Back to Journals » Neuropsychiatric Disease and Treatment » Volume 22
Psychiatric Comorbidity in Chronic Tinnitus: Depression and Anxiety in an Otolaryngology Outpatient Cohort
Authors Sırma E, Dedeoglu S ![]() , Toprak SF, Dönmezdil S
, Toprak SF, Dönmezdil S
Received 17 December 2025
Accepted for publication 27 February 2026
Published 18 March 2026 Volume 2026:22 589644
DOI https://doi.org/10.2147/NDT.S589644
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Taro Kishi
Enes Sırma,1,* Serkan Dedeoglu,1,* Serdar Ferit Toprak,2 Süleyman Dönmezdil3
1Department of Otorhinolaryngology, University of Health Sciences Gazi Yasargil Training and Research Hospital, Diyarbakır, Turkey; 2Department of Audilogy, Artuklu University, Mardin, Turkey; 3Department of Psychology, Artuklu University, Mardin, Turkey
*These authors contributed equally to this work
Correspondence: Serkan Dedeoglu, Department of Otorhinolaryngology, University of Health Sciences, Gazi Yasargil Training and Research Hospital, Diyarbakir, Turkey, Tel +90 532 599 97 29, Email [email protected]
Purpose: Chronic subjective tinnitus is commonly accompanied by psychological distress; however, its independent relationship with depressive and anxiety symptoms in otolaryngology outpatients has not been fully delineated. This study sought to estimate the prevalence of mood symptoms among adults with chronic tinnitus and to determine whether tinnitus severity contributes independently to psychological burden.
Patients and Methods: In this cross-sectional study, 100 adults with subjective tinnitus of at least six months’ duration were evaluated at a tertiary otolaryngology clinic. Participants completed the Tinnitus Handicap Inventory (THI), Beck Depression Inventory–II (BDI-II), and Beck Anxiety Inventory (BAI). Prevalence estimates were compared with population-level data. Associations between tinnitus severity and mood symptoms were examined using correlation analyses and multivariable linear regression adjusted for age, sex, and hearing status.
Results: Mean scores were 47.2 ± 18.3 for THI, 16.1 ± 10.4 for BDI-II, and 19.5 ± 11.2 for BAI. Tinnitus severity showed moderate positive associations with depressive (r = 0.50) and anxiety symptoms (r = 0.48), both p < 0.001. After adjustment, THI scores remained independently associated with higher BDI-II (β = 0.42, p < 0.001) and BAI scores (β = 0.39, p < 0.001). Severe tinnitus (THI ≥ 58) was linked to increased odds of moderate-to-severe depression (OR 3.10, 95% CI 1.52– 6.30) and anxiety (OR 2.84, 95% CI 1.40– 5.72). Clinically relevant depressive and anxiety symptoms were identified in 28% and 31% of participants, respectively.
Conclusion: Greater tinnitus severity is independently associated with elevated symptom severity of depression and anxiety. These findings underscore the importance of routine mental health screening and multidisciplinary management in ENT practice.
Keywords: psychological comorbidity, mood symptoms, tinnitus handicap inventory, otolaryngology outpatients, mental health screening
Introduction
Chronic tinnitus—the perception of sound in the absence of an external stimulus—is a prevalent and distressing condition affecting up to 20% of the adult population worldwide, with approximately 1–3% experiencing severe, life-disrupting symptoms.1 Traditionally regarded as an otologic disorder, tinnitus is now understood as a complex neuropsychiatric condition involving widespread brain networks. Neuroimaging studies have revealed altered activity not only in the auditory cortex, but also in emotion-regulation regions such as the amygdala, hippocampus, and prefrontal cortex, suggesting that tinnitus distress is closely tied to central nervous system processing.2–4
A growing body of evidence indicates that individuals with chronic tinnitus are at elevated risk for psychiatric comorbidities, particularly depression and anxiety.5–7 These symptoms are not merely reactive; they may share common neurobiological substrates with tinnitus itself. For example, dysfunction within the limbic system and the hypothalamic–pituitary–adrenal (HPA) axis has been implicated in both tinnitus severity and affective dysregulation.8,9 Nonetheless, the causal relationships remain contested. Some authors suggest that depression and anxiety predispose individuals to perceive tinnitus as more distressing, while others propose that chronic tinnitus precipitates mood disorders, particularly when poorly habituated.10–12
Despite this emerging conceptual framework, controversy persists regarding the prevalence of psychiatric comorbidity in chronic tinnitus. Notably, unlike previous studies that focused on general or hospitalized populations, this study examines independent associations in an ENT outpatient cohort using standardized psychiatric instruments, thereby addressing a gap in the literature. Further research is needed in patient ENT cohorts using standardized psychiatric screening tools.
The present study aimed to clarify the relationship between tinnitus severity and depressive and anxiety symptoms in a tertiary otolaryngology setting. We hypothesised that higher tinnitus handicap would be associated with greater psychiatric symptom burden, independent of demographic and audiological factors. This investigation provides new insight into the magnitude and clinical significance of psychological distress in chronic tinnitus, with implications for screening and multidisciplinary care.
Materials and Methods
Study Design and Ethics
This cross-sectional observational study was conducted at the Department of Otorhinolaryngology, Gazi Yaşargil Training and Research Hospital, Diyarbakır, Turkey, a tertiary referral center. The study protocol was reviewed and approved by the Clinical Research Ethics Committee of Mardin Artuklu University (Approval No: 2025/7-33; Date: 25 July 2025). All participants provided written informed consent prior to enrolment. The study was conducted in accordance with the principles of the Declaration of Helsinki and applicable local regulatory requirements.
Participants
A total of 100 adult patients (aged ≥18 years) presenting with chronic subjective tinnitus of at least six months’ duration were consecutively recruited between 1 August and 1 October 2025. Inclusion criteria were: (1) diagnosis of chronic subjective tinnitus, (2) sufficient proficiency in Turkish to complete self-report questionnaires, and (3) absence of diagnosed neurological or psychotic disorders. Exclusion criteria included: (1) objective tinnitus attributable to identifiable otologic or vascular causes, (2) initiation or change of psychiatric medication within the preceding three months, (3) severe hearing loss exceeding 70 dB HL, and (4) inability or unwillingness to provide informed consent.
Audiological Assessment
All participants underwent pure-tone audiometry using an Interacoustics AC40 clinical audiometer administered by a certified audiologist in a sound-proof booth, for air and bone conduction thresholds. Following the American Academy of Otolaryngology–Head and Neck Surgery (AAO–HNS) guidelines. Pure-tone average (PTA) thresholds were calculated at 0.5, 1, 2, 3, and 4 kHz in the tinnitus-affected ear. A PTA ≥30 dB HL was considered indicative of clinically significant hearing loss.
Clinical and Psychological Measures
-Tinnitus Handicap Inventory (THI): A 25-item questionnaire assessing functional, emotional, and catastrophic impacts of tinnitus, with total scores ranging from 0 to 100; higher scores indicate greater perceived tinnitus-related handicap.
-Beck Depression Inventory–II (BDI-II): A 21-item measure evaluating depressive symptom severity over the preceding two weeks (score range: 0–63).
-Beck Anxiety Inventory (BAI): A 21-item scale assessing cognitive and somatic anxiety symptoms experienced during the previous week (score range: 0–63).
Each participant self-completed the above questionnaires (under supervision of the research staff if needed). Participants then provided demographic variables (age and sex), tinnitus duration (in months), and audiological findings were also recorded.
Sample Size Estimation
An a priori power analysis was performed using G*Power version 3.1. To detect a medium effect size correlation (r = 0.30) with 80% statistical power at a two-sided alpha level of 0.05, a minimum sample size of 84 participants was required. The final sample of 100 participants exceeded this threshold.
Statistical Analysis
Statistical analyses were conducted using IBM SPSS Statistics version 26.0. Descriptive statistics were calculated for demographic, audiological, and clinical variables. The Shapiro–Wilk test was used to assess normality of continuous data. Associations between tinnitus severity and mood-related measures were examined using Pearson or Spearman correlation coefficients, as appropriate.
Multiple linear regression analyses were performed to evaluate whether THI scores independently predicted depressive (BDI-II) and anxiety (BAI) symptom severity after adjusting for age, sex, and hearing status. Effect sizes were estimated using Cohen’s f2, and odds ratios (ORs) were calculated where applicable. All tests were two-tailed, and a p-value <0.05 was considered statistically significant.
Data Availability
The datasets generated and/or analyzed during the current study are not publicly available due to institutional data protection policies but are available from the corresponding author upon reasonable request.
Use of Generative Artificial Intelligence
No generative artificial intelligence tools were used in the study design, data collection, statistical analysis, or interpretation of results. Limited AI-assisted proofreading was employed solely for grammatical and formatting purposes and did not influence the scientific content.
Results
Participant Characteristics
A total of 100 participants were included in the analysis, of whom 58 were female (58%). The mean age of the study population was 48.5 ± 12.1 years, and the mean duration of tinnitus was 32.4 ± 20.8 months. Clinically significant hearing loss, defined as a pure-tone average (PTA) ≥30 dB HL in the tinnitus-affected ear, was present in 70% of participants. Detailed demographic and clinical characteristics are summarized in Table 1.
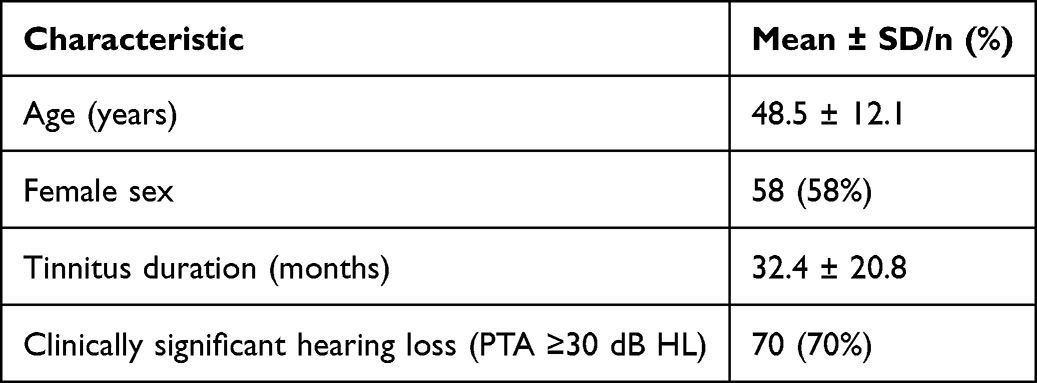 |
Table 1 Demographic and Clinical Characteristics of the Study Population (N = 100) |
Descriptive Scores of Tinnitus and Mood Measures
The mean Tinnitus Handicap Inventory (THI) score was 47.2 ± 18.3, indicating a moderate overall tinnitus-related burden. Mean scores for depressive and anxiety symptoms were 16.1 ± 10.4 on the Beck Depression Inventory–II (BDI-II) and 19.5 ± 11.2 on the Beck Anxiety Inventory (BAI), respectively. A substantial proportion of participants exceeded established cut-off values for clinically relevant symptom severity. The distribution of depression and anxiety severity categories is presented in Table 2.
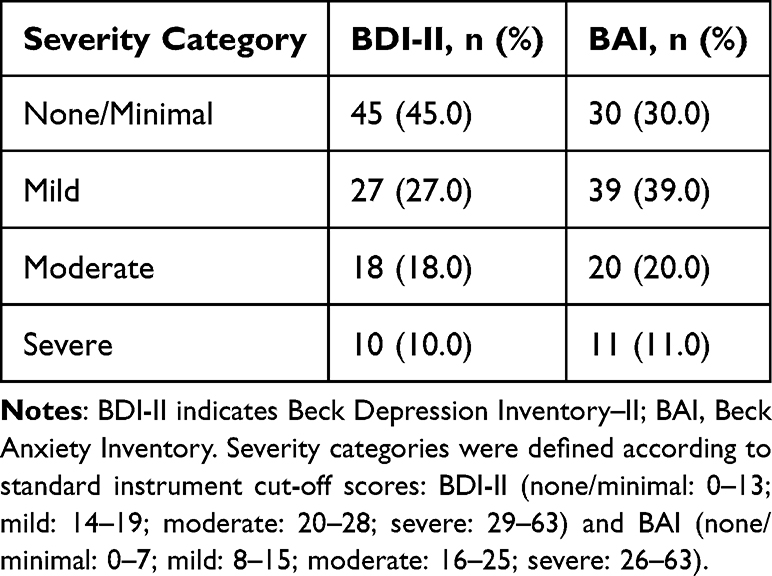 |
Table 2 Severity Classification of Depressive and Anxiety Symptoms According to BDI-II and BAI Scores (N = 100) |
Associations Between Tinnitus Severity and Mood Symptoms
Pearson correlation analyses demonstrated moderate positive associations between tinnitus severity and both depressive and anxiety symptoms. THI scores correlated significantly with BDI-II scores (r = 0.50, p < 0.001) and BAI scores (r = 0.48, p < 0.001). A strong positive correlation was also observed between depressive and anxiety symptoms (r = 0.62, p < 0.001). No significant correlations were identified between age or tinnitus duration and mood symptom scores (all p > 0.10). Correlation analyses revealed significant positive associations between tinnitus severity and both depressive and anxiety symptoms (Table 3).
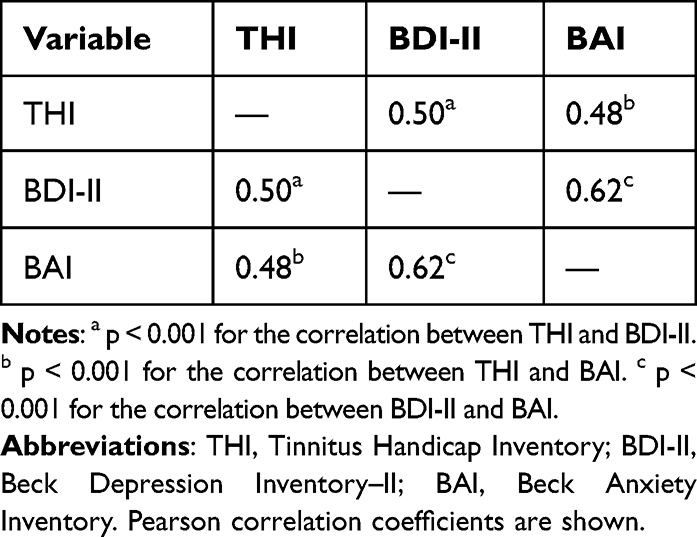 |
Table 3 Correlations Between Tinnitus Severity, Depressive Symptoms, and Anxiety Symptoms |
Multivariable Regression Analyses
Multivariable linear regression models were constructed to examine whether tinnitus severity independently predicted depressive and anxiety symptoms after adjusting for age, sex, and hearing status. In the model predicting BDI-II scores, THI remained a significant independent predictor (β = 0.42, p < 0.001), explaining 25% of the variance (R2 = 0.25). Similarly, THI independently predicted BAI scores (β = 0.39, p < 0.001), with an R2 of 0.21. None of the covariates reached statistical significance. Regression diagnostics confirmed acceptable model assumptions, including absence of multicollinearity (VIF < 1.5), no autocorrelation (Durbin–Watson ≈2), and normally distributed residuals. The relationship between THI and BDI-II scores is illustrated in Figure 1.
 |
Figure 1 Relationship between tinnitus severity and depressive symptoms. Scatterplot illustrating the association between Tinnitus Handicap Inventory (THI) scores and Beck Depression Inventory–II (BDI-II) scores among patients with chronic subjective tinnitus (N = 100). The solid line represents the fitted linear regression, and the shaded area indicates the 95% confidence interval. Higher THI scores were moderately and positively correlated with higher BDI-II scores (Pearson r = 0.50, p < 0.001). Abbreviations: THI, Tinnitus Handicap Inventory; BDI-II, Beck Depression Inventory–II. |
Prevalence and Odds of Clinically Significant Mood Symptoms
Moderate-to-severe depressive symptoms (BDI-II ≥20) were identified in 28% of participants, while moderate-to-severe anxiety symptoms (BAI ≥19) were present in 31%. Patients with severe tinnitus (THI ≥58) exhibited significantly higher odds of both depression (OR = 3.10, 95% CI 1.52–6.30, p = 0.002) and anxiety (OR = 2.84, 95% CI 1.40–5.72, p = 0.004) compared with those with mild tinnitus (THI <38). These findings are summarized in Table 4. The distribution of depression and anxiety severity across tinnitus severity categories is shown in Figure 2.
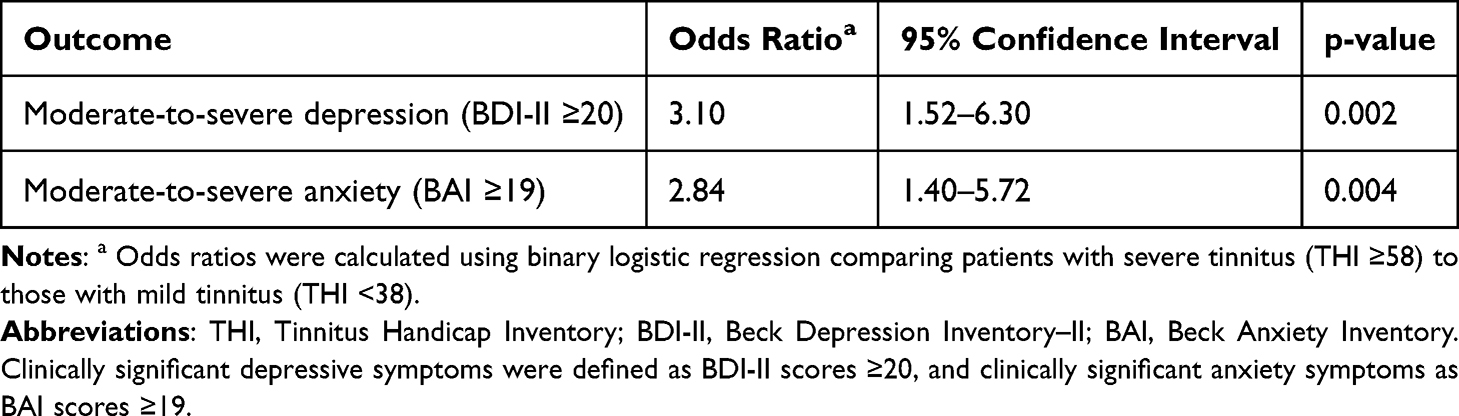 |
Table 4 Odds of Clinically Significant Depressive and Anxiety Symptoms in Patients with Severe Tinnitus Compared with Mild Tinnitus |
 |
Figure 2 Distribution of depressive and anxiety symptom severity across tinnitus severity categories. Bar charts showing the distribution of Beck Depression Inventory–II (BDI-II) and Beck Anxiety Inventory (BAI) severity categories stratified by tinnitus severity based on Tinnitus Handicap Inventory (THI) scores (mild, moderate, and severe). Higher tinnitus severity was associated with a greater proportion of patients exhibiting moderate-to-severe depressive and anxiety symptoms. Severity categories: BDI-II: none/minimal (0–13), mild (14–19), moderate (20–28), severe (29–63). BAI: none/minimal (0–7), mild (8–15), moderate (16–25), severe (26–63). Abbreviations: THI, Tinnitus Handicap Inventory; BDI-II, Beck Depression Inventory–II; BAI, Beck Anxiety Inventory. |
Discussion
This study demonstrated a strong and independent association between tinnitus severity and psychological distress, specifically depressive and anxiety symptoms, among adults with chronic subjective tinnitus. Approximately one-third of participants met criteria for clinically significant depression (28%) or anxiety (31%), substantially exceeding prevalence rates reported in the general population (approximately 6–7%).7 Moreover, tinnitus severity, as measured by the Tinnitus Handicap Inventory (THI), remained a significant independent predictor of both depressive and anxiety symptom severity after adjustment for age, sex, and hearing loss.
These findings are consistent with previous literature emphasizing the substantial psychiatric burden associated with tinnitus. Salazar et al reported a median prevalence of depression of approximately 33% among tinnitus patients across diverse clinical settings,5 while Bhatt et al demonstrated high rates of psychiatric comorbidity in large, population-based samples.6 Similarly, Chen et al used network analysis to show that depressive and anxiety symptoms were present in 25–26% of individuals with tinnitus, compared with approximately 9% in non-tinnitus controls.4 The slightly higher prevalence observed in the present study may be attributable to the tertiary-care otolaryngology setting, which is likely to include patients with more persistent, severe, or distressing tinnitus symptoms.
The observed moderate correlations between THI scores and both depressive and anxiety symptoms (r = 0.50 and r = 0.48, respectively) further support evidence that emotional distress intensifies as perceived tinnitus-related handicap increases.3–5 These findings align with contemporary neurobiological models of tinnitus, which implicate overlapping neural networks involved in auditory processing, emotional regulation, and cognitive control. Functional and structural neuroimaging studies have demonstrated altered activity within the auditory cortex, limbic structures, and prefrontal regions, including the amygdala, insula, and anterior cingulate cortex, in individuals with tinnitus. Such alterations may enhance the emotional salience of the tinnitus percept and contribute to its persistence and associated distress.8,13
The directionality of the relationship between tinnitus and affective symptoms remains a matter of debate. Some authors propose that pre-existing depressive or anxiety disorders predispose individuals to heightened tinnitus-related distress,10 whereas others suggest that chronic tinnitus functions as a persistent stressor capable of precipitating or exacerbating mood disturbances, particularly in the absence of effective coping strategies or therapeutic support.11 Although the cross-sectional design of the present study precludes causal inference, the regression analyses indicate that tinnitus severity contributes meaningfully to psychological symptomatology, independent of key demographic and audiological factors. The incremental contribution of the present study lies in reporting clinically meaningful effect sizes and odds ratios, thereby enhancing the clinical interpretability of the association between tinnitus severity and psychological distress.
Dysregulation of stress-response systems may represent a shared biological pathway linking tinnitus and emotional distress. Prior studies have documented hypothalamic–pituitary–adrenal (HPA) axis hyperactivity in patients with severe tinnitus, reflected by elevated cortisol levels and altered autonomic reactivity.2,12 These neuroendocrine abnormalities closely parallel mechanisms implicated in depressive and anxiety disorders, reinforcing the hypothesis of overlapping pathophysiological processes.9
From a clinical perspective, these findings underscore the importance of routine psychological screening in patients presenting with chronic tinnitus. The use of brief, validated instruments such as the Patient Health Questionnaire-9 or the Generalized Anxiety Disorder-7 may facilitate early identification of comorbid mood disorders and prompt timely intervention. Addressing emotional and cognitive factors through evidence-based approaches, including cognitive behavioral therapy, mindfulness-based interventions, or appropriate pharmacological treatment, may substantially reduce tinnitus-related distress even when the auditory percept itself persists.
Furthermore, the results support a multidisciplinary approach to tinnitus management that integrates otolaryngological, audiological, and mental health expertise. While sound therapy and hearing aids may attenuate tinnitus perception, comprehensive care requires simultaneous attention to the emotional and psychological dimensions of the condition. Future clinical guidelines should therefore emphasize psychosocial evaluation as a core component of tinnitus assessment and management.
Strengths and Limitations
Key strengths of this study include the use of validated assessment instruments (THI, BDI-II, and BAI), an adequately powered sample size, and robust multivariable regression analyses with appropriate diagnostic checks. Nonetheless, several limitations warrant consideration. The single-center design and absence of a non-tinnitus control group limit generalizability. In addition, reliance on self-report questionnaires rather than structured psychiatric interviews may have introduced reporting bias. Cultural and language factors may also restrict extrapolation of the findings beyond the Turkish population.
Future Directions
Future studies should employ longitudinal designs to clarify the temporal and causal relationships between tinnitus severity and mood disturbances. Investigation of additional moderating factors, such as coping styles, personality traits (eg., neuroticism), and neuroendocrine markers, may further elucidate individual vulnerability. Randomized controlled trials evaluating integrated tinnitus and mental health interventions are also needed to inform evidence-based, multidisciplinary treatment strategies.
Clinical Implications
This study demonstrates that chronic subjective tinnitus is closely linked to heightened depressive and anxiety symptoms in a clinical otolaryngology population. Nearly one-third of patients met criteria for moderate-to-severe mood symptoms, a proportion markedly higher than that observed in the general population. Importantly, tinnitus severity, quantified using the Tinnitus Handicap Inventory, was independently associated with both depression and anxiety after accounting for demographic factors and hearing loss.
These findings reinforce the clinical value of incorporating psychosocial screening into routine tinnitus care. Multidisciplinary approaches that combine audiological and mental health interventions may enhance quality of life and overall outcomes for affected individuals. Longitudinal investigations are warranted to clarify causal pathways and to assess the effectiveness of integrated treatment strategies.
Conclusion
This study confirms that chronic subjective tinnitus is strongly associated with elevated symptoms of depression and anxiety. In this clinical sample of otolaryngology outpatients, nearly one-third of patients exhibited moderate-to-severe depressive or anxiety symptoms, substantially exceeding rates reported in the general population. Tinnitus severity, as measured by the Tinnitus Handicap Inventory, emerged as an independent predictor of both depressive and anxiety symptom severity after adjustment for age, sex, and hearing loss.
These findings highlight the importance of routine psychosocial screening as part of comprehensive tinnitus management. Integrating mental health assessment and multidisciplinary care approaches may improve quality of life and overall clinical outcomes for individuals with chronic tinnitus. Future longitudinal studies are needed to clarify causal relationships and to evaluate the effectiveness of integrated therapeutic strategies.
Abbreviations
The following abbreviations are used in this manuscript: ANS, Autonomic Nervous System; BAI, Beck Anxiety Inventory; BDI-II, Beck Depression Inventory–II; CBT, Cognitive-Behavioral Therapy; HPA, Hypothalamic–Pituitary–Adrenal (axis); HPT, Hypothalamic–Pituitary–Thyroid (axis); PTA, Pure Tone Average (hearing threshold); THI, Tinnitus Handicap Inventory.
Data Sharing Statement
The data are not publicly available due to privacy concerns. However, data are available from the corresponding author upon reasonable request.
Ethics Approval
The study was conducted in accordance with the Declaration of Helsinki, and approved by Ethics Committee) of MARDİN ARTUKLU UNIVERSITY Clinical Research Ethics Committee (protocol code 2025/7-33 and date: 25.07.2025).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Jeong JE, Jeon S, Han JS, et al. The mediating effect of psychological distress on the association between BDNF, 5-HTTLPR, and Tinnitus severity. Psychiatry Invest. 2021;18(3):187–9. doi:10.30773/pi.2020.0295
2. Patil JD, Alrashid MA, Eltabbakh A, Fredericks S. The association between stress, emotional states, and tinnitus: a mini-review. Front Aging Neurosci. 2023;15:1131979. doi:10.3389/fnagi.2023.1131979
3. Fetoni AR, Lucidi D, Corso E, Fiorita A, Conti G, Paludetti G. Relationship between subjective Tinnitus perception and psychiatric discomfort. Int Tinnitus J. 2017;20(2):76–82. doi:10.5935/0946-5448.20160015
4. Chen X, Ren L, Xue X, et al. The comorbidity of depression and anxiety symptoms in Tinnitus sufferers: a network analysis. Brain Sci. 2023;13(4):583. doi:10.3390/brainsci13040583
5. Salazar JW, Meisel K, Smith ER, Quiggle A, McCoy DB, Amans MR. Depression in patients with Tinnitus: a systematic review. Otolaryngol Head Neck Surg. 2019;161(1):28–35. doi:10.1177/0194599819835178
6. Bhatt JM, Lin HW, Bhattacharyya N. Prevalence, severity, exposures, and treatment patterns of Tinnitus in the United States. JAMA Otolaryngol Head Neck Surg. 2016;142(10):959–965. doi:10.1001/jamaoto.2016.1700
7. Terlizzi EP, Zablotsky B. Symptoms of anxiety and depression among adults: United States, 2019 and 2022. Natl Health Stat Rep. 2024;213. doi:10.15620/cdc/64018
8. Adjamian P, Sereda M, Hall DA. The mechanisms of tinnitus: perspectives from human functional neuroimaging. Hear Res. 2009;253(1):15–31. doi:10.1016/j.heares.2009.04.001
9. Fioretti A, Natalini E, Riedl D, Moschen R, Eibenstein A. Gender comparison of psychological comorbidities in Tinnitus patients – results of a cross-sectional study. Front Neurosci. 2020;14:704. doi:10.3389/fnins.2020.00704
10. Andersson G. Psychological aspects of tinnitus and the application of cognitive–behavioral therapy. Clinic Psychol Rev. 2002;22(7):977–990. doi:10.1016/S0272-7358(01)00124-6
11. Reynolds P, Gardner D, Lee R. Tinnitus and psychological morbidity: a cross-sectional study to investigate psychological morbidity in tinnitus patients and its relationship with severity of symptoms and illness perceptions. Clin Otolaryngol Allied Sci. 2004;29(6):628–634. doi:10.1111/j.1365-2273.2004.00879.x
12. Reeves WC, Strine TW, Pratt LA, et al. Mental illness surveillance among adults in the United States. MMWR Suppl. 2011;60(3):1–29.
13. Çelik EK, Özsoy F, Ertürk BY. Tinnitus: does it lead to impairments in metacognitive functions and the theory of mind skills? Turk Arch Otorhinolaryngol. 2025;62(4):131–137. doi:10.4274/tao.2024.2024-8-4
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.