Back to Journals » Drug, Healthcare and Patient Safety » Volume 18
Prosthetic Loosening in a Total Hip Arthroplasty Patient After Breast Cancer Chemotherapy and Hormonal Therapy: A Case Report
Authors Li J, Li S, Li C ![]() , Chen Z, Ding Y
, Chen Z, Ding Y
Received 28 May 2025
Accepted for publication 19 December 2025
Published 17 January 2026 Volume 2026:18 543323
DOI https://doi.org/10.2147/DHPS.S543323
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Siew Siang Chua
Jiemin Li,1,* Shixun Li,2,* Changchuan Li,2 Zhong Chen,2 Yue Ding2
1Department of Nurse Administration, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, 510120, People’s Republic of China; 2Department of Orthopaedic Surgery, Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, 510120, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yue Ding, Department of Orthopaedic Surgery, Sun Yat-sen Memorial Hospital, Sun Yat-sen University, Yanjiang Road, No. 107, Guangzhou, Guangdong, 510120, People’s Republic of China, Email [email protected]
Background: Studies have shown that there are a lot of risk factors that could cause periprosthetic osteolysis and aseptic loosening, threatening the life-span of the hip prosthesis. Breast cancer is one of the most frequent malignancy in women. However, the use of breast cancer chemotherapy and hormonal therapy has been shown to significantly elevate the risk of osteoporosis. Chemotherapy can systematically suppress the anabolism of various organs, ultimately leading to bone metabolism dysfunction and osteolysis. Aromatase inhibitors (AI) function by inhibiting the conversion of androgens to estrogen, thereby reducing systemic estrogen levels, which is essential for maintaining bone mass; however, prolonged estrogen deprivation can lead to osteoporosis, which has been proven to pose a significant threat to the survival of hip implants.
Case Presentation: In this case, the patient suffered hip joint tuberculosis and took intertrochanteric osteotomy procedure at age 24. Seventeen years after, she took Total Hip Arthroplasty (THA). She then undertook chemotherapy and hormonal therapy for breast invasive ductal carcinoma (BI-RADS category III), 1 year after her primary THA. Three years later, she was diagnosed with aseptic loosening of her hip prosthesis. A summary and analysis of her treatment were conducted.
Conclusion: Breast cancer chemotherapy and hormonal therapy might be a threat to the stability of THA prosthesis. More attention should be paid when a Total Hip Arthroplasty patient received chemotherapy and hormonal therapy. Further research is needed to fully understand the impact of breast cancer treatments, as current therapies like hormonal therapy can increase the risk of osteoporosis and fractures.
Keywords: THA, aseptic loosening, breast cancer, chemotherapy, hormone therapy
Background
Total joint replacement (TJR) was one of the most revolutionary breakthroughs in joint surgery. It can effectively alleviate joint pain and restore long-term functionality to the joint. Between 2003 and 2018, a significant number of TJRs were performed in England, Wales, and Northern Ireland, with reports indicating that over 2.7 million such surgeries took place.1 This surge is partly attributed to the rising obesity crisis, as evidenced by a sixfold increase in the number of individuals requiring joint replacement surgery over an eight-year period, from 6,191 in 2009–2010 to 41,761 in 2017−2018.1 In 2010, approximately 0.83% of the population in the United States were living with hip prostheses, a number that reflects the growing trend of total hip replacements, which have significantly improved the quality of life for thousands of individuals.2 Most studies have shown that implants can last approximately 25 years; however, there is still variation in the longevity of implants.3 Between 2003 and 2018, the UK has seen 31,410 first revisions of hip prostheses, with aseptic loosening being the leading cause, accounting for 7,644 cases (24.3%). This trend is supported by research indicating that aseptic loosening, often resulting from wear debris and subsequent osteolysis, is a significant complication following hip replacement surgery, necessitating revision procedures. In the United States, from 2012 to 2017, aseptic loosening was diagnosed in 12.0% of patients undergoing hip revision surgeries, as reported in a study published in the Arthritis Journal.4 Various studies have demonstrated that byproducts from prosthesis, which induce an inflammatory reaction, are the primary cause of periprosthetic osteolysis and aseptic loosening. Other mechanical factors, such as micro-motion, stress shielding, and fluid pressure oscillations, may also play a role in periprosthetic osteolysis.5 Furthermore, studies have demonstrated that osteoporosis exacerbates periprosthetic osteolysis, as wear particles from prosthetic implants can activate inflammatory pathways and contribute to bone resorption. Studies indicate that low bone mineral density (BMD) can lead to implant migration post-Total Hip Arthroplasty (THA), resulting in compromised initial stability and a delay in osseointegration.6 Thus, any factor that could cause a systemic or partial bone loss, might be the risk of periprosthetic osteolysis and aseptic loosening.
Breast cancer is the most frequent malignancy in women. In 2018, more than 2.1 million new cases of breast cancer were diagnosed in women, resulting in 626,679 deaths.7 Recent studies have shown that the average incidence of THA among medicare beneficiaries with breast cancer in the United States of America (USA) is 0.29%,8 while in Norway, the incidence is notably higher at 3.46%.9 Additionally, the prevalence of breast cancer in the USA, affecting about 13% of women,4 may contribute to the medicare population statistics. However, the use of breast cancer chemotherapy and hormonal therapy, particularly aromatase inhibitors (AI), has been shown to significantly elevate the risk of osteoporosis,10 which has been proven to pose a significant threat to the survival of hip implants. Chemotherapy can systematically suppress the anabolism of various organs, ultimately leading to bone metabolism dysfunction and osteolysis.11 Aromatase inhibitors (AI) function by inhibiting the conversion of androgens to estrogen, thereby reducing systemic estrogen levels, which is essential for maintaining bone mass through inhibition of osteoclast activity and modulation of the RANK/RANKL pathway;12 however, prolonged estrogen deprivation can lead to osteoporosis.13 Selective estrogen receptor modulators (SERMs) such as tamoxifen and raloxifene could competitively inhibit the binding of estrogen to estrogen receptors (ER), but their effect on bones remains debatable.14
Raloxifene had long been approved by the FDA for prevention and treatment of osteoporosis in postmenopausal women, reducing the risk of vertebral fractures by about 55% in patients without a prior vertebral fracture over 3 years.15 In most studies, tamoxifen was also demonstrated as a bone protector. Tamoxifen-bound ER dimers could interact with the chromatin at estrogen response elements and play a role in inhibiting ER transcriptional activity in the breast.14 On the contrary, ER transcriptional activity will still be activated by tamoxifen-bound ER dimers in bone in postmenopausal women. Studies have reported that tamoxifen is significantly associated with a decreased risk of osteoporosis and osteoporotic fractures.16 However, some studies hold the completely opposite point of view. An increased incidence of fractures was observed in breast cancer patients who used tamoxifen, with 14.7% of tamoxifen users and 12.9% of non-users receiving a fracture diagnosis within 10 years.17 In another study, tamoxifen use is associated with the increased risk of hip fractures among older women with breast cancer, the adjusted odds ratio of hip fracture was 2.29 for tamoxifen users (95% confidence interval 1.92, 2.72)18(These figures are descriptive and not based on statistical comparison; therefore, no P-values were reported in the cited studies). There are also reports demonstrating that tamoxifen showed no significant effects on bone mass in a disease progression model of the change of BMD.19 The exact effect of tamoxifen and breast cancer treatment on bone is still controversial.
Case Presentation
A 46-year-old female patient with total hip arthroplasty (THA) presented to our department complaining of persistent left hip joint pain accompanied by a limb-length discrepancy of 1.5cm in the left lower extremity. Her medical history revealed left hip joint tuberculosis during her youth, culminating in an intertrochanteric osteotomy procedure at age 24.
Seventeen years after the intertrochanteric osteotomy, in 2013, she came to our hospital on a wheelchair with pain on the left hip joint and a shortage of 3cm on the left lower limb, her Harris score on her left hip was 25. Radiological examination showed that her femur head, femur neck and acetabulum were absent, the femur trochanter along with the flat acetabulum had formed a pseudarthrosis on the left hip (Figure 1A). Acetabuloplasty and THA (Reflection SP3 cup, high polymer polyethylene liner, ceramic femoral head and Synergy cemented stem) were then performed (Figure 1B). After the primary surgery, her pain was released and the lower limbs were at the same length, the Harris score had risen up to 85.
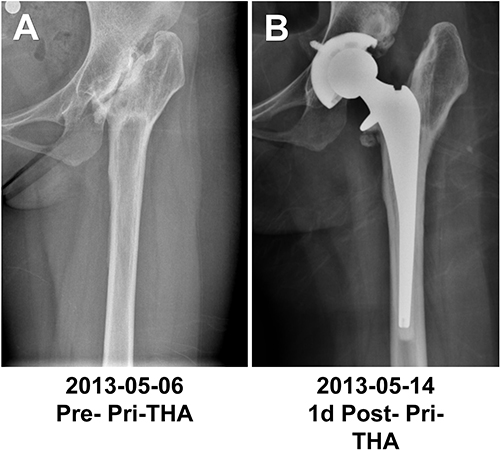 |
Figure 1 X-ray examinations before/post the primary THA. (A): 1 week before primary THA, (B): 1 day post primary THA. |
One year after, she found a mass in her right breast, aspiration biopsy and pathological examination showed the mass was breast invasive ductal carcinoma (T3N0M0, ER(-), PR(-), ERβ(+): 95%, CerbB-2(0), Ki67(+): 15%). She then undertook right breast reservation radical correction in 2014. Afterwards, she received chemotherapy (CEF→T + Dex, Cyclophosphamide 800mg+ Epirubicin 140mg+ 5-FU 800mg +Dexrazoxane 1500mg+ Taxol 280mg) for 6 times and radiotherapy (Surgery field, DT:50Gy/25F) once. From April 2015 until April 2016, she took Tamoxifen for hormone therapy. Her estradiol level was suppressed after the hormone therapy (Figure 2). Throughout the entire treatment period, she experienced no symptoms in her left hip and did not return to our department for follow-up visits. She was a housewife, she was independent in activities of daily living and did moderate physical labor such as housework at home afterwards.
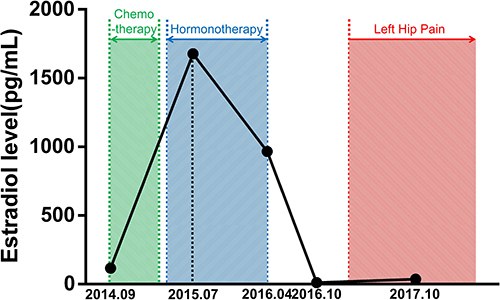 |
Figure 2 Estradiol level during the whole treatment Her estradiol level was tested 5 times during the whole treatment. September 2014 (The time of right breast reservation radical correction): 116pg/mL. July 2015 (Took Tamoxifen for 3 month): 1678pg/mL. April 2016 (Stop taking Tamoxifen): 966pg/mL. October 2016 (Stop taking Tamoxifen 6 months): 11pg/mL. October 2017 (6 months after first dose of zoledronic acid): 35pg/mL. |
On January 2017, she started to feel pain in her left hip again and came to our department on March. Physical examination revealed tenderness at the left hip, with a 1.5cm shortening of the left lower limb, while hip range of motion remained nearly unaffected, yielding a Harris score of 75 at that time. Radiology examination showed a 3mm low density area around the stem, and a 4mm subsidence compared with 4 years ago (Figure 3A). We performed the dual energy x-ray absorptiometry (DXA) to figure out the bone mineral density around the prosthesis. BMD in each area was: Area 1–7: 1.352g/cm2, 1.041g/cm2, 0.940g/cm2, 2.031g/cm2, 0.908g/cm2, 0.889g/cm2, 1.002g/cm2(Figure 3B). Her BMD of the whole body: Right femur neck: BMD: 1.114g/cm2, Z score: 1.4. Right hip: BMD: 1.133g/cm2, Z score: 1.2. Lumbar 1–4: BMD: 1.496g/cm2, Z score: 2.6. Hematological examination showed the Erythrocyte Sedimentation Rate (ESR) was 11mm/h, C-reactive protein (CRP) was 3.11mg/L. By the consideration that the examination during the intertrochanteric osteotomy at the age 24 showed no evidence of infection, and there was no sign of infection during the 17 years afterwards. She was diagnosed as aseptic prosthetic loosening20 and suggested to take revision surgery. However, she refused to take surgery and requested non-surgical treatment. She received 5mg zoledronic acid in order to prevent further osteolysis. On October 2017, radiological examination showed a 5mm low density area around the stem, and a 6mm subsidence compared with 4 years ago (Figure 3C).
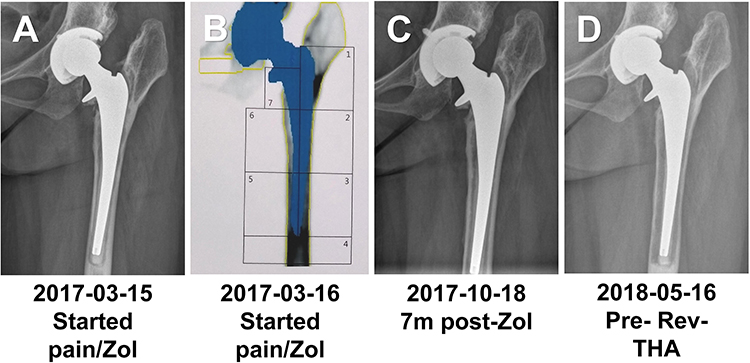 |
Figure 3 X-ray examinations before the revision surgery and BMD examination around the prosthesis. (A): X-ray 4 years post primary THA, (B): The BMD in different area were: Area1: 1.352g/cm2, Area2: 1.041g/cm2, Area3: 0.940g/cm2, Area4: 2.031g/cm2, Area5: 0.908g/cm2, Area6: 0.889g/cm2, Area7: 1.002g/cm2, (C): 7 months post the first 5mg of zoledronic acid, (D): 1 week before revision surgery. |
Afterwards, she kept feeling pain, and the shortening of the left lower limb aggravated. In May 2018, she returned to our department and ultimately decided to undergo revision surgery. This time she had to walk with a walking stick. Her height was 162cm, weight was 68kg, BMI was 25.9 kg/m2 at that time. Physical examination revealed tenderness at the left hip, with a 2.5cm shortening of the left lower limb, while there were still minimal restrictions on the left hip’s range of motion. Her Harris Hip Score for the left hip had diminished to 57, indicating a decline in hip function. Radiological examination showed an 8mm low density area around the stem, and a 10mm subsidence (Figure 3D). Hematological examination showed the ESR was 15mm/h, CRP was 3.14mg/L.
The Echelon Porous Plus HA femoral stem and taper femoral head of Smith & Nephew was prepared. The acetabulum cup was found still stable during the surgery, thus the cup was not revised. However, a periprosthetic femoral fracture occurred while we were removing the cemented stem. The femoral cortex measured less than 2mm in thickness, its razor-thin profile scarcely offering adequate structural reinforcement. We took out all the cement in the femur and then removed the stem. Her femoral cortex around the distal end of the stem were in pieces when we tried to put in the revision stem so that the length of the femur could not be measured accurately. We placed the smallest size of the revision stem in the femur as the new structural reinforcement and repositioned the fracture. Following the reduction, an allograft bone lamella at the interior and a femur plate at the lateral were securely affixed around the femur shaft using cerclage steel wire for stabilization (Figure 4A). Afterwards, the smallest size of the revision stem was removed, and the appropriate size of the stem was placed instead after the femoral medullary dilation. The histopathological examination of the tissue surrounding the prosthesis revealed no signs of wear particles distribution, infection or cancer cells (Figure 4B). She was required to avoid the left lower limb from bearing load for 3 months.
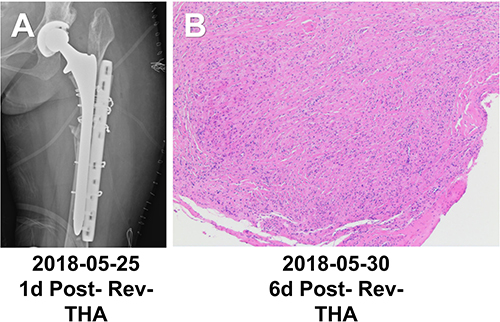 |
Figure 4 X-ray examinations 1d post the revision surgery and Pathological examination of the tissue around the prosthesis. (A): X-ray1 day post revision surgery, (B): No wear particles, infection or cancer cells distribution around the prosthesis. |
Four months after revision, she received another 5mg zoledronic acid in order to prevent further osteolysis. Physical examination showed no tenderness at the left hip, 3cm shortage on the left lower limb this time, and still hardly any limitations on left hip range of motion. She soled her left shoe 3cm higher and was able to walk without a walking-stick, and lived without pain (Harris score: 82). Radiological examination showed the hip prosthesis was stable, and the fracture was healed (Figure 5A). In May 2019, May 2020 and March 2021, she came to countercheck three times. Her hip prosthesis was stable, no pain or limitation of motion in the left hip was observed (Figure 5B–D). Her BMD was improved, and the bone turnover markers were suppressed, indicating the effectiveness of the zoledronic acid treatment (Figure 6). Her X-rays through the entire treatment was summed up in Figure 7. Her entire treatment was summed up as a Chronological Summary in Table 1.
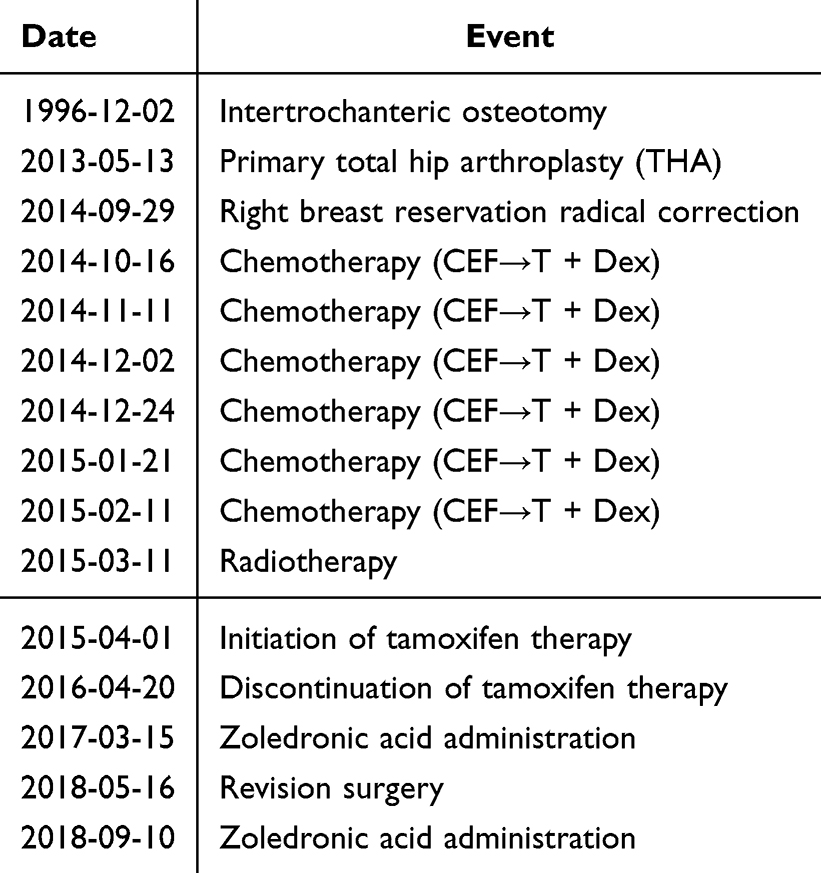 |
Table 1 Chronological Summary of Surgical and Medical Interventions |
 |
Figure 5 X-ray examinations after the revision surgery. The X-ray examinations of the Hip at different time points: (A): Received the second 5mg of zoledronic acid 3month after the revision surgery, (B): 1 year post revision surgery, (C): 2 year post revision surgery, (D): 3 year post revision surgery. |
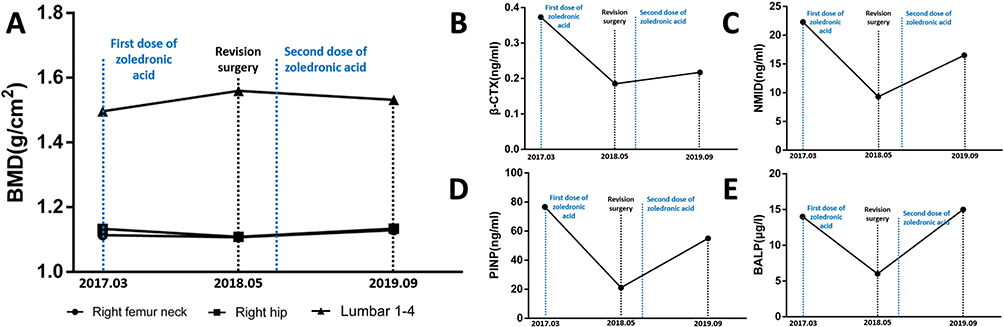 |
Figure 6 Her BMD and the bone turnover level during the whole treatment. (A): Her BMD was tested 3 times during the whole treatment. March 2017 (First dose of zoledronic acid): Right femur neck: BMD: 1.114g/cm2, Z score: 1.4. Right Hip: BMD: 1.133g/cm2, Z score: 1.2. Lumbar 1–4: BMD: 1.496g/cm2, Z score: 2.6. May 2018 (The time of revision surgery): Right femur neck: BMD: 1.107g/cm2, Z score: 1.6. Right hip: BMD: 1.108g/cm2, Z score: 1.0. Lumbar 1–4: BMD: 1.560g/cm2, Z score: 3.4. September 2019 (1 year after the second dose of zoledronic acid): Right femur neck: BMD: 1.129g/cm2, Z score: 1.7. Right hip: BMD: 1.134g/cm2, Z score: 1.2. Lumbar 1–4: BMD: 1.532g/cm2, Z score: 3.5 (B):Her β-CrossLaps (β-CTX) was tested 3 times during the whole treatment. March 2017 (First dose of zoledronic acid): 0.373ng/mL. May 2018 (The time of revision surgery): 0.185ng/mL. September 2019 (1 year after the second dose of zoledronic acid): 0.217ng/mL. (C): Her NMID-Osteocalcin (NMID) was tested 3 times during the whole treatment. March 2017 (First dose of zoledronic acid): 22.3ng/mL. May 2018 (The time of revision surgery): 9.3ng/mL. September 2019 (1 year after the second dose of zoledronic acid): 16.5ng/mL. (D): Her Amino-terminal propeptide of type I procollagen (PINP) was tested 3 times during the whole treatment. March 2017 (First dose of zoledronic acid): 76.59ng/mL. May 2018 (The time of revision surgery): 21.10ng/mL. September 2019 (1 year after the second dose of zoledronic acid): 54.95ng/mL. (E): Her Bone alkaline phosphatase(BALP) was tested 3 times during the whole treatment. March 2017 (First dose of zoledronic acid): 14μg/l. May 2018 (The time of revision surgery): 6μg/l. September 2019 (1 year after the second dose of zoledronic acid): BALP: 15μg/l. |
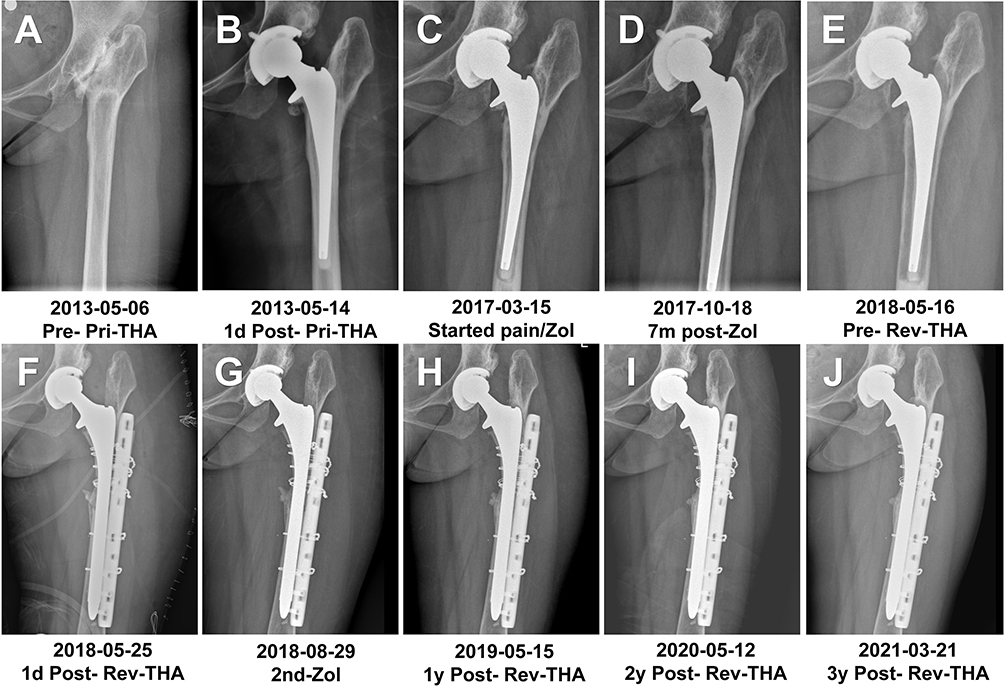 |
Figure 7 X-ray examinations through the whole treatment The X-ray examinations of the Hip at different time points: (A): 1 week before primary THA, (B): 1 day post primary THA, (C): 4 years post primary THA, received the first 5mg of zoledronic acid, (D): 7 months post the first 5mg of zoledronic acid, (E): : 1 week before revision surgery, (F): 1 day post revision surgery, (G): Received the second 5mg of zoledronic acid, (H): 1 year post revision surgery, (I): 2 year post revision surgery, (J): 3 year post revision surgery. |
Discussion
In this case, the patient undertook the primary total hip replacement for the pain and disability of the left hip. The patient’s femoral cortex was thin, classified as C-type of the Dorr classification, so we chose the cemented stem to provide enough stability even she’s only 43 years old. The patient had deformity of her left femur, her marrow cavity of the femur was small, the femoral cortex was thin, and the entotrochanter was missing. To provide enough initial stability, we chose the collared stem. The patient reported satisfaction with the improvement in her quality of life. Pain started to show up and the Harris score started to decrease in the forth year post-operation. ESR and CRP levels were normal, indicating the absence of infection. Dislocation or fracture had never happened. Therefore, she was diagnosed with aseptic loosening, based on her symptom and radiological examination. According to the annual report in UK, most revision that happened 3–7 years after the primary surgery was caused by aseptic loosening.1 The reason for aseptic loosening was confusing.
The main cause of aseptic loosening is usually wear particles, which typically accumulate over a longer period.20 However, in this patient loosening occurred in less than 4 years, suggesting an alternative contributing mechanism. Besides, X-ray images showed no relative displacement between the cup and the head, indicating that there was no obvious wear of the high polymer polyethylene liner. Usually, wear particles from cement or prosthesis should be observed in peri-prosthesis tissues.21 In this patient, pathological examination showed no wear particles distribution, indicating the wear of prosthesis might not be enough to cause aseptic loosening. As for stress shielding, bone resorption would occur in limited areas surrounding the stem, or alternatively, new endosteal bone formation might occur to stabilize the stem.22 In this case, the whole peri-prosthesis bone was absorbed, and there was no sign of endosteal bone formation, the stem was not fixed either. Thus, stress shielding does not seem like the main cause of her loosening. Anyway, micro-motion of the stem cannot be excluded. It is been reported that for cemented stem, the risk of revision was 97% if the subsidence within 2 years was more than 2.6mm, the typical pattern of this kind of loosening was a distal, medial, and posterior migration of the head.23 In this case, the initial stability could not be evaluated because she did not come back for countercheck until she felt pain 4 years post-operation. Her type of loosening was a distal, medial migration of the head, and because of the bone resorption around the stem, micro-motion was likely present beginning in the forth year, and might be the main cause for the aggravation of the bone resorption and the loosening in the fifth year. For osteoporosis, her BMD was tested at the forth year, indicating no primary osteoporosis of the whole body.
Above all, we hypothesize that breast cancer treatment played a primary role in the development and progression of prosthetic loosening in this patient. A prospective study has shown that among 40 premenopausal women with stage I–II breast cancer receiving adjuvant chemotherapy, 31 patients (77.5%) developed chemotherapy-induced ovarian failure, accompanied by a significant decline in bone mineral density (BMD) from a median of 0.993 g/cm2 at baseline to 0.976 g/cm2 and 0.937 g/cm2 at 6 and 12 months, respectively.24 This finding highlights the profound and rapid impact of chemotherapy on bone metabolism in premenopausal women.
As discussed above, cytotoxic chemotherapy can suppress anabolic activity not only in the skeletal system but also in the ovaries, leading to estrogen deficiency and subsequent disruption of bone remodeling balance. In the present case, the patient’s serum estradiol level declined to 11 pg/mL six months after completion of hormonal therapy, while bone turnover markers remained at high-normal levels, suggesting a state of increased bone remodeling and metabolic dysfunction. Such an imbalance favors bone resorption over formation and predisposes to structural bone loss and osteolysis.
Importantly, osteoporosis has been shown to exacerbate periprosthetic osteolysis, as wear particles generated from prosthetic implants can activate inflammatory pathways and stimulate osteoclast-mediated bone resorption.5 Moreover, reduced systemic BMD has been associated with increased implant migration after total hip arthroplasty (THA), resulting in compromised initial stability and delayed osseointegration.6 In our patient, clinical symptoms and radiographic signs of prosthetic instability emerged approximately ten months after treatment-related menopause, temporally correlating with the period of profound estrogen deprivation and altered bone metabolism.
Taken together, these findings suggest that chemotherapy- and hormone therapy–induced bone metabolism disturbances may act as critical systemic contributors to early prosthetic loosening. This case underscores the need for heightened vigilance regarding implant stability in patients with THA who subsequently undergo breast cancer treatment. In such patients, proactive assessment of bone health, closer radiographic surveillance, and early intervention for bone loss may be warranted to mitigate the risk of aseptic loosening and revision failure.
Zoledronic acid has been investigated for its ability to reduce periprosthetic bone loss and thereby lower the risk of aseptic loosening after total joint arthroplasty. By inhibiting osteoclast-mediated bone resorption, zoledronic acid helps preserve periprosthetic bone mineral density, which is critical for long-term implant stability. Several clinical and experimental studies have demonstrated that postoperative administration of zoledronic acid significantly reduces periprosthetic bone loss around femoral and acetabular components, suggesting a protective effect against implant migration and aseptic loosening.25 However, zoledronic acid treatment did raise the BMD of the whole body and inhibit the bone resorption, but the micro-motion of the unstable stem had already took over the progression of loosening, exacerbated the subsidence to 10mm and the thickness of cortical bone to 1–2mm within one year, creating a great challenge for revision surgery. The intraoperative periprosthetic fracture could potentially be prevented if revision surgery is conducted promptly upon the initial diagnosis of prosthesis loosening.
Conclusion
Breast cancer chemotherapy and hormonal therapy might be a threat to the stability of THA prosthesis, initiating and promoting periprosthetic osteolysis and aseptic loosening. We should pay more attention when a THA patient occurred with chemotherapy and hormonal therapy. More studies about the effect of chemotherapy and hormonal therapy on skeleton are required.
Abbreviations
AI, Aromatase inhibitors; BMD, Bone mineral density; CRP, C-reactive protein; DXA, Dual energy x-ray absorptiometry; ER, Estrogen receptors; ESR, Erythrocyte Sedimentation Rate; SERMs, Selective estrogen receptor modulators; TJR, Total joint replacement.
Data Sharing Statement
The research data are obtained from our hospital, which were not publicly available on ethical grounds.
Ethics Approval and Consent to Participate
This research was approved by the Sun Yat-sen Memorial Hospital Ethics committee, and the approval of Sun Yat-sen Memorial Hospital was required for publication of the case details (Ethics approval reference number: SYSEC-KY-KS-2020-174). Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Acknowledgments
The abstract of this paper was presented at the 2022 International Combined Orthopaedic Research Society meeting name “Prosthetic Loosening in a Total Hip Arthroplasty Patient after Breast Cancer Chemotherapy and hormonal therapy: A Case Report” as a presentation with interim findings.26
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Funding
This work was supported by the National Natural Science Fund (82372415), Guangzhou Science and Technology Plan project (SL2023A04J02009,2024A04J4682), and Sun Yat-sen University Clinical Research 5010 Program(2018006).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Ben-Shlomo Y, Blom A, Boulton C, et al. The national joint registry 16th annual report. 2019.
2. Maradit Kremers H, Larson DR, Crowson CS, et al. Prevalence of total Hip and knee replacement in the United States. J Bone Joint Surg Am. 2015;97(17):1386–10. doi:10.2106/JBJS.N.01141
3. JT E, JP E, Walker RW, Blom AW, Whitehouse MR, Sayers A. How long does a Hip replacement last? A systematic review and meta-analysis of case series and national registry reports with more than 15 years of follow-up. Lancet. 2019;393(10172):647–654. doi:10.1016/S0140-6736(18)31665-9
4. American Academy of Orthopaedic Surgeons. American Joint Replacement Registry (AJRR) 2018 Annual Report. 2018.
5. Goodman SB, Gallo J. Periprosthetic osteolysis: mechanisms, prevention and treatment. J Clin Med. 2019;8(12):2091. doi:10.3390/jcm8122091
6. Finnilä S, Moritz N, Svedström E, Alm JJ, Aro HT. Increased migration of uncemented acetabular cups in female total Hip arthroplasty patients with low systemic bone mineral density: a 2-year RSA and 8-year radiographic follow-up study. Acta Orthop. 2016;87:48–54. doi:10.3109/17453674.2015.1115312
7. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
8. Rosas S, Sabeh K, Kurowicki J, et al. National use of total Hip arthroplasty among patients with a history of breast, lung, prostate, colon or bladder cancer: an analysis of the Medicare population. Ann Transl Med. 2017;5:473. doi:10.21037/atm.2017.11.18
9. Dybvik E, Furnes O, Fosså SD, Trovik C, Lie SA. Long-term risk of receiving a total Hip replacement in cancer patients. Cancer Epidemiol. 2009;33:152–157. doi:10.1016/j.canep.2009.06.009
10. Paschou SA, Augoulea A, Lambrinoudaki I. Bone health care in women with breast cancer. Hormones. 2020;19(2):171–178. doi:10.1007/s42000-019-00164-y
11. Shapiro CL, Manola J, Leboff M. Ovarian failure after adjuvant chemotherapy is associated with rapid bone loss in women with early-stage breast cancer. J Clin Oncol. 2001;19(14):3306–3311. doi:10.1200/JCO.2001.19.14.3306
12. Hadji P, Aapro MS, Body JJ, et al. Management of aromatase inhibitor-associated bone loss in postmenopausal women with hormone-sensitive breast cancer: joint position statement of the IOF, CABS, ECTS, IEG, ESCEO, IMS, and SIOG. J Bone Oncol. 2017;7:1–12. doi:10.1016/j.jbo.2017.03.001
13. Waks AG, Winer EP. Breast cancer treatment: a review. JAMA. 2019;321(3):288–300. doi:10.1001/jama.2018.19323
14. Hanker AB, Sudhan DR, Arteaga CL. Overcoming endocrine resistance in breast cancer. Cancer Cell. 2020;37(4):496–513. doi:10.1016/j.ccell.2020.03.009
15. Cosman F, de Beur SJ, LeBoff MS, et al. Clinician’s guide to prevention and treatment of osteoporosis. Osteoporos Int. 2014;25(10):2359–2381. doi:10.1007/s00198-014-2794-2
16. Lee J, Alqudaihi HM, Kang MS, et al. Effect of tamoxifen on the risk of osteoporosis and osteoporotic fracture in younger breast cancer survivors: a nationwide study. Front Oncol. 2020;10:587. doi:10.3389/fonc.2020.00366
17. Stumpf U, Kostev K, Kyvernitakis I, Böcker W, Hadji P. Incidence of fractures in young women with breast cancer: a retrospective cohort study. J Bone Oncol. 2019;18:100254. doi:10.1016/j.jbo.2019.100254
18. Hung SC, Liao KF, Hung HC, et al. Tamoxifen use correlates with increased risk of Hip fractures in older women with breast cancer: a case-control study in Taiwan. Geriatr Gerontol Int. 2018;18:1560–1566.
19. Yoon SK, Bae KS, Cho YS, Han S, Kim H, Lim HS. Disease progression modeling analysis of the change of bone mineral density by postoperative hormone therapies in postmenopausal patients with early breast cancer. J Clin Pharmacol. 2019;59:1–8. doi:10.1002/jcph.1451
20. Anil U, Singh V, Schwarzkopf R. Diagnosis and detection of subtle aseptic loosening in total Hip arthroplasty. J Arthroplasty. 2022;37(8):1494–1500. doi:10.1016/j.arth.2022.02.060
21. Li S, Qiu J, Qin L, et al. NOD2 negatively regulates titanium particle-induced osteolysis in mice. Biomater Sci. 2019;7:2702–2715. doi:10.1039/C9BM00306A
22. Engh CA, Bobyn JD, Glassman AH. Porous-coated Hip replacement: the factors governing bone ingrowth, stress shielding, and clinical results. J Bone Joint Surg Br. 1987;69(1):45–55. doi:10.1302/0301-620X.69B1.3818732
23. Kärrholm J, Herberts P, Hultmark P, Malchau H, Nivbrant B, Thanner J. Radiostereometry of Hip prostheses. Clin Orthop Relat Res. 1997;344:94–110.
24. Oostra DR, Lustberg MB, Reinbolt RE, Pan X, Wesolowski R, Shapiro CL. Association of osteoprotegerin and bone loss after adjuvant chemotherapy in early-stage breast cancer. Mol Cell Endocrinol. 2015;402:51–56. doi:10.1016/j.mce.2014.12.028
25. Gao J, Gao C, Li H, Wang GS, Xu C, Ran J. Effect of zoledronic acid on reducing femoral bone mineral density loss following total Hip arthroplasty: a meta-analysis of randomized controlled trials. Int J Surg. 2017;47:116–126. doi:10.1016/j.ijsu.2017.08.559
26. Ding Y, Li S, Li C, Chen Z, Wu C. Prosthetic loosening in a total Hip arthroplasty patient after breast cancer chemotherapy and hormonal therapy: a case report. Orthop Proc. 2023;105(7):110. doi:10.1302/1358-992X.2023.7.110
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.