Back to Journals » Patient Preference and Adherence » Volume 17
Psychiatric Patients’ Perceived Health Control and Reactance: Implications for Medication Adherence
Authors De las Cuevas C ![]()
Received 17 April 2023
Accepted for publication 5 July 2023
Published 8 July 2023 Volume 2023:17 Pages 1591—1601
DOI https://doi.org/10.2147/PPA.S417608
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Carlos De las Cuevas1,2
1Department of Internal Medicine, Dermatology and Psychiatry, Universidad de La Laguna, San Cristóbal de La Laguna, Canary Islands, Spain; 2Instituto Universitario de Neurociencia (IUNE), Universidad de La Laguna, San Cristóbal de La Laguna, Canary Islands, Spain
Correspondence: Carlos De las Cuevas, Department of Internal Medicine, Dermatology and Psychiatry, Faculty of Medicine of the University of La Laguna, San Cristóbal de La Laguna, Canary Islands, Spain, Tel +34-922-316502, Fax +34-922-319353, Email [email protected]
Abstract: Adherence to prescribed treatment is a major challenge in psychiatry, with non-adherence rates estimated to be as high as 50%. Two factors that have been suggested to influence medication adherence in psychiatric patients are perceived health control and psychological reactance. Perceived health control refers to the belief that one can control their own health outcomes, while psychological reactance refers to the negative response that occurs when individuals perceive their freedom or autonomy to be threatened. The aim of this review is to explore the possible relevance and interaction of perceived health control and psychological reactance in the adherence of psychiatric patients to their treatment. Several studies have suggested that higher levels of perceived health control are associated with better medication adherence, while higher levels of psychological reactance are associated with poorer adherence. Moreover, it has been suggested that patients with high levels of perceived health control may be more likely to experience psychological reactance if they feel that their autonomy is threatened by the treatment regimen. Taken together, these findings suggest that perceived health control and psychological reactance may interact to influence medication adherence in psychiatric patients. Future research could explore ways to enhance patients’ perceived health control while minimizing psychological reactance in order to improve treatment adherence in this population.
Keywords: health locus of control, psychological reactance, psychiatric patients, treatment adherence
Plain Language Summary
Why was the review done? Perceived health control and psychological reactance are related concepts that could be used in health psychology research to understand how individuals make decisions about their health behaviors.
What did the authors do? The authors reviewed the literature about how health locus of control and psychological reactance are associated with psychiatric patients’ adherence to prescribed medications and compared these findings with corresponding to their studies over the last decade in relatively stable outpatients in community psychiatric treatment setting.
What do these results mean? Perceived health control and psychological reactance are really useful concepts in clinical psychiatry practice that can be used to tailor treatment plans, improve treatment adherence, promote patient engagement and empowerment, allowing clinicians to work towards improving patient outcomes and promoting positive health behaviors.
The Unmet Challenge of Medication Non-Adherence in Psychiatric Patients
Although a systematic re‐assessment of recent evidence across multiple meta‐analyses has shown that the efficacy of pharmacotherapies for mental disorders in adults has been overestimated and provided limited additional gain over placebo,1 available psychiatric medications still can be useful in treating a variety of mental health conditions, including depression, anxiety, bipolar disorder, and schizophrenia. However, their effectiveness depends on a number of factors, including the specific medication, the individual’s unique biology and psychological makeup, and their adherence to the prescribed regimen.2,3 Adequate adherence to psychiatric medications is crucial for achieving optimal treatment outcomes. This means taking medications as directed, at the correct time and dose, and for the full duration of the treatment course.4
The magnitude and relevance of the problem of non-adherence to psychiatric treatment are significant. Research indicates that non-adherence rates among psychiatric patients range from 20–50%, depending on the condition and treatment modality.5–8 This suggests that a large proportion of psychiatric patients are not receiving the full benefits of their treatment, leading to significant personal and societal costs.
Non-adherence to prescribed medication can lead to a range of negative consequences for the psychiatric patient, including increased risk of relapse and hospitalization,9,10 and even suicide.11 In addition to the personal toll of inadequate adherence, there are also significant economic costs associated with the problem. Non-adherence can lead to increased healthcare utilization, including emergency department visits and hospitalizations, as well as increased use of costly interventions. This results in increased healthcare spending and reduced efficiency of healthcare systems (Hong et al, 2011; King et al, 2014; Ho et al, 2016).12–14
Overall, the study of adherence to psychiatric treatment is complex and multi-faceted. Understanding the factors that contribute to non-adherence and developing effective strategies to address the problem is critical for improving the quality of life for individuals with psychiatric conditions and reducing the burden on healthcare systems. According to the literature, there are several factors that can influence treatment adherence in psychiatry. Some of the most common predictors of poor adherence to psychiatric treatment include: side effects of medications, complexity of treatment regimens, stigma associated with psychiatric illness, lack of social support, financial barriers, and substance abuse. On the other hand, some of the most consistent predictors of adherence include: therapeutic alliance, perceived benefits of treatment, social support, and access to health care.15–17
Concerning patient characteristics, research has shown that patients’ beliefs and attitudes about their illness and treatment are strongly associated with treatment adherence in psychiatry.18 It is important for healthcare providers to assess patients’ beliefs about their illness and treatment and to address any concerns or misconceptions that may be interfering with treatment adherence. By working with patients to develop a shared understanding of their illness and treatment options, healthcare providers can improve patients’ engagement with treatment and promote better outcomes.
Therefore, it is essential to study this unmet challenge and develop strategies to improve medication adherence. By doing so, clinicians can enhance treatment outcomes, increase patients’ quality of life, and reduce healthcare costs. Moreover, addressing medication non-adherence in psychiatric patients can also contribute to reducing stigma and promoting awareness about mental health issues, thus benefiting society as a whole.
The primary purpose of this traditional or narrative literature review is to analyze and summarize, through a critical approach, the body of literature concerning the roles of perceived health control and psychological reactance in the adherence of psychiatric patients to their treatment. This will be achieved by presenting a comprehensive background of the literature published in PubMed on these topics up to March 2023.
The Health Belief Model Approach
The Health Belief Model (HBM) is a theoretical framework used in healthcare to understand patients’ health-related beliefs and behaviors. The model suggests that an individual’s decision to engage in health-related behaviors is influenced by their perception of the severity and susceptibility of an illness or health condition, the benefits and barriers associated with engaging in a particular behavior, and their self-efficacy or confidence in their ability to engage in the behavior.19,20 The HBM can be useful in the study of patients’ treatment adherence because it helps to identify factors that may be influencing patients’ decision to follow a treatment plan.21
Within this model, two factors that have been suggested to influence medication adherence in psychiatric patients are perceived health control and psychological reactance.
Perceived Health Control
The perception of control is a complex psychological phenomenon that plays an important role in human cognition, behavior, and well-being.22 While it is not necessarily a biological necessity, it is a fundamental aspect of human psychology that has evolved to help us navigate our environment and cope with the challenges of life.
Research suggests that the perception of control can have a significant impact on our mental and physical health, as well as our sense of self-efficacy and resilience.23 When we feel in control, we are more likely to take initiative, persevere in the face of obstacles, and experience a greater sense of well-being. Conversely, when we feel out of control, we may experience feelings of helplessness, anxiety, and depression.
The perception of health control of a patient is influenced by a variety of factors, including their individual beliefs as self-efficacy, past experiences with illness or medical treatment, social support and cultural beliefs and values can shape a patient’s perception of health control.24,25 For example, some research suggests that people who grow up in environments that are unpredictable or chaotic may be more likely to develop a heightened need for control as a way of coping with uncertainty.26
Control beliefs refer to an individual’s perception of their ability to influence or control their environment, which can include and determinate their health behaviors and outcomes.27
Perceived health control and health locus of control are related constructs that both refer to an individual’s beliefs about their ability to control their health outcomes. However, they differ in their focus and scope. Perceived health control is a broad construct that encompasses an individual’s beliefs about their ability to influence their health outcomes through actions such as engaging in healthy behaviors and seeking medical care. It is a more general construct that includes both internal and external factors that can affect one’s health. Health locus of control, on the other hand, is a more specific construct that focuses on an individual’s beliefs about the degree to which their health is influenced by internal or external factors. Specifically, it refers to the extent to which individuals believe that their health is determined by their own actions (internal locus of control) or by external factors such as fate, luck, or the actions of others, such as their doctors (external locus of control).28 It is possible for an individual to have a strong sense of perceived health control but still believe that external factors play a significant role in determining their health outcomes. Conversely, an individual may have an internal locus of control regarding their health but still feel that they have little control over other aspects of their life.29 Overall, both perceived health control and health locus of control are important constructs to consider in healthcare settings as they can impact patients’ health behaviors and treatment outcomes. Understanding patients’ beliefs about their ability to control their health outcomes can help healthcare providers develop more effective interventions to promote health and well-being. In the context of adherence to prescribed treatment, the perception of health control can be a useful factor to study because it can influence an individual’s willingness to follow a prescribed treatment regimen.
In psychiatric clinical practice, De las Cuevas et al (2016)28 have shown that psychiatric outpatients believe their psychiatrists have more influence over their mental health status, even though they know that their own actions can also help them cope with their mental disorder. This supports the dual health control hypothesis, highlighting the relevance in treatment adherence of the balance between external and internal health control beliefs. Patients no-control believers, ie, those with low internal and low external health control beliefs, were more likely to adhere to take an active role in managing their condition and adhere to prescribed treatments, while patients dual-control believers, ie, those with high internal and high external health control beliefs, may feel less motivated to adhere to treatment or to make lifestyle changes that could improve their health.
Therefore, understanding an individual’s perception of health control can help healthcare providers identify patients who may be at risk for non-adherence to prescribed treatments. By addressing these patients’ beliefs about their ability to control their health, healthcare providers can help improve their adherence to treatment and ultimately improve their health outcomes.
Psychological Reactance
Psychological reactance is a term used to describe the emotional and cognitive response that individuals have when they feel that their freedom or autonomy is being threatened or restricted.30,31 It is a complex phenomenon that can be influenced by a variety of factors, including the individual’s sense of control, the perceived importance of the freedom being threatened, the way in which the restriction is communicated, and individual differences in personality such as personality traits.32,33
In healthcare settings, psychological reactance may arise when patients feel that their healthcare provider is trying to exert too much control over their treatment decisions, leading them to resist or reject medical advice. When a patient feels that their freedom to make decisions about their healthcare is being restricted, they may experience reactance and be less likely to adhere to prescribed treatment.34,35 For example, if a healthcare provider takes an overly authoritarian approach to treatment, patients may feel that their autonomy is being threatened and be less willing to follow the prescribed regimen.
In the context of adherence to prescribed treatment, a patient’s psychological reactance can be influenced by several factors, such as:
- Perceived threat to autonomy:31 If a patient perceives that their freedom or autonomy is being threatened by a healthcare provider or treatment regimen, they may experience reactance. This can occur when a patient feels that their preferences or values are not being taken into account or when they feel that they are being coerced or forced to comply with treatment.
- Communication style:36 The communication style of a healthcare provider can also influence psychological reactance. For example, an overly authoritarian or paternalistic approach may be more likely to trigger reactance than a collaborative approach that involves the patient in decision-making.
- Treatment complexity:37 Treatment regimens that are complex or difficult to follow may also increase the likelihood of psychological reactance. Patients may feel that their autonomy is being restricted by the demands of the treatment regimen, leading to resistance or non-adherence.
- Previous experiences:33 Previous experiences with healthcare providers or treatment regimens can also influence psychological reactance. Patients who have had negative experiences may be more likely to experience reactance in the future, particularly if they perceive that their autonomy is being threatened.
In clinical community psychiatric practice, De las Cuevas et al (2014)38 found that in psychiatric outpatients, those with higher levels of reactance proneness (both affective and cognitive) demonstrated lower levels of adherence to their prescribed treatment. The study also noted that patients with high reactance proneness often had an internal attribution of change, which led them to rely on their own resources, personal decisions, and initiatives. On the other hand, patients with low reactance proneness typically had an external attribution of change, which frequently caused them to seek external help and support to achieve their treatment goals. Through the use of structural equation modeling, De las Cuevas et al (2017)39 found that psychiatric patients’ adherence to prescribed treatment was associated with various factors. Firstly, they evidenced a negative association between adherence and cognitive psychological reactance, meaning that as cognitive psychological reactance increased, adherence decreased. Secondly, patients’ trust in their psychiatrists (doctors’ subscale) was positively associated with adherence. Thirdly, patients’ belief that they were in control of their mental health and that their mental health depended on their own actions (internal subscale) was negatively associated with adherence. Additionally, the study found that self-efficacy indirectly influenced treatment adherence through internal health locus of control.
By understanding the role of psychological reactance in adherence to prescribed treatment, healthcare providers can take steps to reduce reactance and improve patient adherence. This may involve taking a more collaborative approach to treatment, involving patients in decision-making and providing them with information about the benefits and risks of different treatment options.40 Additionally, healthcare providers can work to build trust with patients and create a supportive environment that encourages patient autonomy and empowerment.41,42
In addition, the patient’s level of psychological reactance can guide the patient’s therapeutic approach. Based on Beutler et al’s (2002)43 findings, it appears that psychiatric patients who exhibit higher levels of psychological reactance may benefit more from nondirective therapies, while those with lower levels of reactance may benefit more from directive therapies like cognitive-behavioral therapy.
Overall, the factors that contribute to psychological reactance in the context of healthcare are complex and multifactorial. By understanding the conditions that contribute to reactance, healthcare providers can take steps to reduce reactance and improve patient adherence to prescribed treatment.
How to Measure Health Locus of Control and Psychological Reactance
The measurement of health locus of control and psychological reactance have great utility in understanding how individuals perceive and respond to health-related information and interventions. By measuring an individual’s beliefs about their control over their health outcomes (health locus of control) and their emotional and cognitive responses to perceived threats to their freedom and autonomy (psychological reactance), healthcare professionals and researchers could gain a more comprehensive understanding of how individuals engage with health-related information and interventions.
There are several commonly used instruments to measure health locus of control and psychological reactance, but the Multidimensional Health Locus of Control Scale and the Hong Psychological Reactance Scale are the most widely used in research and clinical settings.
Multidimensional Health Locus of Control Scale (MHLC-C)
The MHLC-C is a self-report scale consisting of 18 items designed to measure individuals’ beliefs about what influences their health with respect to any medical or health-related condition.44 The MHLC consists of 18 items, with six items for each dimension. Participants rate their level of agreement with each item on a 6-point Likert scale ranging from “strongly disagree” to “strongly agree”. The scores for each dimension are then calculated separately, with higher scores indicating a stronger belief in that particular dimension of health locus of control. This scale can be easily adapted for use in various contexts. It includes two general dimensions, namely internal and external health locus of control. The internal health control dimension comprises six items that evaluate patients’ beliefs about the extent to which their health is influenced by their behavior. On the other hand, the external health control dimension consists of 12 items and is further divided into three subscales: the Chance subscale, which assesses the belief in fate/luck controlling patients’ health status; the Doctors subscale, which assesses the belief that healthcare professionals have control over patients’ health status; and the Other People subscale, which assesses the belief that other significant people have control over patients’ health status. High scores in the corresponding dimensions indicate high levels of control beliefs.
Hong Psychological Reactance Scale (HPRS)
The HPRS is a self-report questionnaire consisting of 14 items that measures individual differences in reactance proneness. This refers to an individual’s trait propensity to experience psychological reactance. The concept of psychological reactance, as proposed by Hong and Faedda in 1996,45 suggests that when an individual perceives a threat to their freedom, they will be motivated to restore it. Participants respond to each statement in the questionnaire, which can be cognitive (HPRS-C) or affective (HPRS-A), on a five-point Likert scale ranging from strongly disagree (1) to strongly agree (5).
The Patient’s Health Belief Questionnaire on Psychiatric Treatment
Overall, an instrument measuring both health locus of control and psychological reactance could have significant practical applications in the healthcare field and could contribute to a better understanding of the complex interplay between individual beliefs, emotions, and health behaviors. For example, understanding an individual’s health locus of control and psychological reactance could help healthcare professionals tailor their communication and intervention strategies to better resonate with the individual’s beliefs and values, ultimately leading to greater engagement and adherence to treatment plans. Additionally, researchers could use this instrument to gain insights into the factors that influence individuals’ health behaviors and develop interventions that are more effective in promoting positive health outcomes.
Based on items from the Drug Attitude Inventory, the MHLC-C and the HPRS, De las Cuevas et al (2019)46 clinimetrically designed the Patient’s Health Belief Questionnaire on Psychiatric Treatment (PHBQ-PT), a self-report measure designed to assess attitudes and health beliefs predicting treatment adherence of patients with psychiatric disorders.
The PHBQ-PT consists of 17 items that assess four domains of health beliefs or attitudes toward psychiatric medication: positive aspects of medication, negative aspects of medication, internal health locus of control, doctor health locus of control, and psychological reactance. Therefore, PHBQ-PT assess psychiatric patient attitudes toward prescribed treatment, the extent to which a patient feels in control of their health outcomes, as well as the extent to which the patient feels that their autonomy or freedom is being threatened by healthcare providers or treatment regimens.
Each item is rated on a 6-point Likert scale ranging from 1 = strongly disagree to 6 = strongly agree. The PHBQ-PT has been used in various studies to assess health beliefs and treatment adherence in patients with psychiatric disorders, including depression, bipolar disorder, and schizophrenia.47–51
Overall, the PHBQ-PT is a useful tool for assessing health beliefs and treatment adherence in patients with psychiatric disorders, and can help healthcare providers tailor their approach to treatment to improve patient outcomes.
The scores of the five subscales of the instrument can be splitted according to the median score to generate high and low score groups that can be combined producing attitudinal and/or beliefs groups with clinical significance and capable of predicting patient adherence to the prescribed treatment.
The positive and negative aspects of medication subscales combination could generate four attitudinal groups: pharmacophobic (low positive, high negative), indecisive (high positive, high negative), unconcerned (low positive, low negative), and pharmacophilic (low negative, high positive).
The internal and doctor health locus of control subscales combination could generate four types of beliefs about the responsibility for management of the psychiatric disorder: the patient (low doctor, high internal), both (high doctor, high internal), no control (low doctor, low internal), and the psychiatrist (low internal, high doctor).
The psychological reactance and doctor health locus of control subscales combination could generate four types of beliefs about the psychiatric-patient relationship: intransigent (low doctor, high reactance), discordant (high doctor, high reactance), indifferent (low doctor, low reactance), and complacent (low reactance, high doctor).
Table 1 shows the dimensions of the questionnaire and its component symptoms. Figures 1-3 represent graphically the possible interactions between the dimensions with possible clinical significance. Having information about health locus of control, psychological reactance, and attitudes towards medication of psychiatric patients is relevant because it allows healthcare providers to gain a more complete understanding of the patient’s perspective and the factors that may be contributing to non-adherence to prescribed treatments. This knowledge can inform personalized interventions and support that are tailored to the individual patient’s needs, preferences, and beliefs. By addressing these factors, healthcare providers can help to improve medication adherence and ultimately achieve better treatment outcomes and quality of life for patients with psychiatric conditions. Future studies need to verify and further extend the validity of the attitudinal and/or beliefs groups in prediction treatment adherence.
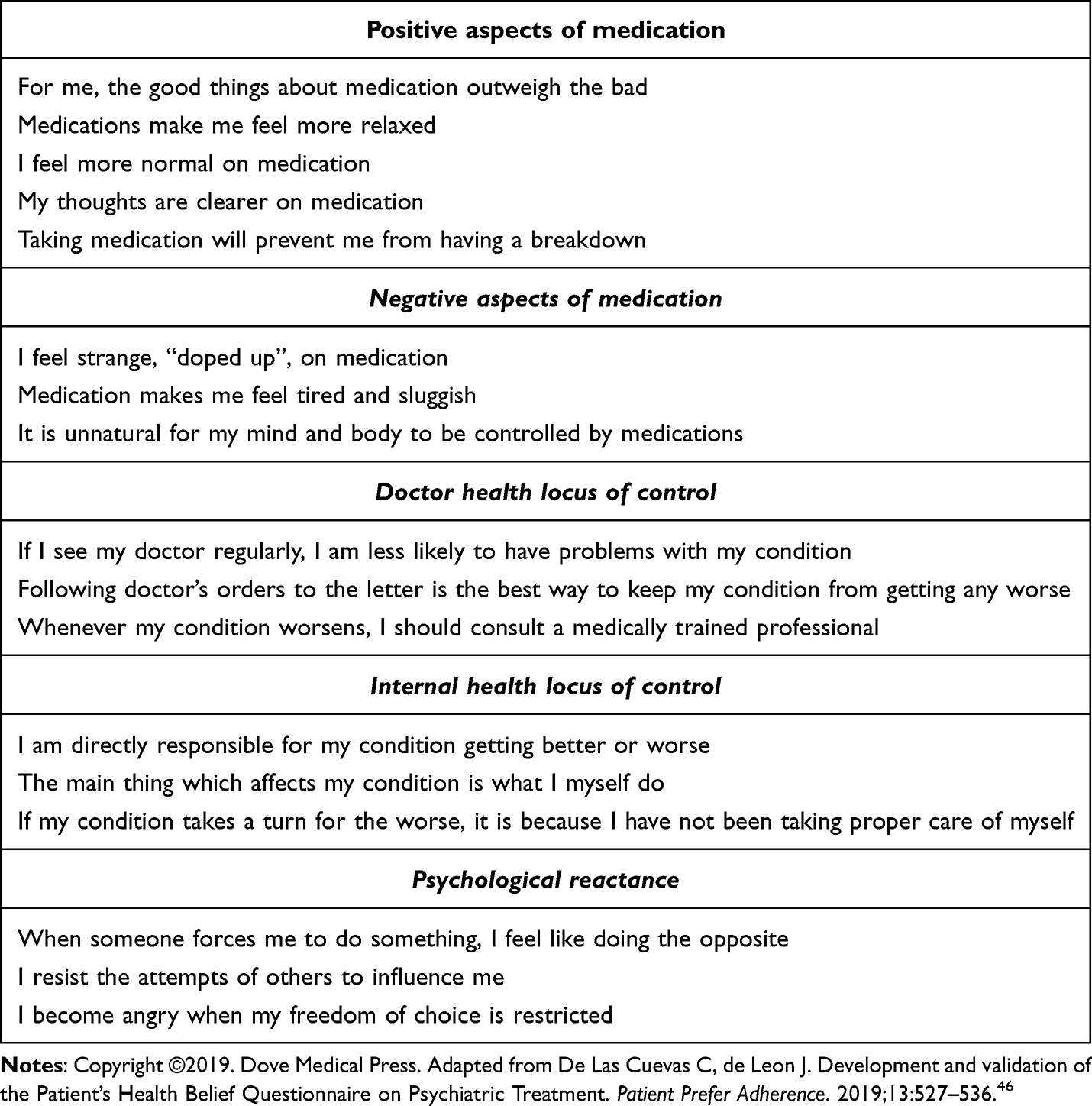 |
Table 1 Patient’s Health Belief Questionnaire on Psychiatric Treatment (PHBQ-PT) Dimensions and Component Items |
 |
Figure 1 Graphic representation of the interaction between the dimensions positive and negative aspects of medication defining the four groups of attitudes towards prescribed psychiatric medications. |
 |
Figure 2 Graphic representation of the interaction between the dimensions internal and doctor health locus of control defining the four groups of beliefs about who is responsible for management of the psychiatric disorder. |
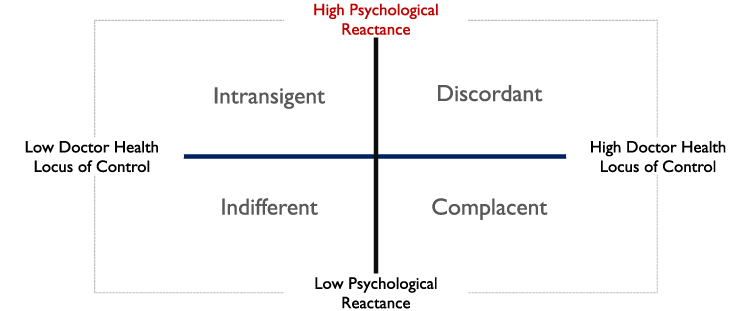 |
Figure 3 Graphic representation of the interaction between the dimensions doctor health locus of control and psychological reactance defining the four groups of preferred type of psychiatrist-patient relationship. |
Finally, although self-reported questionnaires have long been a valuable tool for researchers to gather information on various psychological, behavioral, and sociological constructs, however, it is crucial to acknowledge and address the limitations and biases inherent in relying solely on self-reported data. One significant limitation is the potential for response bias, where participants may consciously or unconsciously provide inaccurate or distorted information. Additionally, social desirability bias may influence respondents to present themselves in a more socially desirable light, leading to biased results. Moreover, memory recall bias can impact the accuracy of self-reported information as individuals may struggle to accurately remember past events or experiences.
How to Promote Perceived Health Control and Reduce Psychological Reactance?
Promoting perceived health control and reducing psychological reactance can be challenging and requires a multifaceted approach that addresses both individual and environmental factors. There are several strategies that can be effective to help individuals feel more in control of their health outcomes and promote healthy behaviors:52–55
- Provide clear and concise information: When providing information about health behaviors or interventions, it is important to be clear and concise. Providing too much information or using complicated terminology can increase feelings of psychological reactance. On the other hand, clear and concise information can help individuals feel more in control of their health outcomes.
- Offer choice: When possible, offer individuals a choice of different health behaviors or interventions. This can help individuals feel more in control of their health outcomes and reduce feelings of psychological reactance. It is important to ensure that the choices offered are all healthy and appropriate for the individual.
- Use positive messaging: When communicating about health behaviors or interventions, it is important to use positive messaging that emphasizes the benefits of healthy behaviors rather than the risks of unhealthy behaviors. This can help individuals feel more in control of their health outcomes and reduce feelings of psychological reactance.
- Enhance self-efficacy: Enhancing individuals’ self-efficacy can help promote perceived health control. This can be achieved by providing opportunities for success, giving positive feedback, and highlighting the individual’s strengths and abilities.
- Create supportive environments: Creating environments that support healthy behaviors can help individuals feel more in control of their health outcomes and reduce feelings of psychological reactance. This can include providing access to healthy foods, safe places to exercise, and social support.
- Involve individuals in decision-making: Involving individuals in decision-making about their health behaviors or interventions can help promote perceived health control and reduce feelings of psychological reactance. This can be achieved by asking individuals about their preferences and goals, and incorporating these into the decision-making process.
As a conclusion of this review, it becomes evident that in psychiatric clinical practice, understanding perceived health control and psychological reactance can be really useful in empowering patients to effectively manage their health and overall well-being. Patients who feel a sense of control over their health may be more receptive to interventions and may be more likely to engage in behaviors that promote their overall health. Healthcare providers can work with patients to identify ways in which they can take an active role in managing their health, which can increase patients’ perceived health control and lead to better health outcomes. At the same time, healthcare providers must be aware of the potential for psychological reactance to arise in clinical settings. By providing patients with information and involving them in the decision-making process, healthcare providers can help patients feel more in control of their healthcare while minimizing the risk of reactance. Additionally, healthcare providers can take steps to build trust and rapport with patients, which can help reduce reactance and improve patient outcomes.
Disclosure
No commercial organizations had any role in the completion or publication of this study. The author declares no conflicts of interest in relation to the subject of the study.
References
1. Leichsenring F, Steinert C, Rabung S, Ioannidis JPA. The efficacy of psychotherapies and pharmacotherapies for mental disorders in adults: an umbrella review and meta-analytic evaluation of recent meta-analyses. World Psychiatry. 2022;21(1):133–145. doi:10.1002/wps.20941
2. Xu J, Mercury J, Zhang Z, Xu F. Psychological, social and behavioural factors that influence drug efficacy: a noteworthy research subject in clinical pharmacology. Br J Clin Pharmacol. 2008;66(6):901–902. doi:10.1111/j.1365-2125.2008.03300.x
3. Brown MT, Bussell JK. Medication adherence: WHO cares? Mayo Clin Proc. 2011;86(4):304–314. doi:10.4065/mcp.2010.0575
4. De Las Cuevas C. Towards a clarification of terminology in medicine taking behavior: compliance, adherence and concordance are related although different terms with different uses. Curr Clin Pharmacol. 2011;6(2):74–77. doi:10.2174/157488411796151110
5. Nosé M, Barbui C, Tansella M. How often do patients with psychosis fail to adhere to treatment programmes? A systematic review. Psychol Med. 2003;33(7):1149–1160. doi:10.1017/s0033291703008328
6. Jónsdóttir H, Opjordsmoen S, Birkenaes AB, et al. Medication adherence in outpatients with severe mental disorders: relation between self-reports and serum level. J Clin Psychopharmacol. 2010;30(2):169–175. doi:10.1097/JCP.0b013e3181d2191e
7. Chapman SC, Horne R. Medication nonadherence and psychiatry. Curr Opin Psychiatry. 2013;26(5):446–452. doi:10.1097/YCO.0b013e3283642da4
8. Semahegn A, Torpey K, Manu A, Assefa N, Tesfaye G, Ankomah A. Psychotropic medication non-adherence and its associated factors among patients with major psychiatric disorders: a systematic review and meta-analysis. Syst Rev. 2020;9(1):17. doi:10.1186/s13643-020-1274-3
9. Morken G, Widen JH, Grawe RW. Non-adherence to antipsychotic medication, relapse and rehospitalisation in recent-onset schizophrenia. BMC Psychiatry. 2008;8:32. doi:10.1186/1471-244X-8-32
10. Tiihonen J, Haukka J, Taylor M, Haddad PM, Patel MX, Korhonen P. A nationwide cohort study of oral and depot antipsychotics after first hospitalization for schizophrenia. Am J Psychiatry. 2011;168(6):603–609. doi:10.1176/appi.ajp.2011.10081224
11. Lindström E, Eriksson L, Levander S. Suicides during 7 years among a catchment area cohort of patients with psychoses. Nord J Psychiatry. 2012;66(1):8–13. doi:10.3109/08039488.2011.577186
12. Hong J, Reed C, Novick D, Haro JM, Aguado J. Clinical and economic consequences of medication non-adherence in the treatment of patients with a manic/mixed episode of bipolar disorder: results from the European Mania in Bipolar Longitudinal Evaluation of Medication (EMBLEM) study. Psychiatry Res. 2011;190(1):110–114. doi:10.1016/j.psychres.2011.04.016
13. King D, Knapp M, Patel A, et al. The impact of non-adherence to medication in patients with schizophrenia on health, social care and societal costs. Analysis of the QUATRO study. Epidemiol Psychiatr Sci. 2014;23(1):61–70. doi:10.1017/S2045796013000097
14. Ho SC, Chong HY, Chaiyakunapruk N, Tangiisuran B, Jacob SA. Clinical and economic impact of non-adherence to antidepressants in major depressive disorder: a systematic review. J Affect Disord. 2016;193:1–10. doi:10.1016/j.jad.2015.12.029
15. Forsner T, Hansson J, Brommels M, Wistedt AA, Forsell Y. Implementing clinical guidelines in psychiatry: a qualitative study of perceived facilitators and barriers. BMC Psychiatry. 2010;10:8. doi:10.1186/1471-244X-10-8
16. Sendt KV, Tracy DK, Bhattacharyya S. A systematic review of factors influencing adherence to antipsychotic medication in schizophrenia-spectrum disorders. Psychiatry Res. 2015;225(1–2):14–30. doi:10.1016/j.psychres.2014.11.002
17. Alcalá JÁ, Fontalba-Navas A, Company-Morales M, Romero-Guillena SL, Gutiérrez-Higueras T, Gutiérrez-Rojas L. Facilitators and Barriers of Medication Adherence Based on Beliefs of Persons with Bipolar Disorder: a Qualitative Study. Int J Environ Res Public Health. 2022;19(13):7633. doi:10.3390/ijerph19137633
18. De Las Cuevas C, de Leon J. Reviving Research on Medication Attitudes for Improving Pharmacotherapy: focusing on Adherence. Psychother Psychosom. 2017;86(2):73–79. doi:10.1159/000450830
19. Rosenstock IM, Strecher VJ, Becker MH. Social learning theory and the Health Belief Model. Health Educ Q. 1988;15(2):175–183. doi:10.1177/109019818801500203
20. Rosenstock IM. Historical origins of the health belief model. Health Educ Monogr. 1974;2:328–335.
21. Jones CJ, Smith H, Llewellyn C. Evaluating the effectiveness of health belief model interventions in improving adherence: a systematic review. Health Psychol Rev. 2014;8(3):253–269. doi:10.1080/17437199.2013.802623
22. Leotti LA, Iyengar SS, Ochsner KN. Born to choose: the origins and value of the need for control. Trends Cogn Sci. 2010;14(10):457–463. doi:10.1016/j.tics.2010.08.001
23. Thompson SC, Spacapan S. Perceptions of control in vulnerable populations. J Soc Issues. 1991;47:1–21. doi:10.1111/j.1540-4560.1991.tb01831.x
24. Leventhal H, Nerenz DR, Steele DJ. Illness Representations and Coping with Health Threats. In: Baum A, Taylor SE, Singer JE, editors. Handbook of Psychology and Health, Volume IV: Social Psychological Aspects of Health, Erlbaum. Hillsdale, NJ; 1984:219–252.
25. Trafimow D, Sheeran P, Conner M, Finlay KA. Evidence that perceived behavioural control is a multidimensional construct: perceived control and perceived difficulty. Br J Soc Psychol. 2002;41(Pt 1):101–121. doi:10.1348/014466602165081
26. Taylor SE. Stress and Coping, in “Health Psychology”.
27. Grotz M, Hapke U, Lampert T, Baumeister H. Health locus of control and health behaviour: results from a nationally representative survey. Psychol Health Med. 2011;16(2):129–140. doi:10.1080/13548506.2010.521570
28. De Las Cuevas C, Peñate W, Cabrera C. Perceived Health Control: a Promising Step Forward in Our Understanding of Treatment Adherence in Psychiatric Care. J Clin Psychiatry. 2016;77(10):e1233–e1239. doi:10.4088/JCP.15m09769
29. De Las Cuevas C, Peñate W, Betancort M, Cabrera C. What do psychiatric patients believe regarding where control over their illness lies? Validation of the multidimensional health locus of control scale in psychiatric outpatient care. J Nerv Ment Dis. 2015;203(2):81–86. doi:10.1097/NMD.0000000000000244
30. Brehm JW. Responses to Loss of Freedom: A Theory of Psychological Reactance. Morristown, NJ: General Learning Press; 1972.
31. Brehm SS, Brehm JW. Psychological Reactance: A Theory of Freedom and Control. London: Academic Press, Inc; 1981.
32. Landau MJ, Kay AC, Whitson JA. Compensatory control and the appeal of a structured world. Psychol Bull. 2015;141(3):694–722. doi:10.1037/a0038703
33. Steindl C, Jonas E, Sittenthaler S, Traut-Mattausch E, Greenberg J. Understanding Psychological Reactance: new Developments and Findings. Z Psychol. 2015;223(4):205–214. doi:10.1027/2151-2604/a000222
34. Graybar SR, Antonuccio DO, Boutilier LR, Varble DL. Psychological reactance as a factor affecting patient compliance to physician advice. Scandinavian J Behav Therapy. 1989;18:43–51. doi:10.1080/16506078909455841
35. Moore A, Sellwood W, Stirling J. Compliance and psychological reactance in schizophrenia. Br J Clin Psychol. 2000;39(3):287–295. doi:10.1348/014466500163293
36. Dillard JP, Shen L. On the Nature of Reactance and its Role in Persuasive Health Communication. Commun Monogr. 2005;72(2):144–168. doi:10.1080/03637750500111815
37. Whitehead D, Russell G. How effective are health education programmes--resistance, reactance, rationality and risk? Recommendations for effective practice. Int J Nurs Stud. 2004;41(2):163–172. doi:10.1016/s0020-7489(03)00117-2
38. De Las Cuevas C, Peñate W, Sanz EJ. The relationship of psychological reactance, health locus of control and sense of self-efficacy with adherence to treatment in psychiatric outpatients with depression. BMC Psychiatry. 2014;14:324. doi:10.1186/s12888-014-0324-6
39. De Las Cuevas C, de Leon J, Peñate W, Betancort M. Factors influencing adherence to psychopharmacological medications in psychiatric patients: a structural equation modeling approach. Patient Prefer Adherence. 2017;11:681–690. doi:10.2147/PPA.S133513
40. Mundal I, Lara-Cabrera ML, Betancort M, De Las Cuevas C. Exploring patterns in psychiatric outpatients’ preferences for involvement in decision-making: a latent class analysis approach. BMC Psychiatry. 2021;21(1):133. doi:10.1186/s12888-021-03137-x
41. Jaeger M, Rossler W. Enhancement of outpatient treatment adherence: patients’ perceptions of coercion, fairness and effectiveness. Psychiatry Res. 2010;180(1):48–53. doi:10.1016/j.psychres.2009.09.011
42. Geller JL. Patient-centered, recovery-oriented psychiatric care and treatment are not always voluntary. Psychiatr Serv. 2012;63(5):493–495. doi:10.1176/appi.ps.201100503
43. Beutler LE, Moleiro C, Talebi H. Resistance in psychotherapy: what conclusions are supported by research. J Clin Psychol. 2002;58(2):207–217. doi:10.1002/jclp.1144
44. Wallston KA, Stein MJ, Smith CA. Form C of the MHLC scales: a condition-specific measure of locus of control. J Pers Assess. 1994;63(3):534–553. doi:10.1207/s15327752jpa6303_10
45. Hong SM, Faedda S. Refinement of the Hong Psychological Reactance Scale. Educ Psychol Meas. 1996;56:173–182. doi:10.1177/0013164496056001014
46. De Las Cuevas C, de Leon J. Development and validation of the Patient’s Health Belief Questionnaire on Psychiatric Treatment. Patient Prefer Adherence. 2019;13:527–536. doi:10.2147/PPA.S201144
47. De Las Cuevas C, Baptista T, Motuca M, et al. Poor Adherence to Oral Psychiatric Medication in Adults with Schizophrenia May Be Influenced by Pharmacophobia, High Internal Health Locus of Control and Treatment Duration. Neuropsychopharmacol Hung. 2021;23(4):388–404.
48. De Las Cuevas C, Motuca M, Baptista T, et al. Poor Adherence to Oral Psychiatric Medication in Adults with Depression: psychological Reactance May Have Specific Effects in Depression. Neuropsychopharmacol Hung. 2021;23(4):374–387.
49. De Las Cuevas C, Villasante-Tezanos GA. Poor Adherence to Oral Psychiatric Medication in Adults with Bipolar Disorder: the Psychiatrist May have More Influence than in Other Severe Mental Illnesses. Neuropsychopharmacol Hung. 2021;23(4):347–362.
50. Lazary J, Pogany L, De Las Cuevas C, Villasante-Tezanos GA, De Leon J. Adherence to psychiatric medications: comparing patients with schizophrenia, bipolar disorder and major depression. Neuropsychopharmacol Hung. 2021;23(4):363–373.
51. Pogany L, De Las Cuevas C, Lazary J. What is the dominant treatment attitude of the psychiatric patients? Neuropsychopharmacol Hung. 2021;23(3):308–318.
52. Dorgeat E, Adeleye A, Lifford KJ, Edwards A. Effectiveness of technological interventions to improve healthcare communication with children with long-term conditions: a systematic review and meta-analysis of randomised controlled trials. Patient Educ Couns. 2022;105(6):1411–1426. doi:10.1016/j.pec.2021.09.033
53. Náfrádi L, Nakamoto K, Schulz PJ. Is patient empowerment the key to promote adherence? A systematic review of the relationship between self-efficacy, health locus of control and medication adherence. PLoS One. 2017;12(10):e0186458. doi:10.1371/journal.pone.0186458
54. Rains SA, Mitchell Turner M. Psychological Reactance and Persuasive Health Communication: a Test and Extension of the Intertwined Model. Hum Commun Res. 2007;33:241–269. doi:10.1111/j.1468-2958.2007.00298.x
55. Reynolds-Tylus T. Psychological Reactance and Persuasive Health Communication: a Review of the Literature. Front Commun. 2019;4(56):1–12. doi:10.3389/fcomm.2019.00056
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.