Back to Journals » Drug, Healthcare and Patient Safety » Volume 14
Psychiatric Disorders and Genotoxicity Following Primary Metal on Polyethylene Total Hip Arthroplasty and Their Correlation to Cobalt/Chromium Levels
Authors Abdel Hamid OI ![]() , Attia ME, Hirshon JM
, Attia ME, Hirshon JM ![]() , El-Shinawi M, El-Hussaini M, El-Setouhy M
, El-Shinawi M, El-Hussaini M, El-Setouhy M ![]()
Received 31 January 2022
Accepted for publication 4 July 2022
Published 18 July 2022 Volume 2022:14 Pages 97—111
DOI https://doi.org/10.2147/DHPS.S360643
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Siew Siang Chua
Omaima I Abdel Hamid,1 Mohamed E Attia,2 Jon M Hirshon,3,4 Mohamed El-Shinawi,5,6 Moustafa El-Hussaini,7 Maged El-Setouhy7,8
1Forensic Medicine and Clinical Toxicology Department, Faculty of Medicine, Zagazig University, Zagazig, Egypt; 2Orthopedics Departments, Faculty of Medicine, Zagazig University, Zagazig, Egypt; 3Department of Emergency Medicine, University of Maryland, School of Medicine, Baltimore, MD, USA; 4Department of Epidemiology and Public Health, University of Maryland, School of Medicine, Baltimore, MD, USA; 5Department of General Surgery, Faculty of Medicine, Ain Shams University, Cairo, Egypt; 6Galala University, Galala City, Suez, Egypt; 7Department of Community, Environmental and Occupational Medicine, Faculty of Medicine, Ain Shams University, Cairo, Egypt; 8Department of Family and Community Medicine, Faculty of Medince, Jazan University, Jazan, Kingdom of Saudi Arabia
Correspondence: Omaima I Abdel Hamid, Forensic Medicine and Clinical Toxicology Department, Faculty of Medicine, Zagazig University, Zagazig, Egypt, Tel +201001664310, Email [email protected]
Introduction: Hip arthroplasty (HA) using implantable metal components is among the commonest orthopedic interventions. However, it can be followed by several complications following corrosion and the release of metal ions. Several studies proved that damaged genomic DNA may contribute to the pathophysiology of mental disorders.
Aim: The current work aims to evaluate the psychiatric disorders in metal on polyethylene hip arthroplasty (MOP-HA) patients and its correlation to cobalt/chromium (Co/Cr) levels and genotoxicity.
Methods: The work was a longitudinal follow-up study including 34 adults with unilateral primary MOP-HA meeting the inclusion and exclusion criteria. Preoperatively, 6, 12-months-postoperatively, patients were examined for cognitive impairment using mini-mental-state-examination (MMSE), depression using major-depressive-inventory (MDI), and blood samples were collected for estimation of Co/Cr, detection of genotoxicity by single-cell-gel-electrophoresis (comet assay) and serum 8-hydroxy-2’–deoxyguanosine (8-OHdG).
Results: Cognitive impairment was reported in 18.5% and 14.8% at 6-months, and 12-months postoperative, respectively. Depressive disorder was recorded in 22.2% at 6-months and 14.8% at 12-months postoperative. The marginal homogeneity tests proved a non-significant difference. There was a non-significant difference in preoperative, 6-months, 12-months postoperative MMSE, and MDI scores. There were significantly increased Co/Cr levels at 6-months postoperative. The levels decreased at 12-months postoperative, however, still significantly higher than preoperative values. There was a significant increase in serum 8-OHdG and the levels were positively correlated to cobalt levels at both 6 and 12-months-postoperative. There was a non-significant difference among preoperative, 6-months, and 12-months postoperative comet assay measurements.
Conclusion: From previous findings, we can conclude that will-functioning MOP hip arthroplasty can induce increased ion levels and positively correlated increase in biochemical markers of genotoxicity (8-OHdG).
Keywords: metal on polyethylene hip arthroplasty, cobalt, chromium, major depressive inventory, mini-mental state examination, genotoxicity
Introduction
Worldwide, there is a dramatic increase in the number of orthopedic surgeries required for hip replacements and total hip arthroplasty (THA) has become one of the most commonly performed surgical procedures.1 Over 200,000 total hip arthroplasty (THA) are performed in the United States annually, and the need for primary THAs is expected to expand by 174% to 574,000 by 2030.2 Although there are no adequate statistics for the THA in Egypt, it is estimated that the number of THA has increased by almost 30% in many countries between 2007 and 2017.3 This surgery is not limited to the elderly as there is an increasing number of hip arthroplasty performed in younger patients with approximately one-third of these surgeries being performed under 60 years of age and 40% being performed under the age of forty.4 Femoral neck fracture and osteoarthritis (OA) are two of the medical conditions necessitating a hip replacement and are most frequently carried out.5 Osteoarthritis may be primary which is diagnosed in the absence of trauma or disease but is associated with risk factors such as age, female gender, obesity anatomical factors, and muscle weakness6 while secondary osteoarthritis occurs with preexisting trauma or diseases such as congenital joint disorders, inflammatory and infectious arthritis, Paget disease, metabolic disorders, Danlos and Marfan syndrome.7 Hip fracture is a major medical issue especially in the elderly population since it is related to high mortality and morbidity.8 The incidence of hip fractures is expanding worldwide along with the expansion of the osteoporotic elderly population.9,10
Hip replacement surgery using implantable metal components has been performed for over 50 years.11 According to the National Joint Registry 18th Annual Report 2021, metal on polyethylene (MoP) is one of the main categories of bearing surfaces for hip replacement.12
However, any metal surrounded by biological systems will corrode, leading to the release of metal ions that cause adverse physiological effects including toxicity, and metal allergy.13,14 Although the majority of cases of hypersensitivity reactions attributed to corrosion products and elevation of cobalt and chromium ions in the blood were reported in metal-on-metal (MOM) implants,15–17 these reactions have been also reported in the metal-on-polyethylene patients.18 Although Bijukumar et al19 showed that the metal wear rate of MOM articulation is approximately 20 times lower than that of MOP articulation, the polyethylene particle wear is reduced in the recently introduced highly cross-linked polyethylene.20 Scully and Teeny21 reported pseudo-tumor formation in a case of MOP total hip arthroplasty. In addition, Cooper et al22 reported corrosion, local tissue reaction, and elevated serum metal levels associated with MoP bearing. The local soft tissue reaction has an exuberant inflammatory nature and is often associated with tissue necrosis/infarction, macrophagic and lymphocytic infiltrate and there is a strong positive correlation between the amount of cobalt and chromium ions and tissue oxidative damage.23 In addition, Eltit et al24 reported adverse local tissue reaction with elevated chemokines, alteration of blood vessels, and elevated levels of cobalt and chromium in the synovial fluid and serum of 17 patients with MoP hip arthroplasty and an equal number of MoM hip arthroplasty patients; they also recorded that MoP systems induce more necrotizing lesions and higher cobalt and chromium levels in the synovial fluid than MoM system.
Cobalt metallosis after revision MoP total hip arthroplasty was reported by Harris et al;25 the condition was manifested by progressively worsening hip pain, memory loss, fatigue, persistent tachycardia, lower extremity sensory loss, and ocular changes associated with elevated cobalt and chromium levels. Even in patients with well-functioning primary MoP total hip replacements, elevated serum metal levels were detected for as long as ten years postoperatively.26
Psychiatric disorders following MoM implant surgery have been recently reported in patients with implant failure requiring revision surgery.27 The authors related these psychiatric problems to one of three mechanisms; either psychological mechanisms such as fear of the possibility of further surgical procedure and continuing problems with pain and mobility or static brain damage caused by Co/Cr toxicity or a dynamic process, that is early-onset dementia sparked by metallosis. However, Clark et al28 reported that chronic exposure to even lower elevated metal levels in asymptomatic patients with well-functioning hip prostheses causes subtle brain structure and function abnormalities.
However, evaluation of the psychiatric disorders in MoP implants which also release cobalt and chromium has not been previously addressed. In addition, understanding the mechanisms underlying the occurrence of psychiatric disorders in these cases remains challenging.
Recently, several studies established the relationship between many psychiatric diseases and a considerably high level of oxidative DNA damage in the brain accompanied by morphological and functional alterations. These findings reveal that damaged genomic DNA may contribute to the pathophysiology of mental disorders.29
Sanson et al30 reported that cobalt and chromium particles released from hip prosthesis can reduce cellular viability, induce DNA damage, and lead to chromosomal aberration. Chromosome translocations and aneuploidy were found in peripheral blood lymphocytes of patients undergoing revision arthroplasty of predominantly metal-on plastic31 and MOM hip replacements.4,32 Briggs et al33 also reported translocation, breaks, loss, and gain of chromosomes in peripheral lymphocytes of patients with MoP hip arthroplasty up to 5 years post-operative. Keegan et al34 reported that exposure to cobalt and chromium both from industry and surgical implants is associated with changes in the peripheral blood, including evidence of oxidative stress.
This current work aims to evaluate the psychiatric disorders in primary MoP hip arthroplasty patients and their correlation to Co/Cr levels and genotoxicity.
Patients and Methods
Ethical Principles
This study was conducted in compliance with the Declaration of Helsinki and after institutional review board (IRB) approval from Ain Shams University (17-9-2017), Zagazig University (4691-26-8-2018), University of Maryland, Baltimore (HP-00077709, 16-11-2018 with modifications approved 7-1-2019). Written informed consent was obtained from patients who agreed to participate after explaining the study objectives, and outcomes and ensuring full confidentiality of data.
Inclusion and Exclusion Criteria
The study included adult patients with a unilateral primary total hip arthroplasty following hip fracture using metal on polyethylene prosthesis [Cobalt chrome metal femoral head with high cross-link polyethylene liner, cementless (Longevity®, from ZIMMER Biomet) without any other metal implant].
The exclusion criteria were patients with depression or psychiatric disorders, patients showing a history of asthma or any hypersensitivity diseases or autoimmune diseases, patients with underlying diseases including end-stage hepatic or renal dysfunction, and patients with occupational exposure to chemicals causing genotoxicity (cobalt, chromium, formaldehyde, hair dyes, lead) or those occupationally exposed to ionizing radiation, patients using medications known to be genotoxic, eg, cancer medications, some antidepressant drugs, corticosteroids, and heavy alcohol drinkers and addicts of other agents proved to be genotoxic including cocaine, cannabis.
Study Design and Procedures
Study Design
The work is a longitudinal follow-up study where the included patients were examined at 0-point (pre-operative) and followed up at 6 and 12 months post-operative. This is based on several previous studies documenting that the peak ion level after metal hip arthroplasty is reached at 3 months,35 6 months,36 6 to 12 months,37 12 months post-operative,38 and other reports of the development of neurological disorders within months following metal implant surgery.39,40
Patient Recruitment and Demographic Data Obtaining
The patients were recruited from Orthopedic Department, Zagazig University Hospitals during the period from February 2020 to August 2020. The demographic data of the patients were obtained. The data included age, gender, residence, education, and socioeconomic status (SES). The socioeconomic status was determined based on the SES scale updated by Fahmy et al.41 The scale assesses several domains including the education domain, economic domain, family domain, and housing sanitation domain. Three classes are categorized namely low socioeconomic status with a score of <40% (<19.2), middle socioeconomic status with a score of 40 to <70% (19.2 to <33.6), and high socioeconomic status with a score of >70% (33.6–48).
Assessment of Cognitive Status Using Mini-Mental State Examination (MMSE)
MMSE was introduced by Folstein et al.42 The test is available in several languages; the Arabic version MMSE-2 which was translated, culturally adapted, and validated by Albanna et al43 was used. In this version, the scales were assessed against the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR) criteria for dementia, as the gold standard. The test takes about 7–10 minutes to complete and it checks a wide series of cognitive functions, including orientation, recall, attention, calculation, language processing, and constructional praxis. The total score is 30 and the cutoff values for the degrees of cognitive deficits were determined according to Folstein and Folstein;44 they considered 27–30 to be normal, 21–26 as mild cognitive impairment, 11–20 as moderate cognitive impairment and ≤10 as severe cognitive. In addition, the most widely used cutoff to suggest dementia is a score of <24 which yielded a sensitivity and specificity of 58% and 98%, respectively.45
Assessment of Depressive Disorder Using Major Depressive Inventory (MDI)
The MDI, developed by Bech et al46 for the World Health Organization (WHO) in 2001, was used in this study. It has the advantage of covering the DSM-IV symptoms of major depression and the International Statistical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10) category of mild, moderate, and severe depression which involves both duration and intensity criteria. The Arabic version (MDI-A), prepared and tested for its reliability and concurrent and discriminant validity by Fawzi et al,47 was used. Originally, MDI used the past 2 weeks as the time frame; however, we focused on questions to exclude the time of the hip fracture to avoid biases in the results by the psychological state resulting from the subsequent pain and immobilization. The MDI-A involved 12 items, however, functionally it is composed of only 10 items because items 8 and 10 are composed of 2 sub-items each (a and b) with the highest score of either a or b is only countable. Answers are recorded on a 6-point Likert-type scale, ranging from 0 (at no time) to 5 (all the time) with a possible range of 0–50. The standardization of the score considered 0–20 to be no or doubtful depression, 21–25 as mild depression, 26–30 as moderate depression, and 31–50 as severe depression.48
Measurement of Serum Cobalt and Chromium Levels
Cobalt and chromium levels were measured according to the method described by Savarino et al49 and Jiang et al.50 Venous blood samples were collected from the antecubital vein of fasting patients in the morning. Trying to avoid metal contamination during the blood sample collection and analysis was done by discarding the first 5 mL of the collected blood to avoid contamination from the needle, and collecting the samples in metal-free vacutainer tubes. In addition, the instruments used during the analysis were soaked in 2% nitric acid (HNO3) in twice-distilled and deionized water, followed by meticulous washing in twice-distilled and deionized water. The blood samples were centrifuged at 800 ×g, 4oC for 10 min, and the separated serum samples were frozen at –70oC till analysis. Consequently, 0.5 mL of nitric acid (HNO3) was added to 0.5 mL of serum, and the resultant mixture was incubated for 24 h; then 4 mL of deionized distilled water was added to the mixture and the amount was estimated. After centrifuging at 8000×g for 3 min, the supernatant was separated and used for the estimation of cobalt and chromium using Buck scientific 210VGP Atomic Absorption Spectrophotometer and the results were expressed as ng/mL.
Assessment of Genotoxicity in Peripheral Blood Samples of Included Patients
Single-Cell Gel Electrophoresis (Comet) Assay
The processes of blood sample collection and storage for the comet assay were performed according to the method described by Al-Salmani et al;51 it has the advantages of being more simplified, suitable for direct use in the alkaline comet assay, the whole blood can be used without the need for pre-analysis separation of peripheral blood mononuclear cells (PBMC) which is highly time-consuming. In addition, this method does not need any cryo-preservative and allows storage of samples for up to 1 month without artifactual DNA damage. Blood samples collected by lancet (~250 μL) were obtained from the side of a finger and transferred, by pipette, into tubes containing sterile Ethylenediamine tetraacetic acid (EDTA) solution (0.4 mg EDTA/250 μL of blood). Samples were then frozen at −80°C for later analysis. Before the assay, the stored samples were allowed to thaw for up to 30 min at 4°C.
As described by Møller et al,52 the alkaline comet assay passes into several steps including preparing a single cell suspension, embedding the cells in agarose, lysis of the cell, alkaline treatment, electrophoresis, neutralization, and DNA staining for the process of visualization and scoring and data analysis.
Each 5 μL of whole blood was suspended in 200 μL of pre-warmed 0.6% low-melting-point (LMP) agarose. 80 μL from the previous suspension was pipetted and distributed directly to each half of the microscope slide which was pre-coated with 1% normal-melting-point (NMP) agarose, and the two gels per slide were allowed to harden under a coverslip, on ice. Eight slides were prepared for each sample and all the slides were given a similar code or number allowing for blind examination and scoring.53
The lysis step was performed by gently removing the coverslips and immersing the slides in pre-chilled lysis buffer at 4°C overnight with protecting the slides from light. The lysis buffer was prepared by adding a 100 mM solution of disodium ethylenediamine tetraacetic acid (Na2EDTA), 2.5 M sodium chloride, and 10 mM tris hydroxymethyl aminomethane in purified water, the pH is adjusted to 10 with 10 N sodium hydroxide solution. Triton X100 and dimethyl sulfoxide were then added to the solution to achieve final concentrations of 1% and 10%, respectively, and then kept at 4–10°C for at least 30 min before use. After removing the slides from the lysis buffer, drain the slides and rinse once with cold neutralization buffer (0.4 M Tris Base in purified water adjusted to pH 7.5 with hydrochloric acid) for 5 min to remove residual detergent and salts.54
The steps of alkali unwinding, electrophoresis, neutralization, and DNA staining were also performed according to Ding et al.54 The slides were located in a fresh electrophoresis buffer (300 mM sodium hydroxide (NaOH), 1 mM Na2EDTA, pH 13.0) inside a horizontal gel electrophoresis chamber for 20 min at 4°C to allow DNA unwinding and expression of alkali-labile sites. Denaturation and electrophoresis were performed under dim light at 4°C. Electrophoresis was carried out for 30 min at 300 mA. After electrophoresis, the slides were washed three times gently using a neutralization buffer (0.4 M Tris-HCl, pH 7.5) to remove excess alkali and detergents. Then, slides were stained with ethidium bromide.
The slide examination was performed using a fluorescence microscope equipped with an appropriate filter and images were captured by a Nikon CCD camera at a 40x objective. The qualitative and quantitative extent of DNA damage in the cells was estimated using the Komet 5 image analysis software developed by Kinetic Imaging Ltd. (Liverpool, UK). Based on the recommendation of Kumaravel et al,55 we used the length of DNA migration [tail length] and the percentage of migrated DNA in the tail [tail DNA %], and the tail moment [correlation between tail length and tail DNA %] as the most reliable comet measurements that would truly reflect the extent of DNA damage. Generally, images of 100 (50 × 2) randomly selected cells are analyzed per sample. The mean value (for 100 cells) was calculated.
Measurement of Serum Level of 8-Hydroxy-2’–Deoxyguanosine (8-OHdG)
Two milliliters of blood were obtained by venipuncture and transferred to serum separation tubes. The samples were allowed to clot for two hours at room temperature and then centrifuged at 1000 rpm for 15 minutes. The serum was separated and stored at −80°C for later estimation of 8-OHdG. The enzyme-linked immunosorbent assay (ELISA) kit from MyBioSource (Catalog Number: MBS704914) was used following the manufacturer’s instructions. The assay utilizes the competitive inhibition enzyme immunoassay method where a competitive inhibition reaction is initiated between the pre-coated 8-OHdG and 8-OHdG in samples and a substrate solution is added to the wells and the color develops opposite to the amount of 8-OHdG in the sample. The color development is stopped and the intensity of the color is measured within 5 minutes, using a microplate reader set to a wavelength of 450 nm.
Patient Follow-Up
At 6 and 12 months postoperative, all patients were assessed for pain and function according to the method described by Konan et al56 to exclude pain and dysfunction as confounders to the occurrence of depression and affection of MDI score. All patients were found to have a well-functioning prosthesis and reported no pain. They were asked to report data about all prescription and non-prescription medications and any post-operative exposure to the substances listed in the exclusion criteria. None of the patients was found to be exposed. MMSE and MDI were assessed in addition to estimating the cobalt and chromium levels, comet assay parameters, and 8-OHdG levels.
Statistical Analysis
Sample Size Calculation
Based on previous a previous study,57 the difference of Cobalt levels/Cr levels between immediately measured postoperatively and 6 and 12 months postoperative showed a relatively large effect size. A sample size of 25 data pairs achieves 80% power to reject the null hypothesis of zero effect size when the population effect size is 0.70 and the significance level (alpha) is 0.017 using a two-sided paired t-test. The level of alpha was calculated according to the Bonferroni correction allowing for three pairwise comparisons. The final sample size will be 34 adding 25% to compensate for dropouts.
Data Curation
Data were collected, tabulated, and managed using Statistical Package for Social Science version 24 (SPSS Inc., Chicago, IL). Quantitative variables were presented as a mean± standard deviation; Repeated measure one-way ANOVA was used to examine the difference in the measured parameters across the three points of time and post-hoc pairwise comparison was done using Bonferroni correction. Pearson correlation coefficient was used to examine the linear relationship between selected variables. Qualitative variables were presented as count and proportions and the Marginal homogeneity test was used to test the changes in proportions across time points. A p-value equal to or less than 0.05 was considered statistically significant.
Results
We approached 37 eligible patients for participation in the study. Three patients declined to participate. The remaining 34 patients were included. Five patients (14.7%) failed to show up for their first postoperative evaluation at 6 months, and 2 patients failed to show up for their final evaluation at 12 months (dropout rate of 5.8% for the final visit). The flow chart of the study is shown in Figure 1.
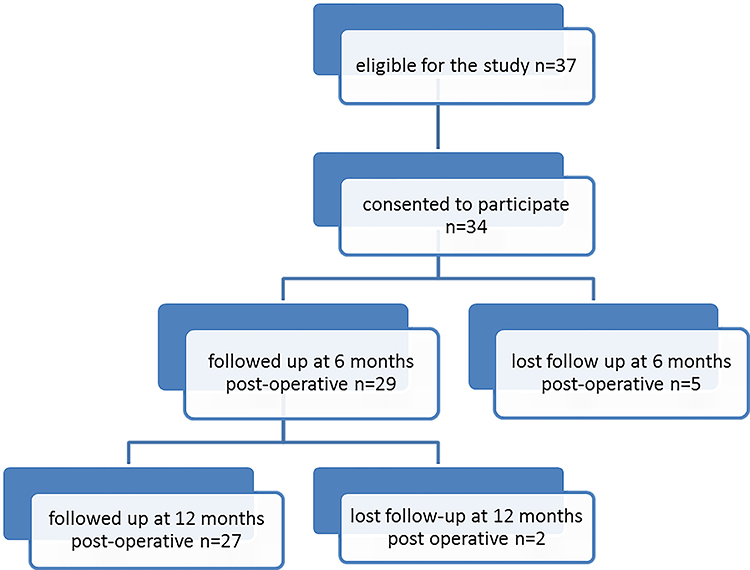 |
Figure 1 A flow chart of the participants throughout the whole study duration. |
The demographic data of the approached cases who completed the follow-up visits (number = 27) are presented in Table 1.
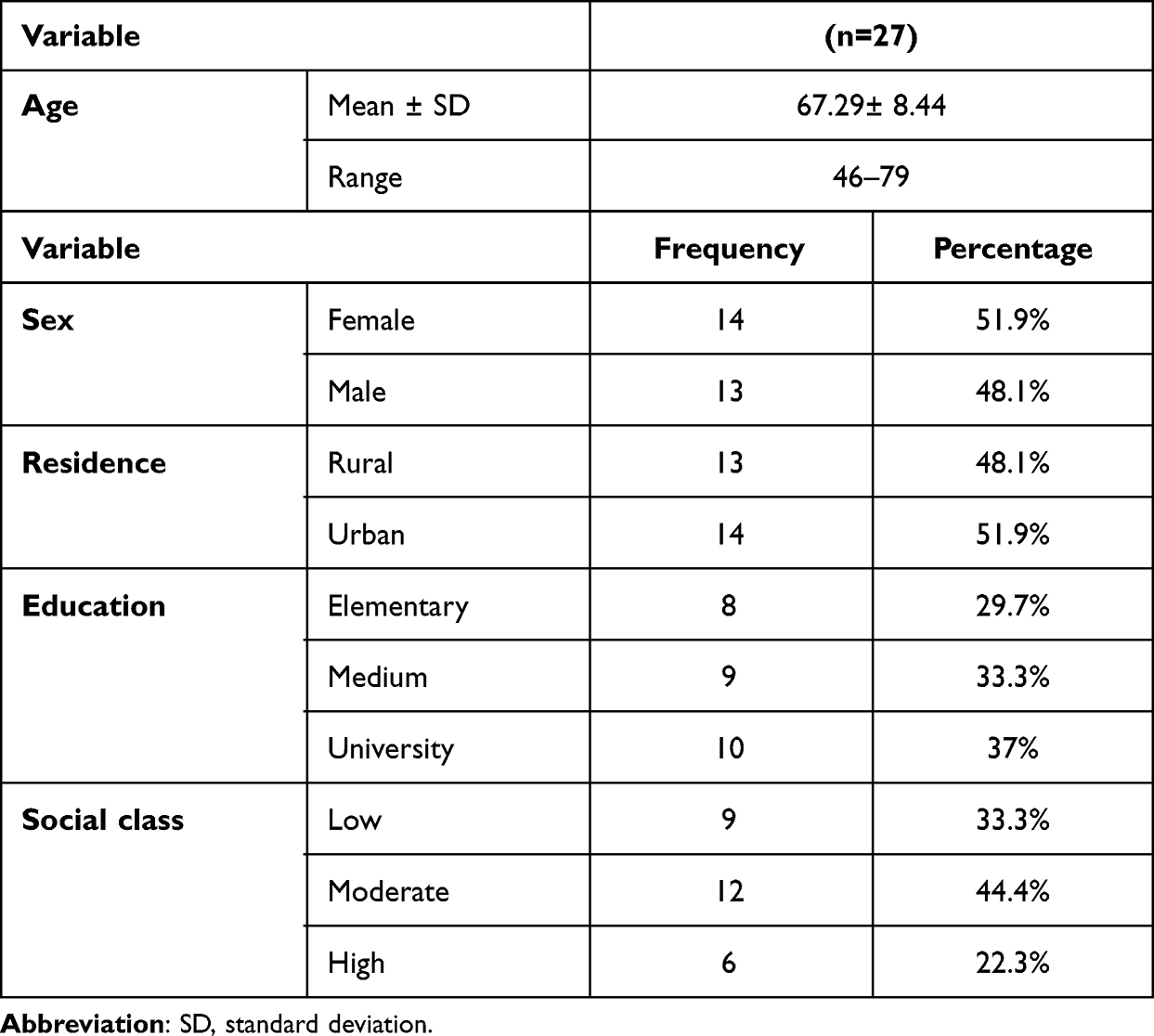 |
Table 1 Demographic Data of Cases of Metal on Polyethylene Hip Implant Surgery Who Completed the Follow-Up |
The mean values and standard deviation of MMSE score preoperatively, 6-months postoperative, and 12-months postoperative are 28.22±1.34, 26.48±4.49, and 26.48±5.03, respectively, with a non-significant difference between the three measures (p = 0.087). Cognitive impairment was reported in 18.5% of patients at 6-months postoperative. However, this percentage decreased to 14.8% at the second postoperative visit. Although the Marginal Homogeneity tests proved no statistical significance between each pair of comparisons, the degree of the deficit is higher in the postoperative follow-up visits (Table 2).
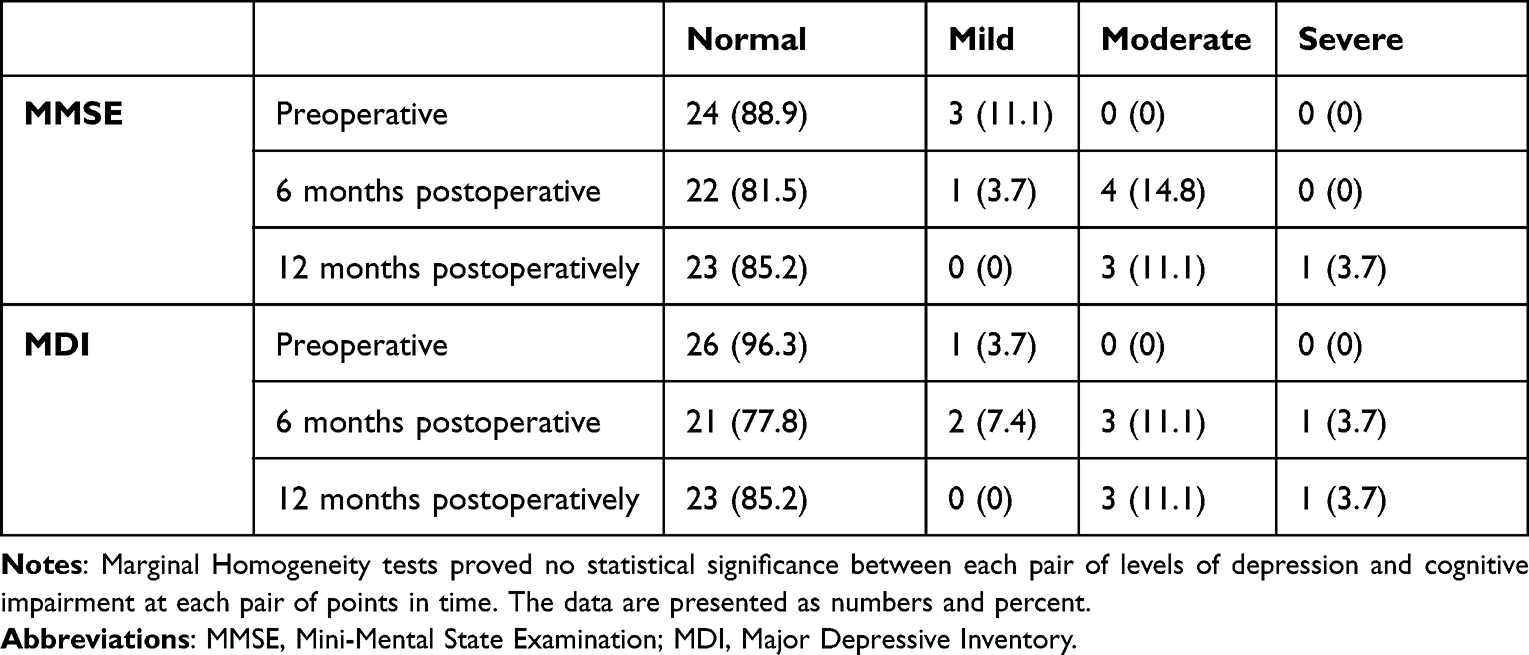 |
Table 2 Comparison of Preoperative, 6 Months, and 12 Months Postoperative MMSE and MDI Categories in the Sample of 27 Co/Cr Metallic Hip Replacement Operations |
In addition, the mean values and standard deviation of MDI score preoperatively, 6-months postoperative, and 12-months postoperative are 16.85± 2.93, 18.67± 5.73, and 18.11±6.08, respectively, with also a non-significant difference between the three measures (p = 0.208). At 6-months postoperative, the presence of depressive disorders in 22.2% of patients included in the study is recorded and distributed as 7.4% mild, 11.1 moderate, and 3.7% severe. The percentage of patients with depressive disorders decreased to 14.8% at 12-months postoperative with no statistically significant difference between each pair of comparisons by Marginal Homogeneity tests (Table 2).
The repeated measure one-way ANOVA test shows a significant difference in the cobalt and chromium levels between the preoperative, 6-months postoperative, and 12-months postoperative measures (p < 0.001). The scatter plot diagram presented in Figures 2 and 3 shows a significant increase in the cobalt and chromium levels 6 months postoperative when compared to preoperative levels (p < 0.001), while at 12 months postoperative the levels were significantly higher from the preoperative level (p < 0.001) and significantly lower than 6 months postoperative levels (p < 0.001). Age and sex proved insignificant when added to the repeated measure ANOVA as between-group variable (Sex) or covariate (Age).
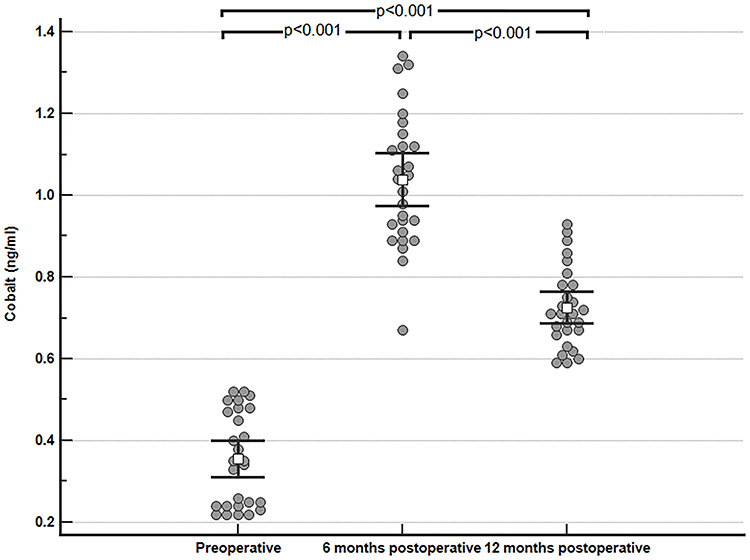 |
Figure 2 A scatter plot diagram comparing the preoperative, 6-months postoperative, and 12-months postoperative values of serum cobalt after MOP hip implant surgery. |
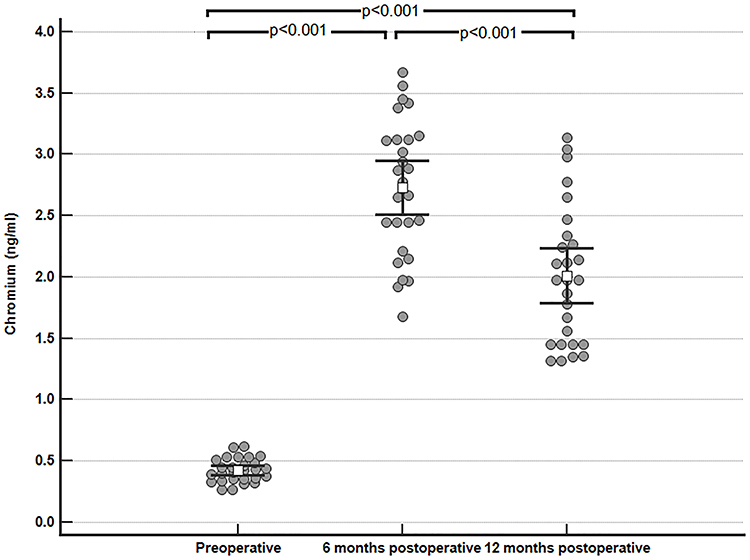 |
Figure 3 A scatter plot diagram comparing the preoperative, 6-months postoperative, and 12-months postoperative values of serum chromium after MOP hip implant surgery. |
The preoperative, 6-months postoperative, and 12-months postoperative mean values and standard deviation of the comet assay parameter percent of DNA in the tail (tail DNA %) are 0.84±0.15, 0.91±0.16, and 0.93±0.16, respectively, with a non-significant difference (p = 0.204). The values of tail length at the three points of measurement are 0.95±0.09, 0.98±0.17, and 0.99±0.17, respectively, with also non-significant differences (p = 0.416). Moreover, the values of the tail moment at the three points of measurement are 0.78±0.15, 0.83±0.15, and 0.88±0.19 with a non-significant difference (p = 0.151).
There is a significant difference between preoperative, 6-months postoperative, and 12-months postoperative 8-OHdG serum levels. The scatter plot chart (Figure 4) shows elevation in 8-OHdG levels 6 months postoperative compared to preoperative values (p < 0.001), while the 12 months postoperative level is significantly lower than 6 months postoperative (p < 0.001) but still significantly higher than preoperative values (p < 0.001).
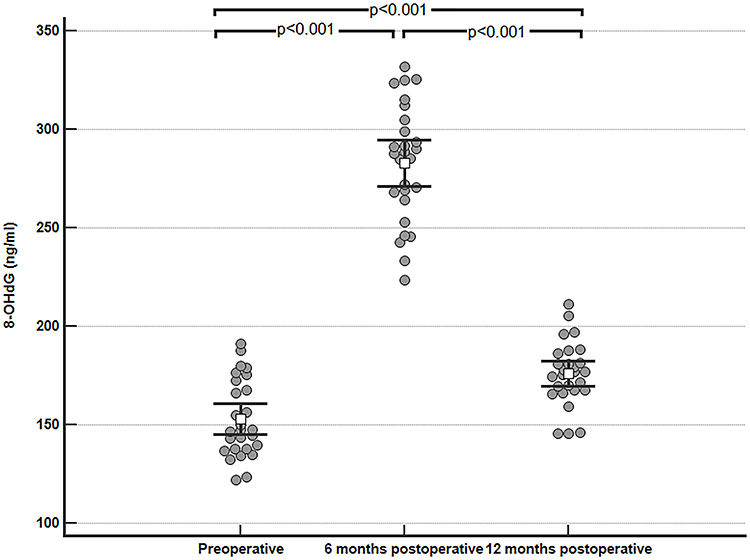 |
Figure 4 A scatter plot diagram comparing the preoperative, 6-months postoperative, and 12-months postoperative values of serum 8-OHdG after MOP Hip implant surgery. |
As shown in Figure 5, there is a strong positive correlation between the values of serum 8-OHdG and the serum cobalt level both at 6-months postoperative (r = 0.888, p < 0.001) and also at 12 months postoperative (r = 0.875, p < 0.001).
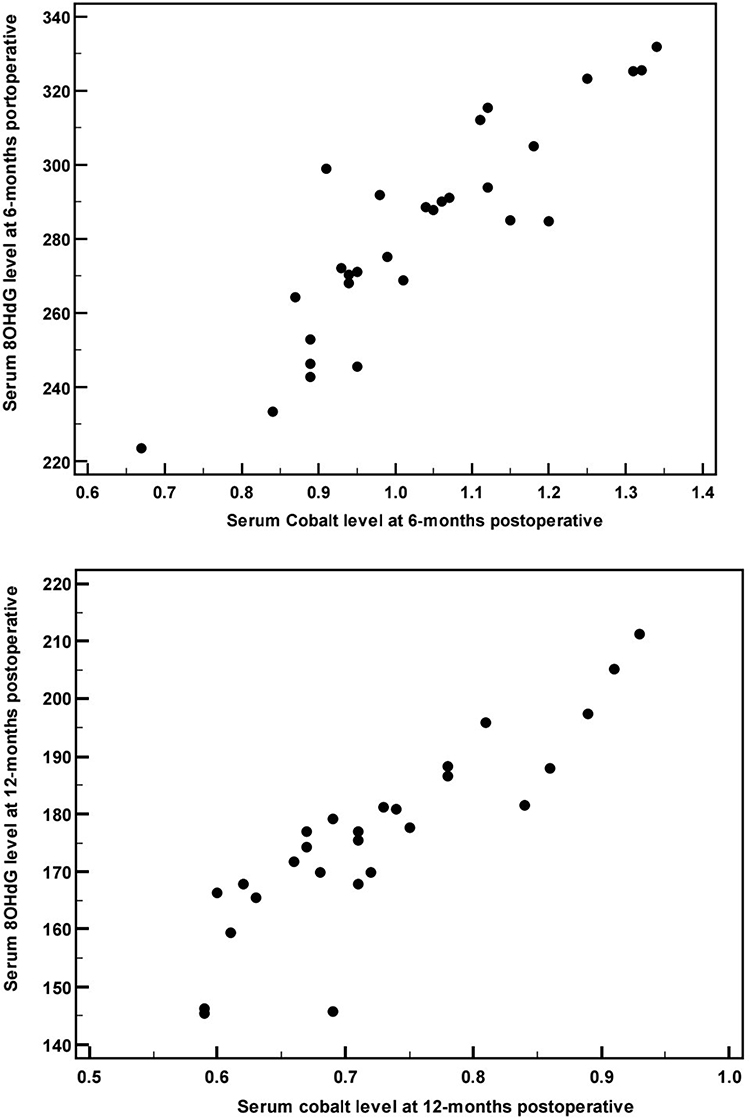 |
Figure 5 Pearson’s correlation between serum cobalt level (horizontal axis) and serum 8-OHdG level (vertical axis) at 6-months postoperative and at 12-months postoperative. |
Discussion
Total hip arthroplasty is one of the commonest and growing surgical procedures performed all over the world. Little is known about the effects of MOP hip arthroplasty on the psychological state of the patients and whether any resultant psychological disorder is related to the Co/Cr levels in patient blood or any genotoxic potential. The current work shows a significant increase in the cobalt and chromium level 6 months postoperative when compared to preoperative levels, while at 12 months postoperative the levels were significantly higher than the control and significantly lower than 6 months postoperative levels. Although in the wear simulator studies MoP bearings have up to 100 times more wear than MOM,58 there is a controversy in the clinical studies reporting serum, urine, and erythrocyte cobalt and chromium levels after MoP THA. Savarino et al59 reported a significant increase in Co and Cr levels up to 18–36 months postoperative compared to preoperative. MacDonald et al60 also reported a 1.5-fold increase in blood cobalt and a 2.2-fold increase in blood chromium from pre-postoperative values. On the contrary, Briggs et al33 showed a non-significant difference between pre- and postoperative cobalt and chromium levels in MOP patients at 1, 2, and 5 years post-operative. Heisel et al36 reported that serum chromium and cobalt levels of the patients with total hip resurfacing arthroplasty continuously increased during the first six months with an insignificant decrease thereafter. However, Back et al61 and Yang et al62 reported an initial increase in ion levels to a peak level at 6 months, followed by a gradual decline. This can be explained by the more rapid wear initial conditioning phase or running-in which is followed by a lower steady-state wear rate.63 The Co levels detected in the blood of the included patients in the current work are even higher than the normal blood levels in occupationally exposed persons considered by the Department of Occupational and Environmental Medicine at O¨rebro University Hospital, Sweden.64 The cobalt and chromium ions are released as a result of two mechanisms: friction between the articulating surfaces producing many nano-sized wear particles and metal surface corrosion.65 Many factors may negatively impact this wear process and increase the metal ion release or lead to higher metal ion levels as suboptimal surgical positioning of the implant,66 impaired renal function and bilateral hip replacement,67 and mixing components from different manufacturers or different types.68 The current work showed that age does not correlate to the blood ions levels in accordance with Pozzuoli et al.15 In addition, the ion levels showed a non-significant difference between males and females in contrast to Delaunay et al69 who reported that female sex seems to be significantly associated with higher circulating metal ions secondary to variations in the metabolism of metal ions. The variability between this study and the current work can be related to the difference in the type of implant.
There was a non-significant difference in the preoperative, 6-months postoperative, and 12-months postoperative MDI scores and a non-significant difference between each pair of comparison by marginal homogeneity test. However, depressive disorders were reported in 22.2% of patients included in the study at 6-months postoperative, while the percentage of patients with depressive disorders decreased to 14.8% at 12-months postoperative. Running in parallel, Lassalle et al70 reported that MOP arthroplasty has more psychiatric comorbidities (14.8%) when compared to other implant types. Although Nguyen et al71 and Cristancho et al72 correlate the depressive symptoms and mental health of the patient to the pain and implant function, the current work raises the concern for the occurrence of depressive symptoms in patients reporting no pain and having a well-functioning prosthesis. In addition, there was a non-significant difference in the preoperative, 6-months postoperative, and 12-months postoperative MMSE score and a non-significant difference between each pair of comparison by marginal homogeneity test. The current work showed the development of cognitive impairment in 18.5% of patients at 6-months postoperative. However, this percentage decreased to 14.8% at the second postoperative visit. Repeated measure analysis removed any confounding effect as education, social class, and residence as the individual was assumed as a control for himself. However, the small sample size made the use of complex models, eg, to test the effect of social status on the relationship between time and the dependent variables, unreliable. Krenk et al73 reported cognitive dysfunction in 18.9% of patients undergoing fast-track hip and knee replacement at one week postoperative and in 10.8% at 3-months postoperative. Previous studies investigating neurological findings due to Co released from prostheses included case series focused on the clinical findings of memory loss, diminished executive function, tremors, hearing and vision loss, depression, and emotional instability.74–77 Effects on the nervous system particularly memory loss, neuropathies, and a decreased visual acuity have also been reported following occupational Co exposure.78,79 Previously, studies documented that cobalt can pass the blood-brain barrier and become deposited in the brain,80 causing brain cell apoptosis mediated by the α subunit of the hypoxia-inducible factor-1 pathway.81,82 Bridges et al83 investigated 123 patients with symptomatic arthroprosthetic elevated cobalt levels using F-18 FDG PET brain imaging and they detected brain regions of hypometabolism including temporal, frontal, Broca’s areas, anterior cingulate, parietal, posterior cingulate, visual, sensorimotor, thalamic, and caudate area in descending order.
The current work proved a significant elevation in 8-OHdG levels 6 months postoperative, while the 12 months postoperative level was significantly lower than 6 months postoperative but still significantly higher than preoperative values. 8-Hydroxydeoxyguanosine (8-OHdG) is an oxidized form of deoxyguanosine nucleoside; it is one of the major ROS-induced oxidative lesions in the DNA structure and is considered a critical biomarker of oxidative nuclear and mitochondrial DNA damage.84 The levels were positively correlated to the cobalt level both at 6 and 12 months postoperative. In vitro studies have suggested that there are two chief mechanisms implicated in the genotoxic potential of Co including the generation of reactive oxygen species (ROS) and the inhibition of DNA repair mechanisms.85 Base excision repair (BER) is the primary pathway involved in DNA repair. The 8-oxoguanine DNA glycosylase (OGG1) is the DNA repair enzyme involved in the BER. OGG1 recognizes and excises ROS-induced DNA lesions such as 8-hydroxy-2-deoxyguanosine (8-OHdG). Pilger et al86 measured 8-OHdG in the urine of patients with THA and reported no significant correlation to the concentrations of metals. However, according to Wang et al,87 the plasma 8-OHdG is more sensitive than urinary 8-OHdG to detect increased oxidative damages induced by risk factors.
Although there was biochemical evidence of oxidative DNA injury, there were no evident structural changes in the DNA of peripheral blood cells. There was no significant difference between mean values of comet assay parameters (tail length, tail DNA% and tail moment mean) preoperative, 6 months postoperative, and 12 months postoperative. This can be explained by either that the part of DNA being oxidized is below the limit needed to induce an evident structural change or that the DNA repair system is not completely inhibited by the elevated ions and is still capable for repairing the oxidative DNA damage. Revising the literature for the genotoxic effects following hip arthroplasty revealed a controversy; Christian et al88 reported that DNA effects would be highly unlikely to occur as a result of wear debris from a CoCr implant. On the other hand, Briggs et al33 reported a significant increase in the chromosomal aberration indices following both MOM and MOP hip arthroplasty. The United Kingdom Government’s Committee on Mutagenicity of Chemicals in Food, Consumer Products, and the Environment stated that some MOP implants can induce genetic damage.89 The variability in the genotoxic potential can be related to many factors such as the type of the implant, duration of the implantation, levels of the metal ions released, whether the implant is well functioning or failed and needs revision surgery or interaction between these factors. Although this work added to the current knowledge regarding the understanding of the psychological disorders and genotoxicity after MOP hip arthroplasty and their correlation to cobalt and chromium levels, there were some limitations including the small number of patients and the relatively short follow-up period.
Conclusion
The current work was addressing the psychiatric disorders and genotoxicity after primary MOP hip arthroplasty and evaluated their possible correlation to cobalt and chromium levels. The study revealed that even well-functioning MOP hip implants can induce increased ion levels and positively correlated increase in biochemical markers of genotoxicity (8-OHdG) indicating the need for regular patient follow-up; however, the change in the scores of cognitive impairment and depression was not significant and they were not correlated to the ion levels.
Abbreviations
BER, base excision repair; Co/Cr, cobalt/chromium; comet assay, single-cell-gel-electrophoresis; DSM-IV-TR, Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision; ELISA, The enzyme-linked immunosorbent assay; HA, Hip arthroplasty; ICD-10, International Statistical Classification of Diseases and Related Health Problems, 10th Revision; LMP, low-melting-point; MDI, major-depressive-inventory; 8-OHdG, 8-hydroxy-2’–deoxyguanosine; MMSE, mini-mental-state-examination; MOM, metal-on-metal; MOP, metal on polyethylene; Na2EDTA, disodium ethylenediamine tetraacetic acid; NaOH, sodium hydroxide; NMP, normal-melting-point; OGG1, 8-oxoguanine DNA glycosylase; PBMC, peripheral blood mononuclear cells; ROS, reactive oxygen species; SES, socioeconomic status; THA, total hip arthroplasty; WHO, World Health Organization.
Funding
This work was funded by the National Institutes of Health, Fogarty International Center, Bethesda, MD (grant number, 2D43TW007296).
Disclosure
The authors declare that there is no conflict of interest in this work.
References
1. Mealy A, Sorensen J. Effects of an aging population on hospital costs related to elective Hip replacements. Public Health. 2020;180:10–16. doi:10.1016/j.puhe.2019.10.013
2. Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision Hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89(4):780–785. doi:10.2106/JBJS.F.00222
3. Taha A, ElZaher EH, ElGanzoury I, et al. Osteosynthesis and outcomes of traumatic periprosthetic femoral fractures after total Hip arthroplasty. Arthroplasty. 2021;31. doi:10.1186/s42836-021-00089-1
4. Dunstan E, Ladon D, Whittingham-Jones P, Carrington R, Briggs TW. Chromosomal aberrations in the peripheral blood of patients with metal-on-metal Hip bearings. J Bone Joint Surg Am. 2008;90(3):517–522. doi:10.2106/JBJS.F.01435
5. Szczesiul J, Bielecki M, Korovessis P. A review of total hip arthroplasty comparison in FNF and OA patients. Adv Orthop. 2021;2021:5563500. doi:10.1155/2021/5563500
6. Donahue SW. Krogh’s principle for musculoskeletal physiology and pathology. J Musculoskelet Neuronal Interact. 2018;18(3):284–291.
7. Krishnan Y, Grodzinsky AJ. Cartilage diseases. Matrix Biol. 2018;71-72:51–69. doi:10.1016/j.matbio.2018.05.005
8. Lee YK, Lee YJ, Ha YC, Koo KH. Five-year relative survival of patients with osteoporotic Hip fracture. J Clin Endocrinol Metab. 2014;99(1):97–100. doi:10.1210/jc.2013-2352
9. Ha YC, Kim TY, Lee A, et al. Current trends and future projections of Hip fracture in South Korea using nationwide claims data. Osteoporos Int. 2016;27(8):2603–2609. doi:10.1007/s00198-016-3576-9
10. Lee YK, Kim JW, Lee MH, Moon KH, Koo KH. Trend in the age-adjusted incidence of hip fractures in South Korea: systematic review. Clin Orthop Surg. 2017;9(4):420–423. doi:10.4055/cios.2017.9.4.420
11. Devlin JJ, Pomerleau AC, Brent J, Morgan BW, Deitchman S, Schwartz M. Clinical features, testing, and management of patients with suspected prosthetic hip-associated cobalt toxicity: a systematic review of cases. J Med Toxicol. 2013;9(4):405–415. doi:10.1007/s13181-013-0320-0
12. The National joint registry 18th annual report; 2021 Available from: https://www.ncbi.nlm.nih.gov/books/NBK576849/#ch3.s17.
13. Steinemann SG. Metal implants and surface reactions. Injury. 1996;27(Suppl 3):SC16–SC22. doi:10.1016/0020-1383(96)89027-9
14. Hallab N. Metal sensitivity in patients with orthopedic implants. J Clin Rheumatol. 2001;7(4):215–218. doi:10.1097/00124743-200108000-00004
15. Pozzuoli A, Berizzi A, Crimì A, et al. Metal ion release, clinical and radiological outcomes in large diameter metal-on-metal total hip arthroplasty at long-term follow-up. Diagnostics. 2020;10(11):941. doi:10.3390/diagnostics10110941
16. Kovochich M, Finley BL, Novick R, et al. Understanding outcomes and toxicological aspects of second generation metal-on-metal hip implants: a state-of-the-art review. Crit Rev Toxicol. 2018;48(10):853–901. doi:10.1080/10408444.2018.1563048
17. Lainiala OS, Moilanen TPS, Hart AJ, Huhtala HSA, Sabah SA, Eskelinen AP. Higher blood cobalt and chromium levels in patients with unilateral metal-on-metal total hip arthroplasties compared to hip resurfacings. J Arthroplasty. 2016;31(6):1261–1266. doi:10.1016/j.arth.2015.11.045
18. de Villiers D, Traynor A, Collins SN, Shelton JC. The increase in cobalt release in metal-on-polyethylene hip bearings in tests with third body abrasives. Proc Inst Mech Eng H. 2015;229(9):611–618. doi:10.1177/0954411915595433
19. Bijukumar DR, Segu A, Souza JCM, et al. Systemic and local toxicity of metal debris released from hip prostheses: a review of experimental approaches. Nanomedicine. 2018;14(3):951–963. doi:10.1016/j.nano.2018.01.001
20. Stambough JB, Pashos G, Bohnenkamp FC, Maloney WJ, Martell JM, Clohisy JC. Long-term results of total hip arthroplasty with 28-millimeter cobalt-chromium femoral heads on highly cross-linked polyethylene in patients 50 years and less. J Arthroplasty. 2016;31(1):162–167. doi:10.1016/j.arth.2015.07.025
21. Scully WF, Teeny SM. Pseudotumor associated with metal-on-polyethylene total hip arthroplasty. Orthopedics. 2013;36(5):e666–e670. doi:10.3928/01477447-20130426-33
22. Cooper HJ, Della Valle CJ, Berger RA, et al. Corrosion at the head-neck taper as a cause for adverse local tissue reactions after total hip arthroplasty. J Bone Joint Surg Am. 2012;94(18):1655–1661. doi:10.2106/jbjs.k.01352
23. Scharf B, Clement CC, Zolla V, et al. Molecular analysis of chromium and cobalt-related toxicity. Sci Rep. 2014;4:5729. doi:10.1038/srep05729
24. Eltit F, Assiri A, Garbuz D, et al. Adverse reactions to metal on polyethylene implants: highly destructive lesions related to elevated concentration of cobalt and chromium in synovial fluid. J Biomed Mater Res A. 2017;105(7):1876–1886. doi:10.1002/jbm.a.36057
25. Harris A, Johnson J, Mansuripur PK, Limbird R. Cobalt toxicity after revision to a metal-on-polyethylene total Hip arthroplasty for fracture of ceramic acetabular component. Arthroplast Today. 2015;1(4):89–91. doi:10.1016/j.artd.2015.09.002
26. Levine BR, Hsu AR, Skipor AK, et al. Ten-year outcome of serum metal ion levels after primary total hip arthroplasty: a concise follow-up of a previous report. J Bone Joint Surg Am. 2013;95(6):512–518. doi:10.2106/JBJS.L.00471
27. Green B, Griffiths E, Almond S. Neuropsychiatric symptoms following metal-on-metal implant failure with cobalt and chromium toxicity. BMC Psychiatry. 2017;17(1):33. doi:10.1186/s12888-016-1174-1
28. Clark MJ, Prentice JR, Hoggard N, Paley MN, Hadjivassiliou M, Wilkinson JM. Brain structure and function in patients after metal-on-metal hip resurfacing. AJNR Am J Neuroradiol. 2014;35(9):1753–1758. doi:10.3174/ajnr.A3922
29. Raza MU, Tufan T, Wang Y, Hill C, Zhu MY. DNA damage in major psychiatric diseases. Neurotox Res. 2016;30(2):251–267. doi:10.1007/s12640-016-9621-9
30. Sansone V, Pagani D, Melato M. The effects on bone cells of metal ions released from orthopaedic implants. A review. Clin Cases Miner Bone Metab. 2013;10(1):34–40. doi:10.11138/ccmbm/2013.10.1.034
31. Doherty AT, Howell RT, Ellis LA, et al. Increased chromosome translocations and aneuploidy in peripheral blood lymphocytes of patients having revision arthroplasty of the Hip. J Bone Joint Surg Br. 2001;83(7):1075–1081. doi:10.1302/0301-620x.83b7.10102
32. Ladon D, Doherty A, Newson R, Turner J, Bhamra M, Case CP. Changes in metal levels and chromosome aberrations in the peripheral blood of patients after metal-on-metal hip arthroplasty. J Arthroplasty. 2004;19(8 Suppl 3):78–83. doi:10.1016/j.arth.2004.09.010
33. Briggs TW, Hanna SA, Kayani B, et al. Metal-on-polyethylene versus metal-on-metal bearing surfaces in total hip arthroplasty: a prospective randomised study investigating metal ion levels and chromosomal aberrations in peripheral lymphocytes. Bone Joint J. 2015;97-B(9):1183–1191. doi:10.1302/0301-620X.97B9.34824
34. Keegan GM, Learmonth ID, Case CP. A systematic comparison of the actual, potential, and theoretical health effects of cobalt and chromium exposures from industry and surgical implants. Crit Rev Toxicol. 2008;38(8):645–674. doi:10.1080/10408440701845534
35. Vendittoli PA, Mottard S, Roy AG, Dupont C, Lavigne M. Chromium and cobalt ion release following the Durom high carbon content, forged metal-on-metal surface replacement of the Hip. J Bone Joint Surg Br. 2007;89(4):441–448. doi:10.1302/0301-620X.89B4.18054
36. Heisel C, Streich N, Krachler M, Jakubowitz E, Kretzer JP. Characterization of the running-in period in total hip resurfacing arthroplasty: an in vivo and in vitro metal ion analysis. J Bone Joint Surg Am. 2008;90(Suppl 3):125–133. doi:10.2106/JBJS.H.00437
37. Daniel J, Ziaee H, Pradhan C, McMinn DJ. Six-year results of a prospective study of metal ion levels in young patients with metal-on-metal hip resurfacings. J Bone Joint Surg Br. 2009;91(2):176–179. doi:10.1302/0301-620X.91B2.21654
38. Hartmann A, Hannemann F, Lützner J, et al. Metal ion concentrations in body fluids after implantation of Hip replacements with metal-on-metal bearing–systematic review of clinical and epidemiological studies. PLoS One. 2013;8(8):e70359. doi:10.1371/journal.pone.0070359
39. Garcia MD, Hur M, Chen JJ, Bhatti MT. Cobalt toxic optic neuropathy and retinopathy: case report and review of the literature. Am J Ophthalmol Case Rep. 2020;17:100606. doi:10.1016/j.ajoc.2020.100606
40. Bradberry SM, Wilkinson JM, Ferner RE. Systemic toxicity related to metal hip prostheses. Clin Toxicol. 2014;52(8):837–847. doi:10.3109/15563650.2014.944977
41. Fahmy SI, Nofal LM, Shehata SF, El Kady HM, Ibrahim HK. Updating indicators for scaling the socioeconomic level of families for health research. J Egypt Public Health Assoc. 2015;90(1):1–7. doi:10.1097/01.EPX.0000461924.05829.93
42. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. doi:10.1016/0022-3956(75)90026-6
43. Albanna M, Yehya A, Khairi A, et al. Validation and cultural adaptation of the Arabic versions of the mini-mental status examination - 2 and mini-Cog test. Neuropsychiatr Dis Treat. 2017;13:793–801. doi:10.2147/NDT.S126825
44. Folstein MF, Folstein SE. Mini Mental State Examination (MMSE): User Manual.
45. Folstein MF, Folstein SE, Fanjiang G. MMSE Mini-Mental State Examination: Clinical Guide. Lutz, FL: Psychological Assessment Resources; 2001.
46. Bech P, Rasmussen NA, Olsen LR, Noerholm V, Abildgaard W. The sensitivity and specificity of the major depression inventory, using the present state examination as the index of diagnostic validity. J Affect Disord. 2001;66(2–3):159–164. doi:10.1016/s0165-0327(00)00309-8
47. Fawzi MH, Fawzi MM, Abu-Hindi W. Arabic version of the major depression inventory as a diagnostic tool: reliability and concurrent and discriminant validity. East Mediterr Health J. 2012;18(4):304–310. doi:10.26719/2012.18.4.304
48. Bech P, Timmerby N, Martiny K, Lunde M, Soendergaard S. Psychometric evaluation of the Major Depression Inventory (MDI) as depression severity scale using the LEAD (Longitudinal Expert Assessment of All Data) as index of validity. BMC Psychiatry. 2015;15(1):190. doi:10.1186/s12888-015-0529-3
49. Savarino L, Cadossi M, Chiarello E, et al. How do metal ion levels change over time in hip resurfacing patients? A cohort study. Sci World J. 2014;2014:291925. doi:10.1155/2014/291925
50. Jiang W, Wan Y, Cui P, Ning X. Intermediate-term trends in serum levels of metal ions after Hip resurfacing arthroplasty. J Orthop Surg Res. 2015;10(1):188. doi:10.1186/s13018-015-0335-0
51. Al-Salmani K, Abbas HHK, Schulpen S, et al. Simplified method for the collection, storage, and comet assay analysis of DNA damage in whole blood. Free Radic Biol Med. 2011;51(3):719–725. doi:10.1016/j.freeradbiomed.2011.05.020
52. Møller P, Azqueta A, Boutet-Robinet E, et al. Minimum Information for Reporting on the Comet Assay (MIRCA): recommendations for describing comet assay procedures and results. Nat Protoc. 2020;15(12):3817–3826. doi:10.1038/s41596-020-0398-1
53. Karbaschi M, Ji Y, Abdulwahed AMS, et al. Evaluation of the major steps in the conventional protocol for the alkaline comet assay. Int J Mol Sci. 2019;20(23):6072. doi:10.3390/ijms20236072
54. Ding W, Bishop ME, Lyn-Cook LE, Davis KJ, Manjanatha MG. In vivo alkaline comet assay and enzyme-modified alkaline comet assay for measuring DNA strand breaks and oxidative DNA damage in rat liver. J Vis Exp. 2016;(111):53833. doi:10.3791/53833
55. Kumaravel TS, Vilhar B, Faux SP, Jha AN. Comet assay measurements: a perspective. Cell Biol Toxicol. 2009;25(1):53–64. doi:10.1007/s10565-007-9043-9
56. Konan S, Tahmassebi J, Haddad FS. The development and validation of a more discriminating functional hip score for research. HSS J. 2012;8(3):198–205. doi:10.1007/s11420-012-9298-4
57. Lhotka C, Szekeres T, Steffan I, Zhuber K, Zweymüller K. Four-year study of cobalt and chromium blood levels in patients managed with two different metal-on-metal total hip replacements. J Orthop Res. 2003;21(2):189–195. doi:10.1016/S0736-0266(02)00152-3
58. Anissian HL, Stark A, Gustafson A, Good V, Clarke IC. Metal-on-metal bearing in hip prosthesis generates 100-fold less wear debris than metal-on-polyethylene. Acta Orthop Scand. 1999;70(6):578–582. doi:10.3109/17453679908997845
59. Savarino L, Granchi D, Ciapetti G, et al. Ion release in patients with metal-on-metal hip bearings in total joint replacement: a comparison with metal-on-polyethylene bearings. J Biomed Mater Res. 2002;63(5):467–474. doi:10.1002/jbm.10299
60. MacDonald SJ, McCalden RW, Chess DG, et al. Metal-on-metal versus polyethylene in hip arthroplasty: a randomized clinical trial. Clin Orthop Relat Res. 2003;(406):282–296. doi:10.1097/01.blo.0000043066.62337.9d
61. Back DL, Young DA, Shimmin AJ. How do serum cobalt and chromium levels change after metal-on-metal hip resurfacing? Clin Orthop Relat Res. 2005;438:177–181. doi:10.1097/01.blo.0000166901.84323.5d
62. Yang J, Shen B, Zhou Z, Pei F, Kang P. Changes in cobalt and chromium levels after metal-on-metal hip resurfacing in young, active Chinese patients. J Arthroplasty. 2011;26(1):65–70.e1. doi:10.1016/j.arth.2009.11.019
63. Afolaranmi GA, Tettey J, Meek RM, Grant MH. Release of chromium from orthopaedic arthroplasties. Open Orthop J. 2008;2:10–18. doi:10.2174/1874325000802010010
64. Wahlqvist F, Bryngelsson IL, Westberg H, Vihlborg P, Andersson L. Dermal and inhalable cobalt exposure-uptake of cobalt for workers at Swedish hard metal plants. PLoS One. 2020;15(8):e0237100. doi:10.1371/journal.pone.0237100
65. Kop AM, Swarts E. Corrosion of a hip stem with a modular neck taper junction: a retrieval study of 16 cases. J Arthroplasty. 2009;24(7):1019–1023. doi:10.1016/j.arth.2008.09.009
66. Langton DJ, Jameson SS, Joyce TJ, Webb J, Nargol AV. The effect of component size and orientation on the concentrations of metal ions after resurfacing arthroplasty of the Hip. J Bone Joint Surg Br. 2008;90(9):1143–1151. doi:10.1302/0301-620X.90B9.20785
67. Pritchett JW. Adverse reaction to metal debris: metallosis of the resurfaced Hip. Curr Orthop Pract. 2012;23(1):50–58. doi:10.1097/BCO.0b013e3182356075
68. Bansal T, Aggarwal S, Dhillon MS, Patel S. Gross trunnion failure in metal on polyethylene total hip arthroplasty-a systematic review of literature. Int Orthop. 2020;44(4):609–621. doi:10.1007/s00264-019-04474-z
69. Delaunay C, Petit I, Learmonth ID, Oger P, Vendittoli PA. Metal-on-metal bearings total hip arthroplasty: the cobalt and chromium ions release concern. Orthop Traumatol Surg Res. 2010;96(8):894–904. doi:10.1016/j.otsr.2010.05.008
70. Lassalle M, Colas S, Rudnichi A, Zureik M, Dray-Spira R. Is there a cardiotoxicity associated with metallic head hip prostheses? A cohort study in the French national health insurance databases. Clin Orthop Relat Res. 2018;476(7):1441–1451. doi:10.1097/01.blo.0000533617.64678.69
71. Nguyen UDT, Perneger T, Franklin PD, Barea C, Hoffmeyer P, Lübbeke A. Improvement in mental health following total hip arthroplasty: the role of pain and function. BMC Musculoskelet Disord. 2019;20(1):307. doi:10.1186/s12891-019-2669-y
72. Cristancho P, Lenze EJ, Avidan MS, Rawson KS. Trajectories of depressive symptoms after hip fracture. Psychol Med. 2016;46(7):1413–1425. doi:10.1017/S0033291715002974
73. Krenk L, Kehlet H, Bæk Hansen T, Solgaard S, Soballe K, Rasmussen LS. Cognitive dysfunction after fast-track hip and knee replacement. Anesth Analg. 2014;118(5):1034–1040. doi:10.1213/ANE.0000000000000194
74. Oldenburg M, Wegner R, Baur X. Severe cobalt intoxication due to prosthesis wear in repeated total hip arthroplasty. J Arthroplasty. 2009;24(5):
75. Rizzetti MC, Liberini P, Zarattini G, et al. Loss of sight and sound. Could it be the hip? Lancet. 2009;373(9668):1052. doi:10.1016/S0140-6736(09)60490-6
76. Ikeda T, Takahashi K, Kabata T, Sakagoshi D, Tomita K, Yamada M. Polyneuropathy caused by cobalt-chromium metallosis after total hip replacement. Muscle Nerve. 2010;42(1):140–143. doi:10.1002/mus.21638
77. Tower SS. Arthroprosthetic cobaltism: neurological and cardiac manifestations in two patients with metal-on-metal arthroplasty: a case report. J Bone Joint Surg Am. 2010;92(17):2847–2851. doi:10.2106/JBJS.J.00125
78. Jordan C, Whitman RD, Harbut M, Tanner B. Memory deficits in workers suffering from hard metal disease. Toxicol Lett. 1990;54(2–3):241–243. doi:10.1016/0378-4274(90)90190-w
79. Meecham HM, Humphrey P. Industrial exposure to cobalt causing optic atrophy and nerve deafness: a case report. J Neurol Neurosurg Psychiatry. 1991;54(4):374–375. doi:10.1136/jnnp.54.4.374
80. Höck A, Demmel U, Schicha H, Kasperek K, Feinendegen LE. Trace element concentration in human brain. Activation analysis of cobalt, iron, rubidium, selenium, zinc, chromium, silver, cesium, antimony and scandium. Brain. 1975;98(1):49–64. doi:10.1093/brain/98.1.49
81. Huk OL, Catelas I, Mwale F, Antoniou J, Zukor DJ, Petit A. Induction of apoptosis and necrosis by metal ions in vitro. J Arthroplasty. 2004;19(8 Suppl 3):84–87. doi:10.1016/j.arth.2004.09.011
82. Karovic O, Tonazzini I, Rebola N, et al. Toxic effects of cobalt in primary cultures of mouse astrocytes. Similarities with hypoxia and role of HIF-1alpha. Biochem Pharmacol. 2007;73(5):694–708. doi:10.1016/j.bcp.2006.11.008
83. Bridges RL, Cho CS, Beck MR, Gessner BD, Tower SS. F-18 FDG PET brain imaging in symptomatic arthroprosthetic cobaltism. Eur J Nucl Med Mol Imaging. 2020;47(8):1961–1970. doi:10.1007/s00259-019-04648-2
84. Valavanidis A, Vlachogianni T, Fiotakis C. 8-hydroxy-2’ -deoxyguanosine (8-OHdG): a critical biomarker of oxidative stress and carcinogenesis. J Environ Sci Health C. 2009;27(2):120–139. doi:10.1080/10590500902885684
85. Beyersmann D, Hartwig A. Carcinogenic metal compounds: recent insight into molecular and cellular mechanisms. Arch Toxicol. 2008;82(8):493–512. doi:10.1007/s00204-008-0313-y
86. Pilger A, Schaffer A, Rüdiger HW, Osterode W. Urinary 8-hydroxydeoxyguanosine and sister chromatid exchanges in patients with total hip replacements. J Toxicol Environ Health A. 2002;65(9):655–664. doi:10.1080/15287390252900359
87. Wang CC, Chen WL, Lin CM, et al. The relationship between plasma and urinary 8-hydroxy-2-deoxyguanosine biomarkers measured by liquid chromatography tandem mass spectrometry. Environ Sci Pollut Res Int. 2016;23(17):17496–17502. doi:10.1007/s11356-016-6898-4
88. Christian WV, Oliver LD, Paustenbach DJ, Kreider ML, Finley BL. Toxicology-based cancer causation analysis of CoCr-containing hip implants: a quantitative assessment of genotoxicity and tumorigenicity studies. J Appl Toxicol. 2014;34(9):939–967. doi:10.1002/jat.3039
89. Sampson B, Hart A. Clinical usefulness of blood metal measurements to assess the failure of metal-on-metal hip implants. Ann Clin Biochem. 2012;49(Pt 2):118–131. doi:10.1258/acb.2011.011141
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.