Back to Journals » Journal of Pain Research » Volume 19
Psychedelics and Ibogaine “Pain Medications” at the Pharmacy Counter: Implications for Pharmacy Practice
Authors Breve F, Berenato FJ, Pergolizzi JV Jr, Varrassi G ![]() , Raffa RB
, Raffa RB ![]()
Received 2 June 2026
Accepted for publication 26 June 2026
Published 8 July 2026 Volume 2026:19 629049
DOI https://doi.org/10.2147/JPR.S629049
Checked for plagiarism Yes
Editor who approved publication: Dr Robert Twillman
Frank Breve,1 Frank J Berenato,2 Joseph V Pergolizzi Jr,3,4 Giustino Varrassi,5 Robert B Raffa3,6
1Clinical Pharmacy, Mid Atlantic PharmaTech Consultants, Ventnor City, NJ, USA; 2Compounding, Med Shoppe, Philadelphia, PA, USA; 3Research and Development, Enalare Therapeutics, Mullica Hill, NJ, USA; 4Anesthesiology, NEMA Research, Naples, FL, USA; 5VIBRA Research Group, Fondazione Paolo Procacci, Roma, Italy; 6School of Pharmacy, Temple University (Emeritus), Philadelphia, PA, USA
Correspondence: Robert B Raffa, Email [email protected]
The regulatory process governing psychedelic substances in the United States is undergoing its most significant transformation since the Controlled Substances Act of 1970. An executive order signed in April 2026 directed federal agencies to accelerate development pathways for psychedelic and related therapies. These developments signal that FDA approval of one or more psychedelic agents is no longer a distant prospect, but a foreseeable regulatory event. Since there is a growing interest and some evidence for psychedelics and ibogaine for treatment of pain (though the field is at different stages of maturity for different compounds and pain types), the executive order will affect pain research and practice.
The directive is an acknowledgement that the pharmacological landscape of psychiatric and addiction medicine is being reshaped by converging forces: a deepening mental health crisis, inadequate response rates to conventional pharmacotherapy in conditions such as treatment-resistant depression (TRD) and post-traumatic stress disorder (PTSD), and a growing body of clinical trial evidence supporting the efficacy of psychedelic-assisted therapies.1–3 The executive order hopes to compress standard review timelines from about six to ten months to about sixty days.4
Approval of psychedelic-assisted therapies (Table 1) will require substantial evolution of pharmacy practice across multiple domains: Controlled Substance Act (CSA) scheduling and controlled substance management, Risk Evaluation and Mitigation Strategy (REMS) program administration, pharmacogenomic screening, drug interaction counseling, patient education, and integration into specialty and clinical pharmacy practice models. Ibogaine presents the most pharmacologically complex scenario, requiring mandatory CYP2D6 genotyping, ECG monitoring protocols, and QT-prolonging drug interaction screening before each administration. The pharmacy profession is uniquely positioned to contribute to the safe implementation of these therapies and needs to proactively develop the competencies, infrastructure, and advocacy frameworks necessary to fulfill that role.
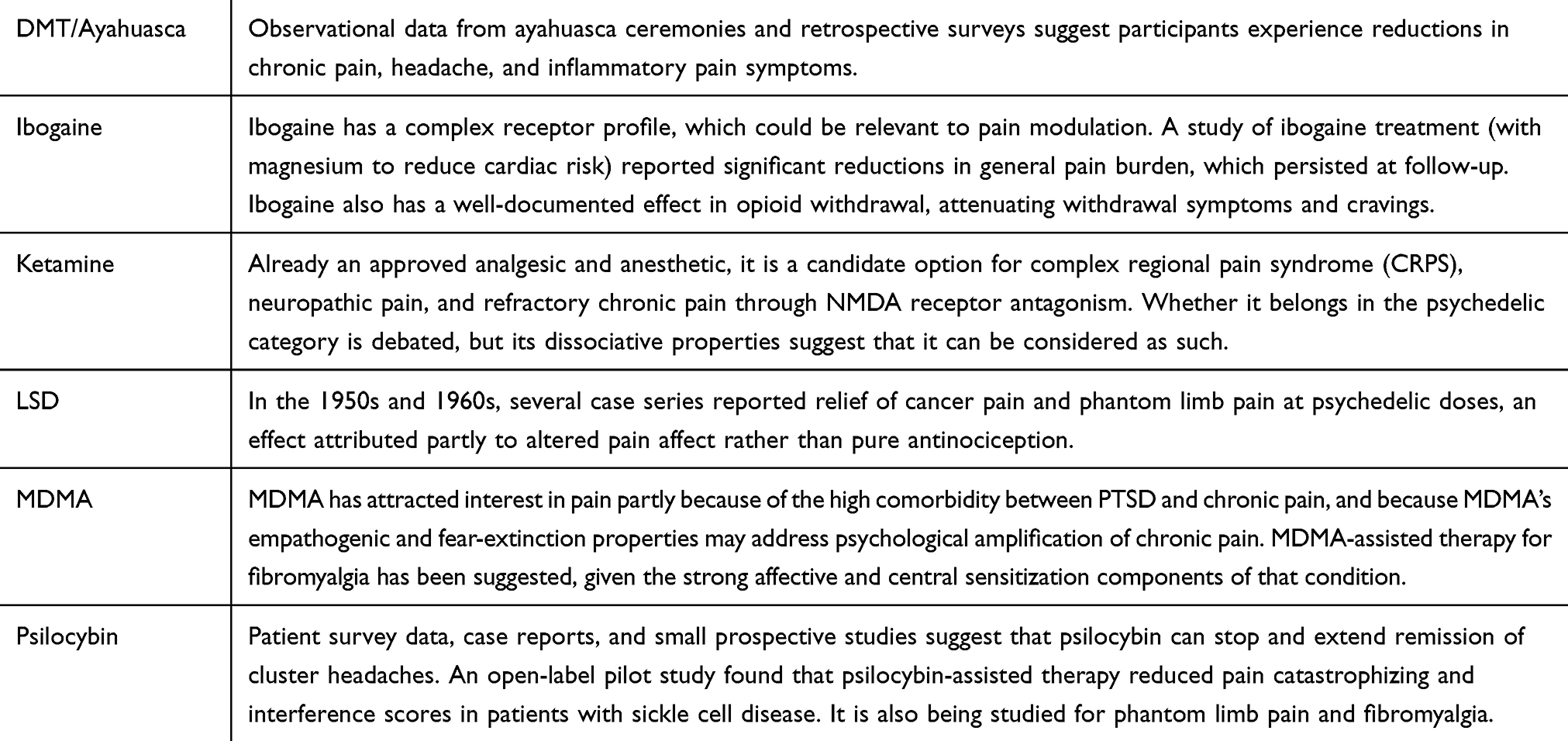 |
Table 1 Some of the Psychedelic-Related Compounds |
Controlled Substance Obligations
Psilocybin, LSD, DMT, MDMA, and ibogaine are currently classified as Schedule I controlled substances, a designation indicating by statute that the substance has no currently accepted medical use in the United States.5 The April 2026 executive order specifically directed the attorney general to expedite rescheduling review for any Schedule I substance that has completed a Phase 3 clinical trial for a serious mental health disorder. For pharmacies, rescheduling from Schedule I to Schedule II or III will create additional dispensing obligations. For example, Schedule II substances require strict inventory recordkeeping, biennial physical inventory, DEA Form 222 ordering or Controlled Substance ordering System (CSOS), DEA Form 41 for waste, and mandatory reporting of losses or thefts on DEA Form 106. Pharmacies that choose to dispense an approved psychedelic will need to register for the relevant schedule, establish specific and secure storage protocols (eg, type of safe and lock, separated C1 and C2, etc), train staff in Schedule II dispensing procedures, and integrate psychedelic dispensing into existing pharmacy information systems.
REMS, DDI Screening, and Medication Reconciliation
The FDA has substantial precedent for requiring a Risk Evaluation and Mitigation Strategy (REMS) as a condition of approval for drugs with serious safety profiles that nonetheless offer meaningful clinical benefit. It has been predicted that any broadly approved clinical use of psilocybin or MDMA will likely require a REMS; such programs require maintenance of patient registries and safety surveillance, but REMS programs can also unfortunately create access inequities when compliance burdens are disproportionately distributed.6 A psychedelic REMS program would almost certainly require pharmacies to be certified dispensers, mandate healthcare provider training as a condition of prescribing authority, and may require evidence of a verified clinical administration setting before dispensing. For clinical pharmacists, a psychedelic REMS would require verifying patient eligibility, confirming safety monitoring data, documenting counseling, and communicating with prescribers when safety criteria are not met.
The drug interaction profiles of psychedelic drugs are clinically complex and will require pharmacists to develop new competency in a rapidly evolving evidence base. The most consequential interaction class involves serotonergic agents. Coadministration of classical serotonergic psychedelics with SSRIs or SNRIs produces two distinct concerns: pharmacodynamic blunting of psychedelic effects via 5-HT2A receptor downregulation, and the theoretical risk of serotonin syndrome.7 Furthermore, lithium combined with classical psychedelics is associated with seizures in approximately 47% of documented case reports, representing one of the most serious and least ambiguous drug–drug interaction contraindications in psychedelic medicine.8 For MDMA, the critical interaction concern involves monoamine oxidase inhibitors (MAOIs), which substantially elevate serotonergic and cardiovascular toxicity risk, and stimulant medications (eg, amphetamines and methylphenidate), whose pharmacodynamic overlap with MDMA’s noradrenaline-releasing mechanism creates cumulative cardiovascular risk. Pharmacist’s medication reconciliation and interaction screening role has been specifically identified as central to psychiatric patient safety in psychedelic therapy contexts, noting that patients with mental health conditions frequently carry complex polypharmacy burdens that require expert review before psychedelic administration.9
Challenges of Ibogaine and Noribogaine
Ibogaine presents perhaps the most pharmacologically and clinically complex scenario of the psychedelic agents currently in development, and its potential approval, or the approval of its active metabolite noribogaine, will create pharmacy practice demands that exceed those of other agents in this class. Ibogaine is a Schedule I agent with a multi-receptor pharmacology engaging NMDA glutamate receptors, nicotinic acetylcholine receptors, opioid receptors, and monoamine transporters simultaneously – a polypharmacology that underlies both its efficacy and its complex safety profile.10,11 The primary concern for pharmacy practice is cardiotoxicity: ibogaine inhibits the cardiac hERG potassium channel and Nav1.5 sodium channel at low micromolar concentrations, producing QTc prolongation and possibility for torsades de pointes (TdP) and fatal ventricular arrhythmia.12,13 Noribogaine, ibogaine’s long-lived active metabolite, can remain in the circulation for extended periods and may contribute to delayed arrhythmogenic risk, requiring cardiac monitoring beyond the duration of the psychedelic experience itself.10 The metabolic clearance of ibogaine is strongly determined by CYP2D6 genotype,14 with the highest risk expected in CYP2D6 poor metabolizers and in patients taking CYP2D6 inhibitors concurrently.15 The pharmacy implications are that clinical pharmacists will need to obtain, interpret, and integrate CYP2D6 genotype results into ibogaine dosing recommendations. Pharmacists who dispense ibogaine will need to be competent in phenotype-genotype translation for CYP2D6, understand the dose-adjustment implications of inhibitor co-prescription, and be able to communicate these individualized risk profiles to prescribers and patients.14,15 The most operationally intensive pharmacy role in ibogaine therapy will be systematic screening for co-prescribed or self-administered QT-prolonging agents before each ibogaine administration. Ibogaine’s hERG channel blockade is additive or synergistic with other QT-prolonging drugs, creating arrhythmia risk that scales with the number and potency of concomitant QT-prolonging medications,12 the list of which spans virtually all major drug classes relevant to patients with substance use disorders and psychiatric comorbidities. Standard pharmacy software drug interaction modules will need to be updated to include ibogaine-specific interaction alerts, and clinical pharmacists embedded in addiction treatment or psychiatric settings will need to conduct prospective medication reconciliation specifically targeting QT liability before ibogaine administration.
Patient Education and Equity of Access
The pharmacist’s patient education role in psychedelic-assisted therapy will need to extend beyond the conventional counseling model of explaining indications, dosing, and common side effects. Patients preparing for a psychedelic therapeutic session require education about the nature of the psychedelic experience itself, including the possibility of intense emotional responses, perceptual alterations, and transient anxiety, as well as guidance on what to communicate to their care team about their current medications, illicit drug use, and medical history.
A REMS-constrained, specialty pharmacy-restricted dispensing model for psychedelic agents, while clinically justified on safety grounds, carries inherent unintentional risk of replicating or amplifying the healthcare access disparities that already characterize mental health treatment in the United States. REMS programs have historically failed and created access problems, and that regulatory requirements incur significant costs that may be passed on to the consumer, limiting access among disadvantaged groups.6 The populations carrying the greatest burden of treatment-resistant depression, PTSD, and opioid use disorder, conditions targeted by psychedelic-assisted therapies, include veterans, racial and ethnic minorities, rural populations, and people experiencing poverty. These groups are precisely those for whom REMS complexity, specialty pharmacy access requirements, and therapy costs represent the highest barriers.
Conclusions
FDA approval of one or more psychedelic agents – a development that has moved from speculative to plausible given the April 2026 federal executive order – will create a new environment that pharmacy practice is perhaps not yet fully equipped to navigate. The required evolution spans controlled substance management under new CSA scheduling frameworks, active participation in REMS program design and administration, pharmacogenomic testing and interpretation for ibogaine’s CYP2D6-dependent dosing, systematic QT-prolonging drug interaction screening, and a redesigned patient education model suited to the unique demands of psychedelic-assisted therapy. This places the pharmacy profession at an important junction. The infrastructure decisions, regulatory frameworks, training standards, and access policies that will govern psychedelic medicine implementation are being determined now. There is an opportunity for active engagement by pharmacy professional organizations, pharmacy schools, and individual clinical pharmacists in the policy conversations, particularly regarding safety considerations, more robust regulatory compliance measures, and the equity implications of the dispensing models that will govern access to these potentially innovative therapies.
Disclosure
Dr Joseph Pergolizzi Jr is a director for and reports grants and personal fees from Enalare Therapeutics Inc, Stock or stock options from Enalare Therapeutics Inc, outside the submitted work. Dr Giustino Varrassi reports honoraria from “Roma Pain Days” for €1,200.00, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Reiff CM, Richman EE, Nemeroff CB. et al. Psychedelics and psychedelic-assisted psychotherapy. Focus (Am Psychiatr Publ). 2021;19(1):95–4. doi:10.1176/appi.focus.19104
2. Mitchell JM, Ot’alora GM, van der Kolk B, et al. MDMA-assisted therapy for moderate to severe PTSD: a randomized, placebo-controlled phase 3 trial. Nat Med. 2023;29(10):2473–2480. doi:10.1038/s41591-023-02565-4
3. Goodwin GM, Aaronson ST, Alvarez O, et al. Single-dose psilocybin for a treatment-resistant episode of major depression. N Engl J Med. 2022;387(18):1637–1648. doi:10.1056/NEJMoa2206443
4. Trump D. Executive Order (April 18): accelerating medical treatments for serious mental illness. Available from: https://www.whitehouse.gov/presidential-actions/2026/04/accelerating-medical-treatments-for-serious-mental-illness/.
5. Bykov K, He M, Gagne JJ. Trends in utilization of prescribed controlled substances in US commercially insured adults, 2004-2019. JAMA Intern Med. 2020;180(7):1006–1008. doi:10.1001/jamainternmed.2020.0989
6. Bradberry MM, Gukasyan N, Raison CL. Toward risk-benefit assessments in psychedelic- and MDMA-assisted therapies. JAMA Psychiatry. 2022;79(6):525–527. doi:10.1001/jamapsychiatry.2022.0665
7. Tap SC, Thomas K, Palenicek T, et al. Concomitant use of antidepressants and classic psychedelics: a scoping review. J Psychopharmacol. 2025;39(10):1072–1088. doi:10.1177/02698811251368360
8. Malcolm B, Thomas K. Serotonin toxicity of serotonergic psychedelics. Psychopharmacology. 2022;239(6):1881–1891. doi:10.1007/s00213-021-05876-x
9. El-Den S, Collins JC, Chen TF, O’Reilly CL. Pharmacists’ roles in mental healthcare: past, present and future. Pharm Pract. 2021;19(3):2545. doi:10.18549/PharmPract.2021.3.2545
10. Esperança MP, Gomes NGM, Campos MG. Ibogaine: therapeutic potential, cardiac safety, and translational perspectives in the treatment of substance use disorders-a scoping review. Molecules. 2026;31(3):545. doi:10.3390/molecules31030545
11. Luz M, Mash DC. Evaluating the toxicity and therapeutic potential of ibogaine in the treatment of chronic opioid abuse. Expert Opin Drug Metab Toxicol. 2021;17(9):1019–1022. doi:10.1080/17425255.2021.1944099
12. Koenig X, Hilber K. The anti-addiction drug ibogaine and the heart: a delicate relation. Molecules. 2015;20(2):2208–2228. doi:10.3390/molecules20022208
13. Rubi L, Eckert D, Boehm S, Hilber K, Koenig X. Anti-addiction drug ibogaine prolongs the action potential in human induced pluripotent stem cell-derived cardiomyocytes. Cardiovasc Toxicol. 2017;17(2):215–218. doi:10.1007/s12012-016-9366-y
14. Knuijver T, Ter Heine R, Schellekens AFA, et al. The pharmacokinetics and pharmacodynamics of ibogaine in opioid use disorder patients. J Psychopharmacol. 2024;38(5):481–488. doi:10.1177/02698811241237873
15. Knuijver T, Schellekens A, Belgers M, et al. Safety of ibogaine administration in detoxification of opioid-dependent individuals: a descriptive open-label observational study. Addiction. 2022;117(1):118–128. doi:10.1111/add.15448
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.