Back to Journals » Risk Management and Healthcare Policy » Volume 19
Providers’ Perspectives and Experiences with Cost-Related Nonadherence to Medications: A Thematic Analysis
Authors Gheshlaghi N, Thomas MM, Manhas K ![]() , De Vera MA
, De Vera MA ![]()
Received 3 September 2025
Accepted for publication 14 February 2026
Published 10 March 2026 Volume 2026:19 564975
DOI https://doi.org/10.2147/RMHP.S564975
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Mecit Can Emre Simsekler
Niloofar Gheshlaghi,1,2 Megan M Thomas,1,2 Kimi Manhas,3 Mary A De Vera1,2,4
1Faculty of Pharmaceutical Sciences, University of British Columbia, Vancouver, BC, Canada; 2Collaboration for Outcomes Research and Evaluation, Vancouver, BC, Canada; 3Provincial Health Services Authority, Cardiac Services BC, Vancouver, BC, Canada; 4Centre for Advancing Health Outcomes, Vancouver, BC, Canada
Correspondence: Mary A De Vera, University of British Columbia, Faculty of Pharmaceutical Sciences, 2405 Wesbrook Mall, Vancouver, BC, V6T 1Z3, Canada, Tel +1-604-827-2138, Email [email protected]
Background: Cost-related medication nonadherence (CRNA), whereby patients do not take medications as prescribed due to their cost, negatively affects health outcomes. While patients’ experiences with CRNA have been characterized, studies have not explored providers’ perspectives. Our objective was to explore the experiences and perspectives of providers caring for patients facing CRNA.
Methods: We conducted a qualitative research study involving one-on-one interviews with individuals 18 years or older and work as health or allied health professionals in Metro Vancouver from August 2023 to April 2024. Interviews were transcribed verbatim and thematic analysis was applied which involved: data familiarization (reviewing transcripts, cross-checking with audio for accuracy); initial coding (labelling concepts in the transcripts); and theme formation (grouping similar codes to capture broader experiences).
Results: Altogether 16 providers participated (12 women, 3 men, 1 non-binary) from diverse disciplines. Thematic analysis led to three themes. The first theme, “how CRNA shapes practice” indicates that providers frequently deal with patients experiencing CRNA which is then associated with significant increases in workload. The second theme, “barriers to supporting patients through CRNA” suggests that most providers have no formal training to help them navigate CRNA and face time constraints in busy practices. The third theme, “making sense of CRNA within practice” highlights how providers conceptualize CRNA and how this then influences their responses to medication affordability challenges. Provider recommendations for addressing CRNA, included access to short-term funds, increased educational resources, and systemic organizational changes to increase provider supports.
Conclusion: CRNA affects not just patients, but also providers who care for them, revealing significant gaps in current systems of support. These insights underscore the need for coordinated policy action on medication affordability and the integration of structured resources within clinical settings to better equip providers to respond to CRNA.
Keywords: medication affordability, provider perspectives, medication nonadherence
Introduction
Cost-related medication nonadherence (CRNA) is characterized by patients taking less than the prescribed medication dose due to medication cost, for example by reducing daily dose, delaying refilling prescriptions, or frequency of medications.1–3 There are many risk factors associated with CRNA including food insecurity, low household income, lack of prescription drug coverage and high out of pocket costs.4–7 Per the 2021 Survey on Access to Health Care and Pharmaceuticals During the Pandemic, about 9% of Canadians (1 in 10) reported not adhering to their prescription due to cost related reasons; individuals without insurance reported CRNAs significantly more often (17% of individuals) than those with insurance (7% of individuals).8 Internationally, CRNA has been documented across high-income countries, including the United States, where patients pay comparatively more for prescription medicines, up to 20% of adults report CRNA,9 and Australia, where 9.4% of women and 5.5% of men report CRNA.10 These findings underscore CRNA as a broad concern with implications for patient safety across many countries. In Canada, where prescription medications are not universally covered under public health insurance, CRNA remains a persistent concern and is central to ongoing pharmacare policy discussions.
To develop meaningful solutions to combat CRNA, it is important to understand the experiences of those who are experiencing it firsthand. From the patients’ perspective, prior qualitative research studies from Canada describe experiences with CRNA.11,12 Collectively, these studies showed that patients’ experiences with CRNA were shaped by financial burden and its impact on well-being. Reported high cost of medications, multidrug therapies, and lack of drug insurance significantly led to CRNA with behaviours including skipping or splitting doses, delaying fills, not filling prescriptions, or substitution with non-optimal medications. Patients’ strategies for dealing with CRNA included borrowing money, seeking lower-cost substitutes, or requesting longer supplies to reduce the frequency of dispensing fees.
Prescribers (providers responsible for ordering medications for their patients) play a significant role in supporting adherence,13 however to our knowledge, there are no prior studies that assessed providers’ experiences with providing care for patients experiencing CRNA. Also overlooked are the experiences of non-prescribers (e.g., nurses, social workers, case workers) who often have close contact with patients during their treatments. To address these limitations, we aimed to explore providers’ experiences in supporting patients with CRNA and understand how CRNA affects them in their role as care providers.
Materials and Methods
Study Design and Setting
This study used a qualitative descriptive methodology14 to explore providers’ experiences with cost-related medication nonadherence, using an inductive thematic analysis approach based on Braun and Clarke’s framework.15 The setting of the study is the Lower Mainland of British Columbia, which is situated within a publicly funded healthcare system. This region was selected because it is the primary location of the research team, allowed feasible access to the study sample of providers, and represented relevant context for examining providers’ experiences with supporting patients with CRNA in a healthcare system where prescription medications are not universally covered.
Ethical Considerations
This study received approval from the Behavioral Research Ethics Board (H23-01874) at the University of British Columbia and was conducted in accordance with the ethical principles of the Declaration of Helsinki. All participants provided informed consent, which included agreement to the publication of anonymized responses/quotes. Participant confidentiality was maintained through the removal of identifying information from transcripts, separation of demographic and interview data, and reporting of only de-identified quotations.
Participants and Recruitment
For the purposes of our study, we define “provider” as a front-line worker with direct patient contact, including both prescribers and non-prescribers. Participants were invited if they: 1) worked in a setting where they have contact with patients; 2) ≥18 years of age; 3) able to speak English or French. Potential participants were identified using snowball sampling, a subset of purposive sampling, where colleagues working in healthcare settings were consulted for suggestions.16,17 A co-author (KM) conducted initial recruitment by emailing potential participants, sharing information about the study and directing them to the study consent form and demographic survey hosted on the UBC Survey Tool, powered by Qualtrics Research Core. In brief, the demographic survey comprised questions on participants’ role (eg, nurse, pharmacist, physician, other [with free text option]), care delivery setting (eg, inpatient, ambulatory clinic, outpatient), specialty (e.g. community health, family practice, medicine, surgery, other [with free text option]), years in the role, sex, gender, and race.
Data Collection
Participants took part in one-on-one semi-structured interviews, conducted by the primary author, who is a pharmaceutical sciences researcher with training in qualitative research methods (NG) for consistency, and supported using the video conferencing platform Zoom (version 5.16.2). Semi-structured interviews were chosen to allow for consistency across participants while providing flexibility to explore individual experiences and perspectives in greater depth, aligning with the study’s exploratory objectives. Interviews were conducted once per participant. A semi-structured interview guide, developed by the research team with diverse expertise in content areas (e.g. medication adherence research), methodologies (e.g. qualitative research), and clinical practice, was used to facilitate conversations (positionality statements found in Supplementary Table 1). This interview guide comprised ten open-ended questions surrounding the experiences and perspectives of providers with CRNA (Supplementary Table 2). Interviews were conducted until saturation point, that is, when interview responses became repetitive across participants and no additional insights were found.18 Saturation was assessed iteratively during concurrent data collection and analysis, and was confirmed through team discussions when additional interviews reinforced existing codes and themes.
Data Analysis
Thematic analysis, a qualitative method for identifying patterns or themes, was chosen for this study due to its suitability for exploring experiences and beliefs.19 An inductive approach was employed, analyzing the data without preconceived outcomes, following a “bottom-up” process based on Braun and Clarke’s framework.15 First, during data familiarization, transcripts were reviewed for accuracy. The initial coding stage involved tagging recurring concepts across the transcripts, which were then grouped into “parent codes” to facilitate theme development. Next, the codes were organized into broader themes, with each theme named based on dominant patterns. These themes were then iteratively refined through discussion within the research team. During this refinement process, we ensured that the themes accurately represented participants’ experiences evaluated subthemes for their independence and overlap, clarified the language for semantic precision, and verified the final set of themes. Throughout the analysis, the research team engaged in reflexive discussions to consider how their backgrounds and assumptions might influence interpretation and to ensure that themes were grounded in participants’ accounts. Interview audio was recorded via Zoom and then transcribed using SONIX, an AI transcription speech to text software and subsequently uploaded to the qualitative data analysis software Nvivo (version 14.23.0).
Results
Providers
Altogether, 16 providers participated interviews which ranged from 30 to 70 minutes in duration. Participants were predominantly women and White (75%) but had significant diversity in worksite and role. Eight participants worked out of community sites, four out of ambulatory clinics, three in acute care, one in primary care and one in a corporate office. Of the professions, pharmacists (clinical and community) were most represented, albeit each from a different work site (e.g. ambulatory clinic, community) and therefore with a varying set of perspectives. Two participants currently in administrative roles were interviewed, providing the administrative perspective on the issue of cost. Nine participants fall into the early-career stage, three in mid-career, and four in the later career stage. Participants predominantly worked in the city of Vancouver, with two working in Burnaby and/or Richmond. Participant characteristics are summarized in Table 1.
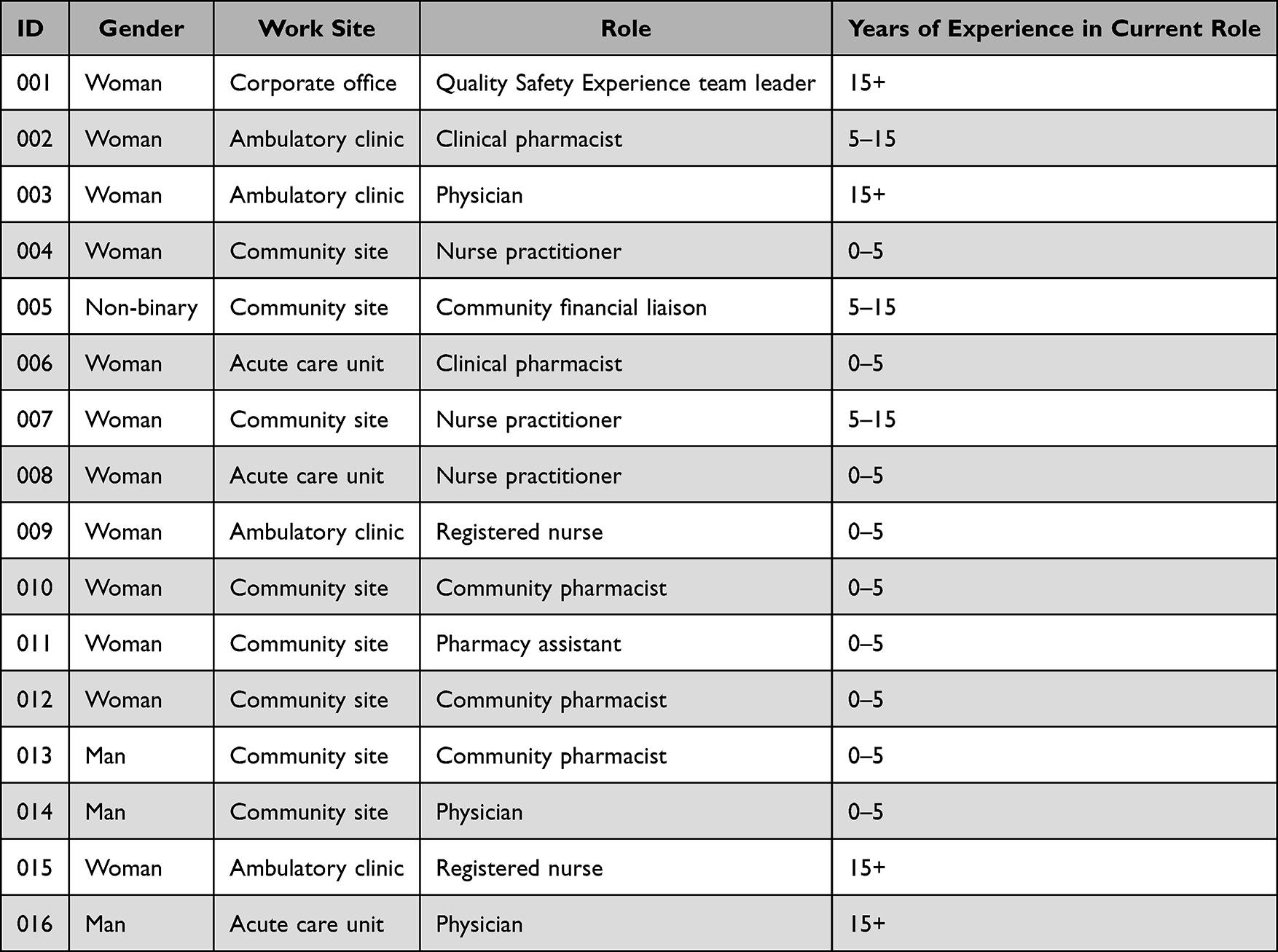 |
Table 1 A Summary of Provider Characteristics |
Thematic Analysis
Thematic analysis of the interview transcripts initially generated 37 codes, which were iteratively refined and organized into in three overarching themes: 1) how CRNA shapes practice, 2) barriers to supporting patients through CRNA, and 3) making sense of CRNA within practice. Several subthemes within each theme capture various associated aspects of participants’ experiences. The themes and corresponding subthemes are illustrated in Figure 1 and illustrative quotes are provided in Table 2.
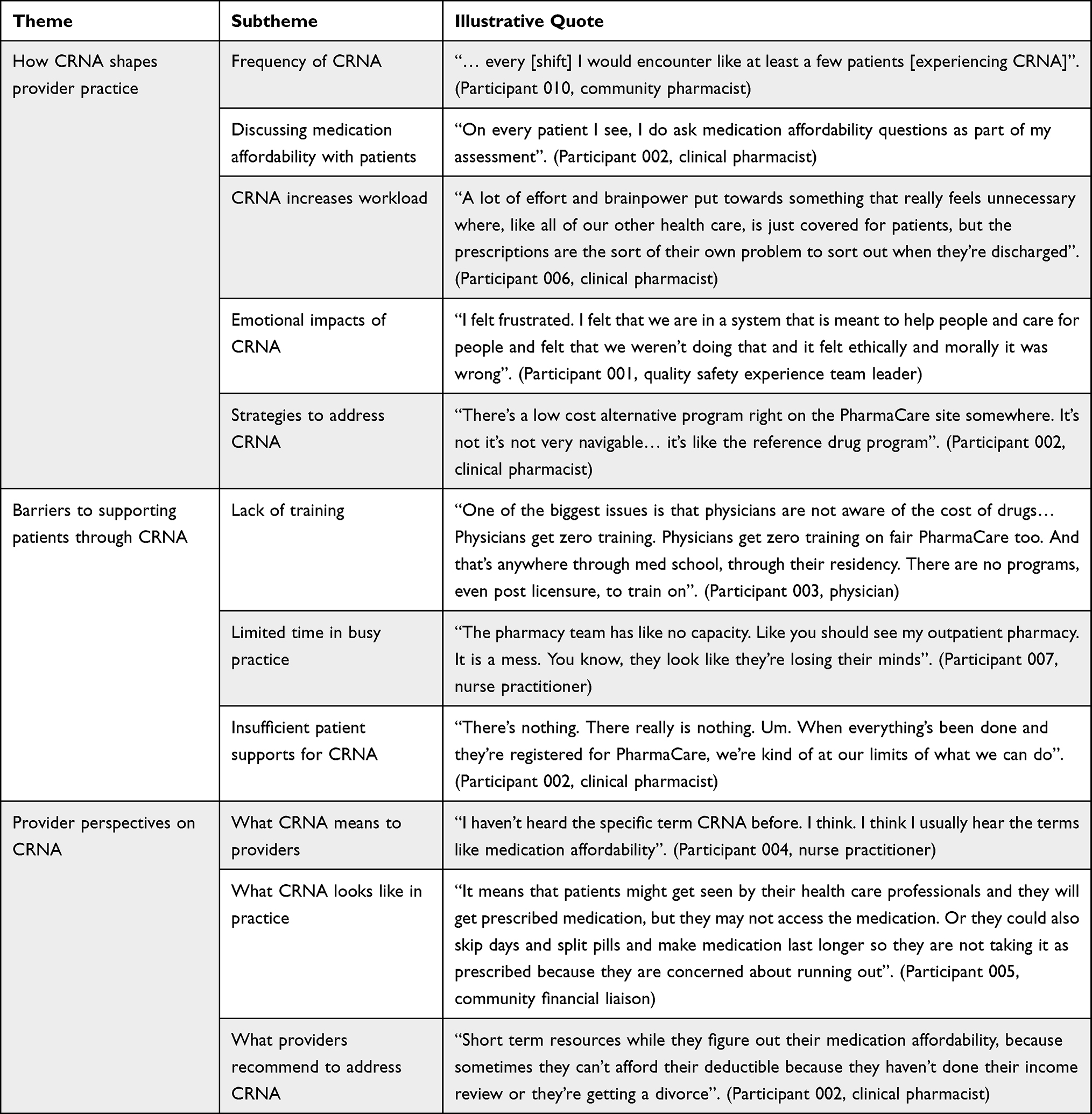 |
Table 2 Summary of Themes and Subthemes with Illustrative Quotes |
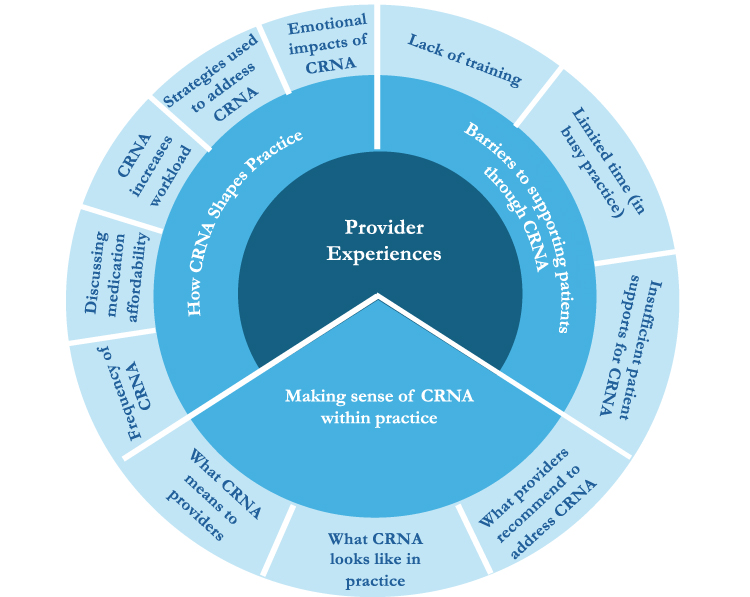 |
Figure 1 Themes (in light blue) and subthemes (in pale blue) from interviews describing providers’ experiences and perspectives with CRNA. |
Theme 1: How CRNA Shapes Provider Practice
The theme “how CRNA shapes provider practice” describes how CRNA influences providers’ practices, both consciously and unconsciously. This theme comprises five subthemes: 1) frequency of CRNA, 2) discussing medication affordability (with patients), 3) CRNA increases workload, 4) strategies used to address CRNA, and 5) emotional impacts of CRNA.
Frequency of CRNA
When reflecting on how often they observe CRNA in their practices, providers shared a wide range of experiences – ranging from “a patient every two to three weeks” in outpatient clinics to “a few patients every eight-hour shift” in a pharmacy. The provider’s role and practice setting may explain such diverse experiences. For example, we found that pharmacists in all settings tend to interact with more patients experiencing CRNA as compared to physicians or nurse practitioners. Many participants stated that they believed pharmacists were most knowledgeable on the topic of medication costs and coverage:
Our pharmacist I think, are more well versed in it than the nurses. (Participant 009, registered nurse)
Presumably because they are viewed as a knowledgeable resource, medication concerns tend to be redirected to pharmacists, especially when experiencing time constraints. For example, a respondent stated that if a case was taking
… too much of my time, then I do have a clinical pharmacist that I can … I can send it [to]. (Participant 008, nurse practitioner)
With respect to practice setting, providers in outpatient settings were also more likely to encounter patients experiencing CRNA than those in inpatient settings. Despite the variability in frequency of cases, most providers in all roles and settings stated overwhelmingly that CRNA is a significant issue for their practice.
Discussing Medication Affordability with Patients
Participants shared that patients rarely bring up the cost of medications; the onus falls on the provider to initiate these conversations. Providers observed that patients are often hesitant to discuss their ability to afford medications, and the topic typically arises only when concerns emerge about a condition not being managed as expected, as noted by this participant:
…[patients are] not coming to us and saying specifically, oh, this isn’t working, I can’t afford these. Instead, they’re sort of doing their own thing. And then if we find out that they’re doing it, [it’s] usually because of something going wrong, and we talked to them about it, [and] it’s usually because of money. (Participant 009, registered nurse)
Our analysis also suggests that providers generally fall into two broad categories: those who are conscious of medication costs and those who consider costs only when prompted by external factors. With respect to the former, some participants shared being
…very conscious of the cost of medications and usually will ask if patients can afford a medication. (Participant 003, physician)
Some providers also include questions about medication affordability as part of their assessment as captured by this quote:
On every patient I see, I do ask medication affordability questions as part of my assessment. (Participant 002, clinical pharmacist)
Those who do not immediately consider the cost of medications shared that they prioritize information on other factors such as
their medications if they get sick or, side effects to watch for… (Participant 009, registered nurse)
Some providers also shared that they “forget the cost piece a lot” (Participant 010, community pharmacist) amongst all their responsibilities.
CRNA Increases Workload
Providers consistently described CRNA as a significant contributor to increased workload, particularly when supporting patients in navigating medication affordability. This burden manifests both proactively—when providers attempt to assess or address potential cost-related barriers before prescribing—and reactively—when CRNA behaviours come to light after treatment has begun. For example, one participant described CRNA as a “huge workload burden” (Participant 002, clinical pharmacist), especially when conversations about insurance coverage or income-based eligibility are required. The process of applying for special authority or navigating public coverage restrictions was cited frequently, particularly by providers working on smaller sites with limited access to specialists. As one participant noted,
It’s definitely a struggle to get medications covered for patients where the special authority criteria requires them to speak with specialists to get coverage. (Participant 006, clinical pharmacist)
When patients report CRNA after a prescription is written, providers often must “circle back more than once with the same patient” (Participant 009, registered nurse), renegotiating treatment plans, coordinating with other clinicians, or sourcing alternative medications. This can feel like unraveling a carefully developed care plan, as described by a clinical pharmacist:
You’re pulling in…other people that you’re engaging in the care of this patient just to get [them] on more streamlined, affordable medications. It’s just very time consuming. (Participant 002, clinical pharmacist)
Ultimately, providers emphasized that addressing CRNA often requires the time and coordination equivalent to caring for multiple patients, especially when affordability concerns were not considered from the outset.
Strategies Used to Address CRNA
While providers agreed there is no standardized approach to addressing CRNA, they described relying on a range of ad hoc strategies to support patients. These generally fell into two main categories: leveraging existing resources and providing supplementary supports. Among existing resources, a common approach was applying for special authority coverage, particularly for medications listed under the BC PharmaCare formulary. This process, although time-consuming, was viewed by many participants as essential to securing partial or full coverage for patients. Another frequently used strategy was altering prescriptions to reduce costs, which included substituting brand name drugs with generics, adjusting dosages to reduce pill burden, or selecting lower-cost alternatives from the same therapeutic class. As one participant noted, this often means prescribing “second-best medications” (Participant 009, registered nurse), but doing so “solves the problem… at least they’re being treated”. Providers also worked to optimize PharmaCare coverage, encouraging patients to register for Fair PharmaCare or layering multiple plans to increase coverage potential. However, participants noted barriers to this approach, including patients not filing taxes, or lack of ID. When formal coverage options were exhausted, providers turned to supplementary resources such as manufacturer cards and free samples, which were described as helpful short-term solutions but unsustainable for long-term management. In some cases, clinics had access to discretionary funds or, as one provider described, “slush funds” to cover medication costs for patients in crisis. As one participant explained,
We’ll try and pay for people’s medications just for the humanity of it. Because without treatment, there’s a 50% mortality rate in two years. (Participant 002, clinical pharmacist)
While these strategies helped mitigate the impact of CRNA, providers emphasized their patchwork nature and the need for more structured supports.
Emotional Impacts of CRNA
Providers described impacts tied to caring for patients experiencing CRNA, which tended to cluster into three types of emotional responses: distress, frustration, and resignation. Feelings of distress often emerged when providers perceived a mismatch between their role in a “system meant to help people” (Participant 001, quality safety experience team leader) and their actual ability to support patients. Many described moral discomfort when unable to secure necessary medications, leading to sentiments such as feeling heavy hearted or that the situation felt wrong or distressing. One provider, reflecting on discharging patients without medications they could not afford, described it as “a death sentence” (Participant 002, clinical pharmacist). Frustration was also common, particularly among those navigating bureaucratic barriers and facing time-intensive processes to secure coverage. As one pharmacist noted:
You spend most of your time trying to get it covered for them. (Participant 006)
Resignation emerged in settings where providers regularly encountered CRNA, such as community pharmacies. Some described becoming emotionally desensitized to repeated cases:
It doesn’t faze me too much… I just have to tell them the same thing. (Participant 010, community pharmacist)
Though they still felt for their patients, these providers expressed a sense of helplessness and acknowledged there was “nothing they could do”, pointing to the cumulative toll of witnessing repeated instances of unmet need.
Theme Two: Barriers to Supporting Patients Through CRNA
Providers identified several barriers that limited their ability to support patients experiencing CRNA, largely reflecting broader constraints related to training, time, and supports for patients. Correspondingly, these barriers fell into three subthemes of: 1) lack of training, 2) limited time (in busy practice), and 3) insufficient patient supports for CRNA.
Lack of Training
Providers described a gap in education and training related to medication affordability and CRNA. Most reported that their understanding of these issues came not from formal education, but from learning “on the job” often in response to patient distress. As one participant noted.
The only way I’ve learned about [medication coverage] is having these patients get upset… (Participant 011, pharmacy assistant)
This lack of training was reported across roles. Similarly, pharmacists and nurse practitioners noted that medication costs and coverage were “not really discussed” in their schooling (Participant 006, clinical pharmacist), and several participants said they were unsure how to navigate programs like special authority coverage. Others mentioned relying on their own searches to find drug cost information, highlighting the lack of accessible, centralized resources. In addition to limited knowledge, providers emphasized the absence of clear guidance or protocols for supporting patients facing CRNA. “I’ve never received any kind of guidance or tools or processes to work with”, shared one nurse practitioner (Participant 009). Another participant stated plainly, “Physicians get zero training” on medication affordability, from medical school through residency (Participant 003). Across roles and settings, providers echoed that CRNA is rarely addressed in training, leaving them to develop their own informal, reactive approaches to patient care.
Limited Time in Busy Practice
Time constraints were a consistent barrier to addressing CRNA, often compounding the lack of training for providers. Many described their workloads as a “never-ending struggle” (Participant 003, clinical pharmacist), leaving little room for conversations about medication affordability during clinical encounters. As one participant noted, “I don’t think people have the time to have these conversations” given competing demands and the volume of patients seen each day (Participant 001, quality safety experience team leader). Some providers made a conscious decision to focus on the clinical responsibilities they are uniquely trained to deliver, delegating affordability concerns to other team members. For example, one nurse practitioner shared that ensuring a patient was enrolled in Fair PharmaCare was “not [their] job”, and should fall to a social worker (Participant 007). In pharmacies, where time pressures were especially acute, providers described teams that “barely stop moving” and appeared overwhelmed (Participants 005 and 007). Pharmacists themselves admitted that cost often falls off the radar until the final step of adjudication, when the receipt reminds them of the issue.
Insufficient Patient Supports for CRNA
Although providers described using various strategies to support patients experiencing CRNA, they consistently felt these resources were limited and often inadequate. For example, concerns were raised about special authority coverage, which may only fund a portion of a recommended treatment course. Providers also expressed frustrations with Fair PharmaCare, citing a general lack of patient awareness about the program and confusion around how coverage works. One pharmacist noted that “a lot of people don’t know that they have to sign up” or understand how the system functions (Participant 010). Even when patients are registered, many struggle to afford their deductibles, which are based on income reported two years prior. As one provider explained,
People could be pretty rich two years ago and they could be broke now. (Participant 005, community financial liaison)
The result is that affordability remains a barrier even for those formally enrolled in the system. Beyond these programs, providers described hitting a wall in terms of available options. Samples were described as unreliable— “the samples dry up” (Participant 002, clinical pharmacist)—and once all avenues were exhausted, many felt there was simply nothing more they could do. As one participant put it, “We’re kind of at our limits of what we can do” (Participant 002), underscoring a shared sense of helplessness in the face of limited patient supports for CRNA.
Theme 3: Making Sense of CRNA within Professional Practice
This final theme captures how providers make sense of and interpret CRNA, adding context to their experiences and shaping how they respond to patients facing medication affordability challenges. While most had never encountered the specific term “cost-related nonadherence” in practice, they immediately recognized the concept. Some used the term “medication affordability” instead, describing CRNA as situations where patients reduce, delay, or forgo medications due to cost—such as splitting doses, using expired prescriptions, or not filling medications at all. When asked about who is most affected, providers noted it was difficult to generalize but pointed to those without private insurance, individuals earning above the PharmaCare subsidy threshold, and patients unfamiliar with the healthcare system, including newcomers to Canada. Many emphasized that CRNA is common, often going unnoticed until follow-up visits when treatment plans fail or patients disclose affordability barriers. Examples of CRNA in practice included patients abandoning prescriptions due to cost, not initiating treatment plans, or delayed recognition that coverage applications were never completed. Finally, participants offered several recommendations to better support patients and providers. These included patient-facing solutions such as a “large scale slush fund” or volunteer-run clinics for navigating medication costs, and provider-focused tools like a centralized database of support resources and embedding affordability questions into standard health assessments. Altogether, these provider perspectives highlight the need for both system-level reform and practice-level supports to meaningfully address CRNA.
Discussion
This study explored how providers experience and respond to patients experiencing CRNA. Through semi-structured interviews with 16 providers across diverse roles and settings in Metro Vancouver, it became clear that CRNA is a frequent and impactful issue—one that not only affects patient outcomes, but also significantly shapes provider workload, emotional well-being, and decision-making. While providers described developing ad hoc strategies to support patients, they frequently felt underprepared, unsupported, and emotionally burdened in doing so. Barriers such as lack of training, limited time during patient encounters, and insufficient patient supports further complicated their ability to intervene effectively. Although the specific term “CRNA” was unfamiliar to most participants, the concept was well recognized. Unsurprisingly, provider recommendations for addressing CRNA emphasized the need for improved education, better access to practical tools, and patient-facing supports like short-term financial aid and dedicated resources to navigate coverage systems.
Findings of our qualitative study among providers reflect existing literature on CRNA. For example, a 2021 systematic review estimated the prevalence of CRNA in Canada to range between 5.1% and 10.2%,1 aligning with providers’ observations of its frequency in practice. A number of qualitative studies have explored patients’ experiences and perspectives on CRNA. Patients commonly reported behaviours such as skipping or delaying medications, borrowing money, requesting free samples, or substituting prescriptions with less effective over-the-counter alternatives.12,20,21 These actions were often driven by financial strain, limited insurance coverage, and inadequate discussions with providers about medication costs—underscoring the difficult trade-offs patients are forced to make between their health and financial well-being.
To our knowledge, this is the first qualitative research study to focus specifically on healthcare providers’ perspectives and experiences with CRNA. The most closely related study is one from 2022 US study by Hamilton et al which included both patients and providers to examine intentional and unintentional nonadherence among individuals with depression and diabetes.22 Although CRNA was not the primary focus, providers in that study identified medication cost as a key social determinant contributing to unintentional nonadherence, often noting that patients were unable to afford prescriptions and returned with uncontrolled symptoms. Our study builds on this foundation by offering a focused exploration of CRNA through the lens of providers. In doing so, it reveals how deeply these cost-related challenges affect not only patient outcomes, but also providers’ emotional well-being, workload, and sense of responsibility—highlighting a critical yet underexplored dimension of CRNA in clinical practice.
Altogether, the findings of this study highlight the pressing need to address CRNA more systematically within clinical practice. Providers emphasized that failure to assess a patient’s ability to afford medications at the time of prescribing often results in disrupted care, including missed or delayed treatments, unnecessary follow-up visits, and emotional distress for both patients and providers. In particular, the emotional burden described by providers can be understood through moral distress and provider burnout. Moral distress arises when clinicians recognize ethically appropriate actions but are constrained by systemic barriers from carrying them out, while burnout reflects the cumulative psychological strain associated with such constraints. As participants suggested, questions about medication affordability should be integrated into routine prescribing workflows—alongside other standard considerations such as allergies or preferred formulations. Framing these questions as a routine part of care may reduce stigma and encourage more open dialogue about cost concerns. However, for such conversations to be effective, providers must also be equipped with the knowledge and resources to respond appropriately. Many participants reported receiving little to no formal training on medication costs, drug coverage systems, or strategies to help patients navigate affordability barriers. This lack of preparation left them feeling frustrated and ineffective in supporting their patients. To address this gap, participants recommended embedding medication affordability content into health professional education—both at the undergraduate level and through continuing education. Evidence from other jurisdictions suggests that even brief educational interventions can significantly increase provider awareness of drug costs and promote cost-sensitive prescribing behavior.
In addition to calling for improved provider education, participants emphasized the need for broader systemic reforms to support patients more directly. Key recommendations included expanding the eligibility and responsiveness of public drug coverage programs—particularly Fair PharmaCare in British Columbia, given the study’s setting—increasing transparency around drug pricing and offering interim solutions such as short-term medication funds or community-based medication counselling clinics. These suggestions reflect a shared recognition that addressing CRNA requires coordinated action at multiple levels: clinical, educational, and policy. The findings also highlight the pressing relevance of Canada’s evolving national pharmacare strategy. Recent commitments by the federal government to build a universal pharmacare system—beginning with free coverage of diabetes medications and contraception—represent an important step toward improving access, affordability, and equitable medication use across the country.23 Providers in this study described how existing gaps in drug coverage—at the time of data collection—led to delayed care, unmanaged symptoms, and repeated clinical encounters driven by cost-related nonadherence. While the recent introduction of national pharmacare marks a promising policy shift, it will take time to realize its full impact. A truly universal and comprehensive pharmacare program remains essential to addressing the persistent burden of CRNA—for both patients navigating affordability barriers and the providers who care for them. As this framework evolves, insights from frontline clinicians, such as those shared in this study, will be critical to informing a pharmacare system that is not only equitable, but also clinically responsive and sustainable. Addressing CRNA is a long-term undertaking, but progress is within reach and urgently needed.
A strength of our study is the inclusion of providers from diverse professional backgrounds and care settings, which enabled a nuanced comparison of how CRNA is experienced across sectors. This is particularly important within the context of a fragmented Canadian healthcare system, where providers often operate in silos—even when caring for the same patient. Despite this diversity, consistent themes emerged across interviews, including a shared recognition of the emotional distress caused when providers are unable to meet patients’ needs due to cost barriers. The consistency of these experiences underscores the pervasiveness of CRNA and suggests the findings are likely transferable across similar healthcare contexts. However, the study is not without limitations. The use of snowball sampling—while useful for recruiting participants with direct experience relevant to the research question—meant that the sample was limited to individuals within the professional circles of clinical collaborators. As a result, the perspectives captured may not fully represent the broader range of experiences across the province or country.
Conclusions
Altogether, this study offers important insights into how CRNA is experienced by healthcare providers and the challenges they face in supporting affected patients. By centering provider perspectives, we gain a fuller understanding of how CRNA disrupts clinical care and contributes to provider distress. These findings underscore the need for more robust infrastructure, training, and policy supports to ensure that medication affordability is not a barrier to effective and compassionate care. With the understanding that providers require robust supports to reduce the burden of CRNA, future work should expand on this foundation, both by engaging a broader range of provider voices and by evaluating interventions aimed at reducing this burden across the healthcare system. Ultimately, in healthcare systems where medication costs remain a barrier to adherence, reliance on ad hoc solutions and provider goodwill is neither equitable nor sustainable, underscoring the need for systemic approaches to medication access.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Holbrook AM, Wang M, Lee M, et al. Cost-related medication nonadherence in Canada: a systematic review of prevalence, predictors, and clinical impact. Syst Rev. 2021;10(1):11. doi:10.1186/s13643-020-01558-5
2. Law MR, Cheng L, Dhalla IA, Heard D, Morgan SG. The effect of cost on adherence to prescription medications in Canada. CMAJ. 2012;184(3):297–12. doi:10.1503/cmaj.111270
3. Law MR, Cheng L, Kolhatkar A, et al. The consequences of patient charges for prescription drugs in Canada: a cross-sectional survey. CMAJ Open. 2018.;6(1):E63–E70. doi:10.9778/cmajo.20180008
4. Men F, Gundersen C, Urquia ML, Tarasuk V. Prescription medication nonadherence associated with food insecurity: a population-based cross-sectional study. CMAJ Open. 2019 ;7(3):E590–E597. doi:10.9778/cmajo.20190075
5. Briesacher BA, Gurwitz JH, Soumerai SB. Patients at-risk for cost-related medication nonadherence: a review of the literature. J Gen Intern Med. 2007;22(6):864–871. doi:10.1007/s11606-007-0180-x
6. Leung VC, Jin Y-P, Hatch W, et al. The relationship between sociodemographic factors and persistence with topical glaucoma medications. J Glaucoma. 2015;24(1):69–76. doi:10.1097/IJG.0000000000000081
7. Lummis HL, Sketris IS, Gubitz GJ, Joffres MR, Flowerdew GJ. Medication persistence rates and factors associated with persistence in patients following stroke: a cohort study. BMC Neurol. 2008;8:25. doi:10.1186/1471-2377-8-25
8. Government of Canada SC. Pharmaceutical access and use during the pandemic. 2022.
9. Dusetzina SB, Besaw RJ, Whitmore CC, et al. Cost-related medication nonadherence and desire for medication cost information among adults aged 65 years and older in the US in 2022. JAMA Network Open. 2023;6(5):e2314211. doi:10.1001/jamanetworkopen.2023.14211
10. Ghinea N. Cost barriers to medication access in Australia: an analysis of the patient experience survey in context. Med J Aust. 2024;221(8):414–416. doi:10.5694/mja2.52427
11. Goldsmith LJ, Kolhatkar A, Popowich D, Holbrook AM, Morgan SG, Law MR. Understanding the patient experience of cost-related non-adherence to prescription medications through typology development and application. Soc Sci Med. 2017;194:51–59. doi:10.1016/j.socscimed.2017.10.007
12. Yaphe H, Adekoya I, Steiner L, Maraj D, O’Campo P, Persaud N. Exploring the experiences of people in Ontario, Canada who have trouble affording medicines: a qualitative concept mapping study. BMJ Open. 2019;9(12):e033933. doi:10.1136/bmjopen-2019-033933
13. Khan R, Socha-Dietrich K. Investing in medication adherence improves health outcomes and health system efficiency: adherence to medicines for diabetes, hypertension, and hyperlipidaemia. OECD Publishing; 2018. Report No.105. doi:10.1787/8178962c-en
14. Tenny S, Brannan JM, Brannan GD. Qualitative Study. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024.
15. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
16. Snowball Sampling. Human Research Protection Program and Institutional Review Board. Oregon State University. Division of Research and Innovation; 2012. https://research.oregonstate.edu/ori/irb/policies-and-guidance-investigators/guidance/snowball-sampling.
17. Purposive sampling Business Research Methodology. Research-Methodology; 2023 https://research-methodology.net/sampling-in-primary-data-collection/purposive-sampling/.
18. Hennink M, Kaiser BN. Sample sizes for saturation in qualitative research: a systematic review of empirical tests. Soc Sci Med. 2021;292:114523. doi:10.1016/j.socscimed.2021.114523
19. Maguire M, Delahunt B. Doing a thematic analysis: a practical, step-by-step guide for learning and teaching scholars. All Irel J High Educ. 2017;9(3).doi:10.62707/aishej.v9i3.335
20. Zheng B, Poulose A, Fulford M, Holbrook A. A pilot study on cost-related medication nonadherence in Ontario. J Popul Ther Clin Pharmacol. 2012 : 12;19(2):e239–247.
21. Sanyal C, Ingram EL, Sketris IS, Peltekian KM, Kirkland S. Coping strategies used by patients infected with Hepatitis C virus who are facing medication costs. Can J Hosp Pharm. 2011;64(2):131–140. doi:10.4212/cjhp.v64i2.997
22. Hamilton JE, Blanco E, Selek S, et al. Patient and provider perspectives on medication non-adherence among patients with depression and/or diabetes in diverse community settings – a qualitative analysis. PPA. 2022;16:1581–1594. doi:10.2147/PPA.S328785
23. Stanbrook MB. The first, fragile foundations of national pharmacare in Canada. CMAJ. 2024;196(40):E1347–E1348. doi:10.1503/cmaj.241650
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.