Back to Journals » Psoriasis: Targets and Therapy » Volume 15
Psoriasis Does Not Seem to Impair Glomerular and Tubular Function – The Comprehensive Study on Serum and Urine
Authors Nowowiejska J, Baran A, Hermanowicz JM, Sieklucka B ![]() , Koper-Lenkiewicz OM
, Koper-Lenkiewicz OM ![]() , Kamińska J
, Kamińska J ![]() , Pawlak K
, Pawlak K ![]() , Pawlak D
, Pawlak D ![]() , Flisiak I
, Flisiak I ![]()
Received 25 March 2025
Accepted for publication 8 July 2025
Published 18 July 2025 Volume 2025:15 Pages 285—299
DOI https://doi.org/10.2147/PTT.S530313
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tina Bhutani
Julia Nowowiejska,1 Anna Baran,1 Justyna Magdalena Hermanowicz,2 Beata Sieklucka,3 Olga Martyna Koper-Lenkiewicz,4 Joanna Kamińska,4 Krystyna Pawlak,3 Dariusz Pawlak,2 Iwona Flisiak1
1Department of Dermatology and Venereology, Medical University of Bialystok, Bialystok, Poland; 2Department of Pharmacodynamics, Medical University of Bialystok, Bialystok, Poland; 3Department of Monitored Pharmacotherapy, Medical University of Bialystok, Bialystok, Poland; 4Department of Clinical Laboratory Diagnostics, Medical University of Bialystok, Bialystok, Poland
Correspondence: Julia Nowowiejska, Department of Dermatology and Venereology, Medical University of Bialystok, Zurawia 14 St., 15-540, Bialystok, Poland, Email [email protected]
Introduction: There is a dispute as to whether patients with psoriasis have impaired kidney function. We aimed to assess several recognized and experimental markers of glomerular filtration and tubular function in such patients to find out whether they have decreased kidney function.
Methods: The study involved 60 patients with psoriasis and 30 volunteers without dermatoses. The following molecules were analyzed by ELISA: serum creatinine, cystatin C, beta-trace protein, albumins, uromodulin; urinary albumins, cystatin C, alpha-1-microglobulin, beta-2-microglobulin, uromodulin, klotho, and fatty acid-binding protein 1, and nephrin.
Results: The following absolute values of markers concentrations were measured in patients, respectively: serum-1.13 (0.6– 1.9)mg/dl, 4.511 (2.356– 10.31)mg/l, 19.8 (2.8– 48)ng/mL, 4.2 (1.9– 8.85)g/dl, 212.3 (32.35– 583.9)ng/mL, urine– 5 (3– 39)g/dl, 24096 (79.94– 99020)ng/mL, 0.9342 (0.2088– 6.213)ng/mL, 22.65 (0.85– 105.8)ng/mL, 6.388 (0.8960– 15.94)ng/mL, 0.08 (0.002– 0.387)ng/mL, 1.773 (1.706– 2.146)ng/mL, 0.128 (0.095– 0.298)ng/mL. The patients had significantly lower serum albumin concentration (p< 0.001) and higher urinary albumin (p< 0.05), significantly higher serum cystatin C (p< 0.01), and absolute urinary nephrin (p< 0.05). There was no difference between patients and controls in terms of serum creatinine or beta trace protein concentration (p> 0.05). There were no significant differences in the concentration of the tubular markers (urinary cystatin C, alpha-1-microglobulin, beta-2-microglobulin, klotho, and fatty acid-binding protein 1) between patients and controls, except for serum and urinary uromodulin, which were significantly lower in patients (p< 0.01, p< 0.001, respectively). We found no significant correlations between the investigated markers’ concentration and clinical or demographic parameters (p> 0.05).
Discussion: Despite the differences between patients and controls in terms of glomerular filtration markers, the median values of markers’ concentration were within normal limits. Based on the assessment of the markers, it does not seem that impaired glomerular and tubular function occurs more frequently in patients with psoriasis. Nevertheless, due to the higher prevalence of diabetes mellitus and arterial hypertension in psoriatics and nephrotoxic properties of antipsoriatic drugs – caution must be exercised and easy screening tools should be considered.
Keywords: psoriasis, glomerular function, tubular function, creatinine, albumin, cystatin C, uromodulin, fatty acid-binding protein 1
Introduction
Psoriasis is a frequent, chronic and incurable skin disease that is an important medical, social, and economic burden.1 Psoriasis is characterized by wide comorbidity, especially associated with arthritis and cardiometabolic disorders, but there are several other accompanying diseases.2 There are many studies investigating a potentially increased risk of kidney disease in patients with psoriasis and it has been reported that patients with psoriasis have a 4.37 times higher risk of death due to kidney diseases than controls.3–5 However, it is a matter of debate whether it is due to psoriasis itself or to other accompanying factors.
Patients with psoriasis have been reported to have kidney dysfunction due to several reasons. First, they suffer more often from diabetes mellitus and arterial hypertension, which are known to exert damage to the kidneys 2. Secondly, there are immunological disturbances in psoriasis that can also affect kidney function; they are especially attributed to IL17A and TNFα, which are central cytokines in the pathogenesis of psoriasis but also are implicated in diabetic nephropathy, glomerulonephritis or nephrotic syndrome.6–9 Lastly, some of the systemic antipsoriatic agents can influence kidneys, such as methotrexate and cyclosporin A.10,11 In case of methotrexate, it is attributed to its precipitation or its metabolites in the renal tubules, as well as its direct damage to the tubular cells.12 Cyclosporin A, on the other hand, can trigger either acute or chronic nephrotoxicity, which is also dose- and therapy duration-dependent. An acute injury is related to the afferent arteriole constriction and hemodynamic dysfunction, whereas the chronic occurs due to chronic hypoperfusion and subsequent architectural alterations due to vasoconstriction.12
We decided to conduct a study on kidney function in patients with psoriasis and we divided our experiment into two parts: first, regarding glomerular filtration, and the other, regarding tubular function.
There are several molecules that could serve as the markers of glomeruli function, and the ideal marker should be only filtered but not secreted or reabsorbed by the tubules;13 or these could be molecules associated with the podocyte membrane integrity.14
Serum creatinine is probably the most widely used glomerular filtration rate (GFR) marker.15 Creatinine originates from creatine, which is the product of muscle metabolism.16 Creatinine serum level depends on several factors, such as sex, muscle mass, diet, and hydration of a subject.17,18 There are several mathematical formulas allowing for counting the GFR based on serum creatinine concentration. One of the disadvantages of the use of creatinine for GFR assessment is that its significant, measurable elevation occurs only when more than half of the active nephrons are damaged.18
Serum cystatin C (Cys-C) is another known marker of GFR, considered more reliable than creatinine,17 however less widely used due to its higher price.18 Cys-C is secreted by nucleated cells,16 and it undergoes filtration in glomeruli.17 Contrary to creatinine, Cys-C is more sensitive and is not dependent on gender, age, or muscle mass.18
Serum beta-trace protein (BTP; lipocalin prostaglandin D2 synthase, L-PDS) is a new suggested marker of GFR.15 Due to its large molecule, it is only filtered in glomeruli, catabolized in tubules, and not secreted.15,19 It seems to be more sensitive than creatinine, however with regard to Cys-C, the scientists argue which one is a more reliable marker.20
Nephrin is a podocyte-specific marker. Its content becomes elevated in the urine when the integrity of the glomerular barrier is compromised.21 Nephrinuria is positively correlated with proteinuria and the severity of podocyte injury.21
Albuminuria is the content of albumin in the urine. Under normal circumstances, the daily excretion of albumins is less than 30 mg, whereas the albumin-to-creatinine ratio (ACR) is less than 30 mg/g.21
There have also been several markers of renal tubular function described. Their assessment in urine may contribute to the diagnosis of reabsorption impairment.
Cystatin C, as mentioned, is filtered in glomeruli, and then reabsorbed and catabolized, so normally only small amounts are found in urine.22 Urinary concentration of Cys-C may mirror the reabsorption in the proximal tubules.23 Increased urinary Cys-C suggests decreased reabsorption.23
Serum and urinary uromodulin (Tamm-Horsfall protein) are the markers of the remaining nephron number.23,24 Uromodulin is a glycoprotein that is synthesized in the tubular cells.24 Studies have shown that a decreased concentration of uromodulin, both in serum and urine, indicates a reduced number of nephrons.24 Plasma uromodulin concentrations are much lower than those in the urine.25
Alpha-1-microglobulin (A1M) is a glycoprotein from the lipocalin superfamily, produced in the liver.23 Similar to cystatin C, it is a marker of proximal tubules dysfunction and its levels increase in the urine of such patients.23
Beta-2-microglobulin (B2M) is the product of the cellular membrane turnover and is filtered in the glomeruli and then reabsorbed in the proximal tubules, hence, an increase in urinary B2M may indicate tubular abnormalities.26
Fatty acid-binding protein 1 (FABP1), also known as liver FABP (L-FABP), plays a role in synthesizing, binding, and transporting long-chain fatty acids, and it also has antioxidant properties. While primarily found in hepatocytes, it can also be present in the intestines and kidneys. Elevated levels of FABP-1 may indicate kidney or lung injury, and it can serve as a predictor for nonalcoholic fatty liver disease (NAFLD).27
Klotho is a protein synthesized by the epithelial cells of renal tubules. It has been shown that decreased concentrations of Klotho in serum or urine are associated with tubular injury and chronic kidney disease development.28
Our aim was to assess the glomeruli and tubular function in patients with psoriasis based on the measurement of glomeruli and tubular function biomarkers, both already recognized, and experimental, in the serum or urine of patients with psoriasis (Table 1).
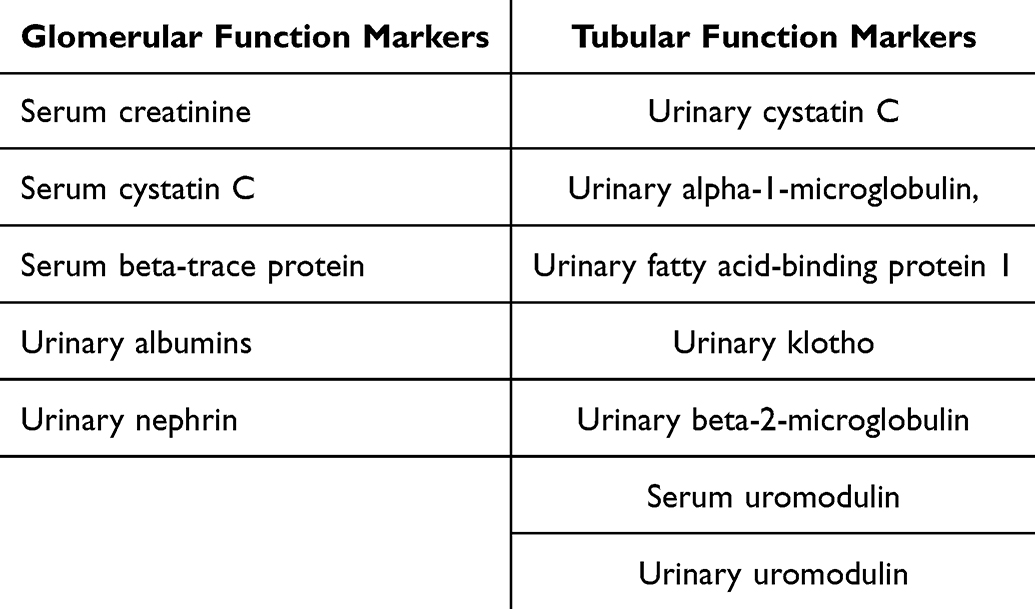 |
Table 1 The Summary of the Analyzed Markers |
Materials and Methods
Ethical Approval
The study was conducted in accordance with the principles of the Helsinki Declaration and approved by the Ethics Committee of the Medical University of Bialystok, Poland, no APK.002.19.2020. All participants gave informed written consent before they were enrolled in the study.
Samples Collection
The study group was composed of 60 patients with psoriasis vulgaris, plaque subtype, diagnosed by a dermatologist, whereas the control group consisted of 30 volunteers without dermatoses, who claimed a negative family history of psoriasis, matched with the study group by sex, age, and body mass index (BMI). All subjects denied a history of any kidney function disorders. They all were of the same ethnicity (Caucasian) and came from a similar geographical area. Individuals who were under the age of 18 years, pregnant, breastfeeding, who had other variants of psoriasis, malignant neoplasms, diabetes mellitus, arterial hypertension, and who received systemic antipsoriatic drugs or other agents of recognized nephrotoxic potential for 3 months prior to enrollment, were excluded from the experiment. Only a few subjects used to take diuretics ad hoc. Other patients did not take any drugs that could influence kidney function. The Psoriasis Activity and Severity Index (PASI) was used to assess the skin lesions’ severity; every patient was evaluated by the same doctor. At the beginning of the study, participants’ fasting venous blood samples and first morning mid-stream urine samples were collected. Blood was centrifuged for 15 minutes at 1000g to obtain serum. Urine was centrifuged for 10 minutes at 2000g. The biological material was stored at −80°C until tested. Biomarkers of glomeruli and tubular function were analyzed in serum or urine by the enzyme-linked immunosorbent assay (ELISA) every time by the same person in the same laboratory. The following molecules were analyzed in serum using the kits provided by the CloudClone®: creatinine (CEV806Ge), cystatin C (SEA896Hu), beta-trace protein (SEA724Hu), albumins (CEB028Hu), and uromodulin (SEG918Hu). The analyzed urinary biomarkers included albumins, nephrin (AEA937Hu), creatinine, cystatin C, alpha-1-microglobulin (SEA217Hu), beta-2-microglobulin (SEA260Hu), uromodulin, klotho (SEH757Hu), and fatty acid-binding protein 1 (SEB566Hu).
First, we examined the GFR classically with the creatinine concentration using the Cockcroft-Gault formula, subsequently, we presented the data on less commonly used glomerular function markers. In the Cockroft-Gault formula, the following parameters are taken into consideration: sex, age, creatinine concentration, and weight. It provides a better insight into subjects who take medications whose dosing depends on kidney function. However, it is not recommended in children, patients with abnormal (too low or too high) muscle mass, or in pregnant women.29
Patients were divided into subgroups based on several clinical parameters, including psoriasis severity, sex, and disease duration. Mild psoriasis was defined as PASI<10 (PASI I), moderate – PASI 10–20 (PASI II), severe psoriasis – PASI>20 (PASI III). Short-lasting psoriasis was defined as less than 15 years, long-lasting as longer than 15 years. Correlations between the concentrations of all markers and the aforementioned clinical parameters.
Statistical Analysis
The data following a normal distribution were expressed as the mean ± standard deviation (SD) and evaluated through one-way analysis of variance (ANOVA). Tukey’s HSD test was applied to determine the significance between specific groups. Non-normally distributed data were presented as the median (range) and analyzed using the non-parametric Kruskal–Wallis test. Comparisons between patients with psoriasis and the control group were performed with either the Student’s t-test or the non-parametric Mann–Whitney test. Correlations between the studied parameters were assessed using Spearman’s rank correlation test. Statistical significance was defined as a p-value below 0.05. All analyses were conducted using GraphPad Prism version 9.4 (LaJolla, California, USA).
Results
60 patients with psoriasis and 30 controls were compared. There was no statistically significant difference between patients and controls in terms of age, gender, or BMI (Table 2). The table also shows the median concentrations of markers (Table 2).
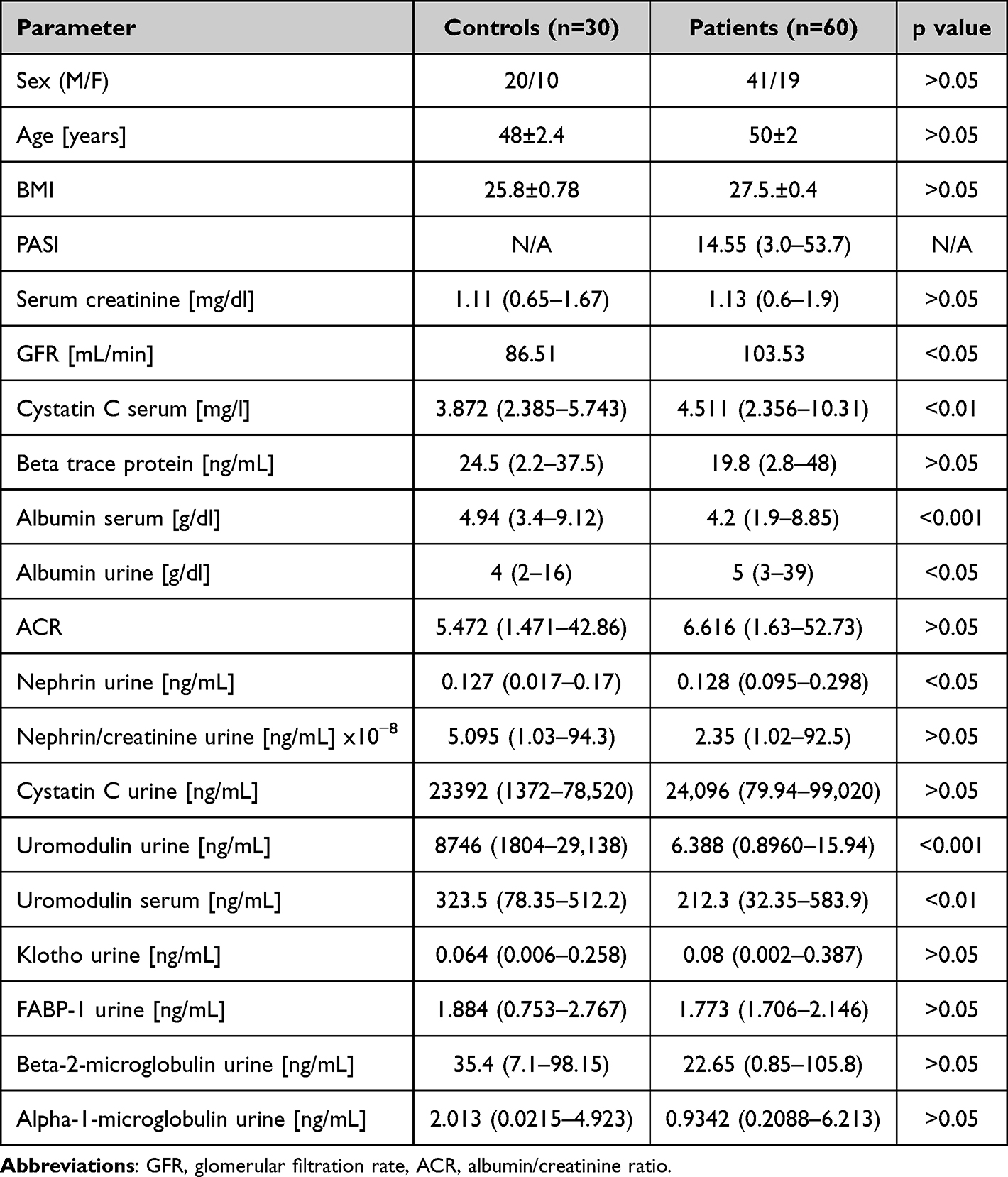 |
Table 2 Basic Characteristics of Patients and Controls |
Albumin
Patients with psoriasis had significantly lower serum concentration of albumins (p<0.001) and significantly higher urinary concentration of albumins (p<0.05) compared to controls (Figure 1A and B). Albumin to creatinine ratio (ACR) was higher, although statistically insignificantly, among patients (Figure 1C). Nevertheless, according to the usual normal limits used (3.5–5 g/dl for serum albumin, <30 mg/g for ACR), both patients and controls had normal median serum albumins and ACR. We did not find any correlations between serum or urinary albumin and psoriasis severity or duration (Figure 1D).
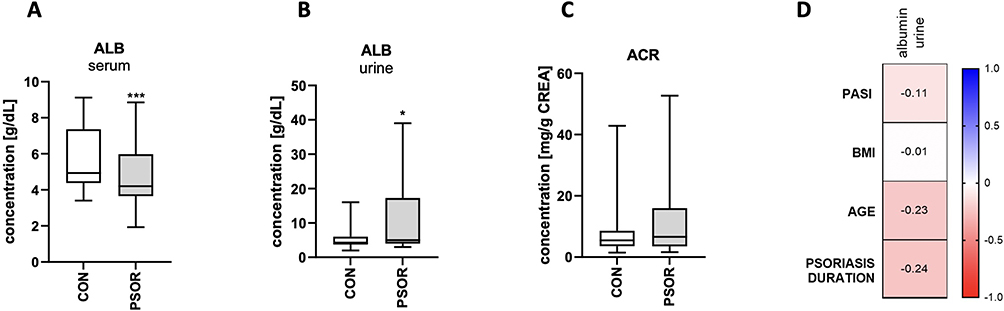 |
Figure 1 Albumins concentration in patients compared to controls in serum (A), and urine (B); albumin to creatinine ratio – ACR in patients compared to controls (C); correlations between urinary albumins and clinical demographic parameters (D). */*** means a statistically significant difference between patients and controls with p<0.05/0.001. |
Cystatin C
Median serum Cys-C concentration was significantly higher in patients compared to controls (p<0.01) (Figure 2a). According to the normal limits of serum Cys-C (0.53–0.95 mg/l), both patients and controls had increased Cys-C concentration. The higher the psoriasis severity in PASI, the higher serum Cys-C concentration, however there were no clear significant differences between the groups (Figure 2b). In patients who have suffered from psoriasis for more than 15 years, the median serum Cys-C concentration was higher, although statistically insignificantly, than in patients with a shorter history of psoriasis (Figure 2c). Based on Spearman correlations, there was no direct correlation between Cys-C concentration and age, BMI, psoriasis severity or duration (Figure 2d).
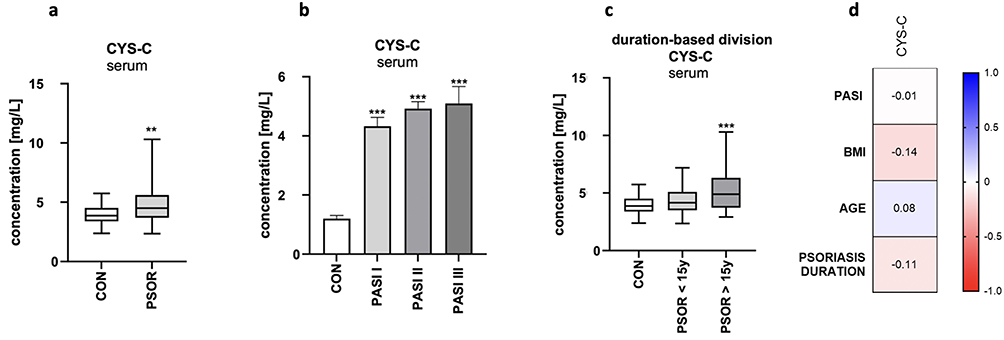 |
Figure 2 Cystatin C concentration in serum of patients compared to controls (a), based on PASI division (b) and based on duration division (c); correlations between serum cystatin C and clinical and demographic parameters (d). **/*** means a statistically significant difference between patients and controls with p<0.01/0.001. |
Beta-Trace Protein
There was no statistically significant difference in median BTP serum concentration between patients and controls (Figure 3a, p>0.05). Taking into account the normal range of BTP in serum (0.37–0.7 mg/l), both patients and controls had decreased median BTP concentration. Moreover, there was no statistically significant difference in BTP serum concentration after the division of patients based on psoriasis severity or duration (Figure 3b and c; p>0.05). There was also no direct correlation between BTP concentration and age, BMI, psoriasis severity, or duration (Figure 3d).
 |
Figure 3 Beta-trace protein concentration in serum of patients compared to controls (a), based on PASI division (b) and based on duration division (c); correlations between serum beta-trace protein and clinical and demographic parameters (d). |
Nephrin
The median absolute urinary concentration of nephrin was significantly higher in patients than in controls (p<0.05, Figure 4a), but to obtain objectivity of the assessment, we also counted the urinary nephrin to creatinine ratio, which was similar in both groups (p>0.05)(Figure 4b). There was no statistically significant difference between particular psoriasis severity subgroups (Figure 4c), as well as no correlation between clinical parameters and demographic (Figure 4d and e).
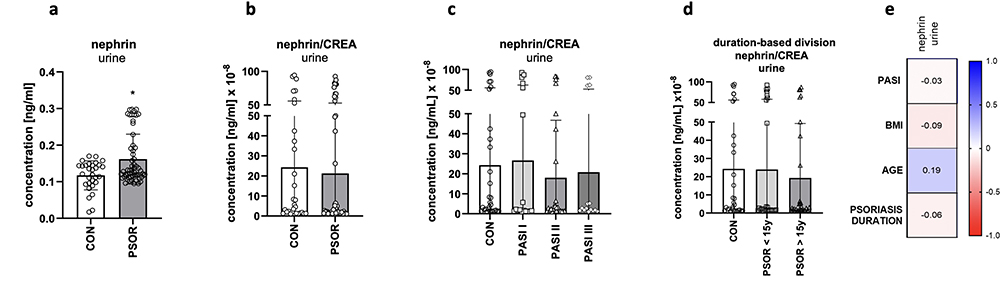 |
Figure 4 Nephrin urinary concentration in patients compared to controls: absolute (a), nephrin to urinary creatinine ratio (b), based on PASI division (c), and based on duration division (d); correlations between urinary nephrin and clinical and demographic parameters (e). * means a statistically significant difference between patients and controls with p<0.05. |
Urinary Cystatin C
Urinary Cys-C concentration was insignificantly different between patients and controls (p>0.05, Figure 5a). After the division of patients into subgroups according to PASI, there were no statistically significant differences in Cys-C concentrations in each subgroup (Figure 5b), nor when patients were divided into subgroups who suffered from psoriasis more or less than 15 years (data not shown). We found no significant correlations between urinary Cys-C concentration and clinical parameters (Figure 5c).
 |
Figure 5 Urinary cystatin C and FABP1 concentrations: (a and d) - absolute concentration in patients compared to controls, (b and e) - concentrations after the division of patients into subgroups according to PASI, (c and f) – correlations between markers’ concentration and several clinical and demographic parameters. |
Fatty Acid-Binding Protein 1
FABP1 urinary concentration was insignificantly different between patients and controls (p>0.05, Figure 5d). After the division of patients into subgroups according to PASI, there were no differences in FABP1 concentrations (Figure 5e), neither when patients were divided into subgroups who suffered from psoriasis more or less than 15 years (data not shown). We found no significant correlations between urinary FABP1 concentration and clinical or demographic parameters (Figure 5f).
Serum and Urinary Uromodulin
Serum uromodulin concentration was significantly lower in patients than in controls (p<0.01, Figure 6a), similar to urinary concentration (p<0.001, Figure 6d). After the division of patients into subgroups according to PASI, there were no significant differences in serum or urinary uromodulin concentrations between each subgroup (Figure 6b and e), neither when patients were divided into subgroups who suffered from psoriasis more or less than 15 years (data not shown). We found no significant correlations between urinary or serum uromodulin concentration and clinical or demographic parameters (Figure 6c and f).
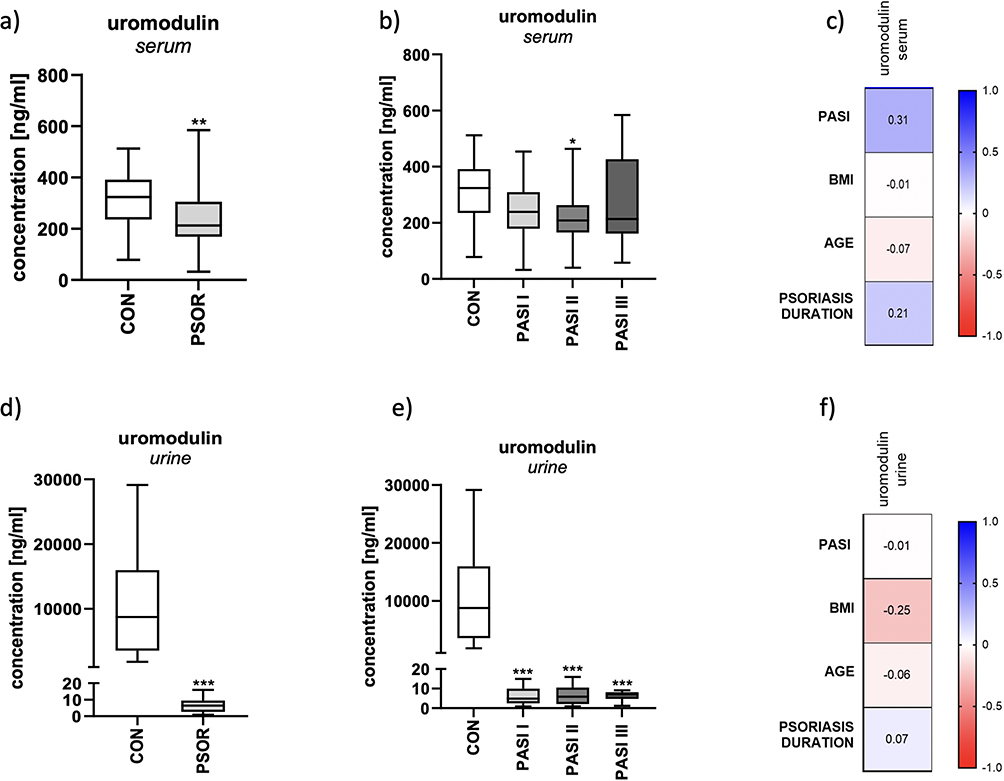 |
Figure 6 Serum (a-c) and urinary (d-f) uromodulin concentrations in patients compared to controls: (a and d) - absolute concentration in patients compared to controls, (b and e) - concentrations after the division of patients into subgroups according to PASI, (c and f) – correlations between markers’ concentration and several clinical and demographic parameters. */**/*** means statistically significant difference with p<0.05/0.01/0.001, respectively. |
Alpha-1-Microglobulin
A1M urinary concentration was insignificantly different between patients and controls (p>0.05, Figure 7a). After the division of patients into subgroups according to PASI, there were no differences in A1M concentrations (Figure 7b), neither when patients were divided into subgroups who suffered from psoriasis more or less than 15 years (data not shown). We found no significant correlations between A1M concentration and clinical parameters (Figure 7c).
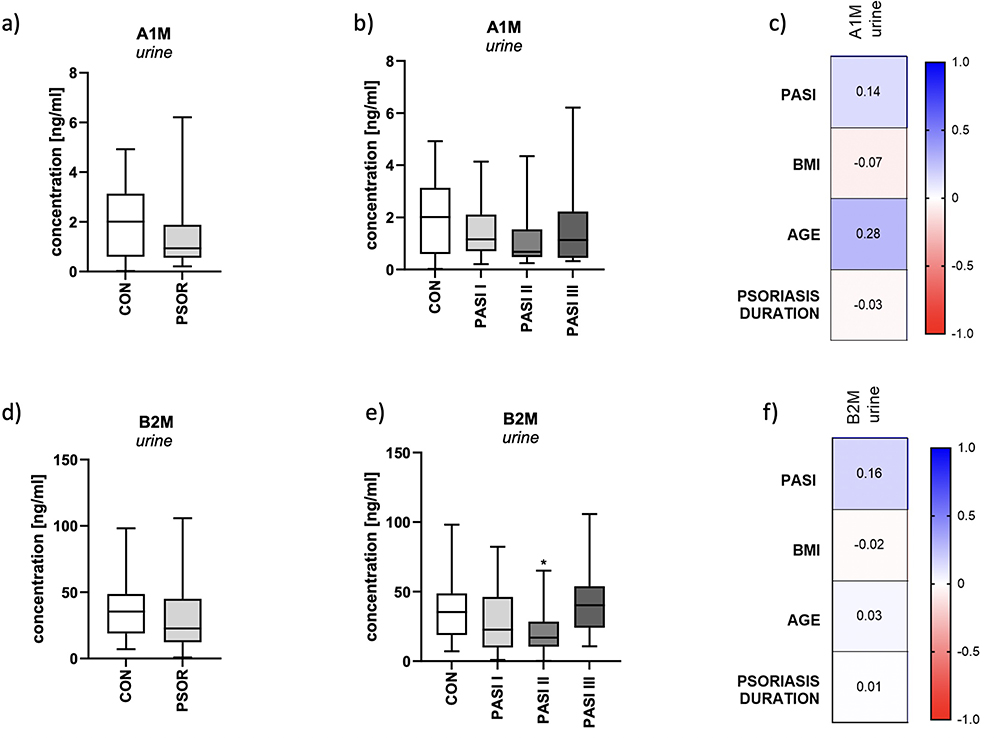 |
Figure 7 Urinary alpha-1-microglobulin (a-c) and beta-2-microglobulin (d-f) concentration: (a and d) - absolute concentration in patients compared to controls, (b and e) - concentrations after the division of patients into subgroups according to PASI, (c and f) – correlations between markers’ concentration and several clinical and demographic parameters. * means a statistically significant difference between patients and controls with p<0.05. |
Beta-2-Microglobulin
B2M urinary concentration was insignificantly different between patients and controls (p>0.05, Figure 7d). After the division of patients into subgroups according to PASI, there were no significant differences in B2M concentrations between the subgroups (Figure 7e), neither when patients were divided into subgroups who suffered from psoriasis more or less than 15 years (data not shown). We found no significant correlations between urinary B2M concentration and clinical and demographic parameters (Figure 7f).
Klotho
Klotho urinary concentration was insignificantly different between patients and controls (p>0.05, Figure 8a). After the division of patients into subgroups according to PASI, there were no significant differences in klotho concentrations between the subgroups (Figure 8b), neither when patients were divided into subgroups who suffered from psoriasis more or less than 15 years (data not shown). We found no significant correlations between urinary klotho concentration and clinical or demographic parameters (Figure 8c).
 |
Figure 8 Urinary klotho concentration: a - absolute concentration in patients compared to controls, b - concentrations after the division of patients into subgroups according to PASI, c – correlations between markers’ concentration and several clinical and demographic parameters. |
All the investigated markers have also not been associated with patients’ sex (p>0.05).
Discussion
We aimed to assess the glomerular filtration and tubular function in patients with psoriasis and managed to find that patients with psoriasis had significantly different results regarding the glomerular function compared to the controls, nevertheless, in some instances, markers’ concentrations remained within normal limits adjusted to our population and geographical location. We also studied seven markers of tubular function and, to the best of our knowledge, we were the first to analyze all of them in serum and urine in this specific group of patients. Based on the presented results, psoriasis itself does not seem to promote renal tubular dysfunction more frequently compared to subjects without dermatoses.
The association between kidney disease and psoriasis still remains uncertain and studies bring inconsistent results.30,31 The difficulty in the discussion of our findings in comparison with others is that not enough studies focus on particular laboratory abnormalities, presenting only the incidence or risk of chronic kidney disease instead.30,31 As for the reports on particular markers, probably the most investigated marker of glomeruli function among psoriasis is creatinine, but there are also reports about albuminuria. The results of available studies are somewhat contradictory. In several experiments, there were no major differences between patients with psoriasis and controls that could indicate kidney impairment independently of the comorbidities.32–34 In several other studies, if any abnormality was found, it was microalbuminuria.35–37
In this experiment, we used recognized, as well as less commonly used markers of glomerular filtration, in order to see if patients with psoriasis are at risk of glomerular dysfunction.
In our study, the serum creatinine concentration was within normal limits, both in patients, and controls, and did not differ significantly between the groups. Moreover, the GFR counted based on serum creatinine concentration was even higher in patients than controls – contrary to the creatinine levels. Cassano et al found significantly higher serum creatinine concentration in patients than in controls but without difference when it came to GFR; moreover, both in patients and controls, these concentrations were still within normal limits.31 Nevertheless, scientists and doctors underline that creatinine clearance is not a perfect tool for GFR assessment due to many variables influencing its concentration. The choice of a particular substance and algorithm for calculations may explain these discrepancies then. This is why newer markers have been suggested however, their use in daily clinical practice is limited due to financial reasons.
Another GFR marker, which is considered more reliable and not confounded by many factors, namely Cys-C, was elevated both in patients and controls, but significantly higher in patients compared to controls, which could indicate more probable glomerular dysfunction in patients with psoriasis. However the concentrations of Cys-C tended to be higher in more severe psoriasis and longer duration of the disease, there were no significant differences between the subgroups to draw clear conclusions. Cys-C had been assessed in patients with psoriasis earlier but only in one study and in terms of the atherosclerosis risk, not the glomerular filtration. Its concentration was higher in patients than controls.38 Nevertheless, atherosclerosis is associated with diabetes mellitus and arterial hypertension, which are obviously risk factors for kidney damage.
Another molecule suggested as GFR marker is BTP. In our study, there was no statistically significant difference between patients and controls in terms of its concentration, also with regard to psoriasis severity. To the best of our knowledge, BTP had never been assessed in the serum of patients with psoriasis before, so we have no data for comparison.
We also investigated the albumins in serum, as well as in urine. We observed normal serum albumin concentration, however much lower in patients with psoriasis. Patients had also higher albuminuria but ACR was within normal limits. In the study by Kaftan et al skin lesions severity and dissemination were associated with microalbuminuria,32 however we did not share this finding. Three other studies documented increased albuminuria in patients with psoriasis than controls.35–37 On the other hand, Cassano et al did not notice significantly higher urinary albumin excretion in patients.34
The last glomerular function marker that we analyzed was nephrin. Inflammatory cytokines (whose concentration is known to be increased in psoriasis) have been found to induce podocyte injury,14 so it seems probable that the podocyte membrane in psoriatic subjects could be compromised. Although in our experiment the absolute urinary concentration of nephrin was significantly higher in patients than in controls, when calculated per urinary creatinine, it was not significantly different. Nephrin was also not associated with psoriasis severity or duration Based on our results, the integrity of the podocyte membrane in patients with psoriasis seems to be intact. We are not aware of any other reports of nephrin assessed in the group of patients with psoriasis, however Ren et al conducted an experiment on mice with induced psoriasis and studied another podocyte marker – podocin. Its expression was decreased in glomeruli after the induction of psoriasis.14
Uromodulin plays a multifaceted role in kidney health and disease. Besides renal disease, it is involved in urinary tract defense, blood pressure regulation, and salt handling.39,40 Its levels reflect kidney function and tubular integrity, and it has potential as an early marker for kidney injury in both kidney diseases and systemic inflammatory conditions. Uromodulin has never been studied in patients with psoriasis before, neither in serum nor in urine. In our experiment, we noticed significantly lower uromodulin concentration in both fluids, which may indicate a decreased nephron number. Psoriasis severity or duration did not affect uromodulin concentration, hence not the alleged tubular dysfunction.
Albeit there were significant differences in uromodulin concentrations between patients and controls, all other investigated markers indicate otherwise – no influence of psoriasis on tubular function. Hence, this matter requires future investigations. Decreased concentrations of uromodulin could also be potentially affected by the salt and protein intake or levels of antidiuretic hormone.25 Moreover, the fact that urinary excretion of uromodulin is known to fluctuate and be highly variable between subjects,25 makes the results difficult to interpret.
Cys-C concentration in serum is considered a reliable marker of GFR, and in urine – a marker of tubular injury.17,23 Besides, Cys-C has been studied in metabolic disorders, such as diabetes mellitus, obesity, or NAFLD,41–43 and in the field of oncology and neurodegenerative disorders.44,45 In our study, we did not notice any significant differences in urinary Cys-C concentration between patients with psoriasis and controls, also with regard to clinical and demographic parameters.
FABP-1 plays a significant role in lipid metabolism, cellular signaling, and the regulation of energy homeostasis. It has been implicated in a variety of diseases, including metabolic disorders (such as NAFLD and insulin resistance), cardiovascular diseases, renal dysfunction, and inflammatory diseases.46,47 FABP-1 has never been studied in psoriatic urine, but it had been analyzed earlier in psoriatic sera by the members of our team. Its serum concentration was significantly elevated compared to subjects without dermatoses, however there was no correlation with PASI.48 Increased serum FABP-1 in patients with psoriasis has been linked rather with metabolic syndrome, however we must take into account that patients suffering from its components (especially diabetes mellitus and arterial hypertension) are at risk of renal complications. In this experiment, there were no significant differences in urinary FABP-1 concentrations between patients with psoriasis and controls.
A1M is used as a biomarker in the field of renal, cardiovascular, autoimmune, and oncologic diseases. Besides kidney dysfunction, it has been explored as a marker for cancer progression and cardiovascular diseases.49,50 Currently, there appears to be limited or no direct research specifically connecting urinary A1M to psoriasis. A1M has never been directly studied in this dermatosis however, A1M gene has been documented to be upregulated in the non-lesional skin of such patients, hence thought to be associated with apoptosis and decreased proliferation51, but no reflections with regards to kidney impairment were made. In our experiment, there were no significant differences in A1M concentrations in urine between patients with psoriasis and controls, nor correlations with clinical parameters, such as psoriasis severity or duration, and demographics.
B2M is a versatile biomarker with roles in kidney disease, hematologic malignancies, inflammatory conditions, infections, and neurological diseases.52–56 Its levels are often reflective of disease activity, immune system activation, and organ dysfunction. Elevated B2M levels can provide important insights into disease prognosis, particularly in renal diseases, autoimmune disorders, and certain cancers. It is especially valuable in monitoring chronic kidney disease, dialysis-related amyloidosis,57 multiple myeloma,53 and HIV infection.55 B2M has already been studied in patients with psoriasis, but only in the blood.58 Its concentration was higher among patients with more severe psoriasis (PASI>10) and correlated with this index.58 We did not observe an analogous finding in psoriatic patients’ urine, since there were no significant differences in B2M concentrations in urine between patients and controls, nor a correlation with psoriasis characteristics. However classic markers, both A1M and B2M may be considered to underestimate tubular dysfunction.22
Klotho is a multifunctional protein that plays a vital role not only in kidney function but also in cardiovascular diseases, metabolic regulation, and aging.59–61 Similar to all above-mentioned markers, klotho has never been analyzed in psoriatics as well, except for one study in which immunohistochemical staining showed β-klotho to be highly expressed in the macrophages infiltrating the dermis of psoriatic plaques,62 and no references to kidney functions were made.
The absence of a correlation between psoriasis severity and all analyzed markers suggests that systemic inflammation associated with psoriasis may not have a significant impact on renal function. This could imply that, while psoriasis is a chronic inflammatory disease, it does not necessarily cause or exacerbate renal damage, at least not in a measurable way by the markers that are commonly used in this indication.
Scientists underline the need for a kidney biopsy to get insight into the origin of kidney dysfunction however it is very difficult to conduct in a real-life setting. Nevertheless, in one study, a few subjects underwent a kidney biopsy, which revealed mesangioproliferative glomerulonephritis with IgA nephropathy, focal proliferative glomerulonephritis, or membranous glomerulonephropathy in the majority of cases.63
The matter of early screening for kidney disorders is not that common in daily dermatological practice. However, there are some existing guidelines that cover this area, for instance, the ones created by the National Psoriasis Foundation and the American Academy of Dermatology. They advise on the assessment of serum creatinine, urea, and albuminuria in psoriatic patients.2 However, in patients who are especially treated with methotrexate and cyclosporin A, it is advised to measure the creatinine concentration and perform urinalysis before the treatment and during the therapy, at the beginning usually every month, then every one or two months. The guidelines on these examinations in patients treated with biologics differ between the drugs and countries.64 In our opinion, simple measures, such as creatinine concentration and urinalysis, are feasible to perform in routine dermatological practice, for instance, once a year in individuals with yet unrecognized disease. The cost-effectiveness of several kidney disorders has been studied, especially chronic kidney disease, considering that such diseases are associated with high morbidity and mortality. Cost-effectiveness has been proven for subjects with diabetes mellitus and arterial hypertension, however the data regarding other specific groups of patients are conflicting since their prevalence and costs of screening have to be analyzed.65,66
To conclude, in our experiment, the majority of markers were significantly different between patients and controls, suggesting glomeruli dysfunction, but, at the same time, they were within normal limits. Hence, we cannot state at this moment that glomerular filtration disturbances are more prevalent in psoriatics. Similar observations were made by other scientists but still, we were probably the first to examine BTP, Cys-C and nephrin in patients with psoriasis, so further studies are needed to obtain deeper insight into this matter. We also did not find meaningful differences regarding the tubular function markers, which have been studied for the first time in patients with psoriasis.
In this paper, we excluded patients who suffer from diabetes mellitus and arterial hypertension, as well as those receiving systemic antipsoriatic drugs or analgesics, hence in real life, the number of patients with kidney complications could actually be higher.
The main limitation is the relatively low number of participants and the lack of kidney imaging tests. Moreover, in case of the tubular markers, a limitation of our considerations may be the fact that there are no reference values for these markers, which makes our observation somewhat difficult to interpret. It is also worth noting that normal limits for laboratory tests may vary between different geographical locations or racial groups.67 Another limitation could be that several patients used to take diuretics ad hoc.
Conclusions
Based on the measurement of several recognized and experimental glomerular and tubular function markers, patients with psoriasis do not seem to be at increased risk of kidney complications. However, we must take into account that patients who take nephrotoxic antipsoriatic drugs, and who suffer from common psoriatic comorbidities, namely diabetes mellitus and arterial hypertension, are usually not included in studies, whereas these factors can increase the risk of kidney damage. Therefore, caution must be taken, and perhaps it would be wise to screen psoriatic patients periodically, at least for serum creatinine, or perform urinalysis, even in those who do not receive systemic treatment. Close monitoring should be exercised in case of existing comorbidities because the actual number of psoriatic patients with renal complications may be higher in a real-life setting.
Ethics Statement
The study was conducted according to the Helsinki Declaration and received the approval of the Bioethics Committee, no APK.002.19.2020.
Acknowledgments
Manuscript preparation was supported during Harvard Medical School’s Polish Clinical Scholars Research Training Program, organised by the Agencja Badan Medycznych (ABM, English: Medical Research Agency, Warsaw, Poland).
Funding
The study was funded by the Medical University of Bialystok, no SUB/1/DN/20/001/1149.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Vanderpuye-Orgle J, Zhao Y, Lu J, et al. Evaluating the economic burden of psoriasis in the United States. J Am Acad Dermatol. 2015;72:961–7.e5. doi:10.1016/j.jaad.2015.02.1099
2. Elmets CA, Leonardi CL, Davis DMR, et al. Joint AAD-NPF guidelines of care for the management and treatment of psoriasis with awareness and attention to comorbidities. J Am Acad Dermatol. 2019;80:1073–1113. doi:10.1016/j.jaad.2018.11.058
3. Abuabara K, Azfar RS, Shin DB, Neimann AL, Troxel AB, Gelfand JM. Cause-specific mortality in patients with severe psoriasis: a population-based cohort study in the U.K. Br J Dermatol. 2010;163:586–592. doi:10.1111/j.1365-2133.2010.09941.x
4. Conti A, Giovannini L, Mandel VD, et al. Chronic kidney disease in psoriasis: a cohort study. J Dtsch Dermatol Ges. 2020;18(5):438–445.
5. Farmer CK, Stevens PE. Chronic kidney disease: psoriasis--a risk factor for chronic kidney disease? Nat Rev Nephrol. 2014;10(1):12–13. doi:10.1038/nrneph.2013.254
6. Cortvrindt C, Speeckaert R, Moerman A, Delanghe JR, Speeckaert MM. The role of interleukin-17A in the pathogenesis of kidney diseases. Pathology. 2017;49:247–258. doi:10.1016/j.pathol.2017.01.003
7. Blauvelt A, Chiricozzi A. The immunologic role of IL-17 in psoriasis and psoriatic arthritis pathogenesis. Clin Rev Allergy Immunol. 2018;55:379–390. doi:10.1007/s12016-018-8702-3
8. Furue K, Ito T, Tsuji G, Kadono T, Furue M. Psoriasis and the TNF/IL23/IL17 axis. G Ital Dermatol Venereol. 2019;154:418–424. doi:10.23736/S0392-0488.18.06202-8
9. Navarro JF, Mora-Fernández C. The role of TNF-alpha in diabetic nephropathy: pathogenic and therapeutic implications. Cytokine Growth Factor Rev. 2006;17:441–450. doi:10.1016/j.cytogfr.2006.09.011
10. Widemann BC, Adamson PC. Understanding and managing methotrexate nephrotoxicity. Oncologist. 2006;11:694–703. doi:10.1634/theoncologist.11-6-694
11. Yu J, Wei X, Gao J, Wang C, Wei W. Role of cyclosporin A in the treatment of kidney disease and nephrotoxicity. Toxicology. 2023;492:153544. doi:10.1016/j.tox.2023.153544
12. Visconti L, Leonardi G, Buemi M, et al. Kidney disease and psoriasis: novel evidences beyond old concepts. Clin Rheumatol. 2016;35:297–302. doi:10.1007/s10067-015-3126-4
13. Brown S. Measurement of Glomerular Filtration Rate (GFR). In: Imaging and Technology in Urology. Elsevier; 2023:205–208.
14. Ren F, Zhang M, Zhang C, Sang H. Psoriasis-like inflammation induced renal dysfunction through the TLR/NF-κB signal pathway. Biomed Res Int. 2020;2020:3535264. doi:10.1155/2020/3535264
15. White CA, Ghazan-Shahi S, Adams MA. β-trace protein: a marker of GFR and other biological pathways. Am J Kidney Dis. 2015;65:131–146. doi:10.1053/j.ajkd.2014.06.038
16. Gu X, Yang B. Methods for assessment of the glomerular filtration rate in laboratory animals. Kidney Dis. 2022;8:381–391. doi:10.1159/000525049
17. Lane B. Molecular markers of kidney injury. Urol Oncol. 2013;31:682–685. doi:10.1016/j.urolonc.2011.05.007
18. Onopiuk A, Tokarzewicz A, Gorodkiewicz E. Cystatin C: a kidney function biomarker. Adv Clin Chem. 2015;68:57–69.
19. Inker LA, Titan S. Measurement and estimation of GFR for use in clinical practice: core curriculum 2021. Am J Kidney Dis. 2021;78:736–749. doi:10.1053/j.ajkd.2021.04.016
20. Orenes-Piñero E, Manzano-Fernández S, López-Cuenca Á, Marín F, Valdés M, Januzzi JL. β-trace protein: from GFR marker to cardiovascular risk predictor. Clin J Am Soc Nephrol. 2013;8:873–881. doi:10.2215/CJN.08870812
21. Younes-Ibrahim MS, Younes-Ibrahim M. Biomarkers and kidney diseases: a brief narrative review. J Lab Precis Med. 2022;7:20. doi:10.21037/jlpm-22-1
22. Conti M, Moutereau S, Zater M, et al. Urinary cystatin C as a specific marker of tubular dysfunction. Clin Chem Lab Med. 2006;44(3):288–291. doi:10.1515/CCLM.2006.050
23. Zhang WR, Parikh CR. Biomarkers of acute and chronic kidney disease. Annu Rev Physiol. 2019;81:309–333. doi:10.1146/annurev-physiol-020518-114605
24. Rysz J, Gluba-Brzózka A, Franczyk B, Jabłonowski Z, Ciałkowska-Rysz A. Novel biomarkers in the diagnosis of chronic kidney disease and the prediction of its outcome. Int J Mol Sci. 2017;18(8):1702. doi:10.3390/ijms18081702
25. Thielemans R, Speeckaert R, Delrue C, De Bruyne S, Oyaert M, Speeckaert MM. Unveiling the hidden power of uromodulin: a promising potential biomarker for kidney diseases. Diagnostics. 2023;13(19):3077. doi:10.3390/diagnostics13193077
26. Zeng X, Hossain D, Bostwick DG, Herrera GA, Zhang PL. Urinary β2-microglobulin is a good indicator of proximal tubule injury: a correlative study with renal biopsies. J Biomark. 2014;2014:492838. doi:10.1155/2014/492838
27. Choromańska B, Myśliwiec P, Dadan J, Hady HR, Chabowski A. Znaczenie kliniczne białek wiążących kwasy tłuszczowe (FABPs) [The clinical significance of fatty acid binding proteins]. Postepy Hig Med Dosw. 2011;65:759–763. doi:10.5604/17322693.966983
28. Li H, Ouyang Y, Lv H, et al. Nanoparticle-mediated Klotho gene therapy prevents acute kidney injury to chronic kidney disease transition through regulating PPARα signaling in renal tubular epithelial cells. Biomaterials. 2024;315:122926. doi:10.1016/j.biomaterials.2024.122926
29. Millar JA. The Cockroft and Gault formula for estimation of creatinine clearance: a friendly deconstruction. N Z Med J. 2012;125(1350):119–122.
30. Wan J, Wang S, Haynes K, Denburg MR, Shin DB, Gelfand JM. Risk of moderate to advanced kidney disease in patients with psoriasis: population based cohort study. BMJ. 2013;347:f5961. doi:10.1136/bmj.f5961
31. Xu JR, Zheng DX, Ahn AB, et al. Psoriasis and chronic kidney disease among the United States adult population. J Am Acad Dermatol. 2023;89:834–837. doi:10.1016/j.jaad.2023.06.011
32. Kaftan O, Kaftan B, Toppare MF, Ekşioğlu M. Renal involvement in psoriasis. Dermatology. 1996;192:189–190. doi:10.1159/000246358
33. Tehranchinia Z, Ghanei E, Mohammadi N, Partovi-Kia M, Rahimi H, Mozafari N. No relation between psoriasis and renal abnormalities: a case-control study. Sci World J. 2018;2018:5301631. doi:10.1155/2018/5301631
34. Cassano N, Vestita M, Carbonara M, Panaro M, Vena GA. Renal function in psoriasis patients. Eur J Dermatol. 2011;21:264–265. doi:10.1684/ejd.2011.1274
35. Szepietowski JC, Bielicka E, Wasik F, Kopec W, Szepietowski T. Microalbuminuria as a subclinical marker of renal impairment in subjects with psoriasis vulgaris. J Eur Acad Dermatol Venereol. 2000;14:513–514. doi:10.1046/j.1468-3083.2000.00119.x
36. Dervisoglu E, Akturk AS, Yildiz K, Kiran R, Yilmaz A. The spectrum of renal abnormalities in patients with psoriasis. Int Urol Nephrol. 2012;44:509–514. doi:10.1007/s11255-011-9966-1
37. Cecchi R, Seghieri G, Gironi A, Tuci F, Giomi A. Relation between urinary albumin excretion and skin involvement in patients with psoriasis. Dermatology. 1992;185:93–95. doi:10.1159/000247420
38. Demirbaş A, Kurtipek GS, Tunçez A, Akyürek F, Demirbaş GU. The role of cystatin-C and fetuin-A in the determination of early atherosclerotic risk in psoriasis patients. Dermatol Ther. 2020;33:e13898. doi:10.1111/dth.13898
39. Ponte B, Pruijm M, Ackermann D, et al. Uromodulin, salt, and 24-hour blood pressure in the general population. Clin J Am Soc Nephrol. 2021;16(5):787–789. doi:10.2215/CJN.11230720
40. Garimella PS, Bartz TM, Ix JH, et al. Urinary uromodulin and risk of urinary tract infections: the cardiovascular health study. Am J Kidney Dis. 2017;69(6):744–751. doi:10.1053/j.ajkd.2016.08.022
41. Li S, Lu J, Gu G, et al. Serum creatinine-to-cystatin C ratio in the progression monitoring of non-alcoholic fatty liver disease. Front Physiol. 2021;12:664100. doi:10.3389/fphys.2021.664100
42. Xiong K, Zhang S, Zhong P, et al. Serum cystatin C for risk stratification of prediabetes and diabetes populations. Diabetes Metab Syndr. 2023;17(11):102882. doi:10.1016/j.dsx.2023.102882
43. Huo YX, Wei W, Liu Y, et al. Serum cystatin C levels are associated with obesity in adolescents aged 14-17 years. Front Endocrinol. 2022;13:816201. doi:10.3389/fendo.2022.816201
44. Leto G, Sepporta MV. The potential of cystatin C as a predictive biomarker in breast cancer. Expert Rev Anticancer Ther. 2020;20(12):1049–1056. doi:10.1080/14737140.2020.1829481
45. Chen X, Huang Y, Bao T, et al. Changes in serum cystatin C levels and the associations with cognitive function in alzheimer’s disease patients. Front Aging Neurosci. 2022;13:790939. doi:10.3389/fnagi.2021.790939
46. Zare-Feyzabadi R, Mozaffari M, Valizadeh M, Ghayour-Mobarhan M. FABP1 gene variant is associated with risk of metabolic syndrome. Comb Chem High Throughput Screen. 2022;25(8):1355–1360. doi:10.2174/1386207324666210603114434
47. Nowowiejska J, Baran A, Flisiak I. Fatty acid-binding proteins in psoriasis—A review. Metabolites. 2022;12:833. doi:10.3390/metabo12090833
48. Baran A, Kiluk P, Maciaszek M, Swiderska M, Flisiak I. Liver fatty acid-binding protein might be a predictive marker of clinical response to systemic treatment in psoriasis. Arch Dermatol Res. 2019;311:389–397. doi:10.1007/s00403-019-01917-w
49. Cui H, Zhang X, Ding X, et al. Urinary alpha1-microglobulin: a new predictor for in-hospital mortality in patients with ST-segment elevation myocardial infarction. Med Sci Monit. 2021;27:e927958. doi:10.12659/MSM.927958
50. Bellei E, Caramaschi S, Giannico GA, et al. Research of prostate cancer urinary diagnostic biomarkers by proteomics: the noteworthy influence of inflammation. Diagnostics. 2023;13(7):1318. doi:10.3390/diagnostics13071318
51. Itoh K, Kawasaki S, Kawamoto S, et al. Identification of differentially expressed genes in psoriasis using expression profiling approaches. Exp Dermatol. 2005;14(9):667–674. doi:10.1111/j.0906-6705.2005.00338.x
52. Argyropoulos CP, Chen SS, Ng YH, et al. Rediscovering beta-2 microglobulin as a biomarker across the spectrum of kidney diseases. Front Med. 2017;4:73.
53. Wang SY, Qiu DB, Fan CH. Correlation between serum Interleukin-33, β2-microglobulin levels and DS stage in patients with multiple myeloma. Zhongguo Shi Yan Xue Ye Xue Za Zhi. 2023;31(3):788–793. doi:10.19746/j.cnki.issn.1009-2137.2023.03.025
54. Sheng Z, Wang L, Chen M, et al. Cerebrospinal fluid β2-microglobulin promotes the tau pathology through microglia-astrocyte communication in Alzheimer’s disease. Alzheimers Res Ther. 2025;17(1):2. doi:10.1186/s13195-024-01665-8
55. Olaniyi JA, Emeka GJ, Onifade AA, Adeyanju AO, Rahamon SK. Changes in haematological parameters and serum beta-2-micro-globulin levels in CD4+ T-cells-stratified Nigerian HIV patients. Eur J Clin Exp Med. 2021;19(1):33–39. doi:10.15584/ejcem.2021.1.5
56. Dinçer A, Torgutalp M, Yayla ME, et al. Serum levels of Beta-2 microglobulin in rheumatoid arthritis patients and its relationship with disease activity: can it be used as a disease activity marker? Aktuelle Rheumatologie. 2020;46:297–304.
57. Zumrutdal A. Role of β2-microglobulin in uremic patients may be greater than originally suspected. World J Nephrol. 2015;4(1):98–104. doi:10.5527/wjn.v4.i1.98
58. Han L, Gan Y, Du J, et al. Evaluation of β2-microglobulin in the condition and prognosis of psoriasis patients. J DermatolTreat. 2024;35(1):2377665. doi:10.1080/09546634.2024.2377665
59. Prud’homme GJ, Wang Q. Anti-inflammatory role of the klotho protein and relevance to aging. Cells. 2024;13(17):1413. doi:10.3390/cells13171413
60. Lanzani C, Citterio L, Vezzoli G. Klotho: a link between cardiovascular and non-cardiovascular mortality. Clin Kidney J. 2020;13(6):926–932. doi:10.1093/ckj/sfaa100
61. Kawai M. The FGF23/Klotho axis in the regulation of mineral and metabolic homeostasis. Horm Mol Biol Clin Investig. 2016;28(1):55–67. doi:10.1515/hmbci-2015-0068
62. Nakai K, Haba R, Kushida Y, Kubota Y. Macrophages express βKlotho in skin lesions of psoriatic patients and the skin of imiquimod-treated mice. J Dermatol. 2018;45(12):1475–1477. doi:10.1111/1346-8138.14671
63. Singh NP, Prakash A, Kubba S, et al. Psoriatic nephropathy-does an entity exist? Ren Fail. 2005;27:123–127.
64. Nast A, Smith C, Spuls PI, et al. EuroGuiDerm Guideline on the systemic treatment of Psoriasis vulgaris - Part 1: treatment and monitoring recommendations. J Eur Acad Dermatol Venereol. 2020;34(11):2461–2498. doi:10.1111/jdv.16915
65. Yeo SC, Wang H, Ang YG, Lim CK, Ooi XY. Cost-effectiveness of screening for chronic kidney disease in the general adult population: a systematic review. Clin Kidney J. 2023;17(1):sfad137. doi:10.1093/ckj/sfad137
66. Rokhman MR, Alkaff FF, van Dorst PWM, et al. Economic evaluations of screening programs for chronic kidney disease: a systematic review. Value Health. 2024;27(1):117–128. doi:10.1016/j.jval.2023.08.003
67. Price MA, Fast PE, Mshai M, et al. Region-specific laboratory reference intervals are important: a systematic review of the data from Africa. PLOS Glob Public Health. 2022;2(11):e0000783. doi:10.1371/journal.pgph.0000783
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.