interest.
References
1. World Health Organization (WHO). International Classification of Diseases.
2. Tabong PT, Adongo PB. Infertility and childlessness: a qualitative study of the experiences of infertile couples in Northern Ghana. BMC Pregnancy Childbirth. 2013;13:72. doi:10.1186/1471-2393-13-72
3. Fabamwo AO, Akinola OI. The understanding and acceptability of assisted reproductive technology (ART) among infertile women in urban Lagos, Nigeria. J Obstet Gynaecol. 2013;33(1):71–74. doi:10.3109/01443615.2012.730077
4. Zhou Z, Zheng D, Wu H, et al. Epidemiology of infertility in China: a population-based study. BJOG. 2018;125(4):432–441. doi:10.1111/1471-0528.14966
5. de Ziegler D, Gambone JC, Meldrum DR, Chapron C. Risk and safety management in infertility and assisted reproductive technology (ART): from the doctor’s office to the ART procedure. Fertil Steril. 2013;100(6):1509–1517. doi:10.1016/j.fertnstert.2013.10.020
6. Mosalanejad L, Khodabakshi Koolee A. Looking at infertility treatment through the lens of the meaning of life: the effect of group logotherapy on psychological distress in infertile women. Int J Fertil Steril. 2013;6(4):224–231.
7. Hess RF, Ross R, Gililland JL
8. Ross R, Hess RF. Social pressure for pregnancy scale: its development, psychometric properties, and potential contributions to infertility and depression research. J Nurs Meas. 2019;27(1):5–15. doi:10.1891/1061-3749.27.1.5
9. Remennick L, Ross R, Hess RF. Childless in the land of imperative motherhood: stigma and coping among infertile Israeli women. Sex Roles. 2000;43(11):821–841. doi:10.1023/A:1011084821700
10. Daibes MA, Safadi RR, Athamneh T, Anees IF, Constantino RE. “Half a woman, half a man; that is how they make me feel”: a qualitative study of rural Jordanian women’s experience of infertility. Cult Health Sex. 2018;20(5):516–530. doi:10.1080/13691058.2017.1359672
11. Watson D, Friend R. Measurement of social-evaluative anxiety. J Consult Clin Psychol. 1969;33(4):448–457. doi:10.1037/h0027806
12. Chen JJ. Investigation on the social status and influencing factors of infertile couples. Chin J Sexual. 2020;29(7):149–151.
13. Jansen NA, Saint Onge JM. An internet forum analysis of stigma power perceptions among women seeking fertility treatment in the United States. Soc Sci Med. 2015;147:184–189. doi:10.1016/j.socscimed.2015.11.002
14. Slade P, O’Neill C, Simpson AJ, Lashen H. The relationship between perceived stigma, disclosure patterns, support and distress in new attendees at an infertility clinic. Hum Reprod. 2007;22(8):2309–2317. doi:10.1093/humrep/dem115
15. Capik A, Aksoy M, Yilmaz E, Yilmaz F. Infertility Stigma Scale: a psychometric study in a Turkish sample. Perspect Psychiatr Care. 2019;55(2):328–335. doi:10.1111/ppc.12360
16. van Brakel WH, Anderson AM, Mutatkar RK, et al. The Participation Scale: measuring a key concept in public health. Disabil Rehabil. 2006;28(4):193–203. doi:10.1080/09638280500192785
17. Fu B, Qin N, Cheng L, et al. Development and validation of an Infertility Stigma Scale for Chinese women. J Psychosom Res. 2015;79(1):69–75. doi:10.1016/j.jpsychores.2014.11.014
18. Latalova K, Kamaradova D, Prasko J. Perspectives on perceived stigma and self-stigma in adult male patients with depression. Neuropsychiatr Dis Treat. 2014;10:1399–1405. doi:10.2147/NDT.S54081
19. Zhang F, Lv Y, Wang Y, et al. The social stigma of infertile women in Zhejiang Province, China: a questionnaire-based study. BMC Womens Health. 2021;21(1):97. doi:10.1186/s12905-021-01246-z
20. Lynch H, McDonagh C, Hennessy E. Social anxiety and depression stigma among adolescents. J Affect Disord. 2021;281:744–750. doi:10.1016/j.jad.2020.11.073
21. Wischmann T, Thorn P. (Male) infertility: what does it mean to men? New evidence from quantitative and qualitative studies. Reprod Biomed Online. 2013;27(3):236–243. doi:10.1016/j.rbmo.2013.06.002
22. Gonzalez LO. Infertility as a transformational process: a framework for psychotherapeutic support of infertile women. Issues Ment Health Nurs. 2000;21(6):619–633. doi:10.1080/01612840050110317
23. Hardy SE, Concato J, Gill TM. Resilience of community-dwelling older persons. J Am Geriatr Soc. 2004;52(2):257–262. doi:10.1111/j.1532-5415.2004.52065.x
24. Pinquart M. Moderating effects of dispositional resilience on associations between hassles and psychological distress. J Appl Dev Psychol. 2009;30(1):53–60. doi:10.1016/j.appdev.2008.10.005
25. Schmidt PJ, Cardoso GM, Ross JL, Haq N, Rubinow DR, Bondy CA. Shyness, social anxiety, and impaired self-esteem in Turner syndrome and premature ovarian failure. JAMA. 2006;295(12):1374–1376. doi:10.1001/jama.295.12.1374
26. Wermelinger Avila MP, Lucchetti AL, Lucchetti G. Association between depression and resilience in older adults: a systematic review and meta-analysis. Int J Geriatr Psychiatry. 2017;32(3):237–246. doi:10.1002/gps.4619
27. Davydov DM, Stewart R, Ritchie K, Chaudieu I. Resilience and mental health. Clin Psychol Rev. 2010;30(5):479–495. doi:10.1016/j.cpr.2010.03.003
28. Herrmann D, Scherg H, Verres R, von Hagens C, Strowitzki T, Wischmann T. Resilience in infertile couples acts as a protective factor against infertility-specific distress and impaired quality of life. J Assist Reprod Genet. 2011;28(11):1111–1117. doi:10.1007/s10815-011-9637-2
29. Duthely LM, Sanchez-Covarrubias AP, Brown MR, et al. Pills, PrEP, and Pals: adherence, stigma, resilience, faith and the need to connect among minority women with HIV/AIDS in a US HIV epicenter. Front Public Health. 2021;9:667331. doi:10.3389/fpubh.2021.667331
30. Post F, Buchta M, Kemmler G, Pardeller S, Frajo-Apor B, Hofer A. Resilience predicts self-stigma and stigma resistance in stabilized patients with bipolar I disorder. Front Psychiatry. 2021;12:678807. doi:10.3389/fpsyt.2021.678807
31. Sexton MB, Byrd MR, von Kluge S. Measuring resilience in women experiencing infertility using the CD-RISC: examining infertility-related stress, general distress, and coping styles. J Psychiatr Res. 2010;44(4):236–241. doi:10.1016/j.jpsychires.2009.06.007
32. Roos A, Faure S, Lochner C, Vythilingum B, Stein DJ. Predictors of distress and anxiety during pregnancy. Afr J Psychiatry. 2013;16(2):118–122. doi:10.4314/ajpsy.v16i2.15
33. Fang M, Li G, Kang X, et al. The role of gender and self-esteem as moderators of the relationship between stigma and psychological distress among infertile couples. Psychol Health Med. 2020;4:1–14.
34. Sobanski JA, Klasa K, Rutkowski K, Dembinska E, Muldner-Nieckowski L, Cyranka K. [Social Avoidance and Distress Scale (SAD) and Fear of Negative Evaluation Scale (FNE)–reliability and the preliminary assessment of validity]. Psychiatr Pol. 2013;47(4):691–703. Polish.
35. Peng CZ, Li LC. Reliability and validity of social avoidance and distress scale in student population. Chin J Clin Psychol. 2003;4:279–281.
36. Pinto A, Phillips KA. Social anxiety in body dysmorphic disorder. Body Image. 2005;2(4):401–405. doi:10.1016/j.bodyim.2005.10.003
37. Jeon BJ, Son SM. Social interaction changes in people with intellectual disabilities through the application of equine-assisted intervention in Korea. Am J Transl Res. 2021;13(4):3573–3581.
38. Connor KM, Davidson JR. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depress Anxiety. 2003;18(2):76–82. doi:10.1002/da.10113
39. Yxz JX. Comparison of the self-resilience scale and the Connor-Davidson resilience scale. J Psychol Sci. 2007;30(5):1169–1171.
40. Li Y, Zhang X, Shi M, Guo S, Wang L. Resilience acts as a moderator in the relationship between infertility-related stress and fertility quality of life among women with infertility: a cross-sectional study. Health Qual Life Outcomes. 2019;17(1):38. doi:10.1186/s12955-019-1099-8
41. Lim JW, Shon EJ, Paek M, Daly B. The dyadic effects of coping and resilience on psychological distress for cancer survivor couples. Support Care Cancer. 2014;22(12):3209–3217. doi:10.1007/s00520-014-2334-9
42. Zhao L, Yang F, Sznajder KK, Zou C, Jia Y, Yang X. Resilience as the mediating factor in the relationship between sleep disturbance and post-stroke depression of stroke patients in China: a structural equation modeling analysis. Front Psychiatry. 2021;12:625002. doi:10.3389/fpsyt.2021.625002
43. Hooper D, Coughlan J, Mullen MR. Structural equation modelling: guidelines for determining model fit. Electron j Bus Res Methods. 2008;6(1):53–60.
44. Bentler PM. Comparative fit indexes in structural models. Psychol Bull. 1990;107(2):238–246. doi:10.1037/0033-2909.107.2.238
45. Levy JA, Landerman LR, Davis LL. Advances in mediation analysis can facilitate nursing research. Nurs Res. 2011;60(5):333–339. doi:10.1097/NNR.0b013e318227efca
46. Jiajing Chen JC, Xiaomei W, Zhang C, Chen S, You Q, Huang W. Investigation of social life of infertile couples and associated factors. Chin J Human Sexual. 2020;29(7):149–151.
47. Wang K, Li J, Zhang JX, Zhang L, Yu J, Jiang P. Psychological characteristics and marital quality of infertile women registered for in vitro fertilization-intracytoplasmic sperm injection in China. Fertil Steril. 2007;87(4):792–798. doi:10.1016/j.fertnstert.2006.07.1534
48. Karabulut A, Ozkan S, Oguz N. Predictors of fertility quality of life (FertiQoL) in infertile women: analysis of confounding factors. Eur J Obstet Gynecol Reprod Biol. 2013;170(1):193–197. doi:10.1016/j.ejogrb.2013.06.029
49. Whiteford LM, Gonzalez L. Stigma: the hidden burden of infertility. Soc Sci Med. 1995;40(1):27–36. doi:10.1016/0277-9536(94)00124-C
50. Van den Broeck U, D’Hooghe T, Enzlin P, Demyttenaere K. Predictors of psychological distress in patients starting IVF treatment: infertility-specific versus general psychological characteristics. Hum Reprod. 2010;25(6):1471–1480. doi:10.1093/humrep/deq030
51. Maurino J, Martinez-Gines ML, Garcia-Dominguez JM, et al. Workplace difficulties, health-related quality of life, and perception of stigma from the perspective of patients with multiple sclerosis. Mult Scler Relat Disord. 2020;41:102046. doi:10.1016/j.msard.2020.102046
52. Wright KB, Mazzone R, Oh H, et al. The influence of U.S. chain restaurant food consumption and obesity in china and south korea: an ecological perspective of food consumption, self-efficacy in weight management, willingness to communicate about weight/ diet, and depression. Health Commun. 2016;31(11):1356–1366. doi:10.1080/10410236.2015.1072124
53. Chan RCH, Mak WWS, Ma GYK, Cheung M. Interpersonal and intrapersonal manifestations of HIV stigma and their impacts on psychological distress and life satisfaction among people living with HIV: toward a dual-process model. Qual Life Res. 2021;30(1):145–156. doi:10.1007/s11136-020-02618-y
54. Townsend L, Musci R, Stuart E, et al. The association of school climate, depression literacy, and mental health stigma among high school students. J Sch Health. 2017;87(8):567–574. doi:10.1111/josh.12527
55. Shrestha S. Internalized stigma, coping and social support with mental illness in Manipal teaching hospital, Pokhara, Nepal. J Nepal Health Res Counc. 2019;17(1):80–84. doi:10.33314/jnhrc.v17i01.2011
56. van der Meulen E, van der Velden PG, Setti I, van Veldhoven M. Predictive value of psychological resilience for mental health disturbances: a three-wave prospective study among police officers. Psychiatry Res. 2018;260:486–494. doi:10.1016/j.psychres.2017.12.014
57. Poole JC, Dobson KS, Pusch D. Childhood adversity and adult depression: the protective role of psychological resilience. Child Abuse Negl. 2017;64:89–100.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.