Back to Journals » Infection and Drug Resistance » Volume 19
Pseudomonas oryzihabitans: An Emerging Opportunistic Pathogen Causing Severe Burn Wound Infection After Improper Moxibustion Patch Use in an Elderly Diabetic Farmer
Authors Wang R, Yu J, Guan Y, Xu X, Cai X ![]()
Received 23 March 2026
Accepted for publication 27 May 2026
Published 3 June 2026 Volume 2026:19 611045
DOI https://doi.org/10.2147/IDR.S611045
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hemant Joshi
Ruofan Wang,1 Jiongbiao Yu,1 Yubin Guan,1 Xiaosong Xu,1 Xiangsheng Cai2
1Clinical Laboratory, The First Affiliated Hospital of Guangdong Pharmaceutical University, Guangzhou, People’s Republic of China; 2Clinical Laboratory, Guangzhou Eleventh People’s Hospital, Guangzhou Cadre and Talent Health Management Center, Guangzhou, People’s Republic of China
Correspondence: Xiangsheng Cai, Email [email protected]
Background: Pseudomonas oryzihabitans, a Gram-negative opportunistic pathogen, is associated with infected burn wounds in elderly patients with underlying diseases. Moxibustion patch-related deep burns in farmers (due to occupational exposure) often have nonspecific manifestations, causing diagnostic delays. This case highlights the synergistic role of microbiologically guided antimicrobial therapy and surgical intervention.
Case Summary: A 71-year-old female farmer with type 2 diabetes and bilateral lower extremity arteriosclerotic occlusive disease developed left lower leg third-degree burn due to improper moxibustion patch use; wound infection occurred after self-treatment. Wound secretion culture confirmed Pseudomonas oryzihabitans (colony count ≥ 106 CFU/mL) sensitive to cefoperazone-sulbactam. She received microbiologically guided antimicrobial therapy combined with surgical debridement, negative pressure wound therapy (NPWT), and elective split-thickness skin grafting. Postoperatively, infection indicators decreased significantly, the wound healed well, and no recurrence or complications were observed.
Conclusion: Elderly patients with underlying diseases are at high risk of such burns and infections. The synergistic application of microbiologically precise antimicrobial therapy and surgical intervention is key to improving efficacy and reducing recurrence.
Keywords: moxibustion patch, third-degree burn, Pseudomonas oryzihabitans, antimicrobial therapy, surgical debridement, negative pressure wound therapy, NPWT
Introduction
As a convenient modified form of traditional Chinese medicine (TCM) thermotherapy, moxibustion patches are widely used for home-based management of chronic pain due to their ease of operation and low cost.1 However, elderly populations, especially farmers with underlying diseases such as diabetes mellitus and vascular disorders, are at high risk of deep burns from improper use. This is attributed to reduced skin sensation, microcirculatory disturbance, impaired tissue healing capacity, insufficient medical knowledge and weak self-protection awareness.2 Burn wounds are susceptible to opportunistic infections, among which Pseudomonas oryzihabitans, a Gram-negative opportunistic pathogen widely distributed in soil, water and other farm environments, poses a significantly higher infection risk to farmers due to occupational exposure.3 The clinical manifestations of Pseudomonas oryzihabitans infection are non-specific, leading to easily delayed diagnosis and treatment, and the presence of underlying diseases further complicates the condition.4 Currently, reports on moxibustion patch-induced burns complicated with Pseudomonas oryzihabitans infection remain scarce.5 The synergistic strategy of microbiological diagnosis‑guided precise antibiotics plus staged surgical repair has been rarely summarized. This article reports a typical case and provides evidence‑based references for clinical diagnosis and treatment.
Case Presentation
History
A 71-year-old female farmer, with a history of long-term farm work, was admitted to the hospital by wheelchair due to “redness, swelling and ulceration of the left lower leg caused by moxibustion patch scald for more than half a month”. Past medical history: type 2 diabetes mellitus for more than 20 years, with a maximum blood glucose of 18 mmol/L, treated with subcutaneous injection of insulin aspart 15 U before three meals + insulin glargine 16 U at bedtime; hypertension, maximum blood pressure of 180 mmHg, regularly taking amlodipine besylate tablets 5 mg qd; hyperlipidemia, treated with clopidogrel bisulfate tablets 75 mg qd and atorvastatin calcium tablets 20 mg qn.
Clinical Findings
Physical examination on admission: body temperature 36.3°C, respiratory rate 19 breaths/min, pulse 78 beats/min, blood pressure 120/69 mmHg. The patient was conscious, with moderate nutrition, admitted by wheelchair. The middle and lower segments of the right thigh were absent; three wounds were observed on the lower 1/2 of the left lower leg: anterior wound 5.5 cm × 5.0 cm, base completely covered with black eschar, with a small amount of yellow purulent secretion at the edge, surrounding skin erythematous and warm; lateral wound 10.0 cm × 5.5 cm, base completely covered with black eschar, surrounding skin erythematous and warm; medial wound 8.0 cm × 4.5 cm, base with 50% black eschar, 25% yellow tissue and 25% red tissue, partial shedding of yellow eschar, surrounding skin erythematous and warm; no fluctuation was felt on palpation of the three wounds. Muscle strength of extremities was grade V, tendon reflexes were normal, and pathological reflexes were negative.
Laboratory and Imaging Examinations
Laboratory examinations: Emergency electrolyte test: potassium 2.92 mmol/L, calcium 2.07 mmol/L; infection markers: serum amyloid A 108.91 mg/L, C-reactive protein 19.9 mg/L; fasting blood glucose 6.9 mmol/L on the next day after admission. Bacterial culture of wound secretions (24-hour blood agar plate) showed Gram-negative bacilli (Figure 1), and identification by VITEK MS MALDI-TOF mass spectrometry confirmed Pseudomonas oryzihabitans (colony count ≥106 CFU/mL) (Figure 2); drug sensitivity test showed sensitivity to multiple antibiotics including cefoperazone-sulbactam, piperacillin-tazobactam and imipenem (Table 1). Imaging examinations: Chest X-ray and electrocardiogram showed no obvious abnormalities, and no surgical contraindications were found.
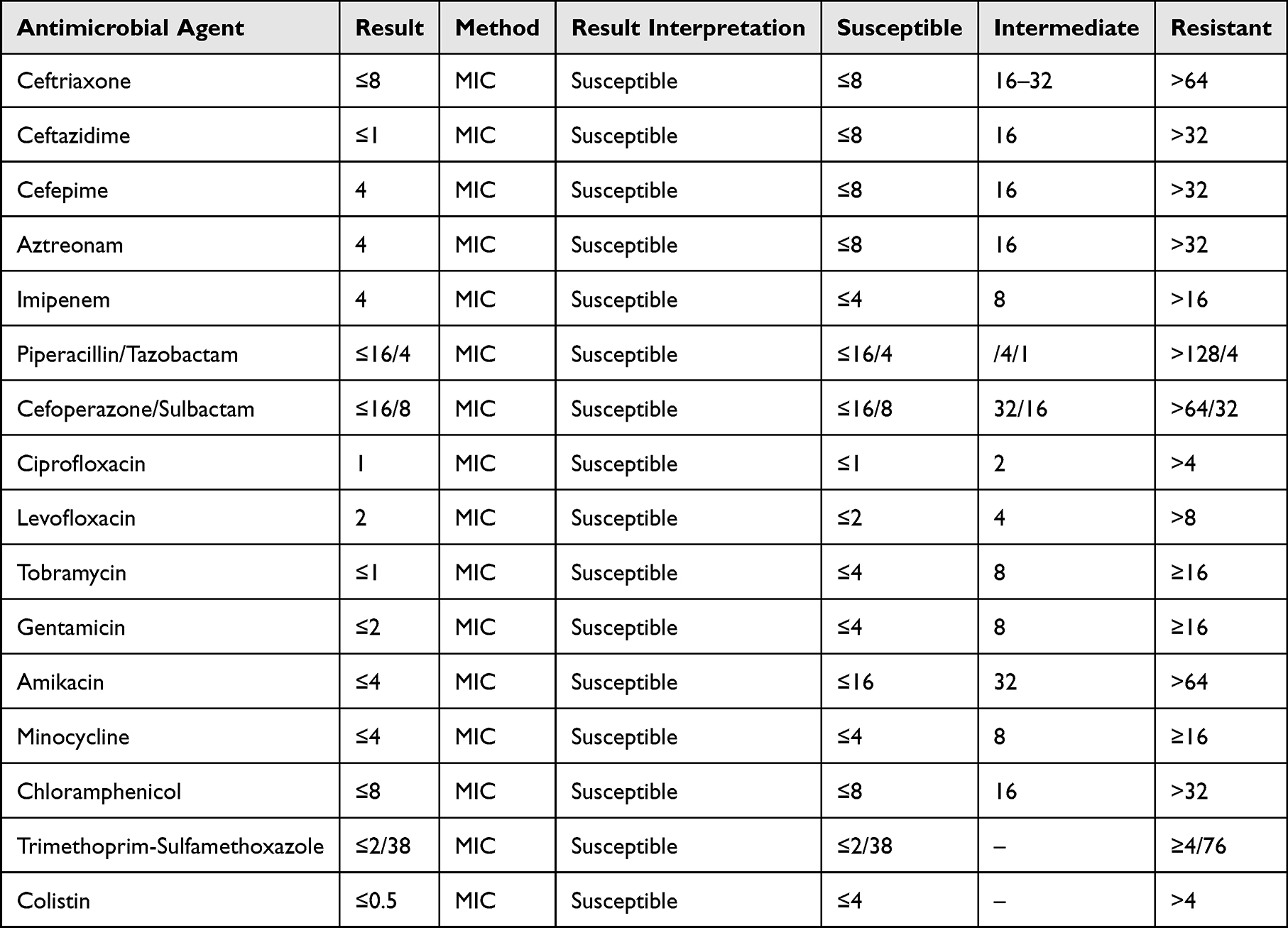 |
Table 1 Antimicrobial Susceptibility Test Results of Pseudomonas oryzihabitans (VITEK 2 Compact System) |
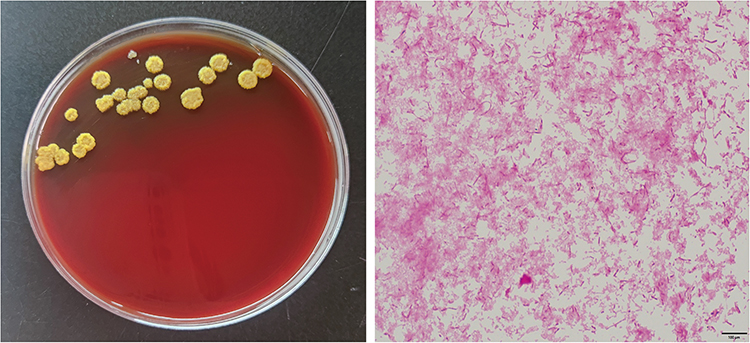 |
Figure 1 Bacterial culture morphology of wound secretions on 24-hour blood agar plate (left) and microscopic Gram staining morphology of bacteria (right). |
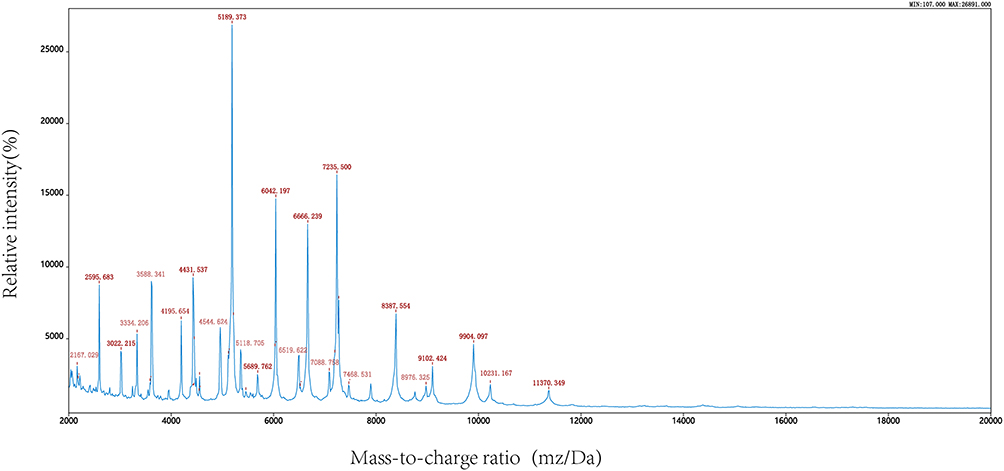 |
Figure 2 VITEK MS MALDI-TOF mass spectrometry identification result of Pseudomonas oryzihabitans. |
Treatment
Based on the patient’s condition, a comprehensive treatment plan of “microbiologically guided antimicrobial therapy + surgical intervention + management of underlying diseases + nutritional support” was adopted: Anti-infection treatment: Cefoperazone-sulbactam was selected according to drug sensitivity results; Surgical intervention: Phased debridement, negative pressure wound therapy and split-thickness skin grafting were performed; Management of underlying diseases: Intensified insulin therapy for hypoglycemia, amlodipine for hypertension to maintain stable blood glucose and blood pressure; Supportive treatment: Potassium chloride supplementation to correct hypokalemia, nutritional support due to NRS 2002 score >3 points, and nadroparin for prevention of deep vein thrombosis. VTE risk score 4 points, moderate risk.
First-stage operation: Under local anesthesia, “debridement of left lower leg burn + negative pressure wound therapy” was performed. Black eschar, necrotic tissues and purulent secretions of the three wounds were thoroughly debrided, hemostasis was achieved, negative pressure sponge was covered, sealed with surgical film, and one negative pressure drainage tube was indwelled to maintain central negative pressure suction. Intraoperative blood loss was about 20 mL, and the operation was smooth.
Postoperative treatment: Cefoperazone-sulbactam anti-infection was continued (course of 10 days), the drainage tube was kept unobstructed and sealed, regular dressing changes were performed, and blood glucose, blood pressure and infection indicators were closely monitored. On the first day after operation, the wound dressing was clean without oozing of blood or fluid; on the third day after operation, re-examination of infection markers showed serum amyloid A 35.2 mg/L and C-reactive protein 8.6 mg/L, which were significantly lower than those before operation; on the seventh day after operation, bacterial culture of wound secretions was negative.
Second-stage operation: Under local anesthesia, “debridement of left lower leg burn + split-thickness skin grafting + negative pressure wound therapy” was performed. Split-thickness skin grafts with an area of 2.5% were harvested from the left thigh, trimmed into 0.3–0.5 cm squares, and covered on the 8.0 cm × 4.5 cm medial wound of the left lower leg. Vaseline gauze, mesh gauze and negative pressure sponge were sequentially applied, and compressive bandaging was performed with surgical film sealing. Intraoperative blood loss was about 5 mL, and the operation was smooth.
Outcomes
The negative pressure device was removed 2 weeks after skin grafting, and granulation tissue grew well in the wound without signs of infection; subsequent regular dressing changes were performed until the wound was completely healed. During follow-up, the wound healed well without complications such as infection recurrence or skin graft necrosis (Figure 3).
 |
Figure 3 The wound treatment status of the patient. (a) Preoperative appearance of the burn wound on the lower 1/2 of the left lower leg (third-degree burn); (b) Anterior wound (5.5cm×5.0cm) with 100% black eschar coverage at the base, a small amount of yellow purulent secretion at the edge, surrounding skin erythema and increased skin temperature, no fluctuation on palpation; (c) Lateral wound (10.0cm×5.5cm) with 100% black eschar coverage at the base, surrounding skin erythema and increased skin temperature, no fluctuation on palpation; Medial wound (8.0cm×4.5cm) with 50% black eschar coverage, 25% yellow tissue and 25% red tissue at the base, partial shedding of yellow eschar, surrounding skin erythema and increased skin temperature, no fluctuation on palpation; (d) Debridement of necrotic tissues and purulent secretions in the skin and subcutaneous tissue, followed by vacuum-assisted closure; (e) Wound healing status 7 days after the first operation (granulation tissue grew well with no obvious exudation); (f) Healing status of the anterior wound 7 days after debridement, split-thickness skin grafting and vacuum-assisted closure; (g) Good healing status of the lateral wound. |
Discussion
This patient presents a rare and clinically innovative case of third-degree burn induced by improper moxibustion patch use, complicated by infection with Pseudomonas oryzihabitans—an emerging opportunistic pathogen that has been rarely reported in burn wound infections, especially in the context of traditional Chinese medicine (TCM)-derived thermal injuries. Beyond the conventional “microbiologically precise antimicrobial therapy + surgical intervention” paradigm.
Pseudomonas oryzihabitans is a Gram-negative, aerobic, flagellated opportunistic pathogen widely distributed in natural environments such as soil and water. Farmers are prone to skin and mucous membrane contamination due to long-term exposure to farm environments.6 In this case, the patient was complicated with diabetes mellitus and arteriosclerotic occlusive disease, with impaired immune function and damaged skin barrier, which provided favorable conditions for bacterial invasion and reproduction.5 The bacterium is characterized by positive catalase and oxidase activity, and some strains can produce β-lactamases or activate efflux pump systems, leading to multidrug resistance.6 Therefore, microbiological testing is crucial for diagnosis and treatment. Bacterial culture of wound secretions combined with mass spectrometry identification can quickly confirm the pathogenic bacteria, interpreted according to CLSI/EUCAST guidelines. A colony count ≥106 CFU/mL confirmed a true infection rather than contamination.7 Drug sensitivity test provides a basis for the selection of antimicrobial agents. In this case, the drug sensitivity results showed that the patient was sensitive to cefoperazone-sulbactam, which was administered for 10 days after operation. Combined with surgical debridement, the infection indicators decreased rapidly, and bacterial culture turned negative 7 days after operation, confirming the effectiveness of precise antimicrobial therapy. Clinically, blind use of broad-spectrum antibiotics should be avoided to prevent the induction of drug resistance. Commonly used sensitive drugs include cefoperazone-sulbactam, piperacillin-tazobactam and carbapenems.8
For deep burn wounds complicated with infection, the core value of surgical intervention lies in removing the source of infection and repairing tissue defects, which complements antimicrobial therapy. Thorough removal of necrotic tissues and purulent secretions can directly reduce bacterial load, eliminate infection foci, prevent bacterial invasion into deep tissues, and create conditions for the effectiveness of antimicrobial agents. In this patient, the preoperative wound was covered with black eschar, under which a large number of bacteria and necrotic tissues were hidden. Simple antimicrobial therapy was difficult to penetrate, and the infection was quickly controlled after debridement with improved wound drainage.9 Postoperative application of vacuum-assisted closure can effectively remove wound exudate, reduce edema, promote local blood circulation, improve the wound microenvironment, and create conditions for granulation tissue growth and subsequent skin grafting.10 It is especially suitable for large-area and irregular infected wounds. For full-thickness skin defects caused by third-degree burns, skin grafting is a key method for wound repair, which can quickly cover the wound, reconstruct the skin barrier, and reduce the risk of reinfection. In this case, first, debridement to control infection, then skin grafting to repair defects, which conforms to the surgical principle of “controlling infection first, then repairing tissue”.11
The synergistic effect of the two is the core to improve the cure rate. Debridement directly removes most bacteria and necrotic tissues, reduces the target of antimicrobial agents, increases local drug concentration, and enhances antimicrobial efficacy;12 Preoperative use of sensitive antibiotics can control systemic infection,13 reduce wound inflammation and edema, and create safe conditions for surgery; postoperative continuation of antimicrobial therapy can eliminate residual bacteria, reduce the risk of surgical site infection, and avoid skin graft failure; Postoperatively, the treatment effect is evaluated and the course of antimicrobial therapy is adjusted according to infection indicators and bacterial culture results, ensuring that skin grafting is performed only after complete control of infection, realizing the orderly progress of “infection control - tissue repair”.
The high-risk factors of this patient include elderly farmer, multiple underlying diseases, improper use of moxibustion patch and self-treatment of the wound.14 For elderly patients with diabetes mellitus and vascular diseases, inform them of the contraindications and risks of moxibustion patch use, and avoid prolonged application;15 After burns, patients should be guided to avoid spontaneous rupture of blisters and topical application of unknown drugs, and seek medical treatment in a timely manner for standardized treatment;16 For occupational exposure populations such as farmers, alert to the risk of infection by environmental pathogenic bacteria such as Pseudomonas oryzihabitans, and perform wound secretion culture early to avoid misdiagnosis and mistreatment.
Conclusion
Elderly patients with underlying diseases are prone to deep burns due to improper use of moxibustion patches, and occupational exposure increases the risk of Pseudomonas oryzihabitans infection. The diagnosis and treatment of such cases should adhere to the principle of “microbiologically precise antimicrobial therapy + synergistic surgical intervention”: early identification of pathogenic bacteria and selection of sensitive antibiotics through bacterial culture and drug sensitivity test, timely debridement to remove infection foci, combined with negative pressure wound therapy and skin grafting to repair wounds, while strengthening the management of underlying diseases and nutritional support. Early pathogen identification, targeted antibiotics and staged surgical intervention are critical to successful treatment.
Abbreviations
CRP, C-reactive Protein; CFU/mL, Colony-Forming Units per Milliliter; MALDI-TOF MS, Matrix-Assisted Laser Desorption/Ionization Time-of-Flight Mass Spectrometry; NPWT, Negative Pressure Wound Therapy; PCT, Procalcitonin; SAA, Serum Amyloid A; TCM, Traditional Chinese Medicine.
Data Sharing Statement
The clinical data, laboratory test results, and related materials involved in this study have been properly archived. Requests for access to the raw data or related materials of this study can be made to the corresponding author. The use of data must comply with relevant ethical norms and data confidentiality requirements.
Ethical Approval and Consent to Participate
This study has been approved by the Ethics Committee of The First Affiliated Hospital of Guangdong Pharmaceutical University (Approval No.: 202512). Written informed consent has been obtained from the patient for participation in the study and the collection and analysis of relevant data. All research procedures comply with the ethical principles of the Helsinki Declaration.
Consent for Publication
The patient has personally provided written consent for the publication of this case report and related clinical data (including imaging pictures, laboratory test data, and treatment records), and has signed the informed consent form for publication, agreeing to the use of relevant materials for academic exchange and publication.
Acknowledgments
We would like to thank the laboratory teams of The First Affiliated Hospital of Guangdong Pharmaceutical University and Guangzhou No.11 People’s Hospital for their technical support and experimental assistance. We also appreciate the collaboration of the multidisciplinary team including Clinical Laboratory, General Surgery Department I andDepartment of Infectious Diseases, involved in the treatment of this case.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study did not receive any external funding support.
Disclosure
All authors (Ruofan Wang, Jiongbiao Yu, Yubin Guan, Xiaosong Xu, Xiangsheng Cai) declare that there are no known conflicts of interest (including but not limited to financial, professional, or personal relationships) that could inappropriately influence or bias the research work reported in this manuscript and its publication. The authors confirm that this declaration is accurate and complete, and agree to the terms of the journal’s conflict of interest policy.
References
1. Wei Y, Qu Y, Yuan A, et al. [Moxibustion at different temperatures for cognitive impairment in type 2 diabetes mellitus: a randomized controlled trial]. Zhongguo Zhen Jiu. 2025;45(9):1233–8. Chinese. doi:10.13703/j.0255-2930.20240903-k0006
2. Schaefer TJ, Szymanski KD. Burn evaluation and management (Archived). In: StatPearls. Treasure Island (FL): StatPearls Publishing LLC.; 2025.
3. Zdziarski P, Paściak M, Chudzik A, et al. Cutaneous tuberculosis-ambiguous transmission, bacterial diversity with biofilm formation in humoral abnormality: case report illustration. Front Public Health. 2023;11:1091373. doi:10.3389/fpubh.2023.1091373
4. Pang F, Tao A, Ayra-Pardo C, et al. Plant organ- and growth stage-diversity of endophytic bacteria with potential as biofertilisers isolated from wheat (Triticum aestivum L.). BMC Plant Biol. 2022;22(1):276. doi:10.1186/s12870-022-03615-8
5. Harsent R, Macleod J, Rowlands RS, et al. The identification of multidrug-resistant microorganisms including Bergeyella zoohelcum acquired from the skin/prosthetic interface of amputees and their susceptibility to Medihoney™ and garlic extract (Allicin). Microorganisms. 2022;10(2):299. doi:10.3390/microorganisms10020299
6. Elbehiry A, Marzouk E, Aldubaib M, et al. Pseudomonas species prevalence, protein analysis, and antibiotic resistance: an evolving public health challenge. AMB Express. 2022;12(1):53. doi:10.1186/s13568-022-01390-1
7. Su J, Zhang D, Du J, et al. The efficacy of negative pressure wound therapy combined with topical oxygen therapy in treating chronic refractory wounds: a systematic review and meta-analysis. Adv Wound Care. 2025.
8. Radzikowska-Büchner E, Łopuszyńska I, Flieger W, et al. An overview of recent developments in the management of burn injuries. Int J Mol Sci. 2023;24(22):16357.
9. Widigdo DAM, Muttaqien Sofro Z, Suseani pangastuti H, et al. The efficacy of Negative Pressure Wound Therapy (NPWT) on healing of diabetic foot ulcers: a literature review. Curr Diabetes Rev. 2024;20(8):1–11. doi:10.2174/0115733998229877230926073555
10. Lahdenperä NI, Lindford A, Kautiainen H, et al. Long-term health-related quality of life after a deep second- or third-degree burn treated with skin grafting. Burns. 2025;51(6):107560. doi:10.1016/j.burns.2025.107560
11. Kuromaru Y, Won P, Madrigal P, et al. Negative pressure wound therapy and its use in burn wounds: an updated systematic review. J Burn Care Res. 2025;46(3):581–589. doi:10.1093/jbcr/iraf001
12. Burgess M, Valdera F, Varon D, et al. The immune and regenerative response to burn injury. Cells. 2022;11(19):3073. doi:10.3390/cells11193073
13. Behera S, Mishra B, Cherian JJ, et al. Efficacy and safety of platelet-rich plasma as an adjunct therapy to split thickness skin graft in burn patients with granulating raw wounds: a prospective, randomized, double-blind study-study protocol. Trials. 2025;26(1):83. doi:10.1186/s13063-025-08757-2
14. Hosseini M, Roberts MS, Aboofazeli R, et al. Measurement of Hansen Solubility Parameters of third-degree burn eschar. Burns. 2022;48(4):860–871. doi:10.1016/j.burns.2021.07.017
15. De Ketele A, Degreef I. Full-thickness skin grafting in preventing recurrence of Dupuytren’s disease: a systematic review. Hand Surg Rehabil. 2023;42(4):273–283. doi:10.1016/j.hansur.2023.06.002
16. Dayya D, O’Neill OJ, Huedo-Medina TB, et al. Debridement of diabetic foot ulcers. Adv Wound Care. 2022;11(12):666–686. doi:10.1089/wound.2021.0016
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.