")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Prurigo Pigmentosa Successfully Treated with Oral Minocycline: A Case Report
Authors Yang J , Hu X, Niu M, Zheng X
Received 7 February 2023
Accepted for publication 4 April 2023
Published 24 April 2023 Volume 2023:16 Pages 1073—1077
DOI https://doi.org/10.2147/CCID.S404859
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Jie Yang,* Xiaohuan Hu,* Mu Niu, Xiaole Zheng
Department of Dermatology, The Fifth People’s Hospital of Hainan Province, Haikou, Hainan Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Mu Niu; Xiaole Zheng, Department of Dermatology, The Fifth People’s Hospital of Hainan Province, No. 8 Longhua Road, Longhua District, Haikou City, Hainan Province, 570206, People’s Republic of China, Email [email protected]; [email protected]
Purpose: We aimed to report a case of prurigo pigmentosa (PP) with blisters.
Patients and Methods: A 21-year-old male patient presented to our hospital with erythema, papules, and blisters all over the front chest and back. Densely distributed round and oval edematous erythema was noted on the neck, front chest, and back of the patient. Histopathologic examination of the skin lesions (blisters) on the chest revealed epidermal cell hyperkeratosis. He was diagnosed with PP and was treated with oral minocycline.
Results: After 1-week minocycline administration, the patient’s itching was relieved, and the blisters dried up. His skin lesions recurred following self-withdrawal from the medication; subsequently, the patient was administered oral minocycline treatment again. After 1-month continuous oral treatment, the drug was discontinued. No recurrence of symptoms was noted.
Conclusion: Oral minocycline is effective for the treatment of PP.
Keywords: prurigo pigmentosa, blister, minocycline, case report
Introduction
On March 18, 2019, a 21-year-old male patient presented to our hospital with erythema, papules, and blisters all over the front chest and back for 10 months. Furthermore, dark red erythema with slight pruritus developed on the front chest and back with unknown etiology. The patient visited a local hospital and was diagnosed with pityrosporum folliculitis. He was treated externally with ketoconazole cream; however, the treatment effect was not good. In the past 3 months, the patient’s skin lesions gradually spread to the neck and abdomen, and portions of the skin lesions were fused into pieces, which were not treated at that time. In the recent 1 month, several blisters accompanied by intense pruritus appeared on the erythematous areas of the front chest and back.
Previous History
The patient denied a previous history of hypertension, diabetes, and other chronic diseases. Moreover, he denied a previous history of tuberculosis, hepatitis B, and other infectious diseases. Furthermore, previous histories of trauma and surgery as well as drug and food allergy were not reported. No similar diseases were reported in the family. The patient has been working for a long time as a fisherman. His diet mainly includes marine fish, shrimps, and other high-protein and high-fat diets, with low intakes of carbohydrates, including rice and noodles, fruits, and vegetables.
Dermatological Examination
His neck, front chest, and back showed densely distributed round and oval edematous erythema. Portions of the erythematous areas had mung bean- to soybean-sized blisters. The blisters had tense walls and clear fluid, were easy to break, and had exudative and scabbed portions. He was Nikolsky sign negative (Figure 1A–D).
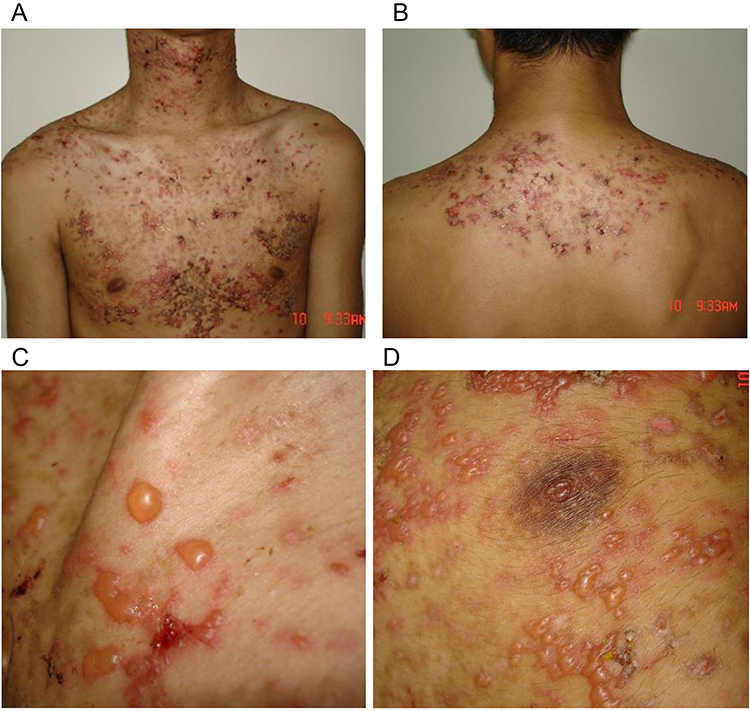 |
Figure 1 Dense distribution of round and oval edematous erythema is observed on the (A) neck, front chest, and (B) back. (C and D) Portions of the erythema show blisters with the size of mung bean to soybean. Moreover, the blisters have tense walls and clear fluid and are easy to break. |
Laboratory and Auxiliary Examination
His routine blood, urine, and stool examination as well as liver and kidney function examination were all not significantly abnormal. The results of antidouble–stranded DNA antibody, anti-BP180 antibody IgG, anti-BP230 antibody IgG, antidesmoglein 1 antibody IgG, antidesmoglein 3 antibody, antiepidermal basement membrane antibody IgG and IgA, and antispinous cell desmosomal antibody IgG and IgA examinations were negative. Additionally, polymerase chain reaction test results for herpes simplex virus types I and II were negative. Bacterial cultures of the blister fluid were negative.
Histopathologic Examination of Skin Lesions
Chest lesions (blisters) showed hyperkeratosis, and the skin lesions were intraepidermal blisters. The top of the blisters was composed of incomplete epidermis with scattered epidermal cells with poor keratosis. A large amount of serous fluid and low lymphocyte, neutrophil, and eosinophil levels were noted in the blisters. Additionally, a significant intracellular and intercellular edema in the lateral wall of the blisters was observed. Moderate infiltration of mixed inflammatory cells below the vesicle was observed. Immunofluorescence revealed negative test results for IgG, IgM, IgA, and C3; pemphigus and dermatitis herpetiformis were ruled out, and salt-split skin immunofluorescence was negative (Figure 2A and B). Subsequently, the patient was diagnosed with prurigo pigmentosa (PP).
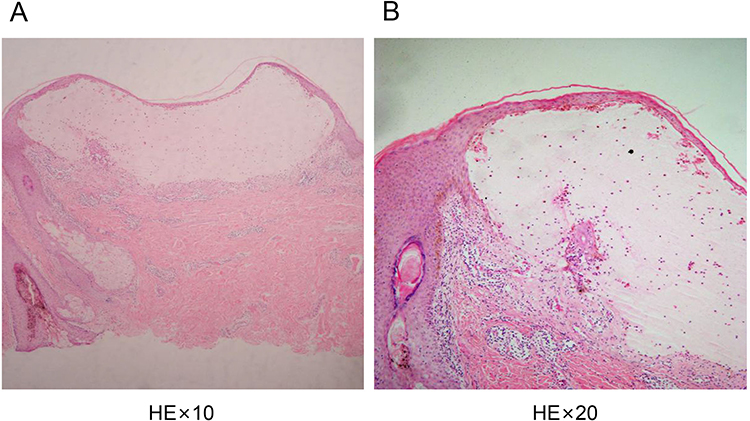 |
Figure 2 Skin lesions are detected as intraepidermal blisters. (A and B) The top of the blisters is composed of incomplete epidermis with scattered epidermal cells with poor keratosis. A large amount of serous fluid and low lymphocyte, neutrophil, and eosinophil levels are noted in the blisters. Additionally, a significant intracellular and intercellular edema in the lateral wall of the blisters is observed. Lastly, moderate infiltration of mixed inflammatory cells below the vesicle is observed. |
Treatment and Care
(1) the patient was instructed to have a reasonable diet by guiding him in increasing his daily intake of carbohydrates, including rice and noodles, fruits, and vegetables. (2) Normal saline was used to wash the erosive surface formed by the rupture of the blister, thereby removing the exudative fluid and necrotic tissue. (3) He was administered oral minocycline 100 mg twice daily. After 1 week, the pruritus was relieved, and the blisters dried up. After self-withdrawal from the medication, the patient resumed fishing, and the skin lesions recurred. He was subsequently administered oral minocycline 100 mg again twice daily. After 1 week, the blisters subsided, and the drug was discontinued after 1-month continuous oral administration. No symptom recurrence was noted during the follow-up visit.
Discussion
PP is a rare chronic inflammatory skin disease, which was first described by Nagashima et al in 1971 and officially named PP in 1978.1,2 PP tends to occur in young females and is prone to recurrence during spring and summer. Typical clinical manifestations include pruritus, erythema, papules, and papulovesicular lesions in the shoulder, back, clavicular region, and chest. Skin lesions accompanied by blisters and bullosa are rare; erythema can resolve itself within a few weeks, and reticular pigmentation spots remain even after the erythra subsides. The specific etiology and pathogenesis of PP are unknown, which may be related to the inflammatory response caused by neutrophil chemotaxis mediated by interleukin (IL)-6 and IL-8.3 Atopic dermatitis, diabetes, pregnancy, sweating, and friction from clothing or nylon shower towels are all possible causes of PP. Recent studies have reported that PP is closely related to ketosis, and cases of PP induced by poor blood sugar control, ketogenic diet, and diet have been reported.4,5 The patient in this report was a local fisherman who has been working for a long time. His diet mainly consisted of high-protein and high-fat diets, including fish and shrimp, with a low intake of carbohydrates, fruits, and vegetables. Furthermore, in a high-heat and high-salt environment, such as the sea, the body sweats easily; therefore, we speculate that diet and sweating may also be the main causes of the disease. In this case, the skin lesions subsided following treatment; however, they recurred when the patient resumed fishing, further confirming our speculation.
The skin histopathology changes of PP will change with disease progression, which has a certain diagnostic value. The histopathological manifestations of the initial lesions were epidermal spongiform edema and ballooning degeneration, necrotic keratinocytes observed on the epidermis, and neutrophil and erythrocyte extravasation around the vessels in the superficial dermis. With the further progression of the disease, the lesions showed mixed inflammatory infiltration of dermal lymphocytes, eosinophils, and neutrophils. Advanced lesions showed hyperkeratosis, parakeratosis, increased pigmentation in the basal layer, and pigmented cells in the superficial dermis.6
PP is easily misdiagnosed as temporary acantholysis derma, confluent and reticulated papillomatosis, and adult Still’s disease with persistent erythra. Temporary acantholysis derma is the most common in middle-aged and older adult males, and lesions most frequently occur near the clavicle, neck, and trunk. The lesions are mostly scattered, clustered, or distributed in bands, manifesting as edematous or acne-like erythema, papules, and blisters. Post-inflammatory hyper- or hypopigmentation may remain even after the lesions subside, and histopathologic changes reveal obvious acantholysis. Moreover, adult Still’s disease is clinically manifested as red papules in the interscapular area and anterior chest, accompanied by obvious pruritus; however, it is often accompanied by joint pain, fever, and other systemic symptoms.7 The typical lesions of confluent and reticulated papillomatosis are verrucous or papillary lesions, with histopathologic manifestations of epidermal papillomatous hyperplasia without inflammatory cell infiltration.8
This disease is self-healing, and some patients can improve or even recover by increasing carbohydrate intake.4 Antihistamine and glucocorticoid treatments are ineffective for this disease, and minocycline is the drug of choice, with a recommended dose of 100–200 mg/day orally.9 Minocycline is a lipophilic derivative of tetracycline, with anti-inflammatory and immunosuppressive effects in addition to its antibacterial properties. Additionally, it can inhibit lymphocyte transformation, antibody production, neutrophil chemotaxis, complement formation, and lipase and collagenase activity. Furthermore, the effectiveness of doxycycline, dapsone, potassium iodide, isotretinoin acid, and macrolide antibiotics have been reported in clinical practice. In this case, oral minocycline treatment was satisfactory.
Ethical Statement
The study was approved by the ethics committee of The Fifth People’s Hospital of Hainan Province.
Consent
The patient provides signed consent for the publication of the case details.
Acknowledgments
The authors thank all those who participated in this study. Jie Yang and Xiaohuan Hu have contributed equally to this work as co-first authors.
Funding
Project supported by Hainan Province Clinical Medical Center.
Disclosure
The authors declare that they have no competing interests.
References
1. Nagashima M, Ohshiro A, Shimizu N. A peculiar pruriginous dermatosis with gross reticular pigmentation. Jpn J Dermatol. 1971;81(2):78–91.
2. Rotstein H, Mason GH. A peculiar pruriginous dermatosis with gross reticular pigmentation. Australas J Dermatol. 1992;33:56–59. doi:10.1111/j.1440-0960.1992.tb00060.x
3. Lu PH, Hui RCY, Yang LC, et al. Prurigo pigmentosa: a clinicopathological study and analysis of associated factors. Int J Dermatol. 2011;50(1):36–44. doi:10.1111/j.1365-4632.2010.04625.x
4. Wong M, Lee E, Wu Y, et al. Treatment of prurigo pigmentosa with diet modification: a medical case study. Hawaii J Med Public Health. 2018;77(5):114–118.
5. Ohnishi T, Kisa H, Ogata E, et al. Prurigo pigmentosa associated with diabetic ketoacidosis. Acta Derm Venereol. 2000;80(6):447–448. doi:10.1080/000155500300080447448
6. Böer A, Misago N, Wolter M, et al. Prurigo pigmentosa: a distinctive inflammatory disease of the skin. Am J Dermatopathol. 2003;25(2):117–129. doi:10.1097/00000372-200304000-00005
7. Tseng HW, Tseng HH, Wu CS. Confluent and reticulate papillomatosis treated with minocycline and tazarotene. Cutis. 2013;91(4):194–197.
8. Lee JY, Hsu CK, Liu MF, et al. Evanescent and persistent pruritic eruptions of adult-onset still disease: a clinical and pathologic study of 36 patients. Semin Arthritis Rheum. 2012;42(3):317–326. doi:10.1016/j.semarthrit.2012.05.003
9. Kim JK, Chung WK, Chang SE, et al. Prurigo pigmentosa: clinicopathological study and analysis of 50 cases in Korea. J Dermatol. 2012;39(11):891–897. doi:10.1111/j.1346-8138.2012.01640.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.