Back to Journals » Drug Design, Development and Therapy » Volume 13
Protective effects of tiopronin against oxidative stress in severely burned patients
Authors Qin FJ, Hu XH, Chen Z, Chen X, Shen YM
Received 16 May 2019
Accepted for publication 9 July 2019
Published 13 August 2019 Volume 2019:13 Pages 2827—2832
DOI https://doi.org/10.2147/DDDT.S215927
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Feng-Jun Qin, Xiao-Hua Hu, Zhong Chen, Xu Chen, Yu-Ming Shen
Department of Burns, Beijing Jishuitan Hospital, Beijing, People’s Republic of China
Objective: Tiopronin is an antioxidant. This study investigated the protective effect of tiopronin on oxidative stress in patients with severe burns.
Method: Patients aged between 16 and 65 years old with >30% body surface area burns admitted to our burn unit from July 2011 to September 2016 were randomly divided into 3 groups: group A treated with tiopronin (15 mg/kg. 24 hrs), group B with vitamin C (792 mg/kg. 24 hrs), the other group with standard treatment (group C). All 3 groups also received standard treatment. Blood superoxide dismutase (SOD), malondialdehyde (MDA), and the biochemical indexes of liver, kidney, and heart were determined before treatment and 24 and 48 hrs after treatment. Samples from 8 normal healthy adult volunteers were also measured. The resuscitation fluid volume requirement for the first 24 hrs was calculated for 3 groups.
Results: The serum levels of MDA and the biochemical indexes in severely burned patients were higher than those in healthy volunteers (P<0.01). The serum SOD level of burn patients was lower (P<0.01). After treatment, the levels of SOD increased, the levels of MDA decreased, and the biochemical indexes of heart, liver, and kidney improved; these changes were more obvious in group A and group B compared to group C (P<0.05), and these changes were more obvious in group A compared to group B (P<0.05) at 48 hrs after treatment. There is less resuscitation fluid volume requirement to maintain adequate stable hemodynamic and urine output in the first 24 hrs in group A and group B compared to group C (P<0.05).
Conclusion: Treatment with tiopronin could exert protective effects against burn-induced oxidative tissue damage and multiple-organ dysfunction, and also could reduce the volume of required fluid resuscitation in severely burned patients.
Keywords: burn, oxygen free radical, oxidative stress, tiopronin, vitamin C, severely burned patients
Introduction
Oxygen free radical (OFR), produced by burns, is an important factor in tissue damage, which can increase vascular permeability and cell membrane lipid peroxidation and cause local and systemic inflammation.1,2 The previous studies reminded that burns can promote lipid peroxidation.3–5 Lipid peroxidation is an autocatalytic reaction which induces toxic metabolism and cell apoptosis. In addition, the application of antioxidants after burns has protective effects on oxidative tissue damage and organ failure.6–8 To improve treatment effects and prevent OFR injuries, antioxidants must be used as early as possible in severely burned patients.3,6
Tiopronin [N-(2-mercaptopropionyl)-glycine] is a commonly used antioxidant with a free mercapto group. Some reports indicated that it is a free radical scavenger that prevents cell membrane damage from free radicals. Tiopronin has been widely used in the treatment of various diseases.9,10 But to date, there are no reports of tiopronin used in burn patients. In addition, vitamin C is water soluble and in the aqueous phase it is an antioxidant. It not only scavenges oxygen radicals, such as superoxide (O2−), hydroxyl radical (OH−), and singlet oxygen (O−), but along with citamin E, it also has a chain breakage-type antioxidizing effect and terminates oxygen radical reaction inside and outside of cell membranes.11 It was widely publicized as a universal antioxidant, which in high doses is a useful and safe therapy for the burn shock period.12–15
As previous work has relied on animal-based models with little clinical information, in this study, we investigated the protective effects of tiopronin against oxidative stress in severely burned patients, using treatment with vitamin C and standard treatment as control.
Methods
The Institutional Ethics Committee of Ji Shui Tan Hospital approved this clinical study, and informed consent was obtained from the patient or legal next of kin.
From July 2011 to September 2016, patients aged between 16 and 65 years, with more than 30% total body surface area (TBSA) burns, were admitted to our burn unit less than 6 hrs postburn. They had no liver or kidney dysfunction. Thirty-six consecutive patients were randomized into 3 groups: group A (n=12), group B (n=12), and group C (n=12). One patient in group A, who died on the second day after admission because of severe inhalation injury, was excluded. The profiles of the three groups were similar regarding age, gender, BSA burns and percent of full-thickness burn, the presence of inhalation injury and whether they required mechanical ventilation (P>0.05,Table 1). Fluid infusion was started immediately after admission according to the Evans formula but with real burns TBSA. The hourly infusion volume was adjusted to maintain stable hemodynamic values (systolic blood pressure>12 kPa, heart rate<120/min, central venous pressure 0.49 kPa–0.98 kPa) and adequate urine output (0.5–1.0 mL/kg/hr). Group A was treated with tiopronin intravenously for 7 days (15 mg/kg.24 hrs, Hennan Province Xinyi Pharmaceutical Co., Ltd, XinXiang City, China), while group B was treated with vitamin C (in the form of L-ascorbic acid) intravenously for 7 days (792 mg/kg.24 hrs, Beijing Double-Crane Pharmaceutical Co., Ltd, Chaoyang District, Beijing, China). Treatment was divided into 4 infusions, group C was treated with standard therapy (including rapid and enough fluid resuscitation according to the Evans formula, nutrition support by enteral nutrition, systemic and topical application of antibiotics, critical care by cardiac monitoring, and so on), and the other 2 groups also received standard therapy.
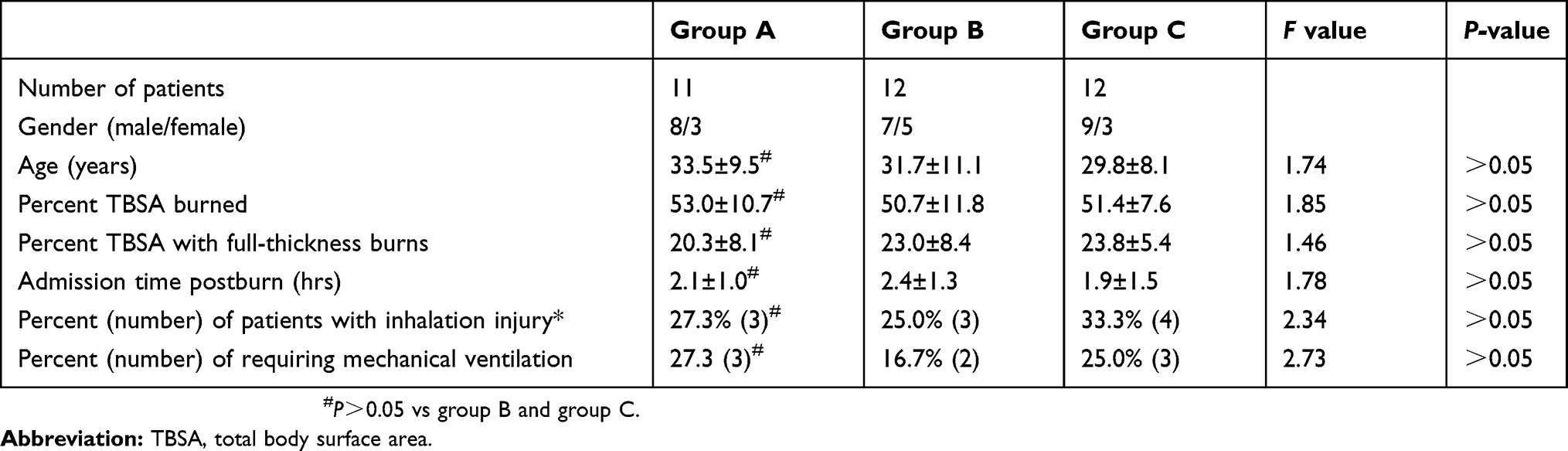 |
Table 1 Patient demographics |
A series of blood samples were collected before treatment; and after treatment at 24 and 48 hrs. Immediately after collection, serum was removed by centrifuge and stored at −20°C as soon as possible until assayed. Samples from eight normal healthy adult volunteers (5 males, 3 females, 18~30 years of age) were also measured.
Malondialdehyde (MDA) level was measured by thiobarbituric acid use MDA kit, and superoxide dismutase (SOD) activity was detected by inhibiting nitrite formation use SOD kit (both kits were issued by Nanjing Jiancheng Bioengineering Institute, Xuanwu District, Nanjing City, China), operated strictly according to the instructions of the kit. Add 0.5ml serum to the MDA kit, measuring optical density (OD) value of MDA at 532 nm using Microplate Reader (BECAM-CULTER, Atlanta Vision Center, Atlanta, Georgia, USA), and also add 0.5ml serum to the SOD kit, measuring OD value of SOD at 550 nm using Microplate Reader, and calculating the concentration of MDA and SOD in serum samples. Alanine aminotransferase (ALT), aspartate aminotransferase (AST), lactate dehydrogenase (LDH), blood urea nitrogen (BUN), creatinine (Cr), creatine kinase-MB (CK-MB), cystatin C (CysC), and cardiac troponinI (CTnI) were determined using automated analyzer (MONRH, BECAM-CULTER and BECK MAN DXC800, USA), operated strictly according to the instructions of the kit (the kits were issued by BECAM-CULTER, Atlanta Vision Center, Atlanta, Georgia, USA). Biochemical indexes of liver, kidney, and heart were determined directly using automated analyzer. The resuscitation fluid volume requirement for 3 groups was calculated during the first 24 hrs.
Statistical analysis
Statistical analysis was performed using SPSS 16.0 software. Values were expressed as mean ± SD. Categorical variables were compared by Chi-square test, repeated-measures ANOVA were compared among groups, and least significant difference (LSD) test for multiple comparisons between groups, P<0.05 was considered significant.
Results
MDA levels in serum were found to be markedly higher in severely burned patients than in healthy volunteers (P<0.01), while treatment reversed these elevations back to normal. In contrast, SOD levels in serum were discernibly lower in burned patients compared to healthy volunteers (P<0.01), while treatment inhibited the depletion of SOD stores. These changes were more obvious in group A and group B compared to that in group C (P<0.05), and these changes were more obvious in group A compared to that in group B (P<0.05) at 48 hrs after treatment (Table 2).
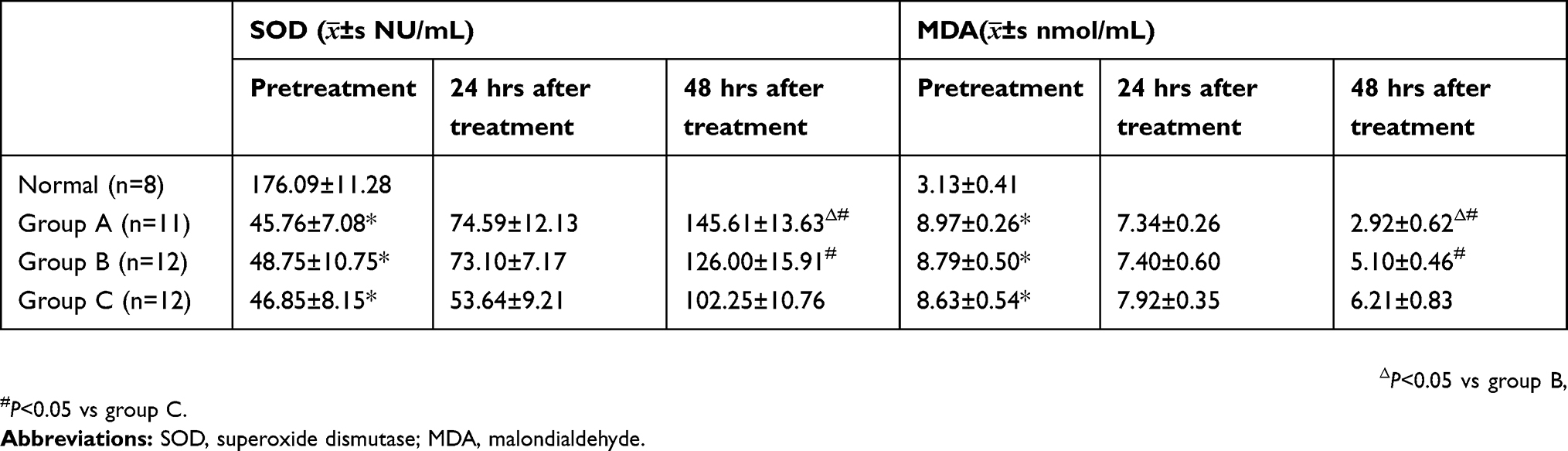 |
Table 2 The serum levels of SOD and MDA |
Serum ALT and AST levels were determined to evaluate the hepatic function; CysC, BUN, and Cr concentrations were studied to assess the renal function; and CTnI, CK-MB, and LDH levels were determined to evaluate the heart function. ALT, AST, CysC, BUN, Cr, CTnI, CK-MB, and LDH levels in burned patients were notably higher than those of healthy volunteers (P<0.01), and this effect was reversed significantly after treatment. There was a statistically significant difference in reversing the elevation of ALT, AST, CysC, CTnI, CK-MB, and LDH in group A and group B compared to that in group C (P<0.05) at 48 hrs after treatment, but there was no obvious difference in reversing the elevation of BUN and Cr in group A and group B compared to that in group C (P>0.05) (Table 3–6). Meanwhile, there was a statistically significant change in reversing the elevation of ALT, AST, CysC, and CTnI in group A compared to that in group B (P<0.05) at 48 hrs after treatment; however, there was no obvious difference in reversing the elevation of CK-MB and LDH in group A compared to that in group B (P>0.05) (Tables 5 and 6).
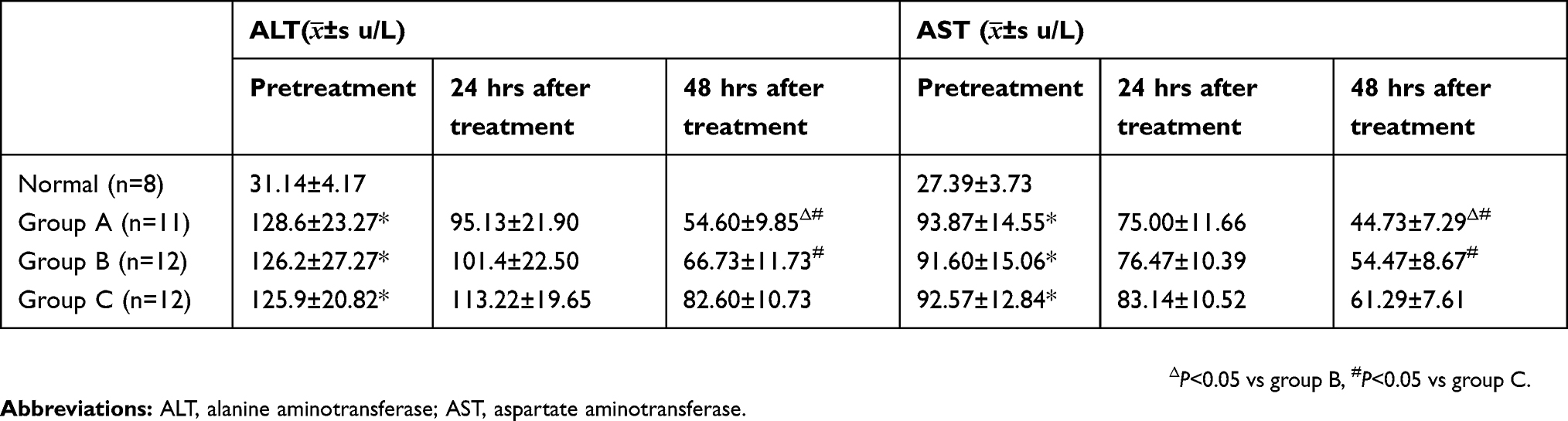 |
Table 3 The serum levels of ALT and AST |
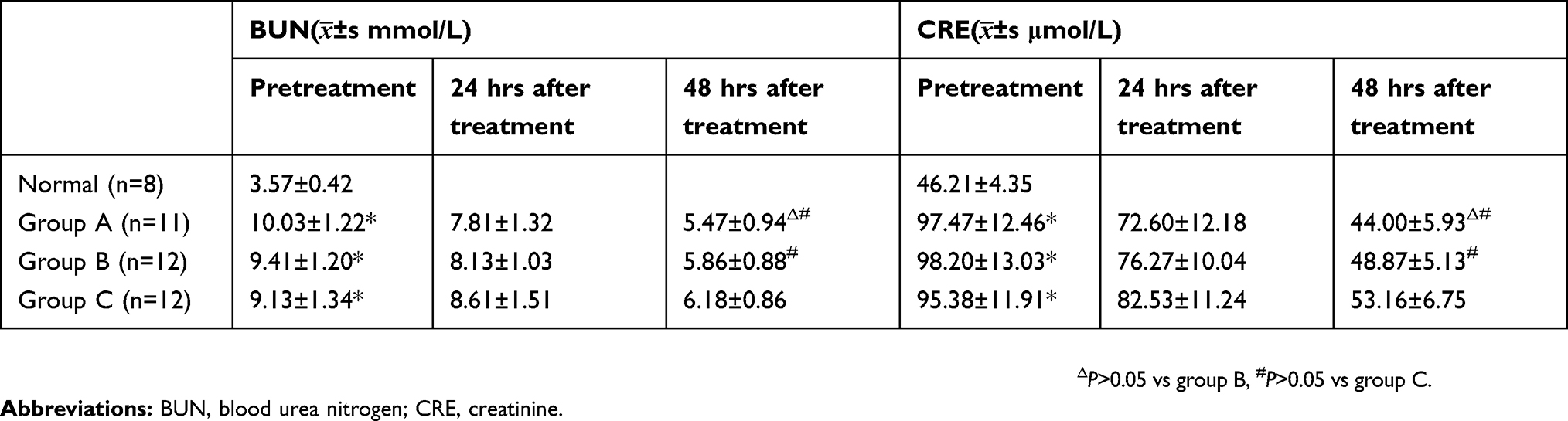 |
Table 4 The serum levels of BUN and CRE |
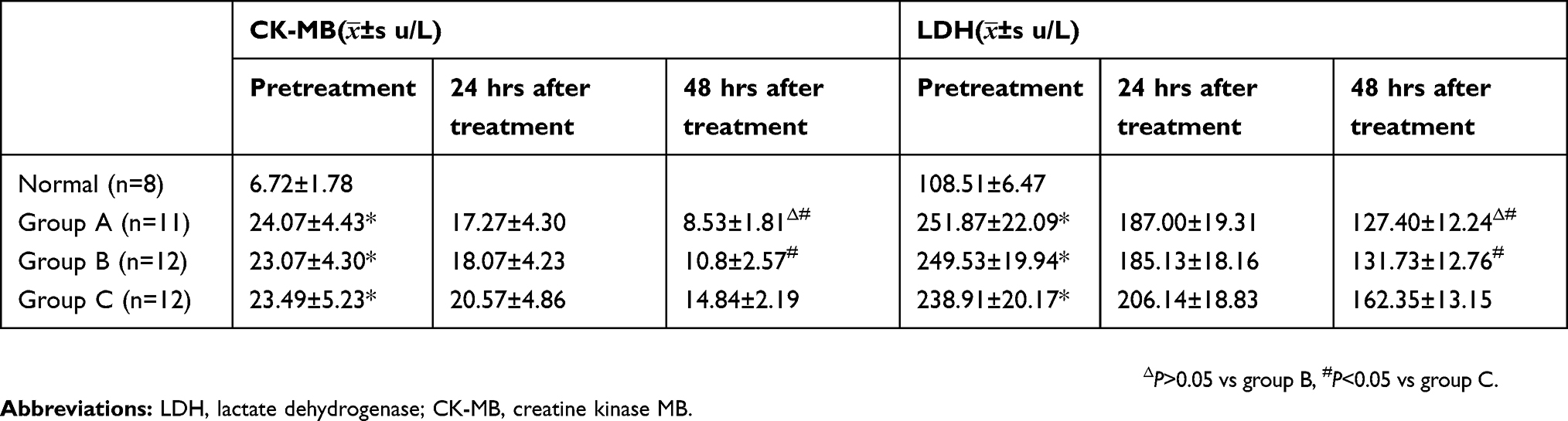 |
Table 5 The serum levels of CK-MB and LDH |
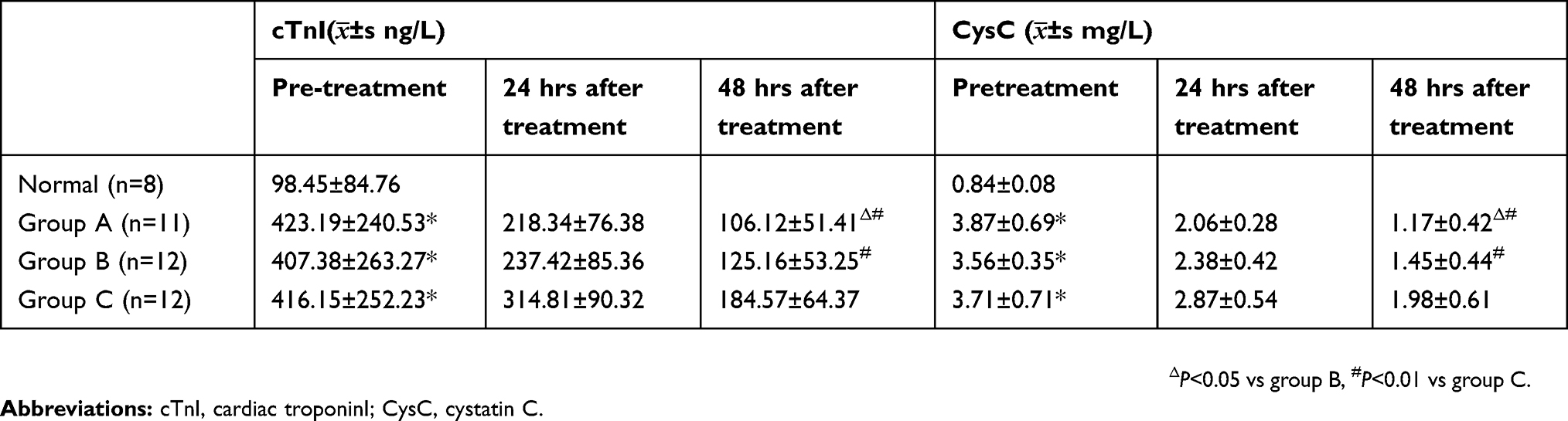 |
Table 6 The serum levels of cTnI and CysC |
The resuscitation fluid volume requirement to maintain adequate stable haemodynamic parameters and urine output in the first 24 hrs in group A = TBSA% × body weight (kg)×1.46 mL (colloid to electrolyte ratio 1:2) + water 2000 mL, whereas group B required = TBSA% × body weight (kg)×1.48 mL (colloid to electrolyte ration 1:2) + water 2000 mL, while group C required = TBSA% × body weight (kg)×1.64 mL (colloid to electrolyte ration 1:2) + water 2000 mL. Compared to group C, it required less resuscitation fluid volume to maintain adequate stable haemodynamic and urine output in group A and group B (P<0.05), but there was no significant difference of resuscitation fluid volume requirement between group A and group B in the first 24 hrs (P>0.05).
Discussion
OFRs are now considered to play an important role in increasing vascular permeability and lipid peroxidation of the cell membrane and initiating local and systemic inflammation.1,2 Burn injury may activate neutrophils to produce additional OFRs via the “respiratory burst” mechanism, utilizing the membrane-bound nicotinamide adenine dinucleotide phosphate (NADPH) oxidase complex.16 However, major burn injuries cause hypovolemia, which requires massive fluid resuscitation, yet adequate fluid resuscitation is often delayed for hours. Restoration of blood flow is necessary, but this restoration may lead to a reperfusion injury. Various studies indicate that OFRs are involved in ischemia–reperfusion injury.2,8,17 Activation of xanthine oxidase via ischemia–reperfusion may generate mass superoxide radicals, subsequently causing the peroxidation of membrane phospholipids, leading to cell death, tissue damage, and distant organ dysfunction. In addition, studies suggested that antioxidants or free radical scavengers are administered after burns and exert protective effects against burn-induced oxidative tissue damage and multiple-organ failure.2,3,6
Measuring OFRs is difficult in clinic because it has a short half-life. MDA is oneterminal metabolite of unsaturated fatty acids peroxidized by attacks from free radicals and is considered to be an index of the level of OFR, thiobarbituric acid method is one of the commonly used methods for the detection of MDA.3 SOD is an important reducing agent and antioxidant involved in maintaining the cellular oxidation reduction balance, which can also scavenge free radicals produced by oxidative stress, and may be useful as an antioxidant and as a cytoprotective agent.18 Combined detection of MDA and SOD can detect OFR injury more effectively.19,20 The present study showed that SOD was markedly depleted and MDA was increased discernibly in severely burned patients, indicating that lipid peroxidation was also increased and that the capacity of antioxidation decreased following severe burns. This result is consistent with the findings of previous studies.6,17
Vitamin C is water soluble and in the aqueous phase is an antioxidant; it not only scavenges oxygen radicals, such as superoxide (O2−), hydroxyl radical (OH−), and singlet oxygen (O−), but along with vitamin E, it also has a chain breakage-type antioxidizing effect and terminates oxygen radical reaction inside and outside of cell membranes.11 Vitamin C can interact with and remove oxygen radicals from vitamin E free radicals and thus regenerate vitamin E. Therefore, vitamin C protects both the capillary endothelium within the burned tissue and the circulating cells. Several experimental and clinical studies have indicated that high-dose vitamin C therapy in severe burns not only reduces the requirement for resuscitation fluid , but also alleviates burn edema and lipid peroxidation.12,13 The optimum dose of Vitamin C for humans has not yet been determined, but a previous study demonstrated that high dose vitamin C (66 mg/kg.hour) administration to humans is safe.13,15,21 This dosage was used in the present study, but was divided into 4 infusions.
Tiopronin, (N-(2-mercaptopropionyl)-glycine), is a commonly used antioxidant with a free thiol (sulphydryl) group. This molecule, in common with other sulfhydryl (SH)-containing compounds, not only scavenges oxygen radicals, such as superoxide (O2−) and hydroxyl radical (OH−), but also improves the capacity of SOD to scavenge oxygen radicals; moreover, its SH groups maintain the intracellular glutathione level. Tiopronin has several advantages over other sulphydryl compounds as a possible clinical antidote and is already used clinically to treat various hepatic disorders, nephrotoxicity, and cystine urolithiasis.9,10,22 This greatly simplifies its introduction as a protective drug. So far, tiopronin has caused very few adverse effects in clinical use. Previous studies have demonstrated that the dose tiopronin (15 mg/kg.24 hrs) administration to humans is safe,9,10 this dosage was used in the present study.
The present study showed that after being treated with tiopronin or vitamin C, levels of SOD were markedly increased; levels of MDA were obviously decreased; and heart, liver, and kidney function was improved. These changes were more obvious in tiopronin group compared with vitamin C group at 48 hrs after treatment. While tiopronin provided more effective protection compared to being treated with vitamin C, the mechanisms remain to be determined.
CTnI is considered the most sensitive and special target to evaluate myocardial injury.23 In this study, CTnI level was obviously decreased when treated with tiopronin compared to vitamin C at 48 hrs after treatment; however, the levels of CK-MB and LDH had no obvious difference. CysC is a more sensitive index of early renal function injury than BUN and Cr.24 Our data reminded that BUN and Cr levels had no obvious difference in tiopronin group, vitamin C group, and the standard control group at 48 hrs after treatment. However, compared with the standard control group, the level of CysC was markedly decreased in tiopronin group and vitamin C group.
Previous studies have indicated that vitamin C inhibits the increased vascular permeability in burned patients, and subsequently reduces the volume of required fluid resuscitation.12,13,21 The present study suggested that compared with the standard control group, it required less resuscitation fluid volume to maintain adequate stable hemodynamic and urine output in tiopronin group and vitamin C group. However, there was no significant difference in resuscitation fluid volume requirement between tiopronin group and vitamin C group in the first 24 hrs. The above results indicated that tiopronin could reduce the volume of required fluid resuscitation, while maintaining adequate stable hemodynamic parameters and urine output.
OFR produced by burns is an important factor in tissue damage and organ dysfunction. Treatment with tiopronin could exert protective effects against burn-induced oxidative tissue damage and multiple-organ dysfunction, and also could reduce the volume of required fluid resuscitation in severely burned patients, and may be a useful therapy for the burn shock period.
Ethical statement
All procedures were performed in accordance with the Declaration of Helsinki of the World Medical Association. The study was approved by the ethics committee of Beijing Jishuitan Hospital, Beijing, China. This written consent for the study was obtained from the patients.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tian KY, Liu XJ, Xu JD, et al. Propofol inhibits burn injury-induced hyperpermeability through an apoptotic signal pathway in microvascular endothelial cells. Braz J Med Biol Res. 2015;48(5):401–407. Epub 2015 Mar 6. doi:10.1590/1414-431X20144107
2. AbuBakr HO, Aljuaydi SH, Abou-Zeid SM, et al. Burn-induced multiple organ injury and protective effect of lutein in rats. Inflammation. 2018;41(3):760–772. doi:10.1007/s10753-018-0730-x
3. Arti P, Mordhwaj S, Stephen M, et al. Oxidative stress and anti-oxidative mobilization in burn injury. Burns. 2008;34(1):6–17. doi:10.1016/j.burns.2007.04.009
4. Mühl D, Woth G, Drenkovics L, et al. Comparison of oxidative stress & leukocyte activation in patients with severe sepsis & burn injury. Indian J Med Res. 2011;134:69–78.
5. Foldi V, Csontos C, Bogar L, et al. Effects of fluid resuscitation methods on burn trauma-induced oxidative stress. J Burn Care Res. 2009;30(6):957–966. doi:10.1097/BCR.0b013e3181bfb75e
6. Jureta W. Free radicals and lipid peroxidation mediated injury in burn trauma: the role of antioxidant therapy. Toxicology. 2003;189(1–2):75–88.
7. Sener G, Kabasakal L, Cetinel S, et al. Leulotriene blocker montelukast receptor protects against burn-induced oxidative injury of the skin and remote organs. Burns. 2005;31:587–596. doi:10.1016/j.burns.2005.01.012
8. Csontos C. Hypovolemia and oxidative stress in patients with burn injuries. Orv Hetil. 2009;150(14):629–639. doi:10.1556/OH.2009.28505
9. Li XP, Wen F, Yang W, et al. The role of tiopronin for the prevention of chemotherapy-related liver toxicity in advanced colorectal cancer patients treated with mFOLFOX7: a prospective analysis. Tumori. 2014;100(4):446–451. doi:10.1700/1636.17908
10. Li J, Qiu X, Guo W, et al. Prospective analysis of tiopronin in prevention of sorafenib and antiviral therapy inducing liver toxicity in advanced hepatitis B virus-related hepatocellular carcinoma. Med Oncol. 2015;32(10):238. doi:10.1007/s12032-015-0684-x
11. Choi SW, Benzie IF, Collins AR, et al. Vitamins C and E: acute interactive effects on biomarkers of antioxidant defence and oxidative stress. Mutat Res. 2004;551(1–2):109–117. doi:10.1016/j.mrfmmm.2004.03.006
12. Dubick MA, Williams C, Elgjo GI, et al. High-dose vitamin C infusion reduces fluid requirements in the resuscitation of burn-injured sheep. Shock. 2005;24(2):139–144.
13. Kahn SA, Beers RJ, Lentz CW, et al. Resuscitation after severe burn injury using high-dose ascorbic acid: a retrospective review. J Burn Care Res. 2011;32(1):110–117. doi:10.1097/BCR.0b013e318204b336
14. Berger MM, Oudemans-van Straaten HM. Vitamin C supplementation in the critically ill patient. Curr Opin Clin Nutr Metab Care. 2015;18(2):193–201. doi:10.1097/MCO.0000000000000148
15. Rizzo JA, Rowan MP, Driscoll IR, et al. Vitamin C in burn resuscitation. Crit Care Clin. 2016;32(4):539–546. doi:10.1016/j.ccc.2016.06.003
16. Fu XJ, Peng YB, Hu YP, et al. NADPH oxidase 1 and its derived reactive oxygen species mediated tissue injury and repair. Oxid Med Cell Longev. 2014;20(14):282–854. doi:10.1155/2014/282854
17. Hong IS, Lee HY, Kim HP. Anti-oxidative effects of Rooibos tea (Aspalathus linearis) on immobilization-induced oxidative stress in rat brain. PLoS One. 2014;9(1):e87061. doi:10.1371/journal.pone.0087061
18. Koizumi T, Goto H, Tanaka H, et al. Lecithinized superoxide dismutase suppresses free radical substrates during the early phase of burn care in rats. J Burn Care Res. 2009;30(2):321–328. doi:10.1097/BCR.0b013e318198e764
19. Wang HY, Liu XY, Han G, et al. LPS induces eardiomyocyte injury through calcium-sensing receptor. Mol Cell Biochem. 2013;379(1–2):153–159. doi:10.1007/s11010-013-1637-3
20. Du JT, Li W, Yang JY, et al. Hydrogen sulfide is endogenously genemted in rat skeletal muscle and exerts a protective effect against oxidative stress. Chin Med J(Eng1). 2013;126(5):930–936.
21. Tanaka H, Matsuda T, Miyagantani Y, Yukioka T, Matsuda H, Shimazaki S. Reduction of resuscitation fluid volumes in severely burned patients using ascorbic administration. Arch Surg. 2000;135:326–331. doi:10.1001/archsurg.135.5.558
22. Fetoni AR, Sergi B, Ferraresi A, Paludetti G, Troiani D. Protective effects of alpha-tocopherol and tiopronin against cisplatin-induced ototoxicity. Acta Otolaryngol. 2004;124:421–426. doi:10.1080/00016480410016559
23. Keller T, Zeller T, Peetz D, et al. Sensitive troponin I assay in early diagnosis of acute myocardial infarction. N Engl J Med. 2009;361(9):868–877. doi:10.1056/NEJMoa0903515
24. Abdelaal NA, Shalaby SA, Khashana AK, et al. Serum cystatin C as an earlier predictor of acute kidney injury than serum creatinine in preterm neonates with respiratory distress syndrome. Saudi J Kidney Dis Transpl. 2017;28(5):1003–1014. doi:10.4103/1319-2442.215148
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.