Back to Journals » Infection and Drug Resistance » Volume 19
Prosthetic Joint Infection Caused by Staphylococcus argenteus: mNGS-Guided Diagnosis and Whole-Genome Characterization of an ST2250 Strain
Authors Li Z ![]() , Zhang Y, Xu H, Wang D
, Zhang Y, Xu H, Wang D ![]() , Yuan L, Su N, Lu H, Li W
, Yuan L, Su N, Lu H, Li W
Received 10 February 2026
Accepted for publication 25 March 2026
Published 15 April 2026 Volume 2026:19 594406
DOI https://doi.org/10.2147/IDR.S594406
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Hazrat Bilal
Zhiqiang Li,1 Yuqiong Zhang,2,3 Hongxing Xu,2,3 Danhua Wang,4 Liruoke Yuan,5 Ning Su,2,3 Han Lu,2,3,* Wenjing Li2,3,*
1Department of Orthopedics, The Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou Municipal Hospital, Gusu School, Nanjing Medical University, Suzhou, People’s Republic of China; 2Department of Clinical Laboratory, The Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou Municipal Hospital, Gusu School, Nanjing Medical University, Suzhou, People’s Republic of China; 3Suzhou Key Laboratory of Intelligent Critical Illness Biomarkers Translational Research, Suzhou, People’s Republic of China; 4Medical Research Center, Key Laboratory of Digital Technology in Medical Diagnostics of Zhejiang Province, Hangzhou, People’s Republic of China; 5Sino-American Joint Academic Program, Pacelli Xuzhou Campus, Xuzhou No.1 Middle School, Xuzhou, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wenjing Li, Email [email protected] Han Lu, Email [email protected]
Background: Staphylococcus argenteus, a member of the Staphylococcus aureus complex, has increasingly been recognized as a human pathogen but is frequently misidentified as S. aureus in routine clinical laboratories. Reports of prosthetic joint infection (PJI) caused by this species remain rare.
Methods: We describe a case of delayed-onset PJI in a 71-year-old woman following total knee arthroplasty. Repeated conventional cultures were negative after empirical vancomycin therapy. Metagenomic next-generation sequencing (mNGS) of wound exudate detected S. argenteus, which guided extended culture and subsequent isolation of low-abundance colonies. Species identification was confirmed by whole-genome sequencing (WGS), multilocus sequence typing (MLST), and reinterpretation of MALDI-TOF MS results. Antimicrobial susceptibility testing (AST) was performed and compared with WGS-based resistance prediction. Phylogenetic analysis was conducted using 452 publicly available S. argenteus genomes.
Aim: This study aimed to describe the clinical diagnosis, microbiological identification, and genomic characterization of a Staphylococcus argenteus strain causing prosthetic joint infection.
Results: The isolate was identified as sequence type ST2250 and lacked the staphyloxanthin operon, consistent with the non-pigmented phenotype. WGS and phenotypic AST showed 100% concordance across 11 clinically relevant antibiotics. Phylogenomic analysis revealed that the strain clustered closely with Southeast Asian lineages. Following targeted therapy with intravenous vancomycin and surgical wound management, the patient showed rapid clinical improvement with resolution of local inflammation and complete wound healing.
Conclusion: This is the first confirmed case of S. argenteus PJI in Suzhou, China. The case highlights the diagnostic value of mNGS in culture-negative PJI, the importance of molecular tools for correctly differentiating S. argenteus from S. aureus, and the potential of WGS to support resistance prediction for rare staphylococcal pathogens.
Keywords: Staphylococcus argenteus, prosthetic joint infection, mNGS, whole-genome sequencing, antimicrobial susceptibility, ST2250
Introduction
Staphylococcus argenteus is a recently recognized member of the Staphylococcus aureus complex and was formerly classified as clonal complex 75 of S. aureus. Although genetically related to S. aureus,1,2 S. argenteus lacks the carotenoid pigment operon (crtOPQMN) and is therefore non-pigmented. Traditional biochemical identification and MALDI-TOF MS often misclassify it as S. aureus, complicating surveillance and clinical management. Over the past decade, S. argenteus has been increasingly reported across Southeast Asia, Australia, and parts of Europe and the Americas. Molecular epidemiological studies suggest that certain sequence types are geographically clustered, reflecting regional transmission patterns and lineage expansion.3 It is associated with skin and soft tissue infections, bacteremia, osteomyelitis, and, rarely, prosthetic joint infections (PJI).4–7 Although PJI are most commonly caused by Staphylococcus aureus and coagulase-negative staphylococci, rare members of the S. aureus complex such as S. argenteus may also act as opportunistic pathogens, particularly in patients with implanted orthopedic devices. The epidemiology, virulence determinants, and antimicrobial resistance characteristics of S. argenteus show considerable diversity across different sequence types (STs). Previous molecular epidemiological studies have demonstrated genotype-specific virulence and resistance profiles, such as the presence of enterotoxin sey in ST2250, while ST1223 commonly carries seb and enterotoxin gene clusters (egc), and ST2198 exhibits higher resistance rates to penicillin, macrolides, and aminoglycosides compared with other lineages.8,9 Prosthetic joint infections caused by uncommon staphylococcal species pose a diagnostic challenge, especially when routine cultures are negative due to prior antibiotic exposure or low bacterial burden.5,10,11 Metagenomic next-generation sequencing (mNGS) and whole-genome sequencing (WGS) provide valuable support for species identification and resistance profiling in these situations.
Here, we describe the clinical course, microbiological workup, WGS characterization, and phylogenomic context of an ST2250 S. argenteus strain isolated from a case of delayed-onset PJI. This is, to our knowledge, the first reported case from Suzhou, China. The genotype–phenotype concordance observed in antimicrobial susceptibility testing further provides evidence supporting the integration of genome-based resistance prediction for rare staphylococci.
Methods
Patient and Clinical Assessment
A 71-year-old woman with a history of right knee osteoarthritis underwent total knee arthroplasty in March 2023. On 3 August 2025, she presented with progressive knee swelling, erythema, purulent exudation, and pain (Figure 1A), and admitted to our hospital. Laboratory evaluation revealed normal leukocyte count, CRP, and PCT but elevated ESR (62 mm/h). Radiographs showed a well-positioned prosthesis without evidence of loosening. Three consecutive microbial cultures (performed on August 3, 4, and 7) failed to isolate pathogenic bacteria. However, Staphylococcus argenteus was detected by mNGS on August 6. Upon admission, the patient was started on empirical vancomycin (1.0 g q12h) for anti-infective therapy, along with wound dressing changes. The wound on the patient’s right knee had fully healed by August 18, when she was discharged from the hospital.
 |
Figure 1 (A) Wound after debridement. (B) Culture results of Staphylococcus argenteus. After 24 hours on blood agar, Staphylococcus argenteus forms silvery-white, circular, convex colonies (2–3 mm in diameter) with entire edges and an opaque, moist texture. Beta-hemolysis is typically present, but the colonies lack the golden pigment characteristic of S. aureus. (C) Comparison of phenotypic antimicrobial susceptibility and whole-genome sequencing-based resistance predictions for S. argenteus ST2250. Green indicates susceptibility (S), red indicates resistance (R). (D) Global phylogenetic tree of S. argenteus. Circular maximum-likelihood tree constructed from whole-genome SNPs, showing geographic distribution of 452 strains. Colors represent different global regions. The triangle marker indicates strain SZ01. (E) Phylogenetic tree of S. argenteus strains in Asia. Rectangular layout with regional color coding, distinguishing Chinese cities (eg, Suzhou, Shanghai, Guangdong) and countries in Asia. The triangle marker indicates strain SZ01. |
According to the European Bone and Joint Infection Society (EBJIS) standards,12 the diagnostic basis primarily falls into four categories: clinical, laboratory, microbiological, and histopathological. In this case, the clinical diagnosis of PJI was established based on the findings of a knee swelling, erythema, purulent exudation, elevated ESR, and the result of mNGS.
Sample Collection and Microbiological Culture
The specimens were inoculated onto blood agar plates and incubated under aerobic conditions at 35°C. Wound exudate samples were collected on August 3, 4, and 7. Routine bacterial cultures were negative (<5 CFU observed) following empirical vancomycin administration. A repeat wound exudate sample collected on August 5 was cultured for 48 hours, yielding two non-pigmented colonies. Initial identification was performed using a MALDI-TOF MS system (Bruker Biotyper, Bruker Daltonics, Germany). The database version used in this study was DB 5989. Due to limited reference spectra for S. argenteus in earlier databases, misidentification as S. aureus may occur.
Metagenomic Next-Generation Sequencing (mNGS)
DNA extracted from the August 5 specimen was sequenced on the MGI-Seq200 platform (single-end, 60 bp). High-quality reads were aligned to microbial databases (RefSeq and NT) for pathogen identification and resistance gene detection.
Whole-Genome Sequencing and MLST
Whole-genome sequencing was performed on a single isolate obtained from the patient sample. The isolate was purified by subculturing, and genomic DNA was extracted from a pool of three individual colonies to ensure sufficient yield and minimize potential heterogeneity. Sequencing was then carried out on the MGIseq-200 platform, and analyzed for MLST, virulence factors, and resistance genes using established databases (ResFinder, PubMLST). Average nucleotide identity and gene presence/absence analyses were performed.
Antimicrobial Susceptibility Testing (AST)
Phenotypic AST was performed using the VITEK 2 AST-GP P639 card and interpreted according to CLSI standards. WGS-based resistance predictions were compared against phenotypic results.
Phylogenetic and Source-Tracing Analysis
A total of 468 publicly available S. argenteus genomes were retrieved from NCBI. After quality filtering, 452 high-quality entries were used for whole-genome SNP phylogenetic reconstruction. Maximum-likelihood trees were generated to evaluate geographic clustering and relatedness to the Suzhou strain (SZ01).
Results and Analysis
Clinical Course
The patient exhibited signs of delayed-onset PJI. Despite multiple negative cultures, mNGS of wound exudate identified S. argenteus. Following targeted therapy with vancomycin 1 g every 12 hours, there was rapid improvement in erythema, swelling, and ulcer healing.
Bacterial Isolation and Species Identification
Extended culture yielded two hemolytic, non-pigmented colonies that MALDI-TOF MS initially misidentified as S. aureus with low confidence score (Figure 1B). WGS confirmed the isolate as S. argenteus and assigned it to ST2250. The strain lacked the crtOPQMN operon (a bacterial gene cluster responsible for the biosynthesis of carotenoid pigments, particularly staphyloxanthin, which contributes to the golden color and oxidative stress resistance in pathogens like Staphylococcus aureus.), consistent with the non-pigmented colony phenotype characteristic of S. argenteus.
Antimicrobial Susceptibility and Genotype–Phenotype Concordance
The isolate was susceptible to oxacillin, vancomycin, teicoplanin, gentamicin, fluoroquinolones, clindamycin, linezolid, rifampicin, tigecycline, and TMP–SMX (trimethoprim–sulfamethoxazole) but resistant to penicillin (Table 1). Phenotypic and genotypic AST results were concordant for all 11 antibiotics tested (Figure 1C), supporting the accuracy of WGS-based resistance prediction for this lineage.
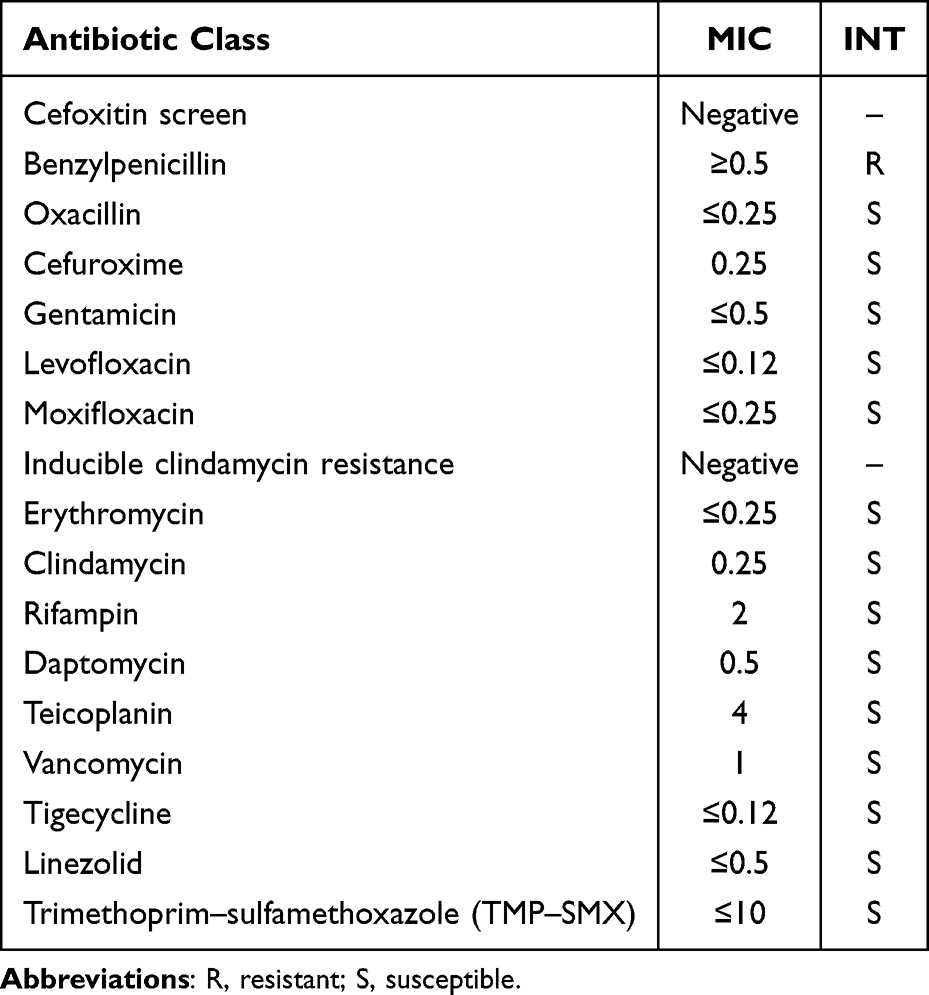 |
Table 1 Antimicrobial Sensitivity Test Results |
Genome analysis revealed the presence of several virulence-associated genes, including immune evasion cluster proteins (Sak and Scn). Antimicrobial resistance gene blaZ was identified. No major antimicrobial resistance genes such as mecA, mecC, or vancomycin resistance determinants were detected. These findings were consistent with the phenotypic antimicrobial susceptibility results.
Phylogenomic Context
Among 452 reference genomes, the Suzhou strain clustered with Southeast Asian ST2250 isolates, especially strains from Indonesia and Vietnam (Figure 1D and E). This suggests a potential regional origin or transmission link, although direct epidemiological data were lacking.
Discussion
This study reports the first-confirmed case of prosthetic joint infection caused by S. argenteus ST2250 in Suzhou, China. The case underscores several important diagnostic and clinical considerations.
First, S. argenteus is easily overlooked in orthopedic infections. Its close resemblance to S. aureus and its non-pigmented appearance can result in misclassification by routine biochemical and mass spectrometry methods.13 In this case, low colony counts following empirical antibiotic therapy contributed to repeated false-negative cultures, emphasizing the need for extended culture and molecular confirmation in suspected PJI.
Second, mNGS proved essential for pathogen detection in the setting of low bacterial burden. By identifying S. argenteus when conventional culture initially failed to identify the pathogen, mNGS guided subsequent targeted culture and enabled definitive species-level confirmation through WGS. Such workflows may significantly improve diagnostic accuracy in culture-negative PJI.
Third, the perfect concordance between phenotypic AST and WGS-based resistance prediction highlights the potential role of genome-based antimicrobial profiling in rare or emerging staphylococci. Although broader validation across species is still required, the results support the use of WGS as a complementary tool in diagnostic microbiology.
Finally, several cases of S. argenteus infections have been reported worldwide, including bacteremia, skin and soft tissue infections, and osteomyelitis.14 However, prosthetic joint infections caused by S. argenteus remain extremely rare. Söderquist et al10 previously reported a case of hip prosthetic joint infection caused by S. argenteus in Sweden, highlighting the diagnostic challenges posed by this species. Similar to our findings, conventional identification methods initially misclassified the isolate as S. aureus. Misidentification may obscure the true epidemiology of S. argenteus infections and may affect surveillance and clinical recognition of this emerging pathogen.
Compared with previously reported isolates, the ST2250 lineage identified in this study clustered with Southeast Asian strains, which is consistent with earlier genomic studies suggesting that S. argenteus is widely distributed in Southeast Asia.15 These findings further support the importance of genomic surveillance to better understand the global epidemiology and transmission patterns of this emerging pathogen.
This study has several limitations. First, it represents a single case report and therefore cannot provide definitive conclusions regarding the epidemiology of S. argenteus PJI. Second, although phylogenomic analysis suggested clustering with Southeast Asian lineages, epidemiological linkage could not be established. Third, interpretation of mNGS results may be challenging in low-biomass samples and should always be considered alongside clinical findings.
Conclusions
This report describes a rare case of prosthetic joint infection caused by S. argenteus ST2250. The pathogen was initially detected by metagenomic next-generation sequencing and subsequently confirmed by whole-genome sequencing. This case highlights the diagnostic challenges in distinguishing S. argenteus from Staphylococcus aureus using routine microbiological methods and underscores the value of molecular approaches in culture-negative infections. Improved recognition of S. argenteus may enhance pathogen identification and understanding of its role in orthopedic infections.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author (Wenjing Li, [email protected]) upon reasonable request.
Ethical Statement
According to the policies of Suzhou Municipal Hospital, ethical approval was not required for the publication of this case report.
Consent to Participate
Written informed consent was obtained from the patient.
Consent for Publication
The patient has provided written informed consent for the case details and images to be published.
Acknowledgments
The authors thank the clinical and laboratory teams at the Affiliated Suzhou Hospital of Nanjing Medical University for their support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This work is supported by the General Program of Jiangsu Commission of Health (Grant No. MQ2024016) and National Natural Science Foundation of China (Grant No.82502817).
Disclosure
The authors declare that there are no financial or personal relationships that could inappropriately influence (bias) their work.
References
1. Mcdonald M, Dougall A, Holt D, et al. Use of a single-nucleotide polymorphism genotyping system to demonstrate the unique epidemiology of methicillin-resistant Staphylococcus aureus in remote aboriginal communities. J Clin Microbiol. 2006;44(10):3720–7. doi:10.1128/JCM.00836-06
2. Holt DC, Holden MT, Tong SY, et al. A very early-branching Staphylococcus aureus lineage lacking the carotenoid pigment staphyloxanthin. Genome Biol Evol. 2011;3:881–895. doi:10.1093/gbe/evr078
3. Becker K, Schaumburg F, Kearns A, et al. Implications of identifying the recently defined members of the Staphylococcus aureus complex S. argenteus and S. schweitzeri: a position paper of members of the ESCMID Study Group for Staphylococci and Staphylococcal Diseases (ESGS). Clin Microbiol Infect. 2019;25(9):1064–1070. doi:10.1016/j.cmi.2019.02.028
4. Zhang DF, Zhi XY, Zhang J, et al. Preliminary comparative genomics revealed pathogenic potential and international spread of Staphylococcus argenteus. BMC Genomics. 2017;18(1):808. doi:10.1186/s12864-017-4149-9
5. Thaipadungpanit J, Amornchai P, Nickerson EK, et al. Clinical and molecular epidemiology of Staphylococcus argenteus infections in Thailand. J Clin Microbiol. 2015;53(3):1005–1008. doi:10.1128/JCM.03049-14
6. Tong SYC, Schaumburg F, Ellington MJ, et al. Novel staphylococcal species that form part of a Staphylococcus aureus-related complex: the non-pigmented Staphylococcus argenteus sp. nov. and the non-human primate-associated Staphylococcus schweitzeri sp. nov. Int J Syst Evol Microbiol. 2015;65(Pt 1):15–22. doi:10.1099/ijs.0.062752-0
7. Bank LEA, Bosch T, Schouls LM, et al. Methicillin-resistant Staphylococcus argenteus in the Netherlands: not a new arrival. Eur J Clin Microbiol Infect Dis. 2021;40(7):1583–1585. doi:10.1007/s10096-021-04204-7
8. Aung MS, Urushibara N, Kawaguchiya M, et al. Distribution of virulence factors and resistance determinants in three genotypes of Staphylococcus argenteus clinical isolates in Japan. Pathogens. 2021;10(2):163. doi:10.3390/pathogens10020163
9. Tun T, Baleivanualala SC, Erdmann MB, et al. An extensively drug-resistant Pseudomonas aeruginosa isolate from Myanmar. J Glob Antimicrob Resist. 2024;36:1–3. doi:10.1016/j.jgar.2023.11.004
10. Soderquist B, Wildeman P, Stenmark B, et al. Staphylococcus argenteus as an etiological agent of prosthetic Hip joint infection: a case presentation. J Bone Jt Infect. 2020;5(4):172–175. doi:10.7150/jbji.44848
11. Gatti G, Taddei F, Marzucco A, et al. Isolation and genomic analysis of a case of Staphylococcus argenteus ST2250 related to sepsis in Italy. Microorganisms. 2024;12(7):1485. doi:10.3390/microorganisms12071485
12. Jesry F, Pandit H, Clarke D, et al. Skin temperature change following infected and non-infected total knee arthroplasty: a systematic review. Cureus. 2025;17(5):e84549. doi:10.7759/cureus.84549
13. Verschuuren T, Bosch T, Mascaro V, et al. External validation of WGS-based antimicrobial susceptibility prediction tools, KOVER-AMR and ResFinder 4.1, for Escherichia coli clinical isolates. Clin Microbiol Infect. 2022;28(11):1465–1470. doi:10.1016/j.cmi.2022.05.024
14. Becker K, Both A, Weißelberg S, et al. Emergence of coagulase-negative staphylococci. Expert Rev Anti Infect Ther. 2020;18(4):349–366. doi:10.1080/14787210.2020.1730813
15. Moradigaravand D, Jamrozy D, Mostowy R, et al. Evolution of the Staphylococcus argenteus ST2250 clone in Northeastern Thailand is linked with the acquisition of livestock-associated Staphylococcal genes. mBio. 2017;8(4). doi:10.1128/mBio.00802-17
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Maternal–Fetal Listeriosis in China: Clinical and Genomic Characteristics From an ST8 Listeria monocytogenes Case
Hu G, Yan W, Dong F, Li G, Zhang X, Li Q, Zhang P, Ji L
Infection and Drug Resistance 2025, 18:1313-1324
Published Date: 8 March 2025