Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Providing Older Adults Experiencing Benign Prostatic Hyperplasia with an Education Booklet to Improve Health Information Recall
Authors Liu J ![]() , Chen X, Zhou Y, Zhang J, Zhang Z, Zhang H, Li X
, Chen X, Zhou Y, Zhang J, Zhang Z, Zhang H, Li X
Received 16 July 2025
Accepted for publication 20 October 2025
Published 1 November 2025 Volume 2025:18 Pages 7061—7071
DOI https://doi.org/10.2147/JMDH.S552838
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jia Liu,1,* Xiaomei Chen,2,* Yuanxiu Zhou,3,* Jing Zhang,1 Zuli Zhang,1 Huan Zhang,1 Xuemei Li1
1Department of Urology, First Affiliated Hospital of Army Medical University, Chongqing, People’s Republic of China; 2Department of Nursing, Chengdu Wenjiang District People’s Hospital, Chengdu, People’s Republic of China; 3Department of Urology, Rongchang District People’s Hospital, Chongqing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xuemei Li, Department of Urology, First Affiliated Hospital of Army Medical University, No. 30, Gaotanyanzheng Street, Shapingba District, Chongqing, 400038, People’s Republic of China, Tel +86-13908306486, Email [email protected]
Background: A common challenge in health education for older surgical patients is poor memory, which hinders the processing of health information. Structured educational materials have been shown to be effective in improving information retention, but there remains a paucity of materials specifically designed to address the cognitive and sensory characteristics of older adults.
Objective: To evaluate the effect of an adapted education booklet based on cognitive load theory and older adults’ preferences on the memory of health information in older surgical adults experiencing benign prostatic hyperplasia (BPH).
Methods: A randomized controlled trial was conducted at a tertiary hospital from January to February 2025. Sixty-four older adults scheduled for BPH surgery were randomly divided into an intervention group (n=32, using an adapted education booklet) and a control group (n=32, using conventional education materials). Both groups received standard perioperative education. Health information recall was evaluated using a standardized questionnaire on the day before discharge. Secondary outcomes included satisfaction with nursing care and the nurse’s support for the booklet.
Results: There were no differences between the two groups in terms of age, body mass index, educational attainment, monthly personal income, and length of hospital stay. Adults in the intervention group demonstrated superior recall of health information and nursing satisfaction compared to the control group (P < 0.001). Over 85% of nurses believed that the booklet did not increase their workload, improved nurse-adult communication, and expressed support for its clinical application.
Conclusion: Adapting an education booklet based on cognitive load theory and older adult preferences can significantly improve health information recall and satisfaction among older adults experiencing BPH. High acceptance among nurses suggests that this intervention has potential for clinical application. This simple, easy-to-administer, and inexpensive method of patient education could be extended to other areas of geriatric surgical education.
Keywords: prostatic hyperplasia, older, educational material, information recall, patient education
Introduction
Studies have confirmed the effective health information recall can increase adult satisfaction and improve adult health-related outcomes.1 Although the World Health Organization advocates for a high-quality communication framework centered on “information integrity, emotional support, and shared decision-making” to improve adults’ recall of health information,2 clinical practice shows that there is a significant gap: 40% to 80% of the verbal information provided by healthcare professionals to adults is immediately forgotten, and more than 50% of the recalled information contains errors.3 Human working memory capacity is limited,4 making it difficult to receive and process large amounts of complex health information through verbal communication alone within a short period of time. Written materials compensate for this deficiency through the following advantages: (a) structured content improves comprehension; (b) comprehensive coverage of key information; (c) continuous accessibility for reference at any time, thereby significantly improving information recall, knowledge retention, and adult satisfaction, which is particularly evident in chronic disease management.5,6 Based on this, we hypothesize that well-designed written educational materials are equally effective in improving information recall among older adults.
In fact, older adults may face some particular challenges in health information recall. First, cognitive decline affects information processing capacity. With age, working memory capacity shrinks and information processing slows down significantly.7 Second, sensory deterioration limits the efficiency of information reception. Among older adults, vision loss and hearing loss are the most common manifestations of sensory deterioration, and hearing loss may result in adults being unable to accurately receive health information conveyed by healthcare professionals.8
While providing general written materials has improved adults’ recall of health information and knowledge to some extent,9 two persistent issues remain. First, even when the most complex information materials are provided, adults’ recall abilities are significantly lower than doctors’ expectations. Second, there is insufficient consideration of the needs and preferences of different types of people. Research shows that optimizing the form and method of information provision can reduce the impact of age-related factors (such as declining working memory and cognitive impairment) on information recall.10 The development of educational materials can help older adults improve health messaging; it may be the key breakthroughs in improving patient education effects.
In principle, there are two ways to overcome this dilemma: better structural expression or design that conforms to preferences. First, a structured expression based on cognitive load theory. Systematic reviews have confirmed that using specific framing strategies when providing information to adults appears to have a positive impact on their recall of information.11 From a cognitive function perspective, designing health materials based on working memory limitations can help adults process health information more effectively.4,12 Cognitive load theory (CLT) was proposed by John Sweller, it emphasizes the significant role of cognitive resources in the information processing process, providing a specific framework for structured educational materials. Research has shown that by following this framework, adults can enhance their understanding and retention of information.13 Furthermore, educational materials tailored to individual preferences are more likely to be perceived as relevant to the individual, leading to better information recall. A review showed that older adults have different preferences for educational materials than younger people.14 They prefer written or downloadable formats, larger fonts, and simpler expressions.
However, in the design of materials for older adults, few studies have used both of the above methods, which take into account the cognitive characteristics of adults and conform to adult preferences. Therefore, this study took benign prostatic hyperplasia(BPH) as its research subject. BPH is a common trouble using the bathroom in older men. Epidemiological surveys have shown that the prevalence of BPH exceeds 50% in men aged 60 years and is as high as 83% in those aged 80 years and over.15 Based on full consideration of the cognitive characteristics of older adults and their preferences for education materials, the research team innovatively developed an education booklet for BPH surgical adults that integrates cognitive adaptation and personalized design. This study aims to evaluate (a) whether the adapted booklet can improve the recall of health information by older surgical adults and (b) whether the use of this booklet can be supported by clinical nurses.
Materials and Methods
Study Design
We designed a randomized controlled trial conducted in older adults scheduled for BPH surgery at a large, tertiary-care, academic medical center. The study was conducted based on the Consolidated Standards of Reporting Trials (CONSORT).
Booklet Adaptation
The booklet was adapted to make it more suitable for older adults. First, the content of the booklet was determined based on currently used education materials and the latest guidelines.16 Then, the booklet was designed based on the principles and strategies of medical education design according to cognitive load theory,13 the specific framework is shown in Figure 1. Then, based on adults’ preferences for educational materials,14 the format of the booklet was determined to be a combination of text and images, using font size 14 or larger, with a colorful printout measuring 20.6 cm × 14.4 cm, and a QR code was generated for the video explanation for adults’ convenience. The quality, comprehensibility, and feasibility of the adapted booklet were assessed by distributing it to urological specialists, researchers, nurses, and older adults with BPH. The Ensuring Quality Information for adults (EQIP) assessment showed high information quality (78.61%±9.23%). At the same time, the results of the patient education Materials Assessment Tool (PEMAT) evaluation showed that the comprehensibility (78.61%±9.23%) and feasibility (88.69%±10.40%) of the booklet were both high. The booklet was subsequently named “Surgical Guidelines for Older Adults Experiencing BPH Surgery”.
 |
Figure 1 Designing education booklet for older adults experiencing BPH based on CLT. |
Study Procedures
We designed a randomized controlled trial conducted in older adults experiencing BPH scheduled for surgery at a large, tertiary-care, academic medical hospital from January to February 2025. The inclusion-exclusion criteria for the study population were as follows: Inclusion criteria: (a) age range of 60 to 90 years old, with an education level of primary school or above; (b) diagnosed with BPH; (c) proposed surgical treatment of the prostate. Exclusion criteria: (a) adults experiencing stroke, dementia, malignant tumor, or hearing impairment; (b) adults experiencing psycho-spiritual diseases; (c) adults or family members who refused to participate in the trial.
94 patients were enrolled in the study. A total of 27 cases met the exclusion criteria and were not randomly assigned. Among them, 17 cases refused to participate, 6 cases had hearing impairments, 3 cases had malignant tumors, and 1 case had surgery cancelled. Subsequently, 67 patients were randomly assigned to the control group and the intervention group, among whom 3 adults refused to use the booklet. The final sample size for this study was 64 cases, 32 cases in each of the two groups. A flowchart of enrollment and adults included in the study is shown in Figure 2.
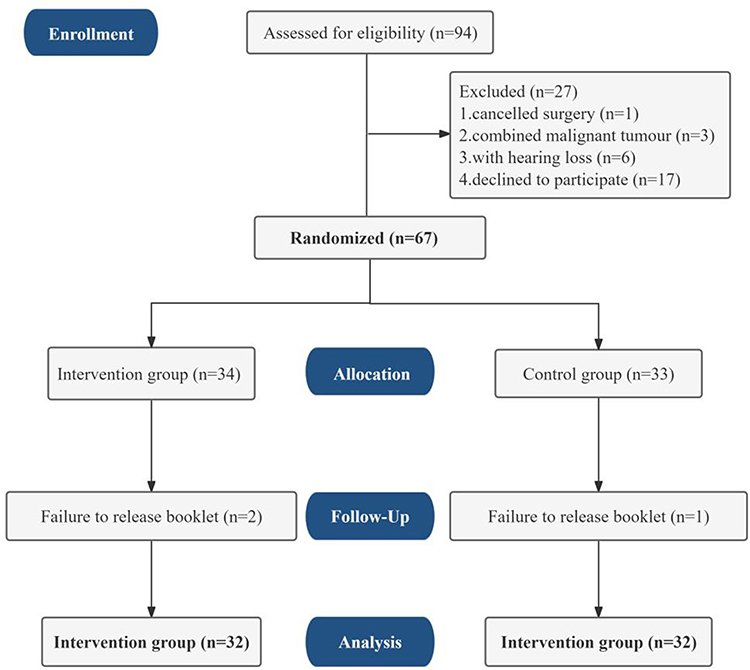 |
Figure 2 Flow diagram of patients enrolled. |
This is a nurse-led study, with educational materials adapted and distributed to patients by a nurse. Patients are enrolled in order of their appointment schedule. The patients were randomly divided into the control group and the intervention group using the random number table method. The control group used the original educational materials to provide health education during hospitalization, and the intervention group used the adapted education booklet to provide health education. To ensure the quality of the study, nurses were trained and assessed on the research process and booklet use before the study began. Nurses used the adapted booklet or original education materials to provide health education to adults on the day before surgery, on the day of surgery, and on the day before discharge. The basic information was obtained from the adult medical record system, and health information recall and satisfaction were evaluated on the day before discharge. At the end of the study, an anonymous questionnaire was administered to the nurses who implemented the intervention to evaluate their support for the use of the booklet. This study used a blinded outcome measure collector and statistical analyst. Since the intervention was the application of an education booklet, it was not possible to blind the intervention implementers and adults.
Outcome Measures
Patient Measurement
Socio-Demographic Data
The questionnaire was designed by the research team based on a literature review and disease characteristics. It included questions on name, age, body mass index(BMI), residence, educational level, monthly personal income, days of hospitalization, and American Society of Anesthesiologists (ASA) classification.
Information Recall
A health information recall questionnaire was designed by the researcher based on the communication booklet, combined with literature research, and after discussion in the group, including health-related information that adults should know, mainly covering 5 aspects of health information, including disease-related knowledge, urinary catheter care, life care, self-observation, and follow-up review. The questionnaire consists of 10 questions, presented in the form of judgment questions, with each item corresponding to three options: “correct”, “wrong”, and “don’t know”, with correct answers counting for 1 point and wrong answers counting for 0 points. Each item was presented in the form of “correct”, “wrong”, and “don’t know” options. The score for each item was summed and divided by 10 to determine the information recall rate, which ranged from 0 to 100%, with higher percentages indicating better information recall.
Nursing Satisfaction
Nursing satisfaction was evaluated using the Newcastle Nursing Satisfaction Scale (NNSS), which was developed by Thomas et al in 1996 to measure the level of adult satisfaction with the quality of nursing services during hospitalization.17 A total of 19 items were included, mainly covering five dimensions: the nurse’s understanding of adults’ conditions, service attitudes, professional skills, knowledge level, and information provided about diseases and treatments. A five-point scale was used, and the total score was calculated on a percentage basis, with the score being positively correlated with the level of adult satisfaction with the quality of nursing services.
Nurse Measurement
After all interventions were completed, each nurse was asked four questions to evaluate their support for the education booklet. The specific content included: (1) This booklet has made my communication with adults more efficient and has increased my satisfaction with work; (2) This booklet has helped me build a more harmonious relationship with adults and provide them with better service; (3) It is easy to use and does not increase my workload; (4) I would recommend this booklet to my colleagues, as it has improved my work efficiency. Each question had five options, ranging from “strongly disagree” to “strongly agree”, with scores ranging from 1 to 5 points, for a total score of 5–20 points. The higher the score, the higher the nurse’s support for the booklet.
Power Calculation
The sample size was calculated based on the health information recall score. According to previous similar research literature,6 the average score of the control group after intervention was 12.06, with a standard deviation of 2.40, while the average score of the experimental group was 9.82, with a standard deviation of 2.81. According to G-power calculations, based on a significance level of 5% and a test efficacy of 80%, each group needed 22 older adults experiencing BPH, with an expected sample loss rate of 20%, and it was finally determined that at least 27 cases would be included in each group.
Data Analysis
This study used Excel for data entry and SPSS 24.0 software for statistical analysis, and statistical significance was set at P< 0.05. Details of the analytical methods are as follows: Quantitative data are expressed as M±SD, and categorical data are expressed as n (%). Baseline data comparisons between groups were performed using the Mann–Whitney U-test and chi-square test. Post-intervention comparisons between groups were performed using the Mann–Whitney U-test. Intra-group comparisons before and after intervention were performed using the Wilcoxon test.
Ethical Consideration
The trial was approved by the Ethics Committee of the First Affiliated Hospital of Army Medical University (NO. (A)KY2025020) and registered with the Chinese Clinical Trial Registry (ChiCTR2500099704). All participant data were anonymized and treated confidentially. Each participant provided informed consent and could withdraw from the study at any time without impact on their medical care.
Results
Characteristics of Patients
The overall study patients were 60–84 years old, with a mean age of 68.69 ± 6.07 years; 6.3%(n=4) of the adults had primary school education, 39.1%(n=25) had junior high school education, 32.8%(n=21) had high school education, and 21.9%(n=14) had university education and above; 32.8% of the adults resided in the rural areas, and 67.2% resided in the urban areas, as shown in Table 1.
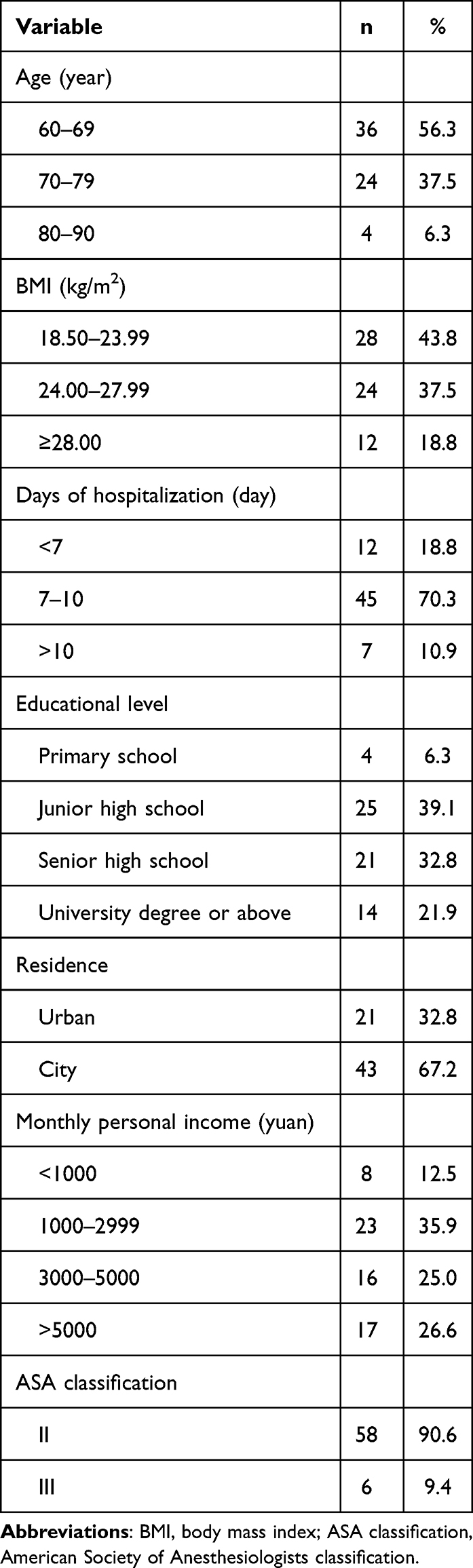 |
Table 1 Characteristics of Patients (n=64) |
Comparison of Patient Characteristics Between the Two Groups
The results of the comparison of the patient characteristics of the control group and the Intervention group showed that there was no difference between the groups (P > 0.05); details are shown in Table 2.
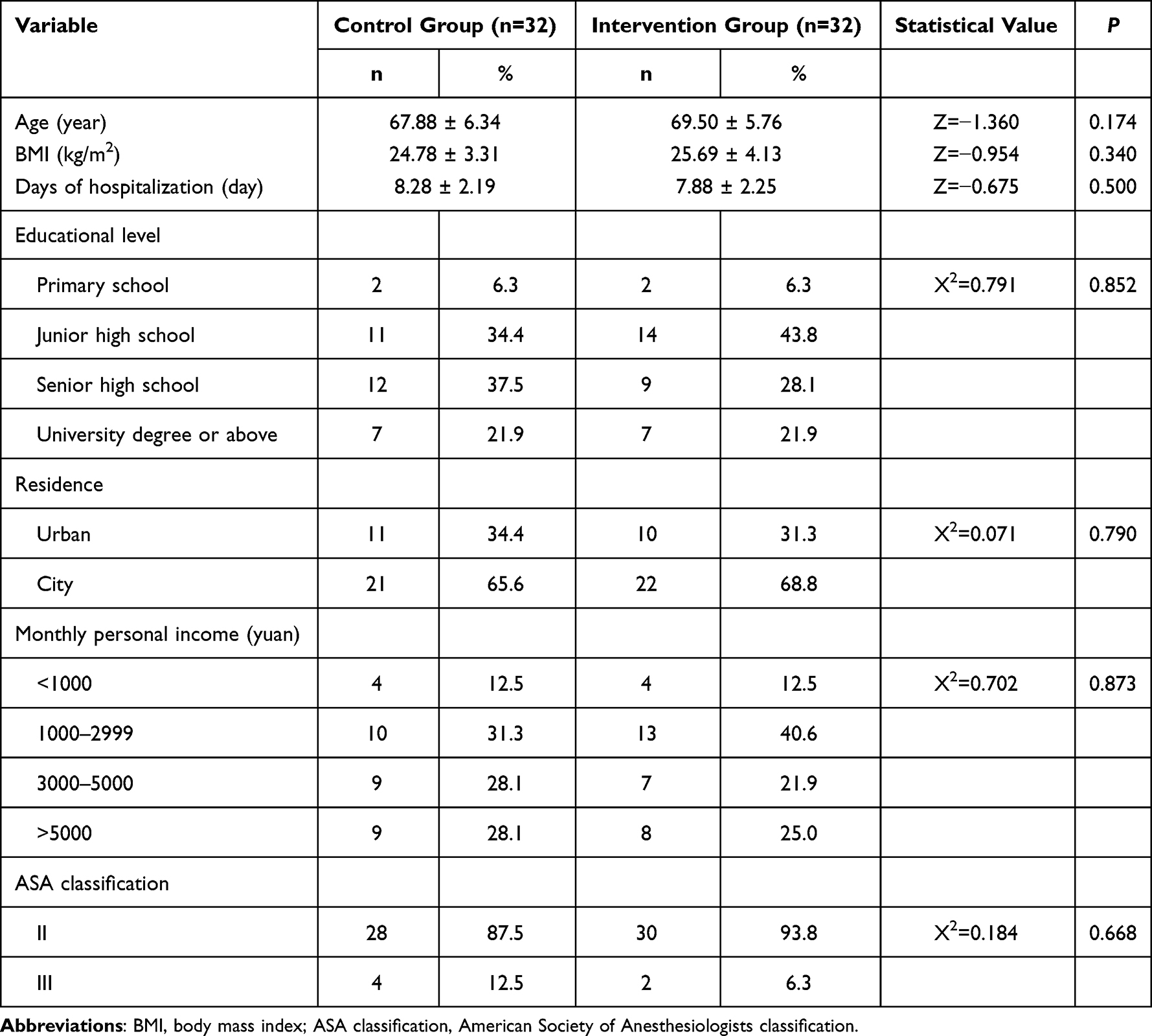 |
Table 2 Comparison of Patient Characteristics Between the Two Groups (n=64) |
Comparison of Health Information Recall and Nursing Satisfaction Between the Two Groups
The results of the study showed that the information recall rate and nursing satisfaction of the experimental group were significantly higher than those of the control group after the intervention (P < 0.001), as shown in Table 3.
 |
Table 3 Comparison of Information Recall and Nursing Satisfaction Between the Two Groups (n=64) (Points, M±SD) |
Support for the Booklet Among Nurses
Fourteen nurses participated in the study, aged 29–43 years old, with 7–28 years of work experience. Among them, 92.85% (n = 13) of the nurses indicated that use of the booklet was very helpful in fostering harmonious adult-provider relationships and that they were satisfied with their work. Additionally, 85.71% (n = 12) of the nurses believed that the booklet did not increase their workload and were willing to recommend it to other colleagues, as detailed in Table 4.
 |
Table 4 Nurses’ Support for the Booklet (n=14) |
Discussion and Conclusion
Discussion
The presentation format of educational materials is significantly associated with adults’ recall of health information.6,11 Based on this, we innovatively combined cognitive load theory with age-friendly design principles to design an adapted version of the educational booklet specifically tailored for older adults undergoing BPH surgery. The results of a randomized controlled trial showed that adults who used the adapted booklet had significantly improved recall of health information. More notably, 85.71% of nurses reported that the booklet did not increase their workload and expressed a willingness to promote its use in their departments. This research provides a practical solution to the problem of poor recall of health information among older adults in clinical practice.
Older surgical adults have significant barriers to accessing health information and often experience information memory bias, which can have a negative impact on postoperative recovery outcomes.18 When faced with complex medical information, this population’s ability to recall information is significantly lower than that of younger adults. This challenge stems from a variety of age-related changes. First, cognitive decline, especially a reduction in working memory capacity, can affect the processing and memory of medical information.19 Second, sensory function deterioration, including decreased vision and hearing, makes small fonts and complex charts ineffective for providing education materials in a single printed version. Traditional health education materials rarely take these age-related changes into account. This study fully considered age-related changes and significantly improved the recall of health information in older BPH surgical adults through the design of an age-appropriate booklet using CLT, similar to the results of previous studies.20
From a cognitive neuroscience perspective, the booklet adapted based on cognitive load theory may enhance memory encoding through three aspects. (a) Manage intrinsic load. Through a modular knowledge structure design, we systematically organized the booklet content into four logically connected sections, with each module containing 4–6 key knowledge points. This structure aligns with Sweller’s cognitive architecture theory,13 making information processing more compatible with the limited cognitive resources of older adults. By incorporating analogies and images to facilitate adult understanding, the adapted booklet features a mixed text design with 30% more visual elements, thereby enhancing the booklet’s comprehensibility. (b) Decrease extraneous load. The booklet reduces irrelevant cognitive load through methods such as a unified information hierarchy (presenting only one core concept per page), eliminating redundant information, and a consistent layout (presenting key prompts in fixed positions). (c) Optimize germane load. The booklet provides multimodal information coordination (face-to-face teaching and video explanations) and sets questions at different stages to promote in-depth processing of information by adults. The synergistic effect of these neurocognitive mechanisms provides a scientific explanation for the booklet’s significant improvement in information recall among older adults. This finding not only verifies the application value of CLT in medical education but also provides quantifiable design principles for the development of age-appropriate health education tools. Moreover, this adapted booklet improved the satisfaction of older adults undergoing surgery for BPH. In recent years, adult satisfaction has gradually become a hot topic in the field of global health policy and has been regarded as an important indicator of the quality of healthcare services and care outcomes.21 Studies have confirmed that effective information exchange between healthcare professionals and adults can significantly increase adult satisfaction.22,23
Through analysis, it was found that the increase in satisfaction in this study may be mainly due to three interrelated mechanisms: First, the booklet was designed based on the preferences of older adults for education materials,14 using visual optimization designs such as font sizes above 18, high-contrast colors, and eye-catching section headings, combined with multimodal compensation strategies such as explanatory illustrations and voice explanations, and providing a written version, which accurately matched the preferences of older adults for education materials. Second, structuring content based on CLT ensured the completeness and accuracy of key information transmission.24 More importantly, most adults feedback that this age-friendly design “demonstrates respect for the older”, and this positive emotional experience was significantly positively correlated with satisfaction.25 From a theoretical perspective, this increase in satisfaction not only directly improves the treatment experience but also further strengthens the health education effect by establishing a positive “emotional-cognitive” feedback loop, providing new intervention ideas for perioperative management of older adults.
The results showed that the application of this adapted education booklet was highly recognized by clinical nurses. Specifically, more than 85.71% of participating nurses believed that the booklet could improve nurse-adult communication and expressed their willingness to recommend it to their colleagues. This finding echoes the results of a study conducted by Pollak et al.26 It is worth noticing that in the evaluation items, “This booklet has helped me build a more harmonious relationship with adults and provide them with better service” received the highest score. This positive attitude may stem from the advantages of the booklet in improving the efficiency and quality of adult education. Firstly, as an aid to adult education, the booklet provides nurse with a systematic health education framework,27,28 which not only ensures consistency in the transmission of health information but also significantly reduces the cognitive burden of organizing educational content on nurses, allowing them to devote more energy to effective interaction with adults. Secondly, by giving the booklet directly to adults, it is convenient for them to refer to it at any time,29 which effectively reduces the risk of information omission or misunderstanding due to individual differences.
Meanwhile, the age-friendly design strategies adopted in the booklet based on adult preferences (including enlarged fonts, high-contrast colors, and a combination of text and images) significantly improved the satisfaction of older adults. This adult-centered design concept not only improved adult satisfaction but also indirectly optimized the quality of nurse-adult interactions. As stated in the WHO’s Effective Communication Framework:2 “When adults feel adequately informed and understood, the doctor-adult relationship naturally improves”. This mechanism effectively explains why healthcare professionals demonstrate such a positive willingness to use and promote the manual, laying the foundation for its application in clinical practice.
This study has the following advantages. First, by applying cognitive load theory, the intervention minimizes information overload, with a critical advantage for older adults with declining working memory. In the future, medical staff can apply this method to other adult surgical patients who need self-care guidance. Second, as a scalable tool requiring minimal staff training, the booklet is particularly valuable for resource-limited settings. Its low-cost nature makes it feasible for widespread adoption in outpatient urology clinics or geriatric surgical pathways. Finally, this intervention aligns with growing demands for adult-centered care while addressing age-related cognitive barriers.
Limitations and Future Directions
Despite the meaningful contributions of our study, there are some limitations. First, the sample size in the randomized control section was small, although the statistical requirements had been met, and with a lack of long-term follow-up data. Future studies may consider including a larger sample size and conducting long-term follow-up and observation. Second, the study was conducted at a single hospital, and the study effects were observed only during hospitalization. Future work should include updating the booklet content according to the latest guidelines, expanding its application to other institutions to complete a multicenter trial, and conducting similar studies targeting older BPH surgery populations. Develop a personalized content recommendation algorithm based on cognitive function (distinguishing between normal and mild cognitive impairment) to respond to the “tiered intervention” initiative outlined in the WHO’s “Ageing and Health Report.”
Conclusions
Our research indicates that education booklets designed based on cognitive load theory and optimized for the preferences of older adults can significantly improve health information recall in older adults undergoing BPH surgery. This intervention is a simple, easy-to-administer, and inexpensive method of adult education, providing a cost-effective solution for improving the effectiveness of health education for older surgical adults.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Ethics Approval
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the First Affiliated Hospital of Army Medical University (NO. (A)KY2025020) and registered with the Chinese Clinical Trial Registry (ChiCTR2500099704).
Consent for Publication
Informed consent was obtained from all adults involved in the study.
Acknowledgments
The authors would like to thank all adults in First Affiliated Hospital of the Army Medical University in Chongqing who participated in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sharkiya SH. Quality communication can improve patient-centred health outcomes among older patients: a rapid review. BMC Health Serv Res. 2023;23(1):886. doi:10.1186/s12913-023-09869-8
2. WHO. WHO strategic framework for effective communications. 2022, Available from: https://www.who.int/about/communications.
3. Kessels RP. Patients’ memory for medical information. J R Soc Med. 2003;96(5):219–222. doi:10.1177/014107680309600504
4. Awh E, Vogel EK. Working memory needs pointers. Trends Cognit Sci. 2025;29(3):230–241. doi:10.1016/j.tics.2024.12.006
5. Costa D, Serra R. The role of communication in managing chronic lower limb wounds. J Multidiscip Healthc. 2025;18:3685–3708. doi:10.2147/jmdh.S533416
6. Webber D, Higgins L, Baker V. Enhancing recall of information from a patient education booklet: a trial using cardiomyopathy patients. Patient Educ Couns. 2001;44(3):263–270. doi:10.1016/s0738-3991(01)00112-4
7. Cowan N. Working memory underpins cognitive development, learning, and education. Educ Psychol Rev. 2014;26(2):197–223. doi:10.1007/s10648-013-9246-y
8. Rotoli J, Moreland C, Mirus C. Implications of inadequate communication: emergency care for deaf and hard-of-hearing patients. Acad Emerg Med. 2025;32(3):374–376. doi:10.1111/acem.15040
9. Shankar J. Patients’ memory for medical information. J R Soc Med. 2003;96(10):520. doi:10.1177/014107680309601027
10. Lund CM, Mikkelsen MK, Theile S, et al. Age-related differences in recall of information and handling of chemotherapy-related side effects in cancer patients: the recap study. Oncologist. 2022;27(2):e185–e193. doi:10.1093/oncolo/oyab034
11. Lie HC, Juvet LK, Street Jr RL, et al. Effects of physicians’ information giving on patient outcomes: a systematic review. J Gen Intern Med. 2022;37(3):651–663. doi:10.1007/s11606-021-07044-5
12. Wilson EA, Wolf MS. Working memory and the design of health materials: a cognitive factors perspective. Patient Educ Couns. 2009;74(3):318–322. doi:10.1016/j.pec.2008.11.005
13. van Merriënboer JJ, Sweller J. Cognitive load theory in health professional education: design principles and strategies. Med Educ. 2010;44(1):85–93. doi:10.1111/j.1365-2923.2009.03498.x
14. Goodman C, Lambert K. Scoping review of the preferences of older adults for patient education materials. Patient Educ Couns. 2023;108:107591. doi:10.1016/j.pec.2022.107591
15. Chughtai B, Forde JC, Thomas DD, et al. Benign prostatic hyperplasia. Nat Rev Dis Primers. 2016;2(1):16031. doi:10.1038/nrdp.2016.31
16. Sandhu JS, Bixler BR, Dahm P, et al. Management of lower urinary tract symptoms attributed to Benign Prostatic Hyperplasia (BPH): AUA guideline amendment 2023. J Urol. 2024;211(1):11–19. doi:10.1097/ju.0000000000003698
17. Thomas LH, McColl E, Priest J, Bond S, Boys RJ. Newcastle satisfaction with nursing scales: an instrument for quality assessments of nursing care. Qual Health Care. 1996;5(2):67–72. doi:10.1136/qshc.5.2.67
18. Wolf MS, Gazmararian JA, Baker DW. Health literacy and functional health status among older adults. Arch Intern Med. 2005;165(17):1946–1952. doi:10.1001/archinte.165.17.1946
19. Gan JM, Riley J, Basting R, Demeyere N, Pendlebury ST. Decision-making capacity in older medical in-patients: frequency of assessment and rates of incapacity by decision-type and underlying brain/mind impairment. Age Ageing. 2023;52(9). doi:10.1093/ageing/afad171
20. Zou L, Zhang Z, Mavilidi M, et al. The synergy of embodied cognition and cognitive load theory for optimized learning. Nat Hum Behav. 2025;9(5):877–885. doi:10.1038/s41562-025-02152-2
21. McFarland DC, Shen MJ, Parker P, Meyerson S, Holcombe RF. Does hospital size affect patient satisfaction? Qual Manag Health Care. 2017;26(4):205–209. doi:10.1097/qmh.0000000000000149
22. Allenbaugh J, Corbelli J, Rack L, Rubio D, Spagnoletti C. A brief communication curriculum improves resident and nurse communication skills and patient satisfaction. J Gen Intern Med. 2019;34(7):1167–1173. doi:10.1007/s11606-019-04951-6
23. Trant AA, Szekely B, Mougalian SS, et al. The impact of communication style on patient satisfaction. Breast Cancer Res Treat. 2019;176(2):349–356. doi:10.1007/s10549-019-05232-w
24. Langewitz W, Ackermann S, Heierle A, Hertwig R, Ghanim L, Bingisser R. Improving patient recall of information: harnessing the power of structure. Patient Educ Couns. 2015;98(6):716–721. doi:10.1016/j.pec.2015.02.003
25. Świątoniowska-Lonc N, Polański J, Tański W, Jankowska-Polańska B. Impact of satisfaction with physician-patient communication on self-care and adherence in patients with hypertension: cross-sectional study. BMC Health Serv Res. 2020;20(1):1046. doi:10.1186/s12913-020-05912-0
26. Pollak KI, Olsen MK, Yang H, et al. Effect of a coaching intervention to improve cardiologist communication: a randomized clinical trial. JAMA Intern Med. 2023;183(6):544–553. doi:10.1001/jamainternmed.2023.0629
27. Navarro B, Liebendorfer A, Voorhees M, et al. Development and assessment of a patient “journey guide” for adult traumatic brachial plexus injury. J Bone Joint Surg Am. 2024;106(2):151–157. doi:10.2106/jbjs.23.00511
28. Leino-Kilpi H, Inkeroinen S, Cabrera E, et al. Instruments for patient education: psychometric evaluation of the Expected Knowledge (EKhp) and the Received Knowledge of Hospital Patients (RKhp). J Multidiscip Healthc. 2020;13:1481–1505. doi:10.2147/jmdh.S271043
29. Özkan ZK, Fındık ÜY. Determination of the effectiveness of informing with the guidance of an education booklet in patients undergoing colonoscopy-a randomized controlled trial. J Perianesth Nurs. 2020;35(5):502–507. doi:10.1016/j.jopan.2019.12.009
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.