Back to Journals » International Journal of Women's Health » Volume 17
Protocols for Endometrial Preparation and Endometrial Pattern Before Embryo Transfer in Patients with Asherman Syndrome
Authors Xiong W, Liu Y, Zhang L, Yang C
Received 11 February 2025
Accepted for publication 21 May 2025
Published 31 May 2025 Volume 2025:17 Pages 1605—1614
DOI https://doi.org/10.2147/IJWH.S521964
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Vinay Kumar
Wenqian Xiong, Yi Liu, Ling Zhang, Chun Yang
Department of Obstetrics and Gynecology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, People’s Republic of China
Correspondence: Chun Yang, Department of Obstetrics and Gynecology, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430022, People’s Republic of China, Email [email protected]
Background: Endometrial thickness measurement (EMT) is not a reliable predictor of clinical pregnancy in Asherman syndrome (AS) patients. The aim of this study is to investigate the impact of endometrial patterns on reproductive outcomes in patients with AS for both fresh and frozen embryo transfers. Additionally, it is essential to determine the preferred endometrial preparation protocol for women in this population who are planning frozen embryo transfer (FET).
Methods: Seventy-six patients diagnosed with Asherman syndrome underwent hysteroscopic adhesiolysis followed by in vitro fertilization-embryo transfer (IVF-ET) at Union Hospital of Huazhong University of Science and Technology between February 2019 and July 2021. This study reviewed the endometrial patterns of 134 embryo transfers and the endometrial preparation protocols of 127 frozen embryo transfer (FET) cycles within this cohort of patients.
Results: The triple-line endometrial pattern before embryo transfer (ET) was found to be a significant predictor of a positive clinical pregnancy outcome (odds ratio 0.315, P = 0.007) and a successful live birth (odds ratio 0.306, P = 0.009). Moreover, the gonadotropin-releasing hormone agonist (GnRHa) downregulation in conjunction with hormone replacement therapy (HRT) protocol showed improvements in both the clinical pregnancy rate (odds ratio 0.218, P = 0.005) and live birth rate (odds ratio 0.362, P = 0.049) compared to the HRT protocol in FET cycles.
Conclusion: A triple-line endometrial pattern before embryo transfer is associated with successful clinical pregnancy and live birth in AS patients undergoing IVF. Additionally, the GnRHa+HRT protocol may increase the clinical pregnancy and live birth rates in AS women undergoing FET cycles.
Keywords: asherman syndrome, FET, IVF, endometrial pattern, endometrial preparation protocol
Introduction
Asherman syndrome results in endometrial fibrosis, where the functional layer is replaced by an unresponsive epithelial monolayer and fibrotic synechiae, leading to indistinguishability between the functional and basal layers.1 Transvaginal ultrasound is routinely used in assisted reproduction technology (ART) to evaluate endometrial receptivity. Some studies have indicated positive associations between endometrial thickness, pattern or both and the reproductive outcomes in IVF cycles;2,3 however, others have found no relationship.4–6 Nevertheless, few studies have focused on the impact of endometrial thickness and pattern on predicting IVF clinical outcomes in AS patients. In 2020, Movilla et al found that the endometrial thickness measurements were not correlated with the clinical pregnancy rate in AS patients.7 Therefore, should endometrial pattern serve as a predictor of clinical pregnancy rate or live birth rate in AS patients?
The hormone replacement therapy (HRT) protocol is the most commonly used method for endometrial preparation in FET cycles due to its flexibility and convenience.8 The ovarian stimulation (OS) protocol is used to mimic the natural process of follicular development and facilitate endogenous estradiol through ovulation induction. The utilization of gonadotropin-releasing hormone agonist (GnRHa) downregulation in conjunction with HRT, known as GnRHa+HRT, effectively inhibits unintended ovulation throughout the HRT cycle. The administration of GnRH agonist results in the downregulation of the pituitary gland, thereby suppressing the secretion of endogenous estrogen, inhibiting endometrial growth, and impeding follicle development.9 Recent retrospective studies suggest that a decrease in estrogen levels could extend the “window of implantation”.10 Additionally, a reduction in LH surge may enhance endometrial receptivity, while an increase in cytokine levels could facilitate embryo adhesion.11,12 Previous researches compared different protocols for endometrial preparation, yielding inconsistent results.13–16 However, few studies have compared different endometrial preparation protocols for AS patients undergoing FET.
Our primary object was to investigate the potential association between the endometrial pattern of AS patients undergoing IVF and their clinical outcomes, including clinical pregnancy rate and live birth rate. Additionally, we aimed to evaluate the impact of different endometrial preparation protocols on the clinical pregnancy rate and live birth rate of AS women undergoing FET.
Materials and Methods
Data Collection
Electronic records for female patients who underwent hysteroscopic adhesiolysis at the Union Hospital of Huazhong University of Science and Technology from February 2019 to July 2021 were reviewed. All patients in the study underwent transcervical resection of adhesions (TCRA), leading to the complete restoration of the normal anatomy of the uterine cavity. In this study, all patients who subsequently attempted conception via IVF-ET in our reproductive center. This retrospective cohort study was approved by the Medical Ethics Committee of the Union Hospital, Tongji Medical College, Huazhong University of Science and Technology. Written informed consent was obtained from all patients. This study complied with the Declaration of Helsinki. The methods were conducted in accordance with the applicable guidelines and regulations. Medical records including age, history of miscarriage, pre-hysteroscopy menstrual pattern, disease course, anti-Müllerian hormone (AMH), body mass index (BMI), preoperative endometrial thickness during the late proliferation phase, maximum endometrial thickness, endometrial pattern in the cycle prior to ET, intrauterine adhesions (IUA) appearance, IUA area, the count of visible uterine cornua or tubal ostia, European Society of Gynecological Endoscopy (ESGE) classification, the number of TCRA, endometrial preparation protocols of FET cycles, embryo type (fresh vs frozen), embryo age at the time of ET (D3 embryo or D5 blastocyst), total number of embryos transferred, number of high-quality embryos transferred, and reproductive outcomes following ART were extracted from the medical record system. High-quality embryos were defined as embryos that reached 7 to 9-cell stage with cytoplasmic fragmentation occupying less than 15% of the embryo surface and had equal size blastomeres. Gardner and Schoolcraft scoring system17 was adopted to assess the quality of blastocyst. The quality of blastocysts was classified as high (AA, AB, BA, and BB), fair (AC, CA, BC, and CB), or poor (CC). Clinical pregnancy rates were calculated by dividing the number of clinical pregnancies by the total number of embryo transfer cycles. Similarly, live birth rates were determined by dividing the number of live births by the total number of embryo transfer cycles.
Patient Selection
The inclusion criteria of AS patients were as follows: (1) IUA was confirmed by hysteroscopy; (2) patients attempting conception through IVF-ET in our hospital; (3) all patients underwent TCRA by the same experienced surgeon; (4) women aged 20–45 years and (5) the surgery was performed between February 2019 and July 2021 in our hospital. The exclusion criteria were as follows: (1) AS due to tuberculosis; (2) other intrauterine diseases (ie, polyps, submucosal myomas); (3) patients with severe systemic disease or contraindications for estrogen therapy or surgery; (4) patients attempted conception spontaneously.
Treatment of Asherman Syndrome
Patients referred to our hospital for management of AS undergo both a transvaginal 3-dimensional ultrasound and a diagnostic/therapeutic hysteroscopy. All patients were completely lysed utilizing hysteroscopic scissors alone until normal uterine cavity anatomy is restored. All patients received IUA severity score according to the European Society of Gynecological Endoscopy classification (ESGE, 1995).18 Adhesiolysis was performed under direct observation and monitored by ultrasonography if necessary. Auto-cross-linked hyaluronic acid (Bioregencorp., China) was introduced into the uterine cavity at the end of TCRA. After that, a heart-shaped COOK intrauterine balloon stent (J-BUS-253000, COOK Medical Corp., US) was inserted into and kept inside the uterine cavity after TCRA. All patients were treated with 3mg/12h estrogen (Progynova, Bayer) orally for 17 days. The patients were then treated with 2mg/12h estrogen orally from the 1st to the 28th day of withdrawal bleeding with 10mg/day dydrogesterone added during the latter half of one cycle. A second look hysteroscopy was performed 1 to 2 months after hysteroscopic adhesiolysis. If any newly forming adhesions were existed, TCRA and the procedure above would be performed again.
IVF/ICSI Protocol
All patients receiving IVF/ICSI at the reproductive center of our hospital in this study, regardless of the superovulation protocol used. Our center generally transfers cleavage-stage embryos on the third day and blastocyst embryos on the fifth day after insemination. The remaining embryos can be frozen after embryo transfer in fresh cycles. Embryos can also be frozen in canceled cycles for reasons such as high OHSS risk, endometrial problems or special controlled ovarian hyperstimulation protocol (mild controlled ovarian stimulation cycle, progestin-primed ovulation stimulation, etc.).
Endometrial Preparation
HRT protocol: From the 3rd day of menstruation, patients were given 2mg/12h of estrogen (Progynova, Bayer) orally for 5 days, and then increased to 3–4mg/12h orally for 7–10 days, followed by ultrasound monitoring. Progesterone was used to assist secretory transformation of the endometrium. When the serum estradiol level exceeded 200 pg/mL and the serum progesterone level was below 2 ng/mL, Crinone vaginal gel (Merck Serono, Denmark) was administered at a dose of 90mg/d (D0) to patients until the day of plasma β-hCG determination (D14). The endometrial thickness and endometrial pattern were assessed on D0.
GnRHa+HRT protocol: 3.75mg triptorelin acetate injection (Decapeptyl, Ferring, Switzerland) was administered during the early follicular phase of the previous menstrual cycle (day one or two), and the HRT protocol was started 28 days later.
OS protocol: Patients were given 2.5mg letrozole daily on cycle days 3–7 with a sequential therapy of 75 IU/d HMG (Lizhu Pharmaceutical Factory, Zhuhai, China) on cycle days 8–10. Then, the first vaginal ultrasound was performed. The size of follicles was recorded. Once at least one dominant follicle reached ≥18mm, then 10,000 IU human chorionic gonadotropin (HCG) was injected intramuscularly to trigger ovulation. On the next day (D0), crinone vaginal gel (Merck Serono, Denmark) was administered at a dose of 90mg/d to patients until the day of plasma β-hCG determination (D14). The endometrial thickness and endometrial pattern were assessed on D0.
Statistical Methods
All statistical analyses were conducted using SPSS 26.0 software (IBM Corp., NY). Continuous variables were compared using Student’s t-tests. Categorical variables were compared using Pearson chi-squared test or Fisher’s exact test. Descriptive parameters were presented as mean ± SD or as a percentage. P-values were two-tailed and considered statistically significant if <0.05. Multivariable logistic regression analyses were applied to examine whether different protocols of endometrial preparation and endometrial pattern affected the reproductive outcomes for AS women undergoing ET cycles.
Results
The study included 76 women, their clinical characteristics are presented in Table 1. Of the 76 AS patients included in our study, the clinical pregnancy rate was 60.5%, and the live birth rate was 50% (Table 1). The clinical pregnancy rate of patients’ age <37 was higher than patients’ age ≥37; however, the difference is not statistically significant (65.6% vs 33.3%, P = 0.053). The numbers of TCRA were significantly differed between patients with and without a clinical pregnancy (P = 0.016). There were no significant differences in AMH, BMI, ESGE classification, pre-hysteroscopy menstrual pattern, history of recurrent spontaneous miscarriage, history of late miscarriage, total number of uterine curettage, gynecologic history, maximum endometrial thickness prior to TCRA, visualization of tubal ostia, and type of adhesions between women with and without clinical pregnancy or live birth.
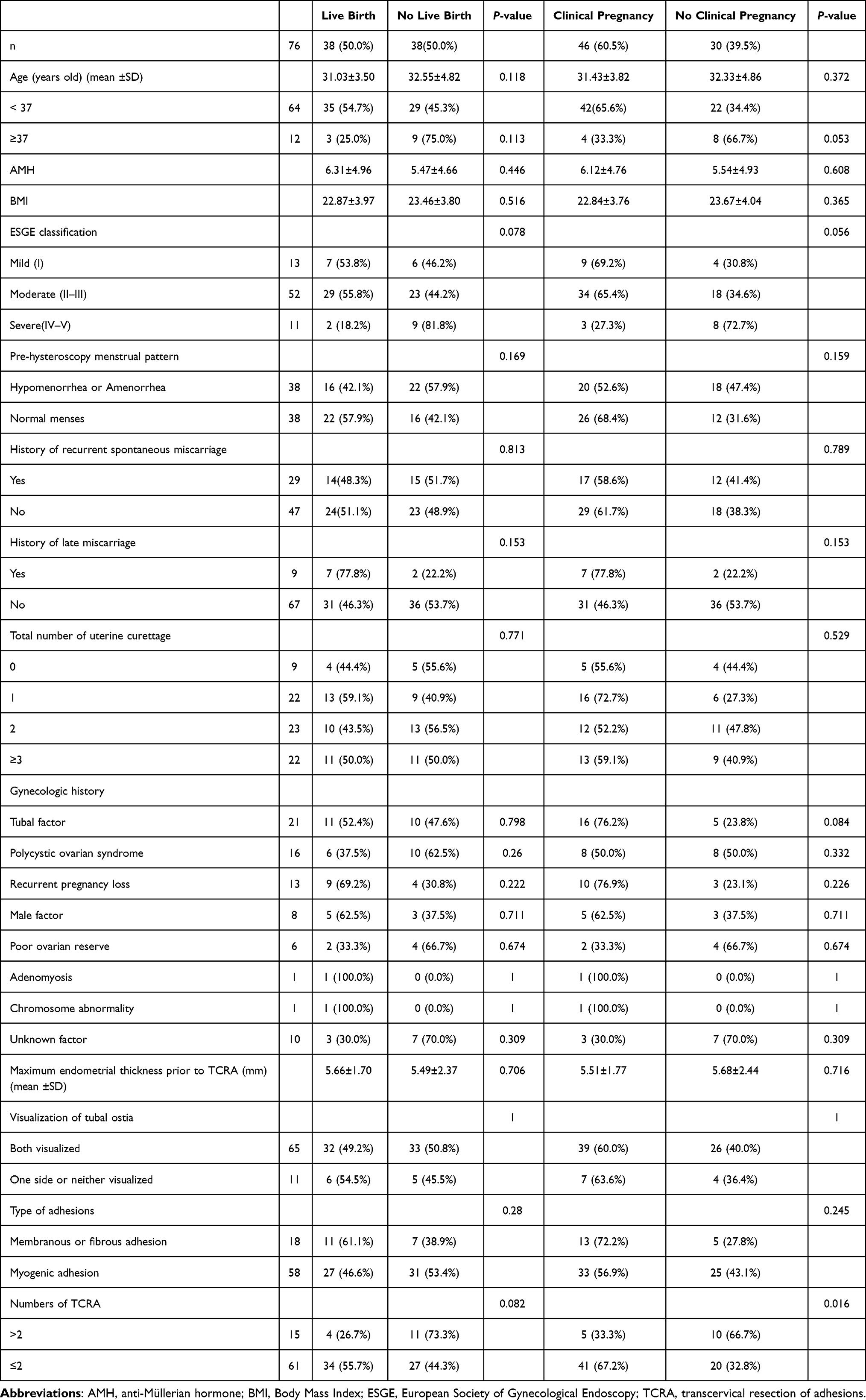 |
Table 1 The Clinical Characteristics of AS Patients |
A total of 134 ETs were performed for the 76 AS patients. Among these, 53 ETs led to a clinical pregnancy (39.6%), and 39 ET’s resulted in a live birth (29.1%) (Table 2). The proportion of women with a triple-line endometrial pattern before ET was significantly higher in the clinical pregnancy group than in the non-clinical pregnancy group (54.7% vs 25.9%, P<0.001, Table 2), while it was similar between the live birth group and the no live birth group (59.0% vs 28.4%, P=0.001). There was a total of 127 ETs undergoing FET. Among them, 87 ETs were carried out with the HRT protocol, 16 with the OS protocol and 24 with the GnRHa+HRT protocol. Seventeen patients were transferred to an alternate protocol following unsuccessful embryo implantation. The proportion of ETs undergoing the HRT protocol in the clinical pregnancy group was significantly lower than in the non-clinical pregnancy group (50.0% vs 80.5%, P=0.001, Table 2), whereas the proportion of ETs undergoing the GnRHa+HRT protocol in the clinical pregnancy group was significantly higher than in the non-clinical pregnancy group (34.0% vs 9.1%, P = 0.001). Additionally, the proportion of ETs undergoing the HRT protocol in the live birth group was significantly lower than in the no live birth group (50.0% vs 75.8%, P=0.013), and the proportion of ETs undergoing the GnRHa+HRT protocol in the live birth group was significantly higher than in the no live birth group (33.3% vs 13.2%, P = 0.013). No significant differences were found in intracytoplasmic sperm injection (ICSI), embryo type, embryo age at the time of ET, total number of embryos transferred, total number of high-quality embryos transferred, or endometrial thickness prior to ET between the clinical pregnancy group and the non-clinical pregnancy group or between the live birth group and the no live birth group. Furthermore, there was no significant difference in the distribution of ESGE classifications among the three distinct endometrial preparation protocols (Supplementary Table 1). Additionally, the patients’ age showed no correlation with endometrial patterns (Supplementary Table 2).
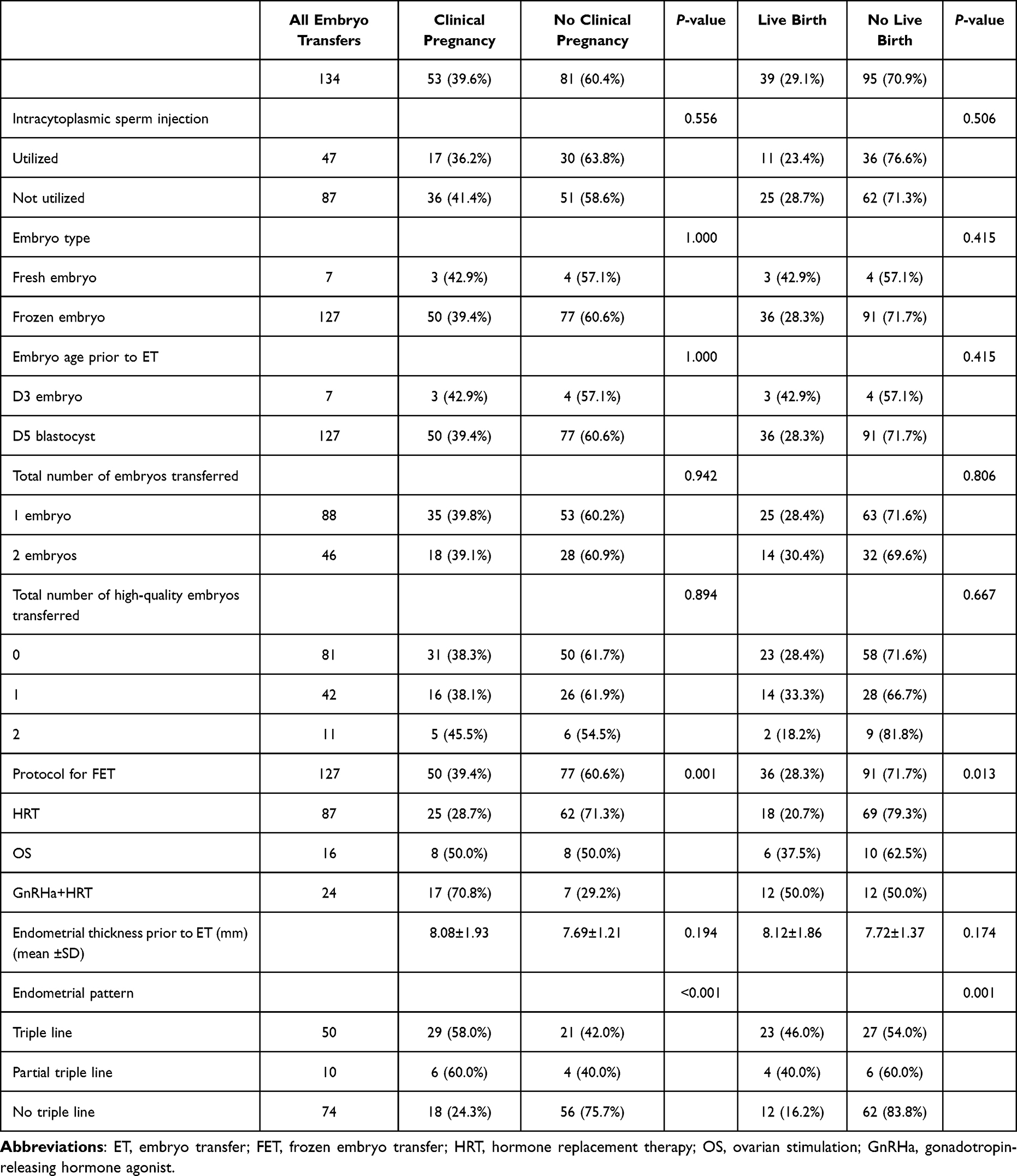 |
Table 2 Embryo Transfers |
In order to determine the independent variables related to the clinical pregnancy rate in patients, we conducted a logistic regression analysis while controlling for potential confounders, such as patient age, ESGE classification, and the number of TCRA (Table 3). The analysis revealed that patient age independently influenced the likelihood of achieving a clinical pregnancy (odds ratio, 5.316; 95% confidence interval, 1.175–24.060; P = 0.030). However, we observed no association between patient age, ESGE classification, number of TCRA, menstrual pattern before hysteroscopy, history of late miscarriage, and live birth rate in the multivariable logistic regression analysis (Table 4).
 |
Table 3 Multivariable Logistic Regression Analysis of Age, ESGE Classification, Numbers of TCRA and Clinical Pregnancy |
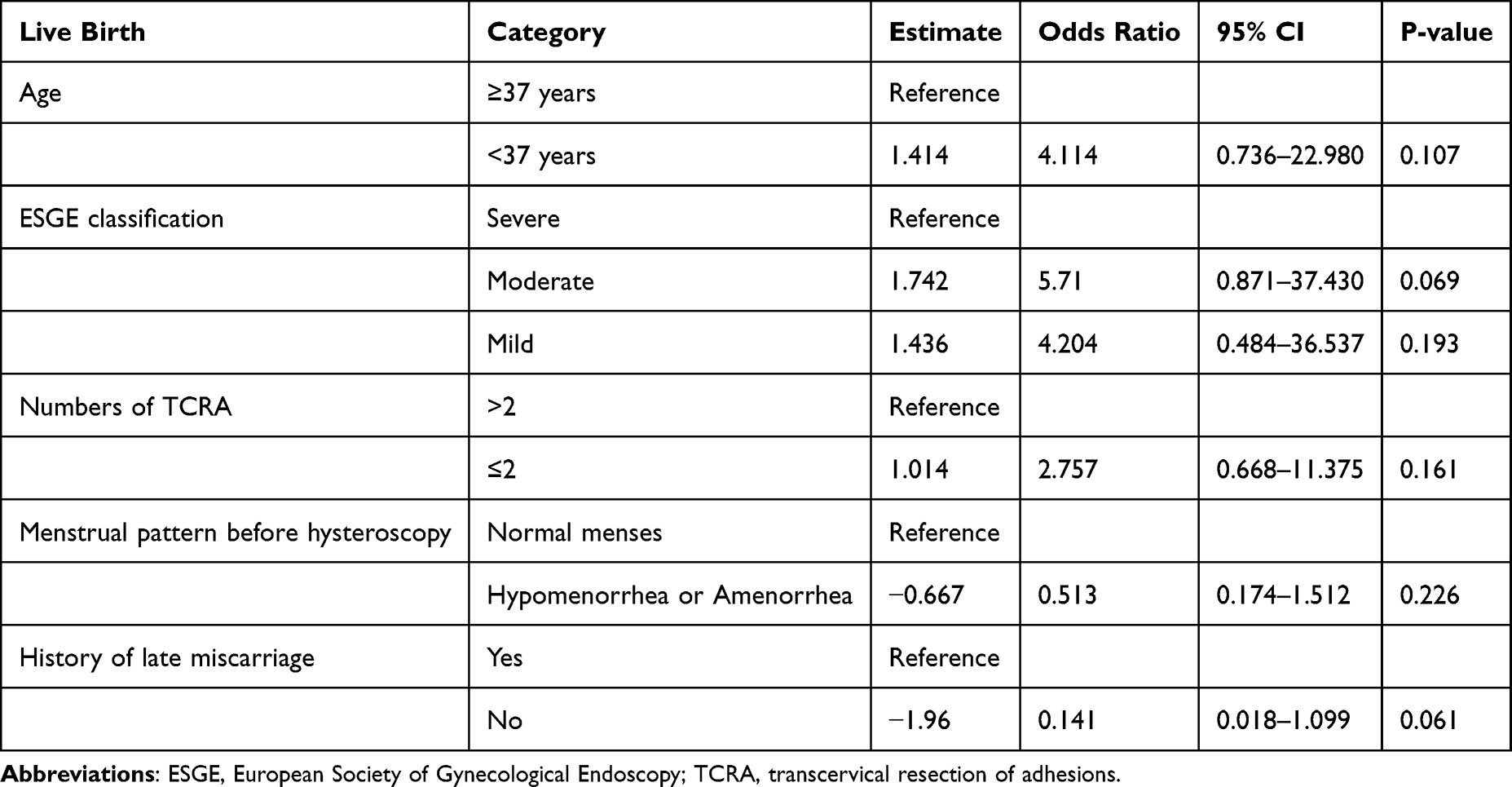 |
Table 4 Multivariable Logistic Regression Analysis of Age, ESGE Classification, Numbers of TCRA, Menstrual Pattern Before Hysteroscopy, History of Late Miscarriage and Live Birth |
Multivariable analysis was used to assess the relationship between FET protocol, endometrial pattern and clinical pregnancy outcome while controlling for embryo quality, age and endometrial thickness (Table 5). We identified that the HRT protocol significantly decreased the odds ratio (OR) of clinical pregnancy compared to the GnRHa+HRT protocol (OR, 0.218, 95% confidence interval, 0.076–0.624; P = 0.005). In addition, we found that the absence of a triple-line endometrial pattern was significantly associated with decreased odds of clinical pregnancy compared to having a triple-line endometrial pattern (OR, 0.315, 95% confidence interval, 0.137–0.727; P = 0.007). Another multivariable analysis was performed to assess the relationship between the FET protocol, endometrial pattern and live birth outcome while controlling for embryo quality, age and endometrial thickness (Table 6). The HRT protocol showed a significant decrease in the odds ratio (OR) of live birth compared to the GnRHa+HRT protocol (OR, 0.362, 95% confidence interval, 0.131–0.995; P = 0.049). Additionally, we found that the absence of a triple-line endometrial pattern was significantly associated with decreased odds of live birth compared to having a triple-line endometrial pattern (OR, 0.306, 95% confidence interval, 0.127–0.740; P = 0.009).
 |
Table 5 Multivariable Logistic Regression Analysis of Protocols of FET, Endometrial Pattern, Quality of Embryo, Age, EMT and Clinical Pregnancy |
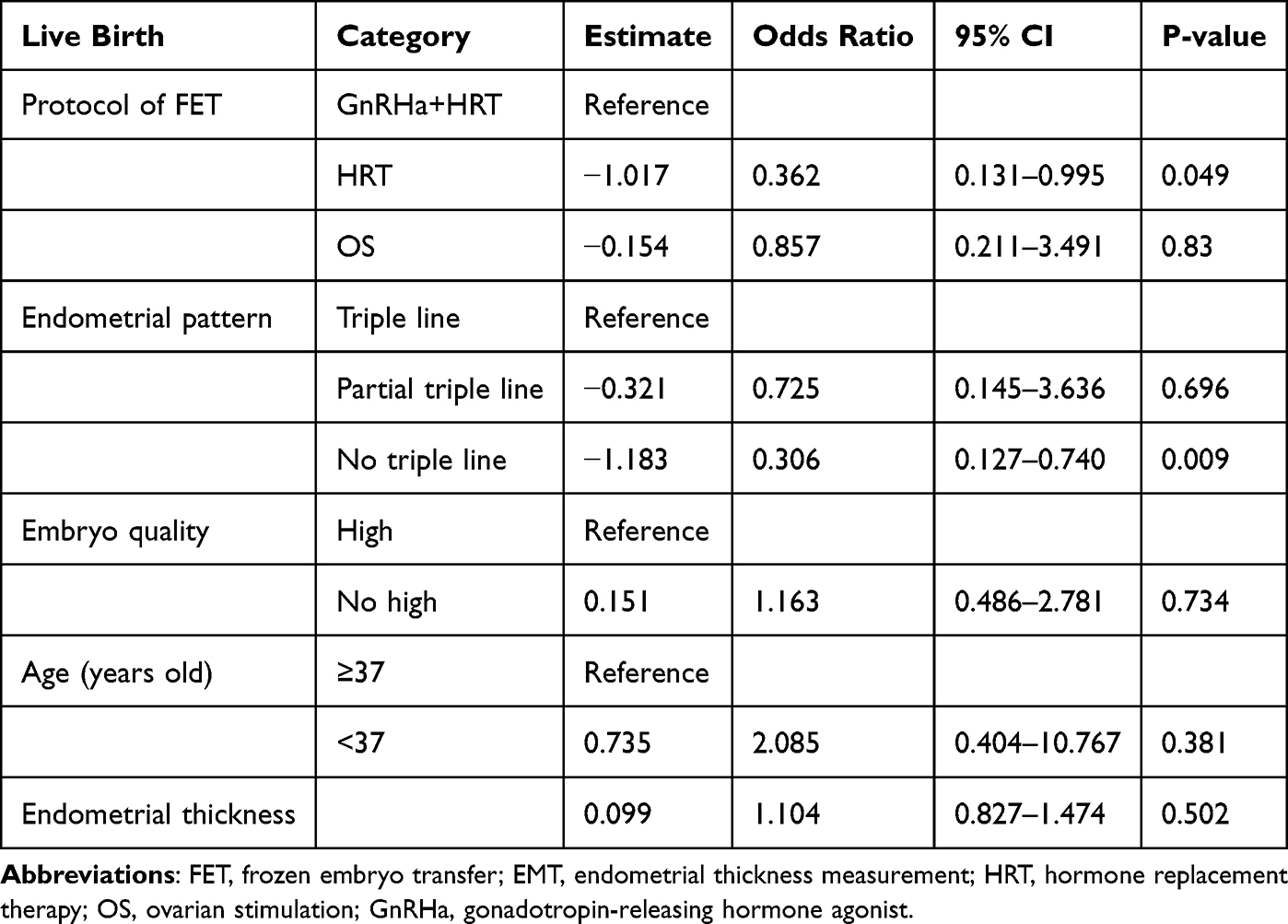 |
Table 6 Multivariable Logistic Regression Analysis of Protocol of FET, Endometrial Pattern, Quality of Embryo, Age, EMT and Live Birth |
Discussion
FET cycles minimized the potential impacts of varying ovarian stimulation protocols and high serum progesterone level on endometrium in fresh cycles. After controlling for the quality of the embryo, our results indicated a correlation between endometrial pattern and clinical outcomes. Those with the triple-line pattern had a significant higher clinical pregnancy rate and live birth rate. However, neither endometrial thickness nor total number of embryos transferred could predict the clinical pregnancy or live birth following FET cycles in patients with AS. A triple-line pattern at ultrasound examination reflects endometrial proliferation. The absence of a triple-line pattern could be a sign of early secretory changes in the endometrium, indicating that the time of maximal endometrial receptivity has passed.19
This finding suggests that administering a single dose of long-acting GnRHa in the early follicular phase of the FET cycle can improve the clinical outcomes of AS patients, possibly by augmenting endometrial receptivity. The optimal method for endometrial preparation in FET cycles, with or without GnRHa pretreatment, lacks consensus in terms of consistently improved pregnancy outcomes.11,20,21 However, few studies have focused on the suitable FET protocol for AS patients. Our findings suggest that the administration of a single dose of long-acting GnRHa in the early follicular phase of the previous menstrual cycle could serve as a novel strategy for endometrial preparation in FET cycles for AS patients. The GnRH/ GnRHR system is expressed in the endometrium, ovaries, and human preimplantation embryos. The expression of this system supports its physiological regulatory role in the functioning of the endometrial receptivity,22 trophoblast invasion,23 and embryo implantation.24,25. Our proposal suggests that the direct action of GnRHa in the previous menstrual cycle may be a potential mechanism for enhancing endometrial receptivity during FET cycles. In a murine model, ovarian stimulation reduced the endometrial expression of the integrin beta-3 subunit, leukaemia inhibitory factor, and the implantation rate during the implantation window, with partial reversal of these effects following GnRHa administration.22 GnRHa exhibits a direct immunomodulatory effect by disrupting the imbalance between Th17 and Treg cells, thereby enhancing endometrial receptivity.26 Furthermore, it can enhance endometrial receptivity by upregulating the expression of αγβ3 integrin in the endometrium, modulating the levels of IL-6 and IL-11 in endometrial stromal cells via miR-124-3p, and enhancing the formation of pinopodes to facilitate embryo implantation.27,28 These mechanisms are crucial in contributing to the favorable clinical outcomes associated with the GnRHa+HRT protocol.
The strength of our study lies in the inclusion of a substantial number of AS patients, considering the rarity of the disease. Additionally, the study has significant clinical implications. We have identified an association between endometrial patterns and pregnancy outcomes, including clinical pregnancy and live birth for AS patients. On the day of progesterone administration, an isoechoic or homogeneous hyperechoic endometrium with a nonprominent or absent central echogenic line may indicate a lower clinical pregnancy and live birth rate. Furthermore, the GnRHa+HRT protocol favors the pregnancy outcomes, compared to the HRT protocol in FET cycles for AS patients.
There are also some limitations in the present study. One significant limitation of our study is its retrospective nature and the lack of a prospective randomized design. Undetected biases might have influenced the outcomes. Consequently, logistic regression analyses were conducted to reduce potential biases. The validation of any results will necessitate a well-designed and adequately powered randomized clinical trial.
Conclusion
The present study indicated that endometrial preparation for AS patients undergoing FET with GnRHa suppression provides better clinical outcomes than without GnRHa. Additionally, the endometrial pattern, rather than endometrial thickness, should be used to determine whether to cancel a scheduled ET in AS patients.
Data Sharing Statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Disclosure
The authors declare they have no conflict of interest. The authors have no relevant financial or non-financial interests to disclose.
References
1. Foix A, Bruno R, Davison T, Baltasar L. The pathology of postcurettage adhesions. Am J Obstet Gynecol. 1966;96:1027–1033. doi:10.1016/0002-9378(66)90452-2
2. Chan JM, Sukumar AI, Ramalingam M, Ranbir Singh SS, Abdullah MF. The impact of endometrial thickness (EMT) on the day of human chorionic gonadotropin (hCG) administration on pregnancy outcomes: a 5-year retrospective cohort analysis in Malaysia. Fertil Res Pract. 2018;4:5. doi:10.1186/s40738-018-0050-8
3. Zhao J, Zhang Q, Wang Y, Li Y. Endometrial pattern, thickness and growth in predicting pregnancy outcome following 3319 IVF cycle. Reprod Biomed Online. 2014;29:291–298. doi:10.1016/j.rbmo.2014.05.011
4. Arce H, Velilla E, López-Teijón M. Association between endometrial thickness in oocyte donation cycles and pregnancy success rates. Reprod Fertil Dev. 2015. doi:10.1071/RD14459
5. Check JH, Dietterich C, Graziano V, Lurie D, Choe JK. Effect of maximal endometrial thickness on outcome after frozen embryo transfer. Fertil Steril. 2004;81:1399–1400. doi:10.1016/j.fertnstert.2004.01.020
6. Zácková T, Järvelä IY, Tapanainen JS, Feyereisl J. Assessment of endometrial and ovarian characteristics using three dimensional power Doppler ultrasound to predict response in frozen embryo transfer cycles. Reprod Biol Endocrinol. 2009;7:151. doi:10.1186/1477-7827-7-151
7. Movilla P, Wang J, Chen T, et al. Endometrial thickness measurements among Asherman syndrome patients prior to embryo transfer. Hum Reprod. 2020;35:2746–2754. doi:10.1093/humrep/deaa273
8. Chang WS, Lin PH, Li CJ, et al. Additional single dose GnRH agonist during luteal phase support may improve live birth rate in GnRHa-HRT frozen-thawed embryo transfer cycle: a retrospective cohort study. BMC Pregnancy Child Birth. 2023;23:174. doi:10.1186/s12884-023-05491-y
9. Conn PM, Crowley WF Jr. Gonadotropin-releasing hormone and its analogs. Annu Rev Med. 1994;45:391–405. doi:10.1146/annurev.med.45.1.391
10. Ma WG, Song H, Das SK, Paria BC, Dey SK. Estrogen is a critical determinant that specifies the duration of the window of uterine receptivity for implantation. Proc Natl Acad Sci U S A. 2003;100:2963–2968. doi:10.1073/pnas.0530162100
11. Xu B, Hou Z, Liu N, Zhao J, Li Y. Pretreatment with a long-acting GnRH agonist for frozen-thawed embryo transfer cycles: how to improve live birth? J Ovarian Res. 2023;16:197. doi:10.1186/s13048-023-01277-0
12. Pan Y, Li F, Yang CX, et al. Correlation between different endometrial preparation protocols and pregnancy outcome of frozen embryo transfer in patients with polycystic ovary syndrome: a retrospective study. Gynecol Endocrinol. 2023;39:2217260. doi:10.1080/09513590.2023.2217260
13. Yarali H, Polat M, Mumusoglu S, Yarali I, Bozdag G. Preparation of endometrium for frozen embryo replacement cycles: a systematic review and meta-analysis. J Assist Reprod Genet. 2016;33:1287–1304. doi:10.1007/s10815-016-0787-0
14. Li C, He YC, Xu JJ, et al. Perinatal outcomes of neonates born from different endometrial preparation protocols after frozen embryo transfer: a retrospective cohort study. BMC Pregnancy Childbirth. 2021;21:341. doi:10.1186/s12884-021-03791-9
15. Mumusoglu S, Polat M, Ozbek IY, et al. Preparation of the Endometrium for Frozen Embryo Transfer: a Systematic Review. Front Endocrinol. 2021;12:688237. doi:10.3389/fendo.2021.688237
16. Glujovsky D, Pesce R, Sueldo C, Quinteiro Retamar AM, Hart RJ, Ciapponi A. Endometrial preparation for women undergoing embryo transfer with frozen embryos or embryos derived from donor oocytes. Cochrane Database Syst Rev. 2020;10:CD006359. doi:10.1002/14651858.CD006359.pub3
17. Matsuura K, Hayashi N, Takiue C, Hirata R, Habara T, Naruse K. Blastocyst quality scoring based on morphologic grading correlates with cell number. Fertil Steril. 2010;94:1135–1137. doi:10.1016/j.fertnstert.2009.11.003
18. Wamsteker K, Deblock S. Diagnostic hysteroscopy: techinique and documentation. In: S C, D MP, editors. Endoscopic Surgery for Gynecologists. London: WB Saunders; 1998:511–524.
19. Bourgain C, Devroey P. The endometrium in stimulated cycles for IVF. Hum Reprod Update. 2003;9:515–522. doi:10.1093/humupd/dmg045
20. Movahedi S, Aleyasin A, Agahosseini M, et al. Endometrial preparation for women undergoing embryo transfer frozen-thawed embryo transfer with and without pretreatment with gonadotropin releasing hormone agonists. J Family Reprod Health. 2018;12:191–196.
21. Kang J, Park J, Chung D, et al. Comparison of the clinical outcome of frozen-thawed embryo transfer with and without pretreatment with a gonadotropin-releasing hormone agonist. Obstet Gynecol Sci. 2018;61:489–496. doi:10.5468/ogs.2018.61.4.489
22. Ruan HC, Zhu XM, Luo Q, et al. Ovarian stimulation with GnRH agonist, but not GnRH antagonist, partially restores the expression of endometrial integrin beta 3 and leukaemia-inhibitory factor and improves uterine receptivity in mice. Hum Reprod. 2006;21:2521–2529. doi:10.1093/humrep/del215
23. Iwashita M, Kudo Y, Shinozaki Y, Takeda Y. Gonadotropin-releasing hormone increases serum human chorionic gonadotropin in pregnant women. Endocr J. 1993;40:539–544. doi:10.1507/endocrj.40.539
24. Maggi R, Cariboni AM, Marelli MM, et al. GnRH and GnRH receptors in the pathophysiology of the human female reproductive system. Hum Reprod Update. 2016;22:358–381. doi:10.1093/humupd/dmv059
25. Casan EM, Raga F, Polan ML. GnRH mRNA and protein expression in human preimplantation embryos. Mol Hum Reprod. 1999;5:234–239. doi:10.1093/molehr/5.3.234
26. Guo Z, Shi P, Hao C. Effect of GnRHa on Th17/Treg cells in peripheral blood of patients with unexplained repeated implantation failure. Arch Gynecol Obstet. 2018;298:1211–1218. doi:10.1007/s00404-018-4874-6
27. Li L, Liu L, Kou Z, Huo M, An J, Zhang X. GnRH agonist treatment regulates IL-6 and IL-11 expression in endometrial stromal cells for patients with HRT regiment in frozen embryo transfer cycles. Reprod Biol. 2022;22:100608. doi:10.1016/j.repbio.2022.100608
28. Cao X, Chang HY, Xu JY, et al. The effectiveness of different down-regulating protocols on in vitro fertilization-embryo transfer in endometriosis: a meta-analysis. Reprod Biol Endocrinol. 2020;18:16. doi:10.1186/s12958-020-00571-6
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.