Back to Journals » Psoriasis: Targets and Therapy » Volume 6
Psoriasis patients’ experiences concerning medical adherence to treatment with topical corticosteroids
Authors Tiedemann Svendsen M ![]() , Ejner Andersen K, Andersen F, Hansen J, Pottegård A
, Ejner Andersen K, Andersen F, Hansen J, Pottegård A ![]() , Johannessen H
, Johannessen H
Received 30 March 2016
Accepted for publication 13 May 2016
Published 23 August 2016 Volume 2016:6 Pages 113—119
DOI https://doi.org/10.2147/PTT.S109557
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Uwe Wollina
Mathias Tiedemann Svendsen,1–3 Klaus Ejner Andersen,1–3 Flemming Andersen,1,3 Jakob Hansen,4 Anton Pottegård,5 Helle Johannessen6
1Department of Dermatology and Allergy Centre, Odense University Hospital, 2Centre for Innovative Medical Technology, Institute of Clinical Research, University of Southern Denmark, Odense C, 3Dermatological Investigations Scandinavia, University of Southern Denmark, Odense C, 4Leo Pharma, Ballerup, 5Clinical Pharmacology, Department of Public Health, University of Southern Denmark, 6Research Unit of User Perspectives, Department of Public Health, University of Southern Denmark, Odense C, Denmark
Abstract: Nonadherence to topical treatment of psoriasis is a common cause of treatment failure. This focus group study was conducted to obtain the patients’ own experiences and explanations regarding medical adherence. The participants consisted of eight primary adherent patients with moderate psoriasis treated with corticosteroid or corticosteroid–calcipotriol combinations, purposefully sampled by age and sex at a dermatology outpatient clinic. Secondary medical adherence was supported by accessibility of the prescribing physician, the prescriber taking time to listen, having a more manageable disease, using a nonstaining product, and establishing routines around treatment at home. Secondary medical adherence was affected negatively by changes in daily routines, if the treatment influenced the patient’s sexual life, having too little time in the consultation room, lack of confidence in the prescriber, diverging information from health care personnel, experiencing side effects, having fear of side effects, impractical formulations of topical products, and impatience regarding time before an effect of the treatment was observed. From this study, the recommendations for the prescribing doctor to improve medical adherence are, the doctor needs to take time to listen to the patient, prescribe a topical product that is easy to apply and less greasy, inform the patients about benefits from treatments, and explain the rationale behind the treatment plan.
Keywords: psoriasis, adherence, corticosteroids, calcipotriol, focus groups
Introduction
Psoriasis is a chronic disease with a prevalence rate of 2%–4% in the Western population.1 Topical corticosteroids and corticosteroid–calcipotriol combinations constitute first line of treatment. In chronic diseases, one of the main causes of treatment failure is medical nonadherence.2 In patients with psoriasis, the rate of medical nonadherence to topically prescribed corticosteroids or corticosteroid combinations is reported to range from 8% to 88%,3,4 addressed in studies using heterogeneous study designs. The multifactorial determinants of medical nonadherence to topical corticosteroids and corticosteroid/calcipotriol combinations have mainly been investigated in survey studies,5,6 while only briefly described in qualitative studies.7,8 This led us to conduct this study, to get the patients’ own experiences and explanations on medical adherence.
Participants and methods
In January 2016, we led two semistructured focus groups using open-ended questions in patients diagnosed with psoriasis and treated with topical corticosteroid and/or corticosteroid–calcipotriol combinations. Participants were purposefully sampled by age and sex at the outpatient clinic at the Department of Dermatology and Allergy Centre, Odense, in December 2015. Upon recruitment, a Psoriasis Area Severity Index score and a Dermatology Life Quality Index score were obtained for each patient. Furthermore, patients were asked if they were primary adherent, ie, having filled their prescription, and provided a measure of self-reported secondary adherence, ie, not applying medication from filled prescription, on a visual analog scale. Finally, patients were asked open questions regarding their living/health conditions and use of antipsoriatic treatments (medical history and sociodemographic characteristics of patients are presented in Tables 1 and 2).
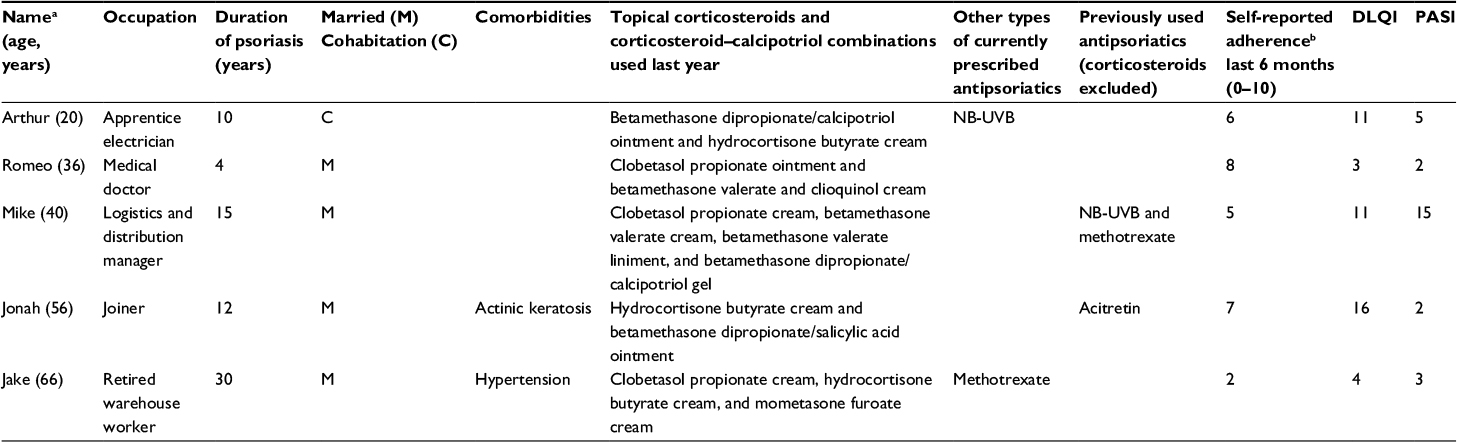 | Table 1 Participant demographics and medical history in focus group held for men Notes: aAll patients are given a fictional name. bIn addition, all patients reported being primary adherent 6 months prior to the study. Abbreviation: DLQI, Dermatology Life Quality Index; PASI, Psoriasis Area Severity Index; NB-UVB, narrowband ultraviolet B phototherapy. |
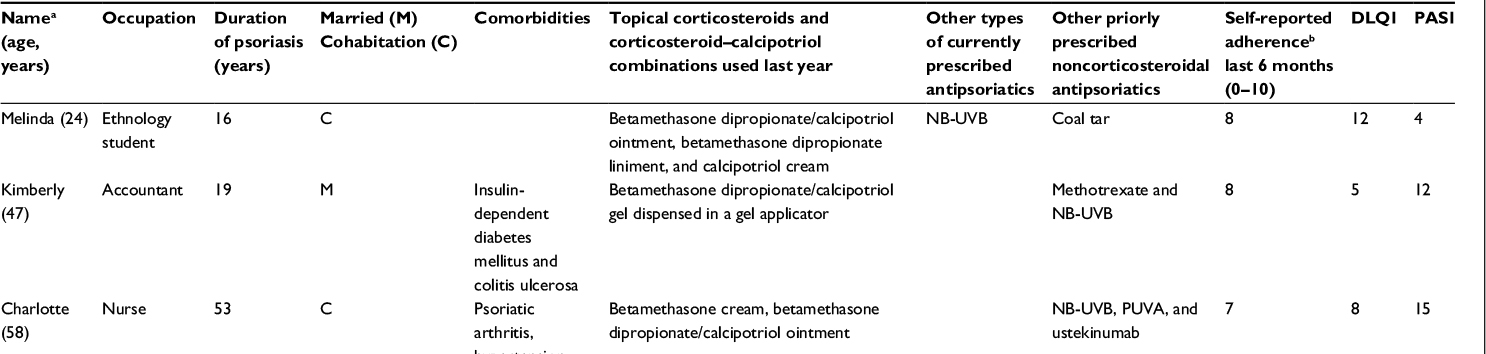 | Table 2 Participant demographics and medical history in focus group held for women Notes: aAll patients are given a fictional name. bIn addition, all patients reported being primary adherent 6 months prior to the study. Abbreviations: DLQI, Dermatology Life Quality Index; PASI, Psoriasis Area Severity Index; NB-UVB, narrowband ultraviolet B phototherapy; PUVA, psoralen combined with ultraviolet A therapy. |
One focus group was held for men and another for women. The study was conducted in accordance with the World Medical Association’s Declaration of Helsinki. Eight primary adherent patients suffering from psoriasis took part in the study, five men and three women. The age range was 20–66 years, with a median age of 43.5 years. The focus groups were led by MTS and HJ in a conference room at the hospital. To demonstrate primary adherence, the patients were asked to bring all the packages of corticosteroids and corticosteroid–calcipotriol combinations they had at home. Initially, while placing the packages on the table in front of them, the patients were briefly asked to introduce themselves and tell about their disease and use of topical antipsoriatics. After this, we continued to discuss reasons for medical nonadherence. The discussions were grouped in five consecutive sections according to the determinants of nonadherence defined by the World Health Organization (WHO)9 listed in Table 3. We used audio recording and continued until all points were discussed. Each focus group lasted ~100 minutes.
 | Table 3 Determinants of nonadherence defined by the World Health Organization (WHO)9 Note: Reprinted by permission from WHO [Report No: WHO/MNC/03.01]. Sabaté E. Adherence to Long-Term Therapies: Evidence for Action. World Health Organization; 2003. © 2003 WHO.9 |
The audio records were transcribed and thereafter manually coded by MTS. In the evaluation, we used deductive qualitative content analyses based on WHO’s five categories for determinants affecting adherence. Codes were grouped into larger categories. Uniformities and variations were revealed by MTS and HJ in a comparative process.
Ethics
Ethical approval was not required for this study according to Danish law. A signed consent was obtained from all participants before the focus groups were held.
Results
All reported determinants influencing medical adherence are given in Tables 4 and 5. Medical adherence was supported by living with a partner, accessibility of the prescribing physician, the prescriber taking time to listen, having a more manageable disease, using a nonstaining product, and establishing routines around treatment at home (Table 4). In contrast, medical adherence was negatively affected by changes in daily routines, if the treatment influenced the patient’s sexual life, having too little time in the consultation room, lack of confidence in the prescriber, diverging information from health care personnel, experiencing side effects, having fear of side effects, impractical formulations of topical products, and impatience regarding time before an effect of the treatment was observed (Table 5). The price of medication was considered high, but the participants prioritized to buy the medication or had the medication paid for by health insurance or family members. Although some of the patients expressed a wish for an effective treatment, they also reported discontinuing treatment when it worked. Six out of eight patients used complementary approaches as a supplement to prescribed treatments; most commonly sun bathing and vitamin supplements (Table 6).
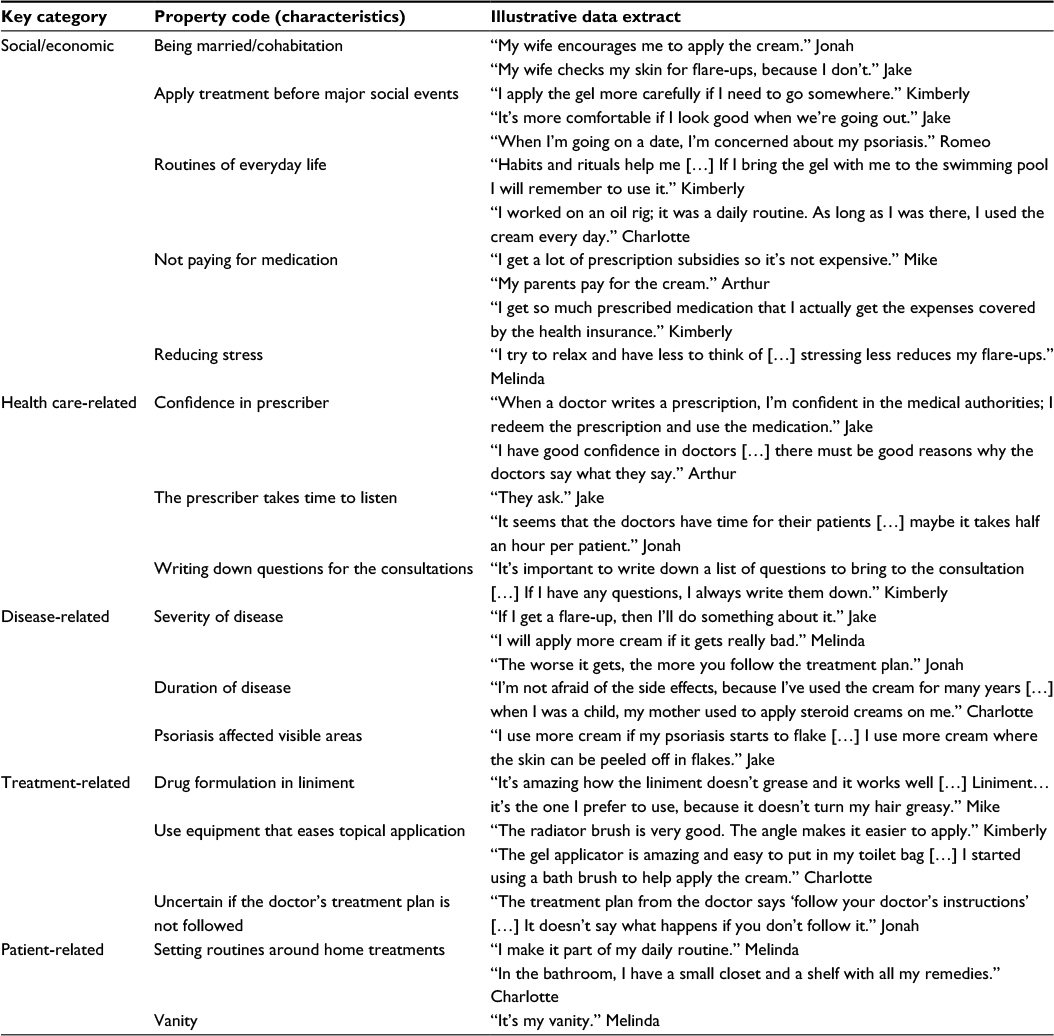 | Table 4 Key categories and property codes relevant to being adherent to prescribed topical corticosteroids and corticosteroid–calcipotriol combinations |
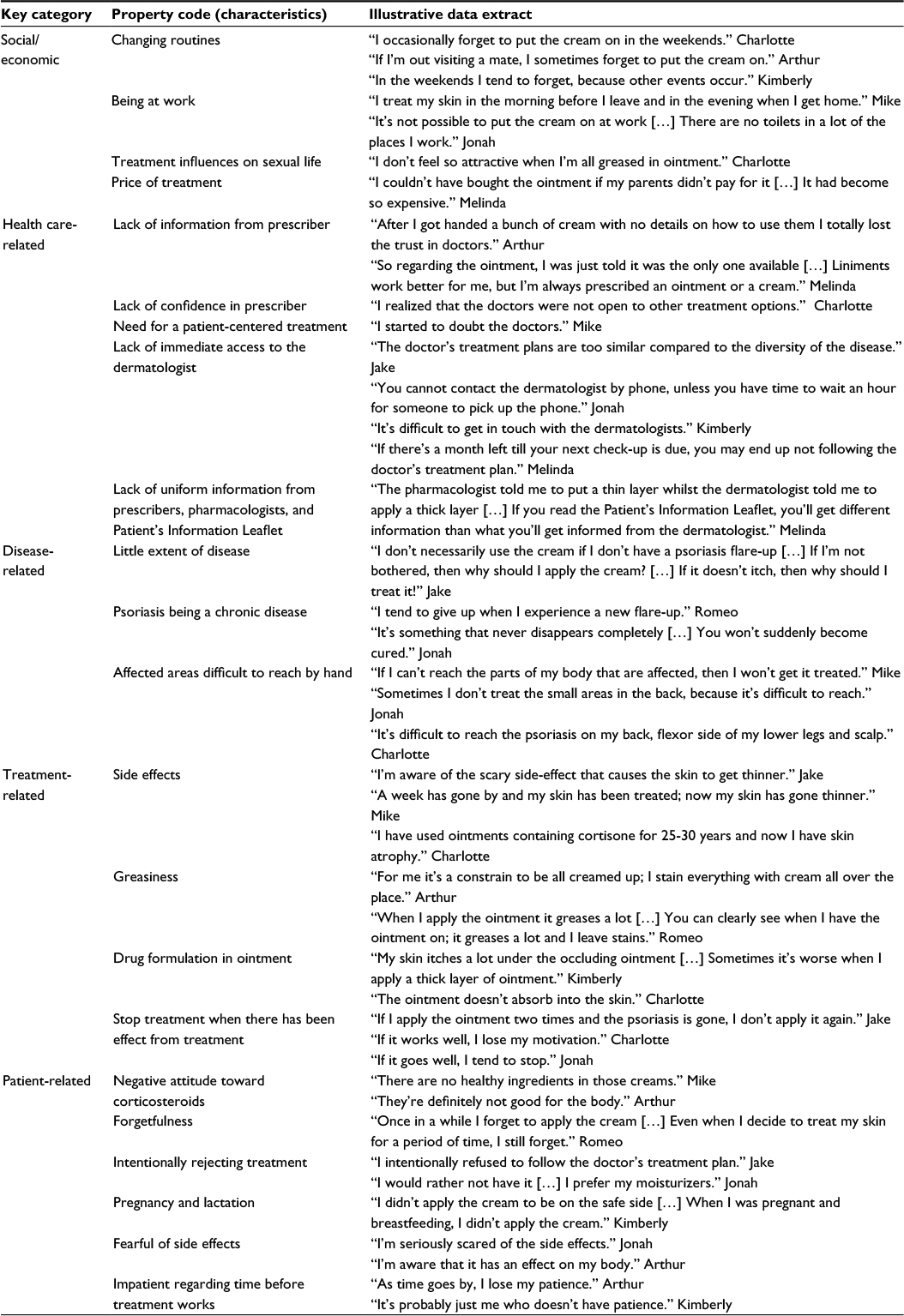 | Table 5 Key categories and property codes relevant to being nonadherent to prescribed topical corticosteroids and corticosteroid–calcipotriol combinations |
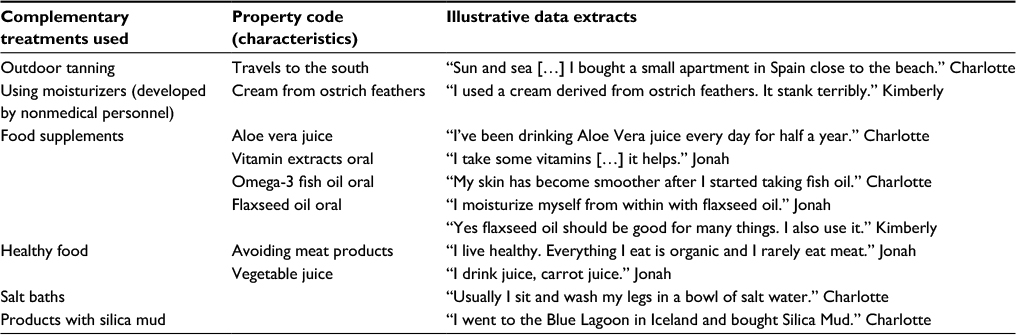 | Table 6 Complementary treatments used |
Discussion
This study adds information on important aspects of living with psoriasis, a disease requiring topical treatment that is both time consuming and impractical for the patient. Using a qualitative research design helped us to provide insight into the nonmeasurable aspects of the patient’s perceptions on medical drugs and daily life. The results from our study may not be representative of all patients with psoriasis. This is stressed by the patients described in this study all being primary adherent and having regular checkups at the hospital clinic. To identify differences in determinants of nonadherence between primary versus secondary nonadherent patients, we recommend future studies to be conducted among topically treated primary nonadherent psoriasis patients. Potentially, participants could also be sampled from other settings, ie, general practice or private dermatologists. The study findings align with those reported in the international literature. In relation to social/economic factors, adherence was limited when patients experienced the disease influencing on their intimate life,10 but improved by receiving support from their partner.3 Considering treatment factors, adherence was limited when patients experienced the treatment as greasy,5 but improved when treatment was easy to apply.5,11 In relation to the health care system, adherence was limited when patients experienced uncertainty regarding the rationale behind the treatment plan,6,7,12 but improved from confidence in the prescriber.6 In relation to the disease, adherence was limited by having areas difficult to reach,6 but improved when suffering from widespread disease.6 In relation to the patients themselves, adherence was limited by patients terminating treatment when initial positive treatment results were reached,5 but improved by establishing routines in their everyday life.5,12 In addition to previous research, this study showed that the patients received help from their partner in checking the skin for flare-ups and assisting in greasing.
Treatments need to be continued after they have shown an initial beneficial effect. Further research is needed to elucidate the effect of, eg, early follow-up visits13 or use of technical support on adherence. Technical support could include sending mobile phone reminders14 or use of patient-supporting apps delivered by smartphones. For the prescriber to help improve adherence, the recommendations from this study are the doctor needs to take time to listen to the patient, prescribe a topical product that is easy to apply and less greasy, inform the patients about benefits from treatments, and explain the rationale behind the treatment plan.
Disclosure
The authors report no conflicts of interest in this work.
References
Parisi R, Symmons DP, Griffiths CE, Ashcroft DM; Identification and Management of Psoriasis and Associated ComorbidiTy (IMPACT) Project Team. Global epidemiology of psoriasis: a systematic review of incidence and prevalence. J Invest Dermatol. 2013;133(2):377–385. | ||
Urquhart J. The odds of the three nons when an aptly prescribed medicine isn’t working: non-compliance, non-absorption, non-response. Br J Clin Pharmacol. 2002;54(2):212–220. | ||
Zaghloul SS, Goodfield MJ. Objective assessment of compliance with psoriasis treatment. Arch Dermatol. 2004;140(4):408–414. | ||
Svedbom A, Dalen J, Mamolo C, Cappelleri JC, Petersson IF, Stahle M. Treatment patterns with topicals, traditional systemics and biologics in psoriasis – a Swedish database analysis. J Eur Acad Dermatol Venereol. 2015;29(2):215–223. | ||
Feldman SR. Disease burden and treatment adherence in psoriasis patients. Cutis. 2013;92(5):258–263. | ||
Burroni AG, Fassino M, Torti A, Visentin E. How do disease perception, treatment features, and dermatologist-patient relationship impact on patients assuming topical treatment? An Italian survey. Patient Relat Outcome Meas. 2015;6:9–17. | ||
Ersser SJ, Cowdell FC, Latter SM, Healy E. Self-management experiences in adults with mild-moderate psoriasis: an exploratory study and implications for improved support. Br J Dermatol. 2010;163(5):1044–1049. | ||
Ring L, Kettis-Lindblad A, Kjellgren KI, Kindell Y, Maroti M, Serup J. Living with skin diseases and topical treatment: patients’ and providers’ perspectives and priorities. J Dermatolog Treat. 2007;18(4):209–218. | ||
Sabaté E. Adherence to Long-Term Therapies: Evidence for Action. Geneva: World Health Organization; 2003. [Report No.: WHO/MNC/03.01]. | ||
Meeuwis K, De Hullu J, Van de Nieuwenhof H, et al. Quality of life and sexual health in patients with genital psoriasis. Br J Dermatol. 2011;164(6):1247–1255. | ||
Eastman WJ, Malahias S, Delconte J, DiBenedetti D. Assessing attributes of topical vehicles for the treatment of acne, atopic dermatitis, and plaque psoriasis. Cutis. 2014;94(1):46–53. | ||
Bewley A, Burrage DM, Ersser SJ, Hansen M, Ward C. Identifying individual psychosocial and adherence support needs in patients with psoriasis: a multinational two-stage qualitative and quantitative study. J Eur Acad Dermatol Venereol. 2014;28(6):763–770. | ||
Davis SA, Lin HC, Yu CH, Balkrishnan R, Feldman SR. Underuse of early follow-up visits: a missed opportunity to improve patients’ adherence. J Drugs Dermatol. 2014;13(7):833–836. | ||
Balato N, Megna M, Costanzo L, Balato A, Ayala F. Educational and motivational support service: a pilot study for mobile-phone-based interventions in patients with psoriasis. Br J Dermatol. 2013;168(1):201–205. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.