Back to Journals » International Journal of Women's Health » Volume 18
Protocol-Specific Luteinizing Hormone Thresholds for IVF Pregnancy Outcomes: The Moderating Role of Age in a Retrospective Study of 217 Cycles
Authors Zhao J, Guan H, Wang M, Tang L, Tang H
Received 16 November 2025
Accepted for publication 16 February 2026
Published 26 February 2026 Volume 2026:18 581964
DOI https://doi.org/10.2147/IJWH.S581964
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Jiahui Zhao, Huijuan Guan, Mei Wang, Lisha Tang, Huaiyun Tang
Department of Reproductive Medicine, Lianyungang Maternal and Child Health Hospital, Lianyungang, Jiangsu, People’s Republic of China
Correspondence: Huaiyun Tang, Department of Reproductive Medicine, Lianyungang Maternal and Child Health Hospital, Lianyungang, Jiangsu, People’s Republic of China, Tel +8651885820353, Email [email protected]
Objective: To explore the impact of trigger-day luteinizing hormone (LH) levels on pregnancy outcomes in antagonist and long protocols during in vitro fertilization (IVF) and determine protocol-specific LH thresholds.
Methods: This retrospective analysis covered 217 IVF/ICSI cycles from January 2023 to April 2024. The relationships between trigger-day LH levels and pregnancy outcomes in the two protocols were compared using ROC curves, multivariate logistic regression, and mediation models.
Results: In the antagonist protocol, LH > 1.45 IU/L was linked to lower oocyte yield, reduced high-quality embryo rates, and a higher risk of clinical pregnancy failure (RR = 2.34, p = 0.006). In the long protocol, LH > 1.0 IU/L was associated with higher clinical pregnancy rates (OR = 2.61, p = 0.026), with 68% of the effect mediated by increased oocyte yield. Age ≤ 35 significantly enhanced these effects (three-way interaction OR = 6.55, p = 0.003).
Conclusion: The antagonist and long protocols should adopt LH thresholds of 1.45 IU/L and 1.0 IU/L, respectively. Age is a key moderator, providing evidence for individualized IVF trigger strategies.
Keywords: luteinizing hormone, antagonist protocol, long protocol, in vitro fertilization, clinical pregnancy, age interaction
Introduction
As a fundamental component of Assisted Reproductive Technology (ART), the success rate of in vitro fertilization (IVF) is affected by numerous factors, with the optimization of ovulation induction regimens being particularly crucial. The antagonist and long protocols, two predominant ovulation induction strategies, differ fundamentally in their mechanisms of pituitary suppression. The antagonist protocol achieves rapid suppression by directly blocking gonadotropin receptors,1 whereas the long protocol employs gonadotropin-releasing hormone (GnRH) agonists to achieve down-regulation.2 Following an initial flare-up effect, luteinizing hormone (LH) levels gradually decrease.
This divergence profoundly alters the endocrine milieu, particularly the physiological dynamics of luteinizing hormone (LH). Research suggests that LH levels on the trigger day have differential impacts on outcomes in the antagonist and long protocols.3–6 Conversely, certain studies indicate that trigger-day LH levels in the antagonist protocol may not significantly affect outcomes.6 In the context of the GnRH agonist long protocol, limited research has investigated the relationship between trigger-day LH levels and pregnancy outcomes following fresh embryo transfer. Current evidence demonstrates a positive correlation between trigger-day LH levels and both clinical pregnancy and live birth rates.7,8 Nonetheless, this body of research does not elucidate the threshold effect of LH in the long protocol and lacks a stratified analysis concerning the critical covariate of age.
The present study identifies three primary research gaps: Firstly, the safe luteinizing hormone (LH) threshold in the antagonist protocol has yet to be determined through receiver operating characteristic (ROC) analysis. Secondly, the hypothesis that the protective effect of elevated LH levels in the long protocol is mediated by oocyte yield remains unsubstantiated by statistical evidence. Thirdly, the influence of age as a moderating factor on the LH threshold has not been quantified. The age cutoff of 35 years was selected based on well-established biological evidence: women aged >35 years exhibit accelerated decline in ovarian reserve, altered gonadotropin sensitivity, and reduced LH receptor expression on granulosa cells, which may modify the physiological effects of LH during ovarian stimulation.9,10 This retrospective cohort analysis seeks to address these gaps by: 1) establishing a personalized LH threshold for the antagonist protocol; 2) elucidating the mechanism by which elevated LH levels confer benefits in the long protocol; and 3) quantifying the interaction between age and protocol. The outcomes of this study are expected to provide an evidence-based framework for individualized ovulation induction strategies, thereby improving in vitro fertilization (IVF) pregnancy outcomes.
Methods
Study Design and Ethics
This single-center retrospective cohort study included 217 consecutive first-time IVF/ICSI cycles performed at the Reproductive Medicine Center of our hospital between January 2023 and April 2024. The study protocol was approved by the institutional ethics committee (Approval No.: LYG-MER2021039). Informed consent was waived as all data were extracted from an anonymized electronic medical record system, ensuring full protection of patient privacy.
Participants
Inclusion criteria: (1) First IVF/ICSI attempt; (2) Age <38 years (23–37 years inclusive); (3) Use of either a flexible antagonist protocol or standard short-acting GnRH agonist long protocol.
Exclusion criteria: (1) Diminished ovarian reserve (AMH <1.1 ng/mL or antral follicle count <5–7, per Bologna criteria11); (2) Poor ovarian response according to the Poseidon classification;12 (3) Chronic diseases (eg, diabetes mellitus, uncontrolled thyroid disorders, autoimmune diseases); (4) Uterine anomalies (eg, Asherman syndrome, submucosal myoma, unicornuate uterus); (5) Recurrent pregnancy loss (≥2 spontaneous abortions). (6) Bilateral or unilateral hydrosalpinx; (7) Chromosomal abnormalities.
Controlled Ovarian Stimulation Protocols
Flexible antagonist protocol: Recombinant FSH (rFSH) 150–300 IU/day was initiated on cycle day 2. Ganirelix 0.25 mg/day was added when the leading follicle reached ≥14 mm or serum estradiol ≥300 pg/mL. Final oocyte maturation was triggered with triptorelin 0.2 mg plus hCG 4000 IU when ≥2 follicles reached ≥17 mm.
Long protocol: Short-acting triptorelin 0.1 mg/day was started in the mid-luteal phase. Pituitary down-regulation was confirmed by ultrasound and hormone tests (luteinizing hormone <2 IU/L, estradiol <50 pg/mL) before initiating rFSH stimulation. Ovulation was triggered with hCG 8000 IU when ≥2 follicles reached ≥17 mm.
Outcome Measures
Primary outcome: Clinical pregnancy rate (CPR), defined as the presence of at least one intrauterine gestational sac with fetal heart activity on transvaginal ultrasound at 4 weeks after embryo transfer.Secondary outcomes: Oocyte yield; metaphase II (MII) oocyte rate (number of MII oocytes/total oocytes retrieved); high-quality embryo rate (number of day-3 embryos with ≥7 cells and ≤20% fragmentation/total embryos); ongoing pregnancy rate (pregnancy ≥10 weeks with fetal heart activity on ultrasound); live birth rate (delivery of at least one live infant after 28 weeks of gestation).
Data Collection and Quality Control
Demographic and clinical data were extracted from electronic medical records, including age, BMI, infertility type and duration, stimulation protocol, days and total dose of gonadotropin (Gn), trigger-day LH and estradiol levels, basal serum LH, FSH, E2, Progesterone, AMH levels, fertilization method, number of transferred embryos, grade of transferred embryos, oocyte yield, usable embryos, high-quality embryos, and pregnancy outcomes. Missing data (<3%) were handled by listwise deletion. Double data entry with cross-verification yielded a κ coefficient of 0.97, indicating excellent inter-rater reliability.
Statistical Analyses
Data analyses were performed using SPSS 26.0, R 4.2.1 (packages: pROC, mediation), and Python (libraries: scikit-learn, statsmodels). Statistical significance was defined as a two-tailed p-value < 0.05 for all analyses. Continuous variables are presented as mean ± SD, with group comparisons using independent t-tests or Mann–Whitney U-tests; categorical variables are presented as n (%), with group comparisons using χ2-tests or Fisher’s exact tests.
Threshold determination: Receiver operating characteristic (ROC) curve analysis was used to identify the optimal LH threshold for predicting pregnancy failure in the antagonist protocol. The area under the curve (AUC), sensitivity, and specificity were calculated, with the cut-off determined by maximizing the Youden index (sensitivity + specificity − 1).
Effect estimation: Relative risk (RR) with 95% confidence intervals (CI) was used for binary outcomes, and mean difference (MD) for continuous outcomes. Odds Ratio (OR) was applied in multivariate logistic regression to identify independent predictors of clinical pregnancy, which differs from RR in that RR directly reflects the risk ratio between exposure and outcome, while OR approximates the risk ratio in low-prevalence outcomes.
Mediation analysis: The Sobel test was used to verify the indirect effect of “LH→oocyte yield→clinical pregnancy” in the long protocol, quantifying the proportion of LH’s effect on pregnancy outcomes mediated by oocyte yield. Oocyte yield was selected as the potential mediator based on the physiological mechanism that LH promotes folliculogenesis and maturation, thereby increasing the number of available oocytes for fertilization. Embryo quality was not selected as a mediator because previous studies have shown that LH primarily affects early follicular development rather than direct modulation of embryo quality.13
Stratified and interaction analyses: Patients were stratified into ≤35 years and >35 years subgroups based on the widely recognized age cutoff in reproductive medicine.10 Differences in LH threshold effects between age subgroups were compared. A three-way interaction term (“age (≤35/ >35 years) × protocol type × LH group (based on protocol-specific thresholds)”) was included in multivariate logistic regression models, with likelihood ratio tests used to assess the significance of interaction effects (α=0.05).
Robustness tests: Threshold stability was verified by 2000 bootstrap resamplings. Inverse probability of treatment weighting (IPTW) was used to control for potential confounders and assess result robustness.
Results
Patient Baseline Characteristics
From January 2023 to April 2024, a cohort of 217 women (aged 20–37 years) undergoing their first IVF/ICSI treatment was enrolled. Participants were categorized into the antagonist protocol group (n=102) and long protocol group (n=115). As shown in Table 1, the mean age was 30.8±3.7 years in the antagonist group and 31.6±3.5 years in the long protocol group (p=0.103), with no significant differences in body mass index (BMI: 23.2±3.7 kg/m2 vs 23.3±3.3 kg/m2, p=0.802), proportion of primary infertility (50.0% vs 58.3%, p=0.224), or duration of infertility. However, the long protocol group had a significantly longer gonadotropin (Gn) administration duration (12.7±2.7 days vs 9.8±1.7 days, p<0.001), higher total Gn dose (2491±748 IU vs 1895±498 IU, p<0.001), and lower trigger-day serum LH level (0.90±0.63 IU/L vs 1.58±1.45 IU/L, p<0.001) compared to the antagonist group. The number of oocytes retrieved did not differ significantly between groups (9.5±3.2 vs 9.6±3.3, p=0.808).
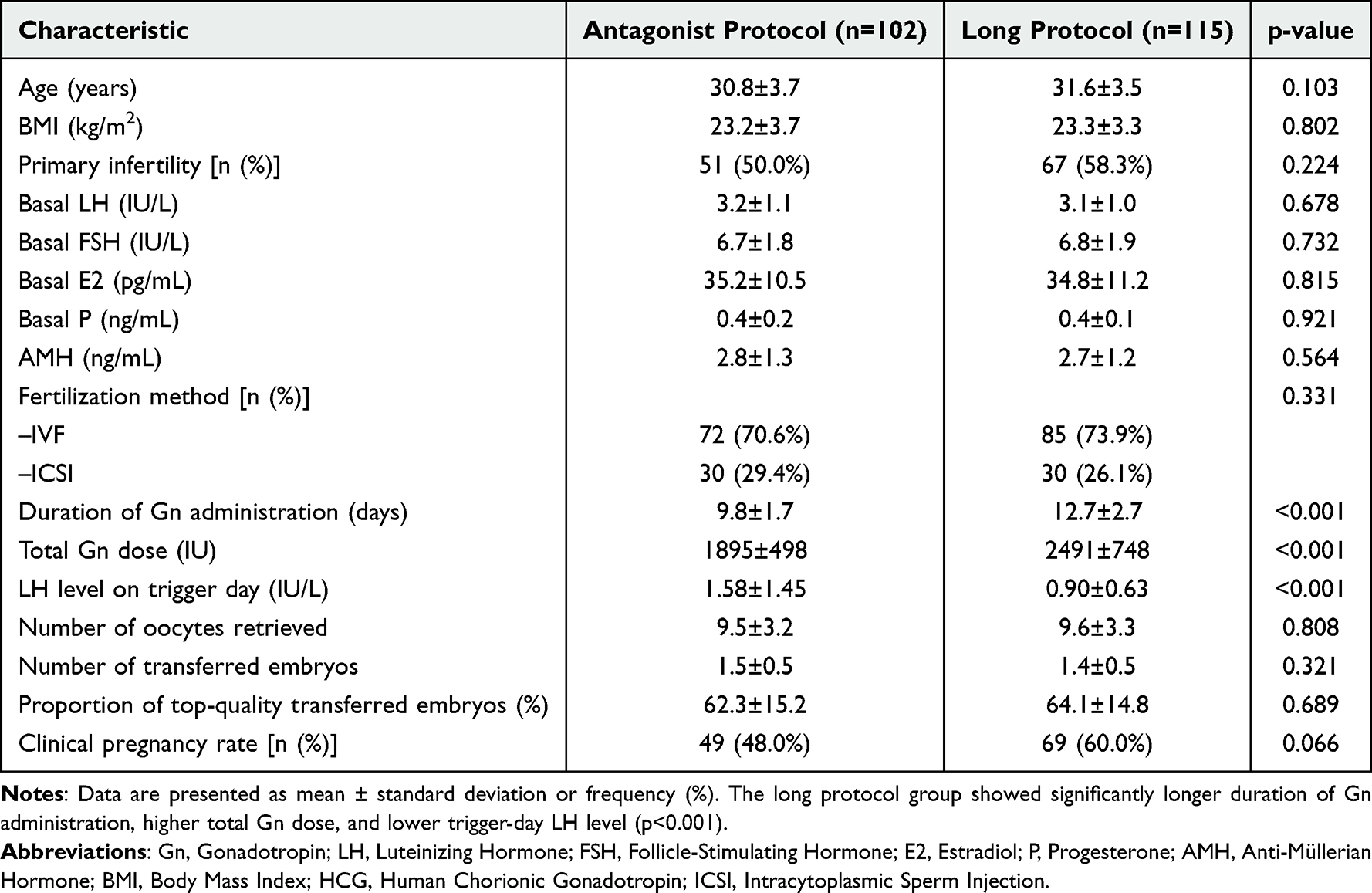 |
Table 1 Comparison of Baseline Characteristics Between the Two Groups |
Protocol-Specific LH Thresholds
Preliminary Analysis of LH Levels and Pregnancy Rate
To initially explore the association between trigger-day LH levels and clinical pregnancy, participants were stratified into three LH groups (≤0.5 IU/L, 0.5<LH≤1.0 IU/L, >1.0 IU/L). The LH grouping was based on commonly used clinical segmentation criteria in the field [6], combined with pre-analysis results of this study (LH=0.5 IU/L and 1.0 IU/L were identified as inflection points for changes in clinical pregnancy rate), to facilitate the preliminary exploration of the dose-response relationship between LH and pregnancy rate. As presented in Table 2, the antagonist protocol showed a gradual decrease in clinical pregnancy rate with increasing LH: 60.6% (LH≤0.5 IU/L, n=33), 46.2% (0.5<LH≤1.0 IU/L, n=26), and 39.5% (LH>1.0 IU/L, n=43) (intragroup p=0.047), with the LH>1.0 IU/L group significantly lower than the LH≤0.5 IU/L group (p=0.036). In contrast, the long protocol exhibited a reverse trend: 54.1% (LH≤0.5 IU/L, n=61), 61.8% (0.5<LH≤1.0 IU/L, n=34), and 75.0% (LH>1.0 IU/L, n=20) (intragroup p=0.053), with the LH>1.0 IU/L group significantly higher than the LH≤0.5 IU/L group (p=0.028).
 |
Table 2 Analysis of Pregnancy Rates by LH Level Groups |
Antagonist Protocol: Optimal LH Threshold and Outcomes
Receiver Operating Characteristic (ROC) curve analysis identified the optimal LH threshold for the antagonist protocol as 1.45 IU/L (AUC=0.664, 95% CI: 0.55–0.78, p=0.002). The ROC curve for the antagonist protocol, including sensitivity (69.4%) and specificity (66.0%) at this threshold, is visualized in Figure 1.
 |
Figure 1 Receiver Operating Characteristic (ROC) Curves for Predicting Clinical Pregnancy in Two Ovarian Stimulation Protocols ROC curves comparing the predictive performance of trigger-day luteinizing hormone (LH) levels for clinical pregnancy in the antagonist protocol (red line) and long protocol (blue line). The area under the curve (AUC) values were 0.664 for the antagonist protocol and 0.655 for the long protocol, indicating moderate predictive ability for both. The 95% confidence intervals (CIs) for the ROC curves were 0.55–0.78 for the antagonist protocol and 0.54–0.77 for the long protocol, neither of which included 0.5, confirming the statistically significant predictive value of LH for pregnancy outcomes.Optimal LH thresholds are marked with scatter points: 1.45 IU/L for the antagonist protocol (red dot) corresponding to 66.0% specificity and 69.4% sensitivity, and 1.0 IU/L for the long protocol (blue dot) corresponding to 65.0% specificity and 72.0% sensitivity. The dashed diagonal line represents the reference line for random prediction (AUC = 0.5). Abbreviations: AUC, Area Under the Curve; LH, Luteinizing Hormone; ROC, Receiver Operating Characteristic. |
As shown in Table 3, the LH>1.45 IU/L subgroup had significantly fewer oocytes retrieved, lower MII oocyte rate, fertilization rate, and high-quality embryo rate than the LH≤1.45 IU/L subgroup (all p<0.05), with no differences in age, BMI, or basal FSH (all p>0.05). The LH>1.45 IU/L subgroup also had a significantly lower clinical pregnancy rate (34.9% vs 57.6%, RR=2.34, 95% CI: 1.28–4.27, p=0.006) and ongoing pregnancy rate (27.9% vs 49.2%, RR=2.16, 95% CI: 1.11–4.20, p=0.024) compared to the LH≤1.45 IU/L subgroup.
 |
Table 3 Cycle Characteristics, Embryonic and Pregnancy Outcomes by LH Threshold in the Antagonist Protocol |
Long Protocol: Optimal LH Threshold and Outcomes
ROC curve analysis determined the optimal LH threshold for the long protocol as 1.0 IU/L (AUC=0.655, 95% CI: 0.54–0.77, p=0.028). Figure 1 also presents the ROC curve for the long protocol, showing a sensitivity of 72.0% and specificity of 65.0% at the 1.0 IU/L threshold. Participants with LH>1.0 IU/L had a higher clinical pregnancy rate (75.0% vs 54.1%, p=0.028) and more oocytes retrieved (10.8±3.5 vs 9.1±3.2, p=0.041) than those with LH≤0.5 IU/L. Table 4 (multivariate logistic regression) confirmed LH>1.0 IU/L (OR=2.61, 95% CI: 1.12–6.08, p=0.026) and oocyte retrieval >10 (OR=3.14, 95% CI: 1.53–6.43, p=0.002) as independent positive predictors of clinical pregnancy. A bootstrap-based mediation model (5000 resamples) showed 68% (95% CI: 41–89%) of LH’s effect on pregnancy was mediated by oocyte yield (indirect effect OR=2.12, 95% CI: 1.21–3.71; Sobel z=2.17, p=0.030).
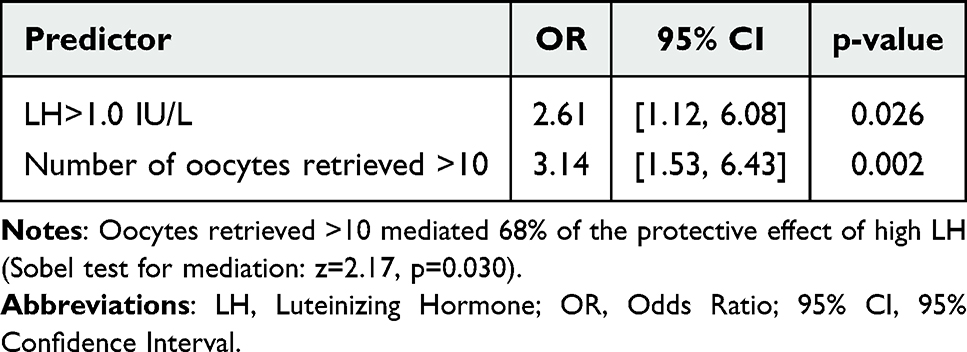 |
Table 4 Multivariate Logistic Regression Analysis of Pregnancy Outcomes in the Long Protocol |
Age-Stratified Analysis
Antagonist Protocol
As shown in Table 5, in patients ≤35 years (n=76), the LH>1.45 IU/L subgroup (n=31) had fewer oocytes retrieved (8.7±3.0 vs 10.8±2.9, p<0.05), lower high-quality embryo rate (34.8±25.1% vs 49.5±22.7%, p<0.05), and a 23.5% lower clinical pregnancy rate (38.7% vs 62.2%, p=0.047) compared to the LH≤1.45 IU/L subgroup (n=45). In patients >35 years (n=26), no significant differences were observed in oocyte retrieval (7.5±3.0 vs 8.7±2.8, p>0.05) or clinical pregnancy rate (25.0% vs 50.0%, p>0.05), though the LH>1.45 IU/L subgroup (n=12) had a lower high-quality embryo rate (26.5±18.5% vs 42.1±21.8%, p<0.01).
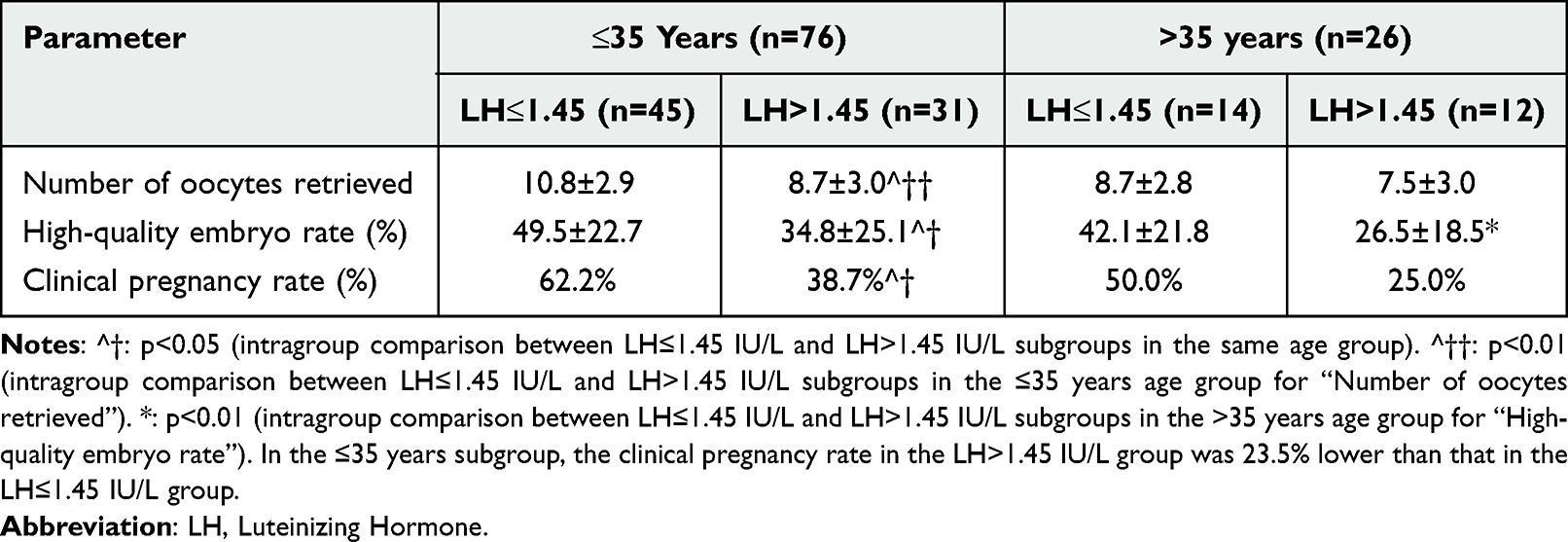 |
Table 5 Age-Stratified Outcomes in the Antagonist Protocol |
Long Protocol
Table 6 shows that in patients ≤35 years (n=85), the LH>1.0 IU/L subgroup (n=15) had a 23.3% higher clinical pregnancy rate (80.0% vs 56.7%, p=0.021) and higher live birth rate (66.7% vs 46.3%, p>0.05) than the combined LH≤1.0 IU/L subgroup (n=70). In patients >35 years (n=30), no significant differences in clinical pregnancy rate (60.0% vs 52.0%, p>0.05) or live birth rate (40.0% vs 40.0%, p>0.05) were found between the LH>1.0 IU/L (n=5) and LH≤1.0 IU/L (n=25) subgroups.
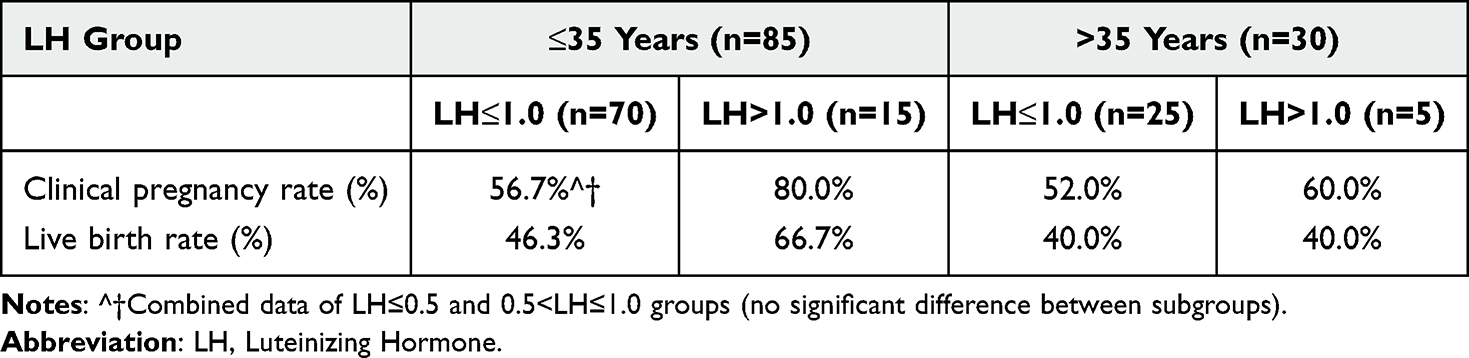 |
Table 6 Age-Stratified Outcomes in the Long Protocol |
Three-Way Interaction of Age, Protocol, and LH
A three-way interaction model (age × protocol × LH group) confirmed age as a critical moderator (Table 7): the interaction term was significant (OR=6.55, 95% CI: 2.56–16.8, p=0.003), and age >35 years weakened the effect of high LH (OR=0.49, 95% CI: 0.27–0.89, p=0.019).
 |
Table 7 Three-Way Interaction Model of Age-Protocol-LH |
Predictive Performance at Thresholds
At the optimal thresholds, the antagonist protocol (1.45 IU/L) had a sensitivity of 69.4%, specificity of 66.0%, positive predictive value (PPV) of 78.6%, and negative predictive value (NPV) of 75.0%. The long protocol (1.0 IU/L) had a sensitivity of 72.0%, specificity of 65.0%, PPV of 75.0%, and NPV of 73.3%. Notably, the AUC values (antagonist protocol: 0.664; long protocol: 0.655) indicate moderate predictive ability of trigger-day LH levels for pregnancy outcomes. This is consistent with the complexity of IVF pregnancy outcomes, which are influenced by multiple factors including follicular synchrony, endometrial thickness, and embryo quality, rather than LH levels alone.
Robustness Verification
Bootstrap resampling (2000 iterations) showed the 95% CI of AUC overlapped with original results by >90%. Sensitivity analysis via propensity score weighting revealed no significant changes in effect direction or magnitude, with details provided in Appendix Table S1.
Discussion
To the best of our knowledge, this study represents the first single-center cohort to systematically assess the impact of trigger-day luteinizing hormone (LH) concentrations on in vitro fertilization (IVF) outcomes under both antagonist and long gonadotropin-releasing hormone (GnRH) agonist protocols, while also quantifying the moderating influence of age. Our results indicate that the two protocols exhibit significantly different tolerances to LH, with critical thresholds of 1.45 IU/L and 1.0 IU/L, respectively, and that chronological age serves as a crucial modifier of these thresholds. These findings challenge the applicability of a uniform LH criterion and support the emerging concept of “precision triggering” as endorsed by recent international consensus.14
The protocol-specific LH thresholds identified in this study provide practical and actionable guidance for individualized ovulation induction strategies in clinical IVF practice. For patients ≤35 years undergoing the antagonist protocol, maintaining trigger-day LH <1.45 IU/L may optimize oocyte yield and subsequent pregnancy outcomes; this clinical goal can be achieved by adjusting the timing of ganirelix administration (initiating earlier in follicular development) or modifying the trigger regimen to reduce endogenous LH elevation. For patients in the long protocol, especially younger women with normal ovarian reserve, allowing LH levels to reach ≥1.0 IU/L on trigger day may enhance follicular response and improve clinical pregnancy rates by harnessing the physiological stimulatory effect of LH on folliculogenesis. These findings emphasize the importance of real-time LH monitoring on trigger day and personalized adjustment of ovarian stimulation protocols based on both patient age and the type of ovulation induction protocol used.
In the antagonist protocol, clinical pregnancy rates decreased by 22.7% when the trigger-day LH levels exceeded 1.45 IU/L. Receiver Operating Characteristic (ROC) curve analysis identified this threshold with high specificity. Mediation modeling demonstrated that elevated LH levels were associated with a reduced oocyte yield, a 7.5% decrease in the rate of metaphase II (MII) oocytes, and a 13.5% reduction in the rate of high-quality embryos, ultimately compromising pregnancy outcomes. Antagonist cycles appear to be particularly susceptible to LH surges, likely due to the rapid and direct suppression of the pituitary gland, which exposes follicles to even brief elevations beyond their developmental tolerance limits.1 These findings are consistent with two recent studies,13,15 but contrast with the results of Liu et al, who reported a favorable effect of higher LH levels.16 The discrepancies may arise from (i) differences in sample size and population heterogeneity—our smaller cohort may emphasize extreme values; (ii) divergent statistical methodologies—Liu utilized tertile splits, whereas we employed an ROC-derived optimized threshold (1.45 IU/L) that is more applicable to clinical decision-making; and (iii) variations in trigger composition—our regimen of triptorelin plus hCG may exacerbate the negative impact of endogenous LH elevations. Furthermore, the adverse effect was restricted to patients aged 35 years or younger, where pregnancy rates decreased by 23.5% when luteinizing hormone (LH) levels exceeded 1.45 IU/L, indicating increased LH sensitivity in younger ovaries.17 In contrast, reduced LH-receptor expression in older patients may mitigate this response.18
In the long protocol, LH levels greater than 1.0 IU/L were associated with a 20.9% increase in clinical pregnancy rates, corroborating previous findings that moderate elevations in LH are advantageous when pituitary down-regulation is substantial.6,8,16 Mediation analysis attributed 68% of this benefit to an increased oocyte yield, suggesting that moderate increases in LH enhance folliculogenesis and ovarian responsiveness.7 However, excessive LH levels may lead to premature luteinization and impair oocyte competence;19,20 the current sample size was insufficient to reliably determine an upper safety threshold for LH in the long protocol, which warrants further investigation in future studies with larger cohorts. Importantly, no protective effect of elevated LH was observed in women older than 35 years, which may be attributed to a series of age-related biological changes in the ovary: (1) Accelerated decline in ovarian reserve leads to a reduced number of primordial and growing follicles and decreased overall responsiveness to gonadotropins;9 (2) Impaired oocyte quality due to increased oxidative stress and mitochondrial dysfunction in oocytes with advancing age;10 (3) Downregulated LH receptor expression on granulosa cells of developing follicles, which weakens the follicular response to LH stimulation;18 (4) Altered endocrine milieu with increased progesterone levels in older patients, which may interfere with LH’s physiological stimulatory effect on folliculogenesis.19
Age was identified as a significant moderator of luteinizing hormone (LH) threshold effects. In women aged 35 years or younger, the positive impact of elevated LH under the long protocol and the negative impact under the antagonist protocol were both intensified. In contrast, older patients exhibited relative resistance to LH fluctuations, a pattern consistent with findings from previous studies on age-related responsiveness.10,18,21 Notably, even within the older subgroup, LH levels exceeding 1.45 IU/L during antagonist cycles were associated with a 15.6% reduction in the rate of high-quality embryos, highlighting the necessity for careful LH monitoring across all age groups.
Based on these findings, we propose an individualized trigger strategy wherein, for antagonist cycles, the trigger-day luteinizing hormone (LH) level should be maintained below 1.45 IU/L, particularly for women aged 35 years or younger. In contrast, for long-protocol cycles, LH levels up to 1.0 IU/L may be permissible to harness its stimulatory potential, provided that excessive elevations are avoided. The implementation of these thresholds is anticipated to optimize cycle management and improve in vitro fertilization (IVF) success rates.
The retrospective, single-center design, even with stringent inclusion and exclusion criteria and rigorous data quality control, cannot completely eliminate selection bias or account for unmeasured confounders such as lifestyle and genetic background. The relatively small sample size for stratification analysis (eg, the >35 years subgroup only included 26 patients) may limit the generalizability of our findings, which is a key limitation of the study. Additionally, the ROC-derived LH thresholds demonstrated only modest discriminatory capacity (antagonist AUC = 0.664; long AUC = 0.655), suggesting that LH alone is neither a definitive nor an independent predictor. Consequently, clinical decisions should incorporate a multidimensional approach, considering factors such as follicular synchrony, endometrial thickness, and comprehensive hormonal profiles, rather than relying solely on the thresholds proposed in this study.
In future studies, multicenter prospective cohorts can be used to validate the LH thresholds identified in this research, and sample sizes can be expanded to explore the upper safety threshold of LH in the long protocol. Additionally, combining indicators such as LH receptor gene polymorphisms and anti-Müllerian hormone (AMH) levels to construct a combined prediction model will further refine personalized protocols and mitigate the limitations of using LH as a single indicator.
Conclusion
This study provides crucial evidence for personalized trigger strategies in IVF treatment. The antagonist and long protocols show different LH sensitivities, with thresholds of 1.45 IU/L and 1.0 IU/L respectively, and age significantly influences this effect. By precisely controlling LH levels on the trigger day and considering patient age and protocol characteristics, IVF pregnancy outcomes can be optimized, offering a new perspective on individualized treatment in reproductive medicine.
Abbreviations
AMH, Anti-Müllerian Hormone; AUC, Area Under the Curve; BMI, Body Mass Index; CI, Confidence Interval; CPR, Clinical Pregnancy Rate; FSH, Follicle-Stimulating Hormone; Gn, Gonadotropin; hCG, Human Chorionic Gonadotropin; ICSI, Intracytoplasmic Sperm Injection; IPTW, Inverse Probability of Treatment Weighting; IU, International Unit; LH, Luteinizing Hormone; MII, Metaphase II; OR, Odds Ratio; rFSH, Recombinant Follicle-Stimulating Hormone; ROC, Receiver Operating Characteristic; RR, Relative Risk; SE, Standard Error.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author (Huaiyun Tang) upon reasonable request.
Ethical Approval
This study was approved by the Institutional Ethics Committee of Lianyungang Maternal and Child Health Hospital (Approval No.: LYG-MER2021039). The study was conducted in accordance with the principles of the Declaration of Helsinki. For this retrospective study using anonymized electronic medical record data, the ethics committee waived the requirement for written informed consent, as patient privacy was fully protected.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Jiangsu Provincial Maternal and Child Health Research Project (Grant No.: F202122).
Disclosure
The authors declare no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Lyttle Schumacher BM, Mersereau JE, Steiner AZ. Cycle day, estrogen level, and lead follicle size: analysis of 27,790 in vitro fertilization cycles to determine optimal start criteria for gonadotropin-releasing hormone antagonist. Fertil Steril. 2018;109(4):633–11. doi:10.1016/j.fertnstert.2017.12.021
2. Verschuere H, Laenen A, Debrock S, Tomassetti C, Lie Fong S. Luteinizing hormone profiles during ovarian stimulation in assisted reproductive treatment. Front Endocrinol. 2024;15:1481546. doi:10.3389/fendo.2024.1481546
3. Zhang Q, Zhang K, Gao Y, et al. Effect of LH level on HCG trigger day on clinical outcomes in patients with diminished ovarian reserve undergoing GnRH-antagonist protocol. Reprod Biol Endocrinol. 2024;22(1):107. doi:10.1186/s12958-024-01280-0
4. Xu Z, Lin Q, Liang Z, et al. Optimising luteinising hormone levels on trigger day for improved ovarian response and pregnancy outcomes in gonadotropin-releasing hormone antagonist protocols: a retrospective cohort study. Bjog. 2025;132(S2):44–52. doi:10.1111/1471-0528.18064
5. Chen Y, Li Y, Li X, et al. Lower serum LH level was related to poor embryo quality and adverse pregnancy outcomes in fixed GnRH antagonist protocol with estradiol pretreatment. Gynecol Endocrinol. 2024;40(1):2409147. doi:10.1080/09513590.2024.2409147
6. Luo X, Deng B, Li L, Ma R, Mai X, Wu Z. LH level on ovulation trigger day has a different impact on the outcomes of agonist and antagonist regimens during in vitro fertilization. J Ovar Res. 2023;16(1):26. doi:10.1186/s13048-023-01110-8
7. Dragotto J, Buzzaccarini G, Etrusco A, et al. Effects of low luteinizing hormone serum levels on oocyte retrieval, fertilization rate, and embryo quality during controlled ovarian stimulation: results from a prospective cohort analysis. Gynecol Obstet Invest. 2024;89(1):50–58. doi:10.1159/000534860
8. Fábregues F, Creus M, Casals G, Carmona F, Balasch J. Outcome from consecutive ICSI cycles in patients treated with recombinant human LH and those supplemented with urinary hCG-based LH activity during controlled ovarian stimulation in the long GnRH-agonist protocol. Gynecol Endocrinol. 2013;29(5):430–435. doi:10.3109/09513590.2012.754873
9. Bao S, Yin T, Liu S. Ovarian aging: energy metabolism of oocytes. J Ovar Res. 2024;17(1):118. doi:10.1186/s13048-024-01427-y
10. Yurchuk T, Petrushko M, Fuller B. State of the art in assisted reproductive technologies for patients with advanced maternal age. Zygote. 2023;31(2):149–156. doi:10.1017/S0967199422000624
11. Ferraretti AP, La Marca A, Fauser BC, Tarlatzis B, Nargund G, Gianaroli L. ESHRE consensus on the definition of ‘poor response’ to ovarian stimulation for in vitro fertilization: the Bologna criteria. Hum Reprod. 2011;26(7):1616–1624. doi:10.1093/humrep/der092
12. Abu-Musa A, Haahr T, Humaidan P. Novel physiology and definition of poor ovarian response; clinical recommendations. Int J Mol Sci. 2020;21(6):2110. doi:10.3390/ijms21062110
13. Sperduti S, Paradiso E, Anzivino C, et al. LH increases the response to FSH in granulosa-lutein cells from sub/poor-responder patients in vitro. Hum Reprod. 2023;38(1):103–112. doi:10.1093/humrep/deac246
14. Ovarian Stimulation T, Bosch E, Broer S, et al. ESHRE guideline: ovarian stimulation for IVF/ICSI†. Hum Reprod Open. 2020;2020(2):hoaa009. doi:10.1093/hropen/hoaa009
15. Kugelman N, Pooni A, Rotshenker-Olshinka K, Bellemare V, Digby A, Dahan MH. Impact of stimulation with luteinizing hormone activity on IVF outcomes in patients with polycystic ovary syndrome. J Turk Ger Gynecol Assoc. 2024;25(2):60–65. doi:10.4274/jtgga.galenos.2024.2023-12-9
16. Liu S, Liu M, Li L, et al. Patients with deep ovarian suppression following gnrh agonist long protocol may benefit from a modified GnRH antagonist protocol: a retrospective cohort study. Front Endocrinol. 2021;12:618580. doi:10.3389/fendo.2021.618580
17. Nasatzky M, Belicha Y, Fainaru O. Clinical parameters that predict a premature LH rise in patients undergoing ovarian stimulation for IVF. Gynecol Endocrinol. 2024;40(1):2365913. doi:10.1080/09513590.2024.2365913
18. Alviggi C, Vigilante L, Cariati F, Conforti A, Humaidan P. The role of recombinant LH in ovarian stimulation: what’s new? Reprod Biol Endocrinol. 2025;23(Suppl 1):38. doi:10.1186/s12958-025-01361-8
19. Bosch E, Labarta E, Crespo J, et al. Circulating progesterone levels and ongoing pregnancy rates in controlled ovarian stimulation cycles for in vitro fertilization: analysis of over 4000 cycles. Hum Reprod. 2010;25(8):2092–2100. doi:10.1093/humrep/deq125
20. Singh R, Kaur S, Yadav S, Bhatia S. Gonadotropins as pharmacological agents in assisted reproductive technology and polycystic ovary syndrome. Trends Endocrinol Metab. 2023;34(4):194–215. doi:10.1016/jtem.2023.02.002
21. Di Segni N, Busnelli A, Secchi M, Cirillo F, Levi-Setti PE. Luteinizing hormone supplementation in women with hypogonadotropic hypogonadism seeking fertility care: insights from a narrative review. Front Endocrinol. 2022;13:907249. doi:10.3389/fendo.2022.907249
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.